 Cornelia M. van Schewick1,2
Cornelia M. van Schewick1,2 Christina Nöltner2
Christina Nöltner2 Svenja Abel1,2
Svenja Abel1,2 Siobhan O. Burns1
Siobhan O. Burns1 Sarita Workman1Andrew Symes1
Sarita Workman1Andrew Symes1 David Guzman1
David Guzman1 Michele Proietti2Alla Bulashevska2Fernando Moreira1Veronika Soetedjo3
Michele Proietti2Alla Bulashevska2Fernando Moreira1Veronika Soetedjo3 David M. Lowe1*
David M. Lowe1* Bodo Grimbacher1,2,4,5,6*
Bodo Grimbacher1,2,4,5,6*- 1Institute of Immunity and Transplantation, Royal Free Hospital, University College London, London, United Kingdom
- 2Center for Chronic Immunodeficiency, Medical Center, Faculty of Medicine, Institute for Immunodeficiency, Albert-Ludwigs-University Freiburg, Freiburg, Germany
- 3Freiburg Center for Data Analysis and Modeling (FDM), IMBI/ZKS, Freiburg, Germany
- 4DZIF – German Center for Infection Research, Satellite Center Freiburg, Freiburg, Germany
- 5CIBSS - Centre for Integrative Biological Signalling Studies, Albert-Ludwigs-University Freiburg, Freiburg, Germany
- 6RESIST – Cluster of Excellence 2155 to Hanover Medical School, Satellite Center Freiburg, Freiburg, Germany
Background: Diarrhoea is the commonest gastrointestinal symptom in patients with common variable immunodeficiency (CVID).
Objective: The aim of this study was to describe the prevalence and clinical presentation of chronic and recurrent diarrhoea in the Royal-Free-Hospital (RFH) London CVID cohort, including symptoms, infections, level of inflammation, and microbial diversity.
Methods: A cross-sectional study of adult CVID patients (139 out of 172 diagnosed with CVID completed the screening questionnaire). Those with diarrhoea ≥6 days/month had stool and blood samples analysed and completed the short Inflammatory Bowel Disease Questionnaire (sIBDQ). BMI, spleen-size, lymphocytes and gut-microbial diversity were compared. Due to logistical and clinical restraints, not all patients could be analysed on all measures.
Results: 46/139 (33.1%) patients had current significant diarrhoea. In patients with past or present diarrhoea, BMI was lower (median 23.7 vs. 26, p = 0.005), malabsorption more common (57.97 vs. 35.71%, p = 0.011). CD4+ lymphocytes were higher in patients with diarrhoea (p = 0.028; n = 138), but CD4+ naïve lymphocytes were significantly higher in non-diarrhoea patients (p = 0.009, N = 28). Nine patients had confirmed or probable current gastrointestinal infections. Calprotectin was >60 μg/g in 13/29 with significant diarrhoea including 9 without infection. SIBDQ revealed a low median score of 4.74. Microbial alpha diversity was significantly lower in CVID patients compared to healthy household controls. There was no significant difference in alpha diversity in relation to antibiotic intake during the 6 weeks prior to providing samples.
Conclusion: Patients with CVID and significant diarrhoea had infections, raised calprotectin, malabsorption, a lower BMI, an impaired quality of life (comparable to active IBD), and they differed from non-diarrhoea patients in their lymphocyte phenotyping. Furthermore, microbial diversity was altered. These findings strongly imply that there may be an inflammatory nature and a systemic predisposition to diarrhoea in CVID, which necessitates further investigation.
Introduction
Common variable immunodeficiency (CVID) is characterised by very low immunoglobulin levels of IgG and IgA or IgM (1) with a poor vaccination response due to impaired B-cell function, raised susceptibility toward infections, and autoimmune, or granulomatous manifestations. It is the commonest symptomatic primary immunodeficiency (PID) in humans (2), representing a heterogeneous set of disorders (3).
Abdominal symptoms are a burden to a large part of investigated CVID cohorts (4–8). Their reported prevalence varies from 21 to 47% (4, 8). For chronic diarrhoea, defined as diarrhoea for ≥4 weeks with or without a minimum of three bowel movements per day (9), numbers vary between 7 and 14% at time of diagnosis (7, 8) and between 22 and 77% during follow up (6–8). This makes diarrhoea the commonest abdominal symptom in CVID patients.
Immunodeficient patients may have acute or chronic Giardia spp. Infections (8, 10) and they can have chronic norovirus infections (11, 12) where bowel histology resembles coeliac disease and faecal calprotectin levels can be raised (13, 14). Campylobacter infections may also occur in CVID patients, including as a chronic infection (8, 15).
However, in addition to chronic infection, there is the suggestion that many CVID bowel complications are a separate entity, or several disease entities, which do not fit common classifications (16). The term “CVID enteropathy,” although it lacks a clear working definition, has been used to describe diverse pathological entities. We therefore focussed on the symptom of diarrhoea and sought to further understand its impact and associations.
In order to assess the relevance of “diarrhoea,” surrogate markers can be used. Calprotectin is a widely used marker indicative of (especially neutrophilic) inflammation (17). The short Inflammatory Bowel Disease Questionnaire (sIBDQ) is a validated 10 item questionnaire for the assessment of the quality of life in IBD patients (18, 19), which may be applicable to other diseases.
A system to classify the heterogenous group of CVID patients is the Euroclass classification system (20), which defines B-lymphocyte dependent phenotypes correlating with clinical features.
So far, only few investigations of the CVID microbiome have been published (21–26). The diversity of microbiota within one individual or its sample (alpha diversity) and the differences in distribution of different microbiota among samples or individuals (beta diversity) can be described. The microbiota reflects many influencing factors such as diet (27, 28), antibiotic intake (29), and genetics (30). The microbiome varies greatly interindividually (31).
The aim of this study was to describe the prevalence and clinical presentation of chronic and recurrent diarrhoea in the Royal-Free-Hospital (RFH) London CVID cohort, including symptoms, infections, level of inflammation, and the gut microbiota.
Materials and Methods
We performed a cross-sectional study of adult CVID patients (Figure 1). One hundred thirty-nine out of 172 patients diagnosed with CVID completed a newly created screening questionnaire on past and present gastrointestinal symptoms (see Supplementary Material). CVID had been diagnosed by a consultant immunologist applying standard diagnostic criteria at the time of diagnosis.
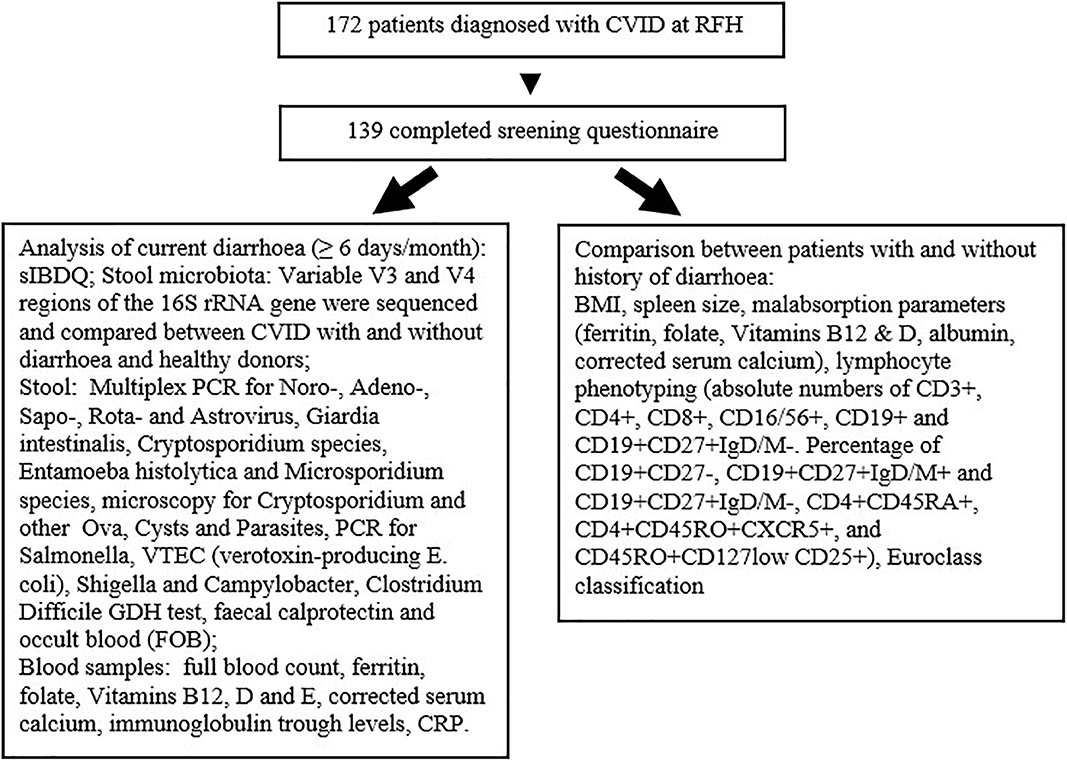
Figure 1. Investigation schema for this study.
Latest body mass index (BMI), spleen size, blood results potentially indicating (mal)absorption, lymphocyte phenotyping, and Euroclass classification were compared between patients with and without a history of diarrhoea according to screening questionnaire.
Patients with significant diarrhoea, defined as loose or liquid stools on ≥6 days/month with no regards to stool frequency had stool analysed for infections, faecal calprotectin, and occult blood (FOB). Blood samples were checked for malabsorption and inflammation and patients completed the sIBDQ. Stool and blood results of one patient who did not complete the screening questionnaire but reported to her doctor constant diarrhoea were included. Four patients who had had episodes of diarrhoea (n = 3) or no diarrhoea (n = 1) at time of screening questionnaire developed current significant diarrhoea and became eligible for these investigations.
The sIBDQ consists of 10 questions. For each item there is a 7-point Likert scale ranging from 1 for the worst to 7 for the best quality of life in this item. Higher scores represent a better quality of life.
Additional stool samples from patients with current significant diarrhoea were collected and used to analyse participants' gut microbiota and that of a person they lived with. A specific questionnaire [based on the Kieler Fragebogen für Erwachsene (32)] was completed (see Supplementary Material). A CVID control group who did not currently or formerly suffer from diarrhoea was also recruited. Stratec Stool collection tubes with Stool DNA stabilizer (Catalogue #: 1038111200) were used for stool collection. After collection, patients were advised to keep samples in the fridge and post within 24 h. After delivery to the RFH, samples were frozen at −80°C until transported to the CCI Freiburg for sequencing. Variable V3 and V4 regions of the 16S rRNA gene were sequenced using the Illumina protocol on an Illumina MiSeq, referring to the Ribosomal Database Project (33).
In order to compare the microbiota of the three study groups (CVID with and without diarrhoea and healthy household controls) alpha diversity was calculated using Shannon diversity, which weights the numbers of species by their relative evenness (34, 35).
Taxa were classified using operational taxonomic units (OTUs) using the Ribosomal Database Project Classifier (36).
Permutational multivariate analysis of variance [PERMANOVA (37)], implemented in the “adonis” function of the R package “vegan” and used with Bray-Curtis dissimilarity measure, was employed to assess the significance of differences in microbial composition between groups, called beta diversity.
For continuous variables, the Mann-Whitney U-test and the Wilcoxon Rank sum test were used. For categorical variables, the Fisher's exact test and Pearson's Chi2-test were used. Two-sided p ≤ 0.05 were considered significant.
If a question was left unanswered in the screening questionnaire or microbiome questionnaire by a participant, the denominator in our report was changed accordingly.
CVID patients and healthy controls provided written informed consent under study protocols approved by NHS Research Ethics Committees (REC 04/Q0501/119 and 08/H0720/46).
Results
Diarrhoea and Other Gastrointestinal Symptoms Are Common in Patients With CVID
One hundred thirty-nine out of 172 patients with the diagnosis of CVID at the RFH were interviewed; demographic details are provided in Table 1. At the time of questioning, 46 of 139 (33.1%) patients had diarrhoea on 6 or more days per month (Figure 2), which we defined as current significant diarrhoea; 69 of 139 (49.6%) patients either had significant diarrhoea at the time of interview or had experienced at least one diarrhoeal episode of 14 days or longer (n = 57). For 41 of these patients, episodes persisted for more than 2 months. Diarrhoea in this cohort was mostly a longstanding problem with a median duration of 15.5 years in those patients with current significant diarrhoea. A Bristol Stool Chart Type of 6 or 7 was assigned by 47 out of 63 patients with a history of diarrhoea who answered this question. The gender ratio in the overall cohort was 0.65 compared to 0.60 in the group of patients with a history of diarrhoea, p = 0.79.
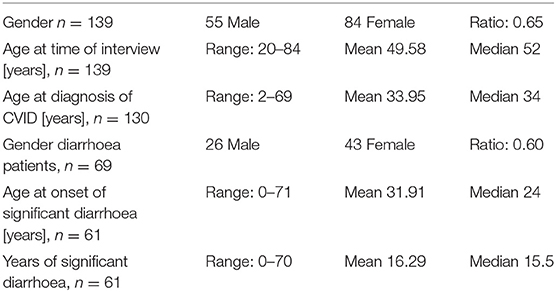
Table 1. Descriptive details of interviewed cohort of CVID patients.
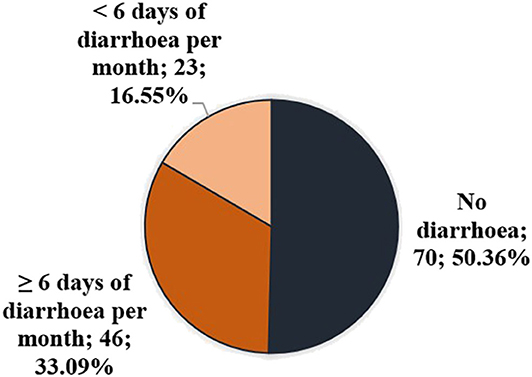
Figure 2. Prevalence of diarrhoea in cohort of CVID patients at time of interview.
Thirty-eight out of 64 patients with past or present diarrhoea (59.4%) reported at least one of four selected symptoms suggestive of IBD (38, 39). Most frequently this was diarrhoea during the night (n = 29), followed by weight loss (n = 18). These symptoms were reported by 71.8% of women compared to 40% of men. Only a minority of these patients had chronic infection (see below).
Abdominal pain (32 out of 65) and urgency to defecate (24 out of 68 patients) were also common symptoms. Seventy-one out of 132 CVID patients (53.8%) admitted frequently suffering from bloating, epigastric pain, belching and/or vomiting. Belching and epigastric pain appeared in 13.6% and 12.9% of patients (18 and 17 patients, respectively) and 46.2% (61 patients) frequently suffered from bloating and distension. Significantly more diarrhoea than non-diarrhoea patients frequently had at least one of the additional symptoms listed above (58.0 vs. 39.7%, p = 0.039).
CVID Patients With Diarrhoea Have Lower naïve CD4+ T Cell Counts
Spleen-size, lymphocyte phenotyping, Euroclass classification, BMI, and malabsorption were compared between diarrhoea and non-diarrhoea patients.
Recent spleen measurements were available for 123 patients. Thirty-nine out of 123 patients (31.7%) had splenomegaly (≥14 cm); proportions were equal in the group with and without diarrhoea.
The first ever measured total CD4+ lymphocyte count in peripheral blood was higher in diarrhoea patients (p = 0.028; n = 138), but there were significantly lower numbers of (first and last measured) naïve CD4+ lymphocytes in patients with diarrhoea (p = 0.009, n = 28 and p = 0.018, n = 28). This is depicted in Figure 3. We did not find low numbers of memory B-cells in blood to be associated with chronic diarrhoea (p = 0.266 for comparison of first, p = 0.374 for last measured memory B-cells, N = 89). There was also no significant difference between the groups in the other measured or calculated lymphocyte numbers (CD3+ T-cells, CD8+ T-cells, CD16/56+ NK cells, CD19+ B cells, switched memory B-cells, naïve B-cells, IgM+ memory B-cells, CD4+ memory T-cells, and T-regulatory cells) (see Supplementary Material).
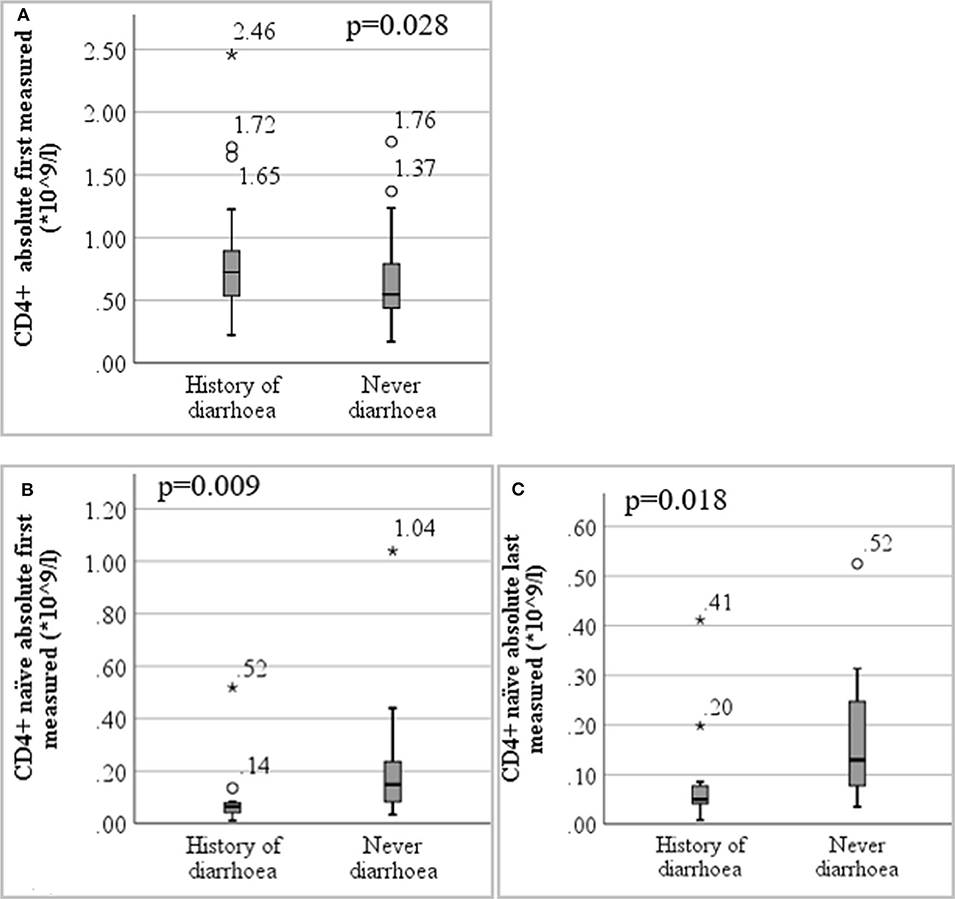
Figure 3. Boxplot of lymphocyte immunophenotyping results detailing (A) first measured CD4+ T-lymphocytes in patients with and without diarrhoea (n = 138) (B) first measured CD4+ naïve T-lymphocytes in patients with and without diarrhoea (n = 28) (C) last measured CD4+ naïve T-lymphocytes in patients with and without diarrhoea (n = 28). *are extreme outlier values (more than three interquartile ranges from the 25th or 75th percentile accordingly).
The Euroclass classification1 was available for 131 patients: 78 were classified as smB+, 14 as B-, 32 as smB-Trnorm and seven as smB-Trhi. SmB+ occurred more often in patients without diarrhoea (67.65 vs. 50.79%) but this difference was not significant.
CVID Patients With Diarrhoea Have Lower Body Mass Index and More Commonly Have Historical Indicators of Malabsorption
The BMI was significantly lower in the group of patients with past or present diarrhoea (median 23.7 in diarrhoea patients vs. 26 in non-diarrhoea patients, p = 0.005, n = 128). Out of seven underweight patients, five had current significant diarrhoea and two had had diarrhoea episodes of several months' length.
The departmental database was searched for the lowest available measurements of ferritin, folate, Vitamin B12, albumin, and corrected serum calcium as indicators of malabsorption. Malabsorption was significantly more common in patients with diarrhoea than without (40 out of 69 vs. 25 out of 70, p = 0.011).
IgA levels in both groups were similar with no significant difference observed (see Supplementary Material).
Patients With Current Significant Diarrhoea Commonly Have Evidence of Gastrointestinal Inflammation and Malabsorption but Active Infection Is Relatively Rare
Thirty-five patients with current significant diarrhoea supplied stool samples for analysis within 7 months from the interview. Of these, nine had presumed current gastrointestinal infection. For 21 patients, we were able to perform all planned tests.
Four out of 30 patients had norovirus detected, one of these was also positive for adenovirus by PCR. One further patient was negative for norovirus in this study but was later on found to be positive. One patient had CMV inclusion bodies in an ileal biopsy 2 years prior to this study, but was negative for all infectious agents tested in this study (which did not include CMV). One patient was positive by PCR for sapovirus. One of 26 patients was positive for Clostridium difficile GDH, but not for its toxin (therefore not considered as a current infection), one of 29 patients tested positive for Giardia lamblia by both PCR and microscopy. One patient had a positive Campylobacter stool PCR although stool culture was negative.
Calprotectin was elevated ≥60 μg/g in 13 out of 29 patients, and in 9 out of 21 when excluding patients with known gastrointestinal infections.
One of 23 tested patients was positive for FOB; this was the patient who had earlier been CMV-positive in a biopsy. Two patients had raised α1-antitrypsin levels in their stool (>0.47 mg/g), potentially suggesting protein losing enteropathy. One of these had norovirus, the other one did not have current test results for gastrointestinal viruses.
Blood from 43 patients was analysed in the laboratory within 6 months from the interview. It was possible to obtain all measurements from 30 patients. Five patients were anaemic, two of these with infection (Giardia, norovirus). Four of 41 patients were deficient in folate of whom two were due to infection (norovirus and CMV). Five of 40 were deficient in calcium (three due to infection: CMV, norovirus, and Giardia), two of 29 were deficient in vitamin E (both had norovirus). Two had IgG serum trough levels <5 g/l, two of 40 were deficient in vitamin B12, four of 41 in vitamin D and one of 43 in albumin (all not due to infection). This amounts to a total of nine of 43 patients (20.93%) presenting with current laboratory signs of malabsorption (excluding vitamin D, IgG trough-level, and anaemia). Of these nine, four patients had an infection (norovirus twice, CMV, and Giardia).
CVID Patients With Diarrhoea Have an Impaired Quality of Life
Twenty-six patients with current significant diarrhoea completed the short Inflammatory Bowel Disease Questionnaire. Most questions ask about the impact of bowel problems during the last 2 weeks and higher scores represent a better quality of life. The mean score per patient across all 10 questions ranged from 3 to 6.4, the median was at 4.74.
Two questions were answered with remarkably low scores, indicating substantially impaired quality of life, as depicted in Figure 4. Those were the questions “How often has the feeling of fatigue or of being tired and worn out been a problem for you during the last 2 weeks?” and “How often during the last 2 weeks have you felt relaxed and free of tension. Notably, these questions are not necessarily linked to the presence of abdominal symptoms. However, very bowel-specific questions, such as “How much of the time during the last 2 weeks have you been troubled by a feeling of having to go to the bathroom even though your bowels were empty?” also received low scores from many patients, and 13 patients replied “some of the time.” This was also the case for the question: “How much of the time during the last 2 weeks have you felt angry as a result of your bowel problem?”. Here, half of the patients assigned replies in the range of 1–4 and said this had been the case “all of the time” (n = 1), “Most of the time” (n = 3), “A good bit of the time” (n = 1), and “Some of the time” (n = 8).
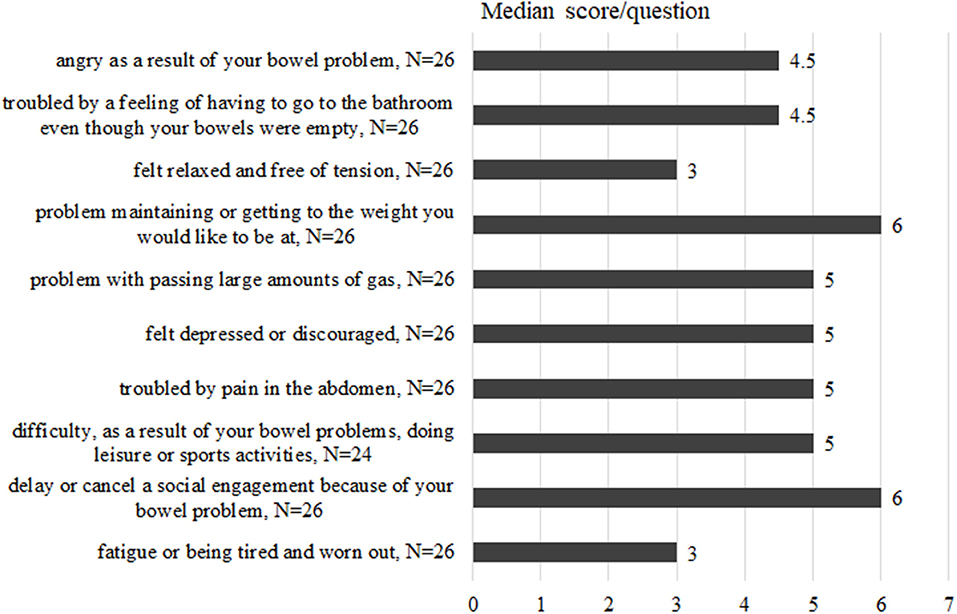
Figure 4. Replies from the sIBDQ completed by 26 CVID patients with current diarrhoea. Questions ask about the impact of bowel problems and quality of life during the last 2 weeks. For each item there is a 7-point Likert scale ranging from 1 for the worst to 7 for the best quality of life in this item. Higher scores represent a better quality of life. Medians for each reply are given in this bar-chart.
Characteristics of Microbiota Subcohort
Stool samples from 15 CVID patients with diarrhoea were collected. Of these, 12 patients also supplied a sample from a healthy household control. Additionally, 15 CVID patients without diarrhoea provided a sample. The microbiome questionnaire (see Supplementary Material) was answered within a mean of 2.49 days (min. 0, max. 52).
The mean age of participants was 57.21 years at time of sampling (min. 20, max. 81, median 60). There were significantly more females in the “CVID with diarrhoea” group, and more male than female participants in the two other groups.
Fifteen of 30 CVID patients included in the study stated they had been taking systemic antibiotics during the last 6 weeks before sampling. Four CVID patients with and two without diarrhoea were taking systemic glucocorticoids at the time of sampling. Patient characteristics are displayed in Table 2.
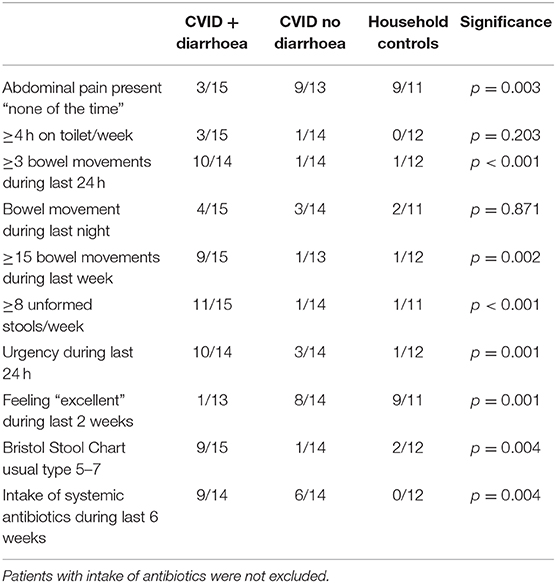
Table 2. Abdominal pain, stool characteristics, and intake of antibiotics during the last 6 weeks.
CVID Patients With Diarrhoea Have an Altered Microbiome
The colonic microbiota of CVID patients with diarrhoea differed significantly from that of CVID patients without diarrhoea in beta diversity [p-value 0.05 PERMANOVA (37) on Bray-Curtis distance].
Looking at the two vertical bar charts (Figure 5) that demonstrate the distribution of taxa at phylum level, alterations in two patients with diarrhoea and norovirus are striking. There is an expansion of Verrucomicrobia in patient No. 10 and an expansion of Proteobacteria in patient No. 15.
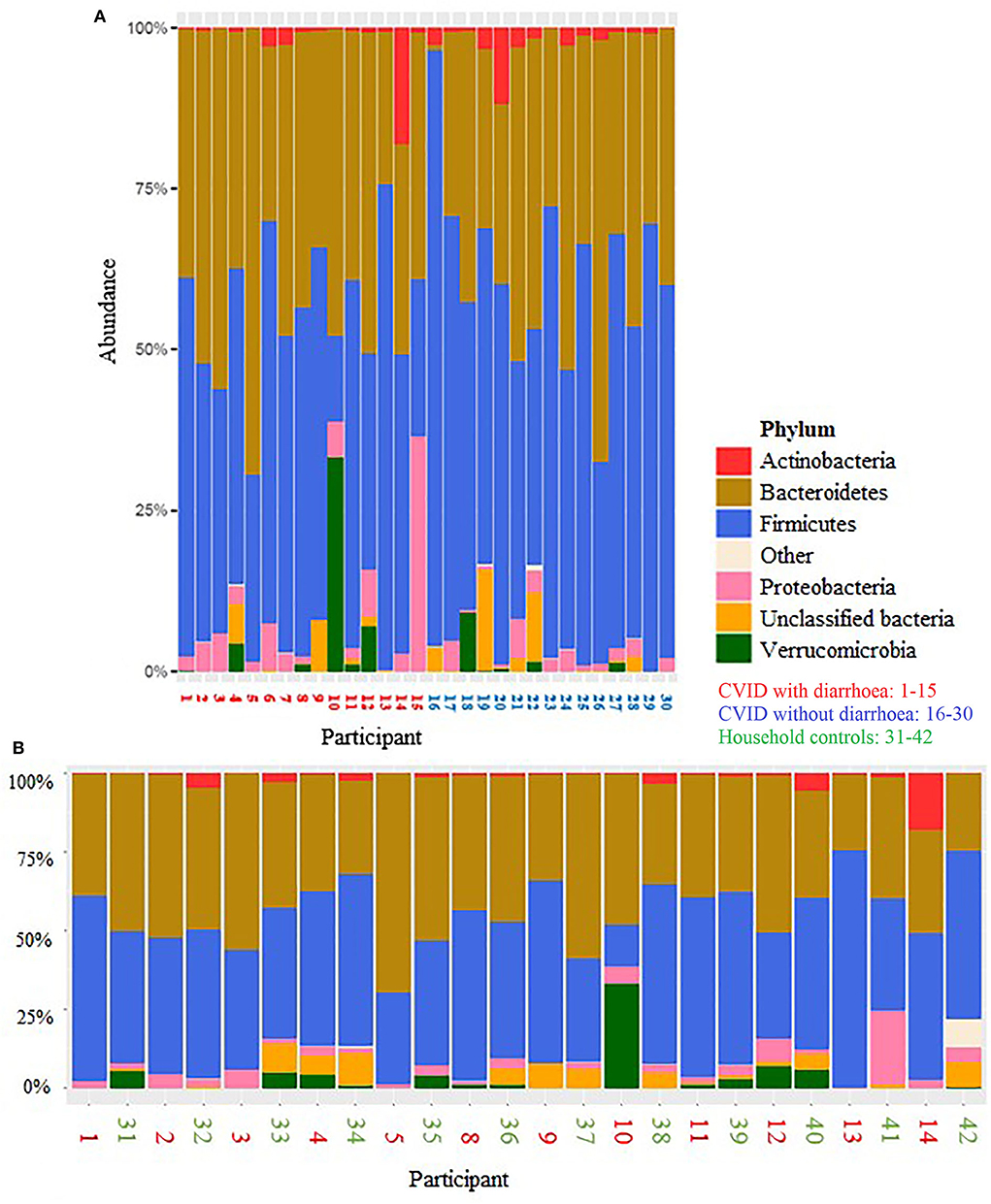
Figure 5. Distribution of taxa at phylum level for (A) CVID patients with diarrhoea (red numbers) and CVID patients without diarrhoea (blue) and (B) CVID patients with diarrhoea (red) and their healthy household controls (neighbouring in green).
One further patient was assumed to have been norovirus positive [No. 2, infection interval estimated by calculating divergence and ancestor dates (40)], one had very rare CMV inclusions in an ileal histopathological sample 2 years earlier (No. 6). One was positive for sapovirus in a current stool-PCR (No. 4) and No. 9 was positive for Giardia lamblia.
The colonic microbiota of CVID patients with diarrhoea did not differ significantly from that of their healthy household controls in beta diversity, p = 0.062, PERMANOVA.
However, alpha diversity (Figure 6) was significantly lower in CVID patients compared to healthy controls (p = 0.009 by Shannon diversity) and specifically in CVID patients with diarrhoea compared to healthy controls (p = 0.003). These differences persist when omitting the six participants with assumed infection (CVID n = 24 vs. healthy controls n = 12, p = 0.001; CVID with diarrhoea (n = 9) vs. healthy controls (n = 12), p = 0.02; CVID without diarrhoea (n = 15) vs. healthy controls (n = 12, p = 0.097).
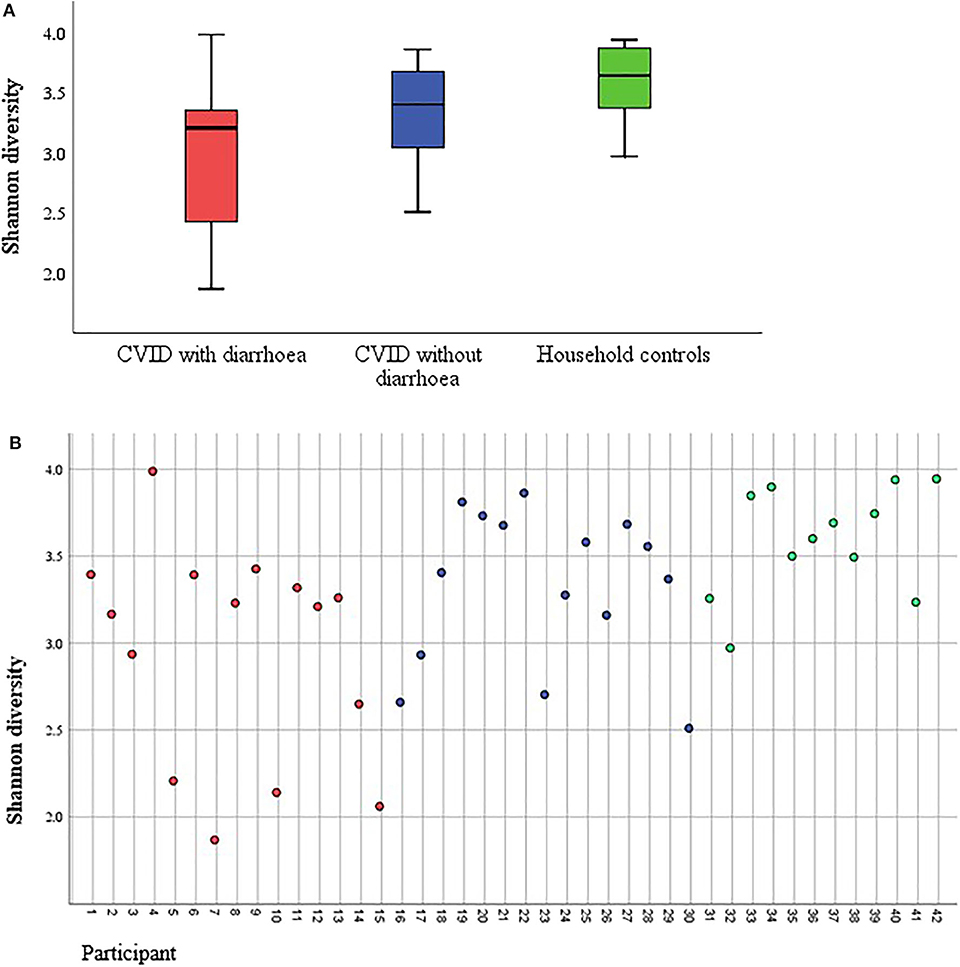
Figure 6. (A) Boxplot of stool microbiota alpha diversity in CVID patients with and without diarrhoea, and household controls without immune deficiency. Alpha diversity depicted with Shannon diversity. (B) Alpha diversity presented as Shannon diversity for every participant. Red, CVID with diarrhoea; blue, CVID without diarrhoea; green, household controls. Three of the patients with diarrhoea were assumed to have been norovirus positive (No. 2, 10, and 15). No. 4 was sapovirus positive and No. 9 was positive for Giardia lamblia. No. 6 had CMV-inclusions in a previous ileal biopsy.
There was no significant difference in alpha diversity between CVID patients with and without diarrhoea (p = 0.065) when looking at all participants. However, omitting participants with infection, there was a significant difference in alpha diversity between CVID patients with diarrhoea (n = 9) and CVID patients without diarrhoea (n = 15), p = 0.04.
There was no difference in Shannon diversity between participants with (n = 15) and without (n = 24) use of antibiotics during the last 6 weeks, p = 0.083, nor when only comparing CVID patients with (n = 15) and without (n = 13) antibiotics during the last 6 weeks, p = 0.420.
Discussion
This study is the largest study to assess longstanding and recurrent diarrhoea in CVID patients by interview. At 33%, the prevalence of longstanding diarrhoea was expectedly high (6–8); in many cases, this was accompanied by abdominal pain, belching, bloating, urgency, or suggestive symptoms of inflammatory bowel disease, although the prevalence of abdominal pain and urgency were not as high as expected.
With its high prevalence, diarrhoea must be seen as a possible warning sign of primary immunodeficiency. This was implemented into the current German guideline for diagnosing PID (41), as suggested by Baumann et al. (42).
A minority of our patients with symptomatic diarrhoea tested positive for infections. Four patients were positive for norovirus at the time of this study. One further patient tested positive after the end of this study, symptomatic with diarrhoea at the time of this study. Woodward et al. (12) suggested norovirus to be causative of the coeliac-like enteropathy observed in CVID. Our study does not look at histology, but all our patients with norovirus infection had villous atrophy on thorough assessment (40). We have recently described our patients with norovirus infection in detail (40).
Sapovirus infection has not been previously described as causative for chronic diarrhoea in CVID patients. Its occurrence has been recorded in renal transplant recipients though (43) and hence it is possible that sapovirus has a pathogenic role in chronic diarrhoea in CVID patients. However, to date we have not seen any infections last more than a period of several weeks. One patient had a positive PCR for Campylobacter, although stool-culture was negative. Chronic infection with Campylobacter is well-recognised in CVID (8, 15). A further patient tested positive for Giardia lamblia, again a commonly described gastrointestinal pathogen (8, 10, 44).
One patient was assumed to have had CMV colitis, as this patient (No. 22) had CMV inclusion bodies in an ileal biopsy, along with ulcers. The patient was not treated with antiviral drugs. There are case reports where a positive effect of virostatic therapy on patients' symptoms has been described (45, 46).
However, most patients did not have clear evidence of infection explaining their symptoms. “CVID enteropathy” has often been classified as an autoimmune phenomenon and grouped with auto-immune phenomena such as autoimmune haemolytic anaemia in studies. So far, no clear autoimmune aetiopathogenesis has been confirmed as causative for CVID enteropathy. Hence, although non-infectious diarrhoea in CVID may have an autoinflammatory origin, it should not be called autoimmune.
Berron-Ruiz et al. found low numbers of memory B-cells to be associated with chronic diarrhoea (47). Our data do not confirm this hypothesis. Diarrhoea correlated with a significantly altered T-lymphocyte population, showing elevated CD4+ lymphocyte numbers, but lower proportions of CD4+naïve lymphocytes. A decrease in naïve CD4+ cells has been shown to be strongly associated with the clinical severity of CVID (48).
Immune dysregulation has been suggested to be associated with enteropathy by Mannon et al., who showed an excess of T-helper (Th)-1 cytokine secretion by lamina propria mononuclear cells in CVID patients with gastrointestinal (GI) symptoms associated with malabsorption, differing from that seen in Crohn's disease (49). Persistent activation of the tumor necrosis factor-system has been demonstrated in subgroups of patients (50). These findings illustrate the role of T-cells and cytokines in CVID-enteropathy and suggest it may be an important aspect.
Regardless of the aetiology of diarrhoea, our sIBDQ results revealed a poor bowel-related quality of life with a median score of 4.74. Voiosu et al. demonstrated that patients with active IBD reached a mean sIBDQ score of 4.8, compared to 5.8 in the group with no endoscopic activity (51). Irvine et al. (18) showed similar results. Quality of life in our CVID patients suffering from diarrhoea is hence as low as in patients with active IBD. The two questions with the lowest scores in our cohort asked for a feeling of fatigue and on having felt relaxed and free of tension during the last 2 weeks. These results signify that recreation and recovery are impeded in this group of patients.
Diarrhoea correlated with low BMI and malabsorption. Previous studies have similarly shown malabsorption in CVID patients with chronic/recurrent diarrhoea (7, 52) and a lower BMI in patients with GI symptoms (49) or villous atrophy (53). This emphasizes the need for suitable therapies for both infection and non-infection associated diarrhoea.
A seminal study performed by Jorgensen et al. examined the diversity of gut microbiota of CVID patients including CVID patients with enteropathy (21). In contrast to this first study, we also included patients with chronic infection and with recent antibiotic usage into our analysis, reflecting “real-world” CVID-associated diarrhoea. Jorgensen et al. (21) found that CVID patients with autoimmune complications (as a group including enteropathy) had a lower alpha diversity than CVID patients without autoimmunity. Also, CVID patients in general had a lower alpha diversity than healthy controls (21). This was also observed by Fiedorova et al. (25). In our study, a significant difference in alpha diversity could be shown between CVID patients and healthy donors as well as between CVID patients with non-infectious diarrhoea and those without diarrhoea. We also observed a significant difference in beta diversity between CVID patients with and without diarrhoea, regardless of infection status. This means that the composition of microbiota was different between these groups. However, this should not be over-interpreted as the household control groups' beta diversity was not significantly different from that of the group of CVID patients with diarrhoea.
It is known that the repeated intake of antibiotics can alter the gut microbiota, beyond clinical recovery (29). Jorgensen et al. (22) demonstrated that Rifaximin provokes a reversible reduction in alpha diversity and an increase of beta diversity in CVID patients without changing the composition of dysbiotic bacteria according to their “dysbiosis index.” CVID patients receive considerable amounts of antibiotics due to severe and recurrent infections throughout their lives. Our data did not show a clear impact of antibiotics but the numbers in each group were relatively small and inter-individual differences in microbiota can render comparisons within small cohorts challenging.
Absence of B-cells was shown to have an impact on the microbiota and on malabsorption in mice (54, 55). It has thus been suggested that an altered gut microbiome might play an important role in the pathogenesis of CVID enteropathy (54, 56). Our results, indicating an altered microbiome in patients with non-infectious diarrhoea, would support this.
Notably, a generally reduced microbial diversity in inactive ulcerative colitis (57) as well as in active IBD (58) has been shown. It would therefore be interesting to know if the microbial diversity remains altered in CVID patients who cease to suffer from diarrhoea. This would suggest that “CVID enteropathy” patients retain an altered microbial diversity as a risk for relapse, but also that changing the microbiotic profile to reduce symptoms might be unnecessary as patients may go into remission despite their altered microbial diversity [similar to the UC patients investigated by Martinez et al. (57)]. At this point it is not clear whether an altered microbiome is the initial driver of enteropathy or whether CVID-related pathological changes in gut function lead directly to the altered microbiome. Longitudinal studies on the microbiome of CVID patients with and without gastrointestinal disease would help to determine this.
We also observed marked changes in the dominant phyla of two patients with norovirus and diarrhoea: one had an expansion of Verrucomicrobia, the other of Proteobacteria. This was similarly observed by Lees et al. (59) in children. Proteobacteria were also more abundant in a study on norovirus infected mice (60) and in some norovirus infected humans (61). There are no previous studies for comparison on the microbiome of CVID patients with infectious diarrhoea.
Our study does have limitations. The screening questionnaire was designed to be a sensitive tool to detect all patients who had current or past diarrhoea even at a relatively modest level. There may have been a response bias, as before patients were contacted, clinic letters and databases were searched for possible GI symptoms and a higher emphasis was made to recruit these patients. Also, patients with abdominal symptoms might have been more motivated to complete the questionnaire.
A second bias influencing the results could be a recall bias. Patients with past diarrhoea might remember their symptoms more or less severely than they actually were. Severity of non-abdominal symptoms might influence how important patients find their GI symptoms.
Patients left out occasional questions in the questionnaires and it was not possible to obtain results for all tests (especially those collected retrospectively), meaning that the datasets were inevitably incomplete.
Stool tests were not always performed on days with diarrhoea. It is unclear whether pathogens can more often be found on days when there are symptoms if diarrhoea is intermittent. In three cases, infection status was not based on current test results but on earlier histology (1 case) and on an estimated infection interval (2 cases).
Overall, our results support the hypothesis that CVID patients commonly suffer bowel disease (16), sometimes associated with infection. CVID patients with diarrhoea of any aetiology have an altered microbiome. The impact of diarrhoea on CVID patients' quality of life is high. It is important to first establish a generally accepted definition of “CVID enteropathy” which we propose should include all CVID patients with longstanding diarrhoea or proven mucosal abnormality on biopsy not attributable to infection. This could be further classified according to the presence or absence of gastrointestinal inflammation, malabsorption, and histological abnormalities. Subsequently, trials of effective treatment to relieve affected patients are needed.
Data Availability Statement
The original data on 16S rRNA sequencing presented in the study are publicly available. This data can be found here: https://doi.org/10.5061/dryad.3j9kd51fz.
Ethics Statement
The studies involving human participants were reviewed and approved by National Research Ethics Service Committee London-Hampstead and National Research Ethics Service North West London. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
This study was conceptualised by BG, DL, and CS. Questionnaires were created by BG, DL, and CS, the questionnaire for analysis of microbiota was based on Kieler Fragebogen für Erwachsene, Studie zur Rolle des Mikrobioms, Erwachsene, Version 1.2, 1st August 2014. Access to clinical data was granted by the Immunology Department, Royal Free Hospital London with support by SB. SW and AS took care of patients' consents and organising appointments. Gaining of clinical data, questioning of patients, gathering samples, and analysis of data was primarily executed by CS. Additionally data was extracted by DG, SA, and FM. Sequencing of stool samples was executed by CN, analysis through AB and MP. Advise for statistical analysis was given by VS. All authors contributed to the article and approved the submitted version.
Funding
This study was supported by the German Research Foundation (DFG), collaborative research center SFB1160/IMPATH. BG receives support through the Deutsche Forschungsgemeinschaft (DFG) under Germany's Excellence Strategy (CIBSS — EXC-2189 — Project ID 390939984, and RESIST — EXC 2155 — Project ID 39087428); through the E-rare programme of the EU, managed by the DFG, grant code GR1617/14-1/iPAD; and through the Netzwerke Seltener Erkrankungen of the German Ministery of Education and Research (BMBF), grant code: GAIN_ 01GM1910A. The research was supported by a Jeffrey Modell Center award. The article processing charge was partly funded by the Albert-Ludwigs-University Freiburg, Germany, in the funding programme Open Access Publishing.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
Prof. Dr. rer. nat. Werner Vach for his help with the statistical analyses. Lea Mollner, Johannes Sperlich, Mirjam Bayer, Drs. Magdalena Dziadzio, Jarka Orosova, Nisha Verma, and Giulia DiColo for their help in data collection. We thank Profs. Andre Franke and Philip Rosenstiel for helping us setting up the 16S rRNA sequencing in Freiburg and sharing with us the “Kieler Fragebogen für Erwachsene”.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2020.01654/full#supplementary-material
Abbreviations
BMI, body mass index; BSC, Bristol Stool Chart; CMV, cytomegalovirus; CVID, common variable immunodeficiency; GI, gastrointestinal; IBD, inflammatory bowel disease; IvIg, intravenous immunoglobulins; No., number; PID, primary immunodeficiency; RFH, Royal Free Hospital London; sIBDQ, short Inflammatory Bowel Disease Questionnaire.
Footnotes
1. ^B– = ≤ 1% B-cells; smB = >1% B-cells; smB+ = >2% switched memory B-cells; smB– = ≤ 2% switched memory B-cells; smB-Trhi = ≥9% transitional B-cells; smB-Trnorm = <9% transitional B-cells.
References
1. Ameratunga R, Brewerton M, Slade C, Jordan A, Gillis D, Steele R, et al. Comparison of diagnostic criteria for common variable immunodeficiency disorder. Front Immunol. (2014) 5:415. doi: 10.3389/fimmu.2014.00415
2. Park MA, Li JT, Hagan JB, Maddox DE, Abraham RS. Common variable immunodeficiency: a new look at an old disease. Lancet. (2008) 372:489–502. doi: 10.1016/S0140-6736(08)61199-X
3. Yazdani R, Hakemi MG, Sherkat R, Homayouni V, Farahani R. Genetic defects and the role of helper T-cells in the pathogenesis of common variable immunodeficiency. Adv Biomed Res. (2013) 3:2. doi: 10.4103/2277-9175.124627
4. Cunningham-Rundles C, Bodian C. Common variable immunodeficiency: clinical and immunological features of 248 patients. Clin Immunol. (1999) 92:34–48. doi: 10.1006/clim.1999.4725
5. Kainulainen L, Nikoskelainen J, Ruuskanen O. Diagnostic findings in 95 Finnish patients with common variable immunodeficiency. J Clin Immunol. (2001) 21:145–9. doi: 10.1023/A:1011012023616
6. Aghamohammadi A, Farhoudi A, Moin M, Rezaei N, Kouhi A, Pourpak Z, et al. Clinical and immunological features of 65 Iranian patients with common variable immunodeficiency. Clin Diagn Lab Immunol. (2005) 12:825–32. doi: 10.1128/CDLI.12.7.825-832.2005
7. Quinti I, Soresina A, Spadaro G, Martino S, Donnanno S, Agostini C, et al. Long-term follow-up and outcome of a large cohort of patients with common variable immunodeficiency. J Clin Immunol. (2007) 27:308–16. doi: 10.1007/s10875-007-9075-1
8. Oksenhendler E, Gérard L, Fieschi C, Malphettes M, Mouillot G, Jaussaud R, et al. Infections in 252 patients with common variable immunodeficiency. Clin Infect Dis. (2008) 46:1547–54. doi: 10.1086/587669
9. Fine KD, Seidel RH, Do K. The prevalence, anatomic distribution, and diagnosis of colonic causes of chronic diarrhea. Gastroint Endosc. (2000) 51:318–26. doi: 10.1016/S0016-5107(00)70362-2
10. Desai L, Kurien RT, Simon EG, Dutta AK, Joseph AJ, Chowdhury SD. Hypogammaglobulinemia-associated gastrointestinal disease–a case series. Indian J Gastroenterol. (2014) 33:560–3. doi: 10.1007/s12664-014-0514-7
11. Green KY. Norovirus infection in immunocompromised hosts. Clin Microbiol Infect. (2014) 20:717–23. doi: 10.1111/1469-0691.12761
12. Woodward JM, Gkrania-Klotsas E, Cordero-Ng AY, Aravinthan A, Bandoh BN, Liu H, et al. The role of chronic norovirus infection in the enteropathy associated with common variable immunodeficiency. Am J Gastroenterol. (2015) 110:320–7. doi: 10.1038/ajg.2014.432
13. Chen CC, Huang JL, Chang CJ, Kong MS. Fecal calprotectin as a correlative marker in clinical severity of infectious diarrhea and usefulness in evaluating bacterial or viral pathogens in children. J Pediatr Gastroenterol Nutr. (2012) 55:541–7. doi: 10.1097/MPG.0b013e318262a718
14. van de Ven AA, Janssen WJ, Schulz LS, van Loon AM, Voorkamp K, Sanders EA, et al. Increased prevalence of gastrointestinal viruses and diminished secretory immunoglobulin a levels in antibody deficiencies. J Clin Immunol. (2014) 34:962–70. doi: 10.1007/s10875-014-0087-3
15. van der Hilst JC, Smits BW, van der Mee JW. Hypogammaglobulinaemia: cumulative experience in 49 patients in a tertiary care institution. Netherlands J Med. (2002) 60:140–7.
16. Teahon K, Webster AD, Price AB, Weston J, Bjarnason I. Studies on the enteropathy associated with primary hypogammaglobulinaemia. Gut. 35:1244–9. doi: 10.1136/gut.35.9.1244
17. Mosli MH, Zou G, Garg SK, Feagan SG, MacDonald JK, Chande N, et al. C-reactive protein, fecal calprotectin, and stool lactoferrin for detection of endoscopic activity in symptomatic inflammatory bowel disease patients: a systematic review and meta-analysis. Am J Gastroenterol. (2015) 110:802. doi: 10.1038/ajg.2015.120
18. Irvine EJ, Zhou Q, Thompson AK. The short inflammatory bowel disease questionnaire: a quality of life instrument for community physicians managing inflammatory bowel disease. CCRPT investigators. Canadian Crohn's relapse prevention trial. Am J Gastroenterol. (1996) 91:1571–8.
19. Jowett SL, Seal CJ, Barton JR, Welfare MR. The short inflammatory bowel disease questionnaire is reliable and responsive to clinically important change in ulcerative colitis. Am J Gastroenterol. (2001) 96:2921–8. doi: 10.1111/j.1572-0241.2001.04682.x
20. Wehr C, Kivioja T, Schmitt C, Ferry B, Witte T, Eren E, et al. The EUROclass trial: defining subgroups in common variable immunodeficiency. Blood. (2008) 111:77–85. doi: 10.1182/blood-2007-06-091744
21. Jorgensen SF, Troseid M, Kummen M, Anmarkrud JA, Michelsen AE, Osnes LT, et al. Altered gut microbiota profile in common variable immunodeficiency associates with levels of lipopolysaccharide and markers of systemic immune activation. Mucosal Immunol. (2016) 9:1455–65. doi: 10.1038/mi.2016.18
22. Jørgensen SF, Macpherson ME, Bjørnetrø T, Holm K, Kummen M, Rashidi A, et al. Rifaximin alters gut microbiota profile, but does not affect systemic inflammation - a randomized controlled trial in common variable immunodeficiency. Sci Rep. (2019) 9:167. doi: 10.1038/s41598-018-35367-7
23. Fadlallah J, Sterlin D, Fieschi C, Parizot C, Dorgham K, El Kafsi H, et al. Synergistic convergence of microbiota-specific systemic IgG and secretory IgA. J. Allergy Clin. Immunol. (2019) 143:1575–85.e4. doi: 10.1016/j.jaci.2018.09.036
24. Sterlin D, Fieschi C, Malphettes M, Larsen M, Gorochov G, Fadlallah J. Immune/microbial interface perturbation in human IgA deficiency. Gut Microbes. (2018) 10:428–33. doi: 10.1080/19490976.2018.1546520
25. Fiedorová K, Radvanský M, Bosák J, Grombiríková H, Němcová E, Králíčková P, et al. Bacterial but not fungal gut microbiota alterations are associated with common variable immunodeficiency (CVID) phenotype. Front Immunol. (2019) 10:1914. doi: 10.3389/fimmu.2019.01914
26. Fadlallah J, El Kafsi H, Sterlin D, Juste C, Parizot C, Dorgham K, et al. Microbial ecology perturbation in human IgA deficiency. Sci Transl Med. 10:eaan1217. doi: 10.1126/scitranslmed.aan1217
27. Wu GD, Chen J, Hoffmann C, Bittinger K, Chen Y-Y, Keilbaugh SA, et al. Linking long-term dietary patterns with gut microbial enterotypes. Science. (2011) 334:105–8. doi: 10.1126/science.1208344
28. David LA, Maurice CF, Carmody RN, Gootenberg DB, Button JE, Wolfe BE, et al. Diet rapidly and reproducibly alters the human gut microbiome. Nature. (2014) 505:559–63. doi: 10.1038/nature12820
29. Dethlefsen L, Relman DA. Incomplete recovery and individualized responses of the human distal gut microbiota to repeated antibiotic perturbation. Proc Natl Acad Sci USA. (2011) 108(Suppl. 1):4554–61. doi: 10.1073/pnas.1000087107
30. Goodrich JK, Waters JL, Poole AC, Sutter JL, Koren O, Blekhman R, et al. Human genetics shape the gut microbiome. Cell. (2014) 159:789–99. doi: 10.1016/j.cell.2014.09.053
31. Eckburg PB, Bik EM, Bernstein CN, Purdom E, Dethlefsen L, Sargent M, et al. Diversity of the human intestinal microbial flora. Science. (2005) 308:1635–8. doi: 10.1126/science.1110591
32. Franke A, et al. Kieler Fragebogen für Erwachsene: Studie zur Rolle des Mikrobioms, Version 1.2. Erwachsene (2014).
33. Cole JR, Wang Q, Fish JA, Chai B, McGarrell DM, Sun Y, et al. Ribosomal database project: data and tools for high throughput rRNA analysis. Nucleic Acids Res. (2014) 42:D633–42. doi: 10.1093/nar/gkt1244
34. Reese AT, Dunn RR, McFall-Ngai MJ. Drivers of microbiome biodiversity: a review of general rules, feces, and ignorance. mBio. (2018) 9:e01294-18. doi: 10.1128/mBio.01294-18
35. Kim B-R, Shin J, Guevarra R, Lee JH, Kim DW, Seol K-H, et al. Deciphering diversity indices for a better understanding of microbial communities. J Microbiol Biotechnol. (2017) 27:2089–93. doi: 10.4014/jmb.1709.09027
36. Wang Q, Garrity GM, Tiedje JM, Cole JR. Naive Bayesian classifier for rapid assignment of rRNA sequences into the new bacterial taxonomy. Appl Environ Microbiol. (2007) 73:5261–7. doi: 10.1128/AEM.00062-07
37. Anderson MJ. Permutational Multivariate Analysis of Variance (PERMANOVA). In: Wiley StatsRef: Statistics Reference Online. (2017). doi: 10.1002/9781118445112.stat07841
38. Sands BE. From symptom to diagnosis: clinical distinctions among various forms of intestinal inflammation. Gastroenterology. (2004) 126:1518–32. doi: 10.1053/j.gastro.2004.02.072
39. Danese S, Fiorino G, Mary J-Y, Lakatos PL, D'Haens G, Moja L, et al. Development of red flags index for early referral of adults with symptoms and signs suggestive of Crohn's disease: an IOIBD initiative. J Crohn's Colitis. (2015) 9:601–6. doi: 10.1093/ecco-jcc/jjv067
40. Brown L-AK, Ruis C, Clark I, Roy S, Brown JR, Albuquerque AS, et al. A comprehensive characterization of chronic norovirus infection in immunodeficient hosts. J Allergy Clin Immunol. (2019) 144:1450–3. doi: 10.1016/j.jaci.2019.07.036
41. Farmand S, Baumann U, von Bernuth H, Borte M, Borte S, Boztug K, et al. Diagnostik auf Vorliegen eines Primä und Weiteren Symptomen von Primären Immundefekten. AWMF (S2k) Leitlinie (2017). Available from: https://www.awmf.org/leitlinien/detail/ll/112-001.html
42. Baumann U, Belohradsky B, Bernuth Hv, Friedrich W, Linde R, Niehues T, et al. Primäre Immundefekte – Warnzeichen und Algorithmen zur Diagnosefindung. Bremen: UNI-MED. (2010) p. 128.
43. Roos-Weil D, Ambert-Balay K, Lanternier F, Mamzer-Bruneel M-F, Nochy D, Pothier P, et al. Impact of norovirus/sapovirus-related diarrhea in renal transplant recipients hospitalized for diarrhea. Transplantation. (2011) 92:61–9. doi: 10.1097/TP.0b013e31821c9392
44. Cunningham-Rundles C. Clinical and immunologic analyses of 103 patients with common variable immunodeficiency. J Clin Immunol. (1989) 9:22–33. doi: 10.1007/BF00917124
45. Lepinski SM, Hamilton JW. Isolated cytomegalovirus ileitis detected by colonoscopy. Gastroenterology. (1990) 98:1704–6. doi: 10.1016/0016-5085(90)91112-J
46. Alkhatib AA, Ahdab MM, Elkhatib FA. Bloody diarrhoea secondary to cytomegalovirus ileitis. Digest Liver Dis. (2011) 43:169. doi: 10.1016/j.dld.2010.01.007
47. Berron-Ruiz L, Lopez-Herrera G, Vargas-Hernandez A, Mogica-Martinez D, Garcia-Latorre E, Blancas-Galicia L, et al. Lymphocytes and B-cell abnormalities in patients with common variable immunodeficiency (CVID). Allergol Immunopathol. (2014) 42:35–43. doi: 10.1016/j.aller.2012.07.016
48. Giovannetti A, Pierdominici M, Mazzetta F, Marziali M, Renzi C, Mileo AM, et al. Unravelling the complexity of T cell abnormalities in common variable immunodeficiency. J Immunol. (2007) 178:3932–43. doi: 10.4049/jimmunol.178.6.3932
49. Mannon PJ, Fuss IJ, Dill S, Friend J, Groden C, Hornung R, et al. Excess IL-12 but not IL-23 accompanies the inflammatory bowel disease associated with common variable immunodeficiency. Gastroenterology. (2006) 131:748–56. doi: 10.1053/j.gastro.2006.06.022
50. Aukrust P, Lien E, Kristoffersen AK, Müller F, Haug CJ, Espevik T, et al. Persistent activation of the tumor necrosis factor system in a subgroup of patients with common variable immunodeficiency–possible immunologic and clinical consequences. Am Soc Hematol. (1996) 87:674–81. doi: 10.1182/blood.V87.2.674.bloodjournal872674
51. Voiosu T, Benguş A, Dinu R, Voiosu AM, Bălănescu P, Băicuş C, et al. Rapid fecal calprotectin level assessment and the SIBDQ score can accurately detect active mucosal inflammation in IBD patients in clinical remission: a prospective study. J Gastrointestin Liver Dis. (2014) 23:273–8. doi: 10.15403/jgld.2014.1121.233.thv
52. Venhoff N, Emmerich F, Neagu M, Salzer U, Koehn C, Driever S, et al. The role of HLA DQ2 and DQ8 in dissecting celiac-like disease in common variable immunodeficiency. J Clin Immunol. (2013) 33:909–16. doi: 10.1007/s10875-013-9892-3
53. Malamut G, Verkarre V, Suarez F, Viallard J-F, Lascaux A-S, Cosnes J, et al. The enteropathy associated with common variable immunodeficiency: the delineated frontiers with celiac disease. Am J Gastroenterol. (2010) 105:2262–75. doi: 10.1038/ajg.2010.214
54. Shulzhenko N, Morgun A, Hsiao W, Battle M, Yao M, Gavrilova O, et al. Crosstalk between B lymphocytes, microbiota and the intestinal epithelium governs immunity versus metabolism in the gut. Nat Med. (2011) 17:1585–93. doi: 10.1038/nm.2505
55. Mohammed AD, Khan MA, Chatzistamou I, Chamseddine D, Williams-Kang K, Perry M, et al. Gut antibody deficiency in a mouse model of CVID results in spontaneous development of a gluten-sensitive enteropathy. Front Immunol. (2019) 10:2484. doi: 10.3389/fimmu.2019.02484
56. Greer RL, Morgun A, Shulzhenko N. Bridging immunity and lipid metabolism by gut microbiota. J Allergy Clin Immunol. (2013) 132:253–62. doi: 10.1016/j.jaci.2013.06.025
57. Martinez C, Antolin M, Santos J, Torrejon A, Casellas F, Borruel N, et al. Unstable composition of the fecal microbiota in ulcerative colitis during clinical remission. Am J Gastroenterol. (2008) 103:643–8. doi: 10.1111/j.1572-0241.2007.01592.x
58. Ott SJ. Reduction in diversity of the colonic mucosa associated bacterial microflora in patients with active inflammatory bowel disease. Gut. (2004) 53:685–93. doi: 10.1136/gut.2003.025403
59. Lees EA, Carrol ED, Ellaby NA, Roberts P, Corless CE, Lenzi L, et al. Characterization of circulating Clostridium difficile strains, host response and intestinal microbiome in hospitalized children with diarrhea. Pediatr Infect Dis J. (2019) 39:221–8. doi: 10.1097/INF.0000000000002559
60. Lee H, Ko G. Antiviral effect of vitamin A on norovirus infection via modulation of the gut microbiome. Sci Rep. (2016) 6:25835. doi: 10.1038/srep25835
Keywords: CVID, diarrhoea, calprotectin, norovirus, microbiome, IBDQ, lymphocytes, quality of life
Citation: van Schewick CM, Nöltner C, Abel S, Burns SO, Workman S, Symes A, Guzman D, Proietti M, Bulashevska A, Moreira F, Soetedjo V, Lowe DM and Grimbacher B (2020) Altered Microbiota, Impaired Quality of Life, Malabsorption, Infection, and Inflammation in CVID Patients With Diarrhoea. Front. Immunol. 11:1654. doi: 10.3389/fimmu.2020.01654
Received: 25 April 2020; Accepted: 22 June 2020;
Published: 31 July 2020.
Edited by:
Antonio Condino-Neto, University of São Paulo, BrazilReviewed by:
Neil Romberg, Children's Hospital of Philadelphia, United StatesMark Ballow, University of South Florida, United States
Copyright © 2020 van Schewick, Nöltner, Abel, Burns, Workman, Symes, Guzman, Proietti, Bulashevska, Moreira, Soetedjo, Lowe and Grimbacher. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: David M. Lowe, ZC5sb3dlQHVjbC5hYy51aw==; Bodo Grimbacher, Ym9kby5ncmltYmFjaGVyQHVuaWtsaW5pay1mcmVpYnVyZy5kZQ==