 Andrea Favre-Bulle1*
Andrea Favre-Bulle1* Maja Stanković1
Maja Stanković1 Tyler Mantaian2Claudia Frei3Sonja Schaefer4Sarah Sharon Gabriel3†Demet Sönmez5
Tyler Mantaian2Claudia Frei3Sonja Schaefer4Sarah Sharon Gabriel3†Demet Sönmez5 Raquel Aguiar-Ibáñez6
Raquel Aguiar-Ibáñez6- 1Global Human Health, MSD, Lucerne, Switzerland
- 2Lumanity, Bethesda, MD, United States
- 3Global Medical and Scientific Affairs, MSD, Lucerne, Switzerland
- 4European Clinical Development, Oncology, MSD, Zurich, Switzerland
- 5Global Medical and Scientific Affairs, MSD, Stockholm, Sweden
- 6Merck Canada, Inc., Kirkland, QC, Canada
Background: Inhibitors of programmed cell death protein 1 (PD-1) and its ligand (PD-L1) (referred to hereafter as anti-PD-(L)1 agents) are approved to treat a variety of advanced-stage cancers. Incorporating these agents into neoadjuvant/adjuvant treatment regimens for early-stage cancers may provide health and economic benefits at the population level.
Methods: A health outcomes projection model compared two scenarios in Switzerland: I) anti-PD-(L)1 agents used only for advanced/metastatic disease, and II) anti-PD-(L)1 agents starting in the neoadjuvant/adjuvant setting. The model focused on three cancers for which anti-PD-(L)1 agents are currently approved in Europe in early stages: melanoma, renal cell carcinoma (RCC), and triple-negative breast cancer (TNBC), projecting clinical evolution over 10 years. Estimated outcomes included life-years, quality-adjusted life-years (QALYs), recurrences/events, active treatments for metastatic disease, adverse events, and deaths.
Results: Of the estimated 10,659 eligible patients during 2022-2031, 9,050 were predicted to initiate neoadjuvant and/or adjuvant treatment with anti-PD-(L)1 agents for treatment of melanoma, RCC, or TNBC. Compared to anti-PD-(L)1 agents being available only in the metastatic setting, use of anti-PD-(L)1 agents in the neoadjuvant and/or adjuvant setting for these 3 cancers was projected to avoid 1,144 recurrences (a 27% decrease), prevent 1,577 active treatments in the metastatic setting (a 35% decrease), avoid 530 deaths (a 23% decrease), and increase life-years without recurrence by 3,416 (a 10% increase).
Conclusion: The use of anti-PD(L)1 agents to treat early-stage cancers in Switzerland is anticipated to result in better outcomes by preventing recurrences/events, active metastatic treatments, and deaths.
1 Introduction
Early detection and treatment can reduce the burden of cancer, which is a major health issue in Europe (1–3). It is estimated that 45,000 new cases of cancer and 17,300 deaths due to cancer occur annually in Switzerland (4). Incidence of breast cancer and melanoma is on the rise in Switzerland (5), which makes early detection and treatment even more important. Renal cell carcinoma (RCC) is one of the most common cancers in Switzerland, and in 80% of the cases, it is diagnosed at an early stage (4, 6). It has been projected that, between 2018 and 2040, there will be 98,000 premature cancer deaths in Switzerland, with a productivity cost of €450,000 per death (7).
Immune checkpoint inhibitors (ICIs), primarily inhibitors of programmed cell death protein 1 (PD-1) or its ligand, programmed cell death ligand 1 (PD-L1), and cytotoxic T-lymphocyte-associated protein 4 (CTLA-4), are now a standard treatment for many types of advanced/metastatic cancer (8). ICIs have the potential of benefiting patients with early-stage cancers (9–11), for whom there is still a high unmet need with the standard of care, as recurrence rates remain high (12–16). The question of expanding these agents as neoadjuvant (before surgery to shrink the tumor) or adjuvant (after surgery to prevent or delay recurrence) treatment options for early-stage tumors requires weighing the higher upfront treatment costs against long-term disease-free survival and other potential benefits.
A health outcomes model was developed to assess the impact of adopting PD-1 or PD-L1 inhibitors (referred to hereafter as anti-PD-(L)1 agents) for the neoadjuvant/adjuvant treatment of early-stage cancers versus reserving them for advanced/metastatic disease (17). In this study, the model was used to determine the health impact of using anti-PD-(L)1 agents in 3 different early-stage cancers in Switzerland over a 10-year period: melanoma, RCC, and triple-negative breast cancer (TNBC).
2 Materials and methods
2.1 Description of the model
The model was designed to quantify the health impact of adding anti-PD-(L)1 agents to traditional cancer treatment/management strategies in the neoadjuvant/adjuvant setting. It compares the difference in clinical outcomes between a scenario in which anti-PD-(L)1 agents are reserved for the advanced/metastatic setting (scenario I) and a scenario in which anti-PD-(L)1 agents are added to the traditional neoadjuvant/adjuvant chemotherapy options (scenario II). Patients enter the model in weekly cycles and initiate treatment with either an anti-PD-(L)1 agent or traditional treatment/management strategies in the neoadjuvant/adjuvant setting. The model tracks the clinical outcomes throughout the average patient journey from initial treatment to recurrence, metastasis, and/or death. Clinical outcomes for the average patient are scaled to account for the number of patients initiating each adjuvant treatment each week throughout the model time horizon. The difference in clinical outcomes between scenario I and scenario II quantifies the impact of adding anti-PD-(L)1 agents to the neoadjuvant/adjuvant treatment/management options.
2.2 Base case settings
The analysis was done from the healthcare system perspective and focused on 3 cancer types: melanoma, RCC, and TNBC. Table 1 shows the base case settings of the model for both scenarios.
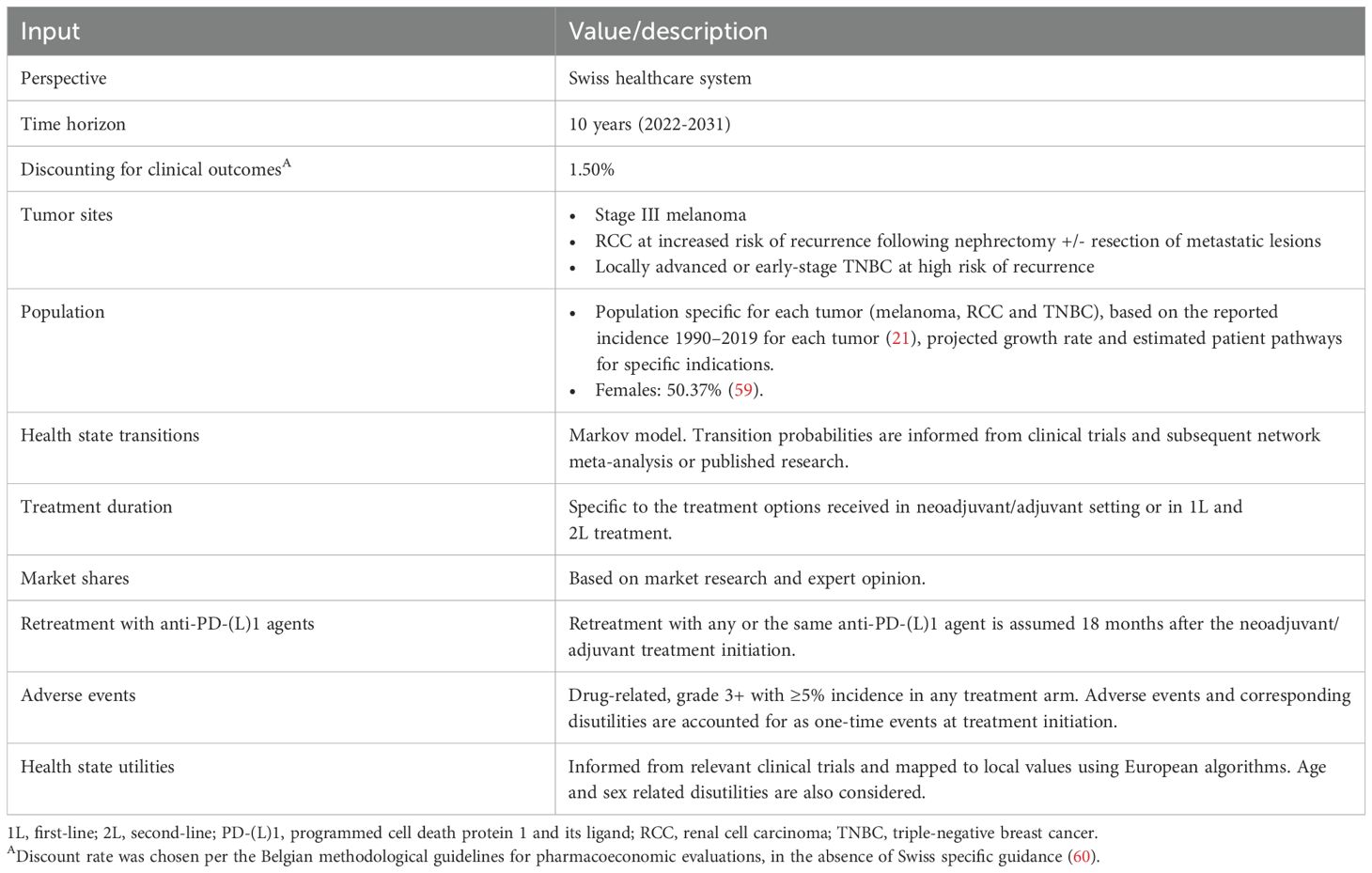
Table 1. Base case settings.
2.3 Inputs and data sources
2.3.1 Population
The target population was patients with melanoma, RCC, and TNBC in Switzerland who were eligible for neoadjuvant/adjuvant treatment with anti-PD-(L)1 agents. Eligibility for anti-PD-(L)1 agents among cancer patients in Switzerland was determined based on the inclusion criteria from the pivotal trials of pembrolizumab in melanoma (KEYNOTE 054 (18)), early-stage RCC (KEYNOTE 564 (19)), and TNBC (KEYNOTE 522 (20)). Briefly, this included patients with stage III melanoma who underwent complete resection; RCC patients with increased risk of recurrence following nephrectomy, or following nephrectomy and resection of metastatic lesions; and TNBC patients with locally advanced or early-stage cancer at high risk of recurrence (Table 1). The number of patients with melanoma, RCC, and TNBC in Switzerland in 2022 was obtained from the Krebsliga Report (4). A combination of scientific literature, internal/external quantitative market research, and consultation with scientific leaders helped to estimate the proportions of the population eligible for treatment with anti-PD-(L)1 agents in the early-stage setting. These numbers were projected out to 2031, assuming the same growth rate as shown in the national incidence reports from 1990-2019 (21).
2.3.2 Treatment patterns
In scenario I, 100% of patients were allocated to management strategies currently used in the early-stage setting. For melanoma, this consisted of watchful waiting or dabrafenib + trametinib; for RCC, it was watchful waiting; and for TNBC, it was chemotherapy. In scenario II, increasing proportions of the patient population were allocated to anti-PD-(L)1 agents as a class over time, using market shares projected from internal estimates. Anti-PD-(L)1 agents were assumed to enter the treatment landscape immediately in the base case. In the current iteration, the model included pembrolizumab and nivolumab, 2 anti-PD-(L)1 agents currently approved for neoadjuvant/adjuvant treatment of cancer in Europe (22, 23).
First-line (1L) and second-line (2L) metastatic therapy was conditional on the treatment received in the adjuvant/neoadjuvant setting and was based on published cost-effectiveness analyses (for melanoma and TNBC (24, 25)) and internal market research (for RCC). Duration of treatment in the base case analysis was based on the Kaplan-Meier curves for time to treatment discontinuation from the pivotal trials (18–20); or on the parametric distributions of patients in each health state (described in the next section); or on the assumption of equivalence to the progression-free survival time (also described below). For all 3 cancers, retreatment with any or the same anti-PD-(L)1 agent was assumed to be 1.5 years after initiation of adjuvant/neoadjuvant treatment (in the absence of local guidelines).
2.3.3 Transitions between health states
The transitions between health states were aligned with those used in prior cost-effectiveness and budget impact models (24, 26–28) accepted by health technology assessment agencies such as the United Kingdom’s National Institute for Health and Care Excellence (29–31). Generally, the population of the recurrence-/event-/disease-free state was modeled as parametric distributions fitted to patient-level data from key pivotal trials (i.e., dependent on the adjuvant/neoadjuvant treatment arm) (18–20), and then used to estimate the probability of transitioning to the locoregional recurrence, metastatic, and death states. Transition probabilities to death were defined as either the trial-based mortality estimates or the background mortality, whichever was larger.
For melanoma and RCC, transitions from the locoregional recurrence state to the metastatic state were assumed to be equivalent across adjuvant treatment arms. These transitions were based on survival analyses of individual patient-level data from database studies (cited in Lai et al. (27) and Favre-Bulle et al. (24)) or were assumed to be equivalent across anti-PD(L)1 agents (18). Transitions to death were assumed to be equivalent across adjuvant treatment arms; in the absence of direct transitions to death or due to the small sample size in the database studies, the maximum between the transition from recurrence-/disease-free to death from the pivotal trial’s intervention arm and the background mortality estimate was used. For TNBC, parametric distributions were fitted to patient-level data; the distribution of the transition from the locoregional recurrence state to the metastatic state or death was based on the pivotal trial data (20).
From the metastatic state to death, several methods were used to derive the transitions for 1L metastatic treatments. These ranged from parametric models (derived from trial data in the advanced/metastatic setting for melanoma and RCC and trial data in the metastatic setting for TNBC) to assuming equivalence between treatments. The parametric models were fitted to patient-level data or based on observed median data, with hazard ratios (HRs) for the remaining treatments derived from network meta-analyses when available (cited in previous studies (24, 26–28)). The transitions for the 1L metastatic treatments were then weighted based on their use, conditional on the adjuvant treatment received, to derive the transitions from the metastatic state that ultimately applied to each adjuvant treatment arm.
Utilities associated with each health state are shown in Supplementary Table 1 and were derived from key pivotal trials (18–20). Utilities were also applied for age and sex as described previously (32).
2.3.4 Adverse events
Adverse events were assumed to occur with each line of therapy. They were modeled as one-time events, with disutility incurred at treatment initiation. For the adjuvant/neoadjuvant treatment setting, baseline risk and mean duration data for anti-PD-(L)1 agents (average weeks per event multiplied by the number of events per patient) were taken from key trials for melanoma (18), RCC (19), and TNBC (20). In some cases, equivalence was assumed across anti-PD(L)1 agents. For the 1L and 2L metastatic treatment settings, baseline risk and mean duration data were derived from clinical trials and other publications for melanoma (33–40), RCC (41–47), and TNBC (48–51) (with equivalence between treatments and/or lines of therapy assumed where no relevant data were available). Only grade 2+ diarrhea and all grade 3+ adverse event types (which include rash, diarrhea, increased ALT/AST) with a frequency of ≥5% in any treatment arm were considered. Disutility values for adverse events in the adjuvant/neoadjuvant and metastatic settings were, respectively: -0.05 and -0.13/-0.14 (1L/2L) for melanoma (18, 33, 52); -0.06 and -0.05 for RCC (19, 41); and -0.02 and -0.03 for TNBC (20, 48).
2.4 Outputs
Outcomes of the analysis were total life-years, recurrence-/event-/disease-free life-years, quality-adjusted life-years (QALYs), events or recurrences (total number), number of active treatments administered for metastatic disease, adverse events (total number), total deaths, and deaths after the first event or recurrence (Supplementary Table 2). Life-years, recurrences, and deaths were linked to specific health states, while treatment for metastatic disease and adverse events were linked to specific treatment settings.
2.5 Sensitivity analyses
The impact of uncertainty on the estimated outcomes was assessed in sensitivity analyses. Scenarios of interest included: assuming 100% uptake of anti-PD-(L)1 agents (vs. the base case percentages), 20% increase/decrease of target population for all years, delayed time to launch of anti-PD-(L)1 agents in scenario II, and no allowance of retreatment with anti-PD-(L)1 agents (vs. retreatment allowed in the base case). Inclusion of subgroups of cancer types (melanoma only, RCC only, TNBC only, melanoma + RCC, melanoma + TNBC, and RCC + TNBC; a total of 6 combinations) was assessed in supplementary analyses.
One-way sensitivity analysis was further used to investigate which of the selected variables had the largest effect on the outcomes. The variables tested were general population size in each year, target population characteristics for each cancer type (size of the eligible population, percentage female, age, and weight), incidence of individual cancers (total incidence and fractional incidence of patients meeting the indication criteria for treatment with anti-PD-(L)1 agents), HRs in the metastatic setting for overall and progression-free survival, the utility associated with specific health states, and the disutility associated with adverse events. All input variables were adjusted by +/- 10% and HRs were adjusted to their lower and upper bounds according to their 95% confidence interval.
3 Results
3.1 Cumulative results
Table 2 shows the annual and cumulative target population for the analysis, which consisted of all patients in Switzerland eligible to initiate adjuvant/neoadjuvant treatment for melanoma, RCC, or TNBC. Of the 10,659 patients in this group over the study period, 9,050 were estimated to receive treatment for their cancer with anti-PD-(L)1 agents in scenario II.

Table 2. Target population and number of patients treated with anti-PD-(L)1 agents, by year.
Comparison of scenarios I and II showed the cumulative health impact of early treatment with anti-PD-(L)1 agents over the study period (Table 3, Supplementary Figure 1). Using anti-PD-(L)1 agents in early-stage cancers vs. limiting their use to the advanced/metastatic setting resulted in gains in total life-years (+1,280; a gain of 3%), recurrence-/event-/disease-free life-years (+3,416; +10%), and QALYs (+1,422; +4%). Benefits were also estimated in terms of 1,144 fewer recurrences (-27%), 1,577 fewer treatments for metastatic disease (-35%), 109 fewer adverse events (-1%), and 530 fewer deaths (-23%).
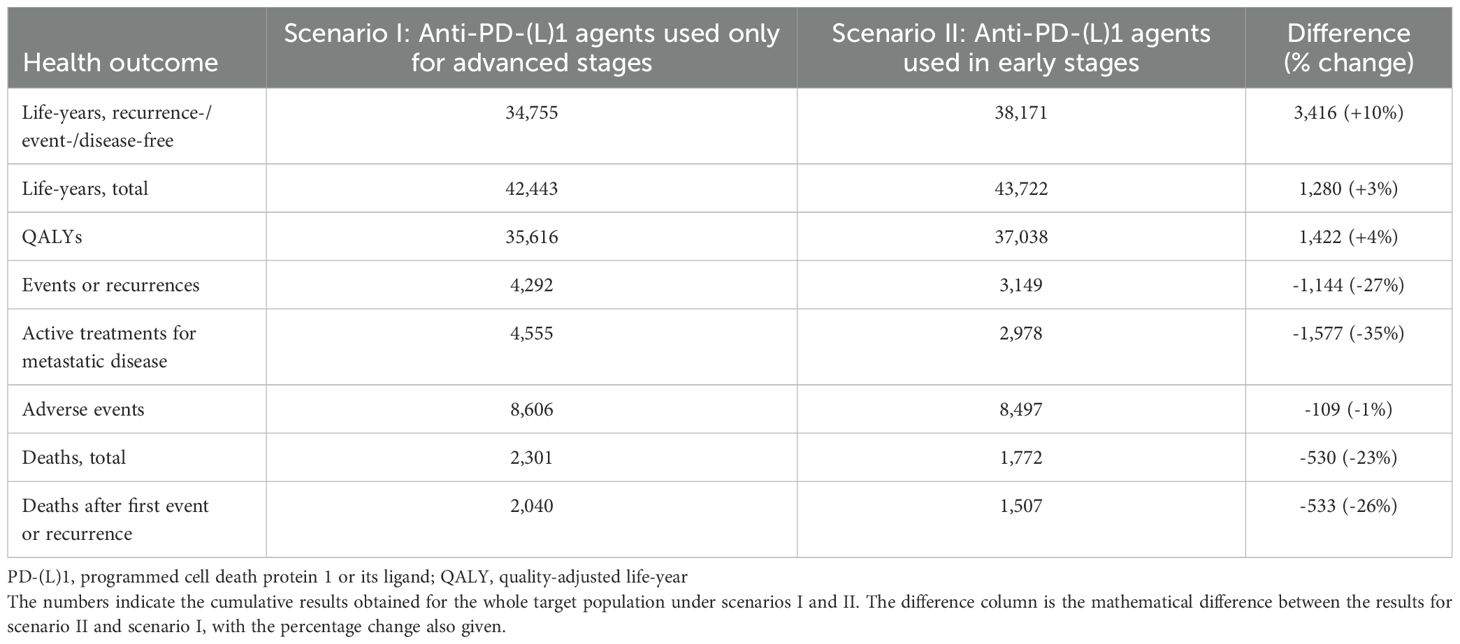
Table 3. Cumulative base case results.
3.2 Health impact over time
Figure 1 shows the model results for each year of the study period. These data indicate that the gains in life-years and reductions in recurrences and deaths produced by using anti-PD-(L)1 agents in early-stage cancers are not realized until several years after implementation of the scenario II treatment policy. Notably, adverse events increased in the first 3 years and decreased thereafter, for a cumulative decrease of 109 events over the total 10-year period. This is explained by the observation of higher rates of adverse events with anti-PD-(L)1 agents vs. other agents in the adjuvant/neoadjuvant setting, which is eventually offset by the reduction in the number metastatic treatments administered after anti-PD-(L)1 agents, and thus fewer patients experience adverse events in the metastatic setting, resulting in fewer adverse events overall.
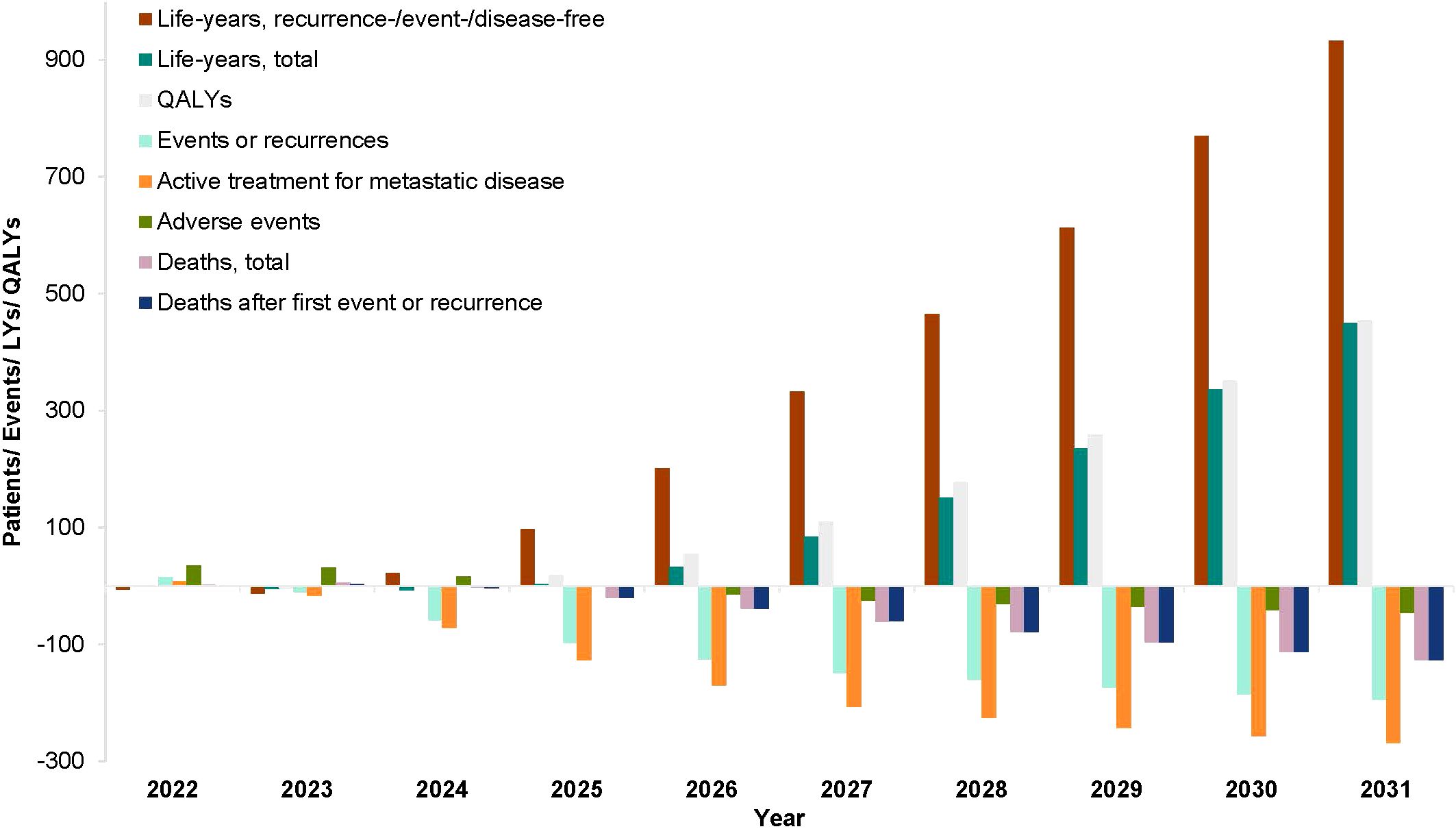
Figure 1. Public health impact of anti-PD-(L)1 agents, by year. QALY, quality-adjusted life-year. The bars indicate the difference between scenarios I and II for the health outcomes listed: life-years (recurrence-/event-/disease-free and total), QALYs, events or recurrences, the number of active treatments for metastatic disease, adverse events, and deaths (after first event/recurrence and total).
3.3 Sensitivity analyses
For scenario-based sensitivity analyses, we varied the uptake of anti-PD-(L)1 agents, the target population, the time to launch of anti-PD-(L)1 agents, the capacity for retreatment with anti-PD-(L)1 agents, and the inclusion of various subgroups of cancer. As expected, greater uptake of anti-PD-(L)1 agents led to positive changes in all outcomes (range +13% to +50%), while delayed time to launch of anti-PD-(L)1 agents led to negative changes in all outcomes (range -6% to -60%; Table 4). Prohibiting retreatment with anti-PD-(L)1 agents decreased life-years (-6%), QALYs (-2%), deaths (-5%), the number of active treatments for metastatic disease (-10%), and the number of adverse events (-69%). Altering the target population by 20% either way produced numerically equivalent changes in the outcomes (data not shown). Results for selected outcomes and additional scenarios are shown in graphical form in Supplementary Figure 2.
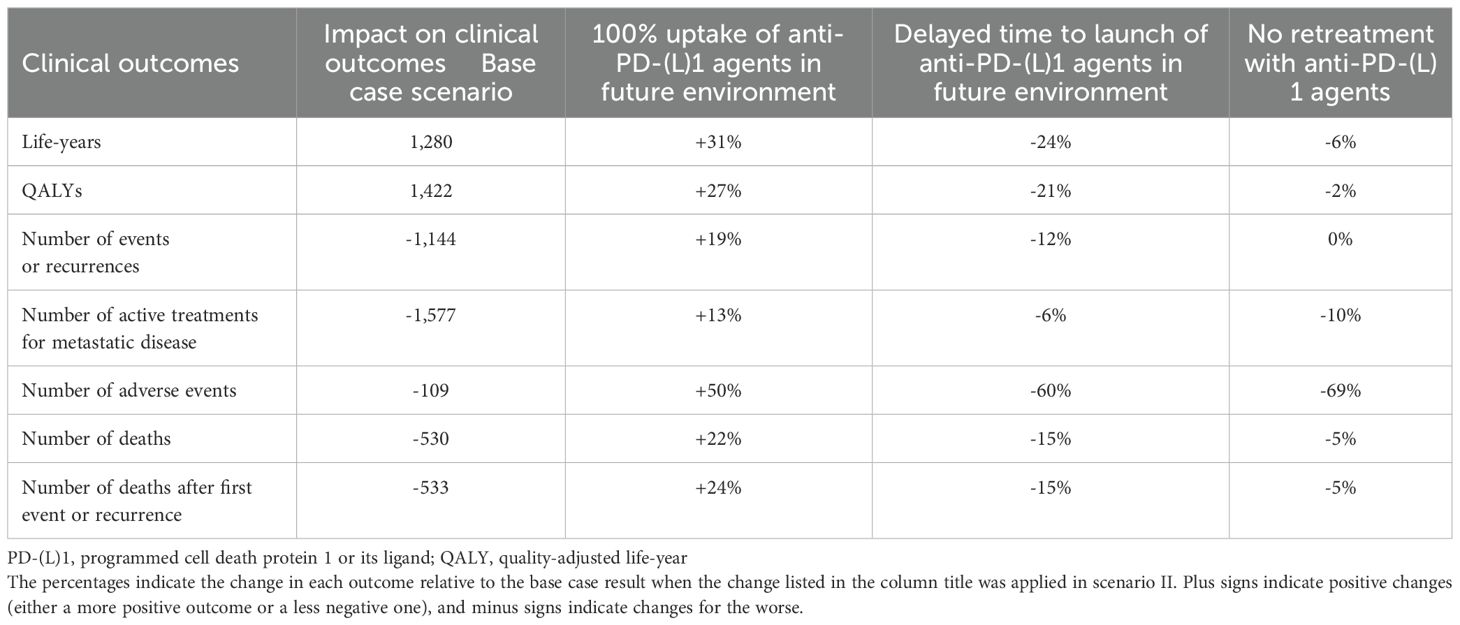
Table 4. Sensitivity analyses.
In the one-way sensitivity analysis (data not shown), the variables with the greatest effect on the results were target population size in years 2022–2025 and the HR for overall survival in melanoma and RCC with pembrolizumab vs. other agents or observation. However, the variation in results was minimal, and values were similar to the base case values for all outcomes of interest.
4 Discussion
We modeled the health impact of making anti-PD-(L)1 agents available for the treatment of early-stage cancer vs. reserving them for the advanced/metastatic setting in Switzerland. The analysis included 3 cancers for which anti-PD-(L)1 agents are indicated for early-stage treatment in Europe. Our results support the incorporation of anti-PD-(L)1 agents into early-stage cancer treatment based on the expected reductions in deaths, recurrences, metastatic treatments, and adverse events at the national level.
Recent studies demonstrate the rapid uptake of ICIs for advanced cancers in Switzerland. Among 41 patients with unresectable advanced/metastatic BRAF mutation-positive cutaneous melanoma treated at one of 5 hospitals in 2016-2018, ICIs were the most common 1L treatment (70.7% of regimens) and the most common treatment overall (52.9% across multiple lines of therapy) (53). Similarly, among 93 stage III/IV melanoma patients receiving adjuvant therapy after tumor resection at Bern University Hospital’s Cancer Center, 96.8% received ICIs (either pembrolizumab or nivolumab) (54). In a broader analysis of medical records from the Bern University Hospital Cancer Center including 5,109 patients with all types of cancer, Wahli et al. showed that the percentage of cancer patients prescribed ICIs increased from 8.6% in 2017 to 22.9% in 2021 and that ICIs constituted 13.2% of the anticancer treatments in 2017, and 28.2% in 2021 (55). Notably, 95% of ICI prescriptions were for patients with stage III/IV disease, suggesting an opportunity for expansion of ICIs into early-stage treatment.
Data from the Cancer Registry of Zurich 1980–2015 showed that relative 5-year survival rates have increased significantly for breast cancer (70% in 1980-1989, 89% in 2010-2015) and melanoma (74%-86% in 1980-1989, 94%-96% in 2010-2015) in the past few decades (56). Real-world studies support the role of ICIs in improving survival rates in melanoma patients in Switzerland. Among patients with stage IV metastatic melanoma treated with chemotherapy in 2008-2009 (n=95) or ICIs in 2008-2014 (n=121) at one of 3 Swiss hospitals, 12-month survival rates in the chemotherapy and ICI groups were 38% and 69%, respectively, and the median overall survival times were 7.4 months and 16.7 months (57).
A recent Markov modeling study found pembrolizumab to be cost-effective vs. observation, the standard of care for stage IIB/C melanoma in Switzerland, with an incremental cost-effectiveness ratio of CHF 27,424/QALY (well below the willingness-to-pay threshold of CHF 100,000/QALY) (24). Notably, this study examined cost-effectiveness in the early-stage setting, and although the base case used a lifetime time horizon, cost-effectiveness was maintained over a shorter horizon of 20 years. Another Swiss study evaluating the cost-effectiveness of pembrolizumab for patients with RCC post-nephrectomy reported an incremental cost-effectiveness ratio of CHF 65,299/QALY compared to observation (28). Similarly, in the United States, adjuvant pembrolizumab for post-nephrectomy RCC was shown to be cost-effective vs. routine surveillance, with an incremental cost-effectiveness ratio of USD 46,327/QALY (27). In TNBC, a Swiss Markov model evaluating event-free survival in the female population found an incremental cost-effectiveness ratio of CHF 14,114/QALY for neoadjuvant/adjuvant pembrolizumab + chemotherapy versus chemotherapy alone, indicating cost-effectiveness (25).
Together, these findings on ICI uptake, survival rates, and cost-effectiveness, along with the results of the current study indicating a significant health benefit, pave the way for the potential use of ICIs in early-stage cancers. Although priority has historically been given to patients with more advanced or aggressive cancers, there is a comparatively greater number of patients with early-stage cancer, and this ultimately translates to more recurrences and deaths at the population level (9). Thus, there is an unmet need to identify effective treatment strategies for early-stage cancers. ICIs as a class, and anti-PD-(L)1 agents in particular, have an important role to play in treatment of early-stage cancers in the neoadjuvant/adjuvant setting (10, 11, 58). At the same time, more work is needed on biomarkers (e.g., immune checkpoint protein expression and tumor mutational burden) as well as prognostic methods to identify the patients most likely to benefit from neoadjuvant/adjuvant treatment.
4.1 Limitations
Two limitations must be considered when interpreting the results of this analysis. First, we used a 10-year time horizon. This likely underestimated the full value of anti-PD-(L)1 agents, and a longer time horizon is warranted to fully capture the range of health benefits experienced by patients. Second, the knowledge base regarding new immunotherapies is rapidly evolving, and additional real-world studies of ICIs in melanoma, and especially RCC and TNBC, where there is currently little information, will be needed to support changes in treatment policy and verify their effects.
4.2 Conclusions
The use of anti-PD-(L)1 agents in the treatment of early-stage cancers is estimated to result in better health outcomes in Switzerland by reducing the number of recurrences and deaths, extending the time patients spend free of recurrences/events/disease, and reducing the number of treatments for metastatic disease. These findings can help policymakers weigh the benefits of incorporating anti-PD-(L)1 agents into treatment guidelines for early-stage cancer and support discussions around investment in anti-PD-(L)1 agents in the adjuvant/neoadjuvant setting.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Author contributions
AF-B: Formal analysis, Conceptualization, Methodology, Writing – review & editing, Data curation, Writing – original draft. MS: Writing – review & editing, Data curation. TM: Methodology, Validation, Conceptualization, Formal analysis, Writing – review & editing. CF: Data curation, Writing – review & editing. SS: Writing – review & editing, Data curation. SG: Data curation, Writing – review & editing. DS: Methodology, Writing – review & editing, Writing – original draft, Data curation, Formal analysis. RA-I: Methodology, Writing – original draft, Conceptualization, Validation, Writing – review & editing, Formal analysis.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. Funding for this research was provided by Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc., Rahway, NJ, USA. The funders of the study had a role in study design, collection, analysis, interpretation of the data, the writing of this article or the decision to submit it for publication.
Acknowledgments
The authors thank Melissa Stauffer, PhD, in collaboration with ScribCo, for medical writing assistance.
Conflict of interest
AF-B, MS, CF, SS, and SG are employees of MSD Switzerland, a subsidiary of Merck & Co., Inc., Rahway, NJ, USA. TM is an employee of Lumanity and received financial support via employment institution from MSD, a subsidiary of Merck & Co., Inc., Rahway, NJ, USA. DS is an employee of MSD Sweden, a subsidiary of Merck & Co., Inc., Rahway, NJ, USA. RA-I is an employee of Merck Canada Inc., a subsidiary of Merck & Co., Inc., Rahway, NJ, USA.
The authors declare that this study received funding from Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc., Rahway, NJ, USA. The funder was involved in the study design, collection, analysis, interpretation of data, the writing of this article and the decision to submit it for publication.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2025.1601377/full#supplementary-material
References
1. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2021) 71:209–49. doi: 10.3322/caac.21660
2. European Commission. Cancer. Available online at: https://health.ec.europa.eu/non-communicable-diseases/cancer_en (Accessed September 1, 2023).
3. World Health Organization. Cancer. Available online at: https://www.who.int/news-room/fact-sheets/detail/cancer (Accessed September 1, 2023).
4. Krebsliga Schweiz. Krebs in der Schweiz: wichtige Zahlen. Available online at: https://www.krebsliga.ch/ueber-krebs/zahlen-fakten/-dl-/fileadmin/downloads/sheets/zahlen-krebs-in-der-schweiz.pdf (Accessed November 30, 2023).
5. Wanner M, Matthes KL, Karavasiloglou N, Limam M, Korol D, and Rohrmann S. 37-year incidence and mortality time trends of common cancer types by sex, age, and stage in the canton of Zurich. Swiss Med Wkly. (2020) 150:w20388. doi: 10.4414/smw.2020.20388
6. Kantonsspital Baselland. Blasenkrebs - Kurz und Bündig. Available online at: https://www.ksbl.ch/kliniken/urologie/leistungen/blasenkrebs (Accessed March 5, 2024).
7. Ortega-Ortega M, Hanly P, Pearce A, Soerjomataram I, and Sharp L. Projected impact on labour productivity costs of cancer-related premature mortality in Europe 2018-2040. Appl Health Econ Health Policy. (2023) 21:877–89. doi: 10.1007/s40258-023-00824-6
8. National Cancer Institute. Immune Checkpoint Inhibitors. Available online at: https://www.cancer.gov/about-cancer/treatment/types/immunotherapy/checkpoint-inhibitors (Accessed October 2, 2023).
9. Poklepovic AS and Luke JJ. Considering adjuvant therapy for stage II melanoma. Cancer. (2020) 126:1166–74. doi: 10.1002/cncr.v126.6
10. Yang T, Li W, Huang T, and Zhou J. Immunotherapy targeting PD-1/PD-L1 in early-stage triple-negative breast cancer. J Pers Med. (2023) 13(3):526. doi: 10.3390/jpm13030526
11. Deleuze A, Saout J, Dugay F, Peyronnet B, Mathieu R, Verhoest G, et al. Immunotherapy in renal cell carcinoma: the future is now. Int J Mol Sci. (2020) 21(7):2532. doi: 10.3390/ijms21072532
12. Aguiar-Ibáñez R, Sharma S, Chawla E, Immadisetty L, Simon S, and Aktan G. CO208 recurrence rates and survival among patients with early-stage cancers: A systematic literature review. Value Health. (2023) 26. doi: 10.1016/j.jval.2023.03.2433
13. Haas NB, Bhattacharya R, Song Y, Rogerio J, Zhang S, Carley C, et al. Variation in recurrence rate and overall survival (OS) outcomes by disease stage and incremental impact of time to recurrence on OS in localized renal cell carcinoma (RCC). J Clin Oncol. (2022) 40:4543. doi: 10.1200/JCO.2022.40.16_suppl.4543
14. Jovanoski N, Bowes K, Brown A, Belleli R, Di Maio D, Chadda S, et al. Survival and quality-of-life outcomes in early-stage NSCLC patients: a literature review of real-world evidence. Lung Cancer Manag. (2023) 12:LMT60. doi: 10.2217/lmt-2023-0003
15. West H, Hu X, Chirovsky D, Walker MS, Wang Y, Kaushiva A, et al. Clinical and economic impact of recurrence in early-stage non-small-cell lung cancer following complete resection. Future Oncol. (2023) 19:1415–27. doi: 10.2217/fon-2023-0024
16. West H, Hu X, Zhang S, Song Y, Chirovsky D, Gao C, et al. Treatment patterns and outcomes in resected early-stage non-small cell lung cancer: an analysis of the SEER-medicare data. Clin Lung Cancer. (2023) 24:260–8. doi: 10.1016/j.cllc.2022.12.005
17. Aguiar-Ibanez R, Neves C, Mantaian T, Abreu A, Sonmez D, Sillah A, et al. CO26 impact in health outcomes of anti-PD(L)1 inhibitors to treat early-stage cancers in Belgium. Value Health. (2023) 26:S18–9. doi: 10.1016/j.jval.2023.03.100
18. Merck Sharp & Dohme LLC. Study of Pembrolizumab (MK-3475) Versus Placebo After Complete Resection of High-Risk Stage III Melanoma (MK-3475-054/1325-MG/KEYNOTE-054). Clinicaltrials.gov (2023). Available at: https://clinicaltrials.gov/study/NCT02362594 (Accessed October 2, 2023).
19. Merck Sharp & Dohme LLC. Safety and Efficacy Study of Pembrolizumab (MK-3475) as Monotherapy in the Adjuvant Treatment of Renal Cell Carcinoma Post Nephrectomy (MK-3475-564/KEYNOTE-564). clinicaltrials.gov (2023). Available at: https://clinicaltrials.gov/study/NCT03142334 (Accessed October 2, 2023).
20. Merck Sharp & Dohme LLC. Study of Pembrolizumab (MK-3475) Plus Chemotherapy vs Placebo Plus Chemotherapy as Neoadjuvant Therapy and Pembrolizumab vs Placebo as Adjuvant Therapy in Participants With Triple Negative Breast Cancer (TNBC) (MK-3475-522/KEYNOTE-522). clinicaltrial.gov. Available at: https://clinicaltrials.gov/study/NCT03036488 (Accessed October 2, 2023).
21. Federal Office of Statistics. NKRS - Neuerkrankungen. Krebsinzidenz 1990-2019: Neuerkrankungen, Raten und Entwicklung pro Krebslokalisation u. Periode. Available online at: https://www.bfs.admin.ch/asset/de/23566688 (Accessed February 28, 2023).
22. European Medicines Agency. KEYTRUDA: Summary of Product Characteristics. Available online at: https://www.ema.europa.eu/en/documents/product-information/keytruda-epar-product-information_en.pdf (Accessed May 18, 2022).
23. European Medicines Agency. OPDIVO: Summary of Product Characteristics. Available online at: https://www.ema.europa.eu/en/documents/product-information/opdivo-epar-product-information_en.pdf (Accessed May 19, 2022).
24. Favre-Bulle A, Bencina G, Zhang S, Jiang R, Andritschke D, and Bhadhuri A. Cost-effectiveness of pembrolizumab as an adjuvant treatment for patients with resected stage IIB or IIC melanoma in Switzerland. J Med Econ. (2023) 26:283–92. doi: 10.1080/13696998.2023.2174748
25. Favre-Bulle A, Huang M, Haiderali A, and Bhadhuri A. Cost-effectiveness of neoadjuvant pembrolizumab plus chemotherapy followed by adjuvant pembrolizumab in patients with high-risk, early-stage, triple-negative breast cancer in Switzerland. Pharmacoecon Open. (2024) 8:91–101. doi: 10.1007/s41669-023-00445-8
26. Huang M, AF P, Haiderali A, Xue W, Yang C, Pan W, et al. Cost-effectiveness of neoadjuvant pembrolizumab plus chemotherapy followed by adjuvant single-agent pembrolizumab for high-risk early-stage triple-negative breast cancer in the United States. Adv Ther. (2023) 40:1153–70. doi: 10.1007/s12325-022-02365-1
27. Lai Y, Bensimon AG, Gao E, Bhattacharya R, Xu R, Chevure J, et al. Cost-effectiveness analysis of pembrolizumab as an adjuvant treatment of renal cell carcinoma post-nephrectomy in the United States. Clin Genitourin Cancer. (2023) 21:612.e1–e11. doi: 10.1016/j.clgc.2023.03.016
28. Schur N, Favre-Bulle A, Flori M, Xiao Y, and Lupatsch JE. Cost-effectiveness of pembrolizumab as an adjuvant treatment of renal cell carcinoma post-nephrectomy in Switzerland. J Med Econ. (2024) 27:1389–97. doi: 10.1080/13696998.2024.2417523
29. National Institute for Health and Care Excellence (NICE). Pembrolizumab for adjuvant treatment of completely resected stage3 melanoma [TA766]. Available online at: https://www.nice.org.uk/guidance/ta766 (Accessed September 1, 2023).
30. National Institute for Health and Care Excellence (NICE). Pembrolizumab for adjuvant treatment of renal cell carcinoma [TA830]. Available online at: https://www.nice.org.uk/guidance/ta830 (Accessed September 1, 2023).
31. National Institute for Health and Care Excellence (NICE). Pembrolizumab for neoadjuvant and adjuvant treatment of triple-negative early or locally advanced breast cancer [TA851]. Available online at: https://www.nice.org.uk/guidance/ta851 (Accessed September 1, 2023).
32. Ara R and Brazier JE. Populating an economic model with health state utility values: moving toward better practice. Value Health. (2010) 13:509–18. doi: 10.1111/j.1524-4733.2010.00700.x
33. Merck Sharp & Dohme LLC. Study to Evaluate the Safety and Efficacy of Two Different Dosing Schedules of Pembrolizumab (MK-3475) Compared to Ipilimumab in Participants With Advanced Melanoma (MK-3475-006/KEYNOTE-006). clinicaltrials.gov (2020). Available at: https://clinicaltrials.gov/study/NCT01866319 (Accessed October 2, 2023).
34. Callahan MK, Kluger H, Postow MA, Segal NH, Lesokhin A, Atkins MB, et al. Nivolumab plus ipilimumab in patients with advanced melanoma: updated survival, response, and safety data in a phase I dose-escalation study. J Clin Oncol. (2018) 36:391–8. doi: 10.1200/JCO.2017.72.2850
35. Hodi FS, Chesney J, Pavlick AC, Robert C, Grossmann KF, McDermott DF, et al. Combined nivolumab and ipilimumab versus ipilimumab alone in patients with advanced melanoma: 2-year overall survival outcomes in a multicentre, randomised, controlled, phase 2 trial. Lancet Oncol. (2016) 17:1558–68. doi: 10.1016/S1470-2045(16)30366-7
36. Long GV, Stroyakovskiy D, Gogas H, Levchenko E, de Braud F, Larkin J, et al. Dabrafenib and trametinib versus dabrafenib and placebo for Val600 BRAF-mutant melanoma: a multicentre, double-blind, phase 3 randomised controlled trial. Lancet. (2015) 386:444–51. doi: 10.1016/S0140-6736(15)60898-4
37. Robert C, Long GV, Brady B, Dutriaux C, Maio M, Mortier L, et al. Nivolumab in previously untreated melanoma without BRAF mutation. N Engl J Med. (2015) 372:320–30. doi: 10.1056/NEJMoa1412082
38. Ascierto PA, Kirkwood JM, Grob JJ, Simeone E, Grimaldi AM, Maio M, et al. The role of BRAF V600 mutation in melanoma. J Transl Med. (2012) 10:85. doi: 10.1186/1479-5876-10-85
39. Chapman PB, Hauschild A, Robert C, Haanen JB, Ascierto P, Larkin J, et al. Improved survival with vemurafenib in melanoma with BRAF V600E mutation. N Engl J Med. (2011) 364:2507–16. doi: 10.1056/NEJMoa1103782
40. Ribas A, Hodi FS, Kurland JF, Shahabi V, Francis S, Konto C, et al. CA184-161: A phase I/II trial of vemurafenib and ipilimumab in patients with BRAF V600 mutation-positive metastatic melanoma. J Clin Oncol. (2012) 30. doi: 10.1200/jco.2012.30.15_suppl.tps8603
41. Merck Sharp & Dohme LLC. Study to Evaluate the Efficacy and Safety of Pembrolizumab (MK-3475) in Combination With Axitinib Versus Sunitinib Monotherapy in Participants With Renal Cell Carcinoma (MK-3475-426/KEYNOTE-426). clinicaltrials.gov (2022). Available at: https://clinicaltrials.gov/study/NCT02853331 (Accessed October 2, 2023).
42. Motzer RJ, Penkov K, Haanen J, Rini B, Albiges L, Campbell MT, et al. Avelumab plus Axitinib versus Sunitinib for Advanced Renal-Cell Carcinoma. N Engl J Med. (2019) 380:1103–15. doi: 10.1056/NEJMoa1816047
43. Choueiri TK, Hessel C, Halabi S, Sanford B, Michaelson MD, Hahn O, et al. Cabozantinib versus sunitinib as initial therapy for metastatic renal cell carcinoma of intermediate or poor risk (Alliance A031203 CABOSUN randomised trial): Progression-free survival by independent review and overall survival update. Eur J Cancer. (2018) 94:115–25. doi: 10.1016/j.ejca.2018.02.012
44. Motzer RJ, Hutson TE, Cella D, Reeves J, Hawkins R, Guo J, et al. Pazopanib versus sunitinib in metastatic renal-cell carcinoma. N Engl J Med. (2013) 369:722–31. doi: 10.1056/NEJMoa1303989
45. Motzer RJ, Nosov D, Eisen T, Bondarenko I, Lesovoy V, Lipatov O, et al. Tivozanib versus sorafenib as initial targeted therapy for patients with metastatic renal cell carcinoma: results from a phase III trial. J Clin Oncol. (2013) 31:3791–9. doi: 10.1200/JCO.2012.47.4940
46. Motzer RJ, Tannir NM, McDermott DF, Aren Frontera O, Melichar B, Choueiri TK, et al. Nivolumab plus Ipilimumab versus Sunitinib in Advanced Renal-Cell Carcinoma. N Engl J Med. (2018) 378:1277–90. doi: 10.1056/NEJMoa1712126
47. Choueiri TK, Powles T, Burotto M, Escudier B, Bourlon MT, Zurawski B, et al. Nivolumab plus Cabozantinib versus Sunitinib for Advanced Renal-Cell Carcinoma. N Engl J Med. (2021) 384:829–41. doi: 10.1056/NEJMoa2026982
48. Merck Sharp & Dohme LLC. Study of Pembrolizumab (MK-3475) Plus Chemotherapy vs. Placebo Plus Chemotherapy for Previously Untreated Locally Recurrent Inoperable or Metastatic Triple Negative Breast Cancer (MK-3475-355/KEYNOTE-355). clinicaltrials.gov (2022). Available at: https://clinicaltrials.gov/study/NCT02819518 (Accessed October 2, 2023).
49. Li YH, Zhou Y, Wang YW, Tong L, Jiang RX, Xiao L, et al. Comparison of apatinib and capecitabine (Xeloda) with capecitabine (Xeloda) in advanced triple-negative breast cancer as third-line therapy: A retrospective study. Med (Baltimore). (2018) 97:e12222. doi: 10.1097/MD.0000000000012222
50. Schmid P, Adams S, Rugo HS, Schneeweiss A, Barrios CH, Iwata H, et al. Atezolizumab and nab-paclitaxel in advanced triple-negative breast cancer. N Engl J Med. (2018) 379:2108–21. doi: 10.1056/NEJMoa1809615
51. Yardley DA, Coleman R, Conte P, Cortes J, Brufsky A, Shtivelband M, et al. nab-Paclitaxel plus carboplatin or gemcitabine versus gemcitabine plus carboplatin as first-line treatment of patients with triple-negative metastatic breast cancer: results from the tnAcity trial. Ann Oncol. (2018) 29:1763–70. doi: 10.1093/annonc/mdy201
52. Merck Sharp & Dohme LLC. Study of Pembrolizumab (MK-3475) Versus Chemotherapy in Participants With Advanced Melanoma (MK-3475-002/P08719/KEYNOTE-002). clinicaltrials.gov (2020). Available at: https://clinicaltrials.gov/study/NCT01704287 (Accessed October 2, 2023).
53. Mangana J, Zihler D, Bossart S, Bronnimann D, Zachariah R, and Gerard CL. Treatment reality of patients with BRAF-mutant advanced/metastatic melanoma in Switzerland in the era of choice. Melanoma Res. (2022) 32:366–72. doi: 10.1097/CMR.0000000000000843
54. Hoffmann M, Hayoz S, and Ozdemir BC. Prescription patterns, recurrence, and toxicity rates of adjuvant treatment for stage III/IV melanoma-A real world single-center analysis. Biol (Basel). (2022) 11(3):422. doi: 10.3390/biology11030422
55. Wahli MN, Hayoz S, Hoch D, Ryser CO, Hoffmann M, Scherz A, et al. The role of immune checkpoint inhibitors in clinical practice: an analysis of the treatment patterns, survival and toxicity rates by sex. J Cancer Res Clin Oncol. (2023) 149:3847–58. doi: 10.1007/s00432-022-04309-2
56. Wanner M, Syleouni ME, Karavasiloglou N, Limam M, Bastiaannet E, Korol D, et al. Time-trends and age and stage differences in 5-year relative survival for common cancer types by sex in the canton of Zurich, Switzerland. Cancer Med. (2023) 12:18165–75. doi: 10.1002/cam4.v12.17
57. Mangana J, Cheng PF, Kaufmann C, Amann VC, Frauchiger AL, Stogner V, et al. Multicenter, real-life experience with checkpoint inhibitors and targeted therapy agents in advanced melanoma patients in Switzerland. Melanoma Res. (2017) 27:358–68. doi: 10.1097/CMR.0000000000000359
58. Dibajnia P, Cardenas LM, and Lalani AA. The emerging landscape of neo/adjuvant immunotherapy in renal cell carcinoma. Hum Vaccin Immunother. (2023) 19:2178217. doi: 10.1080/21645515.2023.2178217
59. Federal Statistical Office. Population (2022). Available online at: https://www.bfs.admin.ch/bfs/en/home/statistics/population.html (Accessed April 4, 2023).
Keywords: immune checkpoint inhibitors, melanoma, nivolumab, pembrolizumab, renal cell carcinoma, triple-negative breast cancer
Citation: Favre-Bulle A, Stanković M, Mantaian T, Frei C, Schaefer S, Gabriel SS, Sönmez D and Aguiar-Ibáñez R (2025) Health impact of using anti-PD-(L)1 agents to treat early-stage cancers in Switzerland: a modeling study. Front. Immunol. 16:1601377. doi: 10.3389/fimmu.2025.1601377
Received: 28 March 2025; Accepted: 05 June 2025;
Published: 03 July 2025.
Edited by:
Claude Lambert, Centre Hospitalier Universitaire (CHU) de Saint-Étienne, FranceReviewed by:
Biljana Bufan, University of Belgrade, SerbiaJorge J. Nieva, University of Southern California, United States
Copyright © 2025 Favre-Bulle, Stanković, Mantaian, Frei, Schaefer, Gabriel, Sönmez and Aguiar-Ibáñez. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Andrea Favre-Bulle, YW5kcmVhLmZhdnJlLWJ1bGxlLnBhbnRvamFAbXNkLmNvbQ==
†ORCID: Sarah Sharon Gabrie, orcid.org/0000-0002-6359-485X