 Pere Riutord-Sbert1†
Pere Riutord-Sbert1† Pedro Juan Tárraga López2,3†
Pedro Juan Tárraga López2,3† Ángel Arturo López-González1,4,5*†
Ángel Arturo López-González1,4,5*† Irene Coll Campayo1†Carla Busquets-Cortés1†
Irene Coll Campayo1†Carla Busquets-Cortés1† José Ignacio Ramírez Manent1,4,5,6†
José Ignacio Ramírez Manent1,4,5,6†- 1ADEMA-Health Group, University Institute for Research in Health Sciences (IUNICS), Palma, Spain
- 2Faculty of Medicine, University of Castilla La Mancha (UCLM), Albacete, Spain
- 3SESCAM (Health Service of Castilla La Mancha), Albacete, Spain
- 4Balearic Islands Health Research Institute Foundation (IDISBA), Palma, Spain
- 5Balearic Islands Health Service, Palma, Spain
- 6Faculty of Medicine, University of the Balearic Islands, Palma, Spain
Background: Obesity is a multifactorial condition shaped by biological, behavioral, socioeconomic, and psychosocial determinants. While lifestyle correlates are well documented, the impact of social isolation on obesity in occupational settings remains insufficiently explored. This study examined associations between sociodemographic variables, health behaviors, and social isolation with multiple obesity indices in a large cohort of Spanish workers.
Methods: We analyzed 117298 employees across Spain (2021–2024). Obesity was defined using body mass index (BMI), waist-to-height ratio (WtHR), Clínica Universidad de Navarra–Body Adiposity Estimator (CUN-BAE), and Metabolic Score for Visceral Fat (METS-VF). Sociodemographic data, lifestyle habits, and social isolation (ENRICHD Social Support Instrument, ESSI) were obtained through standardized protocols. Multivariable logistic regression estimated adjusted odds ratios (OR) and 95% confidence intervals (CI).
Results: Obesity prevalence ranged from 20.4% (BMI) to 39.6% (METS-VF). Male sex (OR up to 2.11, 95% CI 2.05–2.18), older age (OR 2.83, 95% CI 2.71–2.96 for ≥55 years vs. <35), and lower social class (OR 1.62, 95% CI 1.54–1.71) were consistently associated with obesity across all indices. Poor adherence to the Mediterranean diet and physical inactivity increased the likelihood of obesity (OR 1.35 and 1.41, respectively). Social isolation independently predicted higher obesity risk (OR 1.27, 95% CI 1.21–1.33), even after adjusting for sociodemographic and lifestyle factors. Associations remained robust in sensitivity analyses.
Conclusions: Obesity in Spanish workers is strongly associated with sociodemographic disadvantage, unhealthy lifestyles, and psychosocial vulnerability. Social isolation emerged as a novel determinant, reinforcing the need for multidimensional public health strategies that integrate lifestyle promotion, reduction of socioeconomic inequalities, and enhancement of social connectedness.
Introduction
Obesity has emerged as one of the most pressing global public health challenges of the 21st century. The prevalence of obesity has steadily increased worldwide over the last four decades, affecting both developed and developing countries across all age groups and socioeconomic strata. The World Health Organization (WHO) estimates that more than one billion people are currently living with obesity, including 650 million adults, 340 million adolescents, and 39 million children, and these figures are projected to rise further if effective preventive and therapeutic measures are not implemented (1). In Europe, obesity prevalence has doubled since 1980, with more than half of the adult population now being overweight or obese (2). Spain mirrors this concerning trend, with national surveys showing that approximately 21% of adults are obese and more than 55% are overweight, representing a major burden on the healthcare system (3). The occupational setting constitutes a particularly relevant context for studying obesity, as the working population faces unique exposures and constraints that may influence lifestyle behaviors and cardiometabolic health (4).
Obesity is a complex, multifactorial disease characterized by an abnormal or excessive accumulation of adipose tissue that presents health risks beyond simple body weight gain. Its pathophysiology involves an intricate interplay of genetic (5), environmental (6), and behavioral factors (7) that converge on a state of positive energy balance. Dysfunctional adipose tissue plays a central role in mediating the adverse health consequences of obesity. In particular, hypertrophy and hyperplasia of adipocytes result in increased release of free fatty acids, altered secretion of adipokines, and recruitment of pro-inflammatory macrophages, generating a low-grade chronic inflammatory state (5). This inflammatory milieu promotes insulin resistance, endothelial dysfunction, and dyslipidemia, which are hallmarks of obesity-related cardiometabolic disorders (8). Moreover, visceral adiposity appears to be more deleterious than peripheral fat, as ectopic lipid deposition in the liver, pancreas, and skeletal muscle exacerbates metabolic impairment (9). These mechanistic insights underscore the need to move beyond crude measures of body size and towards refined indicators of adiposity and fat distribution in epidemiological and clinical research.
The body mass index (BMI) remains the most widely used measure for defining overweight and obesity due to its simplicity and reproducibility. However, BMI fails to differentiate between lean and fat mass, nor does it adequately capture fat distribution (10). Increasing evidence indicates that central obesity, rather than general obesity, better predicts cardiometabolic risk (11). Accordingly, waist circumference (WC) and waist-to-height ratio (WtHR) have been adopted as complementary measures of abdominal adiposity (12). In addition, more sophisticated anthropometric and metabolic indices have been developed to improve risk stratification. The Clínica Universidad de Navarra–Body Adiposity Estimator (CUN-BAE) is a validated equation that estimates body fat percentage based on BMI, age, and sex, providing a better approximation of adiposity (13). The Metabolic Score for Visceral Fat (METS-VF) integrates BMI, WtHR, triglycerides, and HDL cholesterol to estimate visceral fat, offering enhanced predictive power for cardiometabolic disorders (14). These indices, alongside traditional anthropometric measures, provide a multidimensional assessment of obesity burden and its metabolic correlates, and they constitute the core diagnostic tools applied in the present study.
The adverse health outcomes associated with obesity are well established. Obesity is a major risk factor for type 2 diabetes mellitus (T2DM), hypertension, dyslipidemia, nonalcoholic fatty liver disease (NAFLD), cardiovascular disease (CVD), several cancers, and premature mortality (15–18). It also contributes to impaired physical functioning, musculoskeletal disorders, obstructive sleep apnea, and reduced quality of life (19–21). Epidemiological studies have shown that individuals with obesity have a markedly higher risk of developing T2DM (up to 7-fold increase) and coronary heart disease (2- to 3-fold increase) compared with normal-weight counterparts (22). Importantly, visceral obesity confers additional risk beyond overall adiposity, being strongly linked to insulin resistance, atherogenic dyslipidemia, and hepatic steatosis (23–25). Beyond somatic health, obesity has profound psychosocial consequences, including stigmatization, depression, anxiety, and reduced social participation (26–28). These multidimensional repercussions highlight the importance of investigating obesity within broad biopsychosocial frameworks.
Obesity is unevenly distributed across populations, reflecting the influence of sociodemographic and lifestyle determinants. Socioeconomic status (SES) is a consistent correlate, with lower income, education, and occupational class being associated with higher obesity prevalence (29). This gradient reflects disparities in access to healthy foods, recreational opportunities, healthcare resources, and health literacy. Gender and age also modulate obesity patterns, with women often showing higher rates of severe obesity and men displaying greater central adiposity (30). Lifestyle behaviors remain pivotal: inadequate physical activity, excessive sedentary time, poor adherence to the Mediterranean diet, smoking, and excessive alcohol consumption have all been associated with adverse obesity profiles (31, 32). Chronic stress has been increasingly associated with obesity, particularly visceral fat accumulation, due to dysregulation of the hypothalamic–pituitary–adrenal axis and sustained elevation of cortisol levels (33). Furthermore, poor sleep quality, a growing public health concern, has been linked to metabolic dysregulation and weight gain, reinforcing the multifactorial nature of obesity (34). These behavioral determinants interact with structural and psychosocial factors, producing complex patterns of risk within working populations.
Beyond conventional behavioral and socioeconomic determinants, psychosocial dimensions such as social isolation have gained increasing recognition as contributors to obesity and related metabolic disorders. Social isolation is understood as a state of limited or absent social interactions, which may result from illness, disability, aging, or psychosocial conditions has been linked to both unhealthy behaviors and adverse biological responses (35). This phenomenon has been increasingly recognized as a determinant of health, influencing both mental and physical outcomes, and may act as a contributing factor to obesity. Individuals experiencing isolation are more likely to engage in physical inactivity, poor diet, and smoking, and they may also suffer from elevated stress, dysregulated hypothalamic-pituitary-adrenal (HPA) axis activity, and systemic inflammation (36, 37). Recent studies have demonstrated that social isolation is associated with higher BMI, central adiposity, and increased risk of metabolic syndrome (38, 39). In occupational cohorts, isolation may arise from shift work, job strain, or limited social support, thereby amplifying health risks (40, 41). Evidence also suggests that isolation interacts with other sociodemographic variables, such as age and education, in shaping obesity outcomes (42). Despite growing interest, relatively few large-scale studies have simultaneously examined social isolation alongside classical determinants in relation to refined obesity indices, leaving important gaps in knowledge.
Given the escalating prevalence of obesity and its devastating health consequences, there is an urgent need to deepen our understanding of the factors shaping obesity risk in the workforce. While BMI remains the standard metric, complementary indices such as WtHR, CUN-BAE, and METS-VF provide more nuanced insights into adiposity and its metabolic implications. Moreover, exploring the role of social isolation, alongside sociodemographic and lifestyle determinants, can shed light on underappreciated psychosocial pathways contributing to obesity. Building on previous research with this large Spanish occupational cohort that investigated insulin resistance, type 2 diabetes, and atherogenic dyslipidemia in relation to sociodemographic, lifestyle, and psychosocial factors, the present study extends this framework to obesity. Specifically, we aimed to examine the associations between obesity indices and a broad range of determinants, including age, sex, education, occupational class, physical activity, adherence to the Mediterranean diet, smoking, alcohol consumption, and social isolation. By providing robust evidence from a large working population, this study seeks to inform targeted prevention and intervention strategies aimed at reducing obesity burden and mitigating its cardiometabolic and psychosocial consequences.
Methods
Study design and setting
We conducted a cross‐sectional analysis within an occupational health surveillance program in Spain covering January 2021 to December 2024. Periodic medical assessments were performed in accredited centers following harmonized protocols used in previous analyses of this cohort. The study complied with the Declaration of Helsinki; all participants provided written informed consent prior to inclusion. Approval was obtained from the corresponding institutional research ethics committee.
Participants
The initial sample comprised 118,564 workers undergoing routine examinations. Participants were recruited through consecutive sampling of Spanish workers attending routine occupational health examinations between 2021–2024 years. This approach ensured a representative occupational cohort while minimizing selection bias
Inclusion criteria were: Participants were actively employed, aged between 18 and 69 years, and had complete data available for anthropometric, lifestyle, and sociodemographic variables, and who agreed to participate in the study.
Exclusion criteria were: missing key data (anthropometry, biochemistry, IPAQ, MEDAS, or ESSI); pregnancy; Individuals with severe chronic illnesses (e.g., cancer, advanced cardiovascular disease, or end-stage renal disease) or missing essential, measurement error after predefined quality control rules.
118,491 agreed to participate in the study. After exclusions (n=1,193), the final analytic sample was 117,298 workers (71,384 men; 45,914 women). The selection process is summarized in Figure 1.
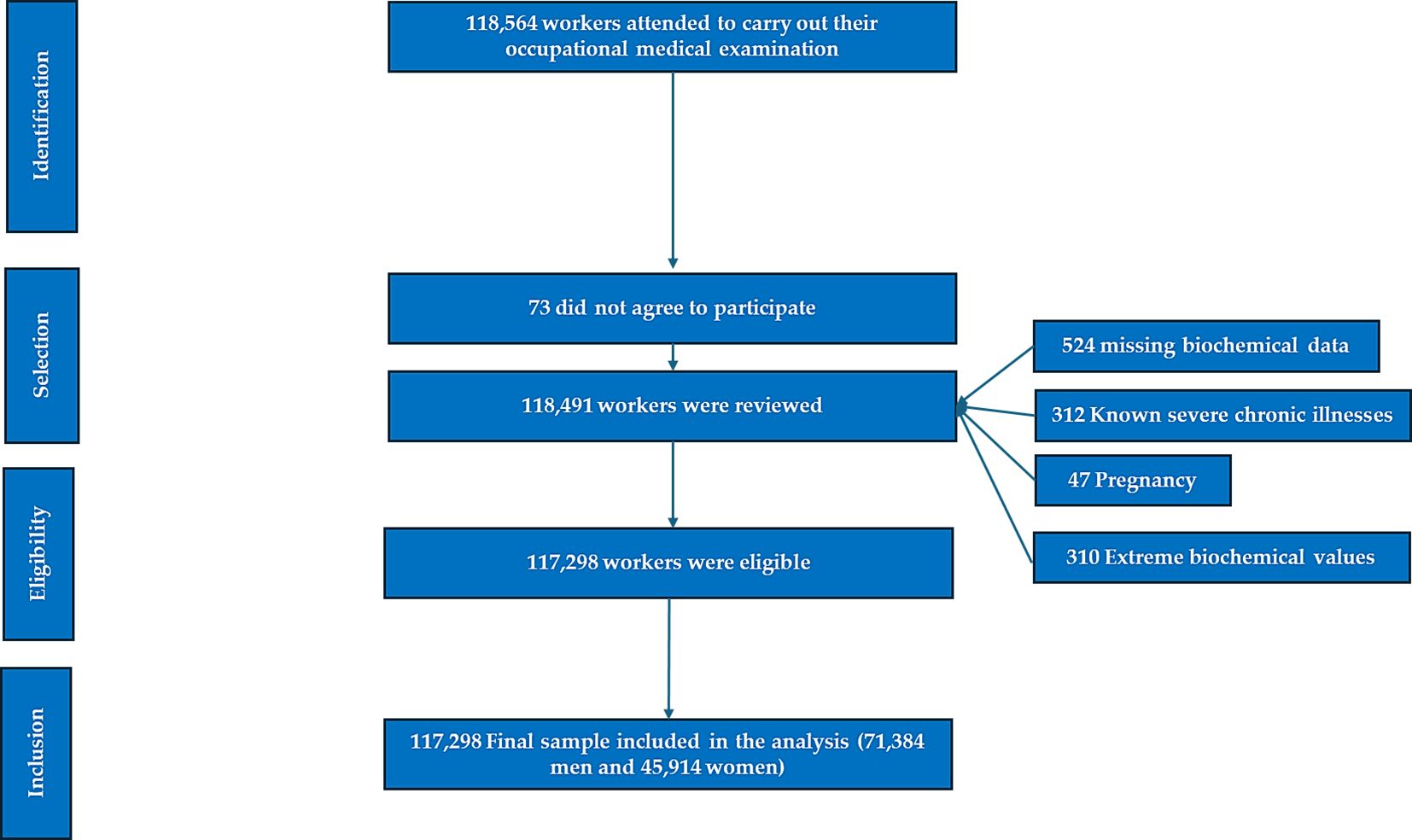
Figure 1. Flowchart - obesity risk study.
Sociodemographic and occupational variables
Age (categorized as 18–39, 40–49, 50–59, 60–69 years) and sex were recorded. Social class was assigned according to the Spanish National Classification of Occupations (CNO-11) and categorized following the standards of the Spanish Society of Epidemiology (SEE) into Classes I–III, as previously applied in this cohort to ensure comparability across studies (43).
Lifestyle habits
Physical activity was assessed with the International Physical Activity Questionnaire (IPAQ), short form, following standard scoring procedures (MET-min/week); participants were categorized as active (≥600 MET-min/week) or inactive (44). Adherence to the Mediterranean diet was measured using the validated 14-item MEDAS screener (score 0–14), dichotomized as high adherence (≥9) vs low (45). Smoking was classified as current smoker vs non-smoker.
Clinical and biochemical measurements
Examinations were conducted by trained personnel using calibrated devices. Weight and height were measured with light clothing and no shoes; waist circumference was taken at the midpoint between the last rib and iliac crest using a non-elastic tape, following WHO recommendations (46). Blood pressure was measured in the seated position after ≥5 minutes of rest; two readings were averaged. Fasting venous blood (≥8–12 h fast) was obtained for total cholesterol, HDL-c, LDL-c, triglycerides, and glucose, determined by standard enzymatic methods on analyzers under external quality assurance. LDL-c was calculated using laboratory-standard procedures when required. Internal QC rules flagged extreme values for recheck or exclusion.
Social isolation assessment
Psychosocial support was measured with the ENRICHD Social Support Instrument (ESSI), a brief, validated instrument comprising five items on emotional/instrumental support, plus items on partner status and network size. Following established practice, low social support (social isolation) was defined as ESSI total ≤18 and responses ≤3 on at least two items; all others were considered normal support (47). This operationalization has been used in epidemiological and occupational settings and in prior analyses of this cohort, facilitating direct comparability.
Obesity indices and case definitions
We evaluated complementary indicators capturing overall adiposity, fat distribution, and estimated visceral adiposity:
● Body Mass Index (BMI): kg/m²; obesity defined as BMI ≥ 30.0 kg/m².
● Waist-to-Height Ratio (WtHR): waist (cm)/height (cm); high WtHR defined as ≥0.50, a widely used screening cut-off for central adiposity.
● CUN BAE (Clínica Universidad de Navarra Body Adiposity Estimator) The formula is: -44.988 + (0.503 x age) + (10.689 x gender) + (3.172 x BMI) - (0.026 x BMI2) + (0.181 x BMI x gender) - (0.02 x BMI x age) - (0.005 x BMI2x gender) + (0.00021 x BMI2 x age). Where male sex equals 0 and female sex equals 1 obesity defined as BF% ≥25% (men) or ≥35% (women) (48).
● Metabolic score for visceral fat (METS-VF) METS-VF = 4.466+0.011 x (Ln (METS-IR))3 + 3.239 x (Ln (WtHR))3 + 0.319 x (Sex) + 0.594 x (Ln(age)). Man = 1 woman = 0 METS-IR = Ln [(2 x glycaemia) + Triglycerides] x BMI)/(Ln[HDLc]) High risk is considered as from 7,18 (49).
Primary outcomes were dichotomous indicators: BMI obesity, high WtHR, CUN-BAE obesity, and high METS-VF.
Statistical analysis
Analyses were performed with SPSS v29.0 (IBM, Armonk, NY). Continuous variables are presented as mean ± SD and categorical variables as counts and percentages. Group differences were tested using Student’s t-test or ANOVA (with Bonferroni correction for multiple comparisons) and χ² tests for categorical data.
We estimated sex-stratified and pooled associations between determinants and each obesity outcome using multivariable logistic regression, reporting adjusted odds ratios (OR) and 95% confidence intervals (CI). Models adjusted for age group, sex (in pooled models), social class, smoking, physical activity (IPAQ), Mediterranean diet adherence (MEDAS), and social isolation (ESSI). To avoid multicollinearity, obesity indices were analyzed separately as outcomes and not jointly as predictors. Variance Inflation Factors (VIF) were inspected (VIF<2 considered acceptable). Model calibration was assessed with the Hosmer–Lemeshow test, and discrimination with the area under the ROC curve (AUC).
Sensitivity analyses included: (i) alternative WtHR cut-offs (0.55) and CUN-BAE obesity thresholds reported in European cohorts; (ii) models further adjusted for systolic BP, triglycerides, and HDL-c; (iii) exclusion of participants with potential measurement outliers; and (iv) complete-case analyses versus multiple imputation for variables with ≤5% missingness (results materially unchanged; complete-case shown). Statistical significance was p < 0.05.
Multivariable logistic regression models were developed to evaluate the associations between sociodemographic, lifestyle, and social isolation variables with obesity indices. Variables were retained in the models using a stepwise backward elimination approach with p < 0.05. Effect modification was assessed by testing interaction terms (e.g., sex × predictor, age × predictor), using a significance criterion of p <0.05. All models were adjusted for sex as a covariate to control for potential confounding. Preliminary sex-stratified analyses showed consistent results between men and women; therefore, for clarity and conciseness, stratified results are not presented in the main manuscript.
Results
The Table 1 summarizes the fundamental anthropometric profile of the cohort stratified by sex. Men displayed greater height and weight compared to women, while mean age differences were small but statistically significant. These findings highlight the sex-specific differences in body size that are critical for interpreting obesity indices. Establishing these baseline differences provides essential context for subsequent analyses, particularly since sex influences fat distribution and the diagnostic accuracy of obesity indices.
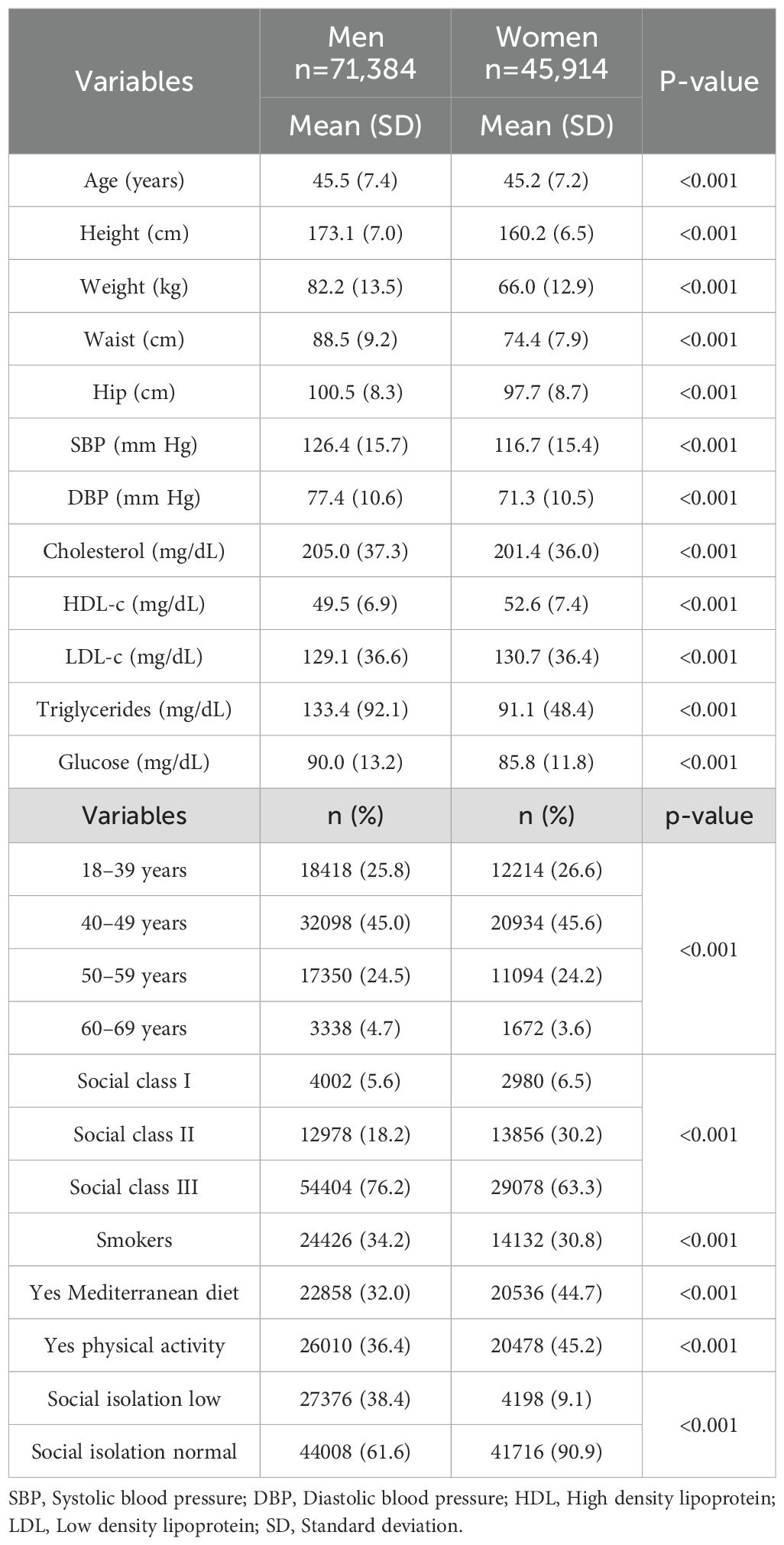
Table 1. Baseline anthropometric characteristics of men and women in the study population.
The Table 2 summarizes the mean and standard deviation of four obesity indices (BMI, WtHR, CUN-BAE, and METS-VF) stratified by sociodemographic and lifestyle characteristics in men and women. Results show a progressive increase in obesity indices with advancing age in both sexes. Social gradients are evident, with participants in lower social classes exhibiting higher adiposity markers compared with those in higher classes. Smoking status was associated with higher mean obesity indices among smokers compared with non-smokers. Furthermore, adherence to the Mediterranean diet and regular physical activity were linked to significantly lower obesity measures, underscoring their protective role. Finally, individuals with low social integration presented with markedly higher obesity indices compared to those with normal social integration, highlighting the potential impact of psychosocial factors on obesity risk.
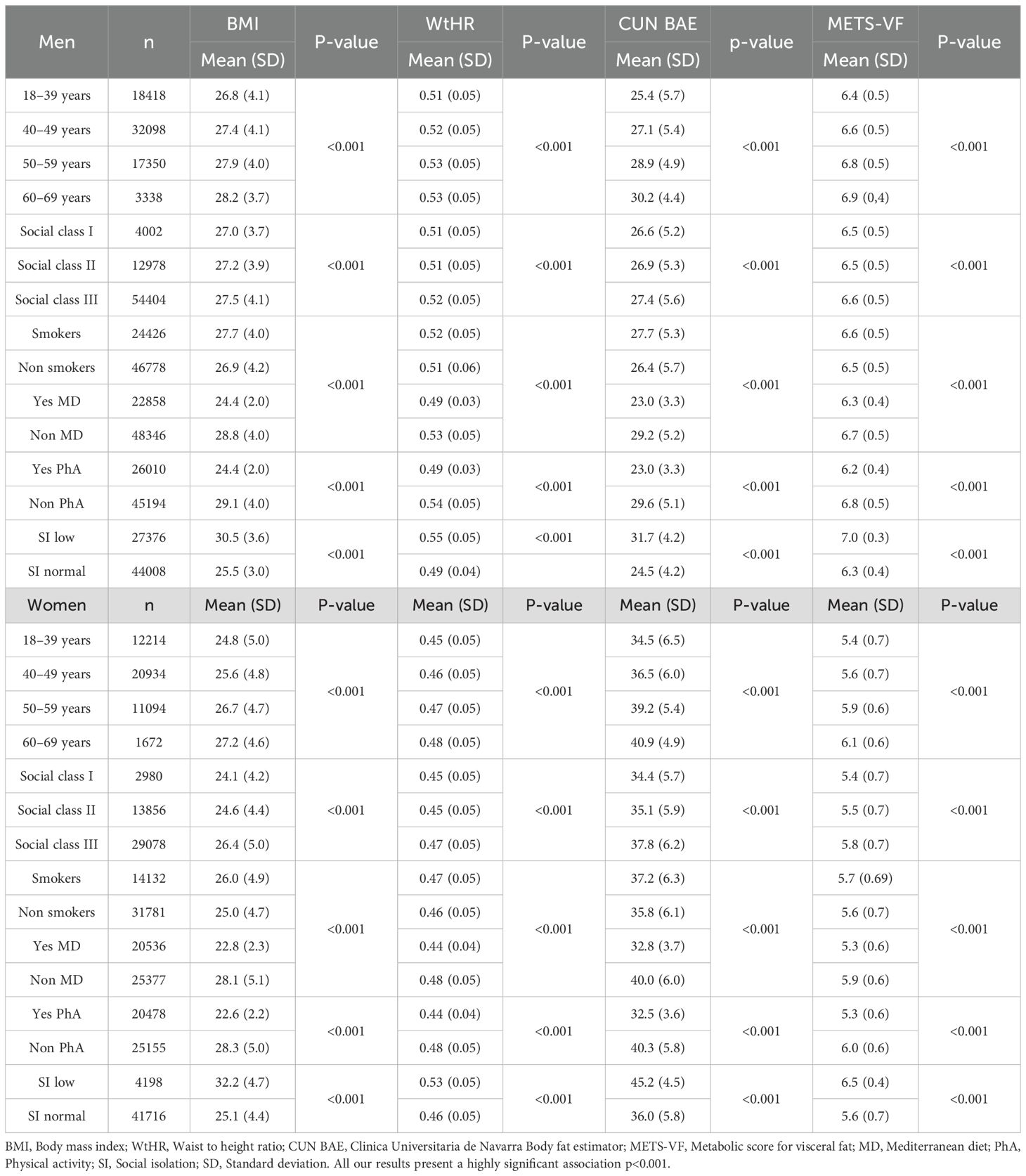
Table 2. Mean values of obesity indices (BMI, WtHR, CUN-BAE, METS-VF) according to age, social class, smoking status, Mediterranean diet adherence, physical activity, and social isolation, stratified by sex.
The Table 3 displays the prevalence of obesity and elevated adiposity according to different anthropometric and metabolic indices across key sociodemographic and lifestyle variables in men and women. The prevalence of obesity increased progressively with age for all indices, with the steepest rise observed in CUN-BAE and METS-VF categories. Clear social inequalities were found, as lower social classes showed higher prevalence of obesity compared with upper social classes. Smokers exhibited higher prevalence of obesity and central adiposity than non-smokers. Conversely, participants adhering to the Mediterranean diet or engaging in regular physical activity showed markedly lower prevalence of obesity across all indices. Importantly, low social integration was associated with significantly higher rates of obesity and central adiposity, reinforcing the role of psychosocial determinants in metabolic health.
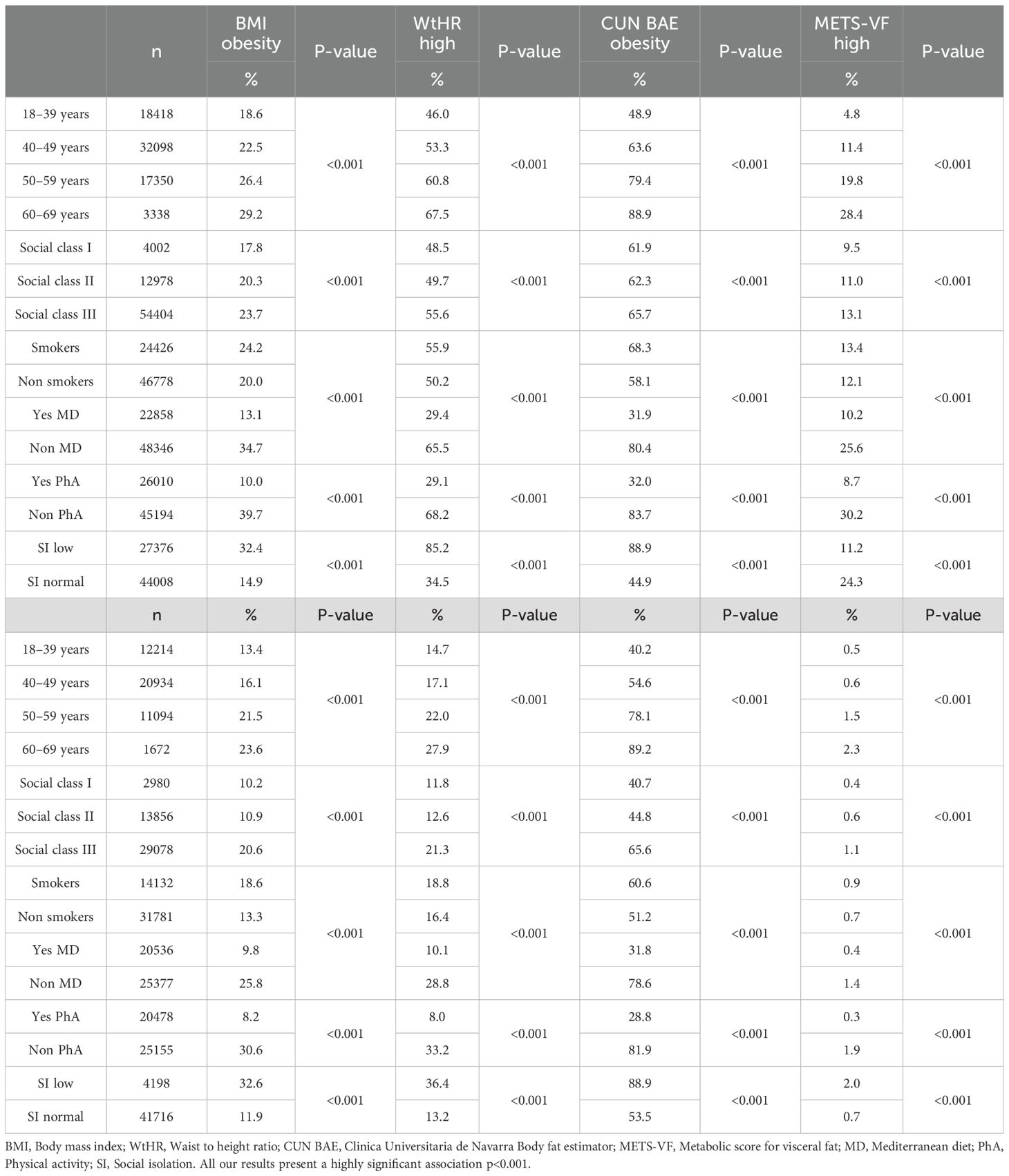
Table 3. Prevalence of obesity and elevated obesity indices (BMI obesity, high WtHR, CUN-BAE obesity, high METS-VF) according to age, social class, smoking status, Mediterranean diet adherence, physical activity, and social isolation, stratified by sex.
The Table 4; Figure 2 presents adjusted odds ratios (OR) and 95% confidence intervals (CI) from multivariable logistic regression models evaluating the associations of sociodemographic, lifestyle, and psychosocial variables with four obesity outcomes. Models were adjusted for potential confounders, including age, social class, smoking, Mediterranean diet adherence, physical activity, and social isolation. Results demonstrate consistent associations across indices: older age groups and lower social classes were strongly associated with higher odds of obesity in both men and women. Smoking was linked to elevated odds of central obesity, particularly with WtHR and METS-VF. Conversely, adherence to the Mediterranean diet and regular physical activity were protective factors, showing reduced odds of obesity across all indices. Notably, social isolation emerged as a significant determinant, with individuals reporting low social integration having higher odds of obesity, independent of traditional lifestyle and socioeconomic factors. These findings underscore the importance of incorporating psychosocial dimensions into obesity prevention strategies.
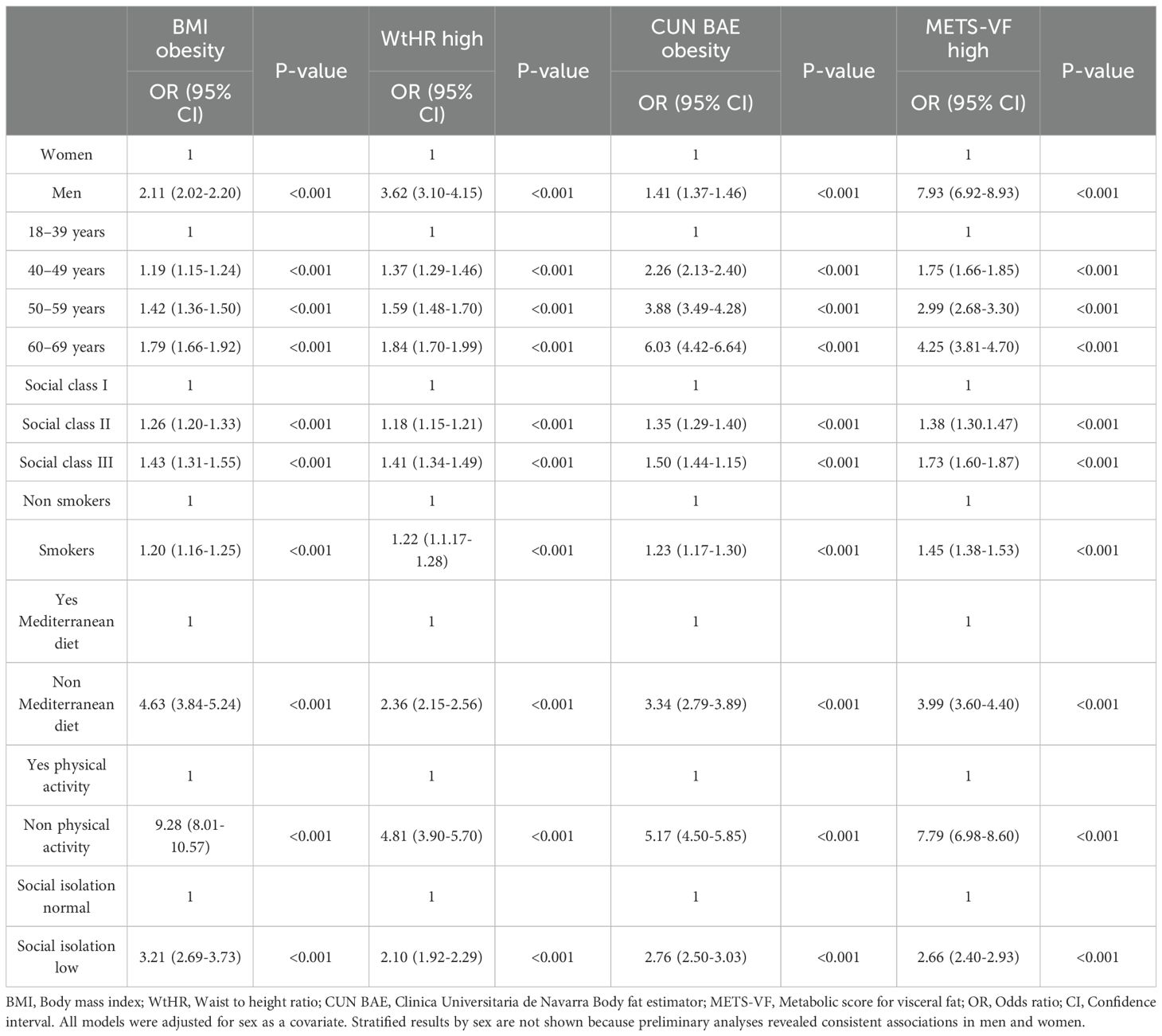
Table 4. Multivariable models assessing the association between sociodemographic, lifestyle, and social isolation variables with obesity indices (adjusted for sex).
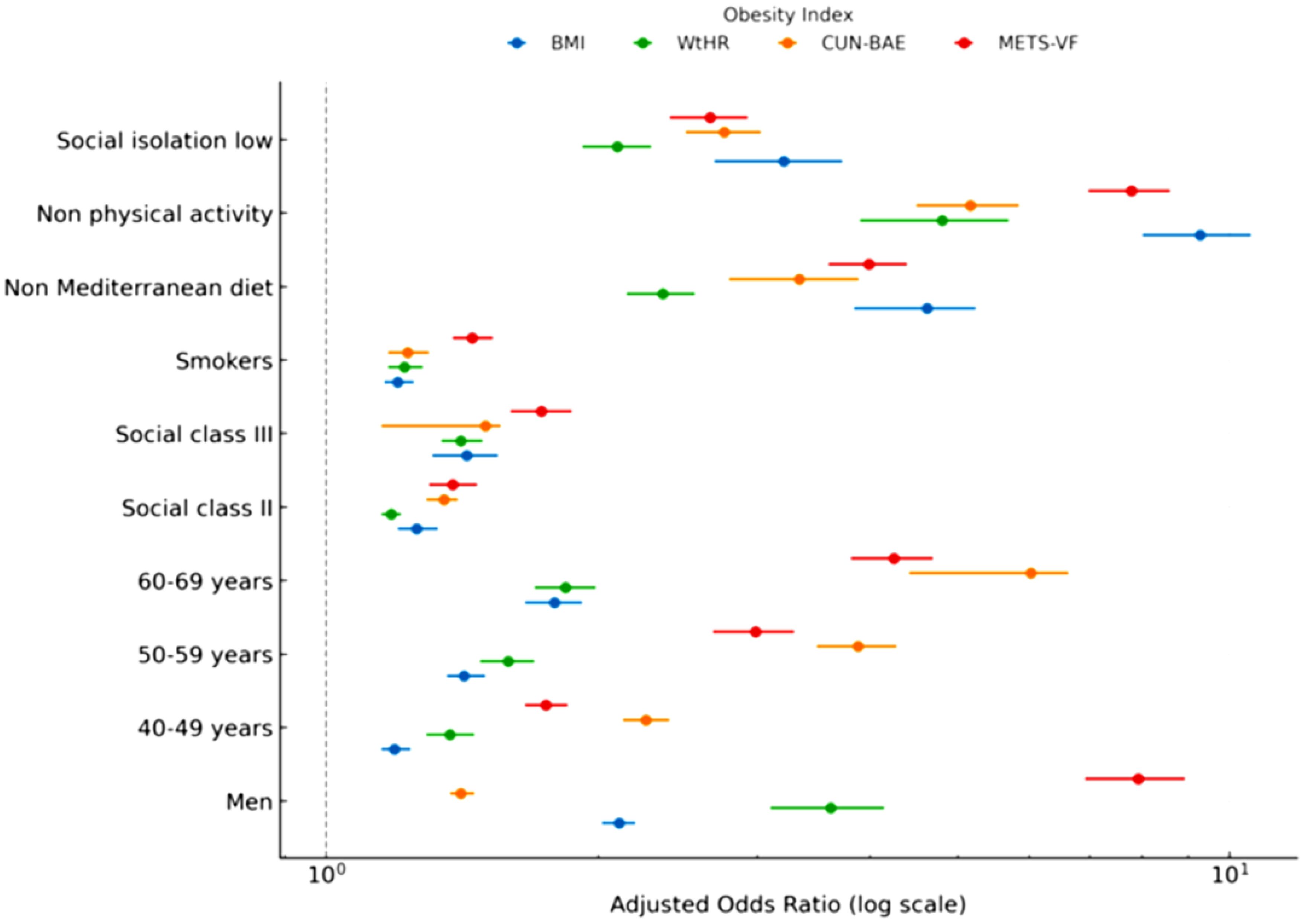
Figure 2. Forest plot of logistic regression results.
Table 4. Adjusted odds ratios (OR) and 95% confidence intervals (CI) for obesity according to sociodemographic variables, lifestyle habits, and social isolation, evaluated across four obesity indices (BMI, WtHR, CUN-BAE, METS-VF). Models were adjusted for age group, sex (in pooled models), social class, smoking, physical activity (IPAQ), Mediterranean diet adherence (MEDAS), and social isolation (ESSI). Reference categories: women, 18–39 years, social class I, non-smokers, high adherence to the Mediterranean diet, physically active, and normal social support.
Discussion
Main findings
In this large occupational cohort of Spanish workers, we found that obesity indices—BMI, WtHR, CUN-BAE, and METS-VF—were strongly associated with sociodemographic characteristics, lifestyle behaviors, and perceived social isolation. Male sex, older age, lower social class, physical inactivity, poor adherence to the Mediterranean diet, smoking, and higher levels of social isolation were consistently linked to greater odds of obesity, irrespective of the index applied. Sensitivity analyses excluding participants with extreme BMI values (<18.5 or >40 kg/m²) and those with missing covariates yielded results consistent with the main findings. These analyses confirmed the robustness of the associations and are presented in Supplementary Tables S5, S6.
Comparison with previous studies
Our findings are consistent with prior epidemiological research that has established sociodemographic disparities in obesity prevalence. Multiple studies have shown that men and older adults exhibit higher rates of central and visceral obesity, measured by WtHR or METS-VF, compared to women and younger populations (50, 51). Lower socioeconomic position is also a recognized determinant of obesity, partly due to disparities in access to healthy foods, occupational demands, and opportunities for physical activity (52, 53). With respect to lifestyle habits, poor diet quality and low levels of physical activity have been repeatedly associated with increased obesity risk in European and Mediterranean cohorts (54, 55). The Mediterranean diet, in particular, has been inversely related to obesity and central adiposity, reflecting its emphasis on nutrient-rich, anti-inflammatory foods (56).
Our study also reinforces emerging evidence linking social isolation to obesity. Recent population-based research has identified social isolation and poor social support as independent predictors of obesity and related cardiometabolic outcomes (42, 57). The mechanisms through which social isolation may contribute to obesity are multifaceted. Isolation due to illness may reduce opportunities for physical activity, while isolation associated with aging or lack of social support can increase sedentary behavior and unhealthy dietary patterns (58, 59). These factors synergistically contribute to weight gain and adiposity, highlighting the importance of addressing psychosocial determinants in obesity prevention strategies (60). Mechanisms proposed include reduced engagement in healthy behaviors, higher prevalence of depression and stress-related eating, and altered physiological pathways involving the hypothalamic–pituitary–adrenal axis (61, 62). By integrating these findings into an occupational setting, our analysis highlights that psychosocial factors, alongside traditional determinants, play an important role in obesity development among working adults.
Potential mechanisms
Several biological and behavioral mechanisms may explain the observed associations. Aging is accompanied by changes in body composition, including a decline in lean mass and preferential fat accumulation in visceral depots, which increases risk for metabolic dysfunction (63). Sex differences may relate to hormonal influences on fat distribution; premenopausal women typically store more subcutaneous fat, whereas men accumulate more visceral fat, which confers greater cardiometabolic risk (64). Lower social class may predispose individuals to energy-dense dietary patterns, reduced leisure time for physical activity, and higher occupational stress, all of which favor weight gain (65).
Lifestyle factors interact synergistically with these determinants. Physical inactivity reduces energy expenditure and alters mitochondrial function, while poor dietary quality promotes adiposity through excessive caloric intake and impaired satiety regulation (66). Smoking shows complex associations; while nicotine can reduce weight in the short term, smoking cessation is often followed by weight gain, and chronic smoking is linked to central obesity and metabolic dysfunction (67). Social isolation further exacerbates these pathways. Individuals with limited social networks may experience higher stress and reduced accountability for maintaining healthy routines, leading to maladaptive behaviors such as sedentary lifestyles and unhealthy eating (68). Physiologically, social isolation has been associated with dysregulation of cortisol, inflammatory cytokines, and autonomic balance, all of which can facilitate fat deposition and insulin resistance (69).
Strengths and limitations
The strengths of this study include its very large sample size, the comprehensive evaluation of four obesity indices that capture distinct dimensions of adiposity, and the simultaneous consideration of sociodemographic, lifestyle, and psychosocial determinants. The inclusion of validated instruments for diet (MEDAS), physical activity (IPAQ), and social isolation (ESSI) enhances the reliability of the measurements. Furthermore, the stratified analyses by sex and the application of multiple sensitivity tests add robustness to the findings.
However, several limitations should be noted. First, the cross-sectional design prevents causal inference; associations may be bidirectional, particularly regarding social isolation and obesity. Longitudinal studies are necessary to clarify temporal relationships. Second, obesity indices, although validated, rely on anthropometric and bioelectrical estimations rather than gold-standard imaging techniques such as DXA or MRI. This may introduce misclassification, though the large sample size likely mitigates random error. Third, although adjustments were made for major confounders, residual confounding by unmeasured variables (e.g., genetic predisposition, occupational stressors, sleep quality) cannot be excluded. Fourth, social isolation was assessed with a brief validated instrument, which may not capture the full spectrum of social connectedness and loneliness. Finally, the study population consisted of Spanish workers, which may limit generalizability to unemployed individuals, older populations, or different cultural contexts.
Although sex was included as an adjusting variable in all multivariable models, preliminary stratified analyses showed consistent associations across men and women, without meaningful differences in direction or magnitude. For this reason, we did not present sex-stratified results, prioritizing clarity and conciseness in the main manuscript.
The consistency of the findings was further supported by sensitivity analyses (Supplementary Tables S5, S6), which excluded participants with extreme BMI values and those with missing covariates, showing that the associations remained robust across different model specifications.
Implications for public health and future research
Our findings have important implications for public health and occupational health strategies. The consistent associations between obesity indices and sociodemographic and lifestyle determinants underscore the need for integrated interventions that go beyond individual-level counseling to address structural and social determinants of health. Workplace-based programs promoting adherence to the Mediterranean diet, physical activity, and smoking cessation may be particularly effective in reducing obesity burden. Additionally, the novel role of social isolation as a correlate of obesity highlights the importance of fostering social support and connectedness in preventive strategies. Interventions that integrate social engagement, peer support, and mental health promotion could yield dual benefits for obesity and overall well-being.
Future research should adopt longitudinal designs to unravel causal pathways linking social isolation and other psychosocial factors with obesity. Studies incorporating biomarkers of stress, inflammation, and neuroendocrine function could elucidate biological mediators. Moreover, comparisons across occupational groups and cultural settings will be necessary to determine the generalizability of these findings. Ultimately, multi-component interventions addressing sociodemographic disparities, lifestyle habits, and psychosocial well-being are likely to be most effective in tackling the obesity epidemic.
Conclusions
In this large occupational cohort of Spanish workers, obesity indices—including BMI, WtHR, CUN-BAE, and METS-VF—were strongly associated with sociodemographic, lifestyle, and psychosocial determinants. Male sex, older age, lower social class, poor adherence to the Mediterranean diet, physical inactivity, smoking, and higher levels of social isolation emerged as consistent correlates of obesity across all indices. These findings underscore the multidimensional nature of obesity, reflecting the interplay of biological, behavioral, socioeconomic, and psychosocial factors.
The study contributes novel evidence by integrating social isolation into the framework of obesity determinants, demonstrating that individuals with limited social support are at higher risk of excess adiposity. This highlights the importance of considering psychosocial environments in addition to traditional biomedical and behavioral factors when addressing obesity.
From a public health perspective, the results emphasize the need for comprehensive prevention strategies that simultaneously target lifestyle behaviors, reduce socioeconomic disparities, and enhance social connectedness. Workplace-based interventions may represent an effective avenue to promote healthy eating, physical activity, and supportive social environments, particularly in populations at elevated cardiometabolic risk.
Future research should prioritize longitudinal studies to clarify causal pathways, assess the role of psychosocial stress and biological mediators, and explore the generalizability of these findings across cultural and occupational settings. Ultimately, tackling obesity will require a multi-level approach that addresses not only individual behaviors but also the broader social and structural determinants of health.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Research Ethics Committee of the Balearic Islands (Comité de Ética de la Investigación de las Islas Baleares, CEI-IB; protocol code IB 4383/20, 26 November 2020). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
ÁL: Conceptualization, Methodology, Writing – review & editing. PR: Conceptualization, Data curation, Investigation, Writing – original draft. PT: Data curation, Writing – original draft. IC: Methodology, Writing – original draft. CB: Conceptualization, Formal Analysis, Writing – original draft, Writing – review & editing. JR: Validation, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, and/or publication of this article.
Acknowledgments
We gratefully acknowledge all study participants for their invaluable contribution of time, commitment, and personal data. We are especially thankful to the occupational health professionals and data management teams, whose expertise in data collection, anonymization, and processing made this research possible. Our appreciation also extends to the technical and administrative staff of ADEMA University School for their consistent support during every stage of the project. Finally, we recognize the collaborating institutions for providing the infrastructure and database access essential to the successful execution of this investigation.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fendo.2025.1695705/full#supplementary-material
References
1. World Health Organization. Obesity and overweight. In: WHO Fact Sheet (2023). Available online at: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (Accessed September 23, 2025).
2. NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: a pooled analysis of 2416 population-based measurement studies in 128·9 million children, adolescents, and adults. Lancet. (2017) 390:2627–42. doi: 10.1016/S0140-6736(17)32129-3
3. Aranceta-Bartrina J, Pérez-Rodrigo C, Alberdi-Aresti G, Ramos-Carrera N, and Lázaro-Masedo S. Prevalence of general obesity and abdominal obesity in the Spanish adult population (Aged 25–64 years) 2014-2015: the ENPE study. Rev Esp Cardiol (Engl Ed). (2016) 69:579–87. doi: 10.1016/j.rec.2016.02.009
4. Marina Arroyo M, Ramírez Gallegos I, López-González AA, Vicente-Herrero MT, Vallejos D, Tárraga López PJ, et al. Equation Córdoba body fat values according to sociodemographic variables and healthy habits in 386924 Spanish workers. Acad J Health Sci. (2024) 39:31–9. doi: 10.3306/AJHS.2024.39.05.31
5. Oztenekecioglu BH, Becer E, and Kalkan R. Examination of the promotor methylation of the TRIM3 gene in obesity. Acad J Health Sci. (2024) 39:87–91. doi: 10.3306/AJHS.2024.39.02.87
6. Deehan EC, Mocanu V, and Madsen KL. Effects of dietary fibre on metabolic health and obesity. Nat Rev Gastroenterol Hepatol. (2024) 21:301–18. doi: 10.1038/s41575-023-00891-z
7. Pigsborg K, Kalea AZ, De Dominicis S, and Magkos F. Behavioral and psychological factors affecting weight loss success. Curr Obes Rep. (2023) 12:223–30. doi: 10.1007/s13679-023-00511-6
8. Kawai T, Autieri MV, and Scalia R. Adipose tissue inflammation and metabolic dysfunction in obesity. Am J Physiol Cell Physiol. (2021) 320:C375–91. doi: 10.1152/ajpcell.00379.2020
9. Wagner R, Eckstein SS, Yamazaki H, Gerst F, Machann J, Jaghutriz BA, et al. Metabolic implications of pancreatic fat accumulation. Nat Rev Endocrinol. (2022) 18:43–54. doi: 10.1038/s41574-021-00573-3
10. Sweatt K, Garvey WT, and Martins C. Strengths and limitations of BMI in the diagnosis of obesity: what is the path forward? Curr Obes Rep. (2024) 13:584–95. doi: 10.1007/s13679-024-00580-1
11. Salmón-Gómez L, Catalán V, Frühbeck G, and Gómez-Ambrosi J. Relevance of body composition in phenotyping the obesities. Rev Endocr Metab Disord. (2023) 24:809–23. doi: 10.1007/s11154-023-09796-3
12. Ashwell M, Gunn P, and Gibson S. Waist-to-height ratio is a better screening tool than waist circumference and BMI for adult cardiometabolic risk factors: systematic review and meta-analysis. Obes Rev. (2012) 13:275–86. doi: 10.1111/j.1467-789X.2011.00952.x
13. López-González AA, Tomás-Gil P, Coll Villalonga JL, Martí-Lliteras P, González San Miguel HM, and Ramírez-Manent JI. Correlation between overweight and obesity scales and blood pressure values in 418.343 Spanish workers. Acad J Health Sci. (2023) 38:44–51. doi: 10.3306/AJHS.2023.38.03.44
14. Feng L, Chen T, Wang X, Xiong C, Chen J, Wu S, et al. Metabolism score for visceral fat (METS-VF): A new predictive surrogate for CKD risk. Diabetes Metab Syndr Obes. (2022) 15:2249–58. doi: 10.2147/DMSO.S370222
15. Ruze R, Liu T, Zou X, Song J, Chen Y, Xu R, et al. Obesity and type 2 diabetes mellitus: connections in epidemiology, pathogenesis, and treatments. Front Endocrinol (Lausanne). (2023) 14:1161521. doi: 10.3389/fendo.2023.1161521
16. Martínez-Almoyna Rifá E, Tomás-Gil P, Coll Villalonga JL, Ramírez-Manent JI, Martí-Lliteras P, and López-González AA. Relationship between nonalcoholic fatty liver disease and liver fibrosis risk scales with overweight and obesity scales in 219,477 spanish workers. Acad J Health Sci. (2023) 38:92–100. doi: 10.3306/AJHS.2023.38.04.92
17. Sastre-Alzamora T, Tomás-Gil P, Paublini H, Pallarés L, Ramírez-Manent JI, and López-González AA. Relationship between different scales of overweight and obesity and heart age values in 139634 spanish workers. Acad J Health Sci. (2023) 38:137–44. doi: 10.3306/AJHS.2023.38.06.137
18. de Andrade Mesquita L, Wayerbacher LF, Schwartsmann G, and Gerchman F. Obesity, diabetes, and cancer: epidemiology, pathophysiology, and potential interventions. Arch Endocrinol Metab. (2023) 67:e000647. doi: 10.20945/2359-3997000000647
19. Nedunchezhiyan U, Varughese I, Sun AR, Wu X, Crawford R, and Prasadam I. Obesity, inflammation, and immune system in osteoarthritis. Front Immunol. (2022) 13:907750. doi: 10.3389/fimmu.2022.907750
20. Kurnool S, McCowen KC, Bernstein NA, and Malhotra A. Sleep apnea, obesity, and diabetes - an intertwined trio. Curr Diabetes Rep. (2023) 23:165–71. doi: 10.1007/s11892-023-01510-6
21. Kumari M and Khanna A. Sarcopenic obesity and its impact on quality of life: A concise review. Curr Aging Sci. (2023) 16:194–8. doi: 10.2174/1874609816666230525161020
22. Powell-Wiley TM, Poirier P, Burke LE, Després JP, Gordon-Larsen P, Lavie CJ, et al. Obesity and cardiovascular disease: A scientific statement from the American heart association. Circulation. (2021) 143:e984–e1010. doi: 10.1161/CIR.0000000000000973
23. Janochova K, Haluzik M, and Buzga M. Visceral fat and insulin resistance - what we know? BioMed Pap Med Fac Univ Palacky Olomouc Czech Repub. (2019) 163:19–27. doi: 10.5507/bp.2018.062
24. Vekic J, Stefanovic A, and Zeljkovic A. Obesity and dyslipidemia: A review of current evidence. Curr Obes Rep. (2023) 12:207–22. doi: 10.1007/s13679-023-00518-z
25. Hanlon CL and Yuan L. Nonalcoholic fatty liver disease: the role of visceral adipose tissue. Clin Liver Dis (Hoboken). (2022) 19:106–10. doi: 10.1002/cld.1183
26. Westbury S, Oyebode O, van Rens T, and Barber TM. Obesity stigma: causes, consequences, and potential solutions. Curr Obes Rep. (2023) 12:10–23. doi: 10.1007/s13679-023-00495-3
27. Fulton S, Décarie-Spain L, Fioramonti X, Guiard B, and Nakajima S. The menace of obesity to depression and anxiety prevalence. Trends Endocrinol Metab. (2022) 33:18–35. doi: 10.1016/j.tem.2021.10.005
28. Smith NR, Zivich PN, and Frerichs L. Social influences on obesity: current knowledge, emerging methods, and directions for future research and practice. Curr Nutr Rep. (2020) 9:31–41. doi: 10.1007/s13668-020-00302-8
29. Daran B, Levasseur P, and Clément M. Updating the association between socioeconomic status and obesity in low-income and lower-middle-income sub-Saharan African countries: A literature review. Obes Rev. (2023) 24:e13601. doi: 10.1111/obr.13601
30. Cooper AJ, Gupta SR, Moustafa AF, and Chao AM. Sex/gender differences in obesity prevalence, comorbidities, and treatment. Curr Obes Rep. (2021) 10:458–66. doi: 10.1007/s13679-021-00453-x
31. Kim MS, Shim I, Fahed AC, Do R, Park WY, Natarajan P, et al. Association of genetic risk, lifestyle, and their interaction with obesity and obesity-related morbidities. Cell Metab. (2024) 36:1494–503.e3. doi: 10.1016/j.cmet.2024.06.004
32. Nascè A and Pataky Z. Quelle relation entre alcool et obésité? [What is the relationship between alcohol and obesity]? Rev Med Suisse. (2023) 19:552–4. doi: 10.53738/REVMED.2023.19.819.552
33. Lengton R, Schoenmakers M, Penninx BWJH, Boon MR, and van Rossum EFC. Glucocorticoids and HPA axis regulation in the stress-obesity connection: A comprehensive overview of biological, physiological and behavioural dimensions. Clin Obes. (2025) 15:e12725. doi: 10.1111/cob.12725
34. Rogers EM, Banks NF, and Jenkins NDM. The effects of sleep disruption on metabolism, hunger, and satiety, and the influence of psychosocial stress and exercise: A narrative review. Diabetes Metab Res Rev. (2024) 40:e3667. doi: 10.1002/dmrr.3667
35. Luo J and Hendryx M. Mediation analysis of social isolation and mortality by health behaviors. Prev Med. (2022) 154:106881. doi: 10.1016/j.ypmed.2021.106881
36. Yue X, Yuan Q, Zhou R, and Wang M. Social isolation, healthy lifestyle, and intrinsic capacity among older adults in China: A longitudinal study. J Nutr Health Aging. (2025) 29:100583. doi: 10.1016/j.jnha.2025.100583
37. Alacreu-Crespo A, Sebti E, Moret RM, and Courtet P. From social stress and isolation to autonomic nervous system dysregulation in suicidal behavior. Curr Psychiatry Rep. (2024) 26:312–22. doi: 10.1007/s11920-024-01503-6
38. Queen NJ, Huang W, Komatineni S, Mansour AG, Xiao R, Chrislip LA, et al. Social isolation exacerbates diet-induced obesity and peripheral inflammation in young male mice under thermoneutrality. iScience. (2023) 26:106259. doi: 10.1016/j.isci.2023.106259
39. Delolmo-Romero S, Correa-Rodríguez M, Sánchez-Martínez MC, Gil-Gutiérrez R, Ortego-Centeno N, and Rueda-Medina B. Social health and its influence on metabolic health among a rural population: A cross-sectional study. Clin Nurs Res. (2024) 33:9–18. doi: 10.1177/10547738231184935
40. Cheng P and Drake CL. Psychological impact of shift work. Curr Sleep Med Rep. (2018) 4:104–9. doi: 10.1007/s40675-018-0114-7
41. Matthews TA and Li J. Adverse childhood experiences, social isolation, job strain, and cardiovascular disease mortality in U.S. Older employees. Med (Kaunas). (2023) 59:1304. doi: 10.3390/medicina59071304
42. Hajek A, Kretzler B, and König HH. The association between obesity and social isolation as well as loneliness in the adult population: A systematic review. Diabetes Metab Syndr Obes. (2021) 14:2765–73. doi: 10.2147/DMSO.S313873
43. Martínez Jover A, López González AA, Tomás Gil P, Coll Villalonga JL, Martí Lliteras P, and Ramírez Manent JI. Variables influencing the appearance of metabolic syndrome with three different definitions in 418.343 spanish workers. Acad J Health Sci. (2023) 38:129–35. doi: 10.3306/AJHS.2023.38.04.129
44. Mestre-Font M, Busquets-Cortés C, Ramírez-Manent JI, Tomás-Gil P, Paublini H, and López-González AA. Influence of sociodemographic variables and healthy habits on the values of overweight and obesity scales in 386,924 Spanish workers. Acad J Health Sci. (2024) 39:27–35. doi: 10.3306/AJHS.2024.39.01.27
45. Celada Roldán C, López Diez J, Rider F, Tárraga Marcos A, Tárraga Marcos ML, Tárraga López PJ, et al. Impact of adherence to the Mediterranean diet on health-related quality of life in poorly controlled diabetics. Acad J Health Sci. (2024) 39:103–12. doi: 10.3306/AJHS.2024.39.01.103
46. WHO. Waist circumference and waist-hip ratio: Report of a WHO expert consultation, Geneva, 8–11 December 2008. Geneva: World Health Organization (2011). Available online at: https://iris.who.int/bitstream/handle/10665/44583/9789241501491_eng.pdf?sequence=1 (Accessed September 23, 2025).
47. Salinas-Rehbein B, Terán-Mendoza O, and Cancino V. Social support and aging: psychometric analysis of the ENRICHD Social Support Instrument in a Chilean population over 50. Psicol Reflex Crit. (2025) 38:1. doi: 10.1186/s41155-024-00329-8
48. Chen X, Geng S, Shi Z, Ding J, Li H, Su D, et al. Association of the CUN-BAE body adiposity estimator and other obesity indicators with cardiometabolic multimorbidity: a cross-sectional study. Sci Rep. (2024) 14:10557. doi: 10.1038/s41598-024-52164-7
49. Bello-Chavolla OY, Antonio-Villa NE, Vargas-Vázquez A, Viveros-Ruiz TL, Almeda-Valdes P, Gomez-Velasco D, et al. Metabolic Score for Visceral Fat (METS-VF), a novel estimator of intra-abdominal fat content and cardio-metabolic health. Clin Nutr. (2020) 39:1613–21. doi: 10.1016/j.clnu.2019.07.012
50. Koceva A, Herman R, Janez A, Rakusa M, and Jensterle M. Sex- and gender-related differences in obesity: from pathophysiological mechanisms to clinical implications. Int J Mol Sci. (2024) 25:7342. doi: 10.3390/ijms25137342
51. Malandrino N, Bhat SZ, Alfaraidhy M, Grewal RS, and Kalyani RR. Obesity and aging. Endocrinol Metab Clin North Am. (2023) 52:317–39. doi: 10.1016/j.ecl.2022.10.001
52. Anekwe CV, Jarrell AR, Townsend MJ, Gaudier GI, Hiserodt JM, and Stanford FC. Socioeconomics of obesity. Curr Obes Rep. (2020) 9:272–9. doi: 10.1007/s13679-020-00398-7
53. Naghizadeh M, Maskouni SJ, Mortazavi Z, Ahmadi M, and Shokri S. The impact of fast food consumption on the development of general and central obesity. Acad J Health Sci. (2024) 39:44–8. doi: 10.3306/AJHS.2024.39.01.44
54. Al-Jawaldeh A and Abbass MMS. Unhealthy dietary habits and obesity: the major risk factors beyond non-communicable diseases in the eastern mediterranean region. Front Nutr. (2022) 9:817808. doi: 10.3389/fnut.2022.817808
55. Mesas AE, Guallar-Castillón P, León-Muñoz LM, Graciani A, López-García E, Gutiérrez-Fisac JL, et al. Obesity-related eating behaviors are associated with low physical activity and poor diet quality in Spain. J Nutr. (2012) 142:1321–8. doi: 10.3945/jn.112.158154
56. Konieczna J, Ruiz-Canela M, Galmes-Panades AM, Abete I, Babio N, Fiol M, et al. An energy-reduced Mediterranean diet, physical activity, and body composition: an interim subgroup analysis of the PREDIMED-plus randomized clinical trial. JAMA Netw Open. (2023) 6:e2337994. doi: 10.1001/jamanetworkopen.2023.37994
57. Zhou J, Tang R, Wang X, Li X, Heianza Y, and Qi L. Improvement of social isolation and loneliness and excess mortality risk in people with obesity. JAMA Netw Open. (2024) 7:e2352824. doi: 10.1001/jamanetworkopen.2023.52824
58. Zhang X, Ravichandran S, Gee GC, Dong TS, Beltrán-Sánchez H, Wang MC, et al. Social isolation, brain food cue processing, eating behaviors, and mental health symptoms. JAMA Netw Open. (2024) 7:e244855. doi: 10.1001/jamanetworkopen.2024.4855
59. Sherman DW, Alfano AR, Alfonso F, Duque CR, Eiroa D, Marrero Y, et al. A systematic review of the relationship between social isolation and physical health in adults. Healthcare (Basel). (2024) 12:1135. doi: 10.3390/healthcare12111135
60. Delerue Matos A, Barbosa F, Cunha C, Voss G, and Correia F. Social isolation, physical inactivity and inadequate diet among European middle-aged and older adults. BMC Public Health. (2021) 21:924. doi: 10.1186/s12889-021-10956-w
61. Wu F and Sheng Y. Social isolation and health-promoting behaviors among older adults living with different health statuses: A cross-sectional study. Int J Nurs Sci. (2021) 8:304–9. doi: 10.1016/j.ijnss.2021.05.007
62. Jensen MM, Friis K, Maindal HT, Hargaard AS, Knudsen MG, Grønkjaer MS, et al. Loneliness is associated with adverse health behaviour and obesity: a Danish population-based study of 122,258 individuals. BMC Public Health. (2025) 25:375. doi: 10.1186/s12889-025-21490-4
63. Santos TWD, Pereira QC, Fortunato IM, Oliveira FS, Alvarez MC, and Ribeiro ML. Body composition and senescence: impact of polyphenols on aging-associated events. Nutrients. (2024) 16:3621. doi: 10.3390/nu16213621
64. Marlatt KL, Pitynski-Miller DR, Gavin KM, Moreau KL, Melanson EL, Santoro N, et al. Body composition and cardiometabolic health across the menopause transition. Obes (Silver Spring). (2022) 30:14–27. doi: 10.1002/oby.23289
65. Li R, Li R, Xie J, Chen J, Liu S, Pan A, et al. Associations of socioeconomic status and healthy lifestyle with incident early-onset and late-onset dementia: a prospective cohort study. Lancet Healthy Longev. (2023) 4:e693–702. doi: 10.1016/S2666-7568(23)00211-8
66. Lemos GO, Torrinhas RS, and Waitzberg DL. Nutrients, physical activity, and mitochondrial dysfunction in the setting of metabolic syndrome. Nutrients. (2023) 15:1217. doi: 10.3390/nu15051217
67. Wu MC, Nfor ON, Liaw YP, Su YJ, and Ho CC. Associations of cigarette smoking with general and abdominal obesity risks among men in Taiwan. BMC Public Health. (2025) 25:649. doi: 10.1186/s12889-025-21821-5
68. Holt-Lunstad J. Loneliness and social isolation as risk factors: the power of social connection in prevention. Am J Lifestyle Med. (2021) 15:567–73. doi: 10.1177/15598276211009454
Keywords: obesity, body mass index, sociodemographic factors, lifestyle, social isolation, Mediterranean diet, motor activity, Spain
Citation: Riutord-Sbert P, Tárraga López PJ, López-González ÁA, Coll Campayo I, Busquets-Cortés C and Ramírez Manent JI (2025) Obesity indices and their sociodemographic, lifestyle, and social isolation correlates in a large Spanish working population. Front. Endocrinol. 16:1695705. doi: 10.3389/fendo.2025.1695705
Received: 30 August 2025; Accepted: 25 September 2025;
Published: 10 October 2025.
Edited by:
Yuanyuan Wang, Monash University, AustraliaReviewed by:
Julian Esparza-Romero, National Council of Science and Technology (CONACYT), MexicoNader Saki, Ahvaz Jundishapur University of Medical Sciences, Iran
Copyright © 2025 Riutord-Sbert, Tárraga López, López-González, Coll Campayo, Busquets-Cortés and Ramírez Manent. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ángel Arturo López-González, YW5nYXJ0dXJvQGdtYWlsLmNvbQ==
†ORCID: Pere Riutord-Sbert, orcid.org/0000-0003-2135-9699
Pedro Juan Tárraga López, orcid.org/0000-0002-5222-5784
Ángel Arturo López-González, orcid.org/0000-0002-7439-8117
Irene Coll Campayo, orcid.org/0000-0002-5423-9290
Carla Busquets-Cortés, orcid.org/0000-0001-9367-2137
José Ignacio Ramírez Manent, orcid.org/0000-0001-6887-4562