 Per Ljungman1,2*
Per Ljungman1,2* Gloria Tridello3Jose Luis Piñana4,5
Gloria Tridello3Jose Luis Piñana4,5 Fabio Ciceri6Henrik Sengeloev7Alexander Kulagin8Stephan Mielke1,9Zeynep Arzu Yegin10
Fabio Ciceri6Henrik Sengeloev7Alexander Kulagin8Stephan Mielke1,9Zeynep Arzu Yegin10 Matthew Collin11Sigrun Einardottir12,13Sophie Ducastelle Lepretre14Johan Maertens15
Matthew Collin11Sigrun Einardottir12,13Sophie Ducastelle Lepretre14Johan Maertens15 Antonio Campos16
Antonio Campos16 Elisabetta Metafuni17
Elisabetta Metafuni17 Herbert Pichler18Frantisek Folber19,20
Herbert Pichler18Frantisek Folber19,20 Carlos Solano3Emma Nicholson21Meltem Kurt Yüksel22Kristina Carlson23Beatriz Aguado24Caroline Besley25Jenny Byrne26
Carlos Solano3Emma Nicholson21Meltem Kurt Yüksel22Kristina Carlson23Beatriz Aguado24Caroline Besley25Jenny Byrne26 Immaculada Heras27Fiona Dignan28
Immaculada Heras27Fiona Dignan28 Nicolaus Kröger29Christine Robin30Anjum Khan31Stig Lenhoff32Anna Grassi33
Nicolaus Kröger29Christine Robin30Anjum Khan31Stig Lenhoff32Anna Grassi33 Veronika Dobsinska34Nuno Miranda35
Veronika Dobsinska34Nuno Miranda35 Maria-Jose Jimenez36
Maria-Jose Jimenez36 Ipek Yonal-Hindilerden37Keith Wilson38
Ipek Yonal-Hindilerden37Keith Wilson38 Dina Averbuch39Simone Cesaro40Alienor Xhaard41Nina Knelange42
Dina Averbuch39Simone Cesaro40Alienor Xhaard41Nina Knelange42 Jan Styczynski43
Jan Styczynski43 Malgorzata Mikulska44
Malgorzata Mikulska44 Rafael de la Camara24
Rafael de la Camara24- 1Department of Cellular Therapy and Allogeneic Stem Cell Transplantation, Karolinska Comprehensive Cancer Center, Karolinska University Hospital Huddinge, Stockholm, Sweden
- 2Division of Hematology, Department of Medicine Huddinge, Karolinska Institutet, Stockholm, Sweden
- 3European Society for Blood and Marrow Transplantation (EBMT) Data Office, Department of Medical Statistics & Bioinformatics, Leiden, Netherlands
- 4Hematology Department, Hospital Clínico Universitario de Valencia, Valencia, Spain
- 5Fundación Investigación del Hospital Clínico de la Comunidad Valenciana (INCLIVA), Instituto de Investigación Sanitaria Hospital Clínico Universitario de Valencia, Valencia, Spain
- 6Istituto di Ricovero e Cura a Carattere Scientifico (IRCCS) Ospedale San Raffaele, University Vita-Salute San Raffaele, Milan, Italy
- 7Department of Hematology, Copenhagen University Hospital, Copenhagen, Denmark
- 8Raisa Memorial (RM) Gorbacheva Research Institute, Pavlov University, St. Petersburg, Russia
- 9Department of Laboratory Medicine, Karolinska Institutet, Stockholm, Sweden
- 10Department of Hematology, Gazi University Faculty of Medicine, Ankara, Türkiye
- 11Translational and Clinical Research Institute and The National Institute for Health and Care Research (NIHR) Newcastle Biomedical Research Centre, Newcastle, United Kingdom
- 12Department of Hematology, Sahlgrenska University Hospital, Gothenburg, Sweden
- 13Department of Internal Medicine, Institute of Medicine, Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden
- 14Service d’Hématologie. Hôpital Lyon Sud, Lyon, France
- 15Department of Hematology University Hospital Gasthuisberg, Leuven, Belgium
- 16Marrow Transplant Department Inst. Português de Oncologia do Porto, Porto, Portugal
- 17Dipartimento di Diagnostica per Immagini, Radioterapia Oncologica e Ematologia, Fondazione Policlinico Universitario Agostino Gemelli Istituto di Ricovero e Cura a Carattere Scientifico (IRCCS), Rome, Italy
- 18St. Anna Children’s Hospital, Department of Pediatrics and Adolescent Medicine, Medical University of Vienna, Vienna, Austria
- 19Department of Internal Medicine, Hematology and Oncology University Hospital Brno, Brno, Czechia
- 20Department of Internal Medicine, Hematology and Oncology Masaryk University, Brno, Czechia
- 21Haematology-oncology Unit Royal Marsden Hospital, London, United Kingdom
- 22Department of Hematology, Ankara University Faculty of Medicine, Ankara, Türkiye
- 23Department of Hematology, Uppsala University Hospital, Uppsala, Sweden
- 24Department of Hematology, Hospital Universitario de la Princesa, Madrid, Spain
- 25University Hospitals Bristol and Weston National Health Service (NHS) Foundation Trust, Bristol, United Kingdom
- 26Department of Haematology Nottingham University Hospital, Nottingham, United Kingdom
- 27Department of Hematology, Hospital Universitario Morales Meseguer, Instituto Murciano de Investigación Biosanitaria (IMIB)-Arrixaca, Universidad de Murcia, Murcia, Spain
- 28Clinical Haematology Department Manchester Royal Infirmary, Manchester, United Kingdom
- 29Department of Stem cell Transplantation, University Hospital Eppendorf, Hamburg, Germany
- 30Assistance Publique-Hôpitaux de Paris (APHP), Henri Mondor Hospital, Department of Hematology, Créteil, France
- 31Department of Haematology Leeds Teaching Hospitals NHS Trust, Leeds, United Kingdom
- 32Department of Hematology Skåne’s University Hospital, Lund, Sweden
- 33Bone Marrow Transplantation Unit, Azienda Sociosanitaria Territoriale (ASST) Papa Giovanni XXIII, Bergamo, Italy
- 34Department of Pediatric Hematology and Oncology, National Institute of Children’s Diseases, Comenius University, Bratislava, Slovakia
- 35Department of Haematology Inst. Portugues Oncologia, Lisbon, Portugal
- 36Department of Clinical Haematology Institut Catala d'Oncologia (ICO)-Hospital Universitari Germans Trias i Pujol, Badalona, Spain
- 37Istanbul Medical Faculty, Adult Hematopoietic Stem Cell Transplant Center, Istanbul University, Istanbul, Türkiye
- 38Blood and Bone Marrow Transplantation Department University of Cardiff, Cardiff, United Kingdom
- 39Pediatric Infectious Diseases Unit, Hadassah Medical Center and Faculty of Medicine, Hebrew University of Jerusalem, Jerusalem, Israel
- 40Pediatric Hematology Oncology, Azienda Ospedaliera Universitaria Integrata, Verona, Italy
- 41Hematology-Transplantation Unit, Department of Hematology: Hôpital St. Louis, Paris, France
- 42European Society for Blood and Marrow Transplantation (EBMT) Leiden Study Unit, European Society for Blood and Marrow Transplantation (EBMT) Data Office, Leiden, Netherlands
- 43Department of Pediatric Hematology and Oncology, Collegium Medicum, Nicolaus Copernicus University Torun, Bydgoszcz, Poland
- 44Division of Infectious Diseases, University of Genoa and Ospedale Policlinico San Martino, Genova, Italy
Introduction: COVID-19 has been associated with high morbidity and mortality in allogeneic hematopoietic stem cell transplant (allo-HCT) recipients.
Methods: This study reports on 986 patients reported to the EBMT registry during the first 29 months of the pandemic.
Results: The median age was 50.3 years (min – max; 1.0 – 80.7). The median time from most recent HCT to diagnosis of COVID-19 was 20 months (min – max; 0.0 – 383.9). The median time was 19.3 (0.0 - 287.6) months during 2020, 21.2 (0.1 - 324.5) months during 2021, and 19.7 (0.1 – 383.9) months during 2022 (p = NS). 145/986 (14.7%) patients died; 124 (12.6%) due to COVID-19 and 21 of other causes. Only 2/204 (1%) fully vaccinated patients died from COVID-19. There was a successive improvement in overall survival over time. In multivariate analysis, increasing age (p<.0001), worse performance status (p<.0001), contracting COVID-19 within the first 30 days (p<.0001) or 30 – 100 days after HCT (p=.003), ongoing immunosuppression (p=.004), pre-existing lung disease (p=.003), and recipient CMV seropositivity (p=.004) had negative impact on overall survival while patients contracting COVID-19 in 2020 (p<.0001) or 2021 (p=.027) had worse overall survival than patients with COVID-19 diagnosed in 2022.
Discussion: Although the outcome of COVID-19 has improved, patients having risk factors were still at risk for severe COVID-19 including death.
Introduction
The SARS-CoV-2 emerged at the end of 2019, and Coronavirus Disease 2019 (COVID-19) started spreading worldwide. The WHO classified COVID-19 as a pandemic on March 11, 2020. During the two years of the pandemic, several variants have emerged including Omicron variants, which started to spread in the end of 2021, and which have been the dominating variants during 2022. It was early recognized that immunocompromised patients were at a high risk for severe COVID-19 with ensuing high mortality. Allogeneic hematopoietic cell transplant recipients (allo-HCT) are prone to develop severe infections with many viruses including community-acquired respiratory viruses. This has been shown to be the case also with SARS-CoV-2. The European Society for Blood and Marrow Transplantation (EBMT) initiated a prospective case collection in February 2020 and two reports have been published about the outcome in autologous and allogeneic HCT recipients and patients having undergone CAR T cell treatment, respectively (1, 2). Both analyses showed a high mortality reaching almost 30% in HCT recipients during the first period of the pandemic. Since then, variants with higher transmissibility but lower lethality have been emerging, and many improvements in management have been implemented including easy access to diagnostic tests, antiviral drugs (remdesivir, nirmatrelvir/ritonavir, molnupiravir), and monoclonal antibodies for treatment, vaccination, and for symptomatic patients improved triage algorithms and supportive care.
This paper aimed to analyze the outcome of COVID-19 in allo-HCT patients from February 2020 to July 2022 with the aim to see if the outcome has improved and if the risk factors are the same for severe and fatal COVID-19 also during the recent Omicron period. We also added CMV serology to the risk factors with the hypothesis that CMV seropositive patients could have worse outcome compared to CMV seronegative.
Methods
This prospective survey has merged newly collected data with previous data existing in the EBMT registry. All patients gave informed consent for their data to be included in the registry. The case record forms have changed during the pandemic as knowledge have been gained but questions included the symptoms, potential risk factors for development of lower respiratory tract disease requiring ventilatory support, treatments, the need for hospitalization, intensive care, and outcome. In addition to the COVID-19 specific forms, the EBMT registry’s so called Minimal Essential Data A (MED-A) was used to extract previously submitted data regarding baseline patient information, data regarding the underlying diagnosis, and the transplant procedure, which were used in the analysis.
Criteria for inclusion in the study were that the patient should be PCR positive for SARS-CoV-2 regardless of symptoms and have undergone an allo-HCT at any time before the diagnosis of COVID-19. From the beginning of 2021, a positive SARS-CoV-2 antigen test was also accepted for study inclusion. The Swedish central Ethical Board (EPM 2020-01731) approved the study and other approvals, if required, were obtained according to national regulations. For this analysis, patients diagnosed with SARS-CoV-2 infection before July 15, 2022 were included and patients needed to have at least six weeks of follow-up.
The analysis was split in patients diagnosed with COVID-19 during the three calendar years (2020, 2021, and 2022). The first period includes the cohort already reported (2). We also did another analysis with the aim to mimic the important phases of the pandemic: February – July 2020 representing the initial phase. Most patients in this cohort were included in our previous publication (2). August 2020 – January 2021, February 2021 – November 2021 representing the early vaccination phase during which the alfa and delta variants were dominating, and finally December 2021 – July 2022 representing the Omicron phase.
Statistics
The main characteristics of patients were reported by descriptive statistics. Median, minimum and maximum values were used for continuous variables, while absolute and percentage frequencies were used for categorical variables. Comparisons between categorical variables were performed by the Chi square or Fisher exact test, as appropriate, while continuous variables were compared by t-test or Kruskal-Wallis test. The overall survival was estimated by using the Kaplan Meier methods, considering the death due to any cause as an event and the time from COVID-19 infection to the latest follow-up as survival time; the difference between groups was tested by the log-rank test. Univariate and multivariate risk factor analysis for overall survival were performed with the Cox regression model. Variables with a p-value < 0.2 at univariate analysis were entered into the multivariate models and selected according to a stepwise selection. A p-value <0.05 was considered statistically significant. All p-values are two-sided.
Due to the presence of missing data, the SMC-FCS imputation technique was used. The complete case analysis will be performed and considered as the main result, whilst the results obtained from the imputed dataset will be considered as sensitivity analysis. All the main analyses were performed using the statistical software SAS v. 9.4 (SAS Institute Inc., Cary, NC, USA), the imputation techniques and the sensitivity analysis were performed by using the software R (https://www.r-project.org/).
Results
Patients
986 patients from 22 countries fulfilled the criteria for inclusion. The median age was 50.3 years (min – max; 1.0 – 80.7) and did not differ over the years. One hundred fourteen patients were children (< 18 years of age; median age 10.5 (1.0 – 17.8)). The distribution of reported cases over time is shown in Figure 1. Details about donor type, conditioning, stem cell source, and GVHD are shown in Table 1.
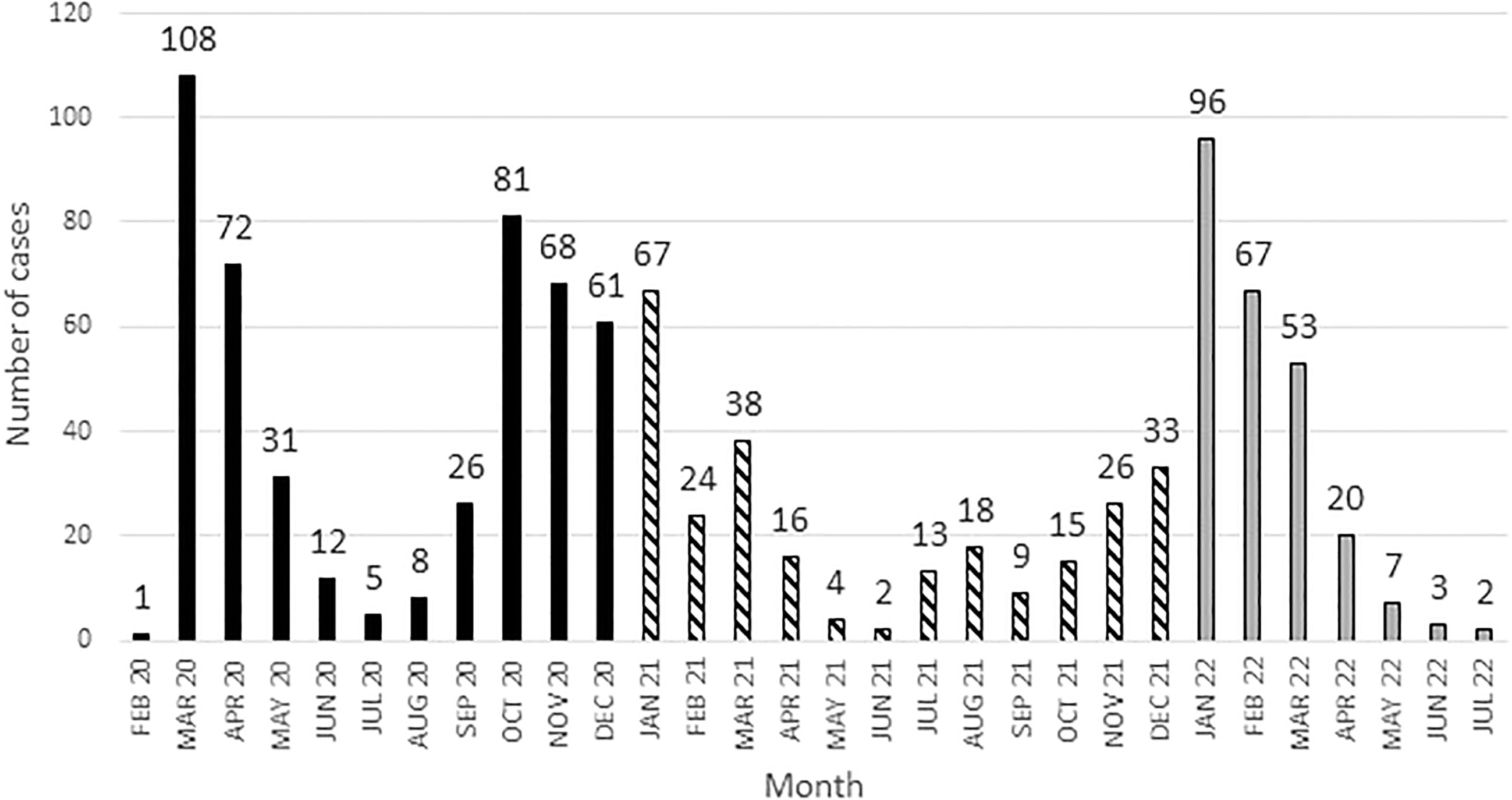
Figure 1 Distribution of cases over time.
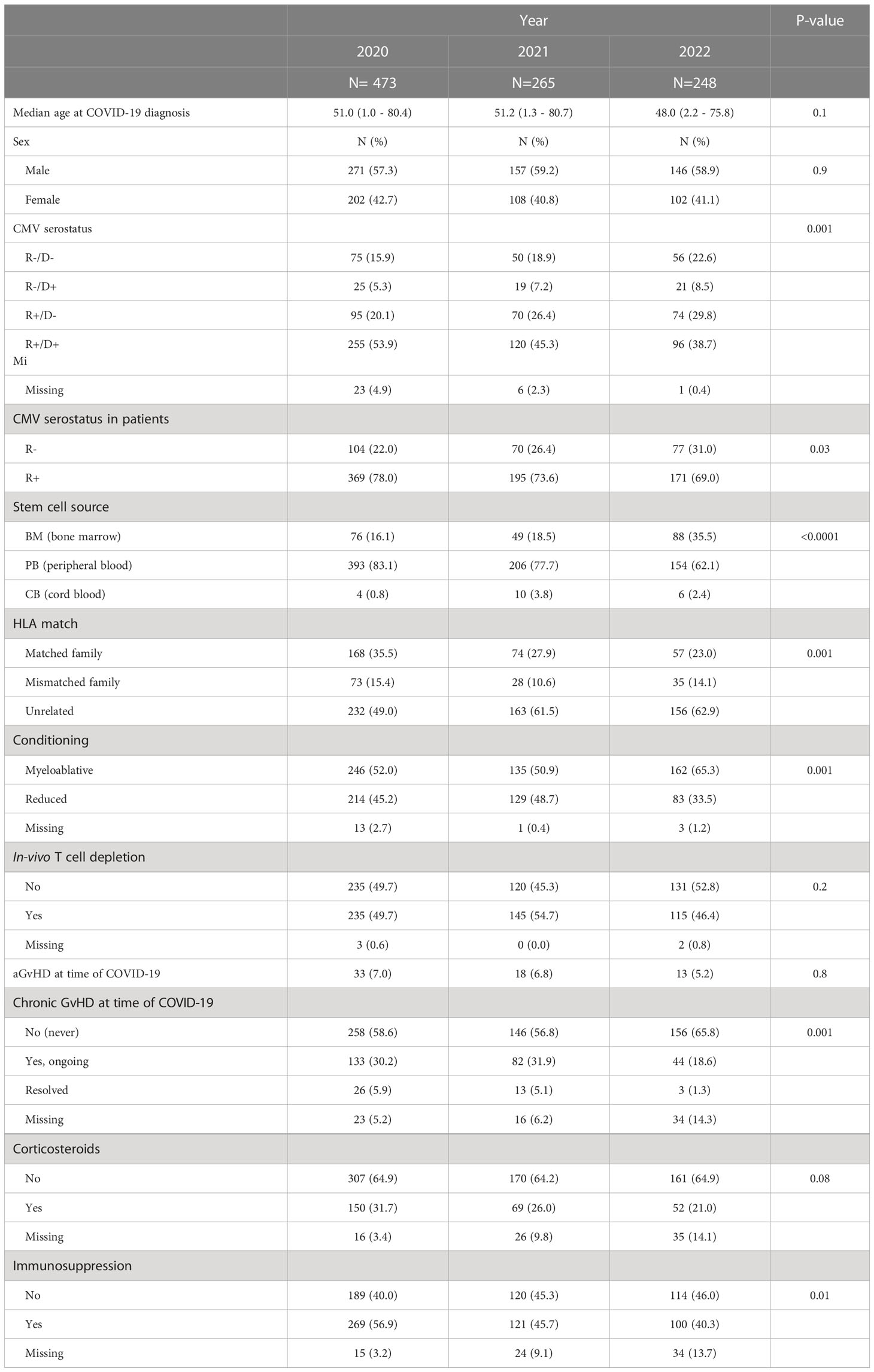
Table 1 Characteristics of patients having undergone allogeneic HCT.
COVID-19
The median time from most recent HCT to diagnosis of COVID-19 was 20 months (min – max; 0.0 – 383.9). The median time was 19.3 (0.0 - 287.6) months during 2020, 21.2 (0.1 - 324.5) months during 2021, and 19.7 (0.1 – 383.9) months during 2022 (p = NS). At the time of diagnosis, fewer patients required oxygen support during the later years (17.3% during 2020, 11.0% during the 2021, and 0.9% during 2022). The proportions of patients with ongoing immunosuppression decreased over the periods (p=0.01). The proportion of the patients being hospitalized during the COVID-19 episode decreased over time with 56.0% hospitalized during 2020, 38.1% during 2021, and 15.9% during 2022 (p<.0001). The proportion of patients with lower respiratory tract disease decreased over time. This decrease was seen both at the time of COVID-19 diagnosis (12.5% in 2020; 10.9% in 2021; 2.8% in 2022) and during follow-up (50.5% in 2020; 30.9% in 2021; 15.7% in 2022). The proportion of patients treated with antiviral drugs or monoclonal antibodies increased over time as such became available (Supplementary Table 2).
Previous vaccination
253 patients had been vaccinated before the diagnosis of COVID-19. 34 patients had received one dose, 77 two doses, 119 three doses, 22 four doses, and one patient had received five doses of vaccine. The absolute majority had received mRNA vaccines. Only two of 204 (1%) fully vaccinated patients (defined as having received at least two doses with the 2nd dose given > 14 days before diagnosis of COVID-19) died from COVID-19 while five patients died from other causes.
Overall survival in COVID-19
At the time of analysis, 145/986 (14.7%) patients had died; 124 patients (12.6%) died from COVID-19 and 21 patients died from other causes. The outcome was significantly better in children (Figure 2), who had a 6-week overall survival of 96.4% (95% CI 89.3% - 98.1%) compared to adults (6-week OS of 87.7% (95% CI 85.2% - 89.8%; P = .01). Survival curves for the three calendar years are shown in Figure 3 showing an improvement in overall survival from 83.8% (95% CI 80.0-86.9) in 2020 to 90.7% (95% CI 86.3-93.7) during 2021, and 95.3% (95% CI 91.6% - 97.4%) during 2022 (p<.0001). Similar differences were seen when survival was analysed based on the different phases of the pandemic (Figure 4). During the first phase (February – July 2020), the survival was 76.8% (95% CI 70.5-82.0. During the second phase before vaccines became available (August 2020 – January 2021), the survival was 88.5% (95% CI 84.1-91.7). The survival had improved further during the phase when the vaccines were introduced also coinciding with the rapid spread of the Delta variant (93.0% (95% CI 87.7-96.0)) and finally the best overall survival was seen when the Omicron variant had become dominant (95.5% (95% CI 92.1-97.4)). The risk for developing lower respiratory tract disease also decreased over time both at the time of diagnosis and during follow-up supporting a lower severity of SARS-CoV-2 infections with time.
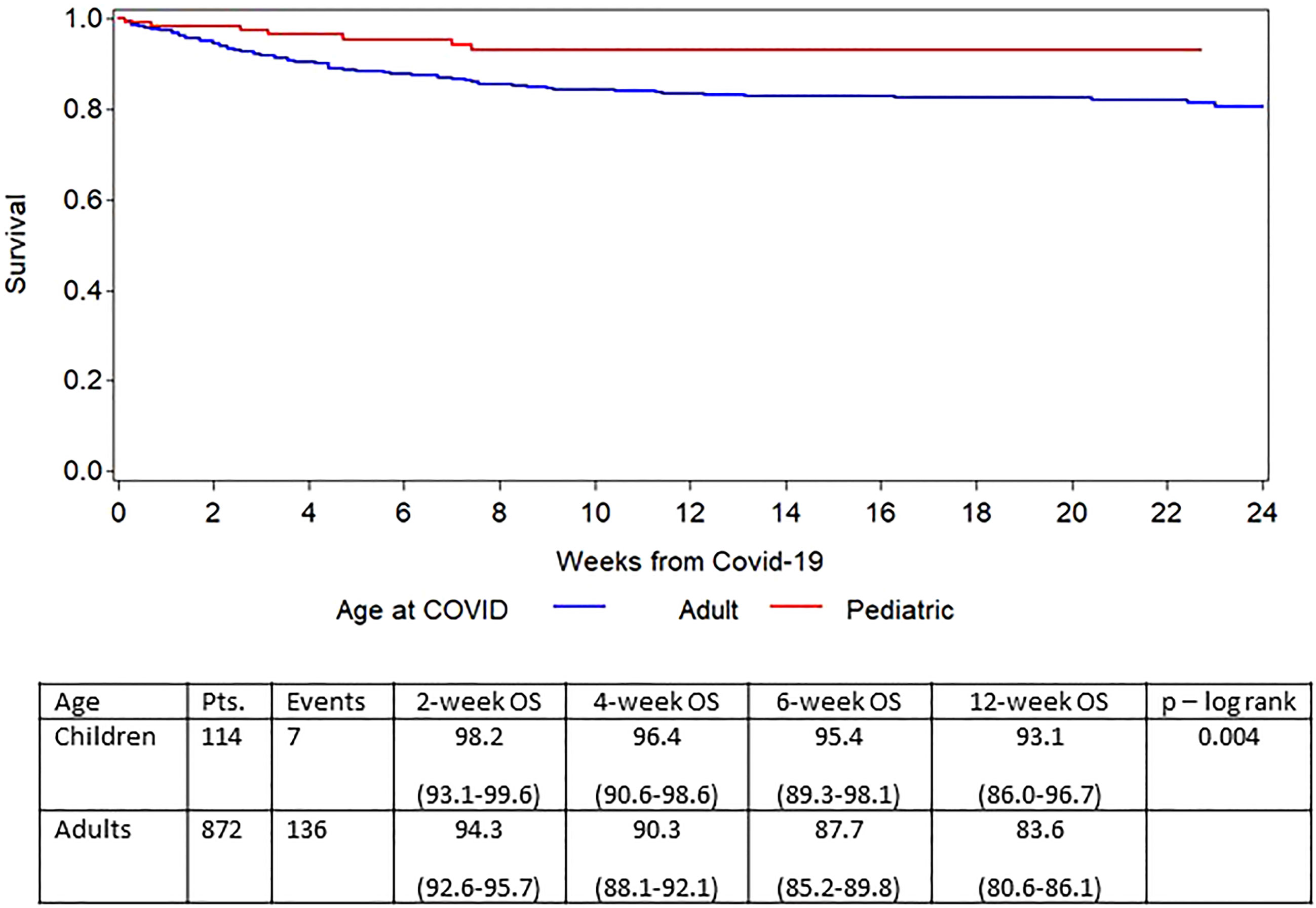
Figure 2 Survival after diagnosis of COVID-19 in adults and children.
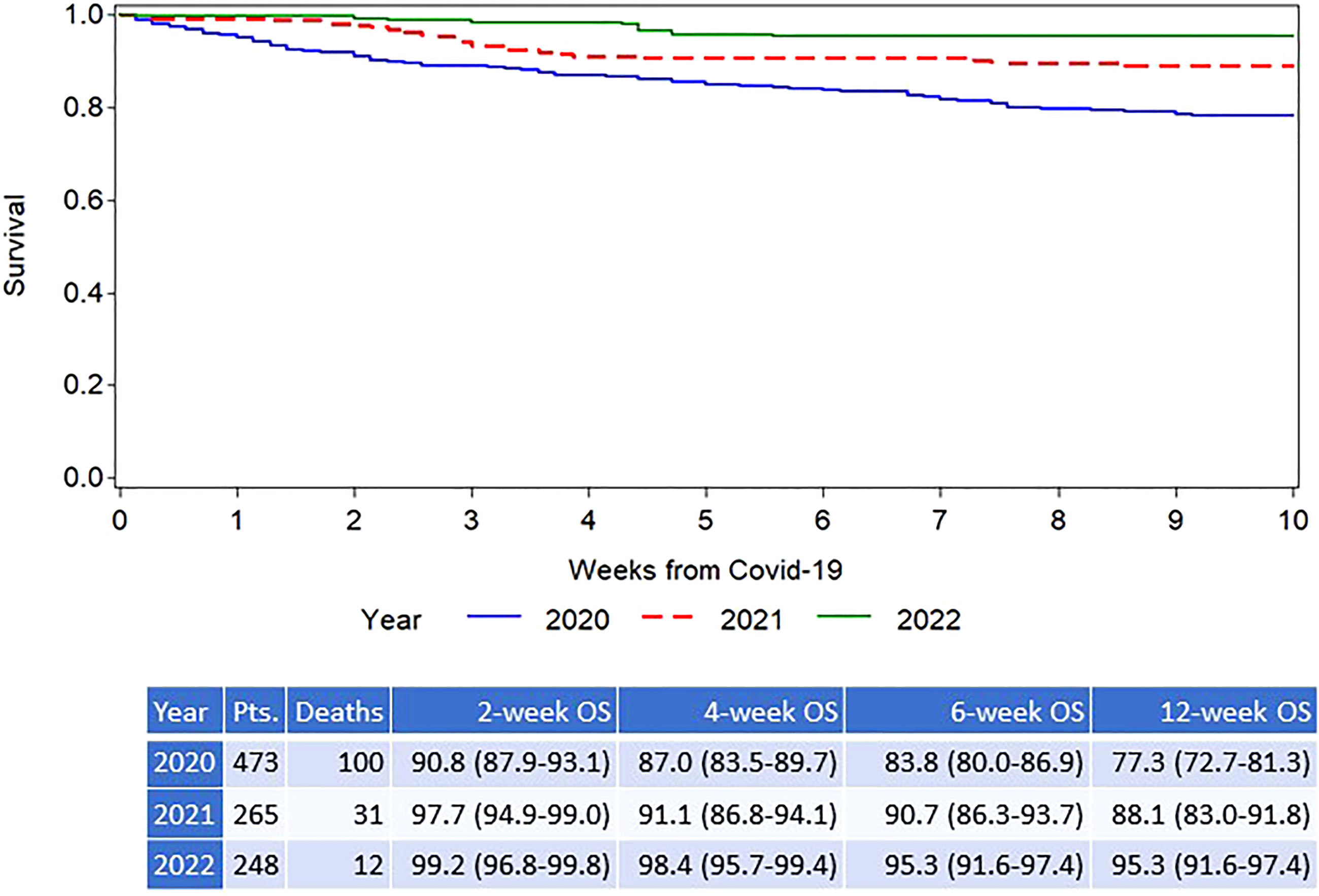
Figure 3 Overall survival after diagnosis of COVID-19 infection in allogeneic HCT recipients; split by calendar year.
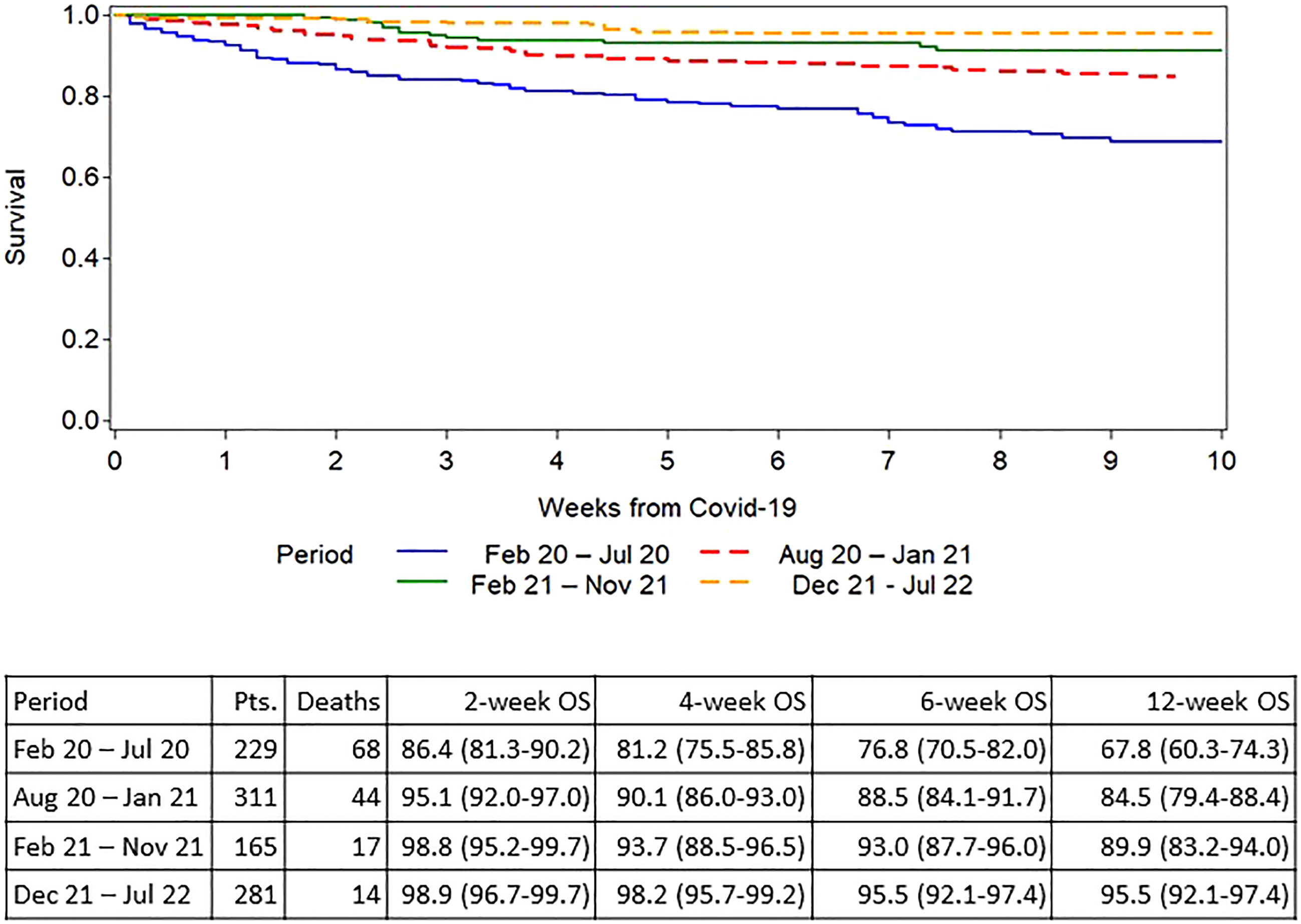
Figure 4 Overall survival after diagnosis of COVID-19 in allogeneic HCT recipients split by pandemic phase.
Univariate risk factors for survival are shown in Supplementary Table 1. Risk factors identified in multivariate analysis for overall survival are shown in Table 2. Increasing age, worse performance status at allo-HCT, contracting COVID-19 a short time after allo HCT especially during the first 30 days after HCT, ongoing immunosuppressive therapy, pre-existing lung pathology, and being CMV seropositive all had negative impact on overall survival while patients contracting COVID-19 in 2021 or 2022 had improved survival. Furthermore, ongoing corticosteroids at diagnosis of COVID-19 had also a negative impact HR 2.69 (95% CI 1.84 – 3.93) but overlapped strongly with ongoing immunosuppression and was therefore not included in the final multivariate model. In addition, we identified in univariate analysis low absolute neutrophil count <0.5 x109/L (p<.0001), and absolute lymphocyte count < 0.2 x 109/L (p<0.006) as significant risk factors. However, due to missing data, these variables could not be included in the multivariate analysis. Factors with no impact on OS in univariate analyses were patient sex, GVHD, underlying diagnosis, and country (data not shown).

Table 2 Overall survival – Multivariate analysis.
The finding that CMV seropositivity in the recipient had a negative impact prompted us to study this risk factor in detail. Figure 5 shows the Kaplan-Meier survival curves for CMV seropositive and CMV seronegative patients, respectively. The overall survival improved over time for both CMV seropositive and CMV seronegative patients but more strongly among the CMV seropositive patients (Table 3). We also looked at the effect on survival for the different donor/recipient CMV serostatus combinations. Compared to HCT with donor and recipient both seronegative as baseline, there was no impact of a negative recipient having a CMV seropositive donor and furthermore there was no additional negative effect of having a CMV seronegative donor to a CMV seropositive patient compared to both being CMV seropositive. Thus, it is the serostatus of the patient independent of the donor that mediates the negative effect.
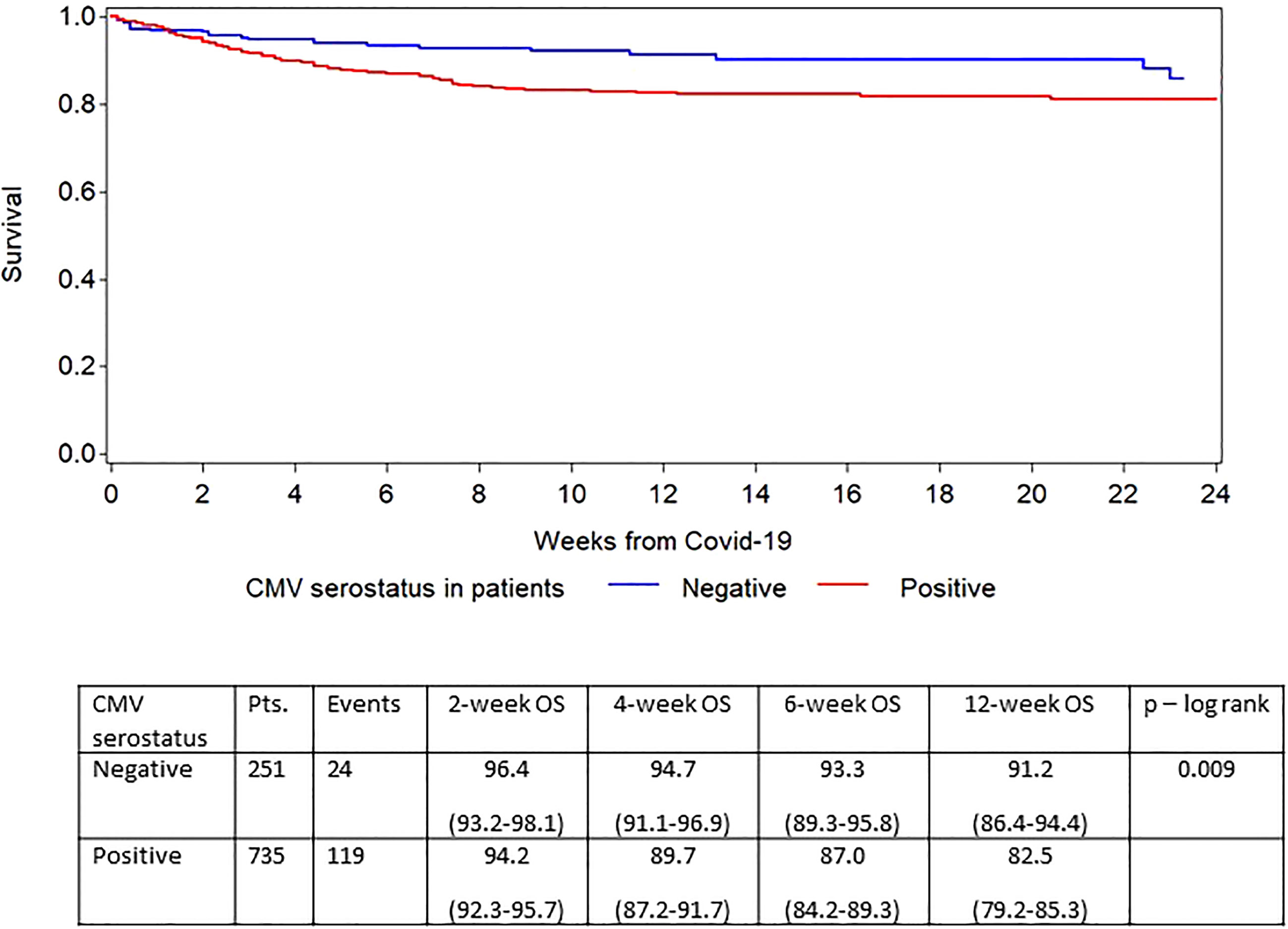
Figure 5 Survival based on recipient CMV serostatus.
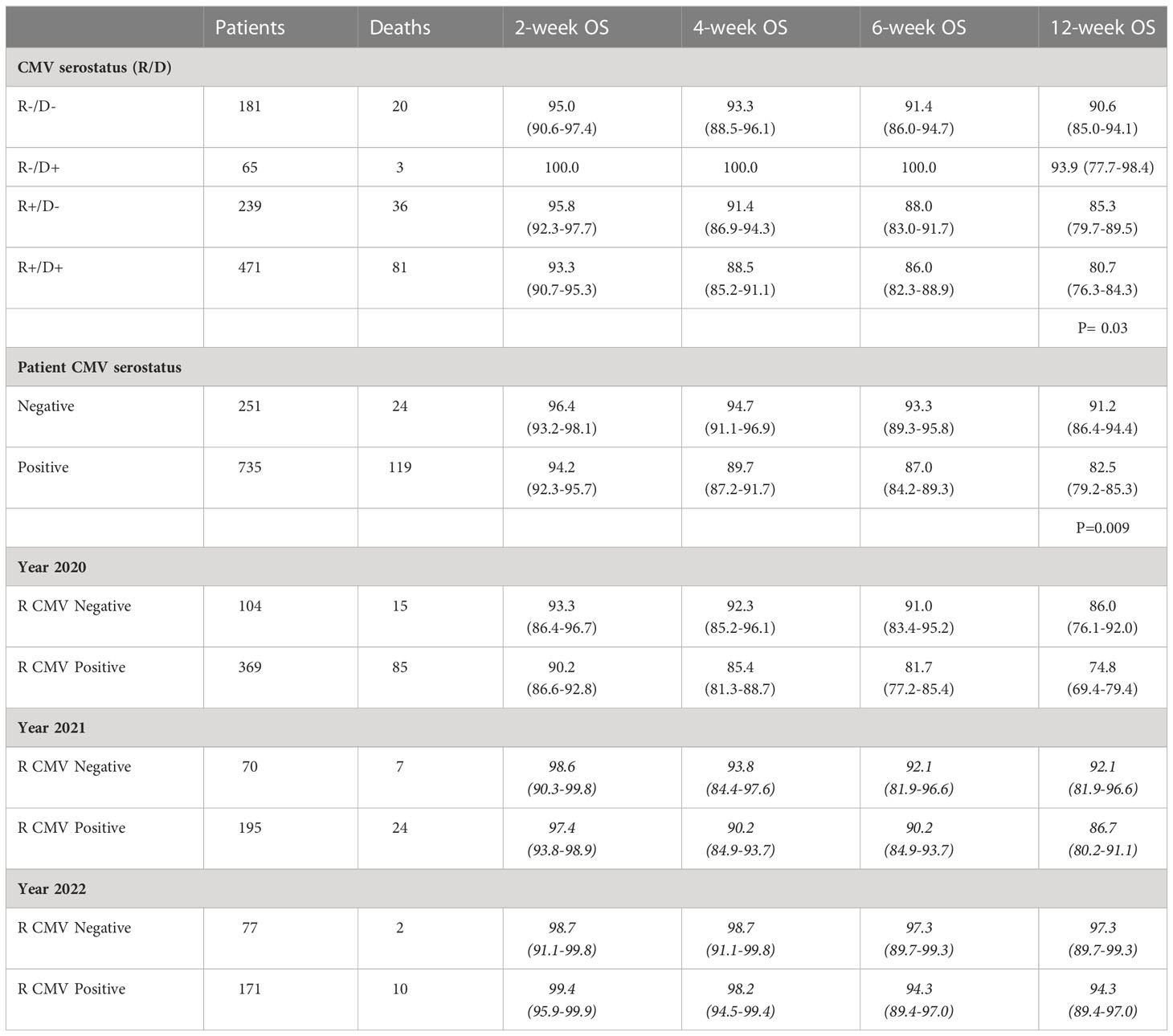
Table 3 Effect of CMV serostatus on overall survival for the different periods.
Discussion
The emergence of SARS-CoV-2 and COVID-19 has had a very strong impact on transplant patients with several reports showing high risks for morbidity and mortality especially during the first months after the emergence of the virus. In a previous report based on the EBMT registry COVID-19 resulted in an attributable mortality of 25% (2). We found a 6-week probability of survival of 77.9% and 72.1% in allogeneic and autologous HCT recipients, respectively (2). The CIBMTR published results on 314 patients (3). Their 30-day survival after diagnosis of COVID-19 was 68% among allogeneic HCT recipients and 67% among autologous HCT recipients. They found age over 50, male sex, and time from HCT to COVID-19 diagnosis of less than a year to be significant risk factors for mortality among allogeneic recipients. Other studies of HCT patients have reported similar outcomes (4–12). Since the early reports, there have been major developments especially with the introduction of vaccines and therapies of COVID-19 but also the spread of Delta and the Omicron variant including many sub-variants. This has resulted in lower mortality in patients with hematological malignancies including allogeneic HCT recipients (13–15), but no large analysis has been performed regarding risk factors and changes in outcome over time in this patient group.
In this report, including by far the largest cohort of allo-HCT recipients analysed until now, we report a successively improved outcome from the initially reported 76.8% 6-week survival to a survival of 95.% during the Omicron phase of the pandemic. Furthermore, the proportion of patients hospitalized and the proportion of patients developing lower respiratory tract disease decreased with time supporting a lower severity of SARS-CoV-2 infection over time.
The patients included in the first phase and here used as a comparator are the same as reported in our previous study (2). The way of collecting data remained the same although the CRFs have been updated to include some new variables over time especially regarding vaccination status, but it can’t be ascertained that the willingness of the centers to report was the same over time as we learned more and more about COVID-19 and its impact on allogeneic HCT recipients.
In our previous study, risk factors having significant impact on overall survival were increasing patient age and poorer performance status. These risk factors remained significant over time in the different pandemic phases and especially children and adolescents continued to do significantly better. Age has been an important factor in most reports on COVID-19 in the general population (16–18). Poor performance status is usually due to comorbidities such as extensive GVHD, but such a correlation was not found this time even in the extended cohort. New risk factors identified for fatal COVID-19 when controlled for year of COVID-19 were being infected the first 100 days and especially the first 30 days after HCT, ongoing immunosuppression, and pre-existing lung pathology. All these were expected considering the impact of other viral infections on early post-transplant morbidity and mortality.
We were surprised in our previous analysis that the time from HCT did not impact overall survival and neither did ongoing immunosuppression nor the presence of GVHD. One question was if these factors would have an impact when analysing a larger cohort and such was indeed the case in this extended cohort. Patients contracting COVID-19 the first 30 days after the HCT had a more than fivefold increase in the HR for death while there was an almost two-fold risk increase during the 30 – 100 days period compared to patients diagnosed with COVID-19 later (p<.0001). It is, however, possible that the later the patient was after transplant, the less likely it was for a patient to be reported to the study especially if the infections were mild. Thus, this effect of time might be even stronger for all SARS-CoV-2 infected allo-HCT patients than what we found. In addition, ongoing immune suppression was also an independent negative factor for survival and immunosuppression is given mostly to patients quite early after HCT. Another possible influencing factor is that patients respond poorly to vaccination performed early after HCT (19–22). All this taken together supports the need for protecting the most vulnerable patients from becoming infected. This high mortality in patients early after transplantation clearly supports the necessity for continued vigilance in the infection control efforts at hospitals performing allo-HCT in particular keeping transplant units as far as possible free from COVID-19 for example by systematic PCR screening and early antiviral therapy.
We also found that CMV serostatus impacted on the risk for dying within 6-weeks after contracting SARS-CoV-2 infection. CMV seropositivity has been reported to increase the risk for hospitalization in patients infected with SARS-CoV-2 (23). Furthermore, CMV seropositivity has been proposed as one possible reason for the severe impact of COVID-19 in the elderly and lower impact in children (24, 25). CMV is a major pathogen after allogeneic HCT and seropositive patients have a decreased overall survival rate and an increased risk of non-relapse mortality after allogeneic HCT (26, 27). CMV can also influence many different immune system functions including those of NK-cells and T cells. We found in this analysis that CMV serostatus has an independent negative effect on overall survival when corrected for other risk factors including year of SARS-CoV-2 infection adding to existing data about the negative effect of CMV on the seriousness of COVID-19. The negative impact existed over time although the survival improved over time in both seropositive and CMV seronegative recipients. Recently Perera et al. showed that patients with severe COVID-19 had higher levels of CMV-specific IgG at the time of COVID-19 (28). Furthermore, they showed in an in vitro study that CMV increases the number of cells infected by SARS-CoV-2 and upregulates the SARS-CoV-2 receptor ACE2, the SARS-CoV-2 cell entry receptor. It is possible that the negative effect is through local CMV replication in the airways We don’t have information on either letermovir prophylaxis or CMV reactivations so we can only speculate about the effects of possible interventions.
We could not find an independent effect of donor serostatus although the number of CMV seronegative patients having received grafts from CMV seropositive individuals was low and even fewer such patients were infected with SARS-CoV-2 during the most vulnerable early period.
The design of this study does not allow to look at the possible protective effects of vaccination since patients fully protected against infection would not have been reported to our registry. However, the rate of fatal COVID-19 among fully vaccinated patients was only 1% strongly supporting high effectiveness against severe COVID-19. This is in agreement with a previous report showing that additional doses of vaccine can improve outcome in patients with hematological malignancies (13). As could be expected, the proportion of patients treated with either monoclonal antibodies or antiviral agents increased with time and this can have improved the outcome of COVID-19.
We conclude that the mortality in and severity of COVID-19 have decreased over time during the pandemic. We have identified several risk factors for mortality including the previously known age and comorbidity. Newly identified risk factors are short time after allogeneic HCT, ongoing immunosuppression, and interestingly CMV seropositive patient status. Additional studies have to be performed to investigate the role of CMV reactivation in outcome of COVID-19
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material. A request can be made to the chairperson of the Infectious Diseases Working Party of the EBMT. Requests to access the datasets should be directed toaWR3cGVibXRAbHVtYy5ubA==.
Ethics statement
The studies involving human participants were reviewed and approved by Swedish Ethics Review Authority. Written informed consent for their data to be reported to the EBMT registry was provided by each participant or their legal guardian.
Author contributions
PL, RC, JLP, JS, MM designed the study and worked as a writing committee. GT is the study statistician. NKn managed the registry data. NKr, DA, SC critically reviewed the manuscript. All other authors submitted cases to the study and critically reviewed the manuscript. All authors contributed to the article and approved the submitted version.
Acknowledgments
The study was performed in collaboration with the Spanish Group of Hematopoietic Stem Cell Transplantation (GETH). We are also grateful to all physicians, nurses, and other staff treating these patients under very challenging circumstances and still being able to help with providing data for this manuscript.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2023.1125824/full#supplementary-material
References
1. Spanjaart AM, Ljungman P, de la Camara R, Tridello G, Ortiz-Maldonado V, Urbano-Ispizua A, et al. Poor outcome of patients with COVID-19 after CAR T-cell therapy for b-cell malignancies: Results of a multicenter study on behalf of the European society for blood and marrow transplantation (EBMT) infectious diseases working party and the European hematology association (EHA) lymphoma group. Leukemia (2021) 35(12):3585–8. doi: 10.1038/s41375-021-01466-0
2. Ljungman P, de la Camara R, Mikulska M, Tridello G, Aguado B, Zahrani MA, et al. COVID-19 and stem cell transplantation; results from an EBMT and GETH multicenter prospective survey. Leukemia (2021) 35(10):2885–94. doi: 10.1038/s41375-021-01302-5
3. Sharma A, Bhatt NS, St Martin A, Abid MB, Bloomquist J, Chemaly RF, et al. Clinical characteristics and outcomes of COVID-19 in haematopoietic stem-cell transplantation recipients: An observational cohort study. Lancet Haematol (2021) 8(3):e185–e93. doi: 10.1016/S2352-3026(20)30429-4
4. Saraceni F, Scortechini I, Mancini G, Mariani M, Federici I, Gaetani M, et al. Severe COVID-19 in a patient with chronic graft-versus-host disease after hematopoietic stem cell transplant successfully treated with ruxolitinib. Transplant Infect Dis (2021) 23(1):e13401. doi: 10.1111/tid.13401
5. Vicent MG, Martinez AP, Trabazo Del Castillo M, Molina B, Sisini L, Moron-Cazalilla G, et al. COVID-19 in pediatric hematopoietic stem cell transplantation: The experience of Spanish group of transplant (GETMON/GETH). Pediatr Blood cancer. (2020) 67(9):e28514. doi: 10.1002/pbc.28514
6. Gampel B, Troullioud Lucas AG, Broglie L, Gartrell-Corrado RD, Lee MT, Levine J, et al. COVID-19 disease in new York city pediatric hematology and oncology patients. Pediatr Blood cancer. (2020) 67(9):e28420. doi: 10.1002/pbc.28420
7. Kanellopoulos A, Ahmed MZ, Kishore B, Lovell R, Horgan C, Paneesha S, et al. COVID-19 in bone marrow transplant recipients: Reflecting on a single centre experience. Br J haematol (2020) 190(2):e67–70. doi: 10.1111/bjh.16856
8. Malard F, Genthon A, Brissot E, van de Wyngaert Z, Marjanovic Z, Ikhlef S, et al. COVID-19 outcomes in patients with hematologic disease. Bone Marrow Transplant. (2020) 55(11):2180–4. doi: 10.1038/s41409-020-0931-4
9. He W, Chen L, Chen L, Yuan G, Fang Y, Chen W, et al. COVID-19 in persons with haematological cancers. Leukemia (2020) 34(6):1637–45. doi: 10.1038/s41375-020-0836-7
10. Martin-Moro F, Marquet J, Piris M, Michael BM, Saez AJ, Corona M, et al. Survival study of hospitalised patients with concurrent COVID-19 and haematological malignancies. Br J haematol (2020) 190(1):e16–20. doi: 10.1111/bjh.16801
11. Shah GL, DeWolf S, Lee YJ, Tamari R, Dahi PB, Lavery JA, et al. Favorable outcomes of COVID-19 in recipients of hematopoietic cell transplantation. J Clin Invest. (2020) 130(12):6656–67. doi: 10.1172/JCI141777
12. Coll E, Fernandez-Ruiz M, Sanchez-Alvarez JE, Martinez-Fernandez JR, Crespo M, Gayoso J, et al. COVID-19 in transplant recipients: The Spanish experience. Am J Transplant (2020). 21(5):1825–1837 10.1111/ajt.16369
13. Salmanton-Garcia J, Marchesi F, Glenthoj A, Bilgin YM, van Praet J, Davila-Valls J, et al. Improved clinical outcome of COVID-19 in hematologic malignancy patients receiving a fourth dose of anti-SARS-CoV-2 vaccine: An EPICOVIDEHA report. Hemasphere (2022) 6(11):e789. doi: 10.1097/HS9.0000000000000789
14. Pagano L, Salmanton-Garcia J, Marchesi F, Blennow O, Gomes da Silva M, Glenthoj A, et al. Breakthrough COVID-19 in vaccinated patients with hematologic malignancies: results from EPICOVIDEHA survey. Blood (2022) 140(26): 2773–2787 doi: 10.1182/blood.2022017257
15. Blennow O, Salmanton-Garcia J, Nowak P, Itri F, Van Doesum J, Lopez-Garcia A, et al. Outcome of infection with omicron SARS-CoV-2 variant in patients with hematological malignancies: An EPICOVIDEHA survey report. Am J hematol (2022) 97(8):E312–E7. doi: 10.1002/ajh.26626
16. Epidemiology Working Group for Ncip Epidemic Response CCfDC, Prevention. [The epidemiological characteristics of an outbreak of 2019 novel coronavirus diseases (COVID-19) in China]. Zhonghua Liu Xing Bing Xue Za Zhi (2020) 41(2):145–51. doi: 10.3760/cma.j.issn.0254-6450.2020.02.003
17. Zhou F, Yu T, Du R, Fan G, Liu Y, Liu Z, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in wuhan, China: A retrospective cohort study. Lancet (2020) 395(10229):1054–62. doi: 10.1016/S0140-6736(20)30566-3
18. Ciceri F, Castagna A, Rovere-Querini P, De Cobelli F, Ruggeri A, Galli L, et al. Early predictors of clinical outcomes of COVID-19 outbreak in Milan, Italy. Clin Immunol (2020) 217:108509. doi: 10.1016/j.clim.2020.108509
19. Bergman P, Blennow O, Hansson L, Mielke S, Nowak P, Chen P, et al. Safety and efficacy of the mRNA BNT162b2 vaccine against SARS-CoV-2 in five groups of immunocompromised patients and healthy controls in a prospective open-label clinical trial. EBioMedicine (2021) 74:103705. doi: 10.1016/j.ebiom.2021.103705
20. Redjoul R, Le Bouter A, Beckerich F, Fourati S, Maury S. Antibody response after second BNT162b2 dose in allogeneic HSCT recipients. Lancet (2021) 398(10297):298–9. doi: 10.1016/S0140-6736(21)01594-4
21. Ram R, Hagin D, Kikozashvilli N, Freund T, Amit O, Bar-On Y, et al. Safety and immunogenicity of the BNT162b2 mRNA COVID-19 vaccine in patients after allogeneic HCT or CD19-based CART therapy-a single-center prospective cohort study. Transplant Cell Ther (2021) 27(9):788–94. doi: 10.1016/j.jtct.2021.06.024
22. Pinana JL, Lopez-Corral L, Martino R, Montoro J, Vazquez L, Perez A, et al. SARS-CoV-2-reactive antibody detection after SARS-CoV-2 vaccination in hematopoietic stem cell transplant recipients: Prospective survey from the Spanish hematopoietic stem cell transplantation and cell therapy group. Am J hematol (2022) 97(1):30–42. doi: 10.1002/ajh.26385
23. Alanio C, Verma A, Mathew D, Gouma S, Liang G, Dunn T, et al. Cytomegalovirus latent infection is associated with an increased risk of COVID-19-related hospitalization. J Infect Dis (2022). 226(3):463–473 doi: 10.1093/infdis/jiac020
24. Zimmermann P, Curtis N. Why is COVID-19 less severe in children? a review of the proposed mechanisms underlying the age-related difference in severity of SARS-CoV-2 infections. Arch Dis childhood (2021). 106(5): 429–439 doi: 10.1136/archdischild-2020-320338
25. Moss P. "The ancient and the new": is there an interaction between cytomegalovirus and SARS-CoV-2 infection? Immun Ageing (2020) 17:14. doi: 10.1186/s12979-020-00185-x
26. Green ML, Leisenring W, Xie H, Mast TC, Cui Y, Sandmaier BM, et al. Cytomegalovirus viral load and mortality after haemopoietic stem cell transplantation in the era of pre-emptive therapy: A retrospective cohort study. Lancet Haematol (2016) 3(3):e119–27. doi: 10.1016/S2352-3026(15)00289-6
27. Schmidt-Hieber M, Tridello G, Ljungman P, Mikulska M, Knelange N, Blaise D, et al. The prognostic impact of the cytomegalovirus serostatus in patients with chronic hematological malignancies after allogeneic hematopoietic stem cell transplantation: a report from the infectious diseases working party of EBMT. Ann hematol (2019) 98(7):1755–63. doi: 10.1007/s00277-019-03669-z
Keywords: COVID-19, allogeneic, stem cell transplantation, CMV, risk factors
Citation: Ljungman P, Tridello G, Piñana JL, Ciceri F, Sengeloev H, Kulagin A, Mielke S, Yegin ZA, Collin M, Einardottir S, Lepretre SD, Maertens J, Campos A, Metafuni E, Pichler H, Folber F, Solano C, Nicholson E, Yüksel MK, Carlson K, Aguado B, Besley C, Byrne J, Heras I, Dignan F, Kröger N, Robin C, Khan A, Lenhoff S, Grassi A, Dobsinska V, Miranda N, Jimenez M-J, Yonal-Hindilerden I, Wilson K, Averbuch D, Cesaro S, Xhaard A, Knelange N, Styczynski J, Mikulska M and de la Camara R (2023) Improved outcomes over time and higher mortality in CMV seropositive allogeneic stem cell transplantation patients with COVID-19; An infectious disease working party study from the European Society for Blood and Marrow Transplantation registry. Front. Immunol. 14:1125824. doi: 10.3389/fimmu.2023.1125824
Received: 16 December 2022; Accepted: 22 February 2023;
Published: 07 March 2023.
Edited by:
Jeff Szer, Royal Melbourne Hospital, AustraliaReviewed by:
Thomas Luft, Heidelberg University Hospital, GermanyShigeo Fuji, Osaka International Cancer Institute, Japan
Copyright © 2023 Ljungman, Tridello, Piñana, Ciceri, Sengeloev, Kulagin, Mielke, Yegin, Collin, Einardottir, Lepretre, Maertens, Campos, Metafuni, Pichler, Folber, Solano, Nicholson, Yüksel, Carlson, Aguado, Besley, Byrne, Heras, Dignan, Kröger, Robin, Khan, Lenhoff, Grassi, Dobsinska, Miranda, Jimenez, Yonal-Hindilerden, Wilson, Averbuch, Cesaro, Xhaard, Knelange, Styczynski, Mikulska and de la Camara. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Per Ljungman, UGVyLkxqdW5nbWFuQGtpLnNl