 Dalma Dobszai1,2Mahmoud Obeidat2Eszter Ágnes Szalai2,3Dániel Sándor Veres2,4Luca Havelda2,5Renáta Papp2,6,7Alim Choi2Bettina Csilla Budai2,5Dominika Csajbók2
Dalma Dobszai1,2Mahmoud Obeidat2Eszter Ágnes Szalai2,3Dániel Sándor Veres2,4Luca Havelda2,5Renáta Papp2,6,7Alim Choi2Bettina Csilla Budai2,5Dominika Csajbók2 Péter Hegyi1,2,5,8†
Péter Hegyi1,2,5,8† Andrea Szentesi1,2*†
Andrea Szentesi1,2*†- 1Institute for Translational Medicine, Medical School, University of Pécs, Pécs, Hungary
- 2Centre for Translational Medicine, Semmelweis University, Budapest, Hungary
- 3Department of Restorative Dentistry and Endodontics, Semmelweis University, Budapest, Hungary
- 4Department of Biophysics and Radiation Biology, Semmelweis University, Budapest, Hungary
- 5Institute of Pancreatic Diseases, Semmelweis University, Budapest, Hungary
- 6Department of Pharmacology and Pharmacotherapy, Semmelweis University, Budapest, Hungary
- 7Center for Pharmacology and Drug Research and Development, Semmelweis University, Budapest, Hungary
- 8Translational Pancreatology Research Group, Interdisciplinary Centre of Excellence for Research Development and Innovation, University of Szeged, Szeged, Hungary
Introduction: The obesity epidemic has led to a rise in related health conditions, with metabolic syndrome (MS) affecting 25% of Western populations. In severe acute pancreatitis (AP), mortality can reach 50%. Previous studies have linked MS elements to increased complications and mortality in AP. This meta-analysis aims to identify potential risk factors and their synergistic effects on AP outcomes.
Methods: We systematically searched PubMed, Embase, and the Cochrane Library up to November 1, 2023, and included studies based on predefined criteria. We examined the impact of MS and its factors (obesity, hypertension, diabetes mellitus, and hypertriglyceridemia) on AP outcomes, calculating pooled odds ratios (OR) with 95% confidence intervals (CIs). The protocol was registered in PROSPERO under number CRD42023471092.
Results: Out of 15,904 records, 89 studies were analyzed. Overweight and obesity were significant risk factors for complications (local OR: 2.677, 95%CI: 1.421-5.044; systemic OR: 2.404, 95%CI: 1.481-3.901) and severe AP (BMI≥30 kg/m2, OR: 3.058, 95%CI: 1.369-6.829). High triglyceride levels were associated with ICU admission (OR: 2.546, 95%CI: 1.529-4.237) and severe AP (OR: 2.686, 95%CI: 1.205-5.989); hypertension increased mortality (OR: 2.135, 95%CI: 1.870-2.437), while diabetes increased the odds of ICU admission (OR: 1.645, 95%CI: 1.358-1.992) and severe AP (OR: 1.49, 95%CI: 1.09-2.03). We found a non-significant trend toward increased odds of severe AP among patients with MS (OR = 1.398, 95% CI: 0.918–2.129).
Conclusion: Individual components of MS are risk factors for complications, severity, and mortality in AP. Lifestyle counseling, education, and treatment of patients with obesity is crucial.
Systematic Review Registration: https://www.crd.york.ac.uk/prospero/, identifier CD42023471092.
1 Introduction
Acute pancreatitis (AP) is a potentially life-threatening gastrointestinal condition requiring hospitalization, with its overall incidence increasing by 3% annually over the past 50 years, placing a huge burden on national healthcare systems (1). While improvements in diagnostic tools and criteria have contributed to this rise, lifestyle factors such as sedentary behavior, poor nutrition, increased alcohol consumption, medication use, smoking, and socioeconomic status also play a major role (1–3). AP can lead to various local and systemic complications linked to pre-existing conditions, with severe cases resulting in organ failure (4). Patients going through transient organ failure or developing local/systemic complications without organ failure are classified as moderately severe, whereas severe cases are characterized by persistent organ failure (4).
Globally, up to 39% of the population is classified as obese or overweight. Since the 1970s, the prevalence of obesity has risen threefold, making it the fifth leading cause of death worldwide (5). Obesity is associated with a greater risk of inpatient mortality, higher hospitalization costs, and overall poorer clinical outcomes in cases of AP (6). A meta-analysis covering all BMI categories revealed that a BMI≥25 elevates the risk of severe AP without impacting mortality, whereas a BMI greater than 30 is linked to increased mortality risk (7). Additionally, our previous cohort analysis identified obesity as an independent predictor of renal failure and prolonged hospital stay (8).
Obesity significantly increases the risk of various chronic comorbidities (such as type 2 diabetes mellitus, dyslipidemia, hypertension, and cancer) (9) that often correlate with poorer outcomes in acute inflammatory conditions (10–13). In particular, visceral fat accumulation is linked to numerous cardiovascular issues as well as increased fat deposits in the liver, muscle, and pancreas (5).
Metabolic syndrome (MS) covers a range of interrelated metabolic disorders that significantly elevate the risk for cardiovascular diseases and overall mortality (14). While definitions vary (15), it typically involves the presence of at least three of the following four conditions: abdominal obesity, impaired glucose metabolism, hypertension, and dyslipidemia. The incidence of MS has sharply risen in recent decades, raising significant public health concerns worldwide (16). The development of MS is influenced by various factors, with lifestyle choices—particularly poor dietary habits and lack of physical activity—playing a crucial role alongside genetic and environmental influences (17).
Given the potentially fatal nature of AP and its complications, the early identification of patients at high risk of developing severe forms of the disease is critically important. To be able to create preventive treatments for severe AP in the future, there is a desperate need to determine the risk of complications and predict severity using the information available upon admission, but at most within the first 24 hours of hospital admission (18).
Earlier studies have associated the components of MS with a higher chance of developing severe AP and an increased risk of mortality (7, 8, 13), however, no comprehensive meta-analysis was carried out to evaluate both the individual and synergistic effects of these factors. This article aims to investigate the interplay between MS and AP and explore their potential implications for clinical practice and public health.
2 Methods
We conducted our meta-analysis following the recommendations of the Cochrane Handbook (19) and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guideline (20) (Supplementary Table S1). The protocol was registered on PROSPERO (21) (CRD42023471092), and we fully adhered to it. The research project is conducted under the Systems Education education-research model coordinated by the Centre for Translational Medicine at Semmelweis University (22).
2.1 Eligibility criteria
Eligibility criteria was determined according to the Population Exposure and Outcome (PEO) framework (23). We included studies reporting on adult patients with AP (P) and included MS and its four elements individually: obesity, hypertriglyceridemia (HTG), diabetes mellitus, and hypertension (E). Our outcomes (O) of interest were AP severity, in-hospital mortality, presence of local pancreatic complications (necrosis, fluid collection, pseudocyst), systemic complications (organ failure), and the need for Intensive Care Unit (ICU) admission. Articles in all languages and from all publication years were included to provide the most comprehensive overview possible. Studies reporting data on pediatric population, conference abstracts, case reports, case series, reviews, and meta-analyses were excluded. No other filters were used.
2.2 Search strategy
We systematically searched PubMed, Embase and the Cochrane Library on November 1, 2023. The search strategy combined terms related to acute pancreatitis and metabolic syndrome or its individual components (e.g., obesity, diabetes, hypertriglyceridemia, hypertension). The complete search strings for each database are provided in Supplementary Methods S1. No language or other restrictions were applied during the literature search. References of the included articles from the original pool investigating the effect of MS on AP outcome were also screened.
2.3 Selection process
After automatic and manual duplicate removal, the selection was performed first according to title and abstract using a specific selection tool (Rayyan) (24), then by full-text content by four independent reviewers (D.D. with A.C. and L.H. with D.C.). Cohen’s kappa coefficient was calculated after every selection step to assess the amount of disagreements that a third (B.Cs.B) independent reviewer subsequently solved.
2.4 Data collection process
The same four independent reviewers manually collected data and cross-checked it to ensure its quality using a standardized collection sheet. The extracted data included information about the study (first author, year of publication, country of origin, study design), demographic data (sample size, sex and age distribution), information on the exposure and the applied definition to determine its presence, and details about the outcomes (definition, frequency, time of measurement). We extracted the raw numbers, or the available odds ratios (ORs) and the corresponding 95% confidence intervals (CIs) as reported.
When analyzing the effect of overweight and obesity, we pooled all patients with a BMI over the normal range and created the group of patients with excess body weight (EBW).
We divided the included articles into two groups based on the applied cut-off value to determine HTG in AP patients. The first group contained articles where all elevated serum triglyceride levels above 150 mg/dL were included; we named it as “AP with HTG” group (8, 25–35). The second group consisted of studies where the exposed patients were diagnosed with “HTG-induced AP” (36–47) (triglyceride level at least 1000 mg/dL or 500 mg/dL with lactescent serum).
2.5 Risk of bias assessment
For the risk of bias assessment, we used the Quality in Prognostic Studies (QUIPS) tool (48). The evaluated domains included the number of study participants, study attrition, measurement of prognostic factors, outcome measurement, study confounding, and statistical analysis and reporting.
2.6 Synthesis methods
As we assumed considerable between-study heterogeneity in all cases, a random-effects model was used to pool effect sizes.
Odds ratio (OR) was used as the pooled effect size measure in our meta-analyses. To calculate the odds ratios and the pooled odds ratio, the total number of patients and those with the event of interest in each group (with and without MS, HTG, hypertension, diabetes or obesity) separately was extracted from the studies. We reported the results as the odds of event of interest in the “MS” group versus the odds of event of interest in the “no MS” group. We also reported the risks and risk differences for the individual studies for easier interpretation.
Some articles reported BMI, subcutaneous adipose tissue (SAT), and visceral adipose tissue (VAT) values across groups with different severities of pancreatitis. However, not all articles provided data for each severity group, and we aimed to compare all three severity categories. Therefore, as an additional form of analysis, we used a three-level (multilevel) meta-analysis model for these analyses.
Results were considered statistically significant if the pooled confidence interval (CI) did not contain the null value. We summarized the findings related to meta-analysis on forest plots. Between-study heterogeneity was described by the between-study variance (τ2) and the Higgins & Thompson’s I2 statistics too (49). We reported the prediction interval if at least eight studies were available for the meta-analysis.
The R software (50) was used for all statistical analyses with the meta (51) package for basic meta-analysis calculations and plots, and the dmetar (52) package for additional influential analysis calculations and plots. We reported additional, detailed information on calculations, data synthesis, publication bias assessment and influential analyses in Supplementary Methods S2. In this study, we examined the effects of MS and its components on AP outcomes through multiple analyses. Due to limitations on the number of figures and results that can be presented, we have included the most relevant findings in the main manuscript. Additional analyses and results, while not fully represented, are summarized and discussed in the Supplementary Materials for further reference.
3 Results
3.1 Search and selection
Our systematic search returned a total of 19,766 articles, and following automatic and manual duplicate removal, 15,904 records were screened. We assessed 392 full texts according to pre-defined eligibility criteria, the details of which are reported in Supplementary Methods S3. We included 106 articles in our systematic review, and 89 studies were eligible for meta-analysis (Figure 1).
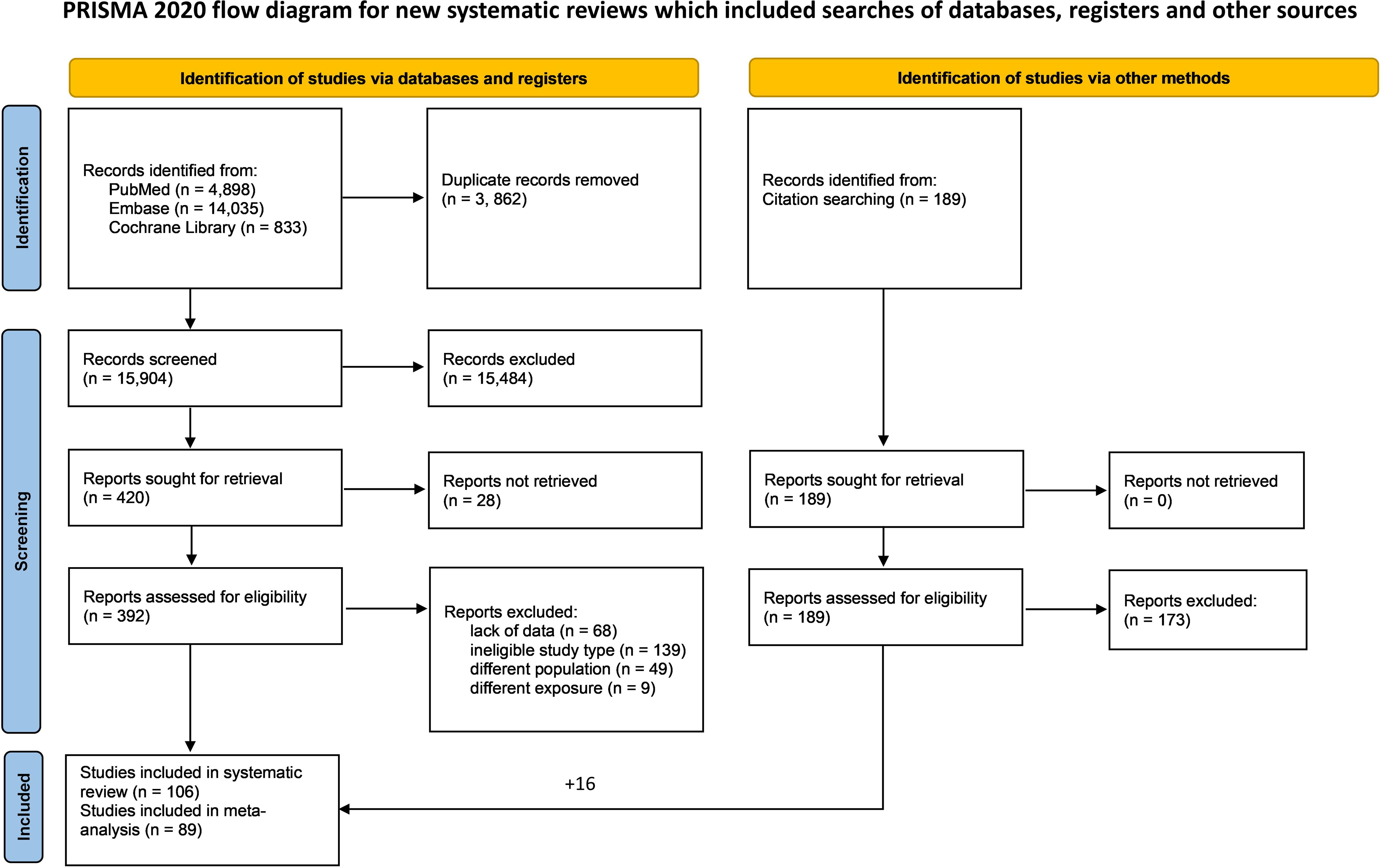
Figure 1. PRISMA flowchart of the selection process.
3.2 Basic characteristics of the included studies
We included both prospective and retrospective observational studies. The sample sizes of the included articles ranged between 85 and 1,330,302. The definition of the investigated exposures was slightly different among the involved studies in some cases, so we performed subgroup analyses based on the applied method. In total, only 17 articles were included in the systematic review either because data reporting was ineligible to pool with the studies enrolled in the quantitative synthesis (27, 45, 53–62) or there was insufficient data on the specific exposure for statistical analysis (63–66). The basic characteristics of the enrolled studies are detailed in Supplementary Table S2.
3.3 Overweight and obesity
Seven studies (8, 67–72) including 1,814 patients reported data on the association between EBW and the development of local complications, while nine studies (8, 67–74) with a sample size of 2,616 reported on systemic complications. Overweight and obesity are found statistically significant predictors of local (OR: 2.677, CI: 1.421-5.044) (Figure 2A) and systemic (OR: 2.404, CI: 1.481-3.901) (Figure 2B) complications. Among these, renal failure (OR: 4.757, CI: 2.073-10.915) and respiratory failure (OR: 1.769, CI: 1.562-2.003) were significantly more frequent among patients with EBW (Supplementary Figures S2, S3). For disease severity and mortality, we performed a subset analysis using eligible articles that defined obesity according to the WHO’s 30 kg/m2 cut-off value. This subset involved 16 articles (8, 58, 67–71, 74–81) with an overall sample size of 4,449. We found that patients with obesity have a more than threefold increased risk of developing severe AP (OR: 3.058, CI: 1.369-6.829) (Figure 2C). The association between EBW and AP severity was also statistically significant when pooling together patients with moderately severe and severe AP – both outcomes were more common among patients with high BMI (OR: 2.276, CI: 1.353-3.828) (Supplementary Figures S4, S5).
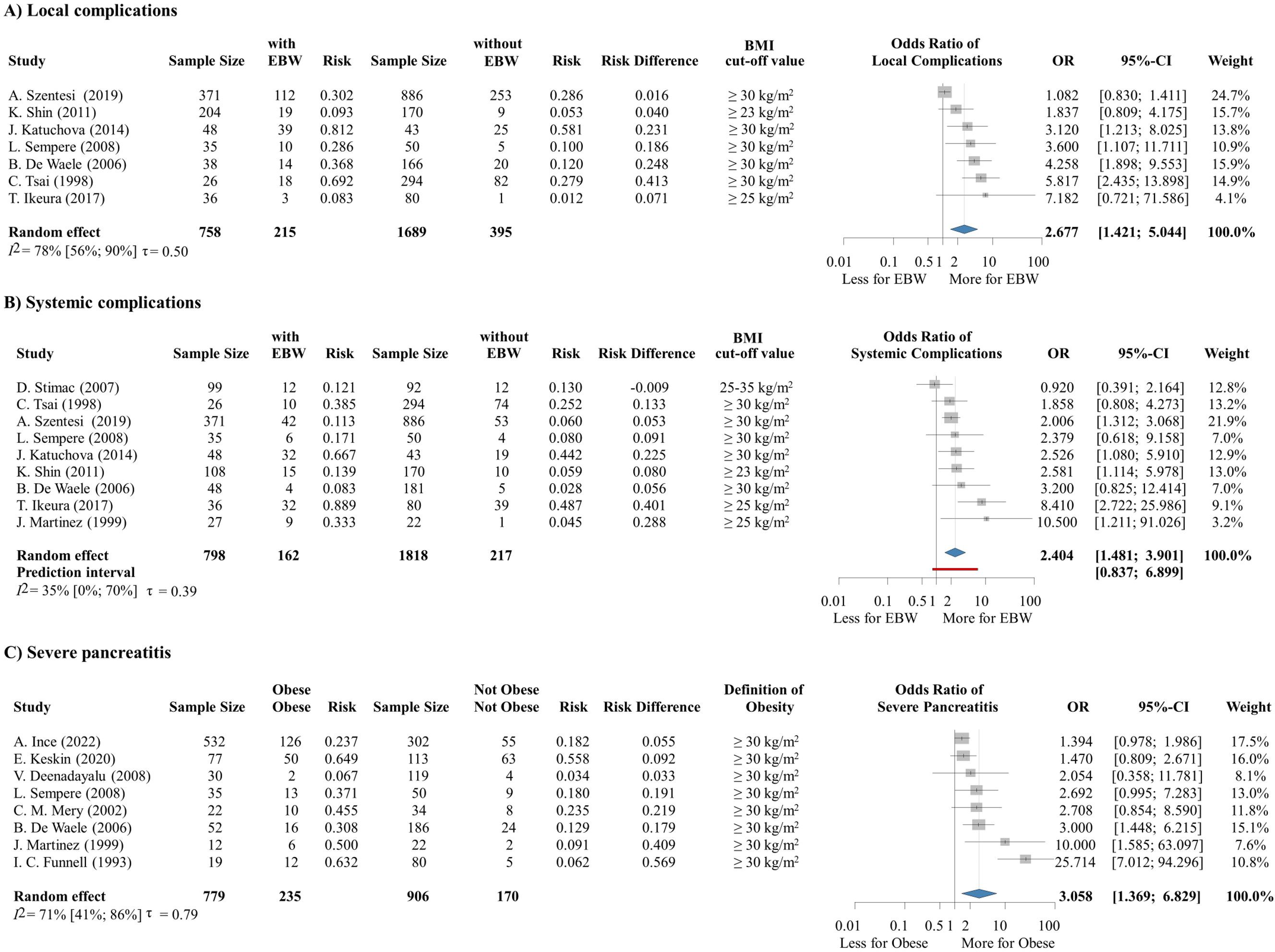
Figure 2. (A) The odds of local and (B) systemic complications is significantly increased in the group of patients with overweight or obesity. (C) The odds of developing severe AP is significantly increased among patients with obesity. EBW, excess body weight; BMI, body-mass index; OR, odds ratio; CI, confidence interval.
We compared the mean BMI of patients in different severity groups with the mean values of two CT-based body composition parameters in the same group. We found that patients with moderately severe and severe AP have higher BMI and increased amount of VAT compared to patients with mild AP, however, we did not observe a difference in the SAT volumes of the groups (Supplementary Figures S6–S9).
3.4 Hypertension
We were able to investigate the effect of pre-existing chronic hypertension on the outcome of AP based on data from 102,496 patients from 13 articles (8, 72, 82–92). According to our analysis, hypertension does not significantly increase the risk of severe AP (OR: 1.243, CI: 0.745-2.076), but it is a statistically significant predictor of mortality (OR: 2.135, CI: 1.870-2.437) (Figure 3).
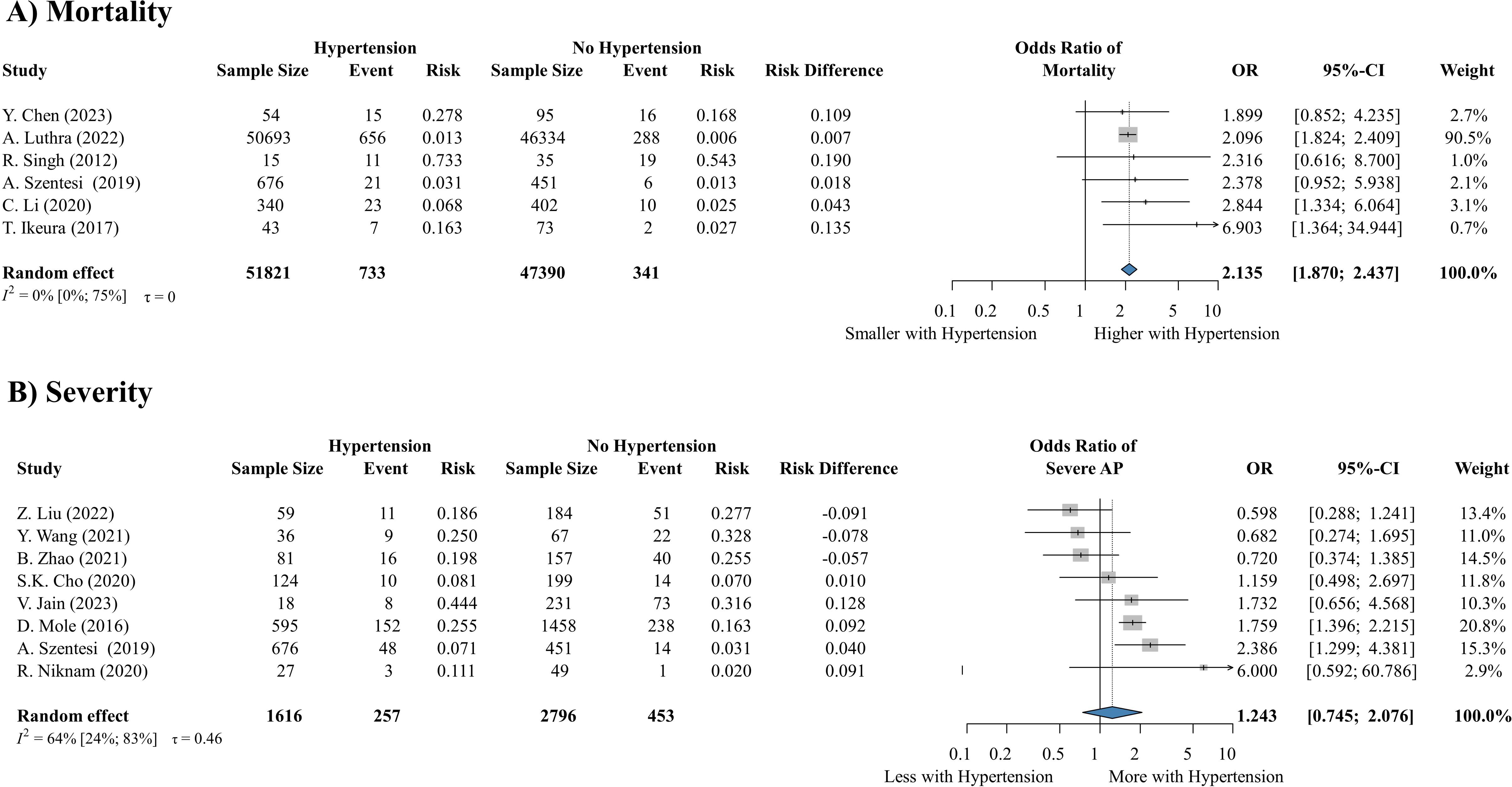
Figure 3. Hypertension significantly increases the risk of (A) mortality, but not severity (B). AP, acute pancreatitis; OR, odds ratio; CI, confidence interval.
3.5 Diabetes
In total, 11 articles (8, 27, 82, 87, 89, 92–97) containing data about 71,876 patients reported the outcomes of AP based on diabetes status. One of our major findings was that pre-existing diabetes mellitus is a risk factor of requiring ICU admission (OR: 1.645, CI: 1.358-1.992) (Figure 4A) and that of renal failure (OR: 1.370, CI: 1.164-1.612) (Figure 4B), and it remarkably increases the odds of severe AP as well (OR: 1.49, CI: 1.09-2.03) (Figure 4C). Diabetes also has a potential effect on mortality (OR: 2.373, CI: 0.320-17.570) (Supplementary Figure S10) and respiratory failure (OR: 1.159, CI: 0.653-2.058) (Supplementary Figure S11), however, these results were not statistically significant.
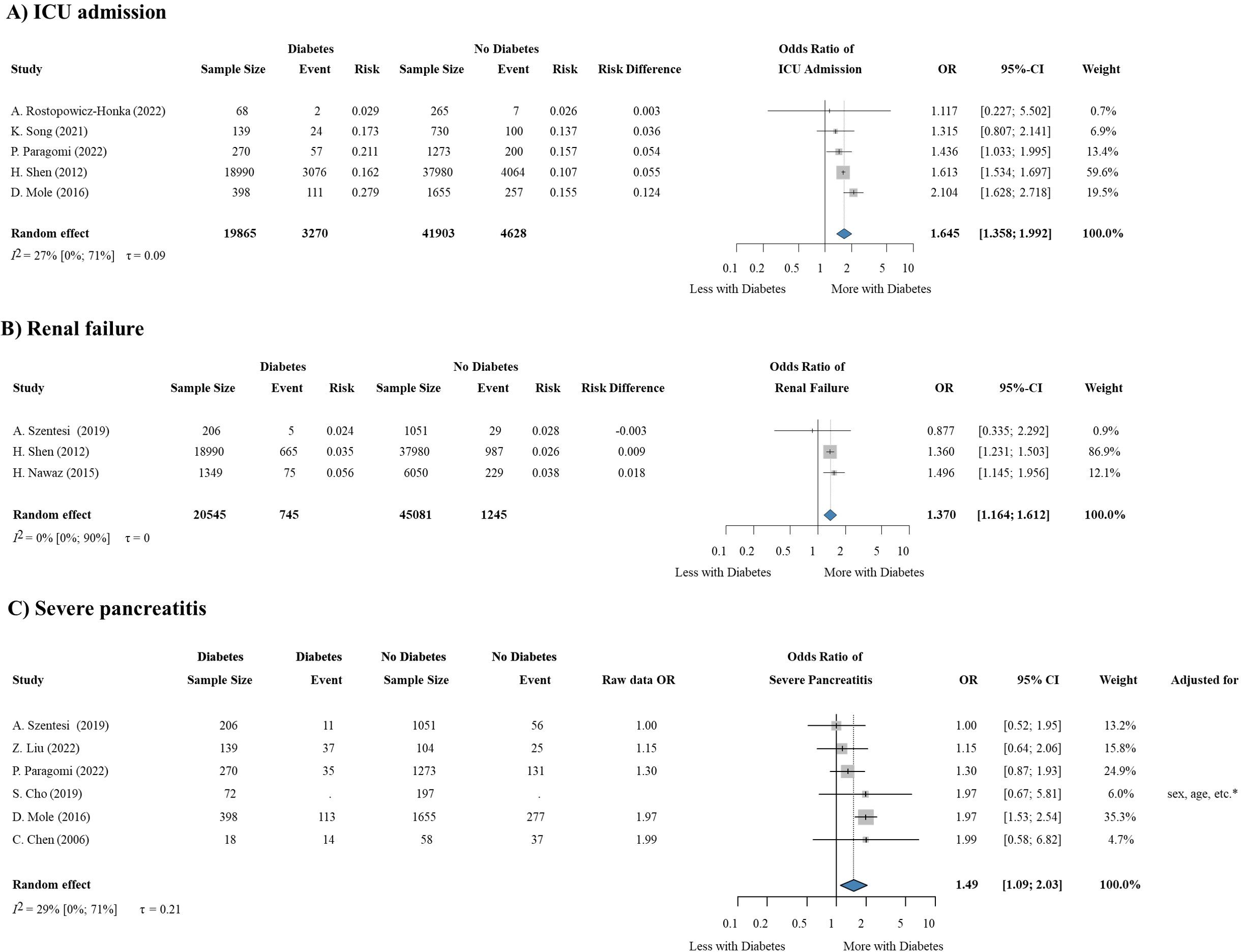
Figure 4. Diabetes is a statistically significant predictor of the need for (A) ICU admission, (B) renal failure and (C) severe pancreatitis. ICU, Intensive Care Unit; OR, odds ratio; CI, confidence interval.
3.6 Hypertriglyceridemia
3.6.1 AP with HTG
Based on 12 studies (8, 25–35) involving 291,733 patients, we could conclude that patients with elevated triglyceride levels on admission have significantly increased odds for being admitted to the ICU (OR: 2.546, CI: 1.529-4.237) (Figure 5A), progressing to the severe form of the disease (OR: 2.686, CI: 1.205-5.989) (Figure 5B) and developing necrosis (OR: 2.364, CI: 1.01-5.535) (Figure 5C).
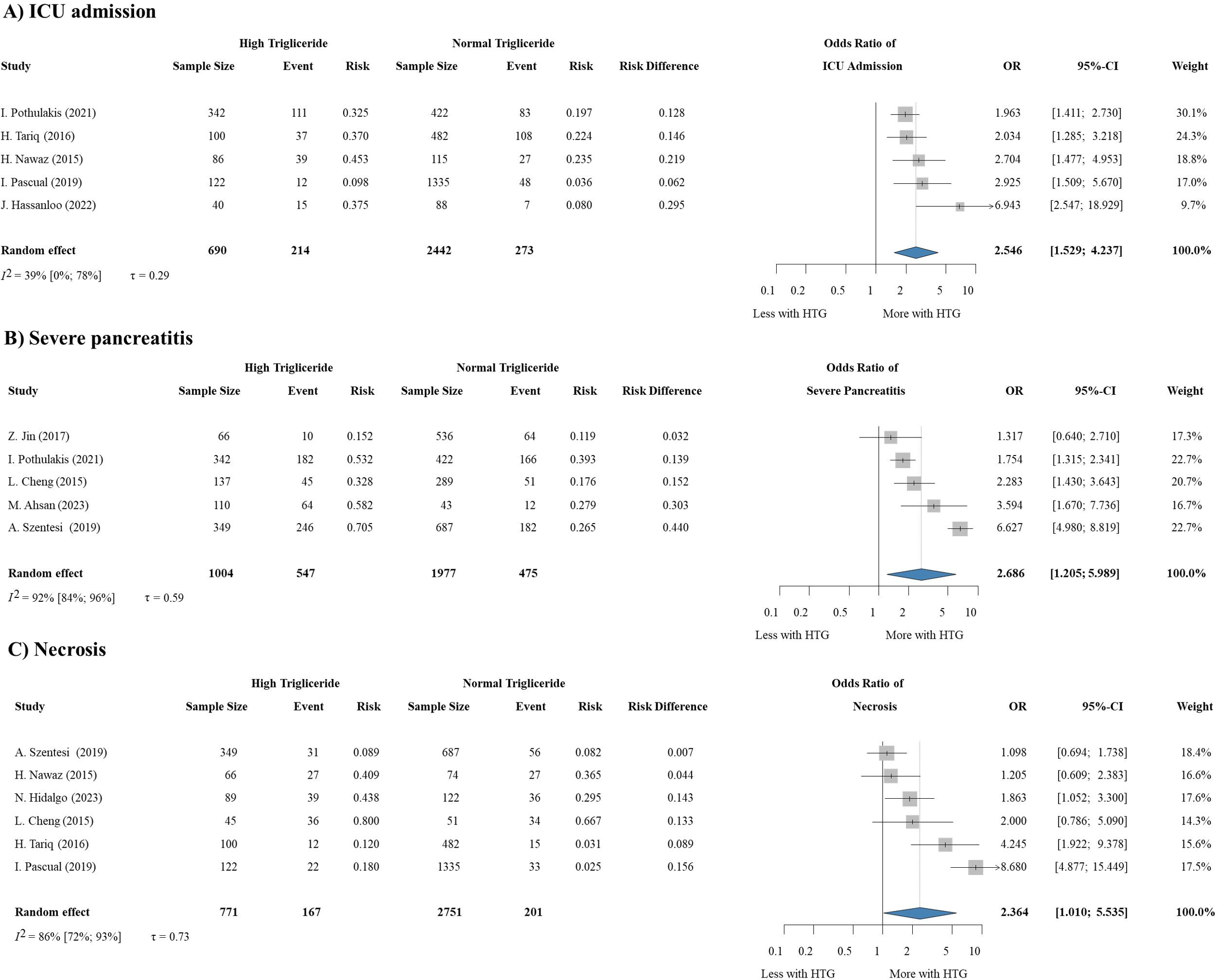
Figure 5. HTG is a predictor of (A) requiring ICU admission, (B) severity, and (C) necrosis development in AP. HTG, hypertriglyceridemia; OR, odds ratio; CI, confidence interval.
3.6.2 HTG induced AP
According to 13 studies (36–47) with an overall sample size of 581,787, patients with HTG-induced AP are more likely to have the severe form of pancreatitis (OR: 2.651, CI: 1.602-4.387) (Supplementary Figure S12) and develop necrosis during the course of the disease (OR: 1.709, CI: 1.070-2.728) (Supplementary Figure S13). HTG etiology has a potential effect on the odds of renal failure (OR: 2.780, CI: 0.531-14.547) and septic shock (OR: 1.91, CI: 0.65-5.62) as well, but these results were not statistically significant (Supplementary Figures S14, S15). The elevated risk of mortality in HTG-induced AP could not be proved in our analysis (OR: 0.987, CI: 0.490-1.988) (Supplementary Figures S16, S17).
3.7 Risk of bias assessment and sensitivity analyses
The risk of bias for attrition, prognostic factor measurement, outcome measurement, and study confounding was low in our analyses. Possible bias was observed in study participation and statistical analysis reporting. The results of our risk of bias assessment are available in Supplementary Figure S1.
Our leave-one-out analyses (where applicable) showed that no single study to be significantly influential, except for Funnel et al. (1993) (76) on the effect of obesity. Although Funnel et al. (1993) had some influence in some analyses, it did not materially change our conclusions.
3.8 Metabolic syndrome
Five articles (6, 8, 88, 98, 99) reported data on MS and AP severity (Figure 6), while 4 studies (6, 8, 88, 99) assessed the risk of mortality in the MS patient group. The overall sample size of the studies included was 137,111. Although the individual analyses of the components indicate an association between MS and AP severity, the odds of severe AP were not significantly increased in the patient group with MS (OR: 1.398, CI: 0.918-2.129) and we did not find a difference in the mortality of the exposed and non-exposed patient groups (Supplementary Figure S18).
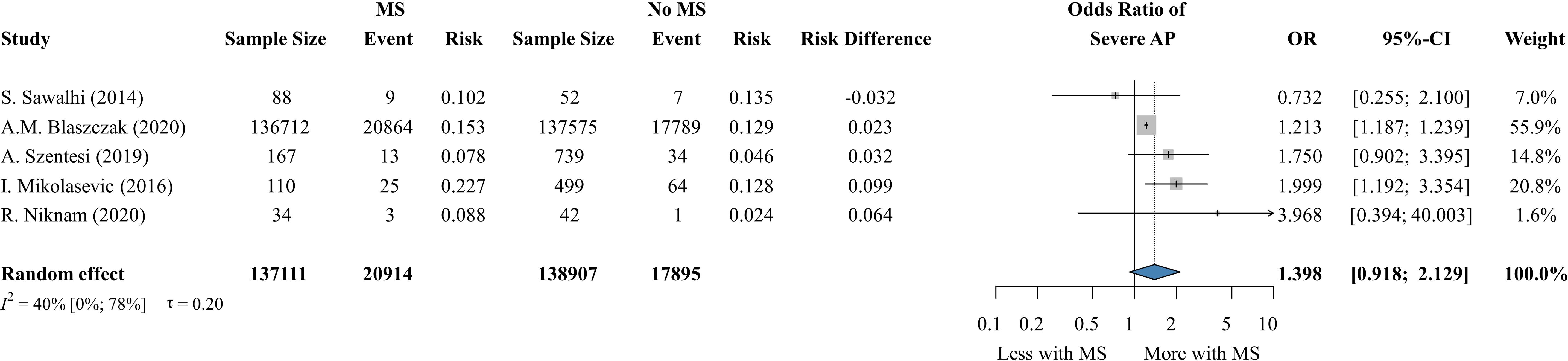
Figure 6. The risk of developing severe AP with and without MS. MS, metabolic syndrome; AP, acute pancreatitis; OR, odds ratio; CI, confidence interval.
4 Discussion
According to our analysis, all investigated individual components of MS are associated with a worse outcome in AP. In our earlier analysis, obesity was found to increase the risk of developing severe AP and even mortality (7), however our new findings highlight the connection between high BMI and the risk of both local and systemic complications.
Obesity is increasingly recognized as a significant risk factor for poorer outcomes in various health conditions due to its multifaceted impact on metabolic and inflammatory pathways. The enhanced accumulation of triglycerides and total fat in organs such as the liver and pancreas lead to insulin resistance, elevating the risk of necrosis and more severe abdominal pain, particularly in AP (100, 101). Moreover, the association between obesity and the development of diabetes is well-documented, implying a direct connection between excess body fat and metabolic dysregulation (102). Obesity is also characterized by low-grade chronic inflammation, marked by elevated levels of pro-inflammatory cytokines that can trigger systemic complications and worsen disease progression (103). Our findings support existing evidence, showing that obesity increases the risk of metabolic disorders and weakens immune responses, leading to worse clinical outcomes. Among the investigated factors, HTG was found to be a risk factor for disease severity, the need for ICU admission, and the development of necrosis, which is almost entirely in accordance with earlier analyses (11, 104). Previous studies have linked HTG to a higher risk of mortality as well. However, in our analysis, eight of the included studies found a connection between HTG and mortality in AP, while three studies (including one large retrospective cohort (30)) did not. As a result, we were unable to confirm the previous findings on this issue in our meta-analysis (Supplementary Figure S13). We were planning to analyze the prognostic role of other lipid parameters, such as high and low-density lipoproteins (HDL and LDL) as well. We did not have enough data from the included articles to perform a statistical analysis focusing on this question, but a cohort study associated abnormal cholesterol concentrations with longer hospital stay, and an elevated risk of mortality, too (66).
Preexisting diabetes was known to lead to a poor outcome of AP, and our results confirm the findings of previous studies about its role in elevating the risk of renal failure and the need for ICU admission (13).
In an earlier cohort study, hypertension was associated with an increased risk of severe AP and systemic complications (8), while we observed an elevated chance for a fatal outcome. Hypertension may exacerbate the outcome of AP through vascular and microcirculatory dysfunctions associated with chronic high blood pressure (105). Furthermore, recent studies have demonstrated that persistent hypertension elevates oxidative stress in the pancreas. This oxidative stress is a key factor in pancreatic inflammation and is ultimately linked to the onset of pancreatitis as well (106, 107).
Although the deteriorating effect of the individual MS components was clear in our analysis we did not find a significant association between MS and AP outcome. This discrepancy may be explained by the heterogeneous definitions of MS across studies, the unweighted combination of its components that may dilute the strong effect of certain factors, and the relatively small number of studies directly investigating MS as a whole. These factors together may have reduced the statistical power to detect a significant association.
We have focused on the in-hospital outcome of AP – due to the limited data on its long-term consequences – but evaluating the post-discharge outcomes would also be crucial. In our recent analysis, we showed that pre-existing cardiovascular diseases and a more severe course of AP can be associated with post-discharge mortality (108). Therefore, to prevent or minimize the late consequences of AP, it would be important to follow up patients, especially those with obesity and any associated comorbidities having a higher risk of a more severe disease course.
4.1 Strengths and limitations
As for the strengths of our analysis, we followed our protocol, which was registered in advance, and applied a rigorous methodology. We performed a comprehensive analysis of a multifactorial condition and assessed the effect of its individual components as well. This study is the first meta-analysis to assess the effect of hypertension on the outcomes of AP, highlighting a significant strength of our research. We showed that obesity worsens both local and systemic complications.
Among the limitations, we should note that we included both prospective and retrospective observational studies, and national databases that often lack a uniform protocol for data collection, which can result in lower data quality. Since the study number was limited, the publication bias and the influence assessment of individual studies have limited diagnostic value. Moreover, this small sample size makes the estimation of heterogeneity highly uncertain. Heterogeneity may also stem from variability in how MS itself was defined across the included studies. Because different diagnostic criteria were applied in different settings (15), direct comparison between studies was challenging. Differences in study design (e.g., prospective vs. retrospective), study populations (including age distribution, comorbidity burden, and severity spectrum), and regional baseline risks (such as prevalence of metabolic comorbidities and healthcare system characteristics) may further contribute to the observed variability. Due to these inconsistencies and the way data were reported, we were unable to stratify our analyses according to specific definitions. Instead, all studies were analyzed together, which we acknowledge as a methodological limitation. Future research using standardized definitions and harmonized reporting of metabolic parameters could allow a more nuanced evaluation of their impact on AP outcomes. Although BMI is currently the most commonly used tool for assessing obesity, it lacks accuracy as it does not account for muscle mass, fat distribution, or variations in body composition, leading to potential misclassifications.
4.2 Implication for research and practice
Our research delivers important insights that have the potential to shape daily clinical practices. Consequently, it qualifies as translational medicine, impacting both scientific inquiry and practical applications (109, 110).
Across the major prognostic models for AP, none systematically incorporate the core components of MS. Although the Ranson (111) and Glasgow–Imrie criteria (112) include admission glucose as a marker of dysglycemia, most of the scores (113–118) omit obesity, triglycerides or chronic hypertension. Only the recently developed EASY-APP (18) integrates glucose and allows entry of BMI or blood pressure into its model, but triglycerides remain absent, and metabolic features are not among its strongest predictors. Our findings indicate that obesity and hypertriglyceridemia are among the most powerful determinants of adverse outcomes, underscoring a gap across all currently applied systems. Future research should therefore examine whether incorporating these metabolic parameters into established or next-generation scores could enhance predictive accuracy and enable earlier, more targeted decision-making.
Patients with MS or its components have a high risk of a poor AP outcome, and therefore require closer monitoring. Considering the high rates of AP recurrence, lifestyle counseling and education of AP patients with obesity is crucial. However, better treatment strategies for overweight and obesity are needed as well to prevent the formation of concomitant metabolic abnormalities; even primary care should address obesity directly, not only the related comorbidities.
Despite the strong link between MS and AP, gaps in the literature persist, particularly regarding causal mechanisms. Future research should prioritize explaining the mechanisms connecting these two conditions to improve clinical practices and public health initiatives.
5 Conclusion
Components of metabolic syndrome are risk factors for complications, severity, and mortality in acute pancreatitis.
Data availability statement
Publicly available datasets were analyzed in this study. This data can be found here: The datasets used in this study can be found in the full-text articles included in the systematic review and meta-analysis.
Author contributions
DD: Writing – original draft, Conceptualization, Project administration, Writing – review & editing, Methodology. MO: Methodology, Conceptualization, Writing – original draft, Writing – review & editing. ES: Writing – review & editing, Methodology, Writing – original draft, Conceptualization. DV: Conceptualization, Writing – review & editing, Writing – original draft, Data curation. LH: Data curation, Conceptualization, Writing – review & editing, Writing – original draft. RP: Conceptualization, Writing – review & editing, Writing – original draft. AC: Writing – review & editing, Writing – original draft, Data curation. BB: Writing – original draft, Data curation, Writing – review & editing. DC: Data curation, Writing – original draft, Writing – review & editing. PH: Writing – review & editing, Methodology, Supervision, Conceptualization, Writing – original draft. AS: Conceptualization, Methodology, Writing – review & editing, Supervision, Writing – original draft.
Funding
The author(s) declare financial support was received for the research and/or publication of this article. Funding was provided by the Centre for Translational Medicine, Semmelweis University, Hungarian Ministry of Innovation and Technology, National Research, Development and Innovation Fund (TKP2021-EGA-23 to Péter Hegyi), NKFIH project grants K131996 and K147265 (to Péter Hegyi), the University of Pécs Medical School Research Fund (300909 to Andrea Szentesi), EKÖP-2024-86 of the National Research, Development and Innovation Fund to Dalma Dobszai. The sponsors had no role in the design, data collection, analysis, interpretation, and manuscript preparation.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fendo.2025.1690754/full#supplementary-material
References
1. Iannuzzi JP, King JA, Leong JH, Quan J, Windsor JW, Tanyingoh D, et al. Global incidence of acute pancreatitis is increasing over time: A systematic review and meta-analysis. Gastroenterology. (2022) 162:122–34. doi: 10.1053/j.gastro.2021.09.043
2. Yazici C, Thaker S, Castellanos KK, Al Rashdan H, Huang Y, Sarraf P, et al. Diet, gut microbiome, and their end metabolites associate with acute pancreatitis risk. Clin Transl Gastroenterol. (2023) 14:e00597. doi: 10.14309/ctg.0000000000000597
3. Chen J, Ruan X, Fu T, Lu S, Gill D, He Z, et al. Sedentary lifestyle, physical activity, and gastrointestinal diseases: evidence from mendelian randomization analysis. EBioMedicine. (2024) 103:105110. doi: 10.1016/j.ebiom.2024.105110
4. Banks PA, Bollen TL, Dervenis C, Gooszen HG, Johnson CD, Sarr MG, et al. Classification of acute pancreatitis–2012: revision of the Atlanta classification and definitions by international consensus. Gut. (2013) 62:102–11. doi: 10.1136/gutjnl-2012-302779
5. De Luca M, Angrisani L, Himpens J, Busetto L, Scopinaro N, Weiner R, et al. Indications for surgery for obesity and weight-related diseases: position statements from the international federation for the surgery of obesity and metabolic disorders (IFSO). Obes Surg. (2016) 26:1659–96. doi: 10.1007/s11695-016-2271-4
6. Blaszczak AM, Krishna SG, Hart PA, Bradley D, Hsueh W, Lara LF, et al. Class III obesity rather than metabolic syndrome impacts clinical outcomes of acute pancreatitis: A propensity score weighted analysis. Pancreatology. (2020) 20:1287–95. doi: 10.1016/j.pan.2020.08.011
7. Dobszai D, Mátrai P, Gyöngyi Z, Csupor D, Bajor J, Erőss B, et al. Body-mass index correlates with severity and mortality in acute pancreatitis: A meta-analysis. World J Gastroenterol. (2019) 25:729–43. doi: 10.3748/wjg.v25.i6.729
8. Szentesi A, Párniczky A, Vincze Á, Bajor J, Gódi S, Sarlós P, et al. Multiple hits in acute pancreatitis: components of metabolic syndrome synergize each other's deteriorating effects. Front Physiol. (2019) 10:1202. doi: 10.3389/fphys.2019.01202
9. Kloock S, Ziegler CG, and Dischinger U. Obesity and its comorbidities, current treatment options and future perspectives: Challenging bariatric surgery? Pharmacol Ther. (2023) 251:108549. doi: 10.1016/j.pharmthera.2023.108549
10. Földi M, Farkas N, Kiss S, Zádori N, Váncsa S, Szakó L, et al. Obesity is a risk factor for developing critical condition in COVID-19 patients: A systematic review and meta-analysis. Obes Rev. (2020) 21:e13095. doi: 10.1111/obr.13095
11. Mosztbacher D, Hanák L, Farkas N, Szentesi A, Mikó A, Bajor J, et al. Hypertriglyceridemia-induced acute pancreatitis: A prospective, multicenter, international cohort analysis of 716 acute pancreatitis cases. Pancreatology. (2020) 20:608–16. doi: 10.1016/j.pan.2020.03.018
12. Chamorro-Pareja N, Karamanis D, Zavras PD, Li W, Mathias P, Kokkinidis D, et al. 377. Diabetes as a prognostic factor for mortality in Coronavirus Disease 19 (COVID-19): a systematic review and meta-analysis comprising 18,506 patients. Open Forum Infect Dis. (2020) 7:377S258. doi: 10.1093/ofid/ofaa439.572
13. Mikó A, Farkas N, Garami A, Szabó I, Vincze Á, Veres G, et al. Preexisting diabetes elevates risk of local and systemic complications in acute pancreatitis: systematic review and meta-analysis. Pancreas. (2018) 47:917–23. doi: 10.1097/mpa.0000000000001122
14. Grundy SM, Brewer HB Jr., Cleeman JI, Smith SC Jr., and Lenfant C. Definition of metabolic syndrome: Report of the National Heart, Lung, and Blood Institute/American Heart Association conference on scientific issues related to definition. Circulation. (2004) 109:433–8. doi: 10.1161/01.Cir.0000111245.75752.C6
15. Kassi E, Pervanidou P, Kaltsas G, and Chrousos G. Metabolic syndrome: definitions and controversies. BMC Med. (2011) 9:48. doi: 10.1186/1741-7015-9-48
16. Kahn R, Buse J, Ferrannini E, and Stern M. The metabolic syndrome: time for a critical appraisal: joint statement from the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care. (2005) 28:2289–304. doi: 10.2337/diacare.28.9.2289
17. Balkau B, Valensi P, Eschwège E, and Slama G. A review of the metabolic syndrome. Diabetes Metab. (2007) 33:405–13. doi: 10.1016/j.diabet.2007.08.001
18. Kui B, Pintér J, Molontay R, Nagy M, Farkas N, Gede N, et al. EASY-APP: An artificial intelligence model and application for early and easy prediction of severity in acute pancreatitis. Clin Transl Med. (2022) 12:e842. doi: 10.1002/ctm2.842
19. Chandler J and Hopewell S. Cochrane methods–twenty years experience in developing systematic review methods. Syst Rev. (2013) 2:76. doi: 10.1186/2046-4053-2-76
20. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Bmj. (2021) 372:n71. doi: 10.1136/bmj.n71
21. Booth A, Clarke M, Dooley G, Ghersi D, Moher D, Petticrew M, et al. PROSPERO at one year: an evaluation of its utility. Syst Rev. (2013) 2:4. doi: 10.1186/2046-4053-2-4
22. Hegyi P and Varró A. Systems education can train the next generation of scientists and clinicians. Nat Med. (2024) 30:3399–400. doi: 10.1038/s41591-024-03315-w
23. Munn Z, Stern C, Aromataris E, Lockwood C, and Jordan Z. What kind of systematic review should I conduct? A proposed typology and guidance for systematic reviewers in the medical and health sciences. BMC Med Res Methodol. (2018) 18:5. doi: 10.1186/s12874-017-0468-4
24. Ouzzani M, Hammady H, Fedorowicz Z, and Elmagarmid A. Rayyan—a web and mobile app for systematic reviews. Systematic Rev. (2016) 5:210. doi: 10.1186/s13643-016-0384-4
25. Pothoulakis I, Paragomi P, Tuft M, Lahooti A, Archibugi L, Capurso G, et al. Association of serum triglyceride levels with severity in acute pancreatitis: results from an international, multicenter cohort study. Digestion. (2021) 102:809–13. doi: 10.1159/000512682
26. Tariq H, Gaduputi V, Peralta R, Abbas N, Nayudu SK, Thet P, et al. Serum triglyceride level: A predictor of complications and outcomes in acute pancreatitis? Can J Gastroenterol Hepatol. (2016) 2016:8198047. doi: 10.1155/2016/8198047
27. Nawaz H, O'Connell M, Papachristou GI, and Yadav D. Severity and natural history of acute pancreatitis in diabetic patients. Pancreatology. (2015) 15:247–52. doi: 10.1016/j.pan.2015.03.013
28. Pascual I, Sanahuja A, García N, Vázquez P, Moreno O, Tosca J, et al. Association of elevated serum triglyceride levels with a more severe course of acute pancreatitis: Cohort analysis of 1457 patients. Pancreatology. (2019) 19:623–9. doi: 10.1016/j.pan.2019.06.006
29. Hassanloo J, Béland-Bonenfant S, Paquette M, Baass A, and Bernard S. Prevalence, severity and management of hypertriglyceridemia-associated pancreatitis; A 7-year retrospective cohort study at Canadian quaternary care hospitals. J Clin Lipidol. (2022) 16:455–62. doi: 10.1016/j.jacl.2022.05.064
30. Simons-Linares CR, Jang S, Sanaka M, Bhatt A, Lopez R, Vargo J, et al. The triad of diabetes ketoacidosis, hypertriglyceridemia and acute pancreatitis How does it affect mortality and morbidity?: A 10-year analysis of the National Inpatient Sample. Med (Baltimore). (2019) 98:e14378. doi: 10.1097/md.0000000000014378
31. Wu Q, Fu M, Zheng K, Bo H, Yang H, Zhong X, et al. Elevated triglycerides level in hospital stay as a risk factor of mortality in patients with severe acute pancreatitis. PloS One. (2018) 13:e0207875. doi: 10.1371/journal.pone.0207875
32. Cheng L, Luo Z, Xiang K, Ren J, Huang Z, Tang L, et al. Clinical significance of serum triglyceride elevation at early stage of acute biliary pancreatitis. BMC Gastroenterol. (2015) 15:19. doi: 10.1186/s12876-015-0254-x
33. Ahsan MS, Datta IK, Bhuiyan TM, Azam MG, Karim MR, Ahamed F, et al. Role of serum triglyceride to detect severity and outcome in acute pancreatitis. Mymensingh Med J. (2023) 32:983–91.
34. Deng LH, Xue P, Xia Q, Yang XN, and Wan MH. Effect of admission hypertriglyceridemia on the episodes of severe acute pancreatitis. World J Gastroenterol. (2008) 14:4558–61. doi: 10.3748/wjg.14.4558
35. Hidalgo NJ, Pando E, Alberti P, Mata R, Fernandes N, Adell M, et al. The role of high serum triglyceride levels on pancreatic necrosis development and related complications. BMC Gastroenterology. (2023) 23:51. doi: 10.1186/s12876-023-02684-9
36. Shaka H, Asotibe JC, Achebe I, and Pudasaini G. Higher inpatient morbidity and mortality in biliary pancreatitis compared to hypertriglyceridemia-induced pancreatitis: a nationwide retrospective study. Cureus. (2020) 12:e10351. doi: 10.7759/cureus.10351
37. Yin G, Cang X, Yu G, Hu G, Ni J, Xiong J, et al. Different clinical presentations of hyperlipidemic acute pancreatitis: A retrospective study. Pancreas. (2015) 44:1105–10. doi: 10.1097/mpa.0000000000000403
38. Li X, Ke L, Dong J, Ye B, Meng L, Mao W, et al. Significantly different clinical features between hypertriglyceridemia and biliary acute pancreatitis: a retrospective study of 730 patients from a tertiary center. BMC Gastroenterology. (2018) 18:89. doi: 10.1186/s12876-018-0821-z
39. Song K, Wu Z, Meng J, Tian W, Zheng S, Mu D, et al. Hypertriglyceridemia as a risk factor for complications of acute pancreatitis and the development of a severity prediction model. HPB. (2023) 25:1065–73. doi: 10.1016/j.hpb.2023.05.006
40. Kim SJ, Kang H, Kim EJ, Kim YS, and Cho JH. Clinical features and outcomes of hypertriglyceridemia-induced acute pancreatitis: Propensity score matching analysis from a prospective acute pancreatitis registry. Pancreatology. (2020) 20:617–21. doi: 10.1016/j.pan.2020.03.013
41. Goyal H, Smith B, Bayer C, Rutherford C, and Shelnut D. Differences in severity and outcomes between hypertriglyceridemia and alcohol-induced pancreatitis. N Am J Med Sci. (2016) 8:82–7. doi: 10.4103/1947-2714.177307
42. Hong W, Lin S, Zippi M, Geng W, Stock S, Zimmer V, et al. High-density lipoprotein cholesterol, blood urea nitrogen, and serum creatinine can predict severe acute pancreatitis. BioMed Res Int. (2017) 2017:1648385. doi: 10.1155/2017/1648385
43. Shafiq S, Patil M, Gowda V, and Devarbhavi H. Hypertriglyceridemia-induced acute pancreatitis - course, outcome, and comparison with non-hypertriglyceridemia associated pancreatitis. Indian J Endocrinol Metab. (2022) 26:459–64. doi: 10.4103/ijem.ijem_206_22
44. Baranyai T, Terzin V, Vajda á, Wittmann T, and Czakó L. Hypertriglyceridemia causes more severe course of acute pancreatitis. Clin Lipidology. (2012) 7:731–6. doi: 10.2217/clp.12.69
45. Navarro S, Cubiella J, Feu F, Zambón D, Fernández-Cruz L, and Ros E. Análisis del curso clínico de la pancreatitis aguda hipertrigliceridémica y su comparación con el de la litiásica [Hypertriglyceridemic acute pancreatitis. Is its clinical course different from lithiasic acute pancreatitis?]. Med Clin (Barc). (2004) 123:567–70. doi: 10.1016/s0025-7753(04)74599-6
46. Sezgin O, Özdoğan O, Yaraş S, Üçbilek E, and Altıntaş E. Evaluation of hypertriglyceridemia-induced acute pancreatitis: A single tertiary care unit experience from Turkey. Turk J Gastroenterol. (2019) 30:271–7. doi: 10.5152/tjg.2018.18292
47. Huang YX, Jia L, Jiang SM, Wang SB, Li MX, and Yang BH. Incidence and clinical features of hyperlipidemic acute pancreatitis from Guangdong, China: a retrospective multicenter study. Pancreas. (2014) 43:548–52. doi: 10.1097/mpa.0000000000000069
48. Hayden JA, van der Windt DA, Cartwright JL, Côté P, and Bombardier C. Assessing bias in studies of prognostic factors. Ann Intern Med. (2013) 158:280–6. doi: 10.7326/0003-4819-158-4-201302190-00009
49. Higgins JP and Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. (2002) 21:1539–58. doi: 10.1002/sim.1186
50. Core Team R. R: A language and environment for statistical computing. (2024). Vienna, Austria: R Foundation for Statistical Computing. Available online at: https://www.R-project.org/ (Accessed April 5, 2025).
51. Schwarzer G. Meta: General package for meta-analysis. (2024). Available online at: https://github.com/guido-s/meta/ (Accessed May 10, 2025).
52. Harrer M, Cuijpers P, Furukawa T, and Ebert DD. dmetar: Companion R Package For The Guide 'Doing Meta-Analysis in R'. R package version 0.1.0. (2019). Available online at: http://dmetar.protectlab.org/ (Accessed December 8, 2024).
53. Balachandra S, Virlos IT, King NK, Siriwardana HP, France MW, and Siriwardena AK. Hyperlipidaemia and outcome in acute pancreatitis. Int J Clin Pract. (2006) 60:156–9. doi: 10.1111/j.1742-1241.2005.00645.x
54. Dawra S, Gupta P, Yadav N, Singh AK, Samanta J, Sinha SK, et al. Association between the distribution of adipose tissue and outcomes in acute pancreatitis: A COMPARISON OF METHODS OF FAT ESTImation. Indian J Radiol Imaging. (2023) 33:12–8. doi: 10.1055/s-0042-1758201
55. Higaki Y, Nishida T, Matsumoto K, Yamaoka S, Osugi N, Sugimoto A, et al. Effect of abdominal visceral fat on mortality risk in patients with severe acute pancreatitis. JGH Open. (2021) 5:1357–62. doi: 10.1002/jgh3.12681
56. Ivanova R, Puerta S, Garrido A, Cueto I, Ferro A, Ariza MJ, et al. Triglyceride levels and apolipoprotein E polymorphism in patients with acute pancreatitis. Hepatobiliary Pancreat Dis Int. (2012) 11:96–101. doi: 10.1016/s1499-3872(11)60131-8
57. Lankisch PG and Schirren CA. Increased body weight as a prognostic parameter for complications in the course of acute pancreatitis. Pancreas. (1990) 5:626–9. doi: 10.1097/00006676-199009000-00021
58. McGuire SP, Keller SL, Maatman TK, Lewellen KA, Ceppa EP, House MG, et al. Obesity worsens local and systemic complications of necrotizing pancreatitis and prolongs disease course. J Gastrointest Surg. (2022) 26:2128–35. doi: 10.1007/s11605-022-05383-0
59. Natu A, Stevens T, Kang L, Yasinow S, Mansoor E, Lopez R, et al. Visceral Adiposity Predicts Severity of Acute Pancreatitis. Pancreas. (2017) 46:776–81. doi: 10.1097/mpa.0000000000000845
60. Nawaz H, Koutroumpakis E, Easler J, Slivka A, Whitcomb DC, Singh VP, et al. Elevated serum triglycerides are independently associated with persistent organ failure in acute pancreatitis. Am J Gastroenterol. (2015) 110:1497–503. doi: 10.1038/ajg.2015.261
61. Shimonov M, Abtomonova Z, Groutz A, Amir H, Khanimov I, and Leibovitz E. Associations between body composition and prognosis of patients admitted because of acute pancreatitis: a retrospective study. Eur J Clin Nutr. (2021) 75:817–22. doi: 10.1038/s41430-020-00789-y
62. Suazo-Baráhona J, Carmona-Sánchez R, Robles-Díaz G, Milke-García P, Vargas-Vorácková F, Uscanga-Domínguez L, et al. Obesity: a risk factor for severe acute biliary and alcoholic pancreatitis. Am J Gastroenterol. (1998) 93:1324–8. doi: 10.1111/j.1572-0241.1998.442_l.x
63. Ding Y, Zhang M, Wang L, Yin T, Wang N, Wu J, et al. Association of the hypertriglyceridemic waist phenotype and severity of acute pancreatitis. Lipids Health Dis. (2019) 18:93. doi: 10.1186/s12944-019-1019-2
64. Han Y, Hu H, Li Q, Deng Z, and Liu D. Triglyceride glucose-body mass index and the risk of progression to diabetes from prediabetes: A 5-year cohort study in Chinese adults. Front Public Health. (2023) 11:1028461. doi: 10.3389/fpubh.2023.1028461
65. Johnson CD, Toh SK, and Campbell MJ. Combination of APACHE-II score and an obesity score (APACHE-O) for the prediction of severe acute pancreatitis. Pancreatology. (2004) 4:1–6. doi: 10.1159/000077021
66. Khan J, Nordback I, and Sand J. Serum lipid levels are associated with the severity of acute pancreatitis. Digestion. (2013) 87:223–8. doi: 10.1159/000348438
67. Shin KY, Lee WS, Chung DW, Heo J, Jung MK, Tak WY, et al. Influence of obesity on the severity and clinical outcome of acute pancreatitis. Gut Liver. (2011) 5:335–9. doi: 10.5009/gnl.2011.5.3.335
68. Katuchova J, Bober J, Harbulak P, Hudak A, Gajdzik T, Kalanin R, et al. Obesity as a risk factor for severe acute pancreatitis patients. Wien Klin Wochenschr. (2014) 126:223–7. doi: 10.1007/s00508-014-0507-7
69. Sempere L, Martinez J, de Madaria E, Lozano B, Sanchez-Paya J, Jover R, et al. Obesity and fat distribution imply a greater systemic inflammatory response and a worse prognosis in acute pancreatitis. Pancreatology. (2008) 8:257–64. doi: 10.1159/000134273
70. De Waele B, Vanmierlo B, Van Nieuwenhove Y, and Delvaux G. Impact of body overweight and class I, II and III obesity on the outcome of acute biliary pancreatitis. Pancreas. (2006) 32:343–5. doi: 10.1097/01.mpa.0000220857.55378.7b
71. Tsai CJ. Is obesity a significant prognostic factor in acute pancreatitis? Dig Dis Sci. (1998) 43:2251–4. doi: 10.1023/a:1026666622394
72. Ikeura T, Kato K, Takaoka M, Shimatani M, Kishimoto M, Nishi K, et al. A body mass index ≥25 kg/m2 is associated with a poor prognosis in patients with acute pancreatitis: a study of Japanese patients. Hepatobiliary Pancreat Dis Int. (2017) 16:645–51. doi: 10.1016/s1499-3872(17)60057-2
73. Stimac D, Krznarić Zrnić I, Radic M, and Zuvic-Butorac M. Outcome of the biliary acute pancreatitis is not associated with body mass index. Pancreas. (2007) 34:165–6. doi: 10.1097/mpa.0b013e31802e003c
74. Martínez J, Sánchez-Payá J, Palazón JM, Aparicio JR, Picó A, and Pérez-Mateo M. Obesity: a prognostic factor of severity in acute pancreatitis. Pancreas. (1999) 19:15–20.
75. Davis PJ, Eltawil KM, Abu-Wasel B, Walsh MJ, Topp T, and Molinari M. Effect of obesity and decompressive laparotomy on mortality in acute pancreatitis requiring intensive care unit admission. World J Surg. (2013) 37:318–32. doi: 10.1007/s00268-012-1821-8
76. Funnell IC, Bornman PC, Weakley SP, Terblanche J, and Marks IN. Obesity: an important prognostic factor in acute pancreatitis. Br J Surg. (1993) 80:484–6. doi: 10.1002/bjs.1800800426
77. Papachristou GI, Papachristou DJ, Avula H, Slivka A, and Whitcomb DC. Obesity increases the severity of acute pancreatitis: performance of APACHE-O score and correlation with the inflammatory response. Pancreatology. (2006) 6:279–85. doi: 10.1159/000092689
78. İnce AT, Seven G, Koçhan K, Kiremitçi S, Yıldız K, and Şentürk H. The course of acute pancreatitis in patients with different BMI groups. Pancreatology. (2022) 22:348–55. doi: 10.1016/j.pan.2022.03.009
79. Biberci Keskin E, Büyükaydın B, Soysal P, Kiremitçi S, Yabacı A, and Şentürk H. The impact of obesity on acute pancreatitis outcomes in older patients. Eur Geriatr Med. (2020) 11:427–32. doi: 10.1007/s41999-020-00305-2
80. Deenadayalu VP, Blaut U, Watkins JL, Barnett J, Freeman M, Geenen J, et al. Does obesity confer an increased risk and/or more severe course of post-ERCP pancreatitis?: a retrospective, multicenter study. J Clin Gastroenterol. (2008) 42:1103–9. doi: 10.1097/MCG.0b013e318159cbd1
81. Mery CM, Rubio V, Duarte-Rojo A, Suazo-Barahona J, Peláez-Luna M, Milke P, et al. Android fat distribution as predictor of severity in acute pancreatitis. Pancreatology. (2002) 2:543–9. doi: 10.1159/000066099
82. Liu ZY, Tian L, Sun XY, Liu ZS, Hao LJ, Shen WW, et al. Development and validation of a risk prediction score for the severity of acute hypertriglyceridemic pancreatitis in Chinese patients. World J gastroenterology. (2022) 28:4846–60. doi: 10.3748/wjg.v28.i33.4846
83. Wang Y, Xu Z, Zhou Y, Xie M, Qi X, Xu Z, et al. Leukocyte cell population data from the blood cell analyzer as a predictive marker for severity of acute pancreatitis. J Clin Lab Anal. (2021) 35:e23863. doi: 10.1002/jcla.23863
84. Zhao B, Sun S, Wang Y, Zhu H, Ni T, Qi X, et al. Cardiac indicator CK-MB might be a predictive marker for severity and organ failure development of acute pancreatitis. Ann Transl Med. (2021) 9:368. doi: 10.21037/atm-20-3095
85. Cho SK, Huh JH, Yoo JS, Kim JW, and Lee KJ. HOMA-estimated insulin resistance as an independent prognostic factor in patients with acute pancreatitis. Sci Rep. (2019) 9:14894. doi: 10.1038/s41598-019-51466-5
86. Jain V, Nath P, Satpathy SK, Panda B, and Patro S. Comparing prognostic scores and inflammatory markers in predicting the severity and mortality of acute pancreatitis. Cureus. (2023) 15:e39515. doi: 10.7759/cureus.39515
87. Mole DJ, Gungabissoon U, Johnston P, Cochrane L, Hopkins L, Wyper GM, et al. Identifying risk factors for progression to critical care admission and death among individuals with acute pancreatitis: a record linkage analysis of Scottish healthcare databases. BMJ Open. (2016) 6:e011474. doi: 10.1136/bmjopen-2016-011474
88. Niknam R, Moradi J, Jahanshahi KA, Mahmoudi L, and Ejtehadi F. Association Between Metabolic Syndrome and Its Components with Severity of Acute Pancreatitis. Diabetes Metab Syndr Obes. (2020) 13:1289–96. doi: 10.2147/dmso.S249128
89. Chen Y, Li Q, Ma L, Cai Z, and Zhou J. Development and internal validation of a practical model to predict 30 days mortality of severe acute pancreatitis patients. Ann Med. (2023) 55:2236648. doi: 10.1080/07853890.2023.2236648
90. Luthra AK, Porter K, Hinton A, Chao WL, Papachristou GI, Conwell DL, et al. A Comparison of Machine Learning Methods and Conventional Logistic Regression for the Prediction of In-Hospital Mortality in Acute Biliary Pancreatitis. Pancreas. (2022) 51:1292–9. doi: 10.1097/mpa.0000000000002208
91. Singh RK, Poddar B, Baronia AK, Azim A, Gurjar M, Singhal S, et al. Audit of patients with severe acute pancreatitis admitted to an intensive care unit. Indian J Gastroenterol. (2012) 31:243–52. doi: 10.1007/s12664-012-0205-1
92. Li C, Ren Q, Wang Z, and Wang G. Early prediction of in-hospital mortality in acute pancreatitis: a retrospective observational cohort study based on a large multicentre critical care database. BMJ Open. (2020) 10:e041893. doi: 10.1136/bmjopen-2020-041893
93. Paragomi P, Papachristou GI, Jeong K, Hinton A, Pothoulakis I, Talukdar R, et al. The relationship between pre-existing diabetes mellitus and the severity of acute pancreatitis: Report from a large international registry. Pancreatology. (2022) 22:85–91. doi: 10.1016/j.pan.2021.10.001
94. Chen CH, Dai CY, Hou NJ, Chen SC, Chuang WL, and Yu ML. Etiology, severity and recurrence of acute pancreatitis in southern taiwan. J Formos Med Assoc. (2006) 105:550–5. doi: 10.1016/s0929-6646(09)60149-2
95. Rostropowicz-Honka A and Brzoza Z. Type 2 Diabetes as a Factor Modifying the Course and Prognosis of Acute Pancreatitis. Clin Diabetology. (2022) 11:387–92. doi: 10.5603/DK.a2022.0057
96. Zhao X, Chang Mei H, Chen L, Jiang L, He M, Chen J, et al. An increased level of haemoglobin A1C predicts a poorer clinical outcome in patients with acute pancreatitis. Clin Endocrinol (Oxf). (2012) 77:241–5. doi: 10.1111/j.1365-2265.2011.04252.x
97. Song K, Guo C-R, Li C-L, and Ding N. Comparison of clinical characteristics in acute pancreatitis with and without diabetes mellitus: a retrospective study. Signa Vitae. (2021) 17:181–7. doi: 10.22514/sv.2020.16.0113
98. Sawalhi S, Al-Maramhy H, Abdelrahman AI, Allah SE, and Al-Jubori S. Does the presence of obesity and/or metabolic syndrome affect the course of acute pancreatitis?: A prospective study. Pancreas. (2014) 43:565–70. doi: 10.1097/mpa.0000000000000028
99. Mikolasevic I, Milic S, Orlic L, Poropat G, Jakopcic I, Franjic N, et al. Metabolic syndrome and acute pancreatitis. Eur J Intern Med. (2016) 32:79–83. doi: 10.1016/j.ejim.2016.04.004
100. Váncsa S, Sipos Z, Váradi A, Nagy R, Ocskay K, Juhász FM, et al. Metabolic-associated fatty liver disease is associated with acute pancreatitis with more severe course: Post hoc analysis of a prospectively collected international registry. United Eur Gastroenterol J. (2023) 11:371–82. doi: 10.1002/ueg2.12389
101. Sbeit W, Abu Elheja F, Msheiil B, Shahin A, Khoury S, Sbeit M, et al. Fatty pancreas was associated with a higher acute pancreatitis Systemic Inflammatory Response Syndrome score at hospital admission. Eur J Gastroenterol Hepatol. (2023) 35:980–4. doi: 10.1097/meg.0000000000002606
102. Abdullah A, Peeters A, de Courten M, and Stoelwinder J. The magnitude of association between overweight and obesity and the risk of diabetes: a meta-analysis of prospective cohort studies. Diabetes Res Clin Pract. (2010) 89:309–19. doi: 10.1016/j.diabres.2010.04.012
103. Khanna D, Khanna S, Khanna P, Kahar P, and Patel BM. Obesity: A Chronic Low-Grade Inflammation and Its Markers. Cureus. (2022) 14:e22711. doi: 10.7759/cureus.22711
104. Kiss L, Fűr G, Mátrai P, Hegyi P, Ivány E, Cazacu IM, et al. The effect of serum triglyceride concentration on the outcome of acute pancreatitis: systematic review and meta-analysis. Sci Rep. (2018) 8:14096. doi: 10.1038/s41598-018-32337-x
105. Durante A, Mazzapicchi A, and Baiardo Redaelli M. Systemic and Cardiac Microvascular Dysfunction in Hypertension. Int J Mol Sci. (2024) 25:13294. doi: 10.3390/ijms252413294
106. Gao S, Park BM, Cha SA, Bae UJ, Park BH, Park WH, et al. Oxidative stress increases the risk of pancreatic β cell damage in chronic renal hypertensive rats. Physiol Rep. (2016) 4:e12900. doi: 10.14814/phy2.12900
107. Kozłowska A, Wojtacha P, Majewski M, and Równiak M. The cytokine alterations/abnormalities and oxidative damage in the pancreas during hypertension development. Pflugers Arch. (2019) 471:1331–40. doi: 10.1007/s00424-019-02312-0
108. Czapári D, Váradi A, Farkas N, Nyári G, Márta K, Váncsa S, et al. Detailed Characteristics of Post-discharge Mortality in Acute Pancreatitis. Gastroenterology. (2023) 165:682–95. doi: 10.1053/j.gastro.2023.05.028
109. Hegyi P, Petersen OH, Holgate S, Erőss B, Garami A, Szakács Z, et al. Academia europaea position paper on translational medicine: the cycle model for translating scientific results into community benefits. J Clin Med. (2020) 9:1532. doi: 10.3390/jcm9051532
110. Hegyi P, Erőss B, Izbéki F, Párniczky A, and Szentesi A. Accelerating the translational medicine cycle: the Academia Europaea pilot. Nat Med. (2021) 27:1317–9. doi: 10.1038/s41591-021-01458-8
111. Ranson JH, Rifkind KM, Roses DF, Fink SD, Eng K, and Spencer FC. Prognostic signs and the role of operative management in acute pancreatitis. Surg Gynecol Obstet. (1974) 139:69–81.
112. Imrie CW, Benjamin IS, Ferguson JC, McKay AJ, Mackenzie I, O'Neill J, et al. A single-centre double-blind trial of Trasylol therapy in primary acute pancreatitis. Br J Surg. (1978) 65:337–41. doi: 10.1002/bjs.1800650514
113. Knaus WA, Draper EA, Wagner DP, and Zimmerman JE. APACHE II: a severity of disease classification system. Crit Care Med. (1985) 13:818–29.
114. Singh VK, Wu BU, Bollen TL, Repas K, Maurer R, Johannes RS, et al. A prospective evaluation of the bedside index for severity in acute pancreatitis score in assessing mortality and intermediate markers of severity in acute pancreatitis. Am J Gastroenterol. (2009) 104:966–71. doi: 10.1038/ajg.2009.28
115. Balthazar EJ, Robinson DL, Megibow AJ, and Ranson JH. Acute pancreatitis: value of CT in establishing prognosis. Radiology. (1990) 174:331–6. doi: 10.1148/radiology.174.2.2296641
116. Marshall JC, Cook DJ, Christou NV, Bernard GR, Sprung CL, and Sibbald WJ. Multiple organ dysfunction score: a reliable descriptor of a complex clinical outcome. Crit Care Med. (1995) 23:1638–52. doi: 10.1097/00003246-199510000-00007
117. Lankisch PG, Weber-Dany B, Hebel K, Maisonneuve P, and Lowenfels AB. The harmless acute pancreatitis score: a clinical algorithm for rapid initial stratification of nonsevere disease. Clin Gastroenterol Hepatol. (2009) 7:702–5. doi: 10.1016/j.cgh.2009.02.020
Keywords: acute, pancreatitis, metabolic, syndrome, obesity, diabetes, hypertriglyceridemia, hypertension
Citation: Dobszai D, Obeidat M, Szalai EÁ, Veres DS, Havelda L, Papp R, Choi A, Budai BC, Csajbók D, Hegyi P and Szentesi A (2025) Metabolic syndrome components individually worsen the outcome of acute pancreatitis: a systematic review and meta-analysis. Front. Endocrinol. 16:1690754. doi: 10.3389/fendo.2025.1690754
Received: 22 August 2025; Accepted: 20 October 2025;
Published: 04 November 2025.
Edited by:
Stephen J. Pandol, Cedars Sinai Medical Center, United StatesReviewed by:
Li Wen, Peking Union Medical College Hospital (CAMS), ChinaXin Zhou, Southwest Medical University, China
Copyright © 2025 Dobszai, Obeidat, Szalai, Veres, Havelda, Papp, Choi, Budai, Csajbók, Hegyi and Szentesi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Andrea Szentesi, c3plbnRlc2lhaUBnbWFpbC5jb20=
†These authors have contributed equally to this work