 Maierhaba Maitiyaer1†
Maierhaba Maitiyaer1† Jingyu Zhang2†
Jingyu Zhang2† Peiyi Li3†
Peiyi Li3† Dingwen Jiang4
Dingwen Jiang4 Huangdong Li2
Huangdong Li2 Zeying Lin1Ziguan Ye1
Zeying Lin1Ziguan Ye1 Yongbao Huo1
Yongbao Huo1 Wenhui Huang1Li Wang2
Wenhui Huang1Li Wang2 Zhiping Liu2*
Zhiping Liu2* Shuilian Yu1*
Shuilian Yu1*- 1Department of Rheumatology, The Second Affiliated Hospital, Guangzhou Medical University, Guangzhou, Guangdong, China
- 2Ophthalmic Center, The Second Affiliated Hospital, Guangzhou Medical University, Guangzhou, Guangdong, China
- 3Department of Rheumatology, Liwan Central Hospital of Guangzhou, Guangzhou, Guangdong, China
- 4Department of Clinical Medicine, The Second School of Clinical Medicine, Guangzhou Medical University, Guangzhou, Guangdong, China
Background: Systemic lupus erythematosus (SLE) and lupus nephritis (LN) are associated with retinal microvascular changes that may reflect disease severity. This study aimed to evaluate differences in retinal vascular density (VD) between SLE patients with and without LN and assess the impact of rheumatological treatments on VD.
Methods: A cross-sectional study was conducted with 54 SLE patients (21 with LN, 33 without LN). Retinal VD was measured using optical coherence tomography angiography (OCTA), focusing on superficial and deep capillary plexus VD (SCP-VD and DCP-VD). The impact of Belimumab and other treatments was analyzed. Linear regression assessed the effects of LN status and treatments on DCP parafoveal VD. Lymphocyte subsets and cytokines were compared before and after Belimumab treatment.
Result: LN patients showed significantly reduced macular vascular density compared with non-LN patients. Belimumab treatment (≥8 times) and hydroxychloroquine use (>5 years) were independently associated with lower DCP-VD, particularly in parafoveal areas. Cumulative doses of HCQ and glucocorticoids negatively correlated with VD. Linear regression showed a significant negative association between Belimumab treatment and parafoveal DCP-VD. Notably, Belimumab treatment led to reductions in serum CD19+ B cells and IL-10 levels.
Conclusions: LN patients demonstrated distinct retinal microvascular alterations. Long-term Belimumab and HCQ treatments were associated with decreased retinal VD. Regular retinal health monitoring was recommended to prevent microvascular complications in SLE patients undergoing prolonged treatment.
1 Introduction
Ocular manifestations are observed in approximately 30% of systemic lupus erythematosus (SLE) patients, affecting various ocular structures. These ocular lesions, including lupus retinopathy and lupus-associated optic neuropathy, contribute to vision loss and serve as important indicators of SLE disease activity (1, 2). Early detection of preclinical retinal microvascular and microstructural alterations is crucial for preventing irreversible ocular and systemic complications and predicting prognosis (1, 3, 4).
Optical coherence tomography angiography (OCTA) is a non-invasive technology that enables high-resolution visualization of retinal vasculature, providing valuable insights into retinal vascular pathologies (5). Previous studies have shown that peripapillary retinal nerve fiber layer (RNFL) thickness and ganglion cell layer (GCL) thickness were vital parameters for glaucoma follow-up, reflecting prognosis and disease severity (6). Additionally, SLE patients exhibit thinning of the RNFL and GCL, suggesting neurodegeneration and early cognitive impairment (7).
OCTA has also revealed reductions in macular vessel density (VD) and foveal avascular zone (FAZ) area size in SLE patients without retinopathy, indicating microvasculature alterations even before ocular involvement. Furthermore, reduced retinal capillary vessel density has been observed in SLE patients with lupus nephritis (LN), suggesting potential early systemic vascular involvement (1, 8, 9). Recently, in our cross-sectional investigation (10), we utilized OCTA to image the microvasculature of the retina. Notable reductions in macular vessel density were observed, specifically within the superficial capillary plexus (SCP), among SLE patients without retinopathy compared to controls (10). These findings highlight the potential role of OCTA as a non-invasive tool for the early detection of systemic vascular changes and associated kidney impairment in lupus patients (3, 11).
It is well known that hydroxychloroquine (HCQ), a commonly used treatment for SLE, can lead to retinal toxicity by binding to melanin in retinal pigment epithelium (RPE) cells (12). This leads to disruptions in retinal cell metabolism and damage to the photoreceptors and outer nuclear layer of the retina (13, 14). Early detection of HCQ-induced retinopathy before RPE cell damage occurs is crucial for preserving vision, as the condition is irreversible and may lead to blindness.
As the number of biological treatment options continues to grow in the field of SLE therapy, there is a growing interest in investigating the effects of these medications on ocular health. Despite the growing body of research on ocular involvement in SLE, the effects of newer biological treatments, such as Belimumab, on ocular health remain largely unexplored.
Belimumab, a recombinant human IgG-1λ monoclonal antibody that inhibits B-cell activating factor, is approved for treating active autoantibody-positive SLE patients (15). It is part of the standard treatment for SLE and LN according to the European League Against Rheumatism (EULAR) 2023 guidelines (16). Recent research has demonstrated that Belimumab holds promise in the treatment of Graves’ Ophthalmopathy (GO) (17, 18). However, there is currently no research indicating its effects on the ocular vasculature of SLE patients.
The objective of this study is to conduct a detailed evaluation of ocular involvement in SLE and LN patients and investigate the influence of Belimumab on retinal microvascular density in these individuals.
2 Materials and methods
2.1 Patients
A total of 54 female patients with SLE from the Second Affiliated Hospital of Guangzhou Medical University were enrolled between September 2019 and October 2023. All SLE patients were diagnosed according to the 2019 EULAR/ACR classification criteria for SLE (19). 21 of the 54 patients included in the study met the diagnostic criteria for LN (20). SLE disease activity was evaluated utilizing the systemic lupus erythematosus disease activity index (SLEDAI)-2K score (21). In the study of Belimumab’s therapeutic effects, we included patients who had received Belimumab ≥8 times for the Belimumab treatment group, consistent with the dosing regimen used in the BLISS-LN trial (15). This cutoff corresponds to 24 weeks of treatment, which is generally sufficient to observe therapeutic effects.The ocular inclusion criteria were defined as follows: (1) best-corrected visual acuity better than 0.1 LogMAR; (2) intraocular pressure < 21 mmHg; (3) spherical equivalent < +2.5 D or > -6.0 D. Exclusion criteria encompassed SLE patients presenting with acute infections, malignancies, and other inflammatory diseases. We also excluded those treated with other biologic agents. The ocular exclusion criteria were defined as follows: (1) spherical equivalent > +6.0 D or <-6.0 D; (2) axial length ≥26 mm; (3) any ocular pathological changes detected on slit lamp, fundus color photography, or optical coherence tomography imaging; (4) history of previous ocular diseases such as glaucoma, cataract or ocular surgery, including refractive surgeries. In cases where both eyes fulfilled the inclusion criteria, data analysis was conducted on the right eye of each participant to prevent any potential bias that could result from the correlation between both eyes of the same individual. Informed consent was obtained from all participants, and the study received approval from the Ethics Committee of the Second Affiliated Hospital of Guangzhou Medical University.
2.2 Clinical and laboratory data and rheumatological treatment
Demographic data, clinical manifestations, and laboratory data were retrieved from the medical records of patients. Patient characteristics encompassed gender, age, disease duration, SLEDAI score, anti ds-DNA antibody positivity, C3, C4, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), albumin, creatinine, glomerular filtration rate (GFR), 24-hour proteinuria and anticardiolipin antibodies(ACL IgG, ACL IgA, ACL IgM, and anti-beta-2 glycoprotein I antibodies, Anti-β2GPI). We also collected data on the usage of Belimumab, HCQ, prednisolone, methotrexate(MTX), cyclophosphamide, mycophenolate mofetil(MMF), cyclophosphamid, cyclosporin A, FK506 in the included patients.
2.3 Ophthalmologic evaluation
Every participant in the study received a comprehensive ophthalmological examination, which included best corrected visual acuity (BCVA), air puff intraocular pressure measurement (IOP), and OCTA examination. A standard LogMAR chart was used to evaluate BCVA in individual eyes for central visual acuity assessment following the Early Treatment of Diabetic Retinopathy Study (ETDRS) protocol (22). The evaluation incorporated the relevant macular and optic disc parameters. OCTA was used to measure RNFL thickness, GCL thickness, SCP-VD(%), and vessel length density (VLD)(%) (Figure 1). Similarly, the identical method was used to measure deep capillary plexus vessel density (DCP-VD) (%) and VLD (%). The FAZ area (mm2) and perimeter (mm) for both groups were also evaluated. Regarding the region of interest for analysis, the macular region was a circular region centered on the macula with a diameter of 1 mm and 2.5 mm respectively. The optic disc area was a circular region centered on the optic disc, with diameters of 1.5 mm, 2.5 mm, 3.5 mm, and 5 mm respectively. Parafoveal refers to the macular area 0.5–1.5 mm from the foveal center, and peripapillary denotes the optic disc region surrounding the optic nerve head. Macular VD was calculated using the ratio of flow pixels to total pixels. Macular VLD was calculated through the ratio of vessel length to total area. FAZ area and perimeter were calculated through manual delineation of the macular central avascular zone. The whole image corresponded to the complete 3 x 3 mm2 area centered on the macula or the entire 6 x 6 mm2 area centered on the optic disc. The analysis of OCTA images was performed using ImageJ software (https://imagej.net/Fiji; NIH, Bethesda, MD) following established quantification protocols (23, 24).
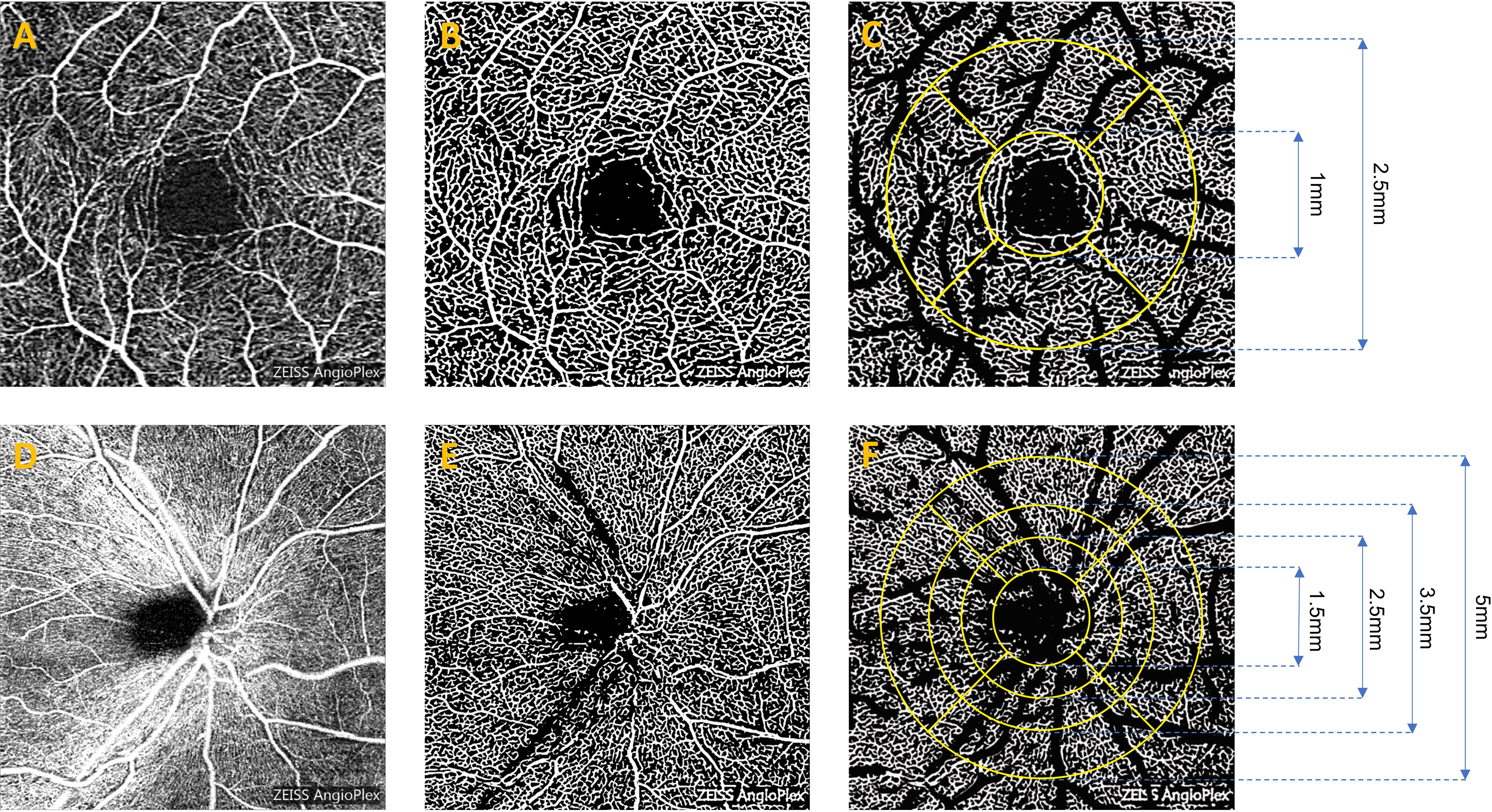
Figure 1. Representative OCTA images for measuring retinal microvasculature parameters in SCP. The original OCTA image revealed macular vessels (A) and peripapillary vessels (D). The binarized image highlighted macular vessels (B) and peripapillary vessels (E). After the removal of large vessels, the image displayed macular vessels (C) and peripapillary vessels (F), which were then used to measure the corresponding subregions. OCTA, Optical Coherence Tomography Angiography; SCP, Superficial Capillary Plexus.
2.4 Statistical analysis
SPSS software (version 25.0), R Statistical Software (http://www.R-project.org, The R Foundation), and Free Statistics analysis platform were used for analysis. The normality of data was assessed using the Shapiro-Wilk test. Normally distributed continuous variables are presented as mean ± standard deviation and compared using the independent t-test. Non-normally distributed variables are presented as median (interquartile range) and compared using the Mann-Whitney U test. Categorical data are expressed as frequencies and analyzed using the chi-square test. For small samples, Fisher’s exact test was applied. Pearson’s correlation coefficient was used to assess linear relationships between normally distributed continuous variables, while Spearman’s rank correlation was used for non-normally distributed continuous and categorical variables. Multiple linear regression analysis was used to identify factors associated with reduced vascular density. No formal correction for multiple comparisons was applied due to the exploratory nature of the study and the potential risk of Type II errors. Statistical significance was defined as P < 0.05.
3 Results
3.1 Baseline characteristics of LN and non-LN patients
Twenty-one SLE patients with LN and 33 SLE patients without LN were recruited in this cross-sectional study. All the collected data regarding patients’ characteristics, SLE activity, and treatment are summarized in Table 1. No statistically significant differences were observed between the two groups in terms of age, gender, disease duration, SLEDAI score, anti ds-DNA antibody positivity, ESR, CRP, C3, C4, albumin, creatinine, GFR, and anticardiolipin antibodies (all P>0.05). LN patients exhibited a notable elevation in 24-hour urine protein levels compared to non-LN patients (961.0mg/d vs. 114.7mg/d, P<0.001). Additionally, there were no significant differences observed in visual acuity and IOP between the two groups of patients. We analyzed two groups of patients receiving rheumatological treatment. Our study results suggested that a higher proportion of patients with LN use prednisolone (90.5% vs 66.7%), MMF(76.1% vs 42.4%), and Belimumab (71.4% vs 36.4%) compared to patients with non-LN. (all P<0.05) (Table 1).
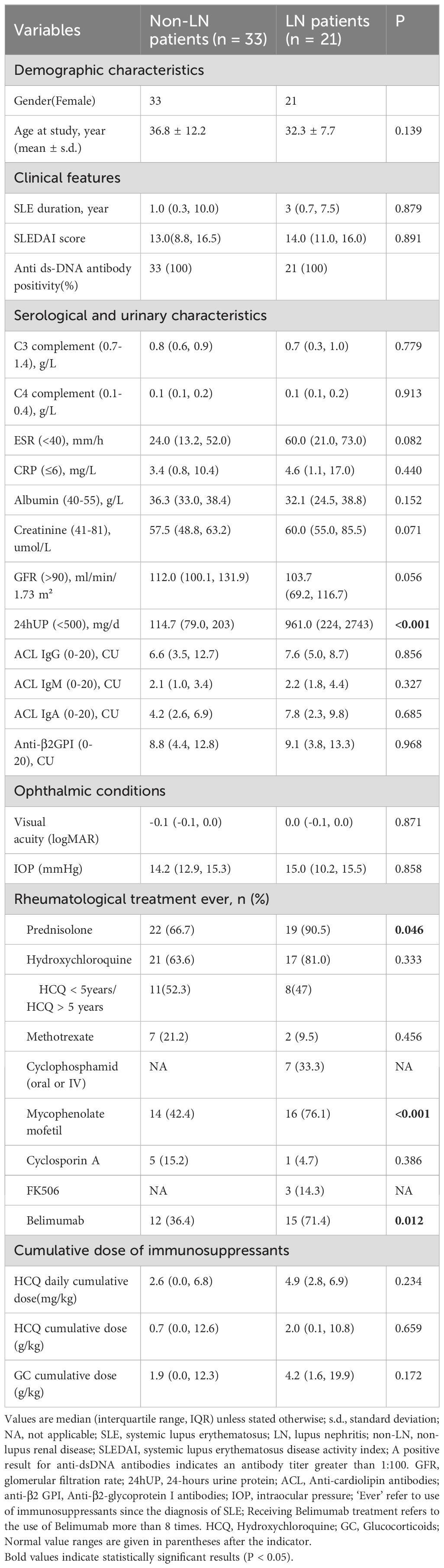
Table 1. Demographic and clinical characteristics in SLE patients with and without LN.
3.2 Retinal microvascular assessment by OCTA
3.2.1 Retinal microvascular differences between LN and Non-LN patients
3.2.1.1 Retinal nerve fiber layer thickness and ganglion cell layer thickness
Our findings did not show any significant difference in the thickness of the RNFL and GCL between the LN and non-LN groups. (all P>0.05, Supplementary Table S1).
3.2.1.2 Superficial and deep capillary density in different areas of the macula
LN patients exhibited diminished superficial vasculature density (SCP-VD) in various regions, encompassing the loop, superior side, temporal side, and whole image region (all P<0.05). Additionally, a notable reduction in superficial vascular length density (SCP-VLD) was observed in the temporal side of LN patients (Table 2, Figure 2).

Table 2. Comparison of macular and optic disc vascular density and vessel length density between SLE patients with and without LN.
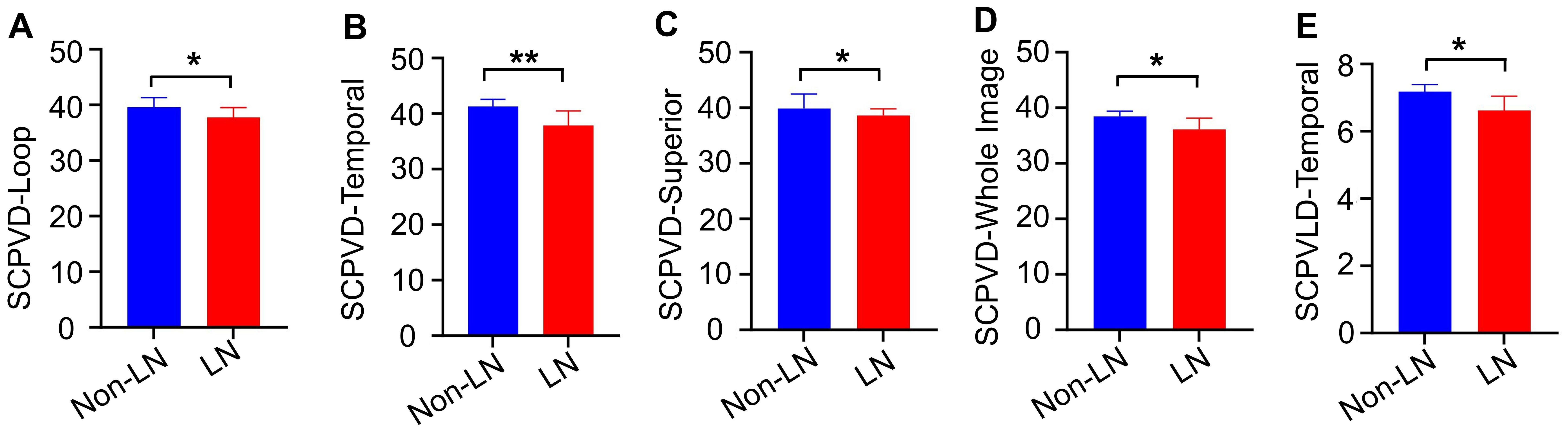
Figure 2. Comparative analysis of retinal microvascular density and vessel length density between LN patients and non-LN patients. We found that compared to non-LN patients, LN patients had lower vessel densities in superficial capillary plexus (SCP-VD)in the loop (A), temporal (B), superior (C), and the whole image (D) areas, as well as lower superficial capillary plexus vessel length density (SCP-VLD) in the temporal area (E). LN, lupus nephritis;*P<0.05, **P<0.01.
3.2.1.3 Foveal avascular zone parameters
A comparative analysis of FAZ parameters was undertaken between patients with LN and those without LN. Nevertheless, no statistically significant differences were identified in either FAZ area or FAZ circle measurements between the two groups (all P>0.05, Table 2).
3.2.1.4 Superficial and deep capillary density in different areas of the optic disc
Patients with LN exhibited elevated SCP-VD in the optic disc region, notably within the 1.5mm circle and temporal side of the inner circle (all P<0.05) (Table 2).
3.2.2 Correlation of vascular parameters with clinical indicators
Our results showed that age, CRP, SLEDAI score and 24-hour urine protein were negatively correlated with VD on multiple sides (Supplementary Table S2).
3.2.3 Retinal vascular changes associated with rheumatological treatments
3.2.3.1 Belimumab
We investigated the vascular density of the superficial and deep capillary plexuses in SLE patients who either used(≥ 8 times) or did not use Belimumab. Notably, our analysis showed that patients who received Belimumab for more than 8 times showed a significant decrease in DCP-VD, particularly in the superior side of the inter circle(19.7 vs 23.0; P=0.023) (Table 3).
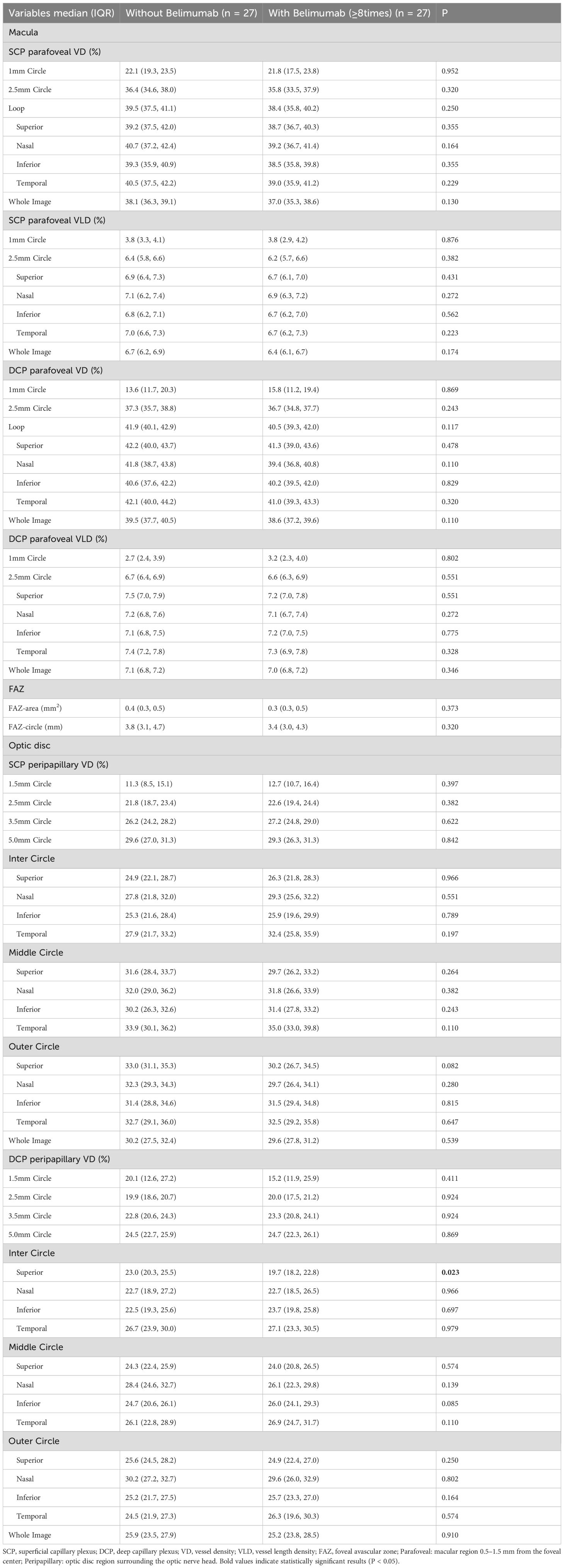
Table 3. Comparison of macular and optic disc vascular density and vessel length density among SLE patients using Belimumab.
3.2.3.2 Hydroxychloroquine
We also evaluated vascular density in the superficial and deep capillary plexuses of SLE patients based on HCQ treatment. In the macular region, SLE patients using HCQ for over 5 years showed significantly lower DCP-VD, particularly in the 1mm circle (12.3 vs. 17.1; P=0.029), 2.5mm circle (35.6 vs. 37.4; P=0.019), loop (39.9 vs. 41.9; P=0.016), and whole image area (38.1 vs. 39.5; P=0.019). DCP-VLD was also reduced in these patients at the 1mm circle (2.5 vs. 3.5; P=0.036), 2.5mm circle (6.4 vs. 6.7; P=0.025), and whole image areas(6.8 vs. 7.1; P=0.028) (Table 4).

Table 4. Comparison of macular and optic disc vascular density and vessel length density based on HCQ treatment duration.
3.2.3.3 Glucocorticoids
Compared to those who never used GC, patients with GC use showed reduced SCP-VD on the inferior side of the optic disc’s middle circle (30.1 vs. 32.5; P=0.042), (Supplementary Table S3).
3.2.3.4 Mycophenolate mofetil
Our results showed that MMF users had lower SCP-VD and SCP-VLD on the macular temporal side (37.2 vs. 40.6; P=0.020 and 6.5 vs. 7.1; P=0.045) and reduced DCP-VD in the optic disc’s 2.5mm circle (18.9 vs. 20.0; P=0.041) and temporal inner circle (24.4 vs. 28.3; P=0.012), with increased DCP-VD on the nasal outer circle (32.0 vs. 28.7; P=0.013) (Supplementary Table S4).
3.2.4 Association between cumulative drug exposure and vascular density
The study explored the relationship between OCTA data and cumulative doses of HCQ and GC in SLE patients. The results indicate a negative correlation between cumulative HCQ doses and SCP-VD in multiple optic disc regions. Similarly, higher cumulative GC doses were negatively correlated with VD in various SCP and DCP regions of the optic disc area (all P<0.05, Table 5, Figure 3).

Table 5. Correlation of ocular indicators with cumulative doses of HCQ and GC in SLE patients.
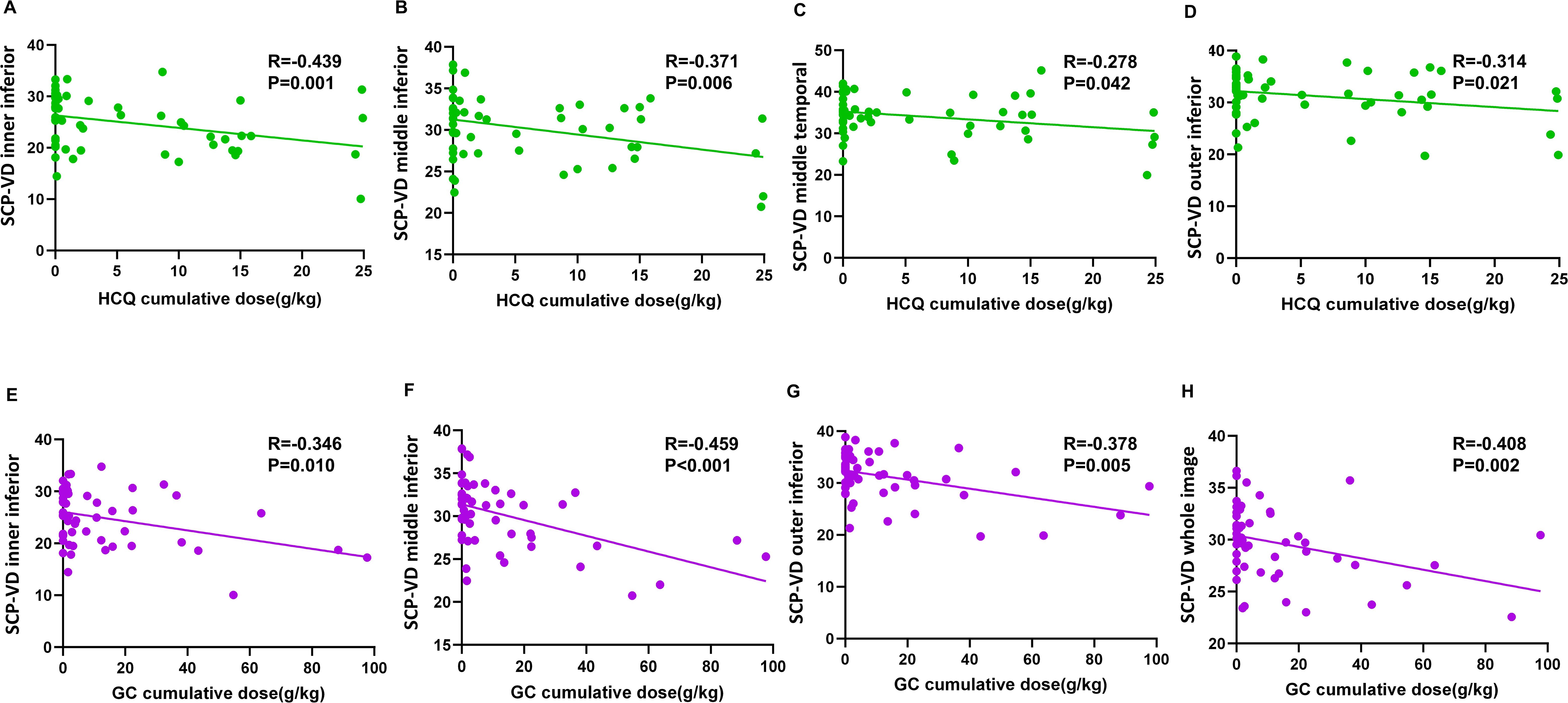
Figure 3. Linear regression scatter plots showed the correlation between retinal vascular density changes and cumulative doses of HCQ (A–D) or GC (E–H) in different retinal regions. HCQ, hydroxychloroquine; GC, glucocorticoid; SCP-VD, superficial capillary plexus vessel density.
3.2.5 Regression analysis of factors associated with parafoveal DCP vessel density
In our univariate regression analysis, it was found that LN, Belimumab treatment, and MMF treatment all had a negative impact on DCP-VD (β < 0). Notably, the effect of Belimumab treatment was statistically significant [β= -2.29 (-4.55~ -0.02), P = 0.048] (Supplementary Table S5, Figure 4). However, in the multivariate analysis, the effects of these agents were attenuated [β=-1.82(-4.17~0.53), P = 0.135] (Supplementary Table S5).
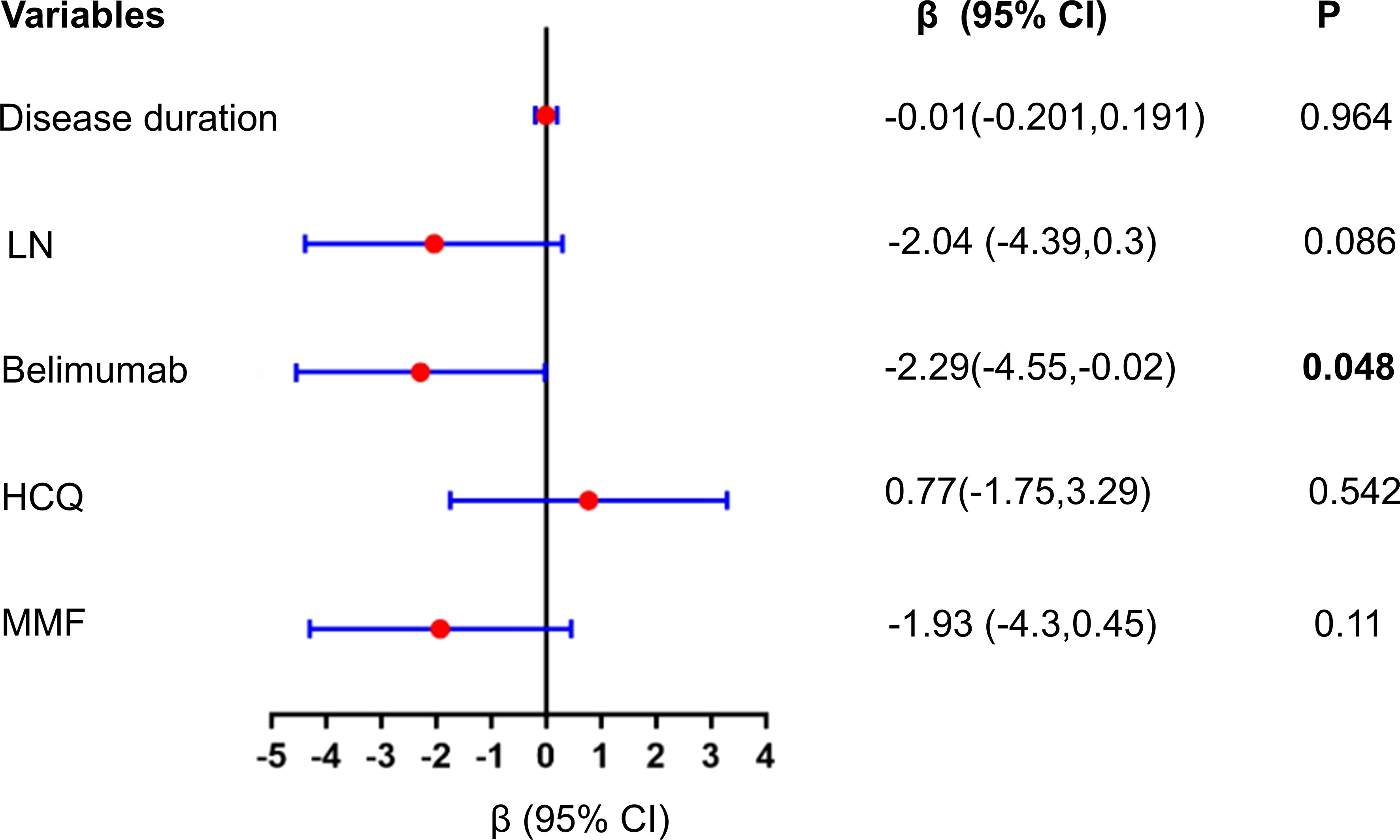
Figure 4. Univariate linear regression analysis of the impact of Belimumab and other factors on DCP peripapillary VD. Univariate regression analysis showed that LN, Belimumab treatment, and MMF treatment all had a negative impact on DCP peripapillary VD (β < 0). Notably, the effect of Belimumab treatment was statistically significant (P = 0.048); DCP, deep capillary plexus; VD, vessel density; LN, lupus nephritis; HCQ, Hydroxychloroquine; MMF, mycophenolate mofetil.
3.3 Comparison of cytokines and lymphocyte subsets before and after Belimumab treatment
We found that patients treated with Belimumab showed a significant decrease in CD19+ B cells (5.2% vs 9.8% ; P < 0.001) and IL-10 levels (0.3 pg/ml vs 0.8 pg/ml ; P = 0.026). There were no statistically significant differences in changes in other lymphocyte subsets and cytokines before and after treatment (Table 6, Figure 5).
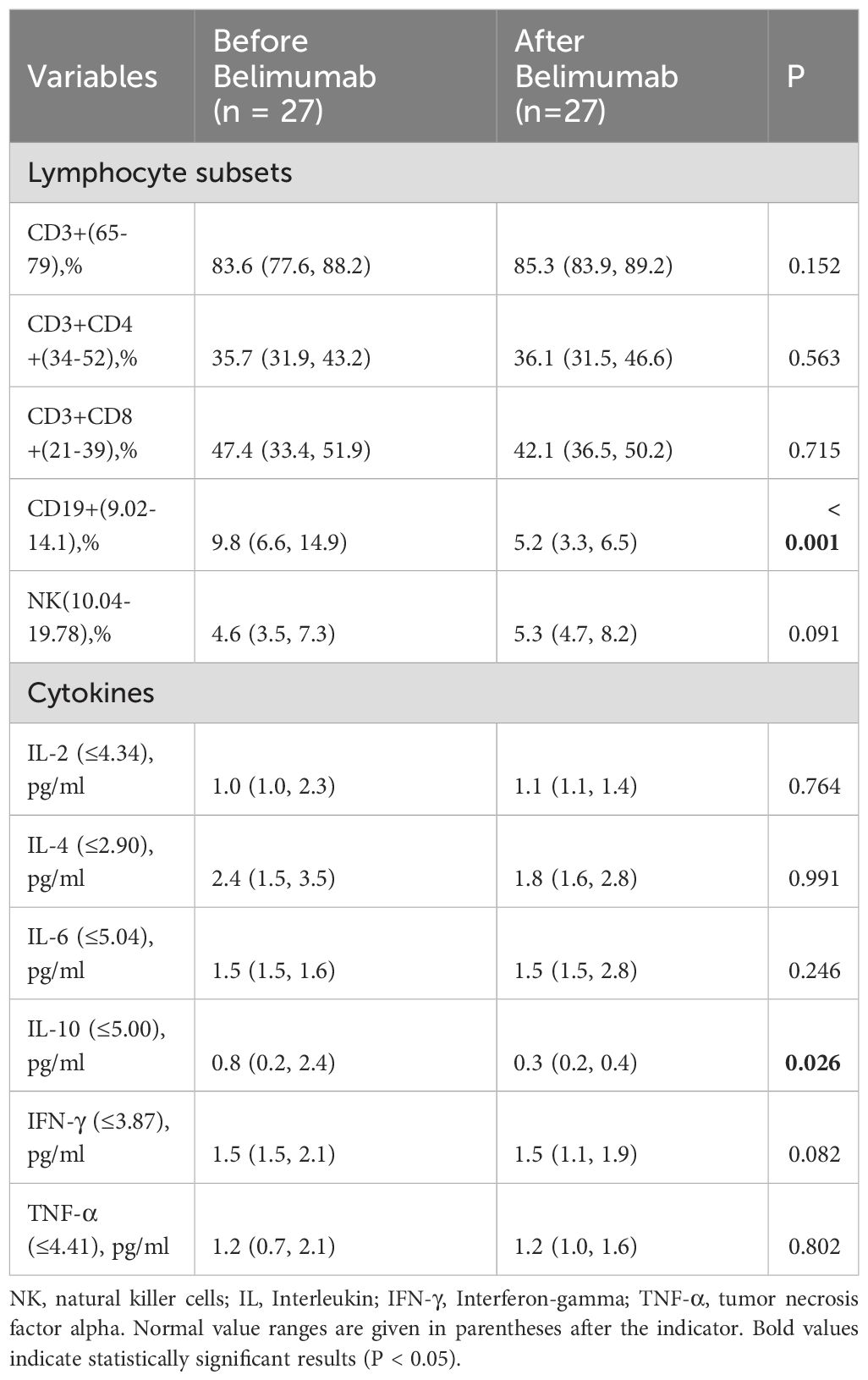
Table 6. Comparison of cytokines and lymphocyte subsets between patients before and after treatment with Belimumab.
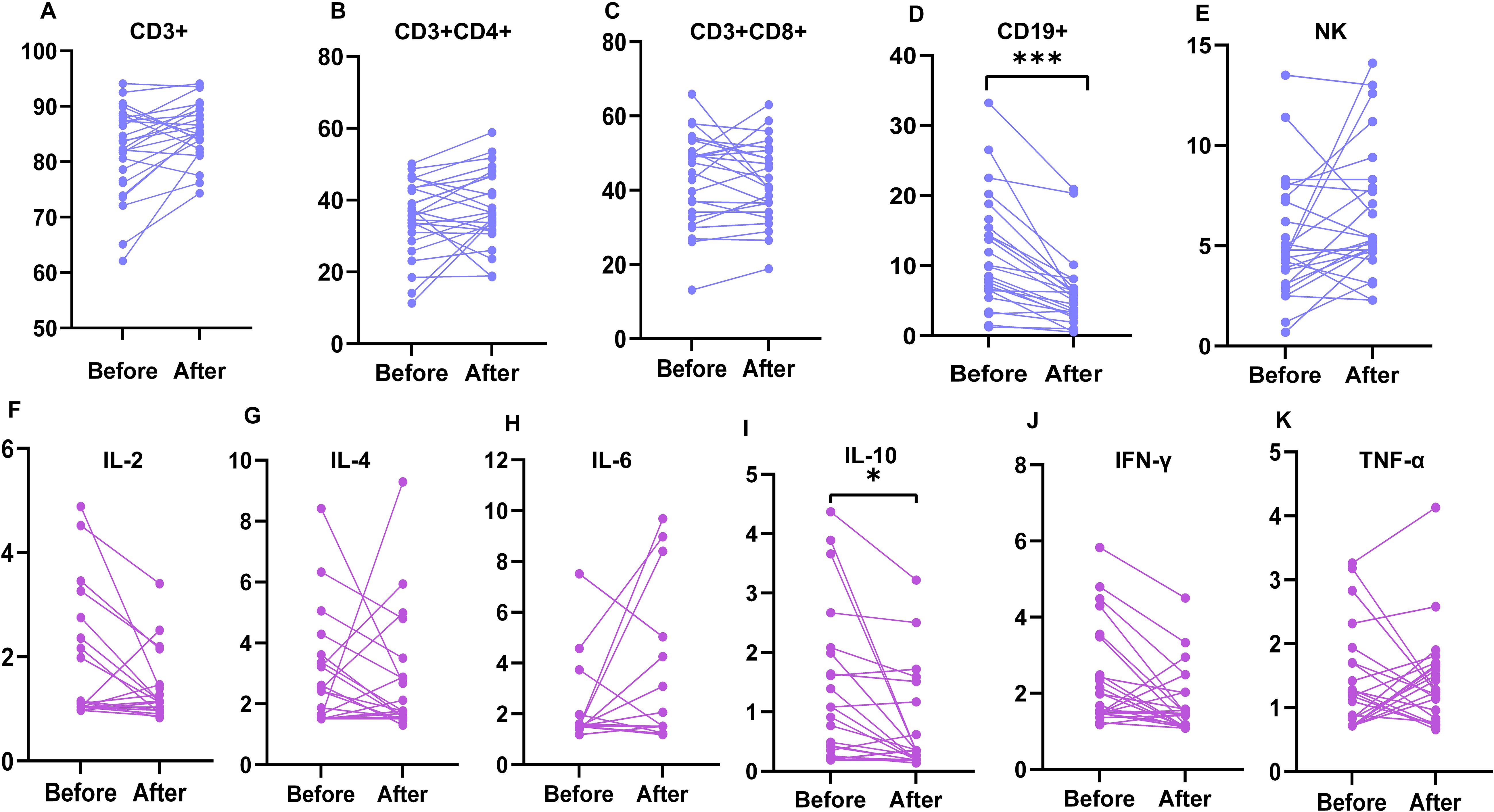
Figure 5. Comparison of lymphocyte subsets and cytokines between patients before and after treatment with Belimumab. The changes in lymphocyte subsets (A–E) and cytokines (F–K) in patients before and after treatment with Belimumab were compared. CD19+ B cells significantly decreased (***P < 0.001), and IL-10 levels increased (*P < 0.05) in treated patients. IL, interleukin; IFN-γ, interferon-gamma; TNF-α, tumor necrosis factor-alpha; NK, natural killer cells.
4 Discussion
SLE patients with LN experience higher morbidity and mortality rates compared to those without nephritis, leading to worse survival outcomes. Furthermore, lupus retinopathy can occur due to a vasculitic process affecting the microvasculature of the retina.The relationship between SLE and ocular vascular involvement is of particular clinical significance and requires comprehensive understanding. Previous studies found reduced retinal microvascular density in SLE patients, particularly those with renal involvement, compred to healthy controls (1, 3, 25). Recognizing the significance of ocular involvement is crucial for comprehensive management and improved outcomes in individuals with LN.
With the advent of steroids and immunosuppressive therapies, the incidence of retinal involvement in SLE patients ranges from 7-29%, which is associated with visual loss (26, 27). The main mechanisms leading to SLE retinopathy are the immune complex-mediated microangiopathic vasculopathy, secondary hypertension resulting in kidney involvement with activation of the renin-angiotensin-aldosterone system (RAAS), and the micro-thrombosis associated with either underlying endothelial injury or antiphospholipid (aPL) antibodies presence (28–30).In SLE patients, due to abnormal activity of the immune system, immune complexes may deposit in ocular tissues, which can lead to inflammation and damage to the retinal blood vessels, resulting in a decrease in retinal vascular density (28).
In SLE patients with early retinal lesions, the subjective perception of visual loss may be subtle due to the absence of prominent clinical manifestations. However, delayed recognition of visual impairment often coincides with the progression of retinal lesions, in concurrence with the advancing SLE pathology, rendering subsequent treatment interventions considerably more complex. Therefore, early detection and diagnosis of ocular involvement are crucial in SLE patients.
In recent years, there has been growing interest in the use of OCTA to detect early ocular vascular damage in systemic conditions, including arterial hypertension (31), diabetes (32), and chronic kidney disease (4). As a multisystemic disease, OCTA plays a particularly significant role in the early assessment of ocular vasculature in patients with SLE.
Wang et al. observed significant reductions in central macular thickness and in both the SCP-VD and DCP-VD of SLE patients compared to healthy controls as determined by OCTA. Additionally, no significant difference was found in retinal vascular densities between the LN and non-LN groups (33). Our research findings demonstrated that in LN patients, the loop area, superior, temporal, and whole image areas in the superficial capillaries exhibited significantly lower densities compared to the non-LN group (p <0.05), consistent with the findings of Conigliaro et al. Remarkably, we observed a significant negative correlation between vascular density and 24-hour urinary protein levels, further elucidating the association between ocular vascular density and renal impairment in patients. These patterns may reflect the cumulative burden of systemic inflammation and immunomodulation on the retinal microcirculation, supporting the utility of OCTA in capturing subclinical vascular damage.
The distinct retinal microvascular alterations in LN patients are strongly associated with shared pathophysiological mechanisms involving both ocular and renal microvasculature. Immune complex deposition induces endothelial activation and inflammation, leading to vascular damage (34). Elevated cytokines such as IL-6 and TNF-α exacerbate systemic inflammation, promoting endothelial dysfunction and microvascular remodeling (35).Furthermore, antiphospholipid antibodies contribute to thrombotic microangiopathy, resulting in vascular occlusion and ischemia (36).
Based on our findings of significantly reduced SCP-VD in LN patients, we further analyzed the associations between clinical parameters and vascular density. Taking into account the observed associations between age and CRP level changes with SCP-VD, therefore, we have considered that the reduction of SCP-VD is associated with vasculitis.
The retinal vasculature is one of the vessels that can be directly observed in SLE patients, and its performance often reflects the degree of systemic vascular damage. Similar to Conigliaro et al. and Ermurat et al. results, our study has revealed a negative correlation between the SLEDAI-2K scores and the retinal microvascular VD (1, 37).
While previous studies have reported enlargement in FAZ parameters in patients with SLE (38, 39), some other studies have failed to confirm this and reported no significant differences between SLE patients and control groups (40, 41). In our study, we didn’t observe an enlargement in the FAZ perimeter and FAZ area in LN patients. Based on our findings, we propose that the changes in vascular density in SLE are more prominent in the perifoveal area, while the parafovea and fovea are comparatively less affected.
In addition to the direct effects of SLE, drugs used in SLE therapy can potentially lead to retinal and visual impairment (42). HCQ was particularly associated with maculopathy and irreversible retinal damage (43). MTX can cause ischemic retinal complications, while cyclosporine can result in decreased visual acuity (44, 45).
To the best of our knowledge, this is the first investigation into the impact of Belimumab on retinal microvascular density in SLE patients. Our findings suggested that the use of Belimumab correlates with a decrease in vascular density.
Belimumab, as an emerging targeted therapy, is widely used in rheumatic diseases such as SLE, LN, and Sjögren’s syndrome, and has shown promising therapeutic outcomes (46–48). Therefore, it is crucial to closely monitor ocular involvement associated with the use of Belimumab to prevent severe visual impairment.
Notably, our research findings indicate a decrease in retinal microvascular vessel density in the patients treated with Belimumab, which has sparked great interest in us. Previous studies have shown promising efficacy of Belimumab in anti-neutrophil cytoplasmic antibody (ANCA)-associated vasculitis and cryoglobulinemic vasculitis (49, 50). However, our research results reveal a reduction in retinal microvascular vessel density in patients treated with Belimumab.
To investigate how Belimumab affects ocular vascular density, we compared cytokine and lymphocyte subset levels among patients before and after Belimumab treatment. We found that patients treated with Belimumab showed a significant decrease in CD19+ B cells and IL-10 levels. Previous studies showed that B-cell activating factor (BAFF) enhances angiogenesis and endothelial cell proliferation by upregulating vascular endothelial growth factor (VEGF) expression (51, 52). Furthermore, studies have indicated a correlation between CD19+ B cell numbers and VEGF expression levels. These cells are pivotal within the tumor microenvironment, influencing both VEGF expression and angiogenesis (53, 54). We hypothesize that the long-term use of Belimumab inhibits BAFF, subsequently altering B cell function and leading to a reduction in CD19+ cell counts, which ultimately affects VEGF expression and vascular density. Although prior immunological studies support this mechanistic pathway, it remains hypothetical due to the absence of direct VEGF measurements in our study. Additionally, our correlation regression analysis indicates that the use of Belimumab treatment negatively impacts DCP peripapillary VD. Our regression analysis, which adjusted for key confounders such as LN prevalence and disease duration (Supplementary Table S6), showed that while these adjustments attenuated Belimumab’s effects, the consistent negative trend observed across both univariate (β = -2.29, P = 0.048) and multivariate analyses (β = -1.82, P = 0.135) suggests a potential role for Belimumab in influencing retinal vascular density. This may justify the inclusion of routine OCTA screening in clinical follow-up protocols for patients with SLE, particularly those receiving biologic agents. However, due to the limited sample size in our study, expanding the cohort is essential to validate the reliability of our findings.
Previous studies have evaluated the effect of HCQ on retinal microvascular structure and suggested its potential protective effect. However, these studies did not conduct subgroup analyses considering factors like cumulative dose and duration of use (1, 55). In contrast, Mihailovic et al. performed a study with low- and high-risk subgroups based on HCQ use duration and cumulative dose, revealing that the protective effect was only present in the low-risk group (38). Our findings indicate that patients treated with HCQ for more than 5 years showed reduced DCP-VD in the 1.5 mm circle, 2.5mm circle and loop area. These results are consistent with the result of Jelena et al (14). We hypothesize that these differences may be attributed to prolonged disease duration and long-term HCQ use. It is worth noting that we conducted further analysis and found a negative correlation between retinal vascular density and the cumulative dose of HCQ and GC in patients. Higher cumulative doses of HCQ and GC may contribute to a reduction in retinal vascular density, emphasizing the potential influence of long-term HCQ treatment on retinal vascular density in SLE patients. Additionally, longer disease duration may also negatively impact retinal vascular density. These findings underscore the importance of regular monitoring and assessment of ocular health in SLE patients, especially those receiving long-term HCQ treatment.
Our study also has several limitations. Our cross-sectional study design limits the ability to establish causal relationships between retinal vascular density changes and Belimumab treatment. While we adjusted for confounders such as LN status and disease duration, the multifactorial nature of retinal microvascular changes makes it challenging to disentangle the effects of treatment from those of disease severity. Additionally, the absence of a healthy control group for comparison limits the generalizability of our findings. The observed associations, while statistically significant, require further investigation to confirm their clinical relevance. To address the limitations of this study, we are conducting ongoing longitudinal cohort studies incorporating serial OCTA imaging to investigate the cumulative effects of Belimumab on microvascular health, aiming to validate these findings and establish their clinical relevance.
5 Conclusion
In conclusion, our study found lower parafoveal SCP-VD of SLE-LN patients without retinopathy compared to SLE patients. Notably, Belimumab treatment resulted in a reduction in peripapillary DCP-VD area. These findings enhance our understanding of treatment effects on retinal vasculature in SLE. Our results highlight the potential of OCTA for early detection of retinal vascular damage in SLE-LN patients without retinopathy. Future studies with larger cohorts can provide further insights into these observations.
These findings support the value of incorporating routine OCTA screening into clinical follow-up for SLE patients, especially those undergoing long-term biologic therapy, to detect subclinical retinal changes. Such integration may facilitate earlier therapeutic intervention and more individualized disease management.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding authors.
Ethics statement
The studies involving humans were approved by The Ethics Committee of the Second Affiliated Hospital of Guangzhou Medical University. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
Author contributions
MM: Conceptualization, Data curation, Software, Visualization, Writing – original draft. JZ: Conceptualization, Data curation, Methodology, Writing – original draft. PL: Conceptualization, Data curation, Software, Visualization, Writing – original draft. DJ: Data curation, Methodology, Software, Visualization, Writing – original draft. HL: Data curation, Visualization, Writing – review & editing. ZeL: Data curation, Methodology, Supervision, Writing – review & editing. ZY: Methodology, Supervision, Writing – review & editing. YH: Methodology, Supervision, Writing – review & editing. WH: Conceptualization, Resources, Supervision, Writing – review & editing. LW: Data curation, Software, Writing – review & editing. ZhL: Conceptualization, Methodology, Supervision, Validation, Writing – review & editing. SY: Conceptualization, Methodology, Resources, Supervision, Validation, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This study was supported by the Guangdong Basic and Applied Basic Research Foundation of Guangdong Province, China (Grant No. 2019A1515011094); the Guangdong Basic and Applied Basic Research Foundation of Guangdong Province, China (Grant No. 2022A1515010471); the Guangzhou Science and Technology Planning Project of Guangdong Province, China (Grant No. 202102010139); Multi-center Clinical Research Project Fund of the Second Affiliated Hospital of Guangzhou Medical University of Guangdong Province, China (Grant No. 2022-LCYJ-YYDZX-05).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2025.1511133/full#supplementary-material
References
1. Conigliaro P, Cesareo M, Chimenti MS, Triggianese P, Canofari C, Aloe G, et al. Evaluation of retinal microvascular density in patients affected by systemic lupus erythematosus: an optical coherence tomography angiography study. Ann Rheum Dis. (2019) 78:287–9. doi: 10.1136/annrheumdis-2018-214235
2. Sivaraj RR, Durrani OM, Denniston AK, Murray PI, and Gordon C. Ocular manifestations of systemic lupus erythematosus. Rheumatol (Oxford England). (2007) 46:1757–62. doi: 10.1093/rheumatology/kem173
3. Conigliaro P, Giannini C, Ferrigno S, Nesi C, Fonti GL, Chimenti MS, et al. Assessment of microvascular involvement in lupus nephritis patients by retinal OCT-angiography and kidney biopsies. Clin Exp Rheumatol. (2023) 41:581–8. doi: 10.55563/clinexprheumatol/p1q482
4. Yeung L, Wu IW, Sun C-C, Liu C-F, Chen S-Y, Tseng C-H, et al. Early retinal microvascular abnormalities in patients with chronic kidney disease. Microcirculation. (2019) 26:e12555. doi: 10.1111/micc.12555
5. Koustenis A, Harris A, Gross J, Januleviciene I, Shah A, and Siesky B. Optical coherence tomography angiography: an overview of the technology and an assessment of applications for clinical research. Br J Ophthalmol. (2017) 101:16–20. doi: 10.1136/bjophthalmol-2016-309389
6. Wu K, Lin C, Lam AK-N, Chan L, and Leung CK-S. Wide-field trend-based progression analysis of combined retinal nerve fiber layer and ganglion cell inner plexiform layer thickness: A new paradigm to improve glaucoma progression detection. Ophthalmol. (2020) 127:1322–30. doi: 10.1016/j.ophtha.2020.03.019
7. Liu GY, Utset TO, and Bernard JT. Retinal nerve fiber layer and macular thinning in systemic lupus erythematosus: an optical coherence tomography study comparing SLE and neuropsychiatric SLE. Lupus. (2015) 24:1169–76. doi: 10.1177/0961203315582285
8. Mizuno Y, Nishide M, Wakabayashi T, Nishida K, and Kumanogoh A. OCTA, a sensitive screening for asymptomatic retinopathy, raises alarm over systemic involvements in patients with SLE. Ann Rheum Diseases. (2020) 79:e17. doi: 10.1136/annrheumdis-2018-214751
9. Bao L, Zhou R, Wu Y, Wang J, Shen M, Lu F, et al. Unique changes in the retinal microvasculature reveal subclinical retinal impairment in patients with systemic lupus erythematosus. Microvasc Res. (2020) 129:103957. doi: 10.1016/j.mvr.2019.103957
10. Li H, Yu S, Li P, Zhang J, Maitiyaer M, Huang AM, et al. Microvasculature alterations of peripapillary retina and macula in systemic lupus erythematosus patients without ocular involvement by optical coherence tomography angiography. Retina. (2023). doi: 10.1097/IAE.0000000000003989
11. Pelegrin L, Morato M, Araujo O, Figueras-Roca M, Zarranz-Ventura J, Adan A, et al. Preclinical ocular changes in systemic lupus erythematosus patients by optical coherence tomography. Rheumatol (Oxford). (2023) 62:2475–82. doi: 10.1093/rheumatology/keac626
12. de Sisternes L, Hu J, Rubin DL, and Marmor MF. Localization of damage in progressive hydroxychloroquine retinopathy on and off the drug: inner versus outer retina, parafovea versus peripheral fovea. Invest Ophthalmol Vis Sci. (2015) 56:3415–26. doi: 10.1167/iovs.14-16345
13. Michaelides M, Stover NB, Francis PJ, and Weleber RG. Retinal toxicity associated with hydroxychloroquine and chloroquine: risk factors, screening, and progression despite cessation of therapy. Arch Ophthalmol. (2011) 129:30–9. doi: 10.1001/archophthalmol.2010.321
14. Vasilijević JB, Kovačević IM, Dijana R, Dačić B, Marić G, and Stanojlović S. Optical coherence tomography angiography parameters in patients taking hydroxychloroquine therapy. Indian J Ophthalmol. (2023) 71:3399–405. doi: 10.4103/IJO.IJO_740_23
15. Furie R, Rovin BH, Houssiau F, Malvar A, Teng YKO, Contreras G, et al. Two-year, randomized, controlled trial of belimumab in lupus nephritis. N Engl J Med. (2020) 383:1117–28. doi: 10.1056/NEJMoa2001180
16. Fanouriakis A, Kostopoulou M, Andersen J, Aringer M, Arnaud L, Bae S-C, et al. EULAR recommendations for the management of systemic lupus erythematosus: 2023 update. Ann Rheum Diseases. (2024) 83:15–29. doi: 10.1136/ard-2023-224762
17. Bartalena L and Tanda ML. Current concepts regarding Graves’ orbitopathy. J Intern Med. (2022) 292:692–716. doi: 10.1111/joim.13524
18. Salvi M and Covelli D. B cells in Graves’ Orbitopathy: more than just a source of antibodies? Eye (Lond). (2019) 33:230–4. doi: 10.1038/s41433-018-0285-y
19. Aringer M, Costenbader K, Daikh D, Brinks R, Mosca M, Ramsey-Goldman R, et al. 2019 European league against rheumatism/American college of rheumatology classification criteria for systemic lupus erythematosus. Arthritis Rheumatol. (2019) 71:1400–12. doi: 10.1002/art.40930
20. Hahn BH, McMahon MA, Wilkinson A, Wallace WD, Daikh DI, Fitzgerald JD, et al. American College of Rheumatology guidelines for screening, treatment, and management of lupus nephritis. Arthritis Care Res (Hoboken). (2012) 64:797–808. doi: 10.1002/acr.21664
21. Gladman DD, Ibañez D, and Urowitz MB. Systemic lupus erythematosus disease activity index 2000. J Rheumatol. (2002) 29:288–91.
22. ETDRS Research Group. Early Treatment Diabetic Retinopathy Study design and baseline patient characteristics. ETDRS report number 7. Ophthalmology. (1991) 98:741–56. doi: 10.1016/S0161-6420(13)38009-9
23. Sun Z, Tang F, Wong R, Lok J, Szeto SKH, Chan JCK, et al. OCT angiography metrics predict progression of diabetic retinopathy and development of diabetic macular edema: A prospective study. Ophthalmol. (2019) 126:1675–84. doi: 10.1016/j.ophtha.2019.06.016
24. Kalra G, Zarranz-Ventura J, Chahal R, Bernal-Morales C, Lupidi M, and Chhablani J. Optical coherence tomography (OCT) angiolytics: a review of OCT angiography quantitative biomarkers. Surv Ophthalmol. (2022) 67:1118–34. doi: 10.1016/j.survophthal.2021.11.002
25. Conigliaro P, Triggianese P, Draghessi G, Canofari C, Aloe G, Chimenti MS, et al. Evidence for the detection of subclinical retinal involvement in systemic lupus erythematosus and Sjögren syndrome: A potential association with therapies. Int Arch Allergy Immunol. (2018) 177:45–56. doi: 10.1159/000488950
26. Davies JB and Rao PK. Ocular manifestations of systemic lupus erythematosus. Curr Opin Ophthalmol. (2008) 19:512–8. doi: 10.1097/ICU.0b013e3283126d34
27. Kharel Sitaula R, Shah DN, and Singh D. Role of lupus retinopathy in systemic lupus erythematosus. J Ophthalmic Inflammation Infect. (2016) 6:15. doi: 10.1186/s12348-016-0081-4
28. Hysa E, Cutolo CA, Gotelli E, Paolino S, Cimmino MA, Pacini G, et al. Ocular microvascular damage in autoimmune rheumatic diseases: The pathophysiological role of the immune system. Autoimmun Rev. (2021) 20:102796. doi: 10.1016/j.autrev.2021.102796
29. Aronson AJ, Ordoñez NG, Diddie KR, and Ernest JT. Immune-complex deposition in the eye in systemic lupus erythematosus. Arch Intern Med. (1979) 139:1312–3. doi: 10.1001/archinte.1979.03630480084026
30. Munguia-Realpozo P, Mendoza-Pinto C, Sierra Benito C, Escarcega RO, Garcia-Carrasco M, Mendez Martinez S, et al. Systemic lupus erythematosus and hypertension. Autoimmun Rev. (2019) 18:102371. doi: 10.1016/j.autrev.2019.102371
31. Donati S, Maresca AM, Cattaneo J, Grossi A, Mazzola M, Caprani SM, et al. Optical coherence tomography angiography and arterial hypertension: A role in identifying subclinical microvascular damage? Eur J Ophthalmol. (2021) 31:158–65. doi: 10.1177/1120672119880390
32. Wang W, He M, Gong X, Wang L, Meng J, Li Y, et al. Association of renal function with retinal vessel density in patients with type 2 diabetes by using swept-source optical coherence tomographic angiography. Br J Ophthalmol. (2020) 104:1768–73. doi: 10.1136/bjophthalmol-2019-315450
33. Wang X, Xie H, Yi Y, Zhou J, Yang H, and Li J. Clinical research of lupus retinopathy: quantitative analysis of retinal vessels by optical coherence tomography angiography in patients with systemic lupus erythematosus. Diagnostics (Basel). (2023) 13. doi: 10.3390/diagnostics13203222
34. Theofilis P, Sagris M, Oikonomou E, Antonopoulos AS, Siasos G, Tsioufis C, et al. Inflammatory mechanisms contributing to endothelial dysfunction. Biomed. (2021) 9. doi: 10.3390/biomedicines9070781
35. Bhol NK, Bhanjadeo MM, Singh AK, Dash UC, Ojha RR, Majhi S, et al. The interplay between cytokines, inflammation, and antioxidants: mechanistic insights and therapeutic potentials of various antioxidants and anti-cytokine compounds. BioMed Pharmacother. (2024) 178:117177. doi: 10.1016/j.biopha.2024.117177
36. Parodis I, Arnaud L, Gerhardsson J, Zickert A, Sundelin B, Malmström V, et al. Antiphospholipid antibodies in lupus nephritis. PloS One. (2016) 11:e0158076. doi: 10.1371/journal.pone.0158076
37. Ermurat S and Koyuncu K. Evaluation of subclinical retinal microvascular changes in systemic lupus erythematosus patients using optical coherence tomography angiography and its relationship with disease activity. Lupus. (2022) 31:541–54. doi: 10.1177/09612033221084222
38. Mihailovic N, Leclaire MD, Eter N, and Brücher VC. Altered microvascular density in patients with systemic lupus erythematosus treated with hydroxychloroquine-an optical coherence tomography angiography study. Graefes Arch Clin Exp Ophthalmol. (2020) 258:2263–9. doi: 10.1007/s00417-020-04788-4
39. Pichi F, Woodstock E, Hay S, and Neri P. Optical coherence tomography angiography findings in systemic lupus erythematosus patients with no ocular disease. Int Ophthalmol. (2020) 40:2111–8. doi: 10.1007/s10792-020-01388-3
40. Arfeen SA, Bahgat N, Adel N, Eissa M, and Khafagy MM. Assessment of superficial and deep retinal vessel density in systemic lupus erythematosus patients using optical coherence tomography angiography. Graefes Arch Clin Exp Ophthalmol. (2020) 258:1261–8. doi: 10.1007/s00417-020-04626-7
41. Işık MU, Akmaz B, Akay F, Güven YZ, Solmaz D, Gercik Ö, et al. Evaluation of subclinical retinopathy and angiopathy with OCT and OCTA in patients with systemic lupus erythematosus. Int Ophthalmol. (2021) 41:143–50. doi: 10.1007/s10792-020-01561-8
42. Dammacco R. Systemic lupus erythematosus and ocular involvement: an overview. Clin Exp Med. (2018) 18:135–49. doi: 10.1007/s10238-017-0479-9
43. Marmor MF, Kellner U, Lai TYY, Melles RB, and Mieler WF. Recommendations on screening for chloroquine and hydroxychloroquine retinopathy (2016 revision). Ophthalmol. (2016) 123:1386–94. doi: 10.1016/j.ophtha.2016.01.058
44. Apaydin C, Gur B, Yakupoglu G, and Saka O. Ocular and visual side effects of systemic cyclosporine. Ann Ophthalmol. (1992) 24:465–9.
45. Kruh J and Foster CS. Corticosteroid-sparing agents: conventional systemic immunosuppressants. Dev Ophthalmol. (2012) 51:29–46. doi: 10.1159/000336185
46. Furie R, Rovin BH, Houssiau F, Contreras G, Teng YKO, Curtis P, et al. Safety and efficacy of belimumab in patients with lupus nephritis: open-label extension of BLISS-LN study. Clin J Am Soc Nephrol. (2022) 17:1620–30. doi: 10.2215/CJN.02520322
47. Strand V, Levy RA, Cervera R, Petri MA, Birch H, Freimuth WW, et al. Improvements in health-related quality of life with belimumab, a B-lymphocyte stimulator-specific inhibitor, in patients with autoantibody-positive systemic lupus erythematosus from the randomised controlled BLISS trials. Ann Rheum Dis. (2014) 73:838–44. doi: 10.1136/annrheumdis-2012-202865
48. Mariette X, Barone F, Baldini C, Bootsma H, Clark KL, De Vita S, et al. A randomized, phase II study of sequential belimumab and rituximab in primary Sjögren’s syndrome. JCI Insight. (2022) 7. doi: 10.1172/jci.insight.163030
49. Jayne D, Blockmans D, Luqmani R, Moiseev S, Ji B, Green Y, et al. Efficacy and safety of belimumab and azathioprine for maintenance of remission in antineutrophil cytoplasmic antibody-associated vasculitis: A randomized controlled study. Arthritis Rheumatol. (2019) 71:952–63. doi: 10.1002/art.40802
50. Saadoun D, Ghembaza A, Riviere S, Mekinian A, Boutemy J, Leroux G, et al. Rituximab plus belimumab in non-infectious refractory cryoglobulinemia vasculitis: A pilot study. J Autoimmun. (2021) 116:102577. doi: 10.1016/j.jaut.2020.102577
51. Chou C-H, Ho C-M, Lai S-L, Chen C-N, Wu Y-M, Shun C-T, et al. B-Cell Activating Factor Enhances Hepatocyte-Driven Angiogenesis via B-Cell CLL/Lymphoma 10/Nuclear Factor-KappaB Signaling during Liver Regeneration. Int J Mol Sci. (2019) 20. doi: 10.3390/ijms20205022
52. Lee G-H, Lee J, Lee J-W, Choi WS, and Moon E-Y. B cell activating factor-dependent expression of vascular endothelial growth factor in MH7A human synoviocytes stimulated with tumor necrosis factor-α. Int Immunopharmacol. (2013) 17:142–7. doi: 10.1016/j.intimp.2013.04.026
53. Nakayama N, Fang I, and Elliott G. Natural killer and B-lymphoid potential in CD34+ cells derived from embryonic stem cells differentiated in the presence of vascular endothelial growth factor. Blood. (1998) 91:2283–95. doi: 10.1182/blood.V91.7.2283
54. Hansson F, Toporski J, Månsson R, Johansson B, Norén-Nyström U, Jacobsen SEW, et al. Exit of pediatric pre-B acute lymphoblastic leukaemia cells from the bone marrow to the peripheral blood is not associated with cell maturation or alterations in gene expression. Mol Cancer. (2008) 7:67. doi: 10.1186/1476-4598-7-67
Keywords: systemic lupus erythematosus, lupus nephritis, optical coherence tomography angiography, retinal microvascular, Belimumab
Citation: Maitiyaer M, Zhang J, Li P, Jiang D, Li H, Lin Z, Ye Z, Huo Y, Huang W, Wang L, Liu Z and Yu S (2025) Belimumab-driven reductions in retinal microvascular density assessed by optical coherence tomography angiography: insights from systemic lupus erythematosus patients. Front. Immunol. 16:1511133. doi: 10.3389/fimmu.2025.1511133
Received: 17 October 2024; Accepted: 05 May 2025;
Published: 16 June 2025.
Edited by:
Alex Fonollosa, Cruces University Hospital, SpainReviewed by:
Olga Araújo, Hospital Clinic of Barcelona, SpainJoseba Artaraz, Hospital de Cruces, Spain
Copyright © 2025 Maitiyaer, Zhang, Li, Jiang, Li, Lin, Ye, Huo, Huang, Wang, Liu and Yu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Shuilian Yu, c2h1aWxpYW4yMDA4QGdtYWlsLmNvbQ==; Zhiping Liu, enhsaXUyMDEzQGd6aG11LmVkdS5jbg==
†These authors have contributed equally to this work and share first authorship