 Daniel Munárriz1†
Daniel Munárriz1† Luis Gerardo Rodríguez-Lobato1*†Lucía López-Corral2
Luis Gerardo Rodríguez-Lobato1*†Lucía López-Corral2 Cristina Arnaldos-Pérez1Valentín Cabañas3Nieves López-Muñoz4†
Cristina Arnaldos-Pérez1Valentín Cabañas3Nieves López-Muñoz4† Aina Oliver-Caldés1Juan Carlos Ponce5Juan Luis Reguera6Ana África Martín2Núria Martínez-Cibrián1†
Aina Oliver-Caldés1Juan Carlos Ponce5Juan Luis Reguera6Ana África Martín2Núria Martínez-Cibrián1† Natalia Tovar1
Natalia Tovar1 Julio Delgado1Elena Guillen1Sara Varea1Paula Rodríguez-Otero5
Julio Delgado1Elena Guillen1Sara Varea1Paula Rodríguez-Otero5 Álvaro Urbano-Ispizua1
Álvaro Urbano-Ispizua1 José María Moraleda3†
José María Moraleda3† Joaquín Martínez-López4
Joaquín Martínez-López4 María-Victoria Mateos2Verónica González De la Calle2†
María-Victoria Mateos2Verónica González De la Calle2† Europa Azucena González-Navarro1
Europa Azucena González-Navarro1 Carlos Fernández de Larrea1*
Carlos Fernández de Larrea1*- 1Hospital Clínic de Barcelona, Instituto de Investigaciones Biomédicas August Pi i Sunyer (IDIBAPS), University of Barcelona, Barcelona, Spain
- 2University Hospital of Salamanca, Biomedical Research Institute of Salamanca Instituto de Investigación Biomédica de Salamanca, Cancer Research Center Instituto de Biología Molecular y Celular del Cáncer (IBMCC), Consejo Superior de Investigaciones Científicas (CSIC) , Salamanca, Spain
- 3Virgen de la Arrixaca University Clinical Hospital, Instituto Murciano de Investigación Biosanitaria-Arrixaca, University of Murcia, Murcia, Spain
- 4University Hospital 12 de Octubre, Complutense University, Centro Nacional de Investigaciones Oncológicas (CNIO), Madrid, Spain
- 5University Clinic of Navarra, Center for Applied Medical Research (CIMA), Instituto de Investigación Sanitaria de Navarra (IDISNA), Centro de Investigación Biomédica en Red (CIBERONC) CB16/12/00369, Pamplona, Spain
- 6Virgen del Rocío University Hospital, Institute of Biomedicine of Seville (IBIS/CSIC/Centro de Investigación Biomédica en Red (CIBERONC)), University of Seville, Seville, Spain
Background: Chimeric antigen receptor T-cell (CAR-T) therapy targeting B-cell maturation antigen (BCMA) has revolutionized multiple myeloma treatment (MM). However, managing its immune-mediated adverse events, particularly macrophage activation syndrome-like (MAS-like), remains challenging due to underreporting.
Methods: This multicentre, retrospective, analytical study evaluated MM patients treated with the anti-BCMA academic product ARI0002h. MAS-like was defined using the University of California San Francisco (UCSF) consensus criteria. Primary endpoints included baseline characteristics, predictive factors, and survival outcomes associated with MAS-like.
Results: Of 80 patients, 12 (15%) met the UCSF criteria for MAS-like. These patients presented higher ISS scores (ISS III: 54.5% vs. 15.2%; p = 0.006), elevated serum monoclonal components (31.3 g/L vs. 6.8 g/L; p = 0.004), and a higher prevalence of extramedullary disease (41.7% vs. 16.2%; p = 0.057). MAS-like typically emerged 9 days post-infusion, with elevated ferritin, followed by LDH (median 11.5 days) and hypofibrinogenemia (median 14 days). One-third of patients met all UCSF criteria, and all exhibited hypertriglyceridemia, hypertransaminasemia, and cytopenias. Histopathological examination was positive in 63% of evaluated patients. Patients who developed MAS-like had poorer responses (CR: 25% vs. 68%; p = 0.008) and shorter median PFS and OS (7 months vs. 21.4 months and 18 months vs. not reached, respectively; p = 0.004). Those meeting all UCSF criteria had even inferior outcomes.
Conclusions: MAS-like is associated with poorer responses, reduced PFS and OS, especially in patients meeting all UCSF criteria. High tumour burden, including elevated monoclonal component, high ISS and extramedullary disease, seems to contribute to MAS-like development.
Introduction
The development of chimeric antigen receptor T-cell (CAR-T) therapy has revolutionized the treatment landscape for multiple myeloma (MM). Thus, CAR-T therapy is considered one of the key therapeutic options, particularly for patients with relapse/refractory multiple myeloma (R/R MM). Among the principal CAR-T therapies worldwide are idecabtagene vicleucel1 (ide-cel) and ciltacabtagene autoleucel (1, 2) (cilta-cel), both of which have demonstrated a favorable efficacy profile. However, the management of the complications associated with CAR-T remains a significant challenge. Notably, non-relapse mortality (NRM) is higher in multiple myeloma (8.0%) compared to other hematologic malignancies such as large B-cell lymphoma (6.1%) and indolent lymphoma (5.7%) (3). Inflammation-related complications, such as cytokine release syndrome (CRS) and Hemophagocytic Lymphohistiocytosis (HLH), account for up to 25% of NRM as reported by Sidana et al. Furthermore, the immunosuppressive treatments used to manage these complications increase the risk of infections, which represent the leading cause of death in these patients (4). Unfortunately, despite the existence of various consensus definitions of CAR-T-related HLH-like, the ambiguous terminology and lack of strict diagnostic criteria hinder accurate diagnosis (5–8).
Secondary HLH related to cellular therapy has gained increasing recognition in recent years with the expanding use of CAR-T. Initially identified through the classical clinical features of HLH, more recently proposed diagnostic frameworks have introduced related definitions, such as Immune Effector Cell-Associated Hemophagocytic Lymphohistiocytosis-Like Syndrome (IEC-HS) and Macrophage Activation Syndrome-like (MAS-like). Although awareness of this manifestation is increasing, it remains insufficiently characterized in clinical trials of anti-BCMA CAR-T therapy (1, 9). Nevertheless, MAS-like constitutes a relatively frequent complication of BCMA-directed CAR-T therapy, with prior studies reporting an incidence of approximately 20% (7, 10). Despite growing concern, the pathogenesis of MAS-like remains unclear. It is characterized by a distinct cytokine profile compared to CRS, with marked elevations of interferon-γ, granzyme B, interleukin-1 receptor antagonist (IL-1RA), and interleukin-10 (11). Some patients exhibit a biphasic expansion of CAR-T cells. The first peak is predominantly composed of PD1+ T effector cells, while the second peak is characterized by T-cell factor 1 positive (TCF1+) T effector cells, which are primarily involved in memory cell responses. This second expansion phase of CAR-T cells has been associated with the development of an uncontrolled inflammatory response (12).
Controlling the inflammatory response is a key challenge in CAR-T therapy for MM. Academic approaches to CAR-T cell therapy are offering novel insights aimed at enhancing safety, minimizing neurological toxicities, and enabling point-of-care treatments where the bench-clinic-bench time is reduced. For example, cesnicabtagen autoleucel (13) (ARI0002h), an academic anti-BCMA CAR-T developed by Hospital Clínic of Barcelona, is administered in three different fractions (10%, 30%, and 60% of total cells), on non-consecutive days. This methodology has been employed since the development of the anti-CD19 CAR T-cell product ARI0001, with the aim of reducing systemic complications. In this regard, a low incidence of high-grade adverse events and only mild and transient neurological toxicity has been observed in ARI0002h, with no late neurotoxicity (13, 14).
With these results from the multicentre clinical trial CARTBCMA-HCB-01, the approval for use under hospital exemption was granted in Spain (13–15). Our group aimed to investigate the incidence, clinical manifestations, predictive factors and prognosis of MAS-like in patients treated with ARI0002h.
Methods
Cesni-cel (ARI0002h)
ARI0002h is a second-generation CD8α-TMD BCMA-4-1BBζ CAR-T product, lentivirally transduced into autologous T cells collected via peripheral blood leukapheresis (16). This CAR-T cell therapy is an academic product developed by Hospital Clínic of Barcelona in collaboration with the University of Barcelona and IDIBAPS. The CAR-T cell production was conducted at two Spanish centers (Hospital Clínic Barcelona and Clínica Universitaria de Navarra), and the infusions were performed at six different Spanish academic institutions.
Study design and population
For this study, patients who received ARI0002h between July 2020 and January 2024 were analysed, included in clinical trial CARTBCMA-HCB-01 or under compassionate use in our institution. Inclusion and exclusion criteria of CARTBCMA-HCB-01 are detailed in the Supplementary Material (annex 1). Patients received intravenously an initial fractionated infusion of 3 × 106 CAR T cells per kg bodyweight in three aliquots (10%, 30% and 60%, separated by 48 hours). If adverse events occurred between administrations, the remaining doses were withheld, except in cases of low-grade toxicity, in which the infusion continued after resolution. A non-fractionated booster dose of up to 3 × 106 CAR T cells per kg bodyweight was administered, at least 100 days after the first infusion (13). This fractioning protocol was also employed in the clinical trial CART19-BE-01 (17) with ARI-0001, and has demonstrated limited immune-related side-effects such as CRS and immune effector cell-associated neurotoxicity (ICANS), without reducing efficacy (14).
The data collected for this study was updated until October 2024. The study was approved by the Institutional Review Board of Hospital Clínic of Barcelona and adhered to the principles of the Declaration of Helsinki.
Definitions and outcomes of interest
MAS-like was defined according to University of California San Francisco (UCSF) consensus criteria: [1] ferritin rise ≥100 mg/L/h within a 24-hour period and [2] minimum fibrinogen <150 mg/dL or maximum lactate dehydrogenase >2 times the upper limit of normal or histopathological diagnosis (hemophagocytosis) (7). Patients were retrospectively assessed and catalogued according to the UCSF criteria. Definition of disease evaluation, such as overall response rate (ORR), complete response (CR), very good partial response (VGPR) and partial response (PR) was done according to International Myeloma Working Group (IMWG) (18).
The main endpoints included an analysis of baseline characteristics, PFS and OS based on patients who developed MAS-like. We also explored how to identify risk factors for developing MAS-like and to characterize the clinical manifestations of this syndrome. In survival analyses, PFS was defined from the CAR-T infusion time to disease progression or death. OS was defined as the time from the day of CAR-T administration to death from any cause.
Variants related to HLH by exome sequencing
We performed targeted exome sequencing focusing on a panel of HLH-related genes believed to influence the predisposition to macrophage activation syndrome (MAS). The genes included in this panel are listed in Supplementary Table 1. Genomic DNA was extracted from peripheral blood, and library preparation was carried out according to the Agilent SureSelect protocol, with sequencing performed using the NovaSeqX platform.
Exome data were analyzed using the Galaxy platform, and quality control was performed using the FastQC tool. Reads were mapped to the reference human genome (hg38) using the BWA-MEM2 tool. Variant calling was performed with the FreeBayes tool, and the identified variants were annotated using the online Ensembl Variant Effect Predictor (19).
Variants were filtered based on their location (exonic regions plus 3 base pairs into the intronic regions), minor allele frequency (<0.04 in GnomAD, to avoid missing polymorphisms considered as risk factors) (20) and predicted impact on protein function. Variants with a frequency >1% in the general population in GnomAD that had not been reported as risk factors were excluded.
Statistical analysis
Continuous variables were assessed using Student’s t-test or appropriate non-parametric methods. Categorical variables were summarized as frequencies and percentages, and statistical comparisons made using Fisher’s test. Median follow-up was calculated using the reverse Kaplan–Meier method. The optimal cutoff points of quantitative variables were determined using receiver operating characteristic (ROC) curve analysis.
Univariate and multivariate logistic regression models were employed to identify factors associated with MAS-like development. The starting point for time-to-event analysis was the CAR T-cell infusion. The development of MAS-like was analysed as a time-varying covariate. Cox proportional hazards regression with backward stepwise selection was utilized to identify factors associated with PFS and OS. A Cox proportional hazards model was fitted to examine the effect of MAS-like on patient survival. The proportionality assumption was evaluated using the Schoenfeld test, which revealed no evidence of violation of this assumption (p = 0.56).
All statistical tests were two-tailed, with significance set at an alpha level of 0.05. For subgroup analyses, p-values were also adjusted using the False Discovery Rate (FDR) method, in the context of a small sample size. Analyses were conducted using RStudio 2024.04.4, and GraphPad Prism 10.
Results
Patient characteristics
A total of 80 patients who received ARI0002h between July 2020 and January 2024 were analysed with a median follow-up of 16.5 months (IQR 9.3-21.8). Among then, 60 patients were included in clinical trial CARTBCMA-HCB-01 and 20 were treated under compassionate use, with similar inclusion and exclusion criteria. The CAR-T cell infusions were performed at six different Spanish academic institutions. The baseline characteristics of the cohort are summarized in Table 1. The median age of patients was 59 years, and the most frequent heavy chain isotype was IgG (51%). Extramedullary disease was observed in 20% of cases, and 38% of patients exhibited high-risk cytogenetics. The median number of prior lines of therapy was 3, with 58% of patients being triple-refractory. Additionally, 21% of patients presented with an International Staging System (ISS) stage III at the time of enrolment. After CAR-T cell therapy, ORR was 96% and CR 62% in the whole series, with a median PFS of 20 months (95% CI 13.8-23.6) and median OS not reached (95% CI 21.5-NR). CRS occurred in 81% of patients (4.6% grade ≥3), with two cases of ICANS (2.5%) grade 1 (Table 2).
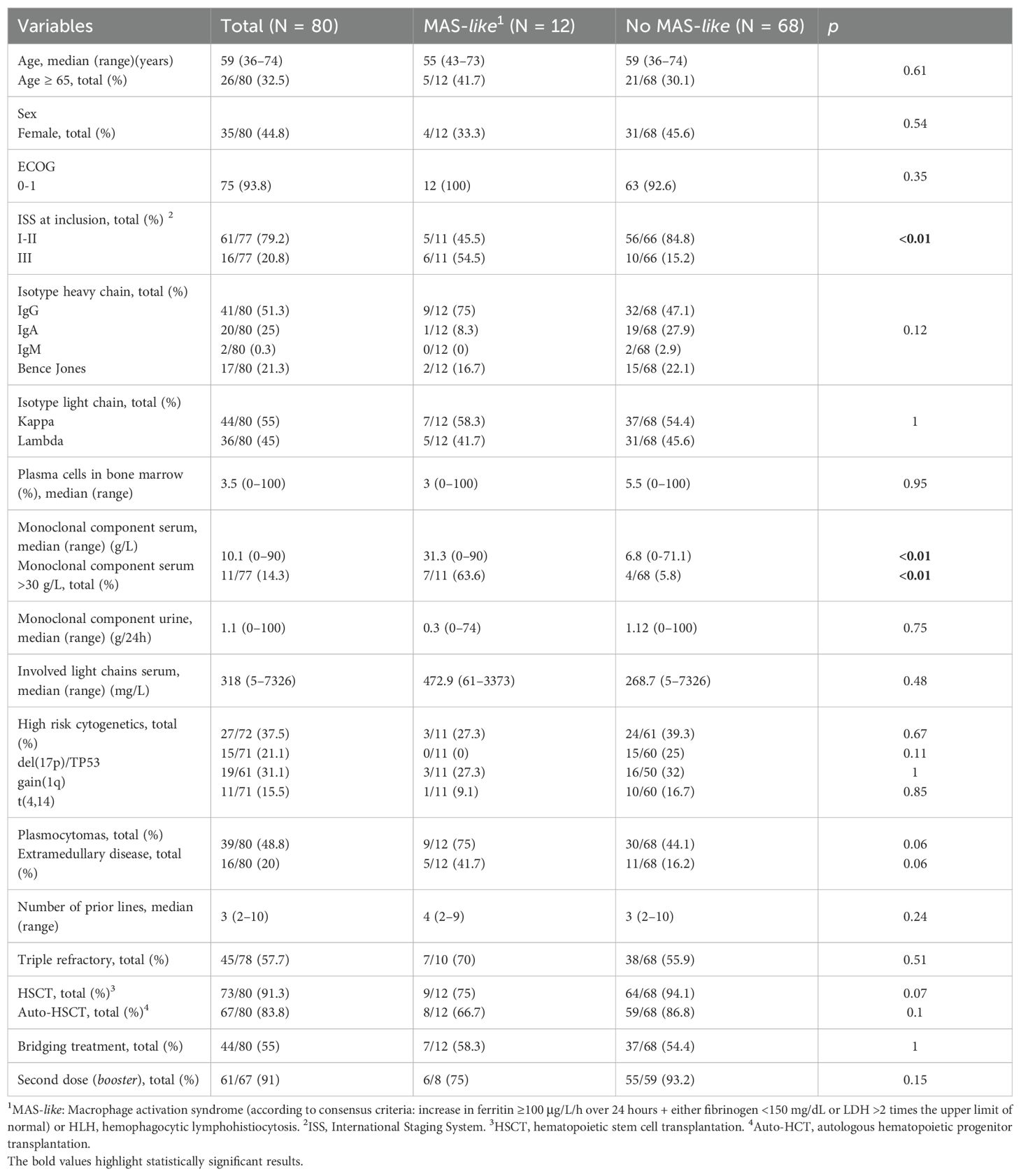
Table 1. Baseline characteristics of the patients analyzed.
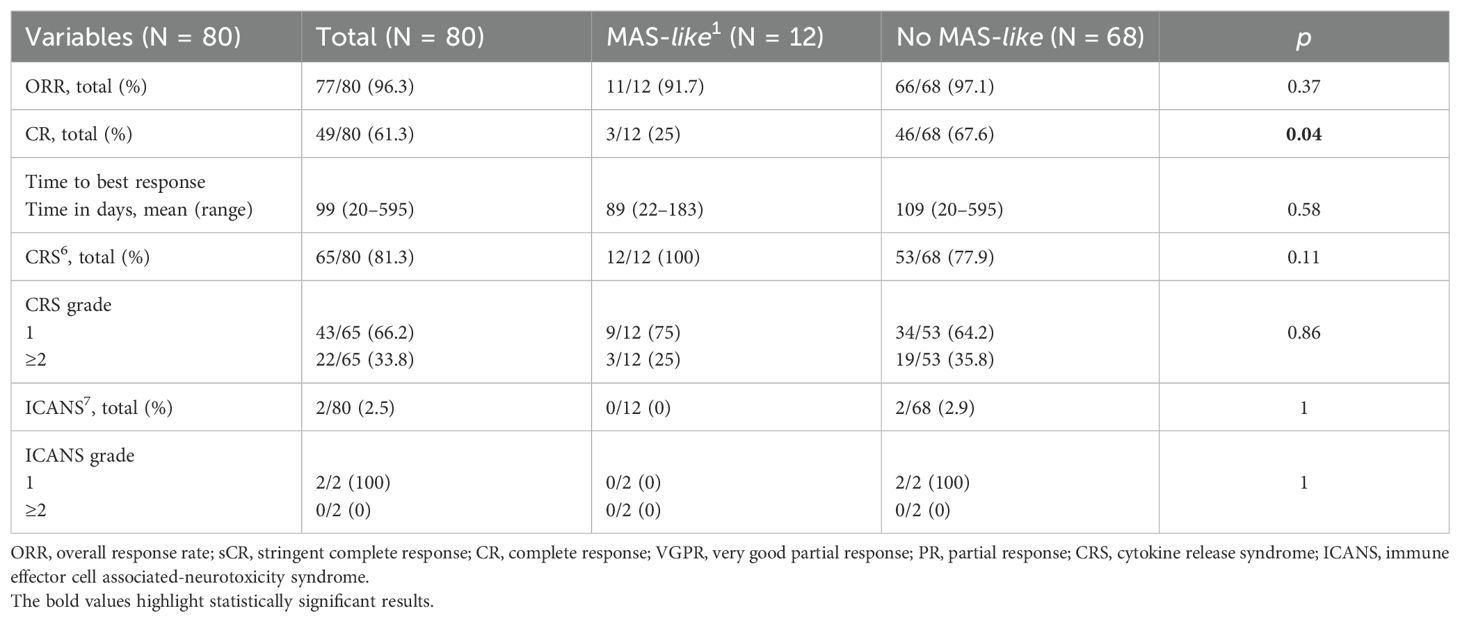
Table 2. Response grade and toxicities (cytokine release syndrome [CRS] and immune effector cell-associated neurotoxicity syndrome [ICANS]) following infusion.
MAS-like syndrome characteristics
Among the 80 patients, 12 met the criteria for MAS-like (15%). These patients had a higher International Staging System (ISS) score at enrolment (ISS III 54.5 vs 15.2%, p = 0.006) and elevated serum monoclonal component levels compared to the controls (31.3 vs 6.8 g/L, p = 0.004). No other significant differences were observed, although there was a higher prevalence of extramedullary disease (41.7% vs. 16.2%, p = 0.057). The incidence of infection prior to infusion (<2 months) was explored and was not found to be increased. Referring to immune kinetics, CAR-T cell expansion and soluble BCMA levels in peripheral blood were analyzed, without revealing any statistically significant differences between patients who developed MAS-like and those who did not.
The characteristics of MAS-like are summarized in Table 3. The syndrome predominantly occurred following the administration of the third fraction of the first dose (83.3%) and approximately 9 days after the first aliquot, characterized by an initial increase in ferritin, which reached its peak at a median of 5 days. This increase was followed by a rise in lactate dehydrogenase (LDH) levels (median 11.5 days), and subsequently by hypofibrinogenemia (median 14 days). The moment when at least two criteria were met was approximately with a median of 10 days (IQR 9.5-14.5). The LDH criterion was met more frequently than the fibrinogen criterion (83.3% vs. 60%). One-third of the patients met all three criteria during the MAS-like episode (33%). In this cohort, the maximum ferritin level (median 10991 ng/mL, IQR 6357-17334) coincided with the minimum fibrinogen level (median 0.81 g/L, IQR 0.77-2), showing a weak negative correlation (-0.38, p = 0.401) (Supplementary Figure 1).
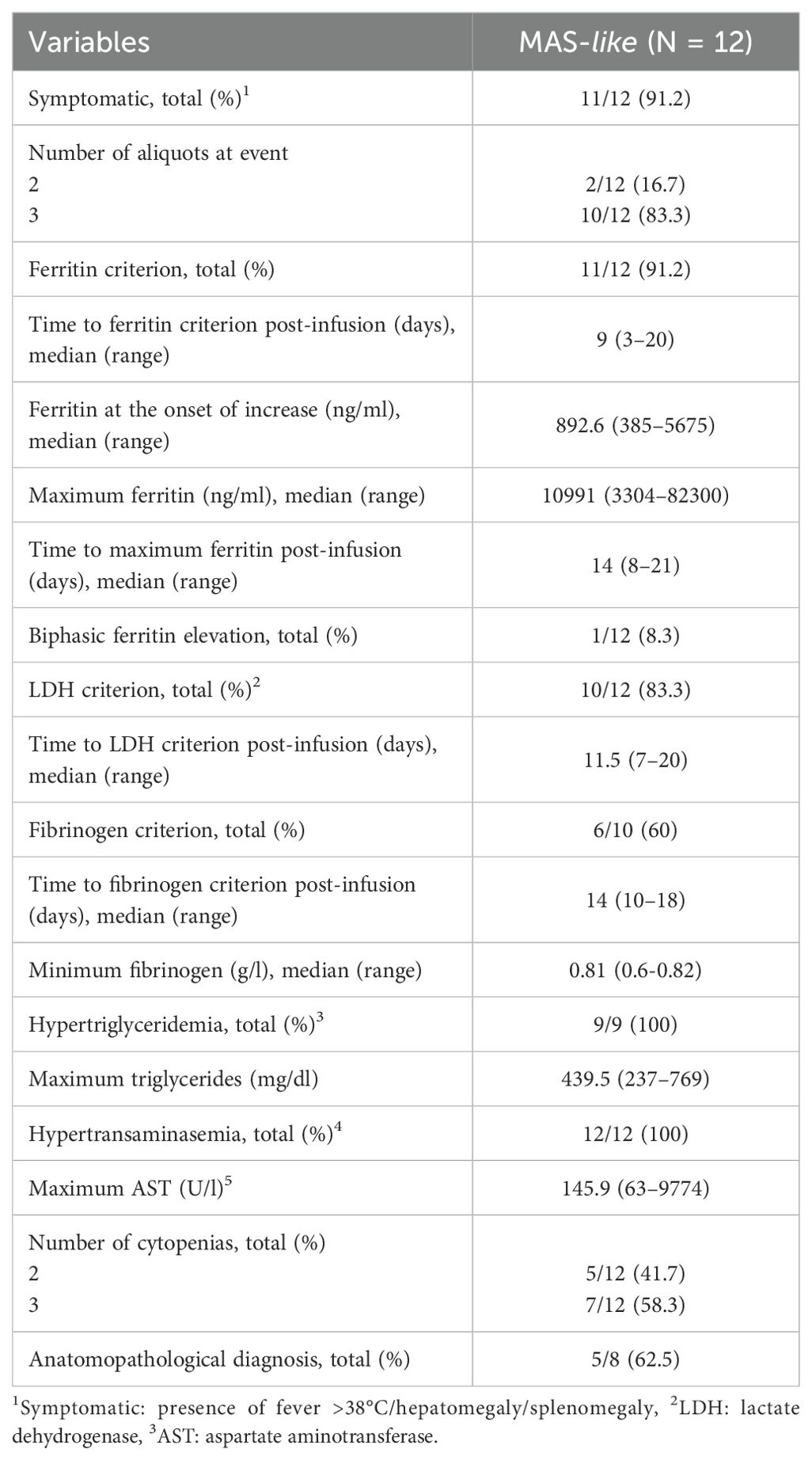
Table 3. Clinical and analytical characteristics of patients affected by MAS-like.
All patients exhibited classical MAS features, including hypertriglyceridemia (>150 mg/dL), hypertransaminasemia (AST >30 U/L), and ≥ 2 cytopenias (defined as haemoglobin <10 g/dl, platelets <100×10^9/l and leucocytes <4×10^9/l). Pancytopenia was found in 58.3% of patients (7 out of 12). Histopathological examination, based on bone marrow aspiration or tissue biopsy, was positive in 5 out of 8 patients evaluated (62.5%).
Association with HLH DNA variants
Sequencing of exonic regions of an HLH-related gene panel was performed on 44 patients (12 who developed MAS-like and 32 who did not). We identified 7 genetic variants in patients who developed MAS-like and 23 in the control group (Supplementary Table 2). Key variants were observed in the PRF1 and UNC13D genes. For instance, the PRF1 Ala91Val variant, known to impair perforin activity (20), was found in 16.7% of patients with MAS-like and 12.5% of patients without MAS-like. Statistical analysis did not show a significant difference, suggesting that other factors might contribute to MAS-like development alongside genetic predispositions.
MAS-like treatment
Treatment was primarily based on tocilizumab (an anti-IL-6 agent), corticosteroids and anakinra (an anti-IL-1 agent). Most patients (75%) received at least one dose of tocilizumab at the standard dose of 8 mg/kg, with 37.5% and 12.5% receiving two and three doses, respectively. Dexamethasone was administered in half of the cases, with daily doses ranging between 10 and 20 mg and a median duration of 3 days. Nearly half of the patients (42%) received combination therapy. Four patients (33%) required anakinra at 8 mg/kg/day, with a median duration of 5 days. No additional drugs commonly employed in MAS-like were used.
Factors associated with the development of MAS-like
In the univariate analysis (Supplementary Table 3A), an ISS score of 3 at screening was associated with an increased risk of developing MAS-like (OR: 6.72, 95% CI: 1.72–26.3, p = 0.006), as was a higher serum monoclonal component (OR: 1.06, 95% CI: 1.02–1.1, p = 0.003). The predictive performance of the serum monoclonal component for MAS-like syndrome was further assessed using ROC analysis, yielding a T value of 4.18 (p = 0.00007). A threshold of 29.4 g/L demonstrated the highest predictive accuracy (AUC: 0.7645, 95% CI: 0.5831–0.9458). Additionally, serum monoclonal component levels greater than 30 g/L were associated with a significantly increased risk (OR: 14.6, 95% CI: 3.28–65.4, p = 0.0004). The presence of extramedullary disease was associated with a non-significantly increased risk (OR: 3.7, 95% CI: 0.99–13.80, p = 0.051). In the multivariate analysis (Supplementary Table 3B), serum monoclonal component greater than 30 g/L remained statistically significant (OR: 10.1, 95% CI: 1.67–61.5, p = 0.01).
Impact of MAS-like development on patient clinical outcomes
The ORR of the cohort was 96%, with 89% of patients achieving at least a VGPR. A stringent complete response was observed in 58% of patients, 28% achieved VGPR, and 8% attained a partial response (Table 2). One patient (1%) was refractory, and 2 patients (3%) died prior to the first evaluation. One of these fatalities was attributed to MAS-like, with histopathological evidence found in the liver tissue. Patients who developed MAS-like exhibited a significantly lower response compared to controls (≥CR 25% vs. 68%, p = 0.008). Furthermore, patients who met all three criteria exhibited a worse response than those who met only two (VGPR or better: 25% vs. 100%, p = 0.04).
Median PFS was shorter in patients who developed MAS-like [7 months (95% CI 4.83-22.87) vs. 21.4 months (95% CI 15.77-25.26)], HR 2.75 (95% CI 1.32-5.69); p = 0.004 (Figure 1A). Median OS for patients who developed MAS-like was 18 months (95% CI 6.35-NR), compared to not reached for the control group, HR 3.61 (95% CI 1.43-9.07); p = 0.004 (Figure 1B). Moreover, patients who met all three UCSF criteria, compared to those who met only two, exhibited significantly poorer PFS [5.45 months (95% CI 0.69-NR) vs 11.83 (95% CI 6.84-NR)]; p = 0.012) and OS [7.82 (95% CI 0.69-NR) vs 21.45 (95% CI 9.17-NR)]; p = 0.017 (Figure 2). Results after FDR correction lose significance due to the small event count. In multivariable analysis, MAS-like lost its statistical significance for PFS and OS, unlike other variables such as the ISS, serum monoclonal component, or extramedullary disease (Supplementary Table 4 and 5).
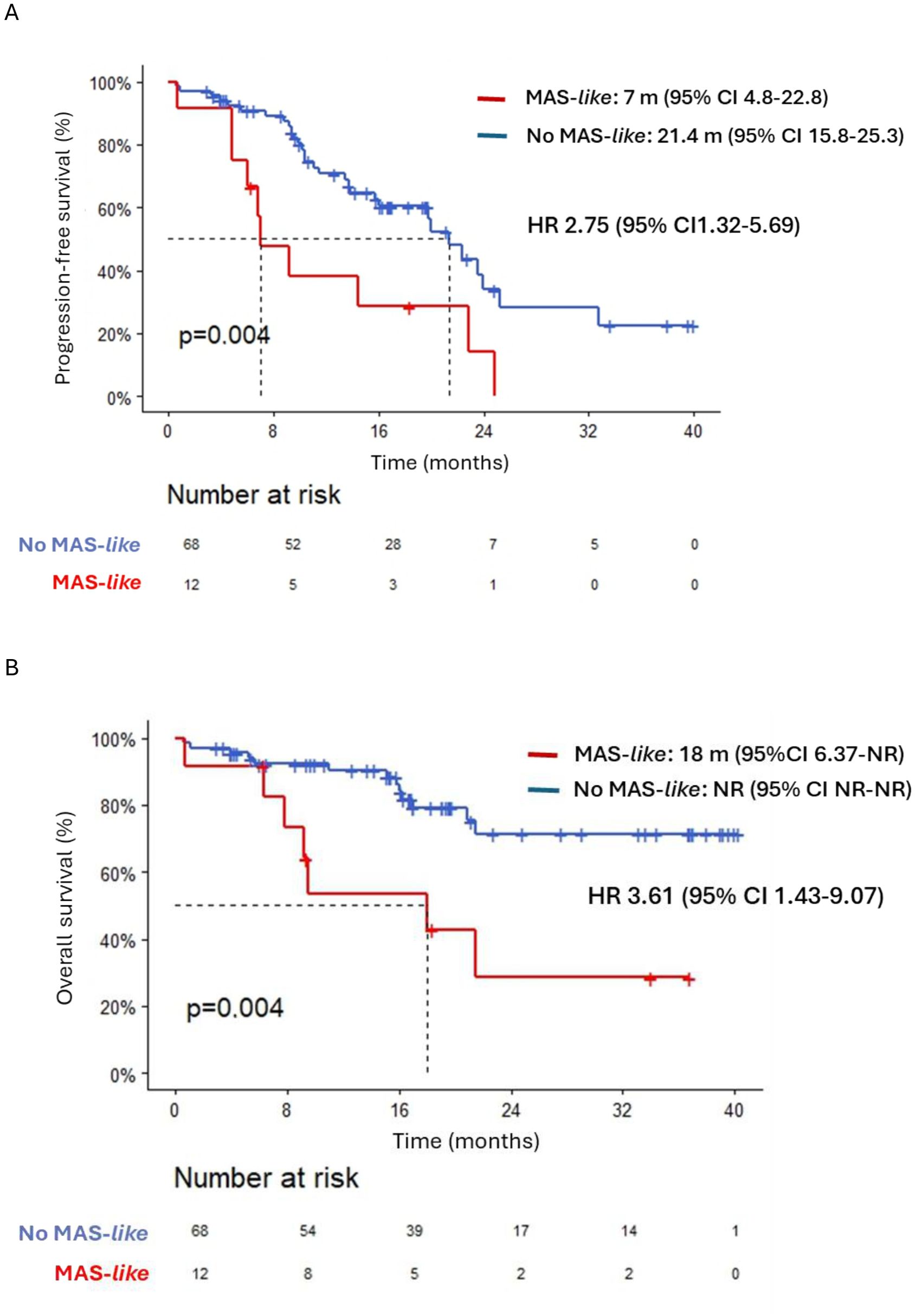
Figure 1. (A) Progression-free survival in patients who developed MAS-like compared to those who did not. (B) Overall survival in patients who developed MAS-like compared to those who did not.
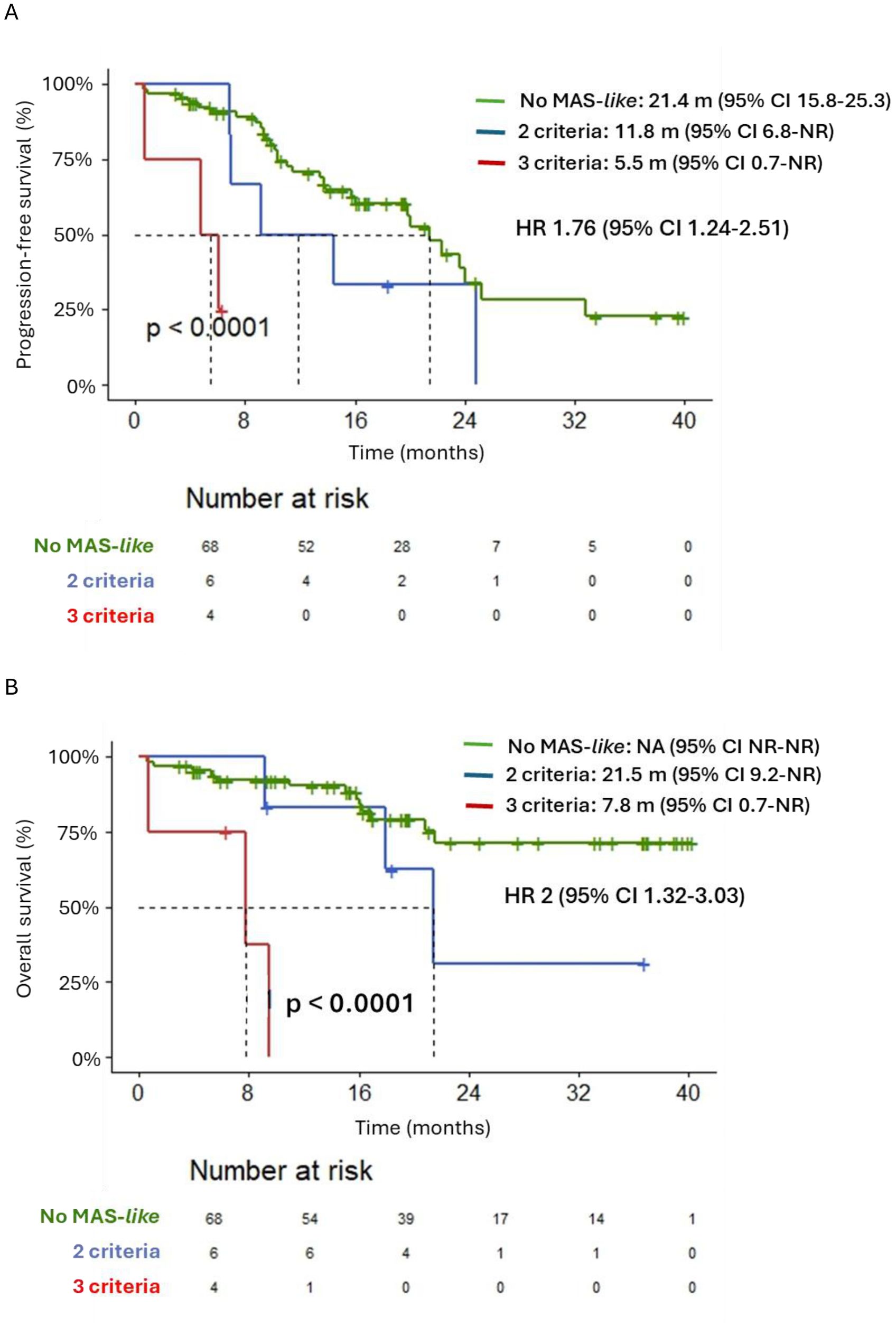
Figure 2. (A) Progression-free survival in patients according to the number of University California San Francisco criteria they met (No MAS-like, MAS-like with 2 criteria and MAS-like with 3 criteria). (B) Overall survival in patients according to the number of University California San Francisco criteria they met (No MAS-like, MAS-like with 2 criteria and MAS-like with 3 criteria).
Discussion
Anti-BCMA CAR T-cell therapy has demonstrated a significant impact on the treatment of patients with MM; however, this novel therapeutic approach is associated with a distinct spectrum of immune-mediated adverse events, such as MAS-like. Notably, this complication is likely underreported in both clinical trials and real-world studies. In the present cohort of 80 patients treated with the anti-BCMA product ARI0002h, we observed an incidence of 15%, which was correlated with poorer treatment responses and reduced survival outcomes.
The diagnosis of secondary HLH/MAS-like remains challenging due to the absence of a definitive diagnostic test and the overlap of its clinical manifestations with other adverse events, such as CRS (21). Consequently, the incidence of MAS-like is not consistently reported in clinical trials and varies depending on the diagnostic criteria employed; many reports are based on retrospective analysis. Furthermore, both the type of tumour and the specific CAR T-cell product used are critical factors influencing the development of this complication. Anti-CD22-targeted CAR T-cell therapies have been associated with a notably high incidence of HLH-like reactions, with rates reaching up to 36% in certain cohorts (22, 23). Anti-CD19-based CAR T-cell therapies, in contrast, appear to be associated with a lower incidence of HLH/MAS-like (24). For instance, the reported incidence of HLH in real-world studies of axicabtagene ciloleucel (axi-cel), based on the HLH-2004 criteria, is up to 5% in patients with diffuse large B-cell lymphoma (DLBCL) (25).
MAS-like appears to be a relatively common entity observed in patients with MM undergoing CAR-T cell therapy. The incidence rates vary from 4% in the ide-cel clinical trial (1) to approximately 20% in certain real-world cohorts of patients treated with anti-BCMA CAR T-cell products (7, 10). As a potential pathophysiological explanation, the upregulation of major histocompatibility complex (MHC)-II expression on MM cells, triggered by IFN-γ, may contribute to the dysregulated immune response within the pro-inflammatory microenvironment following CAR T-cell infusion (26). The lower incidence of MAS-like, according to UCSF criteria, observed in ARI0002h (15%) compared to the 22% reported by Kennedy et al. (7) may be related to the initial fractionated infusion strategy and the withholding of treatment in the presence of adverse events. This hypothesis is supported by the reduced incidence of severe adverse events, such as CRS, in the few products administered in a fractionated schedule, including LCAR-B38M (LEGEND-2 study) and ARI0001 (CART19-BE-01), although differences among constructs should be taken into consideration (17, 27). Differences between MAS-like cases reported with other commercial CAR-T products and ARI0002h may be attributed to the distinct diagnostic criteria used. For this study, the UCSF consensus criteria were selected among other available definitions, owing to their clarity and well-defined requirements. Based on our findings, the UCSF criteria appear to be highly sensitive but may prone to overdiagnosing MAS-like. Nevertheless, our group posits that early diagnosis—prior to the onset of full organ failure and the severe manifestations of the syndrome—may enhance management and improve patient outcomes (28).
Based on our results, a higher tumour burden, as indicated by an increased serum monoclonal component, and a higher ISS at enrolment, were significantly more frequent in patients who developed MAS-like. Indeed, an ISS of III and elevated serum monoclonal component were associated with an increased risk of developing this complication. The involvement of high tumour burden has been previously identified in other hematologic malignancies (29, 30); however, MAS-like predisposing factors associated with CAR T-cell therapy have not been well characterized in multiple myeloma. These findings support the hypothesis of an uncontrolled inflammatory response activated by high tumour antigen concentrations (31). The prevalence of extramedullary disease prior to infusion demonstrated a borderline association (p = 0.057), although its potential role in MAS-like is supported by previous reports indicating that its presence increases the risk of CRS (32). In this context, extramedullary disease may elicit a MAS-like through its tumour microenvironment, which is enriched with M2 polarized tumour-associated macrophages (TAM) that secrete IL-6 (33, 34).
According to the literature, this complication typically manifests in a delayed manner following infusion, most often after the onset of CRS (7, 10, 35). Our findings support this observation, as MAS-like syndrome developed later (median of 10 days after the first infusion to meet UCSF criteria, compared to a median of 7 days for CRS), even when the product was administered in progressively increasing doses, as in the case of ARI0002h. The increase in ferritin levels >100 mg/L/h within a 24-hour period was the most sensitive parameter analysed. This finding supports the value of ferritin measurement when CAR-T inflammatory toxicity is suspected, as it may help to identify patients at risk of developing MAS-like syndrome. LDH appeared to meet the criteria more frequently than fibrinogen, and a significant poor prognosis was observed in patients who met all three criteria. Patients who met the UCSF criteria exhibited other clinical and laboratory features commonly associated with classical MAS, such as hypertransaminasemia, hypertriglyceridemia, and cytopenias (36, 37). Additionally, most patients showed histopathological findings consistent with MAS.
In line with previous reports, ARI0002h demonstrates favourable efficacy outcomes. The median PFS of the entire cohort was 20 months, with the median OS not reached, which is in line with the outcomes of currently approved CAR-T therapies for MM (1, 9). However, patients who developed MAS-like exhibited a poorer response rate (CR 25% vs. 68%) and impaired survival (median PFS 7 months vs. 21.4 months, median OS 18 months vs. not reached). The differences observed were more pronounced in patients who met all three criteria compared to those who met only two (median PFS 5.5 months vs. 11.8 months, median OS 7.8 months vs. 21.5 months). The better outcomes in patients who met only two UCSF criteria may support the necessity of early detection of MAS-like syndrome before all manifestations are fully developed. However, subgroup analyses are severely underpowered (12 events, 4 with UCSF = 3). Therefore, results should be interpreted as hypothesis-generating only. Furthermore, the contribution of a higher tumour burden to the poorer outcomes observed in these patients must be taken into account. Together with the limited sample size and the relatively low frequency of MAS-like as an adverse event, this may explain the loss of statistical significance in the multivariate analysis.
Our genetic analysis suggests a complex interplay between inherited genetic factors and the development of MAS-like in patients undergoing CAR-T therapy. Variants in UNC13D and PRF1, previously reported to impair perforin activity (20), were not statistically significant predictors on their own. However, when combined with high disease burden and extramedullary disease, they may increase the risk of MAS-like, as suggested by our clinical correlation analysis. These findings reinforce the multifactorial nature of MAS in the setting of advanced therapies such as CAR-T. However, the reduced sample size, together with the limited incidence of MAS-like, hampers the ability to draw definitive conclusions and may increase the influence of outliers.
The treatment of MAS-like syndrome requires the control of the inflammatory loop and close monitoring. There is a wide variety of drugs that are often employed without a standard algorithm. Although controversy exists in some cases, the most frequently used drugs are antibodies or recombinant proteins targeting interleukins, such as anakinra (IL-1) or tocilizumab (IL-6), systemic steroids, ruxolitinib (a JAK inhibitor), emapalumab (an IFN-γ inhibitor), and etoposide (31, 38–42). In this study, most patients who developed MAS-like received standard CRS management, which comprises anti-IL6, anti-IL1, and steroids. This is consistent with the initial diagnosis of CRS at the beginning of treatment. Noticeably, a half of patients required two or more drugs (mainly tocilizumab and dexamethasone). The limited use of anakinra may be related to its approval for IEC-HS treatment in our country only after July 2023, by which time most patients had already received ARI0002h. Nonetheless, these observations suggest that CRS and MAS-like syndrome share several features of systemic inflammation, in which prompt therapeutic intervention may be crucial to prevent the establishment of a positive feedback loop.
Our study has several limitations. This multicentre study involved a cohort of 80 patients treated with the same anti-BCMA CAR-T therapy, in a context of scarcity of studies focused on this complication. Nevertheless, the retrospective design and the limitation to a single country may introduce potential biases. Moreover, the analytical criteria employed may be insufficient for accurately differentiating between the hyperinflammation associated with CRS and MAS-like syndrome. Other criteria with different sensitivity and specificity could be explored prospectively in the future.
In summary, the development of MAS-like is associated with poorer responses and shortened PFS and OS in patients with MM treated with ARI0002h, especially in those who meet all three criteria: elevated ferritin, decreased fibrinogen, and increased LDH. Therefore, further research is required to establish diagnostic criteria that enable early identification and timely therapeutic management of MAS-like.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
Ethics statement
The studies involving humans were approved by Institutional Review Board of Hospital Clínic of Barcelona. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
DM: Data curation, Formal Analysis, Investigation, Methodology, Project administration, Writing – original draft, Writing – review & editing. LR-L: Conceptualization, Funding acquisition, Project administration, Supervision, Writing – original draft, Writing – review & editing. LL-C: Data curation, Writing – original draft, Writing – review & editing. CA-P: Data curation, Formal Analysis, Writing – original draft, Writing – review & editing. VC: Writing – original draft, Writing – review & editing. NL-M: Data curation, Writing – review & editing. AO-C: Data curation, Writing – review & editing. JP: Writing – review & editing. JR: Writing – review & editing. AM: Writing – review & editing. NM-C: Data curation, Writing – review & editing. NT: Data curation, Writing – review & editing. JD: Resources, Writing – review & editing. EG: Writing – review & editing. SV: Writing – review & editing. PR-O: Data curation, Writing – review & editing. AU-I: Writing – review & editing. JM: Writing – review & editing. JM: Writing – review & editing. MM: Writing – review & editing. VG: Writing – review & editing. EG-N: Formal Analysis, Supervision, Writing – review & editing. CF: Conceptualization, Funding acquisition, Project administration, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research and/or publication of this article. This study was supported by grants from the Instituto de Salud Carlos III (cofounded by the European Union) and the Spanish Ministry of Health (ICI19/00025 and PI22/00647), the RICORS-TERAV network (RD21/0017/0009 and RD21/0017/0019, RD21/0017/0001, RD21/0017/0006 and RD21/0017/0030), Red de Terapia Celular TERCEL (RD16/0011/0005), Fondo Europeo de Desarrollo Regional, 2021-SGR-01292 (AGAUR; Generalitat de Catalunya), Centro de Investigación Biomédica en Red de Cáncer (CB16/12/00369 and CB16/12/00489), La Caixa Foundation (CP042702/LCF/PR/GN18/50310007), Asociación Española Contra el Cancer LABAE21971FERN, and Fundació Bosch I Aymerich support. AO-C. from the resident grant Ajut Clínic-La Pedrera 2019, granted by Hospital Clínic de Barcelona. LR-L. has received funding from the CRIS Cancer Foundation (project number: PR_TMT_2023-6).
Acknowledgments
The authors would like to sincerely thank the patients and their families for their invaluable participation. We also express our appreciation to all the staff members from the Haematology, Immunology, Clinical Pharmacology, and other departments at Hospital Clínic in Barcelona, Hospital Clínico Universitario de Salamanca, Hospital Clínico Universitario Virgen de la Arrixaca in Murcia, Clínica Universidad de Navarra, and Hospital Universitario Virgen del Rocío in Seville, whose commitment to patient care was essential. In addition, we acknowledge the efforts of the researchers who contributed to the preclinical development of this institutional CAR T-cell construct, as well as the members of the Data and Safety Monitoring Board (DSMB) for their crucial oversight.
Conflict of interest
LR-L declares honoraria and travel grants from Janssen, Amgen, Bristol Myers Squibb, GlaxoSmithKline, Menarini, and Sanofi. NL-M declares support for attending meetings or travel from Janssen, Amgen, Sanofi. AU-I is one of the inventors of ARI0002h patent ownership transferred to Hospital Clinic, IDIBAPS, and University of Barcelona. VG declares consulting or advisory role for Johnson & Johnson and GlaxoSmithKline. Speakers’ Bureau: Johnson & Johnson, GlaxoSmithKline, Pfizer.Travel, Accommodations, Expenses: Johnson & Johnson, GlaxoSmithKline. CF declares receiving grants through his institution from Bristol Myers Squibb, Janssen, and Amgen; reports honoraria from Amgen, Janssen, Bristol Myers Squibb, GlaxoSmithKline, and Sanofi; reports support for attending meetings or travel from Janssen, Bristol Myers Squibb, GlaxoSmithKline, and Amgen; and reports participation on advisory boards with Janssen, Bristol Myers Squibb, Amgen, Pfizer, and Sanofi.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be constructed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2025.1654096/full#supplementary-material
References
1. Munshi NC, Anderson LD, Shah N, Madduri D, Berdeja J, Lonial S, et al. Idecabtagene vicleucel in relapsed and refractory multiple myeloma. N Engl J Med. (2021) 384:705–16. doi: 10.1056/NEJMoa2024850
2. Berdeja JG, Madduri D, Usmani SZ, Jakubowiak A, Agha M, Cohen AD, et al. Ciltacabtagene autoleucel, a B-cell maturation antigen-directed chimeric antigen receptor T-cell therapy in patients with relapsed or refractory multiple myeloma (CARTITUDE-1): a phase 1b/2 open-label study. Lancet. (2021) 398:314–24. doi: 10.1016/S0140-6736(21)00933-8
3. Cordas dos Santos DM, Tix T, Shouval R, Gafter-Gvili A, Alberge JB, Cliff ERS, et al. A systematic review and meta-analysis of nonrelapse mortality after CAR T cell therapy. Nat Med. (2024) 30:2667–78. doi: 10.1038/s41591-024-03084-6
4. Sidana S, Patel KK, Peres LC, Bansal R, Kocoglu MH, Shune L, et al. Safety and efficacy of standard-of-care ciltacabtagene autoleucel for relapsed/refractory multiple myeloma. Blood. (2025) 145:85–97. doi: 10.1182/blood.2024025945
5. Sandler RD, Tattersall RS, Schoemans H, Greco R, Badoglio M, Labopin M, et al. Diagnosis and management of secondary HLH/MAS following HSCT and CAR-T cell therapy in adults; A review of the literature and a survey of practice within EBMT centres on behalf of the autoimmune diseases working party (ADWP) and transplant complications working party (TCWP). Front Immunol. (2020) 11:524. doi: 10.3389/fimmu.2020.00524
6. Neelapu SS, Tummala S, Kebriaei P, Wierda W, Gutierrez C, Locke FL, et al. Chimeric antigen receptor T-cell therapy — assessment and management of toxicities. Nat Rev Clin Oncol. (2018) 15:47–62. doi: 10.1038/nrclinonc.2017.148
7. Kennedy VE, Wong C, Huang CY, Kambhampati S, Wolf J, Martin TG, et al. Macrophage activation syndrome-like (MAS-L) manifestations following BCMA-directed CAR T cells in multiple myeloma. Blood Adv. (2021) 5:5344–8. doi: 10.1182/bloodadvances.2021005020
8. Henter JI, Horne A, Aricó M, Egeler RM, Filipovich AH, Imashuku S, et al. HLH-2004: Diagnostic and therapeutic guidelines for hemophagocytic lymphohistiocytosis. Pediatr Blood Cancer. (2007) 48:124–31. doi: 10.1002/pbc.21039
9. Martin T, Usmani SZ, Berdeja JG, Agha M, Cohen AD, Hari P, et al. Ciltacabtagene autoleucel, an anti–B-cell maturation antigen chimeric antigen receptor T-cell therapy, for relapsed/refractory multiple myeloma: CARTITUDE-1 2-year follow-up. J Clin Oncol. (2023) 41:1265–74. doi: 10.1200/JCO.22.00842
10. Zu C, Wang K, Zhang Q, Hu Y, and Huang H. Clinical features of hemophagocytic syndrome following BCMA CAR-T cell therapy in patients with relapsed/refractory multiple myeloma. Zhejiang Xue Xue Bao Yi Xue Ban J Zhejiang Univ Med Sci. (2022) 51:160–6. doi: 10.3724/zdxbyxb-2022-0039
11. Zu C, Wu S, Zhang M, Wei G, Xu H, Cui J, et al. A distinct cytokine network distinguishes chimeric antigen receptor T cell (CAR-T)-associated hemophagocytic lymphohistiocytosis-like toxicity (carHLH) from severe cytokine release syndrome following CAR-T therapy. Cytotherapy. (2023) 25:1167–75. doi: 10.1016/j.jcyt.2023.06.008
12. Yan W, Xiong Y, Lv R, Du C, Yu T, Zhang S, et al. Uncommon biphasic CAR-T expansion induces hemophagocytic lymphohistiocytosis-like syndrome and fatal multiple infections following BCMA CAR-T cell therapy: a case report. J Immunother Cancer. (2024) 12:e010080. doi: 10.1136/jitc-2024-010080
13. Oliver-Caldés A, González-Calle V, Cabañas V, Español-Rego M, Rodríguez-Otero P, Reguera JL, et al. Fractionated initial infusion and booster dose of ARI0002h, a humanised, BCMA-directed CAR T-cell therapy, for patients with relapsed or refractory multiple myeloma (CARTBCMA-HCB-01): a single-arm, multicentre, academic pilot study. Lancet Oncol. (2023) 24:913–24. doi: 10.1016/S1470-2045(23)00222-X
14. Oliver-Caldes A, Gonzalez-Calle V, Cabañas V, Lopez-Muñoz N, Rodriguez Otero P, Reguera JL, et al. ARI0002h (Cesnicabtagene autoleucel), an academic point-of-care B-cell maturation antigen (BCMA)-directed chimeric antigen receptor (CAR) T-cell strategy: activity and safety after fractionated initial therapy and booster dose in 60 patients with relapsed/refractory multiple myeloma. Blood. (2023) 142:1026. doi: 10.1182/blood-2023-180828
15. Fernandez de Larrea C, Oliver-Caldés A, Gonzalez de la Calle V, Cabañas V, López-Muñoz N, Rodríguez-Otero P, et al. Long-term follow-up of ARI0002h (cesnicabtagene autoleucel), an academic point-of-care B-cell maturation antigen (BCMA)-directed chimeric antigen receptor (CAR) T-cell strategy: Activity and safety after fractionated initial therapy and booster dose in 60 patients with relapsed/refractory multiple myeloma (RRMM). J Clin Oncol. (2024) 42:7544–4. doi: 10.1200/JCO.2024.42.16_suppl.7544
16. Perez-Amill L, Suñe G, Antoñana-Vildosola A, Castella M, Najjar A, Bonet J, et al. Preclinical development of a humanized chimeric antigen receptor against B cell maturation antigen for multiple myeloma. Haematologica. (2021) 106:173–84. doi: 10.3324/haematol.2019.228577
17. Ortíz-Maldonado V, Rives S, Castellà M, Alonso-Saladrigues A, Benítez-Ribas D, Caballero-Baños M, et al. CART19-BE-01: A multicenter trial of ARI-0001 cell therapy in patients with CD19+ Relapsed/refractory Malignancies. Mol Ther. (2021) 29:636–44. doi: 10.1016/j.ymthe.2020.09.027
18. Kumar S, Paiva B, Anderson KC, Durie B, Landgren O, Moreau P, et al. International Myeloma Working Group consensus criteria for response and minimal residual disease assessment in multiple myeloma. Lancet Oncol. (2016) 17:e328–46. doi: 10.1016/S1470-2045(16)30206-6
19. McLaren W, Gil L, Hunt SE, Riat HS, Ritchie GRS, Thormann A, et al. The ensembl variant effect predictor. Genome Biol. (2016) 17:122. doi: 10.1186/s13059-016-0974-4
20. Zhu GH, Zhang LP, Li ZG, Wei A, Yang Y, Tian Y, et al. Associations between PRF1 Ala91Val polymorphism and risk of hemophagocytic lymphohistiocytosis: a meta-analysis based on 1366 subjects. World J Pediatr WJP. (2020) 16:598–606. doi: 10.1007/s12519-020-00351-7
21. Henter JI. Hemophagocytic lymphohistiocytosis. N Engl J Med. (2025) 392:584–98. doi: 10.1056/NEJMra2314005
22. Lichtenstein DA, Schischlik F, Shao L, Steinberg SM, Yates B, Wang HW, et al. Characterization of HLH-like manifestations as a CRS variant in patients receiving CD22 CAR T cells. Blood. (2021) 138:2469–84. doi: 10.1182/blood.2021011898
23. Frank MJ, Baird JH, Kramer AM, Srinagesh HK, Patel S, Brown AK, et al. CD22-directed CAR T-cell therapy for large B-cell lymphomas progressing after CD19-directed CAR T-cell therapy: a dose-finding phase 1 study. Lancet. (2024) 404:353–63. doi: 10.1016/S0140-6736(24)00746-3
24. Priyadarshini S, Harris A, Treisman D, Cupac JN, Li N, Yan D, et al. Hemophagocytic lymphohistiocytosis secondary to CAR-T cells: Update from the FDA and Vizient databases. Am J Hematol. (2022) 97:E374–6. doi: 10.1002/ajh.26668
25. Ahmed S, furqan f, Strati P, Westin J, Fayad L, Hagemeister FB, et al. Haemophagocytic lymphohistiocytosis (HLH) in patients with large B-cell lymphoma treated with standard of care (SOC) axicabtagene ciloleucel (Axi-cel). J Clin Oncol. (2020) 38:8057–7. doi: 10.1200/JCO.2020.38.15_suppl.8057
26. Zhao M, Flynt FL, Hong M, Chen H, Gilbert CA, Briley NT, et al. MHC class II transactivator (CIITA) expression is up regulated in multiple myeloma cells by IFN-γ. Mol Immunol. (2007) 44:2923–32. doi: 10.1016/j.molimm.2007.01.009
27. Zhao WH, Wang BY, Chen LJ, Fu WJ, Xu J, Liu J, et al. Four-year follow-up of LCAR-B38M in relapsed or refractory multiple myeloma: a phase 1, single-arm, open-label, multicenter study in China (LEGEND-2). J Hematol OncolJ Hematol Oncol. (2022) 15:86. doi: 10.1186/s13045-022-01301-8
28. Bilston L, Croden J, Taparia M, Karkhaneh M, Grossman J, and Sun HL. Validation of the HScore and the HLH-2004 diagnostic criteria for the diagnosis of hemophagocytic lymphohistiocytosis in a multicenter cohort. Eur J Haematol. (2022) 109:129–37. doi: 10.1111/ejh.13779
29. Qureshi Z, Altaf F, Jamil A, and Siddique R. Optimization strategies in CAR T-cell therapy: A comprehensive evaluation of cytopenia, HLH/MAS, and other adverse events. Am J Clin Oncol. (2024) 47:607. doi: 10.1097/COC.0000000000001124
30. Hines MR, Keenan C, Alfaro GM, Cheng C, Zhou Y, Sharma A, et al. Hemophagocytic lymphohistiocytosis-like toxicity (carHLH) after CD19-specific CAR T-cell therapy. Br J Haematol. (2021) 194:701–7. doi: 10.1111/bjh.17662
31. Hines MR, Knight TE, McNerney KO, Leick MB, Jain T, Ahmed S, et al. Immune effector cell-associated hemophagocytic lymphohistiocytosis-like syndrome. Transplant Cell Ther. (2023) 29:438.e1–438.e16. doi: 10.1016/j.jtct.2023.03.006
32. Portuguese AJ, Liang EC, Huang JJ, Jeon Y, Dima D, Banerjee R, et al. Extramedullary disease is associated with severe toxicities following B-cell maturation antigen CAR T-cell therapy in multiple myeloma. Haematologica. (2025). doi: 10.3324/haematol.2025.287985
33. Qi Y, Li H, Qi K, Zhu F, Cheng H, Chen W, et al. Clinical outcomes and microenvironment profiling in relapsed/refractory multiple myeloma patients with extramedullary disease receiving anti-BCMA CAR T-cell-based therapy. Am J Hematol. (2024) 99:2286–95. doi: 10.1002/ajh.27469
34. Yunna C, Mengru H, Lei W, and Weidong C. Macrophage M1/M2 polarization. Eur J Pharmacol. (2020) 877:173090. doi: 10.1016/j.ejphar.2020.173090
35. Khurana A, Rosenthal AC, Mohty R, Gaddam M, Bansal R, Hathcock MA, et al. Chimeric antigen receptor T-cell therapy associated hemophagocytic lymphohistiocytosis syndrome: clinical presentation, outcomes, and management. Blood Cancer J. (2024) 14:1–6. doi: 10.1038/s41408-024-01119-2
36. Bojan A, Parvu A, Zsoldos IA, Torok T, and Farcas AD. Macrophage activation syndrome: A diagnostic challenge (Review). Exp Ther Med. (2021) 22:904. doi: 10.3892/etm.2021.10336
37. Fardet L, Galicier L, Lambotte O, Marzac C, Aumont C, Chahwan D, et al. Development and validation of the HScore, a score for the diagnosis of reactive hemophagocytic syndrome. Arthritis Rheumatol Hoboken NJ. (2014) 66:2613–20. doi: 10.1002/art.38690
38. Wohlfarth P, Agis H, Gualdoni GA, Weber J, Staudinger T, Schellongowski P, et al. Interleukin 1 receptor antagonist anakinra, intravenous immunoglobulin, and corticosteroids in the management of critically ill adult patients with hemophagocytic lymphohistiocytosis. J Intensive Care Med. (2019) 34:723–31. doi: 10.1177/0885066617711386
39. Dufranc E, Del Bello A, Belliere J, Kamar N, Faguer S, and TAIDI (Toulouse Acquired Immune Deficiency and Infection) study group. IL6-R blocking with tocilizumab in critically ill patients with hemophagocytic syndrome. Crit Care Lond Engl. (2020) 24:166. doi: 10.1186/s13054-020-02878-7
40. Wang J, Zhang R, Wu X, Li F, Yang H, Liu L, et al. Ruxolitinib-combined doxorubicin-etoposide-methylprednisolone regimen as a salvage therapy for refractory/relapsed haemophagocytic lymphohistiocytosis: a single-arm, multicentre, phase 2 trial. Br J Haematol. (2021) 193:761–8. doi: 10.1111/bjh.17331
41. Wang J, Wang Y, Wu L, Wang X, Jin Z, Gao Z, et al. Ruxolitinib for refractory/relapsed hemophagocytic lymphohistiocytosis. Haematologica. (2020) 105:e210–2. doi: 10.3324/haematol.2019.222471
Keywords: myeloma, anti-BCMA CAR T, MAS-like syndrome, IEC-HS, immunotherapy
Citation: Munárriz D, Rodríguez-Lobato LG, López-Corral L, Arnaldos-Pérez C, Cabañas V, López-Muñoz N, Oliver-Caldés A, Ponce JC, Reguera JL, Martín AÁ, Martínez-Cibrián N, Tovar N, Delgado J, Guillen E, Varea S, Rodríguez-Otero P, Urbano-Ispizua Á, Moraleda JM, Martínez-López J, Mateos M-V, De la Calle VG, González-Navarro EA and Fernández de Larrea C (2025) Macrophage activation syndrome-like in multiple myeloma patients treated with the academic CAR-T against BCMA ARI0002h. Front. Immunol. 16:1654096. doi: 10.3389/fimmu.2025.1654096
Received: 25 June 2025; Accepted: 02 October 2025;
Published: 16 October 2025.
Edited by:
Tuna Mutis, Amsterdam University Medical Center, NetherlandsReviewed by:
Wanhong Zhao, The Second Affiliated Hospital of Xi’an Jiaotong University, ChinaAnne Marijn Kramer, Amsterdam UMC - location VUMC, Netherlands
Copyright © 2025 Munárriz, Rodríguez-Lobato, López-Corral, Arnaldos-Pérez, Cabañas, López-Muñoz, Oliver-Caldés, Ponce, Reguera, Martín, Martínez-Cibrián, Tovar, Delgado, Guillen, Varea, Rodríguez-Otero, Urbano-Ispizua, Moraleda, Martínez-López, Mateos, De la Calle, González-Navarro and Fernández de Larrea. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Luis Gerardo Rodríguez-Lobato, bGdyb2RyaWd1ZXpAY2xpbmljLmNhdA==; Carlos Fernández de Larrea, Y2Zlcm5hbjFAY2xpbmljLmNhdA==
†ORCID: Daniel Munárriz, orcid.org/0009-0005-4977-8782
Luis Gerardo Rodríguez-Lobato, orcid.org/0000-0001-5694-0921
Nieves López-Muñoz, orcid.org/0000-0003-0090-6673
Núria Martínez-Cibrián, orcid.org/0000-0002-8688-1202
José María Moraleda, orcid.org/0000-0001-9080-1466
Verónica González De la Calle, orcid.org/0000-0002-5493-6707