 Zoltán Kiss1†
Zoltán Kiss1† István Wittmann1†
István Wittmann1† Lőrinc Polivka2György Surján3Orsolya Surján4Zsófia Barcza5
Lőrinc Polivka2György Surján3Orsolya Surján4Zsófia Barcza5 Gergő Attila Molnár1Dávid Nagy6,7
Gergő Attila Molnár1Dávid Nagy6,7 Veronika Müller2Krisztina Bogos8
Veronika Müller2Krisztina Bogos8 Péter Nagy9,10,11
Péter Nagy9,10,11 István Kenessey9,12András Wéber9,13Mihály Pálosi14
István Kenessey9,12András Wéber9,13Mihály Pálosi14 János Szlávik15
János Szlávik15 Zsuzsa Schaff12
Zsuzsa Schaff12 Zoltán Szekanecz16Cecília Müller17Miklós Kásler18‡
Zoltán Szekanecz16Cecília Müller17Miklós Kásler18‡ Zoltán Vokó6,7*‡
Zoltán Vokó6,7*‡- 1Second Department of Medicine and Nephrology-Diabetes Center, University of Pécs Medical School, Pécs, Hungary
- 2Department of Pulmonology, Semmelweis University, Budapest, Hungary
- 3Institute of Digital Health Sciences, Semmelweis University, Budapest, Hungary
- 4Department of Deputy Chief Medical Officer II., National Public Health Center, Budapest, Hungary
- 5Syntesia Medical Communications Ltd., Budapest, Hungary
- 6Center for Health Technology Assessment, Semmelweis University, Budapest, Hungary
- 7Syreon Research Institute, Budapest, Hungary
- 8Department of Pulmonology, National Korányi Institute of Pulmonology, Budapest, Hungary
- 9Department of Molecular Immunology and Toxicology and the National Tumor Biology Laboratory, National Institute of Oncology, Budapest, Hungary
- 10Department of Anatomy and Histology, Laboratory of Redox Biology, University of Veterinary Medicine, Budapest, Hungary
- 11Institute of Oncochemistry, University of Debrecen, Debrecen, Hungary
- 12Department of Pathology, Forensic and Insurance Medicine, Semmelweis University, Budapest, Hungary
- 13Cancer Surveillance Branch, International Agency for Research on Cancer, Lyon, France
- 14National Health Insurance Fund, Budapest, Hungary
- 15South-Pest Hospital Centre – National Institute for Infectology and Haematology, Budapest, Hungary
- 16Department of Rheumatology, Faculty of Medicine, University of Debrecen, Debrecen, Hungary
- 17Department of Chief Medical Officer, National Public Health Center, Budapest, Hungary
- 18Ministry of Human Resources, Budapest, Hungary
Background: In Hungary, the pandemic waves in late 2021 and early 2022 were dominated by the Delta and Omicron SARS-CoV-2 variants, respectively. Booster vaccines were offered with one or two doses for the vulnerable population during these periods.
Methods and Findings: The nationwide HUN-VE 2 study examined the effectiveness of primary immunization, single booster, and double booster vaccination in the prevention of Covid-19 related mortality during the Delta and Omicron waves, compared to an unvaccinated control population without prior SARS-CoV-2 infection during the same study periods. The risk of Covid-19 related death was 55% lower during the Omicron vs. Delta wave in the whole study population (n=9,569,648 and n=9,581,927, respectively; rate ratio [RR]: 0.45, 95% confidence interval [CI]: 0.44–0.48). During the Delta wave, the risk of Covid-19 related death was 74% lower in the primary immunized population (RR: 0.26; 95% CI: 0.25–0.28) and 96% lower in the booster immunized population (RR: 0.04; 95% CI: 0.04–0.05), vs. the unvaccinated control group. During the Omicron wave, the risk of Covid-19 related death was 40% lower in the primary immunized population (RR: 0.60; 95% CI: 0.55–0.65) and 82% lower in the booster immunized population (RR: 0.18; 95% CI: 0.16–0.2) vs. the unvaccinated control group. The double booster immunized population had a 93% lower risk of Covid-19 related death compared to those with only one booster dose (RR: 0.07; 95% CI. 0.01–0.46). The benefit of the second booster was slightly more pronounced in older age groups.
Conclusions: The HUN-VE 2 study demonstrated the significantly lower risk of Covid-19 related mortality associated with the Omicron vs. Delta variant and confirmed the benefit of single and double booster vaccination against Covid-19 related death. Furthermore, the results showed the additional benefit of a second booster dose in terms of SARS-CoV-2 infection and Covid-19 related mortality.
Introduction
The first coronavirus disease 2019 (Covid-19) cases were confirmed more than 2 years ago, and several new variants of the SARS-CoV-19 virus have been identified since then (1). Vaccines against SARS-CoV-19 infection with various mechanisms of action became available at the end of 2020 (2–4). In Hungary, 6 different vaccine types were approved by local regulatory authorities during the first half of 2021, when the B.1.1.7 (Alpha) variant dominated the pandemic wave. The HUN-VE study was published in the second half of 2021 and reported high or very high effectiveness for 5 different vaccine types against SARS-CoV-19 infection and Covid-19 related mortality caused by the alpha variant (3). In the meantime, several studies reported declining vaccine effectiveness 6–9 months after the first two doses (5–8). Moreover, the emergence of the new, more contagious Delta variant (B.1.617.2) led to new pandemic waves during the second half of 2021. Therefore, according to the recommendations by Israeli scientists, booster doses of different Covid-19 vaccines became available in several countries (9, 10). Since August 1, 2021, the Hungarian government recommends heterologous or homologous booster vaccination at least 4 months after the primary vaccination course, particularly for vulnerable patient populations including those aged 60 or older and people with chronic diseases (11). The effectiveness of booster vaccines against SARS-CoV-19 infection after waning vaccine immunity was rapidly demonstrated by a number of studies, however, few analyses reported benefits regarding severe outcomes and death (9, 10). By the end of 2021, the new Omicron variant reached Europe, which led to the highest-ever daily infection rates in early 2022 with lower mortality rates (12, 13). In the meantime, certain countries such as Hungary started recommending a second booster shot for the vulnerable population including people aged 60 years or older and those having chronic diseases, however, the fourth dose was available for the whole population (14–16).
The aim of the HUN-VE 2 study was to examine the effectiveness of primary immunization as well as first and second booster doses during the Delta and Omicron waves of the SARS-CoV-2 pandemic in Hungary.
Methods
This nationwide, retrospective, observational study examined the overall effectiveness of primary immunization (first two vaccine doses, or one dose of the Janssen vaccine), first, and second booster vaccines against Covid-19 related death during ascending phases of the Delta and Omicron waves using data from the Hungarian Coronavirus Registry owned by the National Public Health Center (NPHC). We examined two 54-day long observation periods for the outcome of Covid-19 related death: 8 November 2021 to 31 December 2021 (dominant variant: Delta); 1 January 2022 to 23 February 2022 (dominant variant: Omicron) (Figure 1) (14).
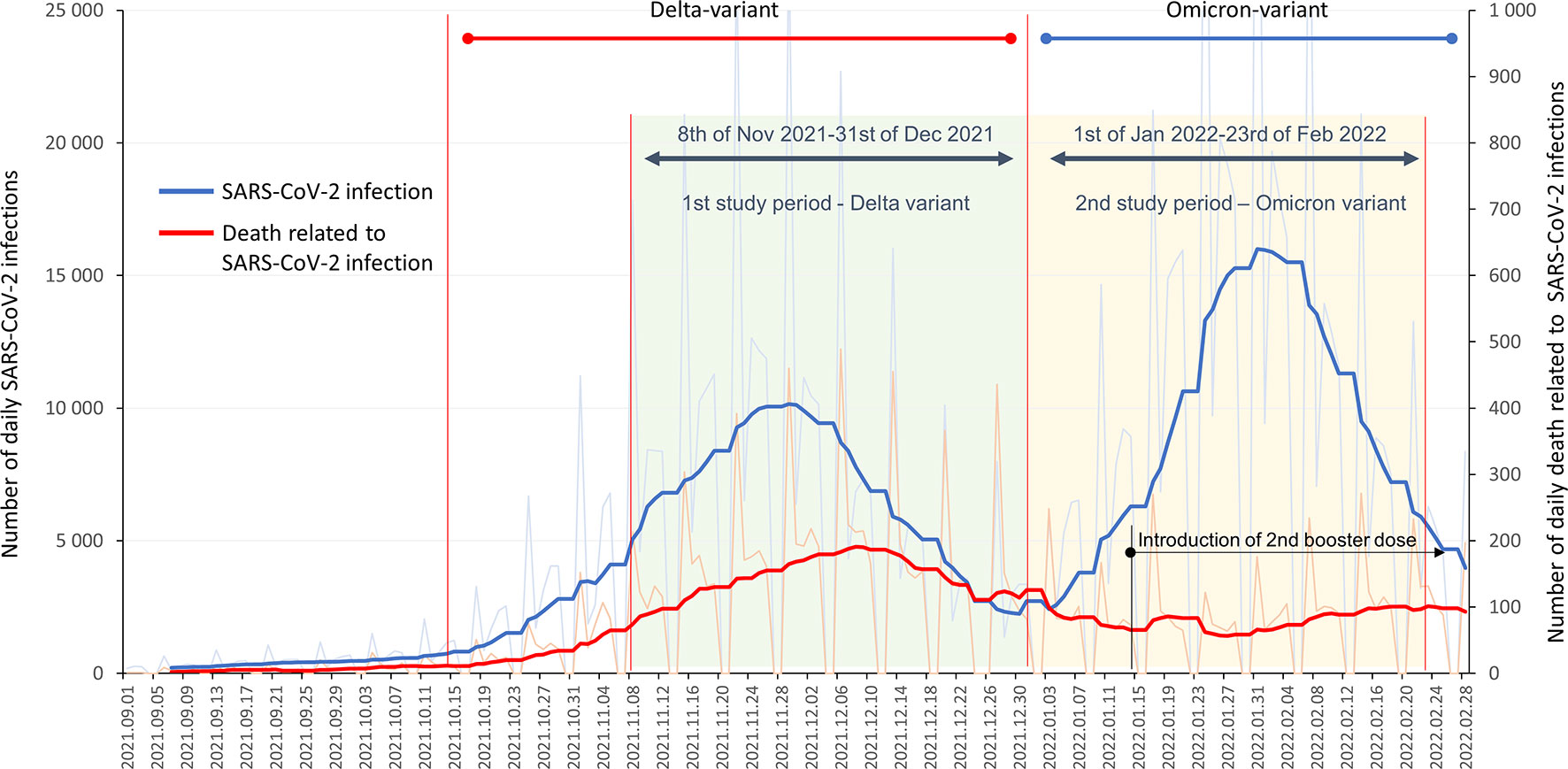
Figure 1 Study periods and timeline of the HUN-VE 2 study together with the reported daily SARS-CoV-2 infections and Covid-19 related mortality in Hungary between 1 September 2021, and 28 February 2022 (source of data: koronavirus.gov.hu).
Our study covers almost 100% of the Hungarian population, aged 16 years or older. The study included Hungarian residents who had active health insurance on 3 March 2021 and were alive on the first day of the respective study period. Cases of SARS-CoV-2 infection were reported by hospital physicians and general practitioners, collected by the NPHC on a daily basis using the centralized system of the National Social Information System (NSIS), and recorded in the Hungarian Coronavirus Register. Covid-19 related mortality was defined as death during SARS-CoV-2 positivity, regardless of whether death was the direct consequence of SARS-CoV-2 infection or other underlying causes (except for clear alternative causes such as trauma). The definition was the same used in the HUN-VE study (3).
Six different vaccine types and their combinations were available in Hungary prior to and during the study period: Pfizer-BioNTech, Moderna, AstraZeneca, Sputnik-V, Sinopharm, Janssen. The separate evaluation of vaccine effectiveness and different vaccine combinations will be reported by a subsequent HUN-VE study (17).
On any day, individuals without any record of SARS-Cov-2 infection at the beginning of each study period were classified as having completed primary immunization if at least 14 days had passed since the administration of the second dose of any vaccine type (or one dose of the Janssen vaccine), booster immunized starting from 14 days after the third dose (or second after the Janssen vaccine), and double booster immunized if at least 14 days had passed since the second booster dose (four times vaccinated or triple vaccinated in the case of the Janssen vaccine). The unvaccinated, control population included individuals who had not received any dose of any Covid-19 vaccine type and had no record of SARS-CoV-2 infection in the Hungarian Coronavirus Register, had active health insurance on 3 March 2021, and were alive on the first day of the respective study period.
The distribution of different types of vaccines as primary immunization, first booster immunization and double booster immunization are shown in Supplementary Tables 1, 2. Supplementary Table 1 also shows data for 8 November 2021, 31 December 2021, and 23 February 2022.
Vaccine effectiveness was examined for the predefined groups based on vaccination status versus the control, unvaccinated population during the Omicron and Delta waves. Additionally, registered rates of SARS-CoV-2 infection and Covid-19 related mortality were compared between the booster and double booster vaccinated populations.
Person-days for vaccination groups by wave were determined by summing the number of persons in a certain group for each day of the two periods from time zero (T0, 8 November 2021 and 1 January 2022, respectively). Average population sizes for all evaluated groups were calculated by dividing the total person-days of a given subgroup by the length of the study period (54 days). Data were stratified by age (16–24, 25–34, 35–44, 45–54, 55–64, 65–74, 75–84, 85≤ years).
Mortality rates were calculated by dividing the number of Covid-19 related deaths by the person-days of observation. Mortality rate ratios were estimated together with their exact 95% confidence intervals (95% CI) by age stratum. Mantel-Haenszel mortality rate ratios were estimated for the total populations to adjust for age.
The study was approved by the Central Ethical Committee of Hungary (OGYÉI/10296-1/2022 and IV/1722-1/2022/EKU) and followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines (18).
Results
Altogether 8,244,440 persons constituted the total study population during the Delta wave. 314,700 persons had SARS-CoV-2 infection (3.82%), of whom 6,571 persons died (0.080% of the investigated population) during the study period (Suppl Fig 1). The average size of the unvaccinated population (without prior SARS-CoV-2 infection) comprised 2,226,526 persons during the Delta wave (27.0% of total), of whom 3,834 (0.172%) died due to Covid-19 (Figure 2). In the total Delta population, the average size of the population with primary immunization was 3,476,436 (42.2%), of whom 2,071 (0.057%) died while having SARS-CoV-2 infection during this study period. 21.1% of this total population received booster immunization, of whom 0.022% (443 persons) died (Figure 2). Mortality rates increased by age, up to 30.38, 13.14, and 2.64 per 100.000 person-days in the oldest age cohort in the non-vaccinated, primary immunized, and booster vaccinated population, respectively.
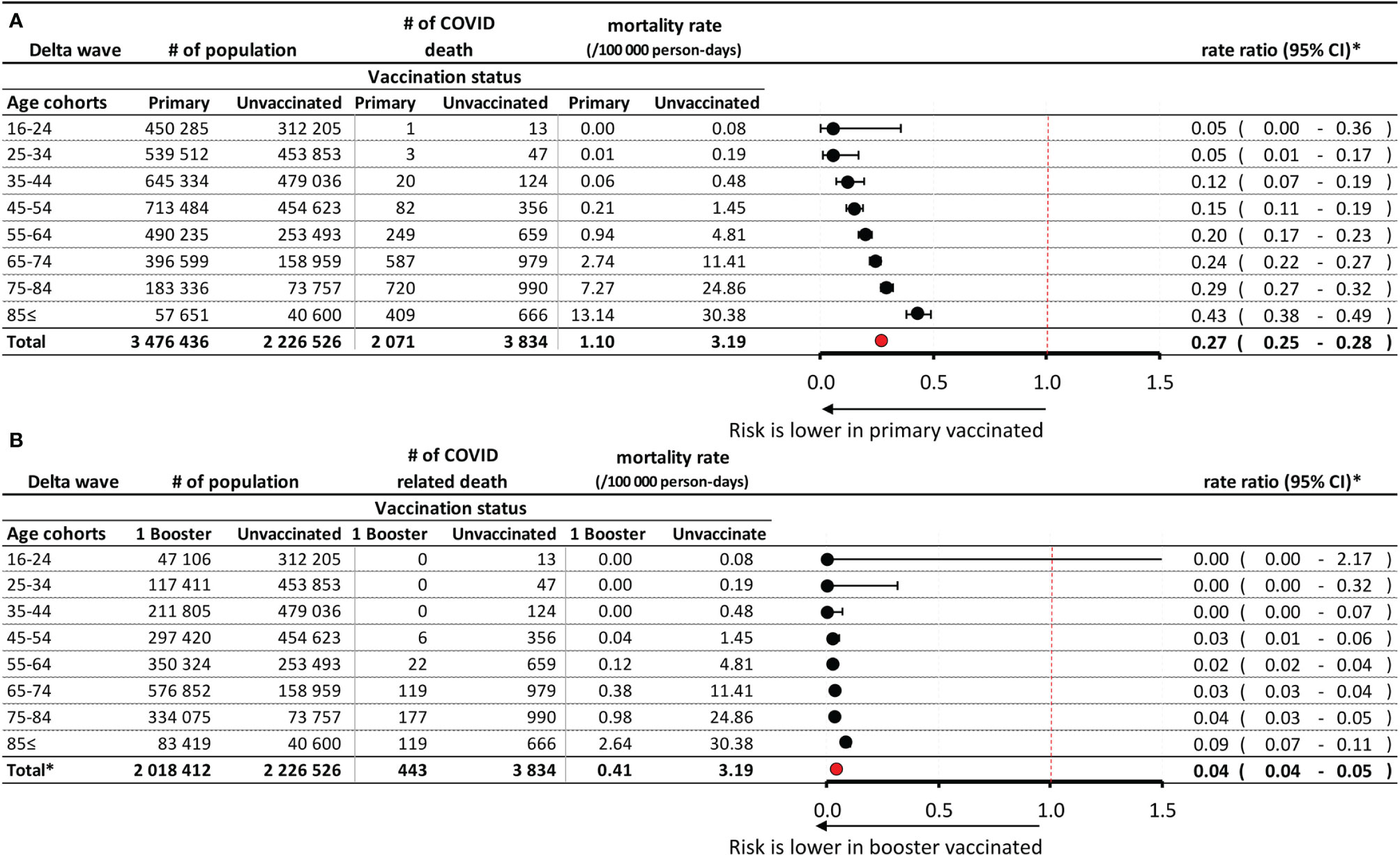
Figure 2 Risk of Covid-19 related mortality during the Delta wave in the primary immunized vs. unvaccinated control population (A), and in the booster vaccinated vs. unvaccinated control population (B), according to age. *Exact confidence intervals for age-specific mortality rate ratios and Mantel-Haenszel pooled mortality rate ratio for the total population adjusted for age.
The total study population for the period of the Omicron wave comprised 8,232,169 persons, of whom 2,792 (0.036%) died due to Covid-19. The average size of the primary immunized and booster vaccinated populations was 2,328,562 persons (28.3%) and 3,297,024 (40.05%), respectively (Supplementary Figure 1). Of the latter, 66.43% were aged 65 years or older. 31,527 persons (0.38%) had received double booster immunization (mostly a fourth dose, except for the Janssen vaccine). In the booster vaccinated population, 845 persons (0.026%) died while having SARS-CoV-2 infection, while in the double booster immunized group, only 1 person died while having SARS-CoV2 infection during the Omicron wave (0.003%). Mortality rates were generally lower during the Omicron wave in most study groups compared to the Delta wave: 1.08 vs. 3.19 per 100.000 person-days in non-vaccinated cohorts, 0.48 vs. 1.10 per 100.000 person-days in the primary immunized populations, and 0.48 vs. 0.41 in the booster vaccinated populations, respectively. During the Omicron wave, the rate of Covid-19 related mortality was only 0.06 per 100.000 person-days in the double booster immunized group.
During the Delta wave, the relative rate (RR) of Covid-19 related mortality was 0.27 in the primary immunized population (95% CI: 0.25–0.28) compared to the unvaccinated control group. The rate ratio increased with age (0.05 in the 16–34 years, and 0.24–0.43 in the 65≤ years age groups). The risk of Covid-19 related mortality was 96% lower in the booster vaccinated population than in the unvaccinated control group (RR: 0.04; 95% CI: 0.04–0.05). The rate ratio was below 0.05% in most age groups, and there was a 100% risk reduction among people aged 0–45 years.
During the Omicron wave in 2022, people with primary immunization had a 40% lower risk of Covid-19 related death than those who received no immunization (RR: 0.60; 95% CI: 0.55–0.65) (Figure 3A). The difference decreased with age. The booster vaccinated population had an 82% lower risk of Covid-19 related mortality compared to unvaccinated controls (RR: 0.18; 95% CI: 0.16–0.20), with a slight decrease in effect with increasing age (Figure 3B). Double booster immunized people had an almost 100% Covid-19 related mortality reduction during the Omicron wave compared to the unvaccinated control population (RR: 0.01; 95% CI: 0.00–0.08) (Figure 3C).
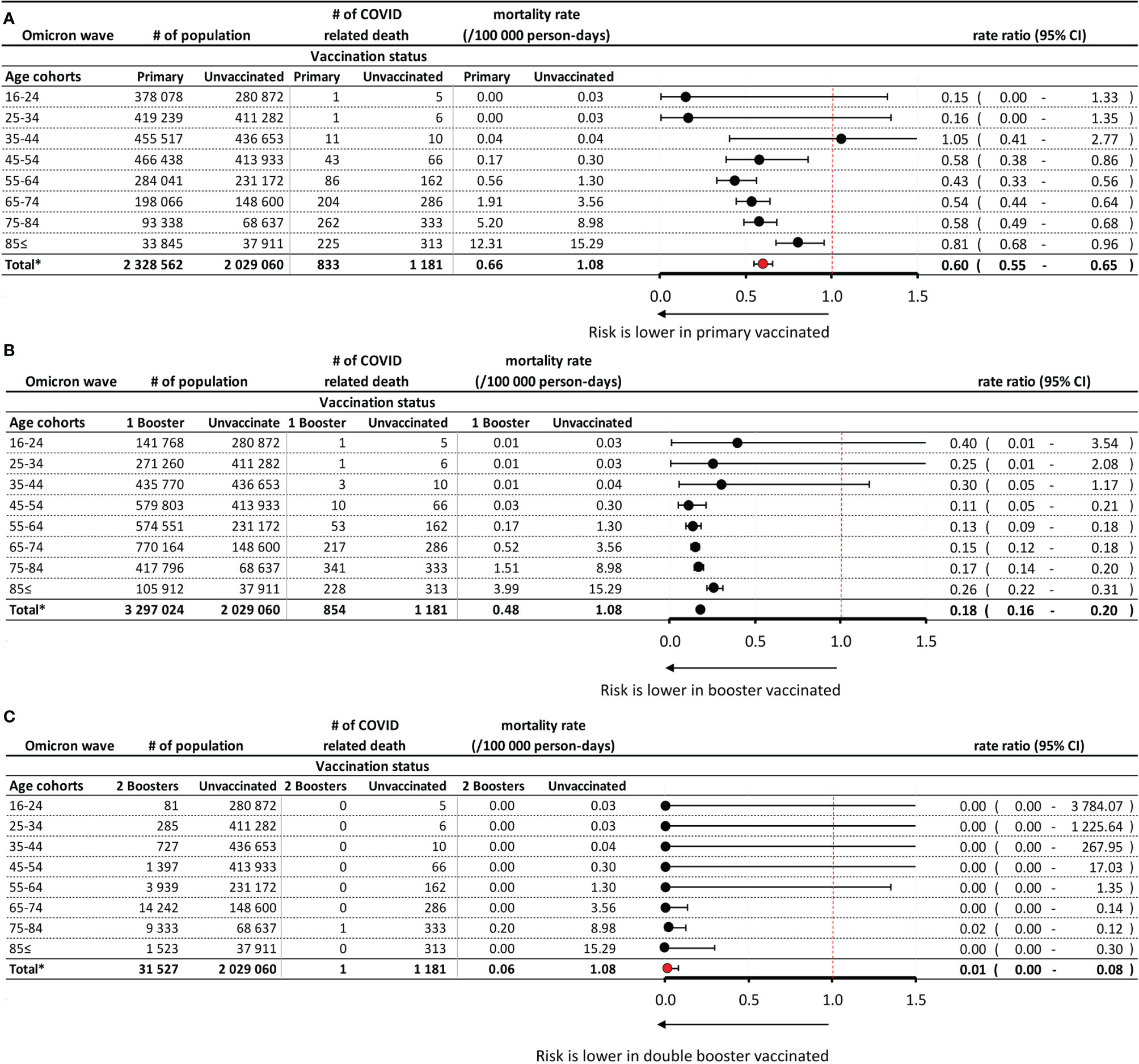
Figure 3 Risk of Covid-19 related mortality during the Omicron wave in the primary immunized vs. unvaccinated control population (A), in the booster vaccinated vs. unvaccinated control population (B), and in the double booster vaccinated vs. unvaccinated control population (C), according to age. *Exact confidence intervals for age-specific mortality rate ratios and Mantel-Haenszel pooled mortality rate ratio for the total population adjusted for age.
There was a 51% lower risk of registered SARS-CoV-2 infection and an almost 93% lower risk of Covid-19 related mortality among people with two booster doses compared to those with only one (RR: 0.49; 95% CI: 0.44–0.53 and RR: 0.07; 95% CI. 0.01–0.46, respectively) (Figures 4A, B). In the age group of 65≤ years, where the majority of booster doses were administered, the mortality reduction was statistically significant (i.e., the 95% CI of the mortality rate ratio does not include the value of 1 in the age groups 65–74 and 75–84 years).
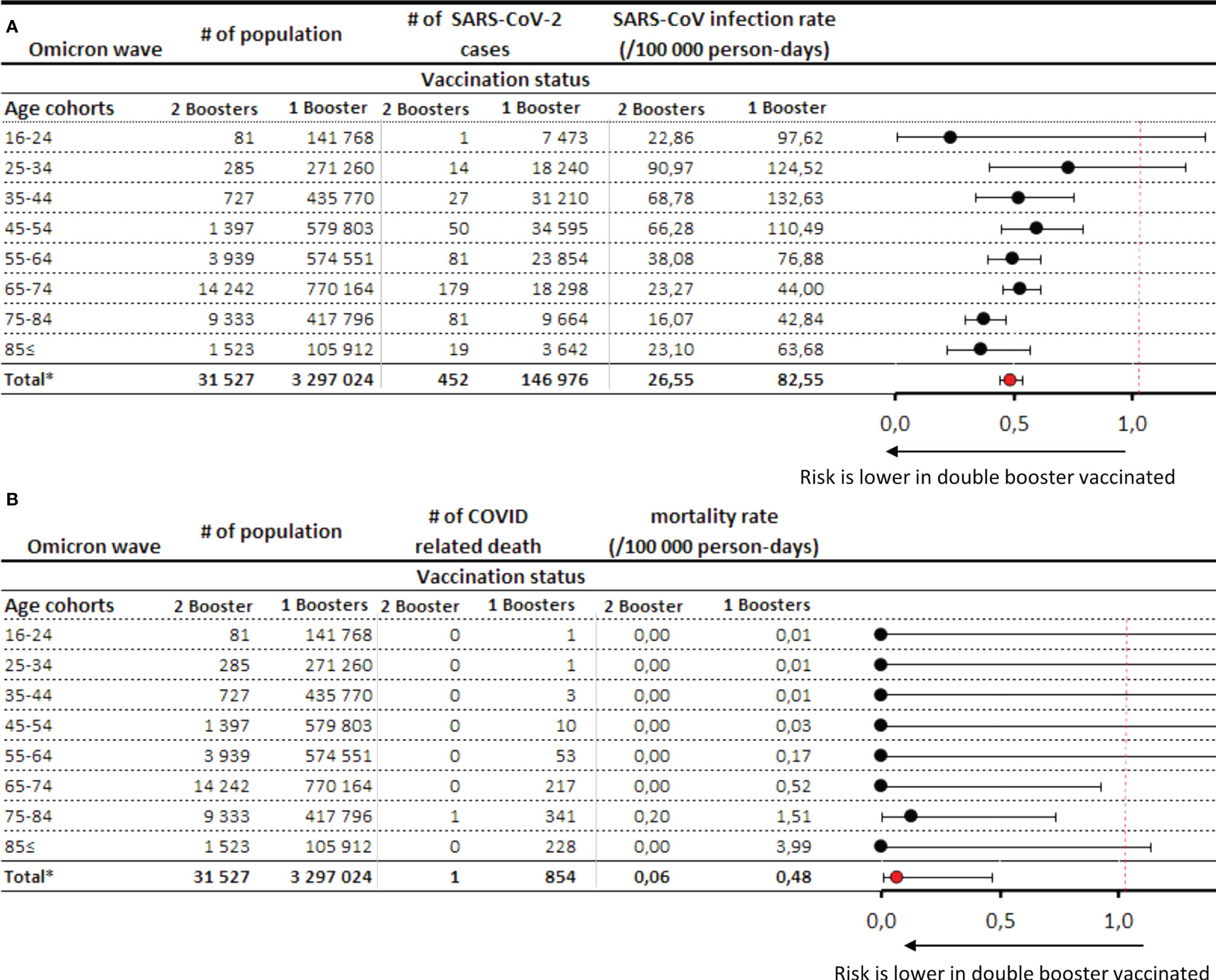
Figure 4 SARS-CoV-2 infection rates (A) and Covid-19 related mortality (B) during the Omicron wave in the double vs. single booster vaccinated population. *Exact confidence intervals for age-specific mortality rate ratios and Mantel-Haenszel pooled mortality rate ratio for the total population adjusted for age.
Overall, the risk of Covid-19 related mortality rate was 55% lower in the total Hungarian population during the Omicron vs. Delta wave (RR: 0.45 95%CI: 0.44-0.48). The difference decreased with age, with RRs of 0.15 (95% CI: 0.06–0.33) and 0.65 (95% CI: 0.59–0.71) in the age groups of 25–34 and 85≤ years, respectively (Supplementary Figure 1).
Booster vaccination provided an additional 85% reduction of mortality risk during the Delta wave (RR: 0.15; 95% CI: 0.13¬-0.17) and an additional 71% reduction during the second study period, dominated by the Omicron variant (RR: 0.29; 95% CI: 0.2–0.32) (Supplementary Figures 2A, B). This benefit had roughly the same size in almost all age cohorts.
SARS-CoV-2 infection rate of populations with different immunization level is detailed by age in Supplementary Table 1 for Delta wave and in Supplementary Table 2 for Omicron wave.
Discussion
Our retrospective study aimed to estimate the effectiveness of primary and booster SARS-CoV-2 vaccination in the pandemic waves dominated by the Delta and Omicron variants in terms of Covid-19 related mortality and explore differences between the two waves in question.
Despite its higher transmissibility, the Omicron variant has been shown to be associated with a significantly lower risk of severe outcomes compared to the Delta variant (19, 20). However, only few studies reported lower rates of the most severe outcome, Covid-19 related mortality. A recent study from South-Africa found a 73% lower risk of mortality with the Omicron vs. Delta variant (21), and the U.S. Centers for Disease Control and Prevention (CDC) reported mortality rates of 9/1,000 persons and 13/1,000 persons for the Omicron and Delta variants, respectively (22). In our study, the mortality rate of Covid-19 during the Omicron wave was 56% lower compared to the period dominated by the Delta wave in the total Hungarian population, with more pronounced differences in younger age groups. The lower risk of Covid-19 related mortality associated with the Omicron variant may be attributed to multiple factors including its potentially lower virulence (23, 24), the increasing proportion of booster immunized people by the time of the Omicron wave, and the significant impact of detected and undetected previous Delta infections (25) which could have provided protection against severe outcomes during the Omicron wave (26). Our results demonstrate the lower risk of mortality associated with the Omicron variant and confirm previous observations from South Africa and the United States.
In our study, the risk of Covid-19 related mortality was 73% lower in people who had received primary immunization (approx. 3.5 million people) compared to the unvaccinated control group during the Delta wave. Booster vaccination, mainly with an mRNA vaccine, provided additional benefits with a 97% lower risk of Covid-19 related mortality compared to the unvaccinated population. The results show that although primary immunization (mainly administered in spring 2021) had already lost effectiveness against SARS-CoV-2 infection by the time of our study period, it still provided significant additional protection against Covid-19 related death (85% relative risk reduction) (27). Our observations are in line with a study conducted among 780,225 U.S. veterans which reported significantly declining vaccine effectiveness for all investigated vaccine types against symptomatic SARS-CoV-2 infection but sustained protection against Covid-19 related death among those infected during the Delta wave (52.2% for Janssen, 75.5% for Moderna, and 70.1% for Pfizer-BioNTech in the age group of ≥65 years) (5). Furthermore, several studies have demonstrated the additional benefits of booster immunization (9, 10). In our study, this benefit was more apparent in older age groups. Compared to the unvaccinated control population, primary immunization and booster immunization resulted in a 76% and 97% lower risk of Covid-19 related mortality in the age group of 65–74 years, respectively.
The rationale for booster vaccines was questioned by several experts who argued that due to the high number of mutations affecting the spike protein of the Omicron variant (9), vaccine effectiveness against infection and severe outcomes may be compromised (21). In a study from the U.K., primary immunization with two doses of the Astra Zeneca or Pfizer-BioNTech vaccines provided limited or no protection against symptomatic disease caused by the Omicron variant, while an mRNA booster after the primary course of immunization significantly increased protection (67.2%–73.9%), although with waning effectiveness over time (60.9%–64.4%) (28).
In Hungary, the Omicron variant was first detected on 13 December 2021 (29) and became dominant by early January 2022 (30), reaching highest-ever daily infection rates on 31 January 2022. On 13 January 2022, the Hungarian government offered the option of a fourth dose for elderly people, healthcare workers and people with chronic diseases if at least 4 months had passed since their previous booster dose. By the end of our study period (23 February 2022), 189,894 people had received the second booster dose (although the average size of the population with at least 14 days since the second booster dose was only 31,527 during the study period), mostly mRNA vaccines (98.46%). There was a 40% lower risk of Covid-19 related mortality in the primary immunized population compared to the unvaccinated control group, despite higher infection rates in the former. In the booster immunized population, the risk of Covid-19 related death was 82% lower than in the unvaccinated group, and the few people who had received their second booster dose (n=31,527) had an almost 100% protection against mortality, with only one Covid-19 related death during the study period. The second booster dose further decreased the rate of SARS-CoV-2 infection by 51% compared to only one booster and provided an additional 93% mortality reduction. Although the short follow-up time of the double booster immunized group and the very low number of patients younger than 65 years in this group limit the interpretation of results related to the effectiveness of the second booster dose, these data confirm the additional short-term benefit of booster doses in the prevention of Covid-19 related mortality during the Omicron wave in the elderly.
The strengths of the HUN-VE-2 study include its nationwide nature, and the analysis of vaccine effectiveness during two consecutive waves of the coronavirus pandemic. Furthermore, the large study populations allowed for the evaluation of different levels of vaccination in different age groups. Nevertheless, our study has some limitations. The proportion of undetected cases might have been high and could have increased during the wave dominated by the Omicron variant. Therefore, we refrained from analyzing registered infections. We made an exemption when we estimated the impact of double booster and single booster vaccination, because we wanted to see how much the effect size is different in the case of SARS-CoV-2 infection and Covid-19 related mortality. Although the infection rates might be underestimated, we assume that the ascertainment bias was not likely to significantly affect the relative rates, as the proportion of unregistered cases among all cases was not likely to substantially differ in the two compared groups.
We studied the effect of vaccination by age, and adjusted for age when studying total populations, but an important limitation of our study is that we could not adjust for other potential confounders, most importantly for chronic diseases. As chronic diseases represent an indication for early vaccination as well as booster vaccination, and are closely related to mortality, this confounding may have influenced our results to a certain extent. However, as booster and second booster vaccinations were especially recommended for elderly people with chronic diseases, vaccine effectiveness was likely to be somewhat underestimated.
Our study is one of the very few demonstrating the benefit of second booster vaccination. Despite declining effectiveness against symptomatic disease caused by the Omicron variant, booster doses still provided protection against Covid-19 accompanying mortality. This suggests that although antibody responses tend to wane over time (28), cellular immune responses may also play a significant part in the protection against severe outcomes, and this protection may be significantly enhanced by a second booster dose. Our findings also raise the possibility that cellular immune responses may have an important role in the protection against upcoming new SARS-CoV-2 variants. A recent study from Israel demonstrated the rapid decline in the regained reduction of viral load achieved by the booster shot 3–4 months after its administration (31). These results strongly correlate with our findings showing more pronounced mortality risk reduction among people who received booster immunization during the Delta wave compared to the Omicron wave. Therefore, Hungarian guidelines recommend a fourth vaccine dose for the vulnerable population after 4 months of their first booster dose.
A clear limitation of our study is a low number of events in certain subgroups, mainly in the younger age cohorts, as indicated by the very wide confidence intervals of the rate ratio for these age groups. Nevertheless, the crude mortality and event rates are reassuring also for the young people regarding the vaccine effectiveness.
During the Delta pandemic wave, the mean time since the last dose of vaccine in case of primary immunization population was overall 188.95 days till the end of the first study period (31st of December 2021), while the mean time since the last dose of vaccine in case of boostered population was 63.30 days. While in second part of our study, during the Omicron pandemic wave, the mean time by the end of second study period (23rd of February 2022) since the last dose of vaccine was 220.26, 100.50 and 25.08 days in the population of those received primary immunization and in cohorts of those, received the 1st and 2nd booster doses, respectively. Hence, the vaccine effectiveness could be impacted by the different vanishing level of vaccine effect as it was proved in several other studies (17, 27).
The nationwide HUN-VE 2 study provides an overview of the protection against Covid-19 related mortality with different levels of vaccination during the Delta and Omicron waves. The results show a significantly lower risk of Covid-19 related mortality during the Omicron wave in the whole study population and confirm the benefits of booster vaccination in the prevention of Covid-19 related death. Furthermore, our study is among the first to report the significant additional benefit of a second booster dose in terms of mortality reduction in older populations, beyond the improvement in protection against symptomatic SARS-CoV-2 infection.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Ethics Statement
The studies involving human participants were reviewed and approved by Central Ethical Committee of Hungary (OGYÉI/10296-1/2022 and IV/1722-1/2022/EKU). Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author Contributions
ZV: Conceptualization, Methodology, Formal analysis, Validation and Writing – Review & Editing; ZK and IW: Conceptualization, Methodology, Investigation, Visualization and Writing – Original Draft; LP Conceptualization, Methodology, Formal analysis, Validation, Data curation; GS, PN, IK, AW: Conceptualization, Methodology, Validation, Review & Editing; DN: Conceptualization, Methodology, Formal analysis; OS, VM, ZSz, JS: Conceptualization, Review & Editing; MK, CM, ZSc: Conceptualization, Methodology, Investigation and Supervision; ZB: Writing – Original Draft; GM: Validation, Project Administration. All authors contributed to the article and approved the submitted version.
Funding
The Center for Health Technology Assessment of the Semmelweis University participated in the project on a contractual basis made with the Ministry of Human Resources of Hungary and received funding. Zsófia Barcza of Syntesia Medical Communications Ltd. received payment for medical writing support from the National Public Health Center of Hungary.
Conflict of Interest
Author ZB was employed by company Syntesia Medical Communications Ltd. ZB of Syntesia Medical Communications Ltd. received payment for medical writing support from the National Public Health Center of Hungary. ZK is employed by MSD Pharma Hungary Ltd., too. However, this provides no relevant conflict of interest for the current research. At the time the study was performed, MK served as the minister of human resources. The ministry includes the secretariat for health.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
The authors would like to thank Richárd Kiss for the initial data curation and dataset validation.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2022.905585/full#supplementary-material
Supplementary Table 1 | Age distribution, infection rate and mortality rate during Delta pandemic wave by immunization level.
Supplementary Table 2 | Age distribution, infection rate and mortality rate during Omicron pandemic wave by immunization level.
References
1. Islam S, Islam T, Islam MR. New Coronavirus Variants are Creating More Challenges to Global Healthcare System: A Brief Report on the Current Knowledge. Clinical pathology. (Ventura County, Calif: Thousand Oaks .)(2022) 15:2632010X221075584. doi: 10.1177/2632010X221075584
2. Rudan I, Adeloye D, Sheikh A. COVID 19: Vaccines, Efficacy and Effects on Variants. Curr Opin Pulm Med (2022) 28(3):180–91. doi: 10.1097/MCP.0000000000000868
3. Vokó Z, Kiss Z, Surján G, Surján O, Barcza Z, Pályi B, et al. Nationwide Effectiveness of Five SARS-CoV-2 Vaccines in Hungary—the HUN-VE Study. Clin Microbiol Infect (2022) 28:398–404. doi: 10.1016/J.CMI.2021.11.011/ATTACHMENT/8664EA2B-925A-49D4-A32E-5730A403E77C/MMC2.DOCX
4. Meggiolaro A, Sane Schepisi M, Nikolaidis GF, Mipatrini D, Siddu A, Rezza G. Effectiveness of Vaccination Against SARS-CoV-2 Infection in the Pre-Delta Era: A Systematic Review and Meta-Analysis. Vaccines (2022) 10:157. doi: 10.3390/VACCINES10020157
5. Cohn BA, Cirillo PM, Murphy CC, Krigbaum NY, Wallace AW. SARS-CoV-2 Vaccine Protection and Deaths Among US Veterans During 2021. Science (80- ) (2022) 375:331–6. doi: 10.1126/SCIENCE.ABM0620/SUPPL_FILE/SCIENCE.ABM0620_MDAR_REPRODUCIBILITY_CHECKLIST.PDF
6. Chemaitelly H, Tang P, Hasan MR, AlMukdad S, Yassine HM, Benslimane FM, et al. Waning of BNT162b2 Vaccine Protection Against SARS-CoV-2 Infection in Qatar. N Engl J Med (2021) 385:e83. doi: 10.1056/NEJMOA2114114/SUPPL_FILE/NEJMOA2114114_DISCLOSURES.PDF
7. Goldberg Y, Mandel M, Bar-On YM, Bodenheimer O, Freedman L, Haas EJ, et al. Waning Immunity After the BNT162b2 Vaccine in Israel. N Engl J Med (2021) 385:e85. doi: 10.1056/NEJMOA2114228/SUPPL_FILE/NEJMOA2114228_DISCLOSURES.PDF
8. Tartof SY, Slezak JM, Fischer H, Hong V, Ackerson BK, Ranasinghe ON, et al. Effectiveness of mRNA BNT162b2 COVID-19 Vaccine Up to 6 Months in a Large Integrated Health System in the USA: A Retrospective Cohort Study. Lancet (2021) 398:1407–16. doi: 10.1016/S0140-6736(21)02183-8/ATTACHMENT/E998365A-8F41-4C9C-997B-8F5A40D3AAD4/MMC1.PDF
9. Barda N, Dagan N, Cohen C, Hernán MA, Lipsitch M, Kohane IS, et al. Effectiveness of a Third Dose of the BNT162b2 mRNA COVID-19 Vaccine for Preventing Severe Outcomes in Israel: An Observational Study. Lancet (2021) 398:2093–100. doi: 10.1016/S0140-6736(21)02249-2/ATTACHMENT/588607F0-89F7-4E80-8E48-FB7CE8C7F7EC/MMC1.PDF
10. Arbel R, Hammerman A, Sergienko R, Friger M, Peretz A, Netzer D, et al. BNT162b2 Vaccine Booster and Mortality Due to Covid-19. N Engl J Med (2021) 385:2413–20. doi: 10.1056/NEJMOA2115624/SUPPL_FILE/NEJMOA2115624_DISCLOSURES.PDF
11. Magyarország Az Első, Ahol Már a Harmadik Oltásra is Lehet Időpontot Foglalni. Available at: https://koronavirus.gov.hu/cikkek/magyarorszag-az-elso-ahol-mar-harmadik-oltasra-lehet-idopontot-foglalni (Accessed March 26, 2022).
12. Karim SSA, Karim QA. Omicron SARS-CoV-2 Variant: A New Chapter in the COVID-19 Pandemic. Lancet (2021) 398:2126–8. doi: 10.1016/S0140-6736(21)02758-6/ATTACHMENT/FB9D1AF8-6927-48BD-B7B7-A5055C3743D5/MMC1.PDF
13. Kozlov M. Omicron’s Feeble Attack on the Lungs Could Make it Less Dangerous. Nature (2022) 601:177. doi: 10.1038/D41586-022-00007-8
14. Introduction of 4th Vaccination by the National Public Health Center (NPHC) Webpage. Available at: https://koronavirus.gov.hu/sites/default/files/sites/default/files/imce/nnk_eljarasrend_2022.01.14._negyedik_oltas.pdf.
15. Teles M, Connolly CM, Frey S, Chiang TP-Y, Alejo JJ, Boyarsky BJ, et al. Attenuated Response to Fourth Dose SARS-CoV-2 Vaccination in Patients With Autoimmune Disease: A Case Series. Ann Rheum Dis (2022), 81(5):738–40. doi: 10.1136/ANNRHEUMDIS-2021-221641. annrheumdis-2021-221641.
16. Regev-Yochay G, Gonen T, Gilboa M, Mandelboim M, Indenbaum V, Amit S, et al. 4th Dose COVID mRNA Vaccines’ Immunogenicity & Efficacy Against Omicron VOC. medRxiv (2022), 386(14):1377–80. doi: 10.1101/2022.02.15.22270948. 2022.02.15.22270948.
17. Vokó Z, Kiss Z, Surján G, Surján O, Barcza Z, Wittmann I, et al. Effectiveness and Waning of Protection With Different SARS-CoV-2 Primary and Booster Vaccines During the Delta Pandemic Wave in 2021 in Hungary (HUN-VE 3 Study). medRxiv. doi: 10.1101/2022.04.14.22273898. 2022.04.14.22273898.
18. Vandenbroucke JP, von Elm E, Altman DG, Gøtzsche PC, Mulrow CD, Pocock SJ, et al. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and Elaboration. Int J Surg (2014) 12:1500–24. doi: 10.1016/J.IJSU.2014.07.014
19. Bhattacharyya RP, Hanage WP. Challenges in Inferring Intrinsic Severity of the SARS-CoV-2 Omicron Variant. N Engl J Med (2022) 386:e14. doi: 10.1056/NEJMP2119682/SUPPL_FILE/NEJMP2119682_DISCLOSURES.PDF
20. Ferguson N, Ghani A, Hinsley W, Volz E. Report 50: Hospitalisation Risk for Omicron Cases in England. Imperial College London. (2021). doi: 10.25561/93035.
21. Davies M-A, Kassanjee R, Rosseau P, Morden E, Johnson L, Solomon W, et al. Outcomes of Laboratory-Confirmed SARS-CoV-2 Infection in the Omicron-Driven Fourth Wave Compared With Previous Waves in the Western Cape Province, South Africa. medRxiv (2022) 13. doi: 10.1101/2022.01.12.22269148. 2022.01.12.22269148.
22. Iuliano AD, Brunkard JM, Boehmer TK, Peterson E, Adjei S, Binder AM, et al. Trends in Disease Severity and Health Care Utilization During the Early Omicron Variant Period Compared With Previous SARS-CoV-2 High Transmission Periods — United States, December 2020–January 2022. MMWR Morb Mortal Wkly Rep (2022) 71:146–52. doi: 10.15585/MMWR.MM7104E4
23. Lewnard JA, Hong VX, Patel MM, Kahn R, Lipsitch M, Tartof SY. Clinical Outcomes Among Patients Infected With Omicron (B.1.1.529) SARS-CoV-2 Variant in Southern California. medRxiv (2022). doi: 10.1101/2022.01.11.22269045. 2022.01.11.22269045.
24. Halfmann PJ, Iida S, Iwatsuki-Horimoto K, Maemura T, Kiso M, Scheaffer SM, et al. SARS-CoV-2 Omicron Virus Causes Attenuated Disease in Mice and Hamsters. Nature (2022) 603(7902):687–92. doi: 10.1038/s41586-022-04441-6
25. Byambasuren O, Dobler CC, Bell K, Rojas DP, Clark J, McLaws ML, et al. Comparison of Seroprevalence of SARS-CoV-2 Infections With Cumulative and Imputed COVID-19 Cases: Systematic Review. PLoS One (2021) 16:e0248946. doi: 10.1371/JOURNAL.PONE.0248946
26. Coronavirus (COVID-19) Infection Survey Technical Article: Impact of Vaccination on Testing Positive in the UK - Office for National Statistics. Available at: https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/articles/coronaviruscovid19infectionsurveytechnicalarticleimpactofvaccinationontestingpositiveintheuk/latest (Accessed March 26, 2022).
27. Pormohammad A, Zarei M, Ghorbani S, Mohammadi M, Neshin SAS, Khatami A, et al. Effectiveness of COVID-19 Vaccines Against Delta (B.1.617.2) Variant: A Systematic Review and Meta-Analysis of Clinical Studies. Vaccines (2021) 10:23. doi: 10.3390/VACCINES10010023
28. Ai J, Zhang H, Zhang Y, Lin K, Zhang Y, Wu J, et al. Omicron Variant Showed Lower Neutralizing Sensitivity Than Other SARS-CoV-2 Variants to Immune Sera Elicited by Vaccines After Boost. Emerg Microbes Infect (2022) 11:337–43. doi: 10.1080/22221751.2021.2022440/SUPPL_FILE/TEMI_A_2022440_SM0105.DOCX
29. Magyarországon is Megjelent Az Omikron Variáns. Available at: https://koronavirus.gov.hu/cikkek/magyarorszagon-megjelent-az-omikron-varians (Accessed March 26, 2022).
30. SARS-CoV-2 Variants Dashboard. Available at: https://www.ecdc.europa.eu/en/covid-19/situation-updates/variants-dashboard (Accessed March 26, 2022).
Keywords: SARS-CoV2 infection, booster vaccine, 4th vaccine, omicron variant (SARS-CoV-2), delta variant (B.1.617.2), vaccine effectiveness, mortality
Citation: Kiss Z, Wittmann I, Polivka L, Surján G, Surján O, Barcza Z, Molnár GA, Nagy D, Müller V, Bogos K, Nagy P, Kenessey I, Wéber A, Pálosi M, Szlávik J, Schaff Z, Szekanecz Z, Müller C, Kásler M and Vokó Z (2022) Nationwide Effectiveness of First and Second SARS-CoV2 Booster Vaccines During the Delta and Omicron Pandemic Waves in Hungary (HUN-VE 2 Study). Front. Immunol. 13:905585. doi: 10.3389/fimmu.2022.905585
Received: 27 March 2022; Accepted: 24 May 2022;
Published: 23 June 2022.
Edited by:
Rong Hai, University of California, Riverside, United StatesReviewed by:
Linfeng Gao, University of California, Irvine, United StatesWeifeng Gu, University of California, Riverside, United States
Copyright © 2022 Kiss, Wittmann, Polivka, Surján, Surján, Barcza, Molnár, Nagy, Müller, Bogos, Nagy, Kenessey, Wéber, Pálosi, Szlávik, Schaff, Szekanecz, Müller, Kásler and Vokó. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Zoltán Vokó, dm9rby56b2x0YW5Ac2VtbWVsd2Vpcy11bml2Lmh1
†These authors contributed equally to this work and share first authorship
‡These authors contributed equally to this work and share senior authorship