 Eulàlia Solà-Porta1
Eulàlia Solà-Porta1 Dolores Redondo-Pachón1,2Jorge Eguía-Núñez3
Dolores Redondo-Pachón1,2Jorge Eguía-Núñez3 Anna Buxeda1,2
Anna Buxeda1,2 José Luís Caro4Javier Gimeno5Luís Campuzano1
José Luís Caro4Javier Gimeno5Luís Campuzano1 Carla Burballa1,2Betty Chamoun2
Carla Burballa1,2Betty Chamoun2 Sara Sanz-Ureña1Judith Federico-Vega1
Sara Sanz-Ureña1Judith Federico-Vega1 Elisenda Alari-Pahissa1Julio Pascual1,6
Elisenda Alari-Pahissa1Julio Pascual1,6 María José Pérez-Sáez1,2†
María José Pérez-Sáez1,2† Marta Crespo1,2*†
Marta Crespo1,2*†- 1Nephropathy Research Group, Hospital del Mar Medical Research Institute, Barcelona, Spain
- 2Department of Nephrology, Hospital del Mar, Barcelona, Spain
- 3Immunology Department, Laboratori de Referència de Catalunya SA, El Prat de Llobregat, Spain
- 4Immunology Department, Hospital Clinic, Barcelona, Spain
- 5Department of Pathology, Hospital del Mar, Barcelona, Spain
- 6Department of Nephrology, Hospital Universitario 12 de Octubre, Madrid, Spain
Introduction: Donor-specific human leukocyte antigens antibodies (HLA-DSA) contribute toantibody-mediated rejection (ABMR) after kidney transplantation (KT). Non-HLA antibodies may play a role in ABMR in the presence of HLA-DSA or the development of microvascular inflammation (MVI) in its absence. Considering both types of antibodies in potential recipients could enhance ABMR/MVI risk assessment.
Methods: We present a case-control study of 121 KT recipients, 46 with ABMR/ MVI diagnosis, and 75 control cases with available sera before and after KT, follow-up HLA antibody monitoring, and biopsies. We determined 60 serum non-HLA antibodies using a multiplex test with an established cutoff. We evaluated their association with ABMR/MVI using a sample median fluorescence intensity (MFI) ratio sum.
Results: Following commercial cutoffs, non-HLA antibodies were detected in 87% of the patients before KT. We found that a high non-HLA antibody MFI ratio sum before KT and at biopsy were associated with an increased risk of ABMR/MVI, independently of HLA sensitization or HLA-DSA (OR = 1.039, p = 0.014 and OR = 1.036, p = 0.024). Antibodies against extracellular non-HLA antigens were associated with ABMR/MVI before KT (OR = 1.053, p = 0.040), but at diagnosis, only antibodies against intracellular non-HLA antigens were associated (OR = 1.062, p = 0.018).
Conclusion: These findings suggest that non-HLA antibody assessment offers valuable complementary information, regardless of HLA sensitization, though appropriate cut-offs should be explored.
Introduction
In kidney transplantation (KT), antibody-mediated rejection (ABMR) remains a barrier to long-term graft survival (1, 2). Donor-specific antibodies (DSA) against human leukocyte antigens (HLA) are central to the pathogenesis of ABMR by triggering endothelial damage and complement activation, innate and adaptive immune responses, and intracellular pathways (3–7). The presence of HLA-DSA, both before and after transplantation, has been strongly associated with ABMR and graft loss (8–10).
The 2017 and 2019 Banff classifications defined ABMR based on compatible histology and histological signs of interaction between the endothelia and antibodies—such as microvascular inflammation (MVI)—in the presence of HLA-DSA or C4d deposits in peritubular capillaries (11, 12). However, ABMR damage can occur even in the absence of detectable HLA-DSA, with antibody involvement inferred from complement activation (13). A subset of patients presents with isolated MVI in the absence of HLA-DSA or complement activation. Although not categorized in these Banff classifications, this pattern of damage influences graft survival (7, 14, 15) and shares certain injury mechanisms with AMBR (7, 16), although not all. The most recent Banff 2022 classification (17) now includes these patients under Category 2, as a subcategory termed MVI, DSA-negative, and C4d-negative.
There has been a growing interest in the potential role of antibodies directed against non-HLA molecules in ABMR (18). Initial studies employed tests that allowed the evaluation of reactions against specific targets such as the major histocompatibility complex class I-related chain A (MICA), angiotensin receptor 1, and endothelin receptor, among others. Although these antibodies have been variably associated with graft outcomes, none of them has shown as strong a correlation with ABMR as HLA-DSA (19–21).
The damage mechanisms of non-HLA antibodies appear to involve a mixture of alloimmune and autoimmune responses depending on each antigen (22). Some antigens induce an alloimmune response based on a non-HLA genetic mismatch between donor and recipient, such as antibodies against MICA or anti-glutathione S-transferase theta 1 (GSTT1) (23). In contrast, most non-HLA antigens seem to induce an autoimmune reaction, as shown in the case of antibodies against self-molecules like angiotensin type 1 receptor, endothelin receptor, or rho GDP dissociation inhibitor beta (24). This raises important questions about why these antibodies target the kidney graft specifically, but not the native kidneys or other organs (25).
The growing identification of non-HLA targets has driven the development of novel and user-friendly detection tests leveraging versatile technology. Multiplex bead panels and antibody detection immunoassays now enable simultaneous testing of multiple non-HLA targets. Using these tools, recent studies have focused on the overall non-HLA antibody burden and its impact on ABMR and graft survival (26–30). Several unresolved questions remain (31), such as which non-HLA antibodies should be included in a multiplex panel, and at what stage in the transplant process should be tested.
In this study, we aimed to characterize a set of non-HLA antibodies in KT recipients with ABMR/MVI and compare them to a control group. Our objective was to evaluate their potential association with ABMR/MVI development paralleling current immune risk assessment strategies based on the patient’s HLA antibody sensitization while on the waiting list.
Materials and methods
Study design and study population
We conducted an observational case-control study that included KT recipients who underwent KT at Hospital del Mar, Barcelona, Spain. The case group included 46 patients who were transplanted between 2006 and 2019, diagnosed with ABMR/MVI (23 with detectable HLA-DSA at diagnosis and 23 without), and with available follow-up protocol or indication biopsies and serum samples both before KT and at the time of the biopsies. The control group consisted of 75 patients selected from a cohort of 131 consecutive KT recipients who were transplanted between 2013 and 2018 at the same center. Eligible controls had available protocol or indication biopsies at 1 and 3 years after KT and serum samples collected before KT and at the time of each biopsy. Patients with damage (Categories 2, 3, 4, and MVI of the Banff 2017 classification) in one or both biopsies were excluded.
The final study population included 121 patients: 46 cases with ABMR/MVI and 75 control cases without damage (Figure 1). For the present analysis, only sera and biopsies 1 year after KT were considered from control cases, knowing that later biopsies did not show ABMR/MVI either. Patients’ serum samples were tested for HLA and non-HLA antibodies before KT and at the time of biopsy.
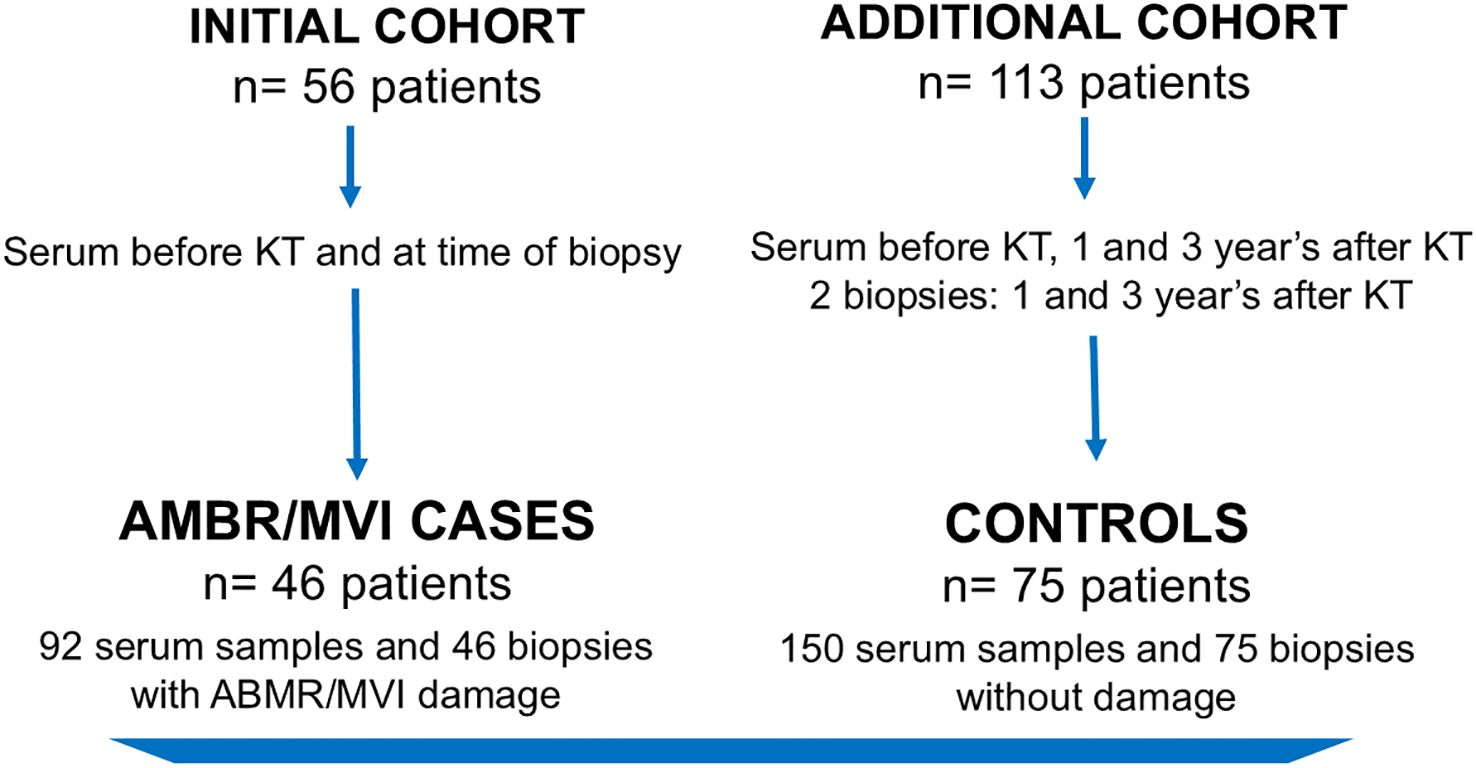
Figure 1. Population flow chart.
HLA antibody detection technique
HLA antibody analysis was performed as previously described (9). In brief, serum samples were first evaluated with screening kits using Lifecodes LifeScreen Deluxe assay (Immucor GTI Diagnostics, Inc®). Depending on the screening positivity for class I or II, further analysis was performed using Lifecodes LSA Class I and/or Class II test (Immucor GTI Diagnostics, Inc®), according to the manufacturer’s instructions. Finally, samples were analyzed on a Luminex 200 (Bio-Rad Luminex®) using Bio-Plex Manager 6.2 for data acquisition and Match It! Antibody v.1.1.0.2 for analysis. The bead was considered positive when at least two of the following values were exceeded: background corrected median fluorescence intensity calculated for each bead >1,000, background corrected ratio >5, and antigen density background corrected ratio >5 under review by two researchers (DRP and JE).
Non-HLA antibody detection technique
Non-HLA antibodies in serum were analyzed with a Lifecodes multiplex bead panel by Immucor® GTI Diagnostics, Inc. (lot num. 3010187) comprising 60 non-HLA antigens conjugated to polystyrene beads (Supplementary Table 1). Forty microliters of non-HLA beads and 10 µl of patient serum were added to each well and then incubated on a rotating platform for 30 min in the dark at room temperature. After incubation, wells were washed to remove unbound antibodies, and 50 µl of a previously diluted phycoerythrin-conjugated anti-human IgG (5 µl of conjugate diluted with 45 µl of wash buffer) was added and further incubated for 30 min in the dark on a rotating platform at room temperature. Samples were analyzed on a Luminex 200 (Bio-Rad Luminex®), and a median fluorescence intensity (MFI) was obtained for each bead.
According to manufacturer instructions, a background corrected MFI and MFI ratio with the cutoff value defined by the manufacturer (MFI/cutoff value) was calculated for each target antigen. Non-HLA antibodies were considered positive when the background corrected MFI value was above the given cutoff, and the MFI ratio was equal to or above 1. For each sample, an absolute count of positive non-HLA antibodies was calculated, as well as an intensity count based on the total sum of the MFI ratio values (MFI/cutoff value) of the positive non-HLA antibodies.
The 60 non-HLA antibodies included in the panel and the cutoffs given by the manufacturer are listed in Supplementary Table 1.
Biopsies
All biopsies were reviewed and retrospectively scored by one pathologist using the Banff 2017 classification and allocated to any of the six Banff diagnostic categories in agreement with researchers (JG, DRP, and AB). Biopsies were categorized as ABMR/MVI for this study when they fulfilled the biopsy diagnosis of ABMR (Banff category 2) or had MVI (glomerulitis and/or peritubular capillaritis ≥2) in the absence of HLA-DSA.
Variables
Clinical data were collected from our local transplant database, including baseline demographic characteristics, transplant characteristics, and periodically registered clinical follow-up variables. For immunological sensitization evaluation before KT, a calculated panel of reactive antibodies (cPRA), using HLA frequencies derived from local bone marrow donors active in Catalunya, was used for the study and clinical KT prioritizing programs. Patients were followed until graft loss (return to dialysis or retransplantation), death, and end of follow-up (1 July 2022).
Statistical analysis
Based on the data distribution, the results of quantitative variables are expressed as mean and standard deviation (SD) or as median and interquartile range (IQR). Categorical variables are described as counts and percentages. Comparisons between groups were done using the Student’s t-test for parametric continuous variables and the U Mann–Whitney test for non-parametric. For categorical variables, a chi-square test was used. Univariable and multivariable logistic regression analyses were used to evaluate odds ratios (ORs) for the occurrence of ABMR/MVI according to the MFI ratio sum and absolute number of non-HLA antibodies and for the individual non-HLA antibodies. Results are expressed as OR and 95% confidence interval (CI). A p-value <0.05 was considered statistically significant, while a p-value <0.1 was considered significant to be included in the multivariable analysis. Statistical analysis was performed using SPSS V 20 (SPSS Inc., Chicago, IL, USA).
Results
Population characteristics
The baseline demographics and clinical characteristics of the 121 patients included are presented in Table 1. A total number of 95 (78.5%) patients received a deceased kidney allograft, 15 (12.4%) underwent preemptive transplantation, and 11 (9.1%) received a repeated KT. Comparison between cases and controls, defined by the presence or absence of ABMR/MVI, showed no significant differences in recipient or donor demographics, except for a higher proportion of female recipients in the ABMR/MVI group (60.9% vs. 34.7%, p = 0.005). Regarding transplantation characteristics, we found, as expected, that patients in the ABMR/MVI group had a higher frequency of pretransplant HLA antibodies (cPRA over 50%, 28.3% vs. 9.3%, p = 0.007) and preformed HLA-DSA (19.6% vs. 2.7%, p = 0.002).
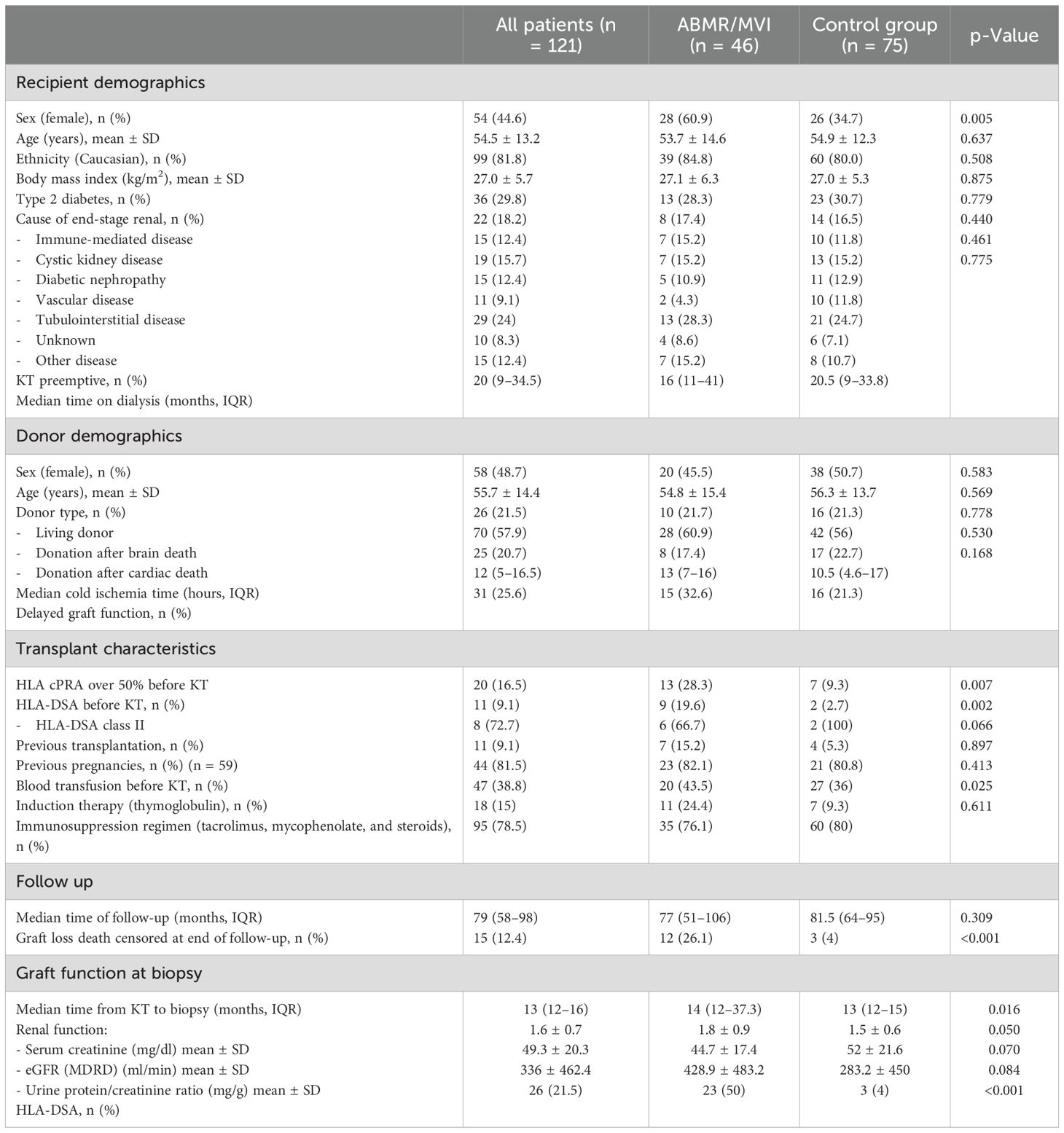
Table 1. Baseline characteristics.
Non-HLA antibodies before transplantation
Of the 121 patient serum samples analyzed before KT, 105 (87%) patients had one or more non-HLA antibodies according to the manufacturer’s cut-offs, with significantly higher prevalence in AMBR/MVI cases compared to controls (97.8% vs. 80%, p = 0.005). Patients had a median of 3 (IQR 1–4.5) non-HLA antibodies and a median MFI ratio sum of 11.7 (IQR 3.7–21.3). Both showed a logarithmic distribution (Figure 2). Compared to controls, patients with ABMR/MVI had a significantly higher number of non-HLA antibodies [median 4 (IQR 2–5) vs. 2 (IQR 1–4), p = 0.001] and a higher MFI ratio sum [median 14.4 (IQR 7.8–26.2) vs. 7.8 (IQR 1.8–16.8), p = 0.001].
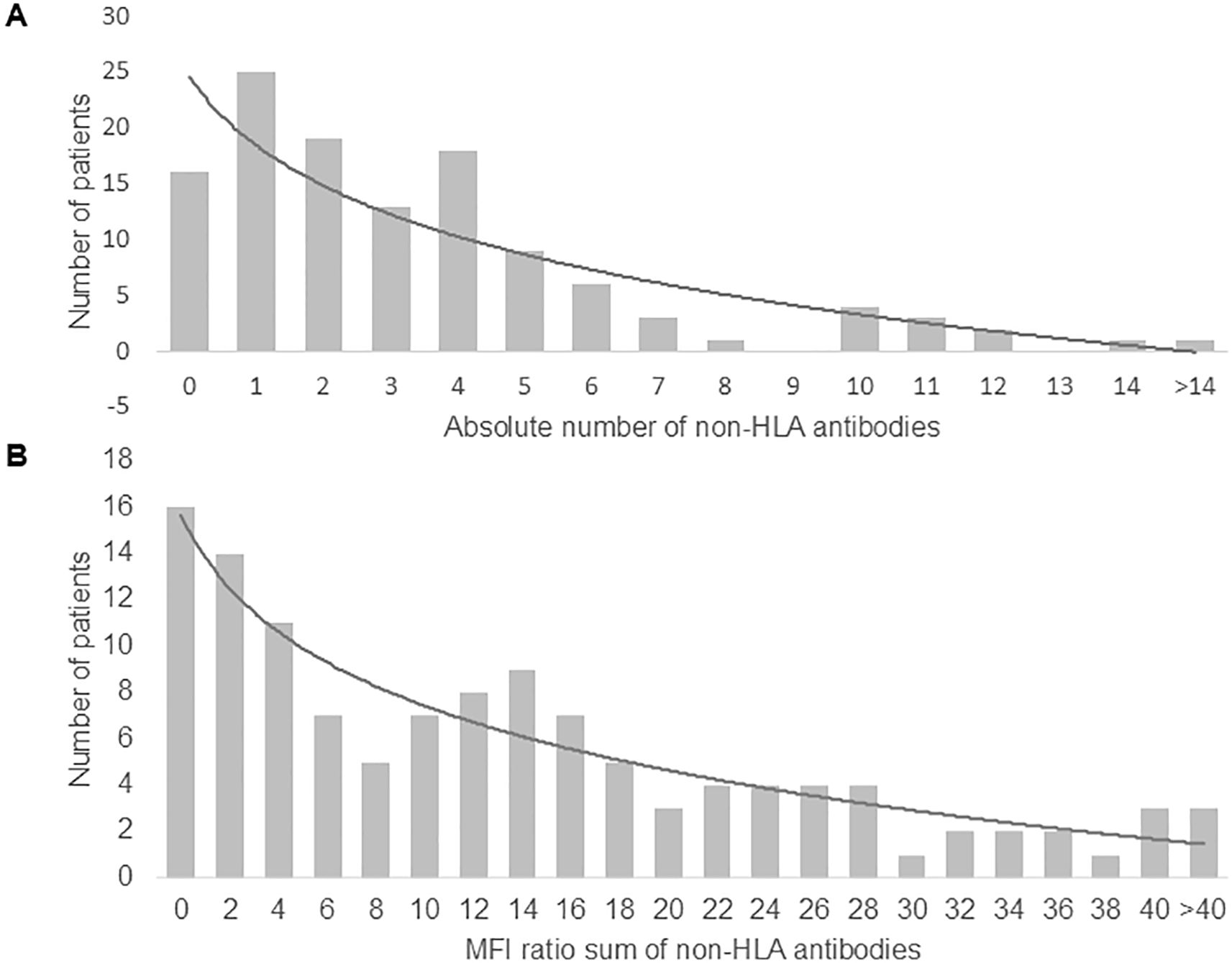
Figure 2. Distribution of patients with pretransplant non-HLA antibodies according to (A) the absolute number of non-HLA antibodies and (B) the MFI ratios sum of the positive non-HLA antibodies per patient.
To assess the association between non-HLA antibodies and ABMR/MVI risk, logistic regression analyses were performed, including the MFI ratio sum of non-HLA antibodies along with baseline and transplant characteristics. Patients with a higher non-HLA MFI ratio sum exhibited higher odds of developing ABMR/MVI [OR = 1.039, CI (95%) 1.008–1.072, p = 0.014], independently of their HLA sensitization status (HLA cPRA over 50% before KT), previous transplantation, and recipient sex (Table 2). This association remained significant after adjusting for the presence of HLA-DSA before KT confirming that the non-HLA antibody effect persists in this context (Supplementary Table 2A). Finally, an analysis using the absolute count of positive non-HLA antibodies yielded similar results (Supplementary Table 2B).
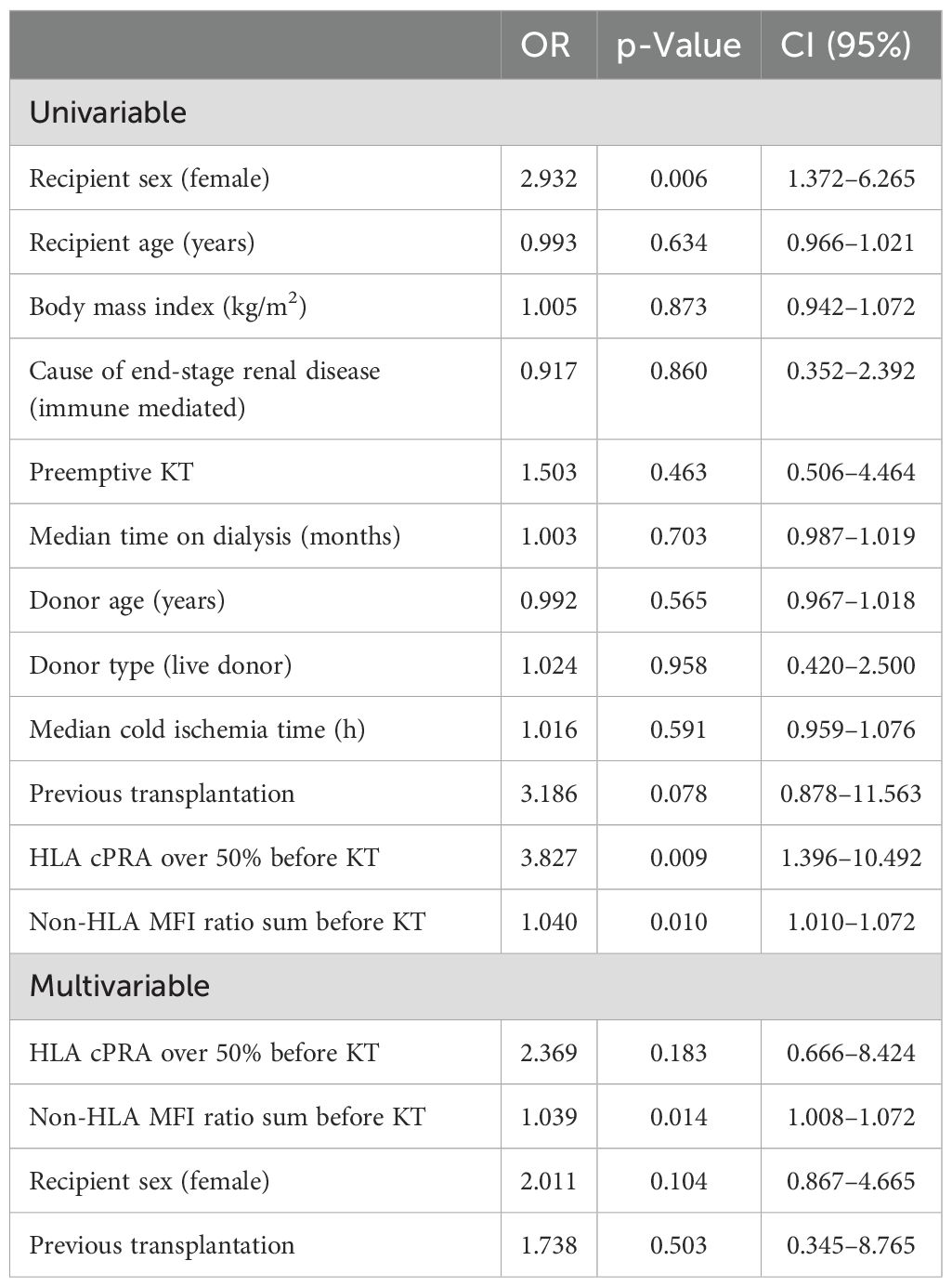
Table 2. Univariable and multivariable logistic regression analysis for ABMR/MVI development according to HLA and non-HLA antibodies before transplantation.
Aiming to elucidate the potential role of multiplex non-HLA tests in the KT recipient assessment, patients were stratified into quartiles based on the non-HLA antibody burden before KT (which combines the number and strength of antibodies). Patients in the fourth quartile of the non-HLA MFI ratio sum (MFI ratio sum >21.3) exhibited the highest odds of developing ABMR/MVI [OR = 5.033, CI (95%) 1.523–16.626, p = 0.008], independently of their HLA sensitization status before KT (Supplementary Table 2C). Among the patients with ABMR/MVI, 39.1% (n = 18) exhibited a non-HLA antibody MFI ratio sum >21.3 before KT (vs. 16% of the controls, p = 0.004) and 28.3% (n = 13) had an HLA cPRA over 50% (vs. 9.3% of the controls, p = 0.007) (Figure 3A). Among the cases with ABMR/MVI lacking detectable HLA and non-HLA antibodies before KT (n = 20), seven presented with de novo HLA-DSA at the time of biopsy diagnosis.
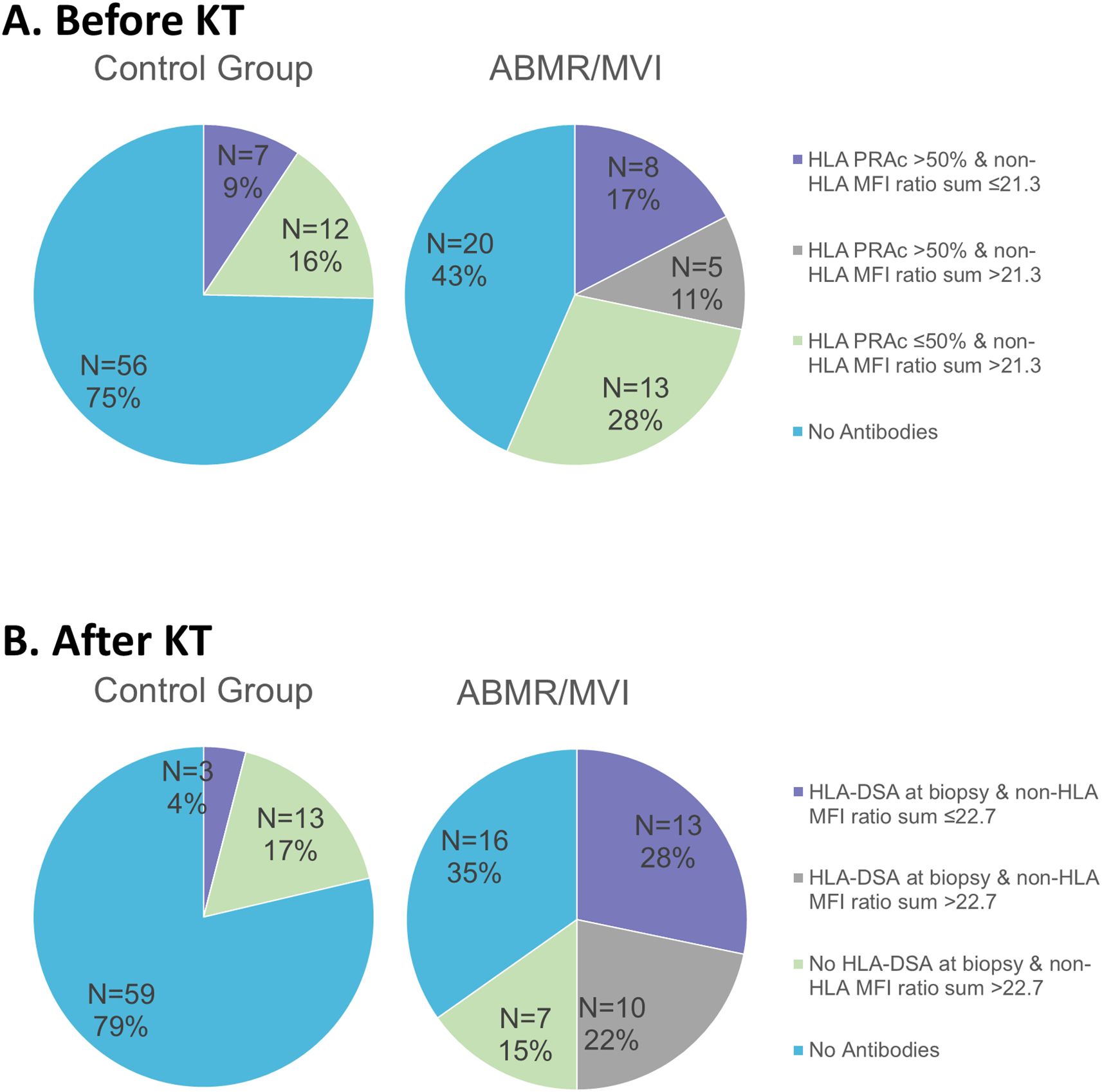
Figure 3. Clinical picture of ABMR/MVI and detection of HLA and non-HLA antibodies: (A) Before transplantation, (B) After transplantation.
We also analyzed whether the cellular localization of the non-HLA antigens could play a role in how the antibodies targeting them associate with the development of ABMR/MVI. The 60 non-HLA panel antigens were classified into extracellular (secreted or plasma membrane) and intracellular antigens (Supplementary Table 1). Logistic regression analyses showed that, before KT, the MFI ratio sum of extracellular, but not intracellular, non-HLA antigens was independently associated with higher odds of ABMR/MVI [OR = 1.053, CI (95%) 1.002–1.107, p = 0.040] (Table 3).
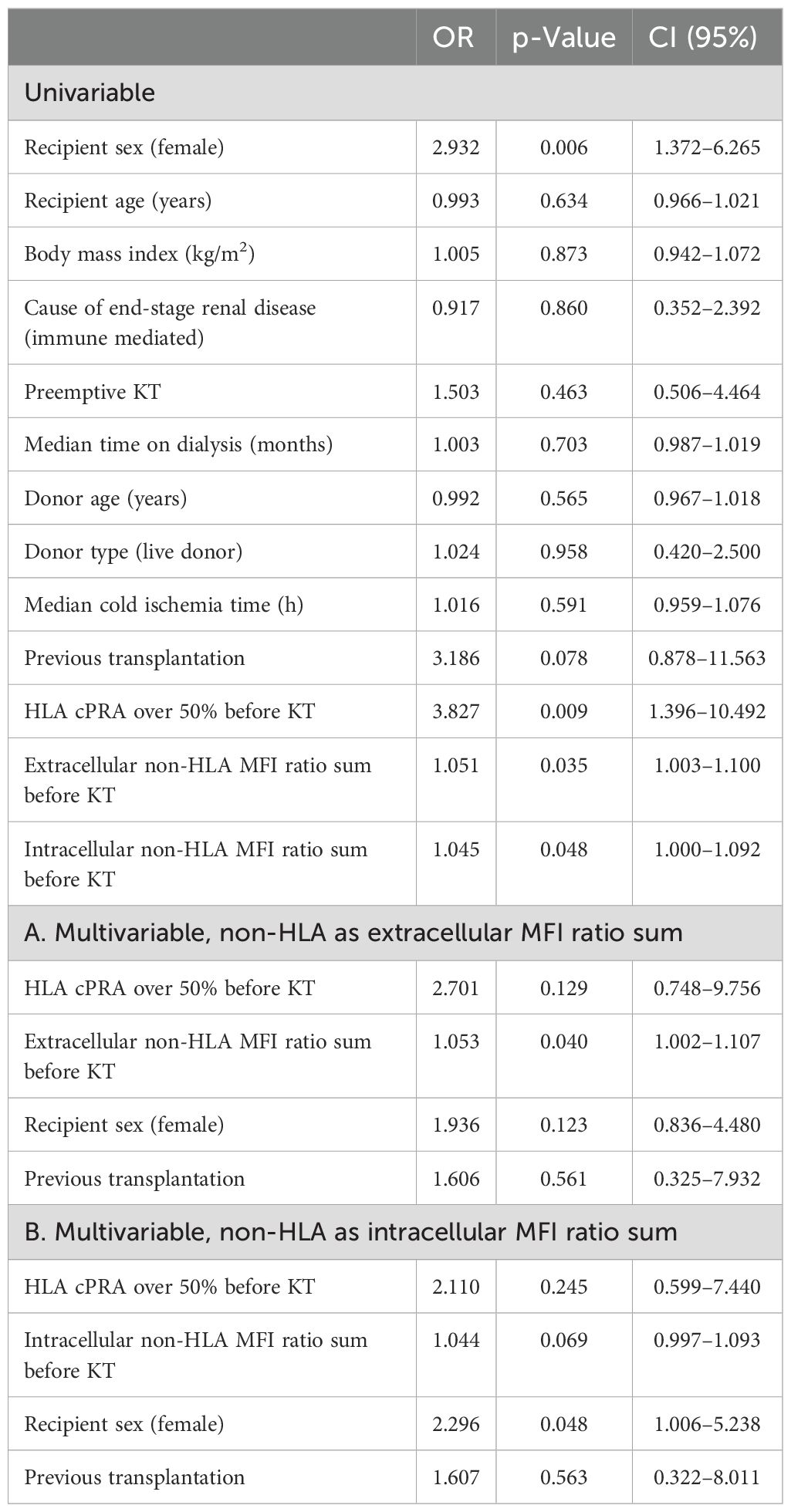
Table 3. Univariable and multivariable logistic regression analysis for ABMR/MVI development according to non-HLA antigen localization.
Last, we assessed the non-HLA impact on clinical outcomes. Patients in the fourth quartile of the non-HLA MFI ratio sum (>21.3) exhibited significantly worse graft function and proteinuria at biopsy time (Supplementary Table 3A). However, these associations were not significant after adjusting for ABMR/MVI diagnosis in a regression analysis. On graft survival, we found no association with high non-HLA ratio sum. In a Cox regression analysis, only ABMR/MVI diagnosis was significantly associated with graft loss [OR = 6.577, CI (95%) 1.830–23.631, p = 0.004] (Supplementary Table 3B).
When evaluating individual non-HLA antibodies before KT, 6 out of the 60 antibodies analyzed were significantly associated with ABMR/MVI in a univariable logistic regression analysis (p < 0.1, Supplementary Table 4). In a multivariable analysis including these six antibodies, along with the presence of an HLA cPRA over 50% before KT and clinical characteristics, we identified that only the detection of antibodies against GSTT1 remained independently associated with ABMR/MVI [OR = 3.664, CI (95%) 1.234–10.883, p = 0.019] (Table 4).

Table 4. Multivariable logistic regression analysis of pretransplant non-HLA antibodies significantly associated with ABMR/MVI and HLA sensitization.
Non-HLA antibodies after transplantation
At the time of biopsy, 103 of 121 patients (85.1%) had one or more non-HLA antibodies, similar to the proportion observed before KT (87%). Specifically, 96 (79%) of the KT recipients maintained the presence of non-HLA antibodies, 9 (7.4%) lost them, and 7 (5.8%) developed de novo non-HLA antibodies. There were no significant differences in the number of antibodies before and after KT (median 3, IQR 1–5; p = 0.722, Wilcoxon test), the MFI ratio sum [median before KT 11.7 (IQR 3.7–21.3) vs. after KT 11.6 (IQR 4.5–22.7); p = 0.767, Wilcoxon test], or its distribution (Supplementary Figure). Patients who developed de novo non-HLA antibodies after transplantation (n = 7) presented a lower non-HLA antibody number [median 2 (IQR 1–8) vs. 3 (IQR 2–6), p = 0.555] and MFI ratio sum [median 6.7 (IQR 4.6–29.8) vs. 14.37, IQR (6.9–23.1), p = 0.283] compared with persisting non-HLA antibodies, though not reaching statistical significance. Histological characteristics of biopsies are detailed in Supplementary Table 5.
Similar to the findings before KT, a higher non-HLA MFI ratio sum at biopsy time was associated with increased odds of ABMR/MVI [OR = 1.031, CI (95%) 1.002–1.060, p = 0.035] independent of HLA-DSA and recipient sex (Table 5A), although no association was found with absolute antibody count (data not shown). Among cases with ABMR/MVI, 37% (n = 17) exhibited a non-HLA antibody MFI ratio sum >22.7 at biopsy (vs. 17% of controls, p = 0.015), and 22% (n = 10) also had HLA-DSA. Of the patients, 35% had no HLA-DSA nor high non-HLA burden (vs. 79% of controls, p < 0.001) (Figure 3B). When replicating the extracellular and intracellular non-HLA antibodies analysis at biopsy time, only antibodies against intracellular non-HLA antigens were significantly associated with ABMR/MVI [OR = 1.062, CI (95%) 1.011–1.116, p = 0.018) (Tables 5B, C).

Table 5. Univariable and multivariable logistic regression analysis for ABMR/MVI development according to HLA and non-HLA antibodies after KT, at biopsy time.
Finally, we individually assessed the association of each non-HLA antibody in serum after KT. In a multivariable analysis, including only the individual antibodies significantly (p < 0.01) associated with ABMR/MVI in previous univariable analysis, only GSTT1 was associated with ABMR/MVI at the time of biopsy [OR = 4.887, CI (95%) 1.740–13.729, p = 0.003] consistent with pretransplant findings (Supplementary Table 6).
Discussion
ABMR stands as a significant contributor to graft loss after KT, with potential development even in the absence of detectable HLA-DSA. Several studies have estimated its prevalence to range from 30% to 60% among biopsies showing histological features suggestive of ABMR (13, 16, 32). Various investigations on non-HLA antibodies have unveiled their potential involvement in ABMR. These studies have assessed the impact of individual antibodies targeting specific molecules, and more recently, they have delved into the analysis involving antibodies against a broader spectrum of molecules (27, 28, 30).
In our study, we examined multiple non-HLA targets and observed that a high overall burden of non-HLA antibodies, both before and after KT, correlated with antibody-mediated damage, encompassing both ABMR and MVI, regardless of the detection of HLA antibodies. Specifically, antibodies targeting extracellular antigens seem to have a predominant role before KT, while those targeting intracellular antigens do it at diagnosis. We postulate that incorporating non-HLA antibodies into the pretransplant immunological risk assessment could prove beneficial.
Using a multiplex test comprising 60 non-HLA antibodies and the manufacturer’s recommended cut-off, we observed that non-HLA antibodies are frequently present in our patients. Specifically, 87% of the recipients exhibited at least one non-HLA antibody before KT. This finding aligns with previous reports: employing a 62-antigen multiplex test, Delville et al. (27) detected non-HLA antibodies in 83% of the patients, and Senev et al. (28) found that 98.7% of the patients had at least one non-HLA antibody before KT when employing an 82-antigen multiplex test. The high prevalence in our study, combined with the fact that before KT, surface and secreted non-HLA antigens seem to be primarily associated with ABMR/MVI, aligns with an autoimmune origin of these antibodies targeting self-molecules arising during the advanced stages of kidney disease as previously described (28, 33).
Our data showed that patients harboring a high pretransplant non-HLA antibody strength, particularly against extracellular targets, had an increased risk of ABMR/MVI. This association persisted after KT. While the association between non-HLA antibodies and ABMR has been explored previously, prior studies have focused on specific patient subsets without HLA-DSA (28) and many assessed sera only at the time of ABMR diagnosis (27, 30, 33). In an analysis before KT integrating multiple tests, Delvile et al. (27) concluded that before KT, non-HLA antigens expressed in the glomerular endothelia, in the absence of HLA-DSA, were linked to early ABMR in a highly selective cohort. In addition, Senev et al. (28) reported that a high non-HLA antibody burden before KT presented an increased risk of developing ABMR in the absence of HLA-DSA. In contrast, our cohort included patients with and without HLA-DSA, and we incorporated an evaluation setting before KT, including HLA sensitization (cPRA), in our analysis. Our findings indicate a significant association between a high non-HLA antibody MFI ratio sum and an augmented risk of ABMR/MVI in our cohort independent of HLA-DSA as a risk factor.
A non-HLA antibody evaluation test could help clinicians more accurately identify recipients at increased risk of developing ABMR/MVI. We propose the integration of non-HLA antibodies into the existing antibody evaluations, analogous to how cPRA is used to estimate a recipient’s HLA sensitization status before a donor is selected, which has been associated with rejection and graft survival (34). However, we suggest that a more restrictive cut-off value for these tests is needed to improve specificity and reduce false positivities. We have used the quartile division to identify patients at risk (MFI ratio sum >21.3 before KT and >22.7 after KT), but further research is required to define a validated threshold to get a more effective biomarker. Moreover, it is also necessary to validate whether only those non-HLA antibodies against extracellular, but not intracellular, antigens are relevant to assess risk before KT.
Even with the incorporation of non-HLA antibody evaluation before KT, 16 out of the 46 patients who developed MVI or ABMR showed neither a high non-HLA MFI ratio sum nor detectable HLA-DSA. Consequently, while the non-HLA antibodies before KT may aid in identifying patients with an increased ABMR/MVI risk independent of HLA sensitization, they are either an imperfect marker or not solely responsible for a proportion of these cases.
Among the 60 individual antibodies assessed, only antibodies against GSTT1 were individually associated with ABMR/MVI, both before and after KT. GSTT1 is a cytosolic protein involved in oxidative cellular damage. Approximately 20% of the Caucasian population lacks this protein due to gene deletion. Aguilera et al. (35–37) linked a donor–recipient genetic incompatibility to hepatitis in liver transplantation (36) and demonstrated that the development of GSTT1 antibodies after KT was associated with ABMR and C4d deposits (37, 38). Comoli et al. (23) recently described an association between GSST1 antibodies and ABMR in a pediatric KT cohort. Our results support these associations and extend them to the broader context of ABMR/MVI before and after KT.
Individual antigens identified to be significantly associated with ABMR risk often differ between studies (26–28, 39). This could be caused by the differences in cohorts, the design of the kits used, or the limited individual effect of each antibody. Based on our findings and prior evidence, we consider that the total number of non-HLA antibodies targeting different antibodies and the concentration of these antibodies before KT may have a greater effect on the risk of developing ABMR than the presence of antibodies to various antigens separately. This is consistent with previous findings from our group regarding other individual non-HLA antigens such as AT1R, endothelin receptor, and MICA (16).
After transplantation, we also found that a high non-HLA antibody burden is associated with an ABMR/MVI diagnosis. Interestingly, in our experience, only the MFI ratio sum, and not the absolute number, of non-HLA antibodies significantly correlated with the occurrence of ABMR/MVI. This observation supports the relevance of the antibody strength as a surrogate of its relative amount in circulation. Nevertheless, it is also relevant to acknowledge that antibodies in our study were considered positive with an MFI ratio ≥1, as indicated by the manufacturer, which could be seen as a lax cutoff that may result in false-positive antibodies when considering only the absolute count and not the MFI.
Notably, the cell localization of the target of those non-HLA antibodies appears to shift after transplantation. A high burden of non-HLA antibodies against intracellular antigens, but not extracellular ones, was associated with ABMR/MVI at diagnosis. As some authors have previously postulated, graft damage occurring during or after transplantation may result in the exposure of intracellular antigens and trigger the development of these antibodies (40).
We consider our study clinically relevant, as it suggests the potential utility of detecting non-HLA antibodies against extracellular targets in the recipients’ immunological risk assessment before transplantation. This additional evaluation may enhance clinicians’ ability to identify individuals at heightened risk of ABMR/MVI, thereby allowing for more tailored management strategies and potentially improving transplant outcomes.
Our study has some limitations. First, it is a single-center, retrospective observational study, which limits the generalizability of the findings without an external validation cohort. Second, the cohort is heterogeneous, encompassing patients with full ABMR and subclinical MVI, mixing indication and protocol biopsies. However, previous studies have already focused on highly selected cases (27, 28), and our findings were consistent even when including more diverse controls and MVI and ABMR cases. Third, our multiplex panel included a limited selection of non-HLA antigens and excluded classical ones such as anti-AT1R. Consequently, antibodies against these antigens were not assessed in our cohort, and their potential synergistic role in ABMR could not be explored. However, other studies using similar multiplex tests found no association between anti-AT1R and ABMR (28,30).
In conclusion, our study demonstrated that non-HLA antibodies are detectable in approximately 87% of KT recipients both before and after transplantation using a non-HLA single antibody multiplex test and the manufacturer’s recommended cut-off. Importantly, we found that a high non-HLA antibody burden before KT, particularly those antibodies targeting extracellular antigens, was independently associated with an increased risk of ABMR/MVI, even after accounting for overall HLA sensitization and the presence of HLA-DSA. These findings support the potential value of incorporating non-HLA evaluation into the current pretransplant immunological risk assessment, solely focused on HLA sensitization. Further prospective studies are required to validate these observations and to optimize cut-off values. Ultimately, this may enable a clinical implementation of non-HLA antibody testing that could improve KT recipients’ risk stratification and management strategies in KT.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Institutional Review Board of Hospital del Mar (2011/4385/I). The studies were conducted in accordance with the local legislation and institutional requirements. The human samples used in this study were acquired from primarily isolated as part of your previous study for which ethical approval was obtained. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
Author contributions
ES-P: Data curation, Methodology, Conceptualization, Writing – review & editing, Writing – original draft, Formal analysis. DR-P: Methodology, Conceptualization, Investigation, Writing – review & editing, Writing – original draft. JE-N: Formal analysis, Data curation, Writing – review & editing. AB: Writing – review & editing, Investigation, Writing – original draft, Data curation, Formal analysis. JC: Data curation, Formal analysis, Validation, Writing – review & editing. JG: Data curation, Writing – review & editing, Methodology, Investigation. LC: Formal analysis, Data curation, Investigation, Writing – review & editing. CB: Writing – review & editing. BC: Writing – review & editing. SS-U: Formal analysis, Investigation, Data curation, Writing – review & editing. JF-V: Writing – review & editing. EA-P: Writing – review & editing. JP: Conceptualization, Writing – review & editing. MP-S: Investigation, Supervision, Writing – review & editing, Conceptualization, Writing – original draft. MC: Project administration, Writing – original draft, Supervision, Investigation, Writing – review & editing, Conceptualization.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This study was performed with funding from projects PI20/00090, funded by Instituto de Salud Carlos III (ISCIII) and co-funded by the European Union, “PI23/00061”, funded by Instituto de Salud Carlos III (ISCIII) FIS-FEDER and co-funded by the European Union, and RICORS program RD24/0004/0003 financed by Instituto de Salud Carlos III (ISCIII) and co-financed by the European Union. MC was partially funded by INT21/00003 Spanish Ministry of Health ISCIII FIS‐FEDER. Immucor provided reagents for non‐HLA antibody detection but had no role in the design of the study or the writing of the manuscript. ES-P did this study as part of her doctoral thesis program at the Department of Medicine from the Universitat Autonoma of Barcelona (UAB).
Acknowledgments
We are indebted to Rosa Causadías, Anna Bach, Guillermo Pedreira, Aida Martínez, Anna Faura, Sara Álvarez, and Marisa Mir for their assistance with the patients. We thank Christine Heylen and Bryan Ryan for their advice on managing reagents and analysis proposals. We thank Anita Chong for her suggestions in the analysis.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2025.1614408/full#supplementary-material
Abbreviations
ABMR, antibody-mediated rejection; CI, confidence interval; cPRA, calculated panel reactive antibodies; GSTT1, glutathione S-transferase theta 1; HLA, human leukocyte antigens; HLA-DSA, HLA donor-specific antibodies; KT, kidney transplantation; MFI, median fluorescence intensity; MICA, major histocompatibility complex class I-related chain A; MVI, microvascular inflammation; OR, odds ratio; PLA2R1, phospholipase A2 receptor 1.
References
1. Einecke G, Sis B, Reeve J, Mengel M, Campbell PM, Hidalgo LG, et al. Antibody-mediated microcirculation injury is the major cause of late kidney transplant failure. Am J Transplant. (2009) 9:2520–31. doi: 10.1111/j.1600-6143.2009.02799.x
2. Lee PC, Terasaki PI, Takemoto SK, Lee PH, Hung CJ, Chen YL, et al. All chronic rejection failures of kidney transplants were preceded by the development of HLA antibodies. Transplantation. (2002) 74:1192–4. doi: 10.1097/00007890-200210270-00025
3. Crespo M, Pascual M, Tolkoff-Rubin N, Mauiyyedi S, Collins AB, Fitzpatrick D, et al. Acute humoral rejection in renal allograft recipients: i. Incidence, serology and clinical characteristics I. Transplantation. (2001) 71:652–8. doi: 10.1097/00007890-200103150-00013
4. Loupy A, Lefaucheur C, Vernerey D, Prugger C, Duong van Huyen J-P, Mooney N, et al. Complement-binding anti-HLA antibodies and kidney-allograft survival. N Engl J Med. (2013) 369:1215–26. doi: 10.1056/nejmoa1302506
5. Raïch-Regué D, Gimeno J, Llinàs-Mallol L, Menéndez S, Benito D, Redondo D, et al. Phosphorylation of S6RP in peritubular capillaries of kidney grafts and circulating HLA donor-specific antibodies. Front Med (Lausanne). (2022) 9:988080. doi: 10.3389/fmed.2022.988080
6. Jin YP, Valenzuela NM, Zhang X, Rozengurt E, and Reed EF. HLA class II–triggered signaling cascades cause endothelial cell proliferation and migration: relevance to antibody-mediated transplant rejection. J Immunol. (2018) 200:2372–90. doi: 10.4049/jimmunol.1701259
7. Buxeda A, Llinàs-Mallol L, Gimeno J, Redondo‑Pachón D, Arias‑Cabrales C, Burballa C, et al. Microvascular inflammation in the absence of human leukocyte antigen-donor-specific antibody and C4d: An orphan category in Banff classification with cytotoxic T and natural killer cell infiltration. Am J Transplant. (2023) 23:464–74. doi: 10.1016/j.ajt.2022.12.018
8. Mohan S, Palanisamy A, Tsapepas D, Tanriover B, Crew RJ, Dube G, et al. Donor-specific antibodies adversely affect kidney allograft outcomes. J Am Soc Nephrol. (2012) 23:2061–71. doi: 10.1681/ASN.2012070664
9. Redondo-Pachón D, Pérez-Sáez MJ, Mir M, Gimeno J, Llinàs‑Mallol L, García C, et al. Impact of persistent and cleared preformed HLA DSA on kidney transplant outcomes. Hum Immunol. (2018) 79:424–31. doi: 10.1016/j.humimm.2018.02.014
10. Lefaucheur C, Loupy A, Hill GS, Andrade J, Nochy D, Antoine C, et al. Preexisting donor-specific HLA antibodies predict outcome in kidney transplantation. J Am Soc Nephrol. (2010) 21:1398–407. doi: 10.1681/ASN.2009101065
11. Loupy A, Haas M, Roufosse C, Naesens M, Adam B, Afrouzian M, et al. The Banff 2019 Kidney Meeting Report (I): Updates on and clarification of criteria for T cell– and antibody-mediated rejection. Am J Transplant. (2020) 20:2318–31. doi: 10.1111/ajt.15898
12. Haas M, Loupy A, Lefaucheur C, Naesens M, Adam B, Afrouzian M, et al. The Banff 2017 Kidney Meeting Report: Revised diagnostic criteria for chronic active T cell–mediated rejection, antibody-mediated rejection, and prospects for integrative endpoints for next-generation clinical trials. Am J Transplant. (2018) 18:293–307. doi: 10.1111/ajt.14625
13. Senev A, Coemans M, Lerut E, Van Sandt V, Daniëls L, Kuypers D, et al. Histological picture of antibody-mediated rejection without donor-specific anti-HLA antibodies: Clinical presentation and implications for outcome. Am J Transplant. (2019) 19:763–80. doi: 10.1111/ajt.15074
14. Parajuli S, Redfield RR, Garg N, Aziz F, Mohamed M, Astor BC, et al. Clinical significance of microvascular inflammation in the absence of anti-HLA DSA in kidney transplantation. Transplantation. (2019) 103:1468–76. doi: 10.1097/TP.0000000000002487
15. Sis B, Jhangri GS, Riopel J, Chang J, De Freitas DG, Hidalgo L, et al, et al. A new diagnostic algorithm for antibody-mediated microcirculation inflammation in kidney transplants. Am J Transplant. (2012) 12:1168–79. doi: 10.1111/j.1600-6143.2011.03931.x
16. Crespo M, Llinàs-Mallol L, Redondo-Pachón D, Butler C, Gimeno J, Pérez‑Saéz MJ, et al. Non-HLA antibodies and epitope mismatches in kidney transplant recipients with histological antibody-mediated rejection. Front Immunol. (2021) 12:703457. doi: 10.3389/fimmu.2021.703457
17. Naesens M, Roufosse C, Haas M, Lefaucheur C, Mannon RB, Adam BA, et al. The Banff 2022 Kidney Meeting Report: Reappraisal of microvascular inflammation and the role of biopsy-based transcript diagnostics. Am J Transplant. (2023) 24:338–349. doi: 10.1016/j.ajt.2023.10.016
18. Jackson AM, Sigdel TK, Delville M, Hsieh SC, Dai H, Bagnasco S, et al. Endothelial cell antibodies associated with novel targets and increased rejection. J Am Soc Nephrol. (2015) 26:1161–71. doi: 10.1681/ASN.2013121277
19. Lefaucheur C, Louis K, Philippe A, Loupy A, and Coates PT. The emerging field of non–human leukocyte antigen antibodies in transplant medicine and beyond. Kidney Int. (2021) 100:787–98. doi: 10.1016/j.kint.2021.04.044
20. Dragun D, Müller DN, Bräsen JH, Fritsche L, Nieminen-Kelhä M, Dechend R, et al. Angiotensin II type 1-receptor activating antibodies in renal-allograft rejection. N Engl J Med. (2005) 352:558–69. Available online at: www.nejm.org (Accessed May 21, 2024).
21. Delville M, Charreau B, Rabant M, Legendre C, and Anglicheau D. Pathogenesis of non-HLA antibodies in solid organ transplantation: Where do we stand? Hum Immunol. (2016) 77:1055–62. doi: 10.1016/j.humimm.2016.05.021
22. Sorohan BM, Baston C, Tacu D, Bucşa C, Ţincu C, Vizireanu P, et al. Non-HLA antibodies in kidney transplantation: immunity and genetic insights. Biomedicines. (2022) 10:1506. doi: 10.3390/biomedicines10071506
23. Comoli P, Cioni M, Ray B, Tagliamacco A, Innocente A, Caridi G, et al. Anti-glutathione S-transferase theta 1 antibodies correlate with graft loss in non-sensitized pediatric kidney recipients. Front Med (Lausanne). (2022) 9:1035400. doi: 10.3389/fmed.2022.1035400
24. Kardol-Hoefnagel T, Van Logtestijn SALM, and Otten HG. A review on the function and regulation of ARHGDIB/rhoGDI2 expression including the hypothetical role of ARHGDIB/rhoGDI2 autoantibodies in kidney transplantation. Transplant Direct. (2020) 6:E548. doi: 10.1097/TXD.0000000000000993
25. Callemeyn J, Lamarthée B, Koenig A, Koshy P, Thaunat O, and Naesens M. Allorecognition and the spectrum of kidney transplant rejection. Kidney Int. (2022) 101:692–710. doi: 10.1016/j.kint.2021.11.029
26. Butler CL, Hickey MJ, Jiang N, Zheng Y, Gjertson D, Zhang Q, et al. Discovery of non-HLA antibodies associated with cardiac allograft rejection and development and validation of a non-HLA antigen multiplex panel: From bench to bedside. Am J Transplant. (2020) 20:2768–80. doi: 10.1111/ajt.15863
27. Delville M, Lamarthée B, Pagie S, See SB, Rabant M, Burger C, et al. Early acute microvascular kidney transplant rejection in the absence of anti-HLA antibodies is associated with preformed IgG antibodies against diverse glomerular endothelial cell antigens. J Am Soc Nephrol. (2019) 30:692–709. doi: 10.1681/ASN.2018080868
28. Senev A, Ray B, Lerut E, Hariharan J, Heylen C, Kuypers D, et al. The pre-transplant non-HLA antibody burden associates with the development of histology of antibody-mediated rejection after kidney transplantation. Front Immunol. (2022) 13:809059. doi: 10.3389/fimmu.2022.809059
29. Lamarthee B, Burger C, Leclaire C, Lebraud E, Zablocki A, Morin L, et al. CRISPR/Cas9-engineered HLA-deleted glomerular endothelial cells as a tool to predict pathogenic non-HLA antibodies in kidney transplant recipients. J Am Soc Nephrol. (2021) 32:3231–51. doi: 10.1681/ASN.2021050689
30. See SB, Mantell BS, Clerkin KJ, Ray B, Vasilescu ER, Marboe CC, et al. Profiling non-HLA antibody responses in antibody-mediated rejection following heart transplantation. Am J Transplant. (2020) 20:2571–80. doi: 10.1111/ajt.15871
31. Tambur AR, Bestard O, Campbell P, Chong AS, Crespo M, Ford ML, et al. Sensitization in transplantation: assessment of risk 2022 working group meeting report. Am J Transplant. (2023) 23:133–49. doi: 10.1016/j.ajt.2022.11.009
32. Burballa C, Pérez-Saéz MJ, Redondo-Pachón D, García C, Mir M, Arias-Cabrales C, et al. Luminex screening first vs direct single antigen bead assays: Different strategies for HLA antibody monitoring after kidney transplantation. Hum Immunol. (2020) 81:293–9. doi: 10.1016/j.humimm.2020.03.003
33. See SB, Yang X, Burger C, Lamarthée B, Snanoudj R, Shihab R, et al. Natural antibodies are associated with rejection and long-term renal allograft loss in a multicenter international cohort. Transplantation. (2023) 107:1580–92. doi: 10.1097/TP.0000000000004472
34. Huber L, Lachmann N, Niemann M, Naik M, Liefeldt L, Glander P, et al. Pretransplant virtual PRA and long-term outcomes of kidney transplant recipients. Transplant Int. (2015) 28:710–9. doi: 10.1111/tri.12533
35. Aguilera I, Wichmann I, Gentil MA, Gonzalez-Escribano F, and Nuñez-Roldan A. Alloimmune response against donor glutathione S-transferase T1 antigen in renal transplant recipients. Am J Kidney Diseases. (2005) 46:345–50. doi: 10.1053/j.ajkd.2005.04.022
36. Aguilera I, Sousa JM, Gavilán F, Bernardos A, Wichmann I, and Nuñez-Roldán A. Glutathione S-transferase T1 mismatch constitutes a risk factor for de novo immune hepatitis after liver transplantation. Liver Transplant. (2004) 10:1166–72. doi: 10.1002/lt.20209
37. Aguilera I, Alvarez-Marquez A, Gentil MA, Fernandez-Alonso J, Fijo J, Saez C, et al. Anti-glutathione S-transferase T1 antibody-mediated rejection in C4d-positive renal allograft recipients. Nephrol Dialysis Transplant. (2008) 23:2393–8. doi: 10.1093/ndt/gfm955
38. Álvarez-Márquez A, Aguilera I, Gentil MA, Caro JL, Bernal G, Fernández-Alonso J, et al. Donor-specific antibodies against HLA, MICA, and GSTT1 in patients with allograft rejection and C4d deposition in renal biopsies. Transplantation. (2009) 87:94–9. doi: 10.1097/TP.0b013e31818bd790
39. Kamburova EG, Kardol-Hoefnagel T, Wisse BW, Joosten I, Allebes WA, van der Meer A, et al. Development and validation of a multiplex non-HLA antibody assay for the screening of kidney transplant recipients. Front Immunol. (2018) 9:3002. doi: 10.3389/fimmu.2018.03002
Keywords: non-HLA antibodies, HLA, ABMR, antibody-mediated rejection, MVI, microvascular inflammation, GSTT1
Citation: Solà-Porta E, Redondo-Pachón D, Eguía-Núñez J, Buxeda A, Caro JL, Gimeno J, Campuzano L, Burballa C, Chamoun B, Sanz-Ureña S, Federico-Vega J, Alari-Pahissa E, Pascual J, Pérez-Sáez MJ and Crespo M (2025) Risk assessment of antibody-mediated damage based on the detection of HLA and non-HLA antibodies toward extracellular antigens before kidney transplantation. Front. Immunol. 16:1614408. doi: 10.3389/fimmu.2025.1614408
Received: 18 April 2025; Accepted: 16 July 2025;
Published: 12 August 2025.
Edited by:
Caner Süsal, Koç Üniversitesi, TürkiyeReviewed by:
Ilias Doxiadis, University Hospital Leipzig, GermanySebahat Akgül, Koç University, Türkiye
Copyright © 2025 Solà-Porta, Redondo-Pachón, Eguía-Núñez, Buxeda, Caro, Gimeno, Campuzano, Burballa, Chamoun, Sanz-Ureña, Federico-Vega, Alari-Pahissa, Pascual, Pérez-Sáez and Crespo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marta Crespo, bWNyZXNwb0Bwc21hci5jYXQ=
†These authors have contributed equally to this work