 Maria Anna Siciliano1
Maria Anna Siciliano1 Maria d’Apolito2
Maria d’Apolito2 Teresa Del Giudice1
Teresa Del Giudice1 Giulio Caridà3
Giulio Caridà3 Francesco Grillone1
Francesco Grillone1 Giampiero Porzio4
Giampiero Porzio4 Raffaele Giusti5
Raffaele Giusti5 Pierfrancesco Tassone3
Pierfrancesco Tassone3 Vito Barbieri1
Vito Barbieri1 Pierosandro Tagliaferri3*
Pierosandro Tagliaferri3*- 1Oncology Unit, Oncology Department, “Azienda Ospedaliero Universitaria (AOU) Dulbecco” Hospital, Catanzaro, Italy
- 2Oncology Unit, Tiberio Evoli Hospital, Melito di Porto Salvo, Reggio Calabria, Italy
- 3Department of Experimental and Clinical Medicine, Magna Græcia University, Catanzaro, Italy
- 4Tuscany Tumor Association, Oncological Home Care Service, Florence, Italy
- 5Oncology Unit, Azienda Ospedaliera-Universitaria Sant’Andrea, Rome, Italy
Background: Immune checkpoint inhibitors (ICIs) redefined the treatment of non-small cell lung cancer (NSCLC) but their efficacy in elderly and frail patients remains unclear due to immune-senescence and the underrepresentation of these populations in clinical trials. This systematic review and meta-analysis aimed to evaluate and rank first-line ICI-based therapies in NSCLC, stratified by age and performance status (PS).
Methods: A comprehensive search for randomized controlled trials (RCTs) of ICI regimens, pairwise and network meta-analyses (NMA) based on age (<65, ≥65, ≥75 years) and PS (0 vs. 1) were conducted. Endpoints were overall survival (OS) and progression-free survival (PFS).
Results: ICIs significantly improved OS and PFS versus chemotherapy (CT) in most subgroups. No OS benefit was observed in patients over 75 years. In younger patients, ICI+CT combinations (e.g. pembrolizumab+CT, cemiplimab+CT, camrelizumab+CT) ranked highest for OS and PFS. Among ≥65y patients, cemiplimab ranked first reaching statistical significance in most comparisons, while pembrolizumab was the most effective option for PFS. Stratified by PS, cemiplimab+CT ranked highest for OS in PS 0 patients, whereas cemiplimab was preferred in PS 1 patients. Overall, combination regimens were more effective in younger/fit patients, while monotherapy was more effective in older/PS 1 patients, suggesting a different benefit-risk balance. Anti-PD-1 therapies (alone or in combination) outperformed anti-PD-L1 and anti-CTLA-4 therapies in OS.
Conclusions: This meta-analysis highlights how the efficacy of ICIs in advanced NSCLC varies by age and PS. These findings support a tailored approach to immunotherapy and emphasize the need for trials specifically targeting frail and elderly populations.
1 Introduction
The introduction of immune checkpoint inhibitors (ICIs) has paved the way for radical changes in the treatment of advanced/metastatic non-small cell lung cancer (NSCLC). The superiority of ICIs over standard chemotherapy (CT) has been widely demonstrated; however, there is now a rising need to identify which patients are most likely to benefit from immunotherapy (IT). In this challenging scenario, ICIs-based therapy in elderly/frail patients is still a relevant point of discussion that requires further investigation. In clinical practice, more than half of all patients with NSCLC are aged over 70 years, and nearly 10% are 80 years or older (1). Due to immune-senescence, there is a hypothetical risk of reduced efficacy and increased toxicity with ICIs. However, some data from clinical trials suggest that older patients might benefit from IT similarly to younger patients, with an acceptable safety profile (2). However, clinical trials mostly include patients with a performance status (PS) of 0–1 and median age at trial enrollment was about 10 years younger than the median age of NSCLC diagnosis. For this reason, data on ≥75 years or those with PS 2 patients are mostly derived from post-hoc analyses of small subgroups with limited statistical power and high risk of selection bias. Unlike CT, ICIs treatment is often given until disease progression or unacceptable toxicity, and the impact of this long-term treatment remains unclear. Additionally, the combination of IT and CT has become the standard of care in first-line NSCLC improving efficacy as compared to CT alone but also leading to a higher rate of adverse events. Therefore, there is a rising medical need to identify the most appropriated treatment strategy for frail and elderly populations to avoid over- or under-treatment and preventing useless toxicity. Indeed, this requires the design of pragmatic clinical trials that enroll populations as more similar to those observed in the real-life setting.
2 Methods
2.2 Systematic literature review
According to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines, we conducted a systematic review using PubMed, Embase, Cochrane Library and relevant abstracts and presentations from major meeting databases (Supplementary Figure S1) (3). Timeframe was set from January 2010 to September 2024.
2.2 Data extraction and quality assessment
Data were independently extracted by two investigators (MAS and GC) performing the database searches and record selection, following a predefined protocol. Any disagreements were resolved through consensus. Both investigators assessed the risk of bias of the included studies using Cochrane risk of bias tool (4). The risk of bias was evaluated using the modified Cochrane Collaboration tool for randomized controlled trials (RCTs), evaluating the following domains: random sequence generation (selection bias), allocation concealment (selection bias), blinding of participants and investigators, blinding of outcome assessment (detection bias), incomplete outcome data (attrition bias), and selective reporting (reporting bias) (Supplementary Figure S2).
2.3 Study selection
Inclusion criteria: (1) phase 2 or 3 RCTs; (2) advanced/metastatic non-oncogene-addicted NSCLC; (3) comparison of two or more first-line treatments, including ICIs; (4) detailed outcomes including progression free survival (PFS) and overall survival (OS), stratified by age and/or PS. Studies that did not meet these criteria were excluded from the meta-analysis. Trials focusing on targeted therapy, radiotherapy, immune cells or cytokines, maintenance strategies or health-related quality of life were also excluded.
2.4 Endpoints
The primary endpoints of the meta-analysis were OS and PFS, analyzed in the overall population and stratified by age and PS. Specifically, subgroup analyses were conducted based on age (<65 years, ≥ 65 years, ≥75 years) and PS (0, ≥1). For both OS and PFS, hazard ratios (HRs) and corresponding confidence intervals (CIs) were extracted.
2.5 Pairwise meta-analysis
Pairwise meta-analyses were performed to compare IT-based therapy versus CT using Review Manager version 5.4 (Cochrane). For each pairwise meta-analysis, Cochrane’s Q test was used to assess statistical significance, with significance defined as a p-value ≤ 0.05. The presence of publication bias was excluded by visual inspection of funnel plots.
2.6 Network meta-analysis
Due to the heterogeneity of therapeutic strategies and the lack of direct comparisons, a Bayesian Network Meta-Analysis (NMA) was conducted. This analysis was performed using STATA (StataCorp, version 17) with a graphical interface and the mvmeta package. A Bayesian NMA was carried out for each outcome of interest using a Markov Chain Monte Carlo simulation with up to 30,000 iterations. Trials missing specific outcome data (e.g., HR for OS) were excluded from the corresponding NMA. The outcomes are reported with corresponding 95% credible intervals (CrIs). To identify the most credible treatment in the outcome of interest, we ranked the treatments using the surface under the cumulative ranking curve (SUCRA), derived by using command sucra. The closer the SUCRA value is to 1, the more probable the treatment is to rank as the best for the outcome of interest.
3 Results
3.1 Systematic literature review and description of eligible trials
A total of 289 of 3939 reports were screened by title and abstract. Further 257 articles were excluded from the qualitative evaluation. Thirty-two were selected by full text screening and were finally included in this analysis, involving 19.461 patients and 23 treatment regimens (Supplementary Figure S3). Of these, only studies reporting the necessary outcome data were included in the subsequent analyses. In the pairwise meta-analysis, 24 articles were included for OS and 20 for PFS. In the NMA, 26 articles were included in the analysis for OS and 22 for PFS. The experimental arm featured 6 ICI-monotherapy regimens [Keynote(KN)-024 (5), KN-042 (6), CheckMate(CM)-026 (7), IMpower(IM)-110 (8), Empower-lung 1 (9), IM-132 (10), Javelin Lung-100 (11), Mystic trial (12)], 3 dual-ICI strategy [CM-227 part I (13), KN-598 (14), Neptune (15)], 12 ICI/CT-regimens [KN-189 (16), NCT01285609 (17), KN-407 (18), CameL (19), CameL-Sq (20), Choice-01 (21), Empower-lung 3 (22), Gemstone-302 (23), IM-130 (24), IM-131 (25), CM-227 part II (26),Poseidon part I (27), Rationale-304 (28), Rationale-307 (29), Astrum-004 (30), Nippon (31), Orient-11 (32), Orient-12 (33), Innovent (34)], and 2 dual ICI/CT combinations [CM-9LA (35), Poseidon part II (27), CCTBG34 (36)]. Among them, 7 RCTs included only squamous (SQ) histology, 4 RCTs included only NSQ histology while the remaining studies included mixed histology. Regarding PD-L1 expression, 4 trials enrolled only patients with PD-L1 >50%, 1 trial included only patients with PD-L1>25% and 4 trials only patients with PD-L1 >1%. All other studies included patients with mixed PD-L1 expression levels. Details of included trials were provided in Table 1.
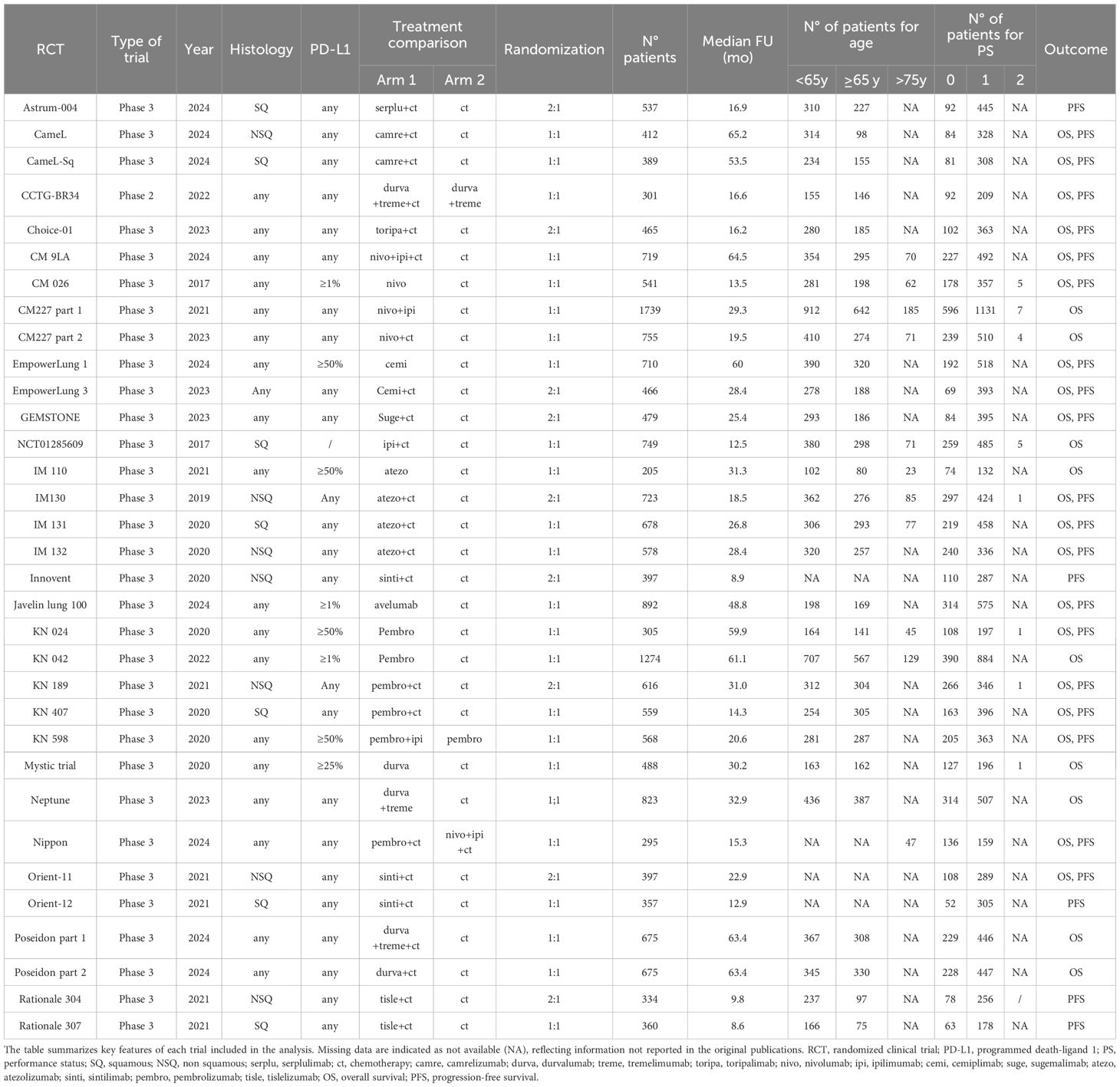
Table 1. Characteristics of included trials.
3.2 Pairwise meta-analysis
To compare ICIs-based therapy with CT, a pairwise analysis stratified by patient age and PS was carried out. ICIs-based regimens were associated with a statistically significant reduction in the risk of death (<65 years: HR vs CT 0,75; 95% CI 0.68-0.82; ≥65 years: HR Vs CT 0.80; 95% CI 0.76-0.85; PS 0: HR Vs CT 0.87; 95% CI 0.68-0.80; PS 1: HR Vs CT 0.77; 95% CI 0.72-0.83) and disease progression (<65y: HR vs CT 0.58; 95% CI 0.51-0.65; ≥65y: HR Vs CT 0.63; 95% CI 0.57-0.70; PS 0: HR Vs CT 0.62; 95% CI 0.51-0.75; PS 1: HR Vs CT 0.59; 95% CI 0.54-0.65) (Supplementary Figures S4, S5). Across all subgroups, the impact of ICIs-based therapy on reducing the risk of disease progression was greater than its effect on OS. ICI monotherapy appeared to perform better in OS in patients with ≥65 years (HR 0.76; 95% CI 0.65-0.88), whereas in patients <65 years ICI plus CT were more effective. In younger patients, ICI/CT demonstrated a 58% reduction in the risk of death, compared to 16% for single ICI and 27% for dual ICI/CT. The combination of dual ICIs without CT did not improve OS compared to CT alone, although this finding is based on two studies only. Instead, for older patients, ICI monotherapy showed a slight advantage. In the <65 years subgroup, ICI/CT was also superior for PFS, as for OS (HR 0.54). Notably, in the ≥75 years population, ICI-based regimens were not associated with a statistically significant OS benefit compared to CT alone, though this data is based on few studies and patients (Supplementary Figure S5), resulting in low statistical power and limiting the certainty of this finding. PFS could not be analyzed in this subgroup due to insufficient data. Regarding PS, OS differences were minimal between groups, whereas for PFS, ICI/CT performed slightly better in both PS 0 and PS 1 patients (Supplementary Figure S6). Finally, breaking down the studies by ICIs type, anti-PD-1 therapy whether alone or in combination, performed better in OS than anti-PDL1 or anti-CTLA4 regimens (Supplementary Figure S6). A graphical summary of the pairwise meta-analysis results was shown in Figure 1.
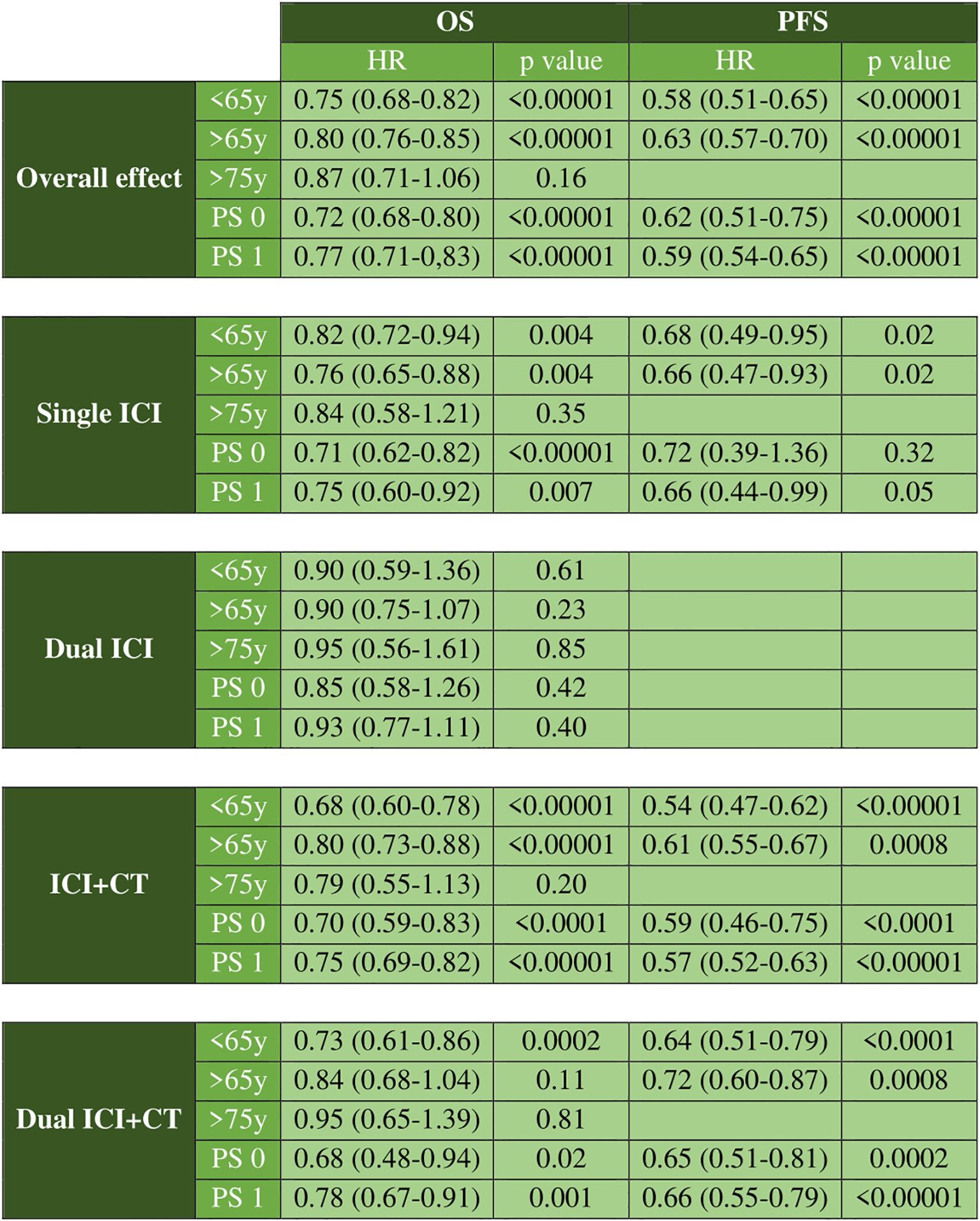
Figure 1. Graphical summary of pairwise meta-analysis results. Overall effect and results grouped by therapeutic regimen for OS and PFS.
3.3 NMA age analysis: OS and PFS
In the NMA analysis, pembrolizumab+CT (HR Vs CT 0.20; 95% CrI 0.09-0.45; SUCRA 94,1%), cemiplimab+CT (HR Vs CT 0.22; 95% CrI 0.09-0.56; SUCRA 89%) and camrelizumab+CT (HR Vs CT 0.28; 95% CrI 0.12-0.62; SUCRA 81,3%) ranked highest for OS in patients with <65 years. For patients ≥65 years, cemiplimab monotherapy ranked first in OS (HR 0.27; 95% CrI 0.17-0.41; SUCRA 99,5%) reaching statistical significance in most comparisons. Similar to the pairwise meta-analysis and facing the same statistical limitations, the NMA confirmed that in patients aged ≥75 years, ICIs-based therapy did not improve OS compared to CT (Figure 2; Supplementary Figure S7). For PFS analysis, camrelizumab+CT (HR 0.14; 95% CrI 0.05-0.38; SUCRA 86,4%) and pembrolizumab+CT (HR 0.15; 95% CrI 0.05-0.43; SUCRA 81.3%) ranked highest for patients <65 years. In contrast, pembrolizumab monotherapy had the highest probability of being the best treatment for reducing the risk of progression in patients ≥65 years (HR 0.14; 95% CrI 0.10-0.19; SUCRA 90%) (Supplementary Figure S8). Treatments with available data for both OS and PFS were compared using SUCRA rankings, visualized in a grouped heatmap and sorted by mean SUCRA value. Notably, in patients with <65 years, ICI/CT combinations had the highest probability of being the most effective in reducing the risk of death, while in patients with ≥65 years, ICI monotherapy ranked first (Figure 3).
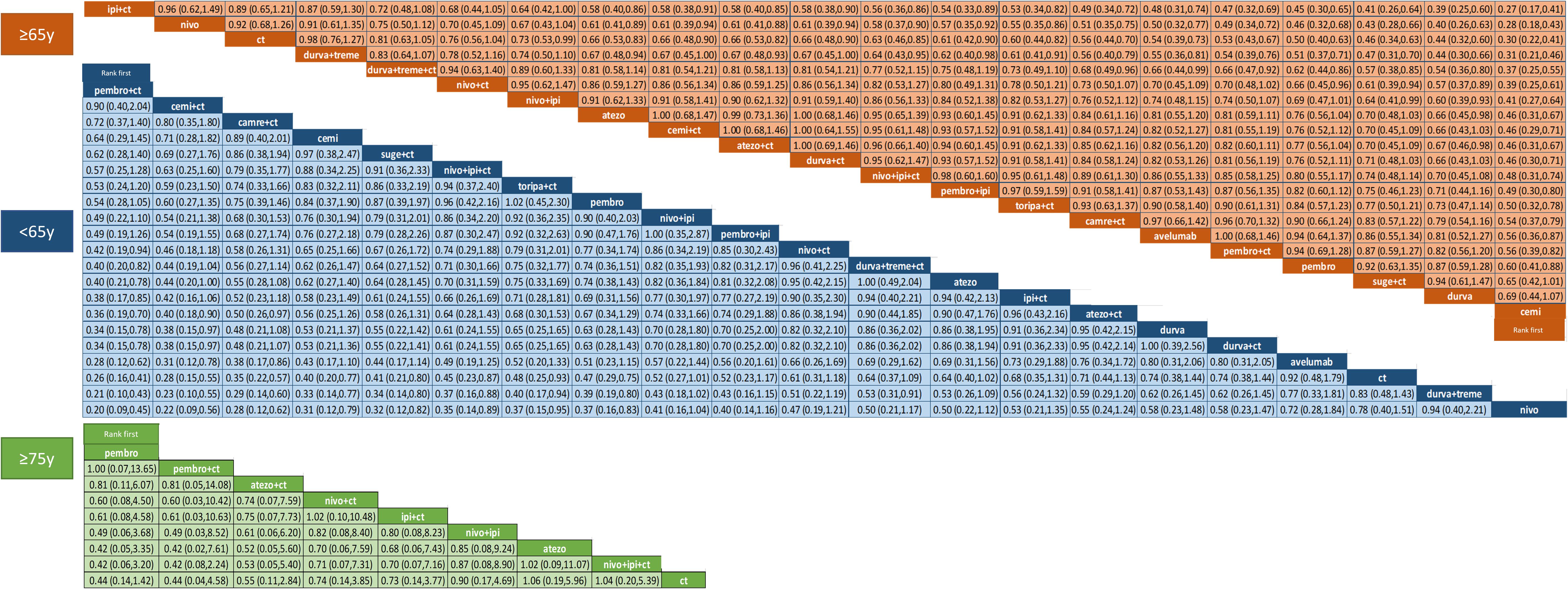
Figure 2. Hazard ratios and 95% CrI for OS of the NMA in age cohorts. The results are presented as column-defined treatment versus row-defined treatment.
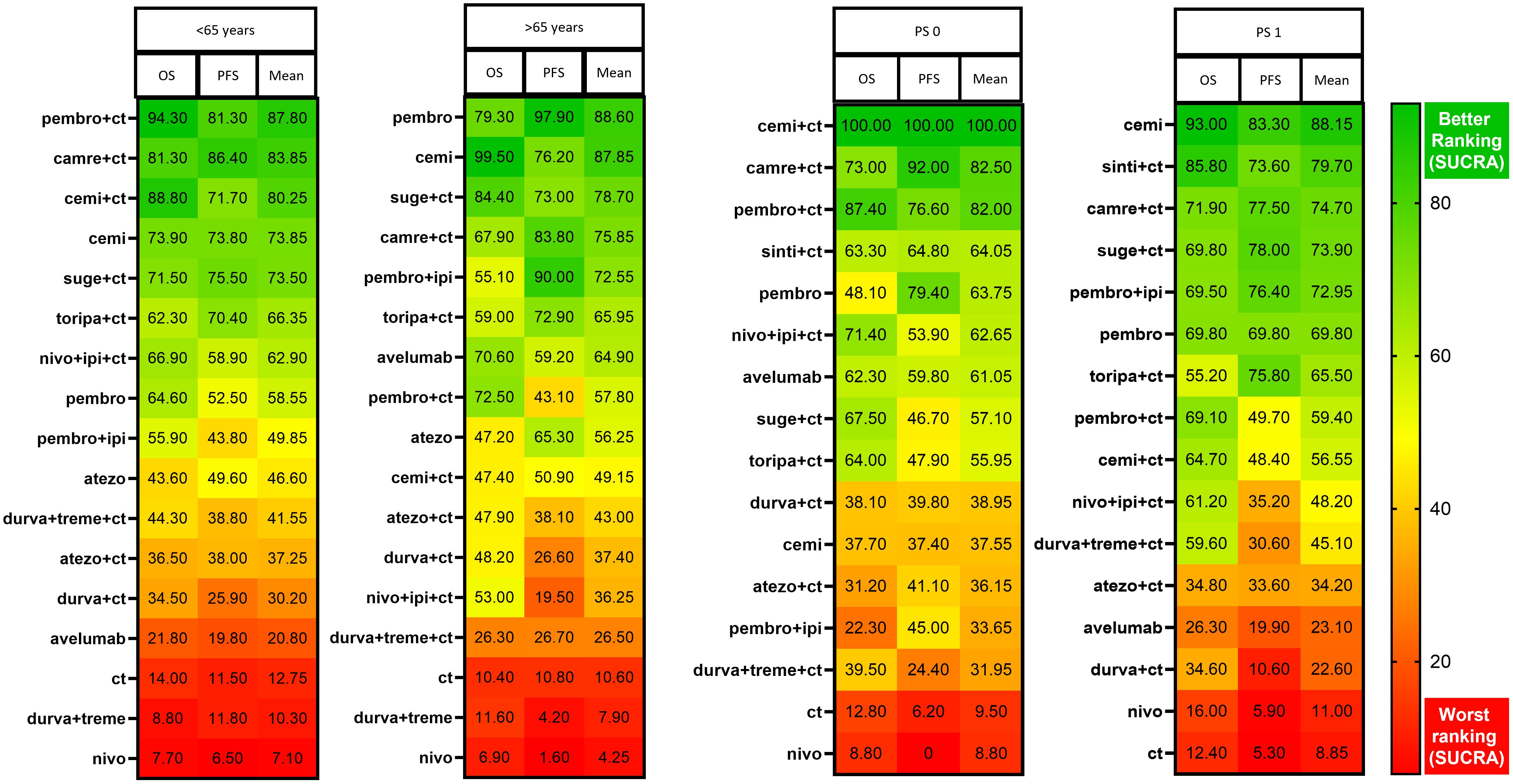
Figure 3. Ranking of treatments based on NMA across age and PS subgroups. All of the SUCRA values for each regimen with regard to PFS and OS. An average SUCRA and the average ranking are provided.
3.4 NMA PS analysis: OS and PFS
In terms of reducing the risk of death in patients with PS 0, cemiplimab/CT ranked first in NMA with a statistically significant advantage over all other treatments (HR Vs CT 0.05; 95% CrI 0.02-0.12; SUCRA 100%). In contrast, pembrolizumab/CT ranked second (HR Vs CT 0.22; 95% CrI 0.10-0.49; SUCRA 87,4%) (Figure 4; Supplementary Figure S9). Instead, for patients with PS 1, cemiplimab ranked first in OS. However, both pembrolizumab/CT and cemiplimab/CT performed worse in PS 1 patients compared to those with PS 0. Conversely, pembrolizumab monotherapy ranked higher in the PS 0 subgroup. For PFS, camrelizumab/CT and cemiplimab/CT ranked first. Notably, all ICIs-based treatments outperformed CT (Figure 4; Supplementary Figure S9). A grouped heatmap for PS is shown in Figure 3, highlighting that in PS 0 patients ICI/CT combinations had the highest probability of being the best treatment for both OS and PFS. Meanwhile, in PS 1 patients, cemiplimab monotherapy ranked first.
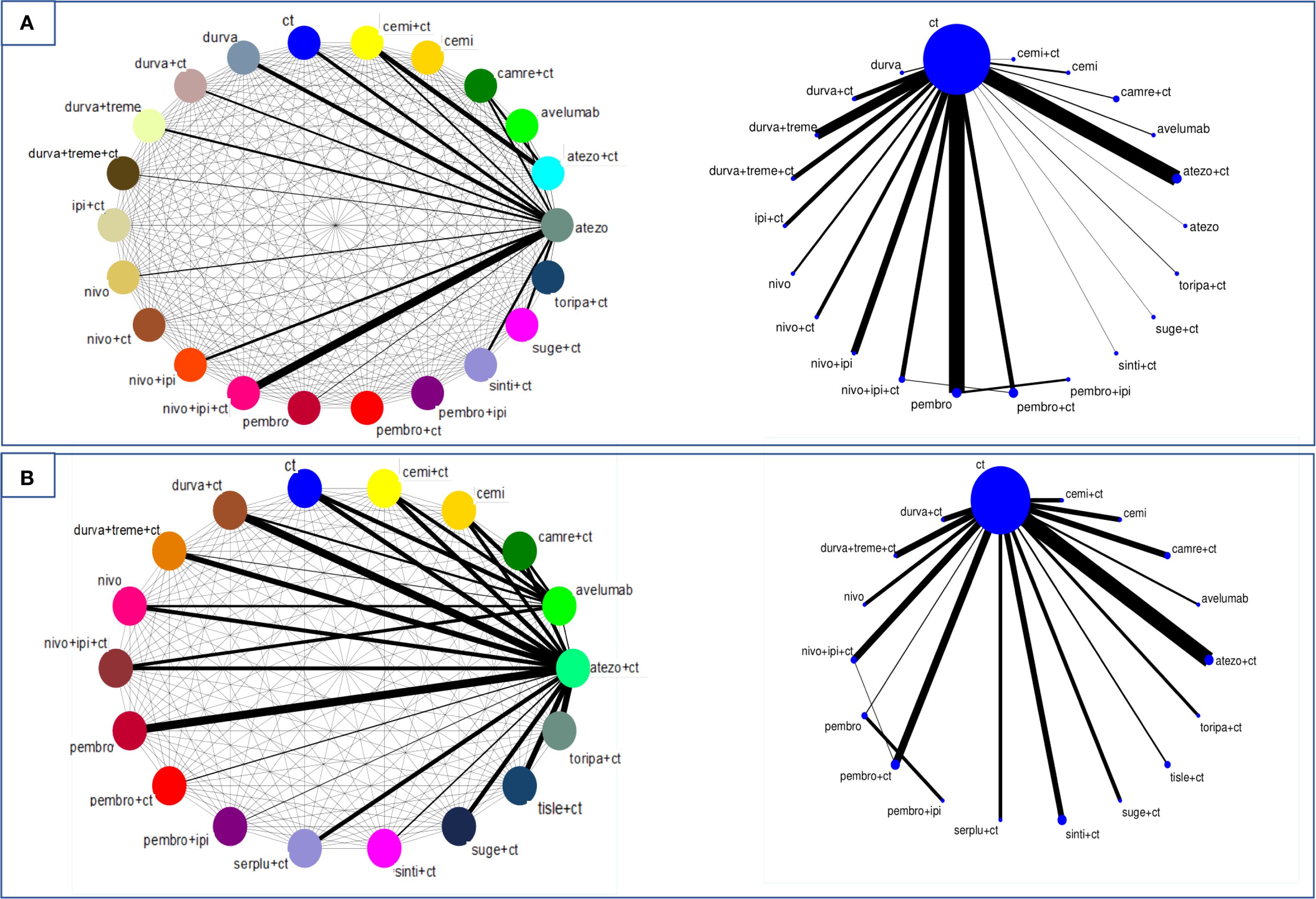
Figure 4. Network plot of direct (right) and indirect (left) comparison of the studies included in the analysis for OS (A) and PFS (B) in the PS cohort. Each circular node represents a treatment type. The thickness of the lines is proportional to the number of patients in head-to-head comparisons.
4 Discussion
IT with ICIs has become a cornerstone in the treatment of advanced/metastatic NSCLC. There is growing interest in defining the efficacy and safety of this approach in older and frail patients, identifying the most effective treatments in this setting. Due to the poorly characterized immune-senescence phenomenon, it remains unclear whether ICIs-based treatments are less effective in older patients. Aging-related changes in the immune system, collectively known as immune-senescence, may contribute to resistance to IT (37). Thymic involution and chronic antigenic stimulation cause naive T cells to convert into virtual memory cells, potentially impairing immune responses to pathogens and tumors. Additionally, the reduced number of naive CD8+ T cells, along with an increase in antigen-experienced CD4+ and CD8+ T cells, leads to a diminished capacity to respond to newly encountered antigens. Furthermore, decrease of costimulatory signals (like CD28 and CD27 on T cell) or the upregulation of Tim-3 and CD57 were described in the elderly and have been linked to reduced response to ICIs (38). Immune-senescence phenomenon involves also B cells and innate immune response (39).
Despite this, individual clinical trials have shown a similar survival benefit of ICIs compared to CT across younger and older patients with an acceptable safety profile, based however on underpowered post-hoc analyses unable to definitely address this crucial point. At this aim, this systematic review and meta-analysis were carried out to summarize and rank the efficacy of first line ICIs-based treatments in advanced/metastatic NSCLC, considering age and PS. Our findings confirmed that ICIs-based regimens significantly improved OS and PFS compared to CT in all subgroups, with a greater impact on PFS. A previous meta-analysis by Zhou et al. found that PFS benefits were more pronounced than OS benefit in the first-line setting, whereas the opposite was observed in later treatments lines (40). For patients over 75 years, our analysis did not demonstrate a statistically significant OS benefit of ICIs over CT. This finding may be due to limited data and small sample size of this subgroup, thereby limiting the confidence in the observed outcome. PFS could not be analyzed due to insufficient data (only 3 studies). Notably, only IM-131 (25) reported a statistical significant PFS (77 patients), whereas CM-9LA (70 patients) and NIPPON (47 patients) showed negative outcomes (31, 35). Caution is required in interpreting these results, and validation in larger cohorts of elderly patients is needed.
In older patients, ICI monotherapy seems to perform better in the pairwise as well as NMA, while ICI+CT was the best strategy in younger patients. In patients aged over 65 years ICI+CT (pembrolizumab+CT, cemiplimab+CT and camrelizumab+CT) ranked highest in OS, though without statistical significance in all comparisons. In patients over 65 years cemiplimab monotherapy ranked first in OS with statistical significance for most comparisons. For PFS, camrelizumab+CT and pembrolizumab+CT ranked highest in <65 years (with a statistical significance only over nivolumab, CT, durvalumab+tremelimumab, avelumab, and atezolizumab+CT) whereas pembrolizumab monotherapy had the highest probability of reducing disease progression in ≥65 years (non-statistically significant comparisons: pembrolizumab+ipilimumab, camrelizumab+CT, cemiplimab, toripalimab+CT, serplulimab+CT). When stratified by PS, OS differences between PS 0 and PS 1 were minimal whereas for PFS ICI/CT performed slightly better in both PS 0 and PS 1. In PS 0 patients, cemiplimab+CT ranked first in OS (statistically significant vs. all treatments) with pembrolizumab+CT ranked second. In PS 1, cemiplimab monotherapy performed best in OS, while cemiplimab+CT and pembrolizumab+CT performed worse than in PS 0.
These rankings led us to conclude that: i) combination therapies appear more effective in younger and fit patients, potentially due to a stronger immune response and/or better treatment tolerance; ii) mono immune-therapy appeared more effective in older and PS 1 patients, likely reflecting a different benefit-risk balance and reduced treatment tolerance. Furthermore, our analysis of ICIs type demonstrated that anti-PD1 therapy (alone or in combination), outperformed anti-PD-L1 and anti-CTLA-4 regimens in OS.
Unlike previous meta-analyses investigating this field, our study provides a more comprehensive comparison of available treatment strategies in this setting, including the largest number of RCTs and the most recent data updates. Moreover, at the best of our knowledge this is the first NMA considering both age and PS to investigate the frailty scenario.
Our results should be evaluated in the current landscape of studies focused on the relevance of age and PS. Landre et al. performed a NMA considering only patients over 65 years, demonstrating OS and PFS benefit of the anti-PD-1/PD-L1 plus CT, but with no consistent evidence in patients aged over 75 years (41). In a NMA focused only on older patients with PDL-1 ≥50%, cemiplimab monotherapy emerged as the preferred treatment strategy, consistent with our previous findings (42). Instead, Sun et al. found similar OS efficacy across age groups but no PFS benefit in either young and older patients (though their analysis included only 8 trials) (43). Regarding PS, an interesting meta-analysis in real-world advanced NSCLC patients with PS ≥2 reported detrimental effects of ICIs therapy on OS, PFS and ORR, raising concerns about treatment suitability in frail patients (42). All together these studies support our finding of relevant role of age and PS in predicting effectiveness of immune-oncology strategies. However, it should be emphasized the under-representation of frail patients in clinical trials, limiting the applicability of trials data in real-world clinical practice. Chronological age and PS alone do not fully capture a patient’s condition; a comprehensive, multidisciplinary evaluation is necessary to assess overall PS and health. PS deterioration may result from various factors, including disease burden, comorbidities, age, and the overall frailty, making it critical to differentiate between cancer-related PS decline and other underlying conditions. Comprehensive Geriatric Assessment (CGA) represents a well-established, multidimensional approach for evaluating older patients. Initially developed within geriatrics, CGA has been increasingly applied in oncology to guide treatment decisions in elderly cancer patients and to better characterize frailty (44). Recent prospective data in elderly NSCLC patients undergoing CGA suggest that frailty, comorbidities, and low albumin levels are associated with worse survival outcomes and higher toxicity, highlighting the importance of CGA-guided treatment decisions (45). Among elderly patients, safety concerns remain a key consideration due to impaired renal and/or cardiac function, increased comorbidities, declining organ function and cognitive impairment (46). Studies suggest that ICIs safety profile is comparable between older/frail and fit patients, though CT-based combinations inevitably increase toxicity (47–49). Therefore, adequate geriatric screening is essential to prevent both over- or under-treatment in this population.
Several limitations of this meta-analysis should be acknowledged. Firstly, data were extrapolated from published RCTs rather than individual patient data. Heterogeneity was evident when pooling data across different ICIs or CT backbone, trial design, histology and PD-L1 expression. Formal analyses of safety and toxicity stratified by age/PS could not be performed because data were not reported in clinical trials. Additionally, several data points relied on post-hoc analyses and ongoing trials have yet to report survival outcomes, introducing potential bias. Longer follow-up is needed to fully assess the long-term impact of ICIs on OS. Furthermore, in older patients (≥75 years), non-cancer-related mortality may significantly interfere with OS outcomes in phase III trials.
5 Conclusions
This systematic review and meta-analysis confirmed that ICI-based therapy significantly improved OS and PFS compared to CT across all subgroups, except for patients with ≥75 years. The best treatment strategy seems to vary by age and PS, with ICI monotherapy being most effective in older/PS 1 patients, while ICI+CT combinations performed better in younger/PS 0 patients. In conclusion, there is an urgent need to design future RCTs focusing on the use of IT in frail populations as a whole, improving patients stratification using geriatric tools. Considering that the rate of end-of-life IT is increasing, this could guide the clinicians in discriminating situations of over- or under-treatment, providing recommendations for clinical practice in selecting optimal strategies in these patients.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Author contributions
MAS: Conceptualization, Writing – original draft, Formal Analysis. Md’A: Writing – review & editing. TD: Writing – review & editing. GC: Writing – original draft, Formal Analysis. FG: Writing – review & editing. GP: Writing – review & editing. RG:Writing – review & editing. PTas: Writing – review & editing, Supervision. VB: Writing – review & editing. PTag: Writing – review & editing, Supervision.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
This manuscript has been supported by Institutional funds.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2025.1635056/full#supplementary-material
References
1. Available online at: https://seer.cancer.gov/statfacts/html/lungb.html (Accessed May 20, 2025).
2. Smith A, Boby J, Benny S, Ghazali N, Vermeulen E, and George M. Immunotherapy in Older Patients with Cancer: A Narrative Review. IJGM. (2024) 17:305–13. doi: 10.2147/IJGM.S435001
3. Hutton B, Salanti G, Caldwell DM, Chaimani A, Schmid CH, Cameron C, et al. The PRISMA Extension Statement for Reporting of Systematic Reviews Incorporating Network Meta-analyses of Health Care Interventions: Checklist and Explanations. Ann Intern Med. (2015) 162:777–84. doi: 10.7326/M14-2385
4. Higgins JPT, Altman DG, Gotzsche PC, Juni P, Moher D, Oxman AD, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. (2011) 343. doi: 10.1136/bmj.d5928
5. Reck M, Rodríguez-Abreu D, Robinson AG, Hui R, Csőszi T, Fülöp A, et al. Five-Year Outcomes With Pembrolizumab Versus Chemotherapy for Metastatic Non–Small-Cell Lung Cancer With PD-L1 Tumor Proportion Score ≥ 50%. JCO. (2021) 39:2339–49. doi: 10.1200/JCO.21.00174
6. De Castro G, Kudaba I, Wu YL, Lopes G, Kowalski DM, Turna HZ, et al. Five-Year Outcomes With Pembrolizumab Versus Chemotherapy as First-Line Therapy in Patients With Non–Small-Cell Lung Cancer and Programmed Death Ligand-1 Tumor Proportion Score ≥ 1% in the KEYNOTE-042 Study. JCO. (2023) 41:1986–91. doi: 10.1200/JCO.21.02885
7. Carbone DP, Reck M, Paz-Ares L, Creelan B, Horn L, Steins M, et al. First-Line Nivolumab in Stage IV or Recurrent Non–Small-Cell Lung Cancer. N Engl J Med. (2017) 376:2415–26. doi: 10.1056/NEJMoa1613493
8. Jassem J, De Marinis F, Giaccone G, Vergnenegre A, Barrios CH, Morise M, et al. Updated Overall Survival Analysis From IMpower110: Atezolizumab Versus Platinum-Based Chemotherapy in Treatment-Naive Programmed Death-Ligand 1–Selected NSCLC. J Thorac Oncol. (2021) 16:1872–82. doi: 10.1016/j.jtho.2021.06.019
9. Özgüroğlu M, Kilickap S, Sezer A, Gümüş M, Bondarenko I, Gogishvili M, et al. First-line cemiplimab monotherapy and continued cemiplimab beyond progression plus chemotherapy for advanced non-small-cell lung cancer with PD-L1 50% or more (EMPOWER-Lung 1): 35-month follow-up from a mutlicentre, open-label, randomised, phase 3 trial. Lancet Oncol. (2023) 24:989–1001. doi: 10.1016/S1470-2045(23)00329-7
10. Nishio M, Barlesi F, West H, Ball S, Bordoni R, Cobo M, et al. Atezolizumab Plus Chemotherapy for First-Line Treatment of Nonsquamous NSCLC: Results From the Randomized Phase 3 IMpower132 Trial. J Thorac Oncol. (2021) 16:653–64. doi: 10.1016/j.jtho.2020.11.025
11. Reck M, Barlesi F, Yang JCH, Westeel V, Felip E, Özgüroğlu M, et al. Avelumab Versus Platinum-Based Doublet Chemotherapy as First-Line Treatment for Patients With High-Expression Programmed Death-Ligand 1–Positive Metastatic NSCLC: Primary Analysis From the Phase 3 JAVELIN Lung 100 Trial. J Thorac Oncol. (2024) 19:297–313. doi: 10.1016/j.jtho.2023.09.1445
12. Rizvi NA, Cho BC, Reinmuth N, Lee KH, Luft A, Ahn MJ, et al. Durvalumab With or Without Tremelimumab vs Standard Chemotherapy in First-line Treatment of Metastatic Non–Small Cell Lung Cancer: The MYSTIC Phase 3 Randomized Clinical Trial. JAMA Oncol. (2020) 6:661. doi: 10.1001/jamaoncol.2020.0237
13. Brahmer JR, Lee JS, Ciuleanu TE, Bernabe Caro R, Nishio M, Urban L, et al. Five-Year Survival Outcomes With Nivolumab Plus Ipilimumab Versus Chemotherapy as First-Line Treatment for Metastatic Non–Small-Cell Lung Cancer in CheckMate 227. JCO. (2023) 41:1200–12. doi: 10.1200/JCO.22.01503
14. Boyer M, Şendur MAN, Rodríguez-Abreu D, Park K, Lee DH, Çiçin I, et al. Pembrolizumab Plus Ipilimumab or Placebo for Metastatic Non–Small-Cell Lung Cancer With PD-L1 Tumor Proportion Score ≥ 50%: Randomized, Double-Blind Phase III KEYNOTE-598 Study. JCO. (2021) 39:2327–38. doi: 10.1200/JCO.20.03579
15. De Castro G, Rizvi NA, Schmid P, Syrigos K, Martin C, Yamamoto N, et al. NEPTUNE: Phase 3 Study of First-Line Durvalumab Plus Tremelimumab in Patients With Metastatic NSCLC. J Thorac Oncol. (2023) 18:106–19. doi: 10.1016/j.jtho.2022.09.223
16. Garassino MC, Gadgeel S, Speranza G, Felip E, Esteban E, Dómine M, et al. Pembrolizumab Plus Pemetrexed and Platinum in Nonsquamous Non–Small-Cell Lung Cancer: 5-Year Outcomes From the Phase 3 KEYNOTE-189 Study. JCO. (2023) 41:1992–8. doi: 10.1200/JCO.22.01989
17. Govindan R, Szczesna A, Ahn MJ, Schneider CP, Gonzalez Mella PF, Barlesi F, et al. Phase III Trial of Ipilimumab Combined With Paclitaxel and Carboplatin in Advanced Squamous Non–Small-Cell Lung Cancer. JCO. (2017) 35:3449–57. doi: 10.1200/JCO.2016.71.7629
18. Novello S, Kowalski DM, Luft A, Gümüş M, Vicente D, Mazières J, et al. Pembrolizumab Plus Chemotherapy in Squamous Non–Small-Cell Lung Cancer: 5-Year Update of the Phase III KEYNOTE-407 Study. JCO. (2023) 41:1999–2006. doi: 10.1200/JCO.22.01990
19. Zhou C, Chen G, Huang Y, Zhou J, Lin L, Feng J, et al. Camrelizumab plus carboplatin and pemetrexed as first-line therapy for advanced non-squamous non-small-cell lung cancer: 5-year outcomes of the CameL randomized phase 3 study. J Immunother Cancer. (2024) 12:e009240. doi: 10.1136/jitc-2024-009240
20. Ren S, Chen J, Xu X, Jiang T, Cheng Y, Chen G, et al. Camrelizumab Plus Carboplatin and Paclitaxel as First-Line Treatment for Advanced Squamous NSCLC (CameL-Sq): A Phase 3 Trial. J Thorac Oncol. (2022) 17:544–57. doi: 10.1016/j.jtho.2021.11.018
21. Wang Z, Wu L, Li B, Cheng Y, Li X, Wang X, et al. Toripalimab Plus Chemotherapy for Patients With Treatment-Naive Advanced Non–Small-Cell Lung Cancer: A Multicenter Randomized Phase III Trial (CHOICE-01). JCO. (2023) 41:651–63. doi: 10.1200/JCO.22.00727
22. Baramidze A, Makharadze T, Gogishvili M, Melkadze T, Giorgadze D, Penkov K, et al. Cemiplimab plus chemotherapy versus chemotherapy alone in non-small cell lung cancer with PD-L1 ≥ 1%: A subgroup analysis from the EMPOWER-Lung 3 part 2 trial. Lung Cancer. (2024) 193:107821. doi: 10.1016/j.lungcan.2024.107821
23. Zhou C, Wang Z, Sun M, Cao L, Ma Z, Wu R, et al. Interim survival analysis of the randomized phase III GEMSTONE-302 trial: sugemalimab or placebo plus chemotherapy as first-line treatment for metastatic NSCLC. Nat Cancer. (2023) 4:860–71. doi: 10.1038/s43018-023-00578-z
24. West H, McCleod M, Hussein M, Morabito A, Rittmeyer A, Conter HJ, et al. Atezolizumab in combination with carboplatin plus nab-paclitaxel chemotherapy compared with chemotherapy alone as first-line treatment for metastatic non-squamous non-small-cell lung cancer (IMpower130): a multicentre, randomised, open-label, phase 3 trial. Lancet Oncol. (2019) 20:924–37. doi: 10.1016/S1470-2045(19)30167-6
25. Jotte R, Cappuzzo F, Vynnychenko I, Stroyakovskiy D, Rodríguez-Abreu D, Hussein M, et al. Atezolizumab in Combination With Carboplatin and Nab-Paclitaxel in Advanced Squamous NSCLC (IMpower131): Results From a Randomized Phase III Trial. J Thorac Oncol. (2020) 15:1351–60. doi: 10.1016/j.jtho.2020.03.028
26. Borghaei H, O’Byrne KJ, Paz-Ares L, Ciuleanu TE, Yu X, Pluzanski A, et al. Nivolumab plus chemotherapy in first-line metastatic non-small-cell lung cancer: results of the phase III CheckMate 227 Part 2 trial. ESMO Open. (2023) 8:102065. doi: 10.1016/j.esmoop.2023.102065
27. Peters S, Cho BC, Luft AV, Alatorre-Alexander J, Geater SL, Laktionov K, et al. Durvalumab With or Without Tremelimumab in Combination With Chemotherapy in First-Line Metastatic NSCLC: Five-Year Overall Survival Outcomes From the Phase 3 POSEIDON Trial. J Thorac Oncol. (2024) :S1556086424022640. doi: 10.1016/j.jtho.2024.09.1381
28. Lu S, Wang J, Yu Y, Yu X, Hu Y, Ma Z, et al. Tislelizumab plus chemotherapy as first-line treatment of locally advanced or metastatic nonsquamous non-small-cell lung cancer (final analysis of RATIONALE-304: a randomized phase III trial). ESMO Open. (2024) 9:103728. doi: 10.1016/j.esmoop.2024.103728
29. Wang J, Lu S, Yu X, Hu Y, Sun Y, Wang Z, et al. RATIONALE-307: Tislelizumab plus chemotherapy versus chemotherapy alone as first-line treatment for advanced squamous NSCLC in patients aged ≥ 65. JCO. (2021) 39:9102–2. doi: 10.1200/JCO.2021.39.15_suppl.9102
30. Zhou C, Hu Y, Arkania E, Kilickap S, Ying K, Xu F, et al. A global phase 3 study of serplulimab plus chemotherapy as first-line treatment for advanced squamous non-small-cell lung cancer (ASTRUM-004). Cancer Cell. (2024) 42:198–208. doi: 10.1016/j.ccell.2023.12.004
31. Shiraishi Y, Nomura S, Sugawara S, Horinouchi H, Yoneshima Y, Hayashi H, et al. Comparison of platinum combination chemotherapy plus pembrolizumab versus platinum combination chemotherapy plus nivolumab–ipilimumab for treatment-naive advanced non-small-cell lung cancer in Japan (JCOG2007): an open-label, multicentre, randomised, phase 3 trial. Lancet Respir Med. (2024) 12:877–87. doi: 10.1016/S2213-2600(24)00185-1
32. Yang Y, Sun J, Wang Z, Fang J, Yu Q, Han B, et al. Updated Overall Survival Data and Predictive Biomarkers of Sintilimab Plus Pemetrexed and Platinum as First-Line Treatment for Locally Advanced or Metastatic Nonsquamous NSCLC in the Phase 3 ORIENT-11 Study. J Thorac Oncol. (2021) 16:2109–20. doi: 10.1016/j.jtho.2021.07.015
33. Zhou C, Wu L, Fan Y, Wang Z, Liu L, Chen G, et al. Sintilimab Plus Platinum and Gemcitabine as First-Line Treatment for Advanced or Metastatic Squamous NSCLC: Results From a Randomized, Double-Blind, Phase 3 Trial (ORIENT-12). J Thorac Oncol. (2021) 16:1501–11. doi: 10.1016/j.jtho.2021.04.011
34. Yang Y, Wang Z, Fang J, Yu Q, Han B, Cang S, et al. Efficacy and Safety of Sintilimab Plus Pemetrexed and Platinum as First-Line Treatment for Locally Advanced or Metastatic Nonsquamous NSCLC: a Randomized, Double-Blind, Phase 3 Study (Oncology pRogram by InnovENT anti-PD-1-11). J Thorac Oncol. (2020) 15:1636–46. doi: 10.1016/j.jtho.2020.07.014
35. Carbone DP, Ciuleanu TE, Schenker M, Cobo-Dols M, Bordenave S, Juan-Vidal O, et al. First-line (1L) nivolumab (N) + ipilimumab (I) + chemotherapy (C) vs C alone in patients (pts) with metastatic NSCLC (mNSCLC) from CheckMate 9LA: 4-y clinical update and outcomes by tumor histologic subtype (THS). JCO. (2023) 41(17_suppl):LBA9023–LBA9023. doi: 10.1200/JCO.2023.41.17_suppl.LBA9023
36. Leighl NB, Laurie SA, Goss GD, Hughes BGM, Stockler MR, Tsao MS, et al. CCTG BR.34: A randomized trial of durvalumab and tremelimumab +/- platinum-based chemotherapy in patients with metastatic (Stage IV) squamous or nonsquamous non-small cell lung cancer (NSCLC). JCO. (2020) 38:9502–2. doi: 10.1200/JCO.2020.38.15_suppl.9502
37. Ferrara R, Mezquita L, Auclin E, Chaput N, and Besse B. Immunosenescence and immunecheckpoint inhibitors in non-small cell lung cancer patients: Does age really matter? Cancer Treat Rev. (2017) 60:60–8. doi: 10.1016/j.ctrv.2017.08.003
38. Moreira A, Gross S, Kirchberger MC, Erdmann M, Schuler G, and Heinzerling L. Senescence markers: Predictive for response to checkpoint inhibitors. Intl J Cancer. (2019) 144:1147–50. doi: 10.1002/ijc.31763
39. Casaluce F, Sgambato A, Maione P, Spagnuolo A, and Gridelli C. Lung cancer, elderly and immune checkpoint inhibitors. J Thorac Dis. (2018) 10:S1474–81. doi: 10.21037/jtd.2018.05.90
40. Zhou Z, Ren S, Chen L, Zhou C, and Jiang T. Differences in treatment effect size between progression-free survival and overall survival in anti-PD-1/PD-L1 inhibitors-based trials in advanced NSCLC: a systematic review and meta-analysis. Transl Lung Cancer Res. (2021) 10:2562–72. doi: 10.21037/tlcr-21-199
41. Landre T, Chouaïd C, Sadaoui N, Bouharati D, and Taleb C. Clinical benefit of anti-PD-1/PD-L1 plus chemotherapy in first-line treatment for patients over the age of 65 or 75 with metastatic non-small cell lung cancer (NSCLC). J Chemother. (2024) 36:675–81. doi: 10.1080/1120009X.2024.2308978
42. Dall’Olio FG, Maggio I, Massucci M, Mollica V, Fragomeno B, and Ardizzoni A. ECOG performance status ≥2 as a prognostic factor in patients with advanced non small cell lung cancer treated with immune checkpoint inhibitors—A systematic review and meta-analysis of real world data. Lung Cancer. (2020) 145:95–104. doi: 10.1016/j.lungcan.2020.04.027
43. Sun YM, Wang Y, Sun XX, Chen J, Gong ZP, and Meng HY. Clinical Efficacy of Immune Checkpoint Inhibitors in Older Non-small-Cell Lung Cancer Patients: A Meta-Analysis. Front Oncol. (2020) 10:558454. doi: 10.3389/fonc.2020.558454
44. He S, Shepherd HL, Agar M, and Shaw J. The value and effectiveness of geriatric assessments for older adults with cancer: an umbrella review. BMC Geriatr. (2024) 24:1001. doi: 10.1186/s12877-024-05607-9
45. Skampardonis K, Papagianni ED, Leontopoulou V, Lazarou A, Christodoulopoulos G, Perifanou-Sotiri S, et al. Prospective observational study to evaluate efficacy and safety of immunotherapy (IO) in elderly (eld) patients (pts) with non-small cell lung cancer (NSCLC) undergoing comprehensive geriatric assessment (CGA). (2025) JCO. 43:e20603–e20603. doi: 10.1200/JCO.2025.43.16_suppl.e20603
46. Takayuki N, Keiko T, Junji U, Yoshiko K, Nobuyo T, Tadaaki Y, et al. Advanced Non-Small-Cell Lung Cancer in Elderly Patients: Patient Features and Therapeutic Management. BioMed Res Int. (2018) 2018:1–8. doi: 10.1155/2018/8202971
47. Felip E, Ardizzoni A, Ciuleanu T, Cobo M, Laktionov K, Szilasi M, et al. CheckMate 171: A phase 2 trial of nivolumab in patients with previously treated advanced squamous non-small cell lung cancer, including ECOG PS 2 and elderly populations. Eur J Cancer. (2020) 127:160–72. doi: 10.1016/j.ejca.2019.11.019
48. Spigel D, Schwartzberg L, Waterhouse D, Chandler J, Hussein M, Jotte R, et al. P3.02c-026 Is Nivolumab Safe and Effective in Elderly and PS2 Patients with Non-Small Cell Lung Cancer (NSCLC)? Results of CheckMate 153. J Thorac Oncol. (2017) 12:S1287–8. doi: 10.1016/j.jtho.2016.11.1821
Keywords: non-small cell lung cancer, checkpoint inhibitors, network meta-analysis, systematic review, frail, older
Citation: Siciliano MA, d’Apolito M, Del Giudice T, Caridà G, Grillone F, Porzio G, Giusti R, Tassone P, Barbieri V and Tagliaferri P (2025) Do age and performance status matter? A systematic review and network meta-analysis of immunotherapy studies in untreated advanced/metastatic non-oncogene addicted NSCLC. Front. Immunol. 16:1635056. doi: 10.3389/fimmu.2025.1635056
Received: 25 May 2025; Accepted: 05 September 2025;
Published: 23 September 2025.
Edited by:
Michael Rückert, Universitätsklinikum Erlangen, GermanyReviewed by:
Zsuzsanna Orosz, University of Debrecen, HungaryDaisuke Morinaga, Hokkaido University Hospital, Japan
Mathias Sonnhoff, Hannover Medical School, Germany
Copyright © 2025 Siciliano, d’Apolito, Del Giudice, Caridà, Grillone, Porzio, Giusti, Tassone, Barbieri and Tagliaferri. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Pierosandro Tagliaferri, dGFnbGlhZmVycmlAdW5pY3ouaXQ=