 Erika Biegelmeyer1
Erika Biegelmeyer1 Mariana de Freitas Aguiar1
Mariana de Freitas Aguiar1 Priscila Dias Cardoso Ribeiro1
Priscila Dias Cardoso Ribeiro1 Ketty Lysie Libardi Lira Machado2Camila Maria Paiva França Telles3Sandra Lúcia Euzébio Ribeiro3Natália Sarzi Sartori4Rodrigo Poubel Vieira de Rezende5Ana Karla Guedes de Melo6
Ketty Lysie Libardi Lira Machado2Camila Maria Paiva França Telles3Sandra Lúcia Euzébio Ribeiro3Natália Sarzi Sartori4Rodrigo Poubel Vieira de Rezende5Ana Karla Guedes de Melo6 Vitor Alves Cruz7
Vitor Alves Cruz7 Rejane Maria Rodrigues de Abreu Vieira8Adriana Maria Kakehasi9Maria Cecília Dias Corrêa10
Rejane Maria Rodrigues de Abreu Vieira8Adriana Maria Kakehasi9Maria Cecília Dias Corrêa10 Valderilio Feijó Azevedo11
Valderilio Feijó Azevedo11 Olindo Assis Martins-Filho12Flávia Maria Matos Melo Campos Peixoto1Vanessa de Oliveira Magalhães1
Olindo Assis Martins-Filho12Flávia Maria Matos Melo Campos Peixoto1Vanessa de Oliveira Magalhães1 Maria da Penha Gomes Gouveia2Thaís Evelyn Karnopp4Katia Lino Baptista5Tâmara Santos Melo6Jozelia Rêgo7
Maria da Penha Gomes Gouveia2Thaís Evelyn Karnopp4Katia Lino Baptista5Tâmara Santos Melo6Jozelia Rêgo7 Adah Sophia Rodrigues Vieira8Anna Carolina Faria Moreira Gomes Tavares9Victória Dornelas Paz Carvalho10
Adah Sophia Rodrigues Vieira8Anna Carolina Faria Moreira Gomes Tavares9Victória Dornelas Paz Carvalho10 Vanessa Peruhype-Magalhães12Laiza Hombre Dias2
Vanessa Peruhype-Magalhães12Laiza Hombre Dias2 Raquel Lima de Lima3Kimberly Rossana da Silva Gonçalves4Natália Rodrigues Querido Fortes5Débora Marques Veghini2Jônatas Almeida Amorim3Raiza Casian Tuão2Karina Rosemarie Lallemand Tapia2
Raquel Lima de Lima3Kimberly Rossana da Silva Gonçalves4Natália Rodrigues Querido Fortes5Débora Marques Veghini2Jônatas Almeida Amorim3Raiza Casian Tuão2Karina Rosemarie Lallemand Tapia2 Cristiane Kayser1
Cristiane Kayser1 Charlles Heldan de Moura Castro1Maressa Barbosa Beloni Lirio2Juliana Bühring3
Charlles Heldan de Moura Castro1Maressa Barbosa Beloni Lirio2Juliana Bühring3 Ricardo Machado Xavier4
Ricardo Machado Xavier4 Andréa Teixeira-Carvalho12Viviane Angelina de Souza10
Andréa Teixeira-Carvalho12Viviane Angelina de Souza10 Odirlei André Monticielo4Gilda Aparecida Ferreira9
Odirlei André Monticielo4Gilda Aparecida Ferreira9 Marcelo de Medeiros Pinheiro1
Marcelo de Medeiros Pinheiro1 Edgard Torres dos Reis Neto1
Edgard Torres dos Reis Neto1 Emilia Inoue Sato1
Emilia Inoue Sato1 Valeria Valim2
Valeria Valim2 Gecilmara Salviato Pileggi1
Gecilmara Salviato Pileggi1 Alexandre Wagner Silva de Souza1*
Alexandre Wagner Silva de Souza1*- 1Rheumatology Division, Escola Paulista de Medicina da Universidade Federal de São Paulo (EPM-UNIFESP), São Paulo, SP, Brazil
- 2Rheumatology Division, Hospital Universitário Cassiano Antônio Moraes da Universidade Federal do Espírito Santo (HUCAM-UFES), Vitória, ES, Brazil
- 3Rheumatology Division, Faculdade de Medicina, Universidade Federal do Amazonas (FM- UFAM), Manaus, AM, Brazil
- 4Rheumatology Division, Hospital de Clínicas de Porto Alegre (HCPA), Universidade Federal do Rio Grande do Sul (UFRGS), Porto Alegre, RS, Brazil
- 5Rheumatology Division, Universidade Federal Fluminense, Niterói, RJ, Brazil
- 6Rheumatology Division, Hospital Universitário Lauro Wanderley, Universidade Federal da Paraíba (UFPB), João Pessoa, PB, Brazil
- 7Rheumatology Division, Universidade Federal de Goiás, Goiânia, GO, Brazil
- 8Rheumatology Division, Hospital Geral de Fortaleza (HGF), Universidade de Fortaleza (UNIFOR), Fortaleza, CE, Brazil
- 9Rheumatology Division, Hospital das Clínicas - Empresa Brasileira de Serviços Hospitalares (HC-EBSERH), Universidade Federal de Minas Gerais (UFMG), Belo Horizonte, MG, Brazil
- 10Rheumatology Division, Universidade Federal de Juiz de Fora, Juiz de Fora, MG, Brazil
- 11Edumed - Educação em Saúde S/S Ltda, Research Institute, Curitiba, PR, Brazil
- 12Instituto Renè Rachou, Fundação Oswaldo Cruz (FIOCRUZ-Minas), Belo Horizonte, MG, Brazil
Background/objectives: Patients with systemic vasculitis faced the risk of severe COVID-19 and high mortality during the pandemic. Although SARS-CoV-2 vaccination mitigates these outcomes, vaccine hesitancy persists, and data on immunogenicity and safety in vasculitis is still limited. This study aims to assess response to primary and booster doses of SARS-CoV-2 vaccination in systemic vasculitis.
Methods: This multicenter cohort study including systemic vasculitis included patients from SAFER study (Safety and Efficacy of COVID-19 Vaccines in Rheumatic Diseases). We evaluated serum IgG levels against the SARS-CoV-2 spike protein receptor-binding domain (IgG anti-RBD) at baseline and 28 days post-vaccination, disease activity scores, new cases of COVID-19 infections, and adverse events.
Results: Seventy-three patients with systemic vasculitis were included. Behçet’s disease (n=39), Takayasu arteritis (n=15), and antineutrophil cytoplasmic antibody-associated vasculitis (n=14) were the most common vasculitis forms. The majority of the patients had no comorbidities and were in remission. Seventy patients received one, 65 two, and 60 three vaccine doses. ChAdOx1 nCoV-19 (AstraZeneca/Oxford) (n=36) and CoronaVac (Sinovac) (n=25) were primarily the most common vaccines, while BNT162b2 (Pfizer–BioNTech) was usually the booster vaccine. ChAdOx1 nCoV-19 induced higher IgG anti-RBD than CoronaVac after two doses (p=0.002), but this difference disappeared after the booster dose. No differences in vaccine response were noted between heterologous and homologous regimens or vasculitis types. The new cases of COVID-19 (16.9%), hospitalization (1.5%), and mortality (1.5%) rates were relatively low following vaccination. Disease activity remained stable, and adverse events were mostly mild. Only one severe adverse event was observed.
Conclusion: Different SARS-CoV-2 vaccines demonstrated immunogenicity and clinical effectiveness in systemic vasculitis. The three-dose schedule was safe without increasing relapse risk.
1 Introduction
The COVID-19 pandemic led to elevated morbidity and mortality rates in vulnerable populations, particularly immunosuppressed patients with immune-mediated rheumatic diseases (IMRDs) (1, 2). Factors such as disease activity, comorbidities, and specific medications (e.g., rituximab, cyclophosphamide, and high-dose glucocorticoids) were associated with worsening prognosis (2–7). The risk of severe COVID-19 differed among IMRDs, with worse outcomes seen in those with rheumatoid arthritis (RA), systemic sclerosis (SSc), idiopathic inflammatory myopathies, and systemic vasculitis (3, 8–11).
Systemic vasculitis is a heterogeneous group of rare, systemic autoimmune diseases characterized by inflammation and/or necrosis of blood vessel walls of varying sizes (12). The prevalence and phenotypic expression of specific forms of systemic vasculitis may vary based on ethnic and geographic factors (13–16). When compared to other IMRDs, systemic vasculitis frequently requires intensive immunosuppression due to its severity (17, 18). Furthermore, factors such as the subacute onset and protean manifestations of systemic vasculitis, delayed diagnosis, and the potentially aggressive nature of systemic vasculitis can often lead to permanent damage to target organs (17, 18). These features contribute to the increased risk of severe COVID-19 in this group of diseases (11).
Vaccination against SARS-CoV-2 is the main strategy to reduce adverse outcomes associated with COVID-19 (19–23) as evidenced by a reduction in overall population mortality following its introduction Nevertheless, vaccine hesitancy persists, usually driven by safety concerns (24–28). Although, several isolated case reports describe new-onset vasculitis following COVID-19 vaccination (29–31), large pharmacovigilance and epidemiological studies have not demonstrated a causal association, suggesting that such events may be a result of coincidental temporal clustering (32–34). In addition, we still see apprehension towards possible disease flares in patients with established systemic vasculitis after vaccination (20–34).
Numerous studies have investigated the immune response to SARS-CoV-2 vaccines in IMRDs, and most data focus on the more prevalent IMRD (35–44). Nevertheless, due to the rarity of systemic vasculitides, fewer studies have assessed immunization in this specific group of diseases (45–48). Most published studies on vasculitis immunization usually examine a single subtype of vasculitis, with relatively small sample sizes, focusing mainly on safety or immunogenicity following two or three doses of homologous vaccines (45–51). Furthermore, some IMRD cohort studies have reported lower immunogenicity in patients with vasculitis, which is usually attributed to those with AAV (52).
Studies evaluating SARS-CoV-2 vaccination in Behçet’s disease (BD) stand out for having the largest sample sizes among vasculitis patients, but all of them were conducted in Turkey, an endemic area for BD (53–55). They focused mainly on immune responses after two vaccine doses, comparing CoronaVac and BNT162b2, with additional doses assessed only for safety (53–55). Antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis (AAV) is the most studied group regarding immunogenicity for SARS-CoV-2 vaccination (45–51), but most studies evaluate the vaccine response in patients under rituximab (RTX) therapy after two or three homologous doses. There is less evidence for those not receiving B-cell–depleting therapy or for those receiving heterologous schemes (45–51). In patients with giant cell arteritis (GCA), immunogenicity and safety were evaluated only up to the booster dose (56–59).
SARS-CoV-2 vaccination was less investigated in Takayasu arteritis (TAK) compared to other systemic vasculitides. Two online surveys explored the frequency of vaccination and disease relapse (28, 60). They observed higher vaccination adherence in Turkey (91%) (60), whereas coverage was lower in China (i.e., 42% received at least 2 doses) (28). Across different cohorts, vaccination was consistently well tolerated and not associated with disease flare. However, a critical knowledge gap remains. No study to date has evaluated the immunogenicity of vaccines or antibody responses in longitudinal cohorts, leaving the efficacy of SARS-CoV-2 vaccination in TAK still uncertain.SARS-CoV-2 vaccination in other forms of vasculitis, such as cryoglobulinemic vasculitis and IgA vasculitis (IgAV) in adults, were evaluated in some studies assessing immunogenicity and safety after the primary series (61–63).
Regarding safety, previous studies have shown a low frequency of relapses after two doses of vaccine in IgAV patients (63), as well as after three homologous doses in AAV and GCA (45, 64, 65). Conversely, an increased relapse rate has been reported in cryoglobulinemic and in BD after SARS-CoV-2 vaccination (54, 55, 61, 62). Although in BD most relapses were mild and predominantly mucocutaneous, severe manifestations still occurred in a few patients (55). Overall, variability across vasculitis subtypes underscores the need for more comprehensive data.
In summary, despite the growing body of evidence, key uncertainties remain. BD data are still limited to an endemic population, and most AAV studies focus on patients undergoing rituximab therapy. Furthermore, immunogenicity has not been assessed in longitudinal TAK cohorts, and the safety of additional doses of heterologous vaccine platforms remains limited for certain vasculitis subtypes. Moreover, concerns about vaccine-related relapses in clinical practice reinforce the need for studies that address both immunogenicity and safety across systemic vasculitides. Hence, this study aims to analyze the vaccine response to three doses of SARS-CoV-2 vaccines (ChAdOx1nCoV-19/Oxford–AstraZeneca, CoronaVac, and BNT162b2/Pfizer–BioNTech) in a multicenter real-life cohort of Brazilian patients with systemic vasculitis. We assessed immunogenicity, clinical effectiveness, adverse event profiles, and relapse rates. We also compared immunogenicity across vasculitis subtypes and examined the influence of csDMARDs and bDMARDs.
2 Materials and methods
2.1 Patients
This observational, multicenter, real-life, and prospective cohort study involved patients with systemic vasculitis who underwent SARS-CoV-2 vaccination between May 2021 and March 2024, across ten sites in Brazil. The study is a subset analysis of the Brazilian SAFER project (Study of Safety, Effectiveness, and Duration of Immunity after Vaccination against SARS-CoV-2 in Patients with Immune-mediated Chronic Inflammatory Diseases) (40–43). The SAFER project is supported by the Brazilian Society of Rheumatology and the Department of Science and Technology of the Ministry of Health of Brazil. Patients were eligible if they were 18 years or older, met diagnostic or classification criteria for specific forms of vasculitis (66–74) (Supplementary Table S1), were SARS-CoV-2 vaccination-naïve at enrollment, and had a minimum follow-up time of 4 weeks after receiving at least one dose of the SARS-CoV-2 vaccine. The following forms of systemic vasculitis were included in the study: BD, TAK, polyarteritis nodosa (PAN), IgAV, cryoglobulinemic vasculitis, primary angiitis of the central nervous system (PACNS), thromboangiitis obliterans, and AAV including granulomatosis with polyangiitis (GPA), and eosinophilic granulomatosis with polyangiitis (EGPA).
Exclusion criteria included pregnancy, history of severe adverse reactions to any previously administered vaccines, and secondary causes of immunosuppression such as living with HIV (i.e., CD4+ T cell count <200 cells/mm3), organ transplant, primary immunodeficiency, cancer, or history of disorders of the thymus (e.g., myasthenia gravis, thymoma, absence of the thymus or surgical removal).SARS-CoV-2 vaccination was postponed for patients who had received rituximab within the last six months, intravenous (IV) cyclophosphamide pulse therapy within the last three months, IV glucocorticoid (GC) pulse therapy, IV immunoglobulins, or underwent plasmapheresis within the previous 30 days, as well as those who received any blood product transfusions within 30 days before study inclusion. Additionally, vaccination was postponed for at least four weeks after suspicion or confirmed diagnosis of SARS-CoV-2 (i.e., via RT-PCR or rapid test), or two weeks after receiving another type of vaccine.
This study was performed according to Helsinki’s declaration and its updates. The institutional review board approved the study protocol at each site and all study participants gave written informed consent (CAAE 43479221.0.1001.5505).
2.2 Vaccines
The following SARS-CoV-2 vaccines were included in the analysis: the inactivated SARS-CoV-2 virus vaccine (CoronaVac/Sinovac/Butantan), the mRNA-based vaccine BNT162b2 (Pfizer-BioNTech), the adenoviral vector vaccines ChAdOx1 nCoV-19 (AstraZeneca/Oxford), and Ad26COV2-S (Janssen/Johnson&Johnson). This study was conducted in accordance with the protocols outlined by Brazil’s National Immunization Program, and vaccines were made available by the Brazilian public health system (75, 76). CoronaVac was administered in two doses 28 days apart; BNT162b2 in two doses 21 days apart; ChAdOx1 in two doses 12 weeks apart; and Ad26.COV2-S as a single-dose scheme. Booster doses were recommended at least four months after completion of the primary series or two months for Ad26.COV2-S.
2.3 Follow-up assessments
The study visit schedule included a baseline visit (T0) before vaccination, and three follow-up visits (i.e., T1, T2, and T3), carried out at least 28 days after the administration of each vaccine dose, totaling three doses. The T1 visit occurred after the first dose, T2 after the completion of the full vaccination schedule, and T3 after the booster dose. During each visit, we collected blood samples and assessed patients for signs and symptoms related to vasculitis using specific disease activity tools for each form of vasculitis, as well as therapeutic interventions. A diary of symptoms was provided for patients to complete for 28 days after vaccination, and active monitoring of severe adverse events was conducted at each subsequent visit. The data were recorded using the Research Electronic Data Capture (REDCap) tool.
2.4 SARS-CoV-2 serologic assays
Immunogenicity was assessed by measuring IgG antibodies against the SARS-CoV-2 spike receptor-binding domain (IgG-RBD) using a chemiluminescent microparticle immunoassay (CMIA) for qualitative and semi-quantitative detection (SARS-CoV-2 IgG-II Quant assay, Abbott Laboratories, Green Oaks, IL, USA) (77). The titers of IgG-RBD antibodies were expressed as geometric mean (GMT) and described in binding antibody units (BAU/mL). Seropositivity was defined as IgG-RBD antibody titers of 7.1 BAU/mL or higher. The increase in IgG-RBD GMT titers after each vaccine dose was compared between different doses during the follow-up and among different vaccine types. The rate of IgG-RBD titer increase after each dose was calculated.
2.5 Diagnostic confirmation of COVID-19 infection and suspected cases
Confirmed cases of COVID-19 were defined as patients testing positive for SARS-CoV-2 via reverse transcription-polymerase chain reaction (RT-PCR) or validated antigen tests. Due to limited testing accessibility in our population, suspected cases were also included to minimize data loss. Suspected cases were classified according to Brazilian Ministry of Health definition, as patients presenting characteristic COVID-19 symptoms, including fever, dry cough, and respiratory distress, in conjunction with a loss of smell or taste or a history of close contact with a confirmed COVID-19 case within the preceding two weeks.
2.6 Tools to assess disease activity
Disease activity was assessed using specific tools for each type of vasculitis. The Birmingham Vasculitis Activity Score (BVAS) v3 was used to evaluate AAV, PAN, cryoglobulinemic vasculitis, and IgAV patients. Active disease was defined as BVAS v3 ≥ 1 (78). The short form of the Brazilian version of Behçet’s Disease Current Activity Form (BR-BDCAF) was used to evaluate disease activity in BD, and a score ≥ 2 was regarded as an active disease (79). In TAK patients, disease activity was defined according to Kerr’s criteria (80).
2.7 Study endpoints
The primary endpoint of this study was the immunogenicity of SARS-CoV-2 vaccination after the booster dose, evaluated as IgG-RBD GMT titers and seropositivity four weeks following the booster dose. Secondary endpoints included seropositivity after each dose, and the comparison of vaccine responses among different SARS-CoV-2 vaccines, as well as between homologous and heterologous vaccination schemes, and among different types of vasculitis. Additionally, the influence of current therapy on the immunogenicity of SARS-CoV-2 vaccination was assessed, as well as the clinical effectiveness of SARS-CoV-2 vaccines and vaccination schemes during the follow-up period. Safety outcomes included the number of disease relapses, changes in disease activity scores after each dose, and the adverse events profile after the SARS-CoV-2 vaccination.
2.8 Statistics
The proportions between groups were compared using the chi-square test or Fisher’s exact test for categorical variables. For continuous variables, the mean and standard deviation (SD), as well as the median and interquartile range (IQR), were calculated according to the normality of the data. The interquartile range was expressed as Q1–Q3. Continuous variables were compared using the Student’s t-test or the Mann-Whitney test, respectively. For comparisons among three or more groups, one-way analysis of variance (ANOVA) or the Kruskal-Wallis test was used.
For the longitudinal analysis of IgG titers, data were normalized using base 10 logarithms, and the median increase in titers was calculated after each dose. The variation in normalized IgG titers over time was assessed using repeated measures (ANOVA). The rate of increase between doses was expressed as medians and compared using the non-parametric Wilcoxon/Mann-Whitney test, with Bonferroni correction.
To identify predictors of higher or lower anti-RBD IgG titer responses after the booster dose, univariate linear regression was used to select variables for the multivariate analysis. A p-value < 0.2 was the criterion for the inclusion of an independent variable in the backward stepwise multivariate model. If this criterion was not met, a biological model was constructed for multivariate linear regression analysis, including the main factors known to influence vaccine responses. All statistical analyses were carried out using the Stata statistical package (v.17) and R (v.4.2.0).
3 Results
3.1 Profile of the whole cohort
Seventy-three patients with systemic vasculitis were assessed at baseline, 70 patients received the first SARS-CoV-2 vaccine dose, 65 completed the primary vaccination series, and 60 patients received the booster dose (Figure 1).

Figure 1. Flow chart and follow-up reporting the number of patients investigated for Sars-Cov-2 immunogenicity at different time points in the study. (A) shows the patient inclusion flowchart; (B) illustrates the study follow-up schedule of visit intervals concerning vaccine doses. IMRD, Immune-mediated rheumatic diseases; SAFER, Study on Safety, Effectiveness, and Duration of Immunity after SARS-CoV-2 Vaccination in Patients with Chronic Immune-Mediated Inflammatory Diseases.
At baseline, the majority of patients were female, Whites and Mestizos represented the largest group. Table 1 depicts demographic parameters, and the frequency of each vasculitis form and its therapy. The three main vasculitis forms included in the study were BD, TAK, and AAV. About half of the cohort had comorbidities, with hypertension and obesity being the most common. In terms of therapy, over half of the patients were taking csDMARDs, and more than one-third were on bDMARDs, primarily TNFi or tocilizumab. Only a few were under rituximab therapy. Glucocorticoids were used by about one-third of the patients, typically in low daily doses. Approximately half of the patients had at least one comorbidity, including hypertension (31.5%), obesity (12.3%), diabetes (8.2%), heart disease (4.1%), and lung disease (1.4%). None of the patients had end-stage kidney disease. Around two-thirds of participants underwent heterologous vaccination regimens combining ChAdOx1 nCoV-19, CoronaVac, and BNT162b2, whereas homologous regimens were mainly based on ChAdOx1 nCoV-19 (Figure 2).

Table 1. Baseline features of vasculitis patients undergoing different SARS-CoV-2 vaccination schemes in the cohort.
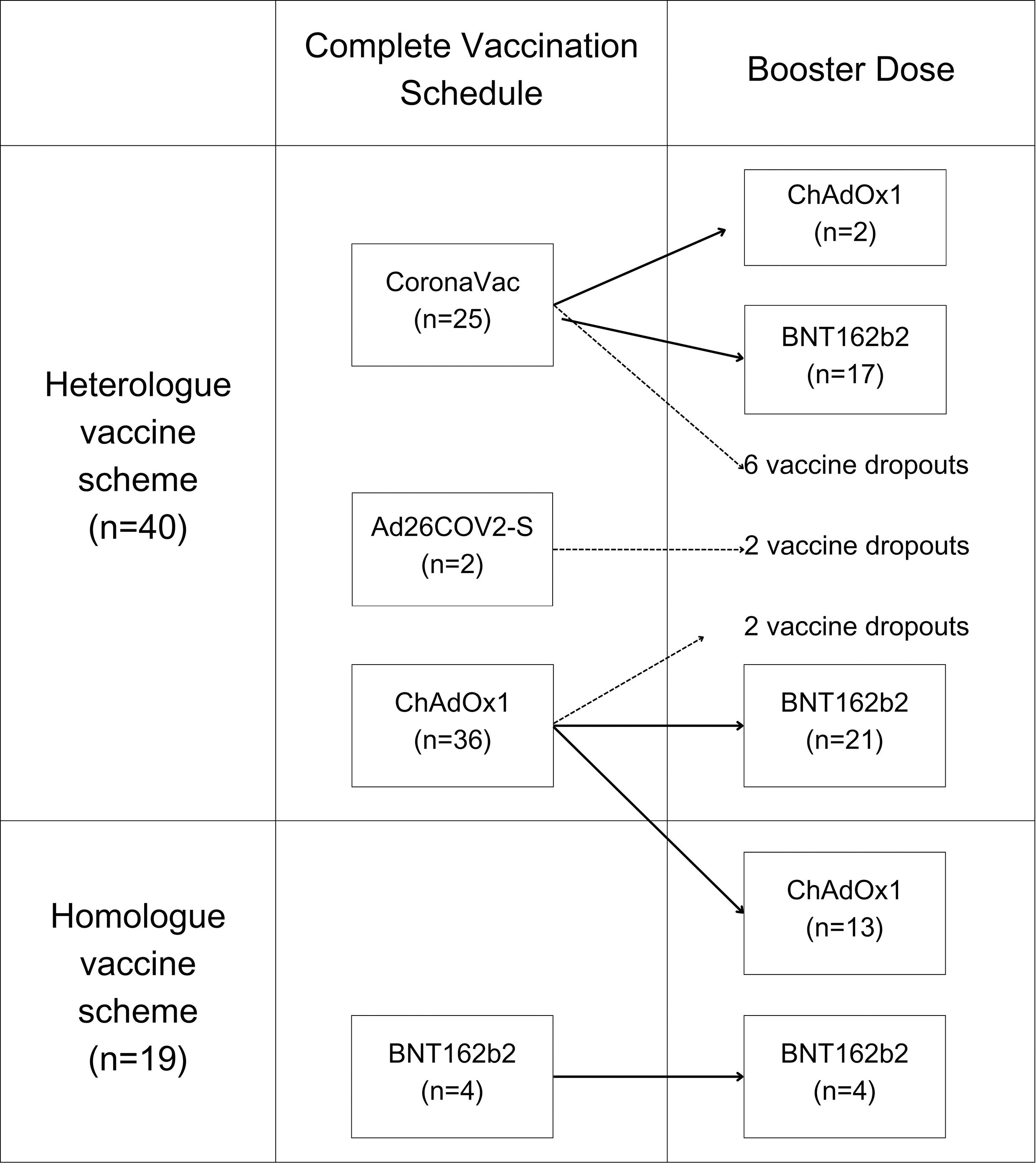
Figure 2. Vaccination distribution between homologous and heterologous vaccination schedules.
3.2 Comparison of baseline features of study participants
Vasculitis patients originally immunized by CoronaVac had a higher frequency of previous COVID-19 infection compared to those vaccinated with ChAdOx1 nCoV-19. Additionally, AAV patients were more frequently vaccinated with a heterologous regimen than with a homologous one. These differences, along with the frequency of bDMARD use (e.g., TNFi/tocilizumab in BD and TAK; rituximab in a few AAV patients), are summarized in Table 1 and Supplementary Table S1. No other significant differences regarding demographic data, comorbidities, diagnosis of vasculitis, or therapy at the baseline visit were found between the different SARS-CoV-2 vaccination schemes.
3.3 Immunogenicity to SARS-CoV-2 vaccines
At the baseline visit before SARS-CoV-2 vaccination, the CoronaVac group had higher mean levels of IgG-RBD titers (Supplementary Table S2, Figure 3A) and a higher seropositivity rate (47.8% vs. 13.9%; p=0.004) compared to the ChAdOx1 nCoV-19 group (Figure 4A, Supplementary Table S3). These findings are consistent with a higher COVID-19 pre-exposure rate in the CoronaVac group. After the primary SARS-CoV-2 vaccination series (i.e., T2 visit), the ChAdOx1 nCoV-19 group achieved significantly higher levels of immunogenicity compared to the CoronaVac group (Supplementary Table S2, Figure 3A), even though there was no significant difference regarding the seropositivity rate between the groups (94.1% vs. 90.9% respectively; p=0.13) (Figure 4A). After the booster dose (i.e., T3 visit), both groups achieved similar IgG-RBD titers, regardless of the vaccine scheme used (Supplementary Table S2).
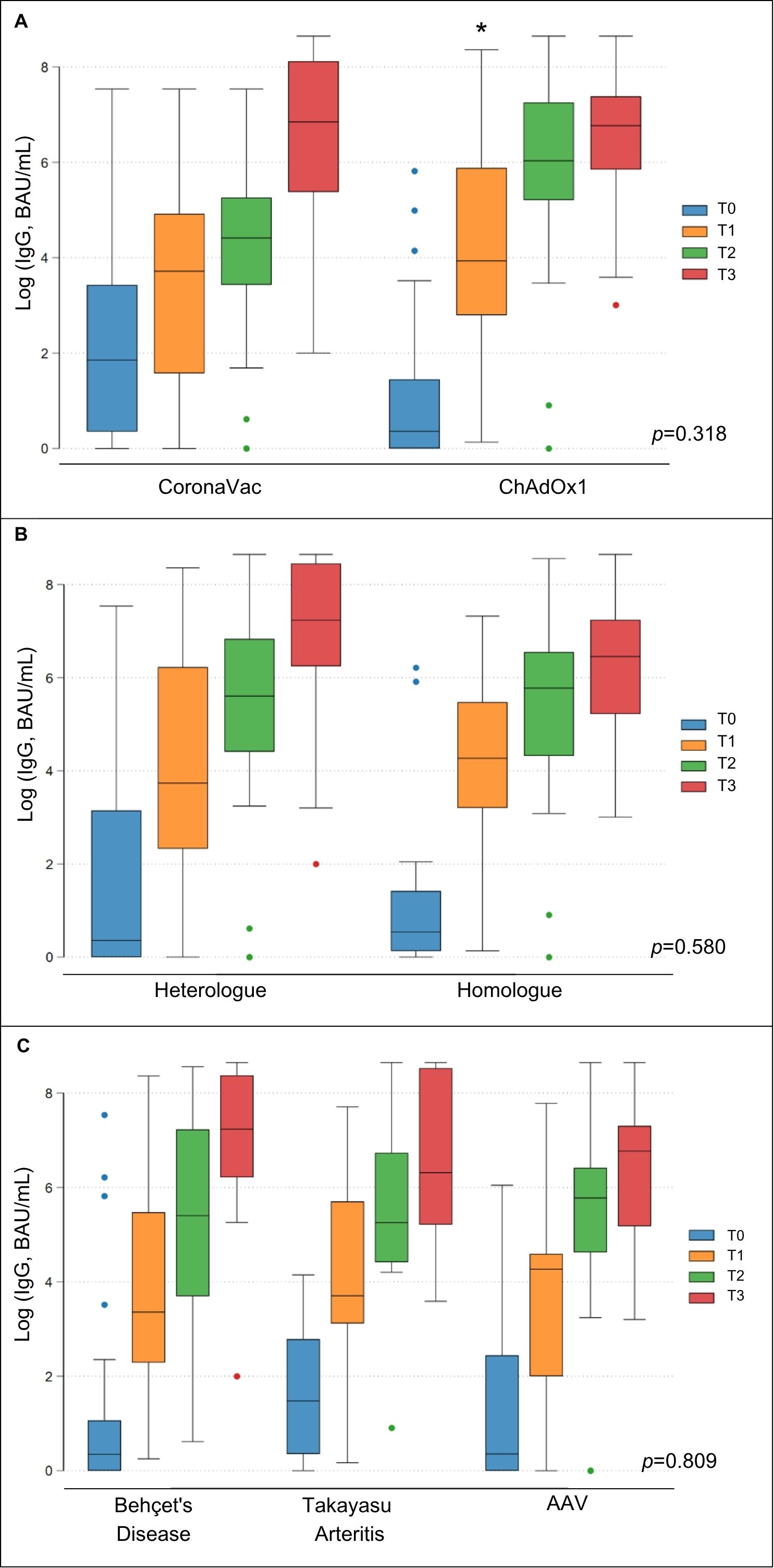
Figure 3. Immunogenicity of SARS-CoV-2 vaccination in subgroups of vasculitis patients. Boxplot graphs describe the comparison of the geometric means of IgG anti-RBD antibodies between vasculitis patients vaccinated with Coronavac or ChAdOx1 nCoV-19 (A), between those immunized with heterologous or homologous vaccine schemes (B) and between different forms of vasculitis (C). T0, baseline visit; T1, 28 days after first dose; T2, 28 days after second dose; T3, 28 days after third dose of SARS-CoV-2 vaccine; *Flags significant results.
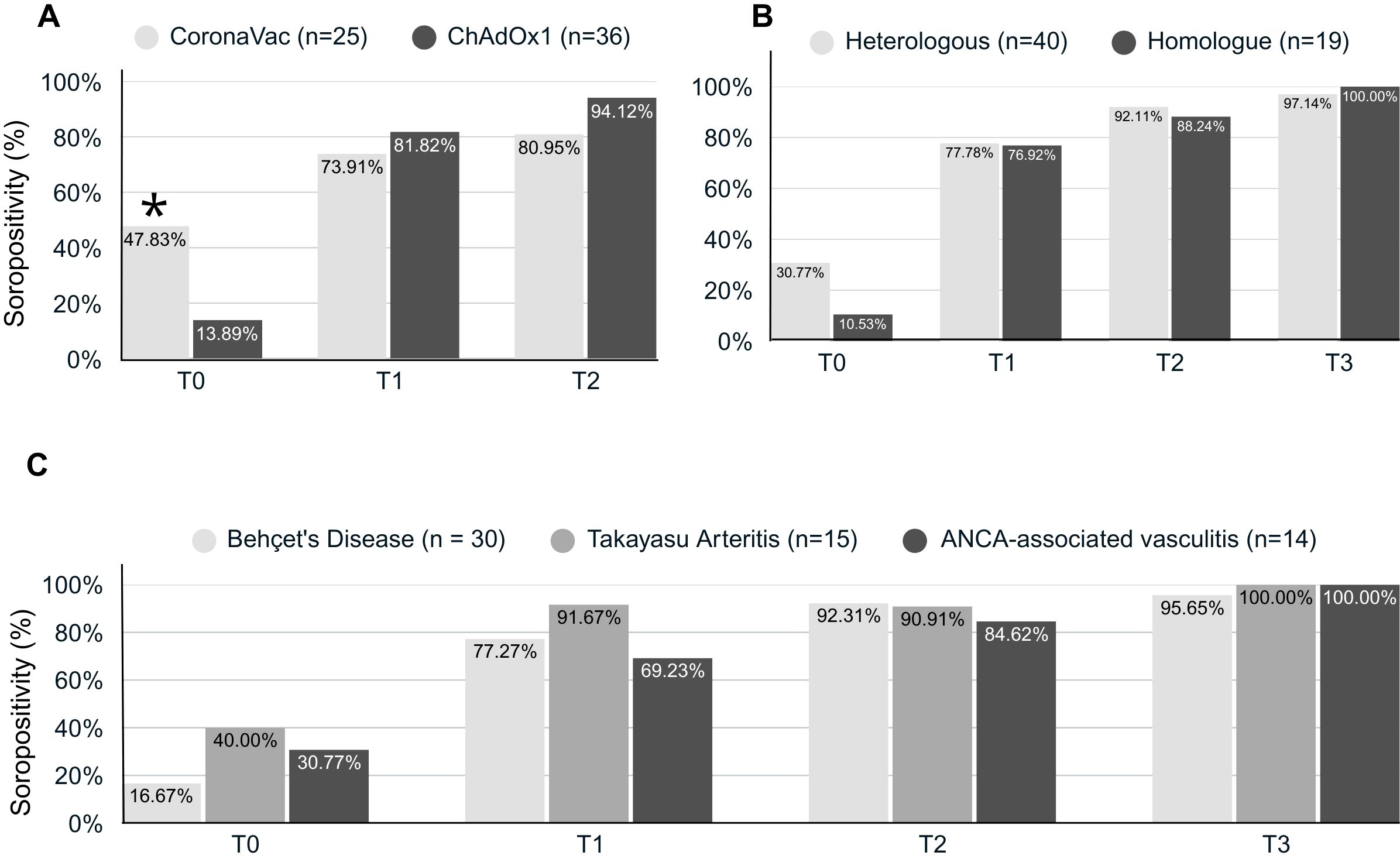
Figure 4. Seropositivity against SARS-CoV-2 in vasculitis patients. Bar charts graphs describe the comparison of the seropositivity (responder) of IgG anti-RBD antibodies between vasculitis patients vaccinated with Coronavac or ChAdOx1 nCoV-19 (A), between those immunized with heterologous or homologous vaccine schemes (B) and between different forms of vasculitis (C). T0, baseline visit; T1, 28 days after first dose; T2, 28 days after second dose; T3, 28 days after third dose of SARS-CoV-2 vaccine; *Flags significant results.
When comparing heterologous and homologous SARS-CoV-2 vaccination schemes, no significant differences were observed in the mean IgG anti-RBD titers between both schemes (p=0.580). However, the heterologous group had only a tendency for higher mean IgG anti-RBD titers (p=0.073) at the T3 visit (Supplementary Table S2, Figure 3B). The seropositivity rates were also similar between patients who underwent a homologous and heterologous SARS-CoV-2 vaccination scheme at baseline and during the follow-up (p > 0.05) (Figure 4B, Supplementary Table S3).
When patients with BD, TAK, and AAV were compared regarding levels of immunogenicity to SARS-CoV-2 vaccination, no significant differences were found in mean levels of IgG-RBD antibodies during the follow-up period (p=0.809) (Supplementary Table S2, Figures 3C, 4C, Supplementary Table S4). A significant rise in IgG-RBD antibody titers was observed within each group over time (p<0.0001).
For all groups, the IgG-RBD GMT increment rate was higher after the first dose of the SARS-CoV-2 vaccine, but this IgG-RBD GMT rise gradually declined with subsequent vaccine doses (Table 2). An exception for this was observed in the group initially allocated to vaccination with CoronaVac, as this group exhibited the lowest IgG-RBD GMT increment after the first and particularly after the second dose. Interestingly, this group showed higher GMT increments after the booster dose, typically administered with BNT162b2, catching up with IgG-RBD GMT levels comparable to levels achieved by other vaccines.
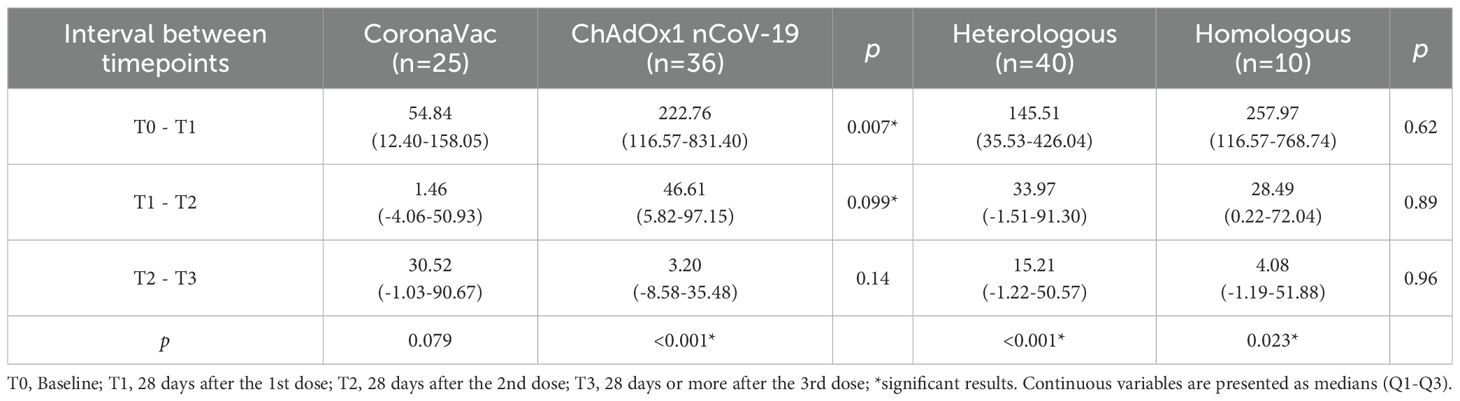
Table 2. Median of the log increment rates of anti-RBD IgG levels after each vaccine dose.
3.4 Clinical effectiveness SARS-CoV-2 vaccination in vasculitis
After the first two doses of SARS-CoV-2 vaccination, three patients (4.9%) developed either suspected or confirmed COVID-19, all of whom were in the CoronaVac group (Supplementary Table S5). Following the booster dose, ten patients (16.9%) developed COVID-19, but no significant differences were found between the different vaccine groups (Supplementary Table S6).
Only one case of severe COVID-19 that resulted in death was observed in the study. The patient was a 63-year-old and had IgAV with renal involvement characterized by nephrotic-range proteinuria, with chronic kidney disease (CKD) as a permanent damage. The patient had been treated with RTX one year prior to vaccination and had been maintained on long-term prednisone therapy between 6–10 mg/day for approximately ten years. Despite remission, disease recurred upon discontinuation of low-dose prednisone. After vaccination, the patient did not show any humoral response following the initial two doses of ChAdOx1 nCoV-19. The first reactive serology (IgG anti-RBD: 2.2 log10 BAU/mL) was detected only after the booster dose. Severe COVID-19 symptoms emerged two months after the booster, leading to ICU admission due to respiratory failure, and ultimately resulting in death. The adverse outcome was attributed to multifactorial risks, including CKD, advanced age, and vaccine anergy related to prior RTX and chronic GC therapy. Importantly, no IgAV disease activity was detected during this adverse event. In this cohort, no other severe cases of COVID-19 were reported. Thus, hospitalization and mortality rates were 1.5% each among 65 patients who received three vaccine doses.
3.5 Predictors of IgG anti-RBD antibody titers after vaccination
The univariate linear regression was first used as a screening tool to explore potential predictors of anti-RBD IgG titers after the third SARS-CoV-2 vaccine dose. Although only one variable met the conventional p-value threshold of <0.2, we decided to build a multivariate model including key variables of clinical relevance (i.e., rituximab, immunosuppressants, type of vasculitis, and vaccination scheme), regardless of their univariate statistical significance. This approach aimed to account for potential confounders while minimizing model overfitting. The analysis showed that the immune response was not significantly affected by medication use, vaccination schedule, or type of vasculitis in this study (Table 3).

Table 3. Univariate and multivariate linear regression to evaluate predictors of immunogenicity response after three doses of vaccine.
3.6 Safety of SARS-CoV-2 vaccination in vasculitis patients
The frequency of patients presenting active disease was similar at inclusion and during follow-up with successive vaccine doses (Table 4). The BVAS v3 and BR-BDCAFs scores did not change significantly before or after SARS-CoV-2 vaccination, as the frequency of patients in remission and those remaining at very low disease activity remained stable throughout the study (Table 4). No thromboembolic events were reported in BD patients after SARS-CoV-2 vaccination. However, we observed one severe adverse event related to a life-threatening disease relapse in an 80-year-old female patient with EGPA. Before receiving the booster dose, the patient had signs of mild active disease, and approximately five days after the BNT162b2 booster, the disease activity flared up with the development of myocarditis, fleeting pulmonary infiltrates, and eosinophilia. The possibility of myocarditis associated with the BNT162b2 vaccine was ruled out, as the patient did not fit the typical profile of individuals who develop this vaccine-related complication and had other features consistent with active EGPA. The patient was hospitalized and treated with intravenous methylprednisolone and cyclophosphamide pulse therapy, as well as with high-dose glucocorticoids, showing a good response to therapy. In the investigator’s opinion, immunization was likely to contribute to the vasculitis flare-up of an underlying disease activity.
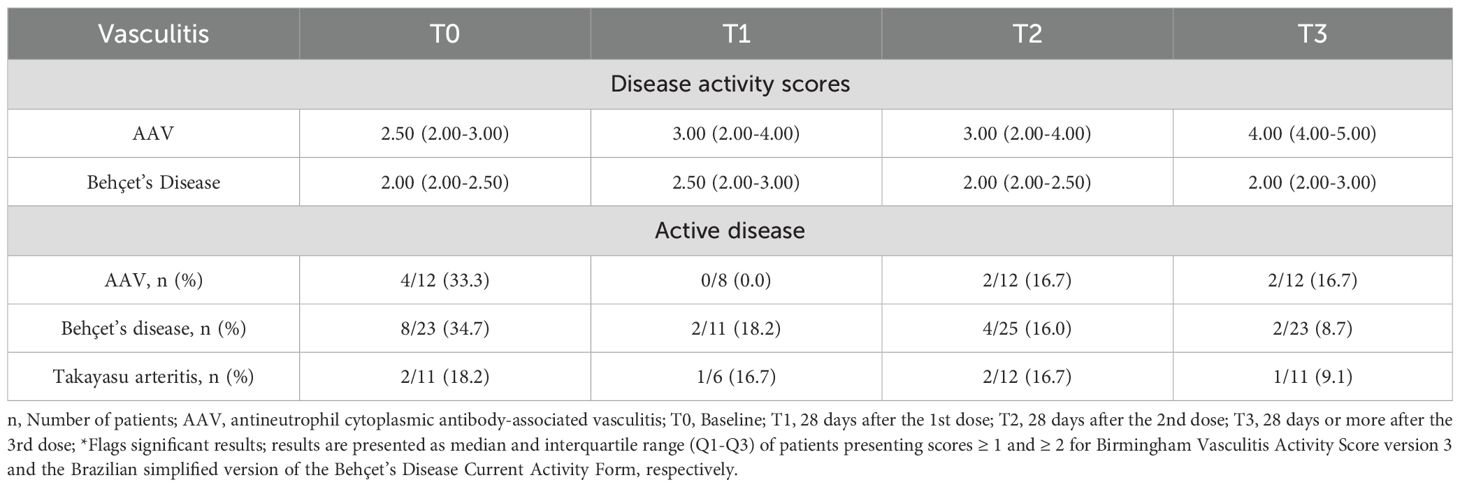
Table 4. Assessment of disease activity in ANCA-associated vasculitis and Behçet’s disease before and after each vaccine dose.
Most adverse events (AEs) related to SARS-CoV-2 vaccination were mild. Injection-site pain and skin rashes were more frequent in vasculitis patients undergoing the first ChAdOx1 nCoV-19 dose compared to CoronaVac. There were no other significant differences regarding AEs between vaccination groups, neither in the complete schedule (Table 5) nor in the booster dose scheme (Supplementary Table S7).
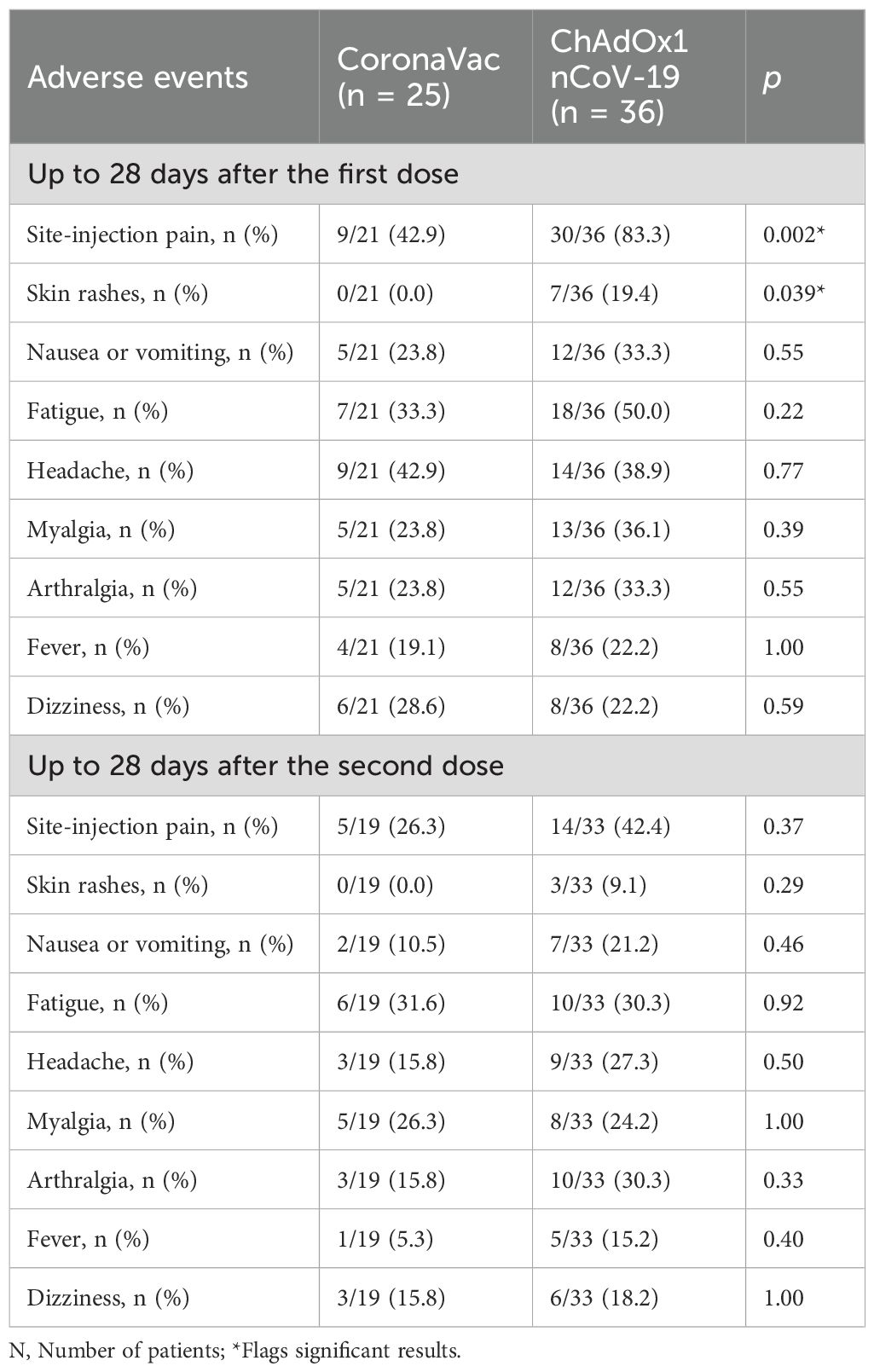
Table 5. Comparisons of safety between CoronaVac and ChAdOx1 nCoV-19 vaccines in vasculitis patients after the complete vaccination schedule.
A total of four SAEs (serious adverse events) were reported, two of which were described above (i.e., severe COVID-19 in a patient with IgAV and myocarditis due to EGPA). In addition to these events, there was one death following severe dengue infection in a patient with BD, unrelated to SARS-CoV-2 vaccination, and one case of intracranial hemorrhage due to the rupture of an intracranial aneurysm in a patient with BD on TNFi therapy, who was in remission. This severe event occurred several months after the booster dose and is unlikely to be related to SARS-CoV-2 vaccination. Only one of the severe adverse events observed in this study was directly related to the SARS-CoV-2 vaccine, that is, myocarditis due to EGPA in a patient who received the vaccination while presenting with mild active disease.
4 Discussion
In this prospective cohort study of planned vaccination, we evaluated the immune vaccine response, clinical effectiveness, and safety of SARS-CoV-2 vaccination in patients with systemic vasculitis. All vaccine schedules evaluated in this study demonstrated an increase in anti-RBD IgG titers, with the ChAdOx1 nCoV-19 vaccine showing greater immunogenicity than the CoronaVac vaccine after the complete schedule. However, this initial difference in vaccine response between ChAdOx1 nCoV-19 and CoronaVac disappeared after the booster dose, usually done with the BNT162b2 vaccine. Additionally, there were no differences in the immune response between homologous and heterologous vaccine schedules. The rate of suspected or confirmed COVID-19 cases after the booster dose was as low as 16.9%, accompanied by a low COVID-19 mortality (i.e., 1.5%). The use of immunosuppressive medications was not shown to affect the immunogenicity of SARS-CoV-2 vaccination in this population. However, we acknowledge that this study may not have sufficient statistical power to detect associations. In terms of safety, all SARS-CoV-2 vaccines demonstrated a favorable safety profile as no increase in disease relapses was observed throughout the study, and most reported adverse events were mild in intensity. However, there was one serious adverse event attributed to vaccination, occurring in a patient with active disease at the time of immunization.
The ChAdOx1 nCoV-19 vaccine induced higher mean GMT anti-RBD IgG titers and a greater increment rate than CoronaVac after the complete schedule. This finding is consistent with previous studies that identified lower immunogenicity of inactivated vaccines compared to other vaccine platforms (53, 81). However, the group vaccinated with CoronaVac had higher pre-existing viral exposure, which may have influenced the lower increment rate to vaccination observed in this group. Indeed, it is well-known that a short interval between SARS-CoV-2 infection and vaccination can result in a reduced immune response (82, 83). Despite these initial differences, seropositivity remained similar between both vaccines throughout the primary vaccination schedule.
The booster dose increased anti-RBD IgG titers in all patient groups, regardless of the initially administered vaccine platforms. It proved to be particularly important in patients with a less robust immunogenic response to the first two SARS-CoV-2 vaccine doses. A previous study including Brazilian AAV patients showed that a booster dose of CoronaVac increased antibody titers as well, indicating the benefits of the booster even with an inactivated vaccine (47). On the other hand, other studies indicate that some patients persisted unresponsive even after receiving the third dose of mRNA vaccines (45), suggesting that additional SARS-CoV-2 vaccine doses are likely needed for adequate protection in non-responders. Furthermore, the booster dose provided extra protection against mutant strains of SARS-CoV-2, such as Delta and Omicron, across various populations (45, 84).
Our population did not differ in immunogenicity between homologous and heterologous vaccine schedules. This topic has generated controversy in literature. While some studies found superiority in heterologous schedules (42, 81, 85, 86), other - including ours- did not (87), and some even favored homologous boosting (88). We believe that this variability in results of immunogenicity between homologous and heterologous vaccine schedules may be attributed to the specific characteristics of each studied population and size of the sample. It is possible that diversifying vaccine platforms does not significantly impact the immune response as long as the vaccines used are effective and administered in a schedule of at least three doses.
Our study demonstrated a low frequency of suspected or confirmed COVID-19 (16.9%) following the complete vaccination schedule and booster dose. Another study including BD patients reported 10.1% COVID-19 cases after two doses of CoronaVac and 1.4% after BNT162b2, when patients were still under social distancing measures (54). In our study, the booster dose was close to the end of social distancing measures, accompanied by modifications in population social behavior and the emergence of the Delta and Omicron SARS-CoV-2 variants. This suggests that our patients with vasculitis may have had a higher viral exposure to SARS-CoV-2 during the booster phase compared to the primary series.
We also report low hospitalization (1.5%) and mortality (1.5%) rates due to COVID-19. For comparison reasons, the hospitalization rate of COVID-19 in Latin America prior to SARS-CoV-2 vaccination was 22%, with a mortality rate of 4% (89). For individuals living with vasculitis, these rates were even higher, ranging between 23% and 38% for hospitalizations and between 9% and 28% for mortality (8–11). Other studies including IMRD patients have demonstrated similar benefits of SARS-CoV-2 vaccine effectiveness, showing a reduction in hospitalizations from 25.0% to 4.8% and mortality from 5.7% to 0% in patients with a complete vaccination schedule (41, 65, 90). These studies found that COVID-19 mortality was associated with high disease activity and the use of GC, while the number of SARS-CoV-2 vaccine doses was shown to be a protective factor. To the best of our knowledge, our study is the first to demonstrate low mortality and hospitalization rates in patients with systemic vasculitis after SARS-CoV-2 vaccination. It is worth noting that the only severe case of COVID-19 occurred in a patient who did not adequately respond to the initial SARS-CoV-2 vaccine doses, reinforcing the importance of booster doses for protection against severe COVID-19 outcomes.
Robust evidence supports that immunosuppressive therapies such as GCs, MTX ≥20 mg, MMF, and RTX are major determinants of impaired SARS-CoV-2 vaccine immunogenicity (50, 58, 91–94). In GCA, for example, patients under MTX therapy have shown reduced humoral responses after two doses of the SARS-CoV-2 vaccine, with recovery only after receiving booster doses. In contrast, patients treated with tocilizumab mounted a higher antibody response (57–59). This effect was even more pronounced when MTX was combined with moderate to high doses of GC (58). In AAV, RTX-treated patients consistently exhibited lower seropositivity rates and faster antibody waning compared to non-RTX patients, even after a booster dose (48, 49). Nevertheless, SARS-CoV-2 vaccination can still induce cellular responses in RTX users, and provide partial protection, despite B-cell depletion (48, 49). In studies including BD patients, TNFi was associated with lower serological responses after one dose of CoronaVac. However, it did not affect by mRNA vaccine immunogenicity (53).
On the other hand, in our cohort, the univariate and multivariate analyses did not show that these medications significantly affected on SARS-CoV-2 vaccine immunogenicity. We acknowledge that this discrepancy is likely due to the limited number of patients taking these medications and the timing of vaccination in relation to treatment. Only five patients were on RTX, and they were all vaccinated at least six months after their last infusion, a period when B-cell repopulation is likely to occur in most patients. Regarding GCs, most of the literature describes reduced responses after the first or second dose. However, a third dose may compensate for the initial deficit (57–59). Moreover, only a few patients were taking MMF (n=8) or high-dose MTX (n=3), which limited the possibility of analyzing these drugs individually. Therefore, these findings should not be interpreted as evidence that immunosuppressive therapy has no impact on vaccine responses. Rather, they should be understood as a consequence of the small number of patients taking these drugs in our cohort, the distribution of treatments, and the possible compensatory effect of booster doses (45, 46, 48, 49, 53, 56–59).
Additionally, this is the first study to compare the vaccine response to SARS-CoV-2 among different forms of systemic vasculitis, while other studies were restricted to include only specific forms of vasculitis (45–51) or compared the immunogenicity of vasculitis with other IMDRs (95–97). In our study, patients with AAV, TAK, and BD demonstrated equivalent vaccine responses, which contrasts with most AAV series reporting lower seroconversion rates than other diseases (45, 47, 49, 51). The seropositivity rates in our AAV patients reached 69.2%, 84.2%, and 100% after each dose of SARS-CoV-2 vaccine, whereas other studies reported 0–21% after the first dose and 28–66% after the second dose (45, 47, 49, 51). We attribute this difference to the low frequency of rituximab use in our cohort. These findings reinforce the idea that impaired humoral responses in AAV are largely driven by RTX exposure rather than by the underlying disease itself (45, 46, 48, 49).
Our study is the first to evaluate the immunogenicity against SARS-CoV-2 in patients with TAK (61). We have shown clinical effectiveness, safety, and a low rate of disease relapse in this population. In a previous study, patients with TAK were included as a whole group in a large cohort of systemic autoimmune diseases, but no analyses were made regarding their vaccine response (98). Other studies have evaluated the behavior of TAK patients during the COVID-19 pandemic, and reported flare rates of 28.5%. These flares were most often associated with unsupervised discontinuation of immunosuppressive therapy or delays in medical follow-up (60). In contrast, a Chinese study found that a SARS-CoV-2 infection itself did not increase the risk of flare, with relapse rates actually lower among infected compared with uninfected patients (28). European surveys reported that most TAK patients were in remission, and no flares were attributed to either infection or vaccination (99, 100).
Furthermore, in cohort studies including different IMDR, the vasculitis group had a reduced response compared to other diseases, usually at the expense of AAV patients using RTX (95–97). In another study that compared vasculitis patients from the SAFER study with other systemic autoimmune diseases in the same cohort, there was a trend toward a lower humoral response in patients with vasculitis, inflammatory myopathies, and systemic sclerosis, while patients with Sjögren’s disease and systemic lupus erythematosus tended to have a better response to SARS-CoV-2 vaccination (42).
Since this was a planned vaccination study, most patients were in remission at baseline, and this profile was maintained throughout the follow-up. The frequency of active disease remained stable in the follow-up visits of the study. Active disease was found in 4.6% of the whole group and in 16.0%, 8.6% and 9.0% in AAV, BD and TAK patients, respectively. Additionally, the median scores for disease activity, such as BVASv3 and BR-BDCAFs were at similar levels throughout the study, reinforcing that the vaccine did not increase disease activity scores or relapses in patients in remission or with mild disease activity.
One patient with EGPA developed a severe disease relapse with a significant temporal relation after the vaccine. In this case, the disease activity was already underway at the time of the third vaccine dose and we believe that the vaccine likely influenced the worsening of the disease. Indeed, there is a theoretical risk of autoimmune disease exacerbation after COVID-19 vaccination, although severe relapses are rare, and the benefits of vaccination outweigh these risks. In this context, the American College of Rheumatology (ACR) guidelines recommend that vaccination can be administered to patients with active disease, as long as it is not severe, whereas patients presenting life-threatening manifestations or major organ dysfunction should wait for disease control before immunization (101).
Other studies corroborate the safety of SARS-CoV-2 vaccination concerning disease relapses in systemic vasculitis, as most of them showed low disease relapse rates after vaccination. A cohort with similar features to ours, including different types of systemic vasculitis, observed a 0.9% rate of disease relapses in 107 patients (102). In patients with AAV, no increased frequency of relapses or hospitalizations were observed after SARS-CoV-2 vaccination (45, 64). Another study also found a low frequency of relapses (i.e., 0.5%) in patients with IgAV, characterized by transient renal function impairment, but with no severe adverse events (63). Disease relapses were observed in 5.3% to 12.7% of patients with cryoglobulinemic vasculitis (61, 62) and in 7.1% of patients with GCA who underwent SARS-CoV-2 vaccination (58). Regarding SARS-CoV-2 vaccination in BD, studies conducted in Turkey reported higher relapse rates in BD (i.e., 16% to 53%) compared to our findings (54, 55). Relapses were mostly mild and mucocutaneous. However, up to 4% of BD patients experienced severe relapses, including uveitis, venous thrombosis, and even neurological involvement (54). Notably, Turkey is an endemic country for BD, providing larger and more representative samples for such studies. In relation to SARS-CoV-2 vaccination in TAK, an internet-based data collection revealed results comparable to ours, showing a low rate of disease relapse (i.e., 8%) by TAK patients after vaccination (28). These data indicate that the frequency and susceptibility to relapses upon SARS-CoV-2 vaccination may vary among different types of vasculitis. However, the overall relapse rates are low and comparable to the usual disease activity rates in this population, which reinforces the safety of SARS-CoV-2 vaccination for these patients.
The profile of AEs observed in this study was predominantly mild. Injection-site pain, fatigue, and headache were the most frequent AEs, which is similar to the literature (45, 47, 54, 55, 57, 62, 102). Additionally, age appears to be a protective factor for the frequency of AEs seemed to be lower in older compared to younger patients with vasculitis (57, 102).
4.1 Limitations
We acknowledge some limitations to this study. The main limitation is the small sample size, which, combined with the heterogeneity of vasculitis subtypes and concomitant medications, may have limited the power to perform specific analyses, such as the impact of immunosuppressive therapies on vaccine response. Consequently, the study is underpowered for such analyses. However, it provides valuable real-life data that, when combined with findings from other cohorts, may help generate more consistent evidence. Another limitation was the loss of patients during follow-up, although the patient loss in our study was similar to that reported in other studies (55). Additionally, the difficulty in monitoring and confirming COVID-19 cases was challenging, as PCR testing was not performed in all suspected cases, and over time, people ceased testing. To minimize underreporting, we included unconfirmed typical COVID-19 cases (e.g., anosmia and known contact with confirmed COVID-19 cases) and we focused on severe COVID-19 presentations. Finally, the absence of a non-vasculitis control group limits direct comparisons with the general population.
4.2 Clinical implications and future directions
Despite these limitations, our study provides novel real-life data on SARS-CoV-2 vaccination in systemic vasculitis, which is a rare and clinically diverse group of diseases. We directly compared vaccine responses across vasculitis subtypes and provided longitudinal data on TAK. Clinically, the results reinforce current recommendations to complete at least three vaccine doses to achieve adequate immunogenicity, as well as to prioritize vaccination for patients in remission, with careful timing in relation to immunobiological therapies such as RTX (103). The observed reassuring safety profile may also contribute to reducing vaccine hesitancy among patients and physicians. Although limited, the study provides valuable real-life data on rare diseases. Additionally, combining our findings with results from other cohorts may generate more consistent evidence (48, 49, 53, 58, 61, 103).
5 Conclusion
To the best of our knowledge, this is the first real-life study to compare the immunogenicity, clinical efficacy, and safety of different SARS-CoV-2 vaccines in a population comprising exclusively patients with systemic vasculitis, including the first longitudinal data reported in TAK. Our study emphasizes the importance of completing a minimum of three vaccine doses to ensure adequate immunogenicity and that vaccination is safe in patients with low disease activity or in remission, with no increased risk of relapse. Hence, our results support the recommendations to prioritize vaccination for patients in remission and to time vaccinations according to the nadir of immunobiological drugs, such as RTX.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved the local ethics commettees of the instituions involved in this study and by COMISSÃO NACIONAL DE ÉTICA EM PESQUISA (CONEP). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
EB: Conceptualization, Methodology, Writing – original draft, Writing – review & editing, Data curation, Formal Analysis, Investigation. MF: Conceptualization, Data curation, Investigation, Methodology, Writing – review & editing. PD: Data curation, Investigation, Methodology, Writing – review & editing. KM: Data curation, Investigation, Methodology, Writing – review & editing. CP: Data curation, Investigation, Methodology, Writing – review & editing. SE: Data curation, Investigation, Methodology, Writing – review & editing. NS: Methodology, Software, Supervision, Writing – review & editing. RP: Data curation, Investigation, Methodology, Writing – review & editing. AG: Data curation, Investigation, Methodology, Writing – review & editing. VAC: Investigation, Methodology, Supervision, Writing – review & editing. RR: Investigation, Methodology, Supervision, Writing – review & editing. AK: Investigation, Methodology, Supervision, Writing – review & editing. MD: Investigation, Methodology, Supervision, Writing – review & editing. VFA: Data curation, Investigation, Methodology, Writing – review & editing. OM-F: Data curation, Investigation, Methodology, Writing – review & editing. FM: Data curation, Investigation, Methodology, Writing – review & editing. VO: Data curation, Investigation, Methodology, Writing – review & editing. MG: Data curation, Investigation, Methodology, Writing – review & editing. TK: Data curation, Investigation, Methodology, Writing – review & editing. KLB: Data curation, Investigation, Methodology, Writing – review & editing. TS: Data curation, Investigation, Methodology, Writing – review & editing. JR: Data curation, Investigation, Methodology, Writing – review & editing. AR: Data curation, Investigation, Methodology, Writing – review & editing. AF: Data curation, Investigation, Methodology, Writing – review & editing. VD: Data curation, Investigation, Methodology, Writing – review & editing. VP-M: Data curation, Investigation, Methodology, Writing – review & editing. LD: Data curation, Investigation, Methodology, Writing – review & editing. RL: Data curation, Investigation, Methodology, Writing – review & editing. KS: Data curation, Investigation, Methodology, Writing – review & editing. NR: Data curation, Investigation, Methodology, Writing – review & editing. DM: Data curation, Investigation, Methodology, Writing – review & editing. JA: Data curation, Investigation, Methodology, Writing – review & editing. RT: Data curation, Investigation, Methodology, Writing – review & editing. KLT: Data curation, Investigation, Methodology, Writing – review & editing. CK: Data curation, Investigation, Methodology, Writing – review & editing. CC: Data curation, Investigation, Methodology, Writing – review & editing. MB: Data curation, Investigation, Writing – review & editing. JB: Data curation, Investigation, Writing – review & editing. RX: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – review & editing. AT-C: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – review & editing. VA: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – review & editing. OM: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – review & editing. GF: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – review & editing. MP: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – review & editing. ET: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – review & editing. ES: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – review & editing. VV: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. GP: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. AS: Conceptualization, Formal Analysis, Investigation, Methodology, Supervision, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research and/or publication of this article. This study received funding from the Brazilian Society of Rheumatology (Funding number: 392 SBR2021SAFER001), Ministério da Saúde do Brasil, MS, Departamento de Ciência e Tecnologia 393 (DECIT) and Fundação para o Desenvolvimento Científico e Tecnológico em Saúde (Fiotec). The funders were not involved in the study design, collection, analysis, interpretation of data, the writing of this article, or the decision to submit it for publication.
Acknowledgments
The authors thank the Network of Observational Studies for monitoring the effectiveness, safety of vaccination against COVID-19 in Brazil, linked to the Fundação Oswaldo Cruz, Fiocruz, Instituto de Tecnologia em Imunobiológicos, Departamento de Assuntos Médicos, Estudos Clínicos e Vigilaência Pós Registro, for the technical and operational support. To the participating centers: Universidade Federal do Espírito Santo (UFES),Universidade Federal de São Paulo (UNIFESP), Universidade Federal de Minas Gerais (UFMG), Universidade Federal da Paraíba (UFPB), Universidade Federal Fluminense (UFF), Universidade Federal de Juiz de Fora (UFJF), Universidade federal de Goiás (UFG), Universidade Federal do Rio Grande do Sul (UFRGS), Hospital universitário da Universidade Federal do Amazonas (UFAM); Hospital Geral da universidade Federal do Ceará (UFCE), EDUMED research center de Curitiba Associates with Universidade Federal do Paraná (UFPR), Serviços Especializados em Reumatologia da Bahia (SER) e centros de refereência em Gastroenterologia com pesquisadores cadastrados do GEDIIB). To the collaborating researchers integrating the SAFER-study task force: AR, Adriana Maria Kakehasi, Adriana Ribas Andrade, AS, Aline Teixeira de Landa, AG, Ana Luisa Souza Pedreira, Ana Paula Neves Burian, André Gustavo Cunha Trolese, AT-C, Andrese Aline Gasparin, Andrieli Caroline Mehl, AF, Anna Carolina Simões Moulin, Antonio Luiz Boechat, Artur José Azevedo Pereira, Bárbara Oliveira Souza, Barbara Polli, Camila da Silva Cendon Duran, CP, Carolina Strauss Estevez Gadelha, Catherine Pancotto, CC, Clara Lyra de Andrade Stefanon, Clarissa Ruas Yasuda, CK, Cyrla Zaltman, Danielle Cristina Filgueira Alves Batista, Débora Cerqueira Calderaro, DM, Edgard Torres dos Reis-Neto, Eduardo Yasuda, ES, Erica Vieira Serrano, EB, Fernanda Dazilio dos Reis, Filipe Faé, FM, Flavia Zon Pretti, Gabriel Smith Sobral Vieira, Gabriela Guimarães Nogueira, GP, Gilda Aparecida Ferreira, Guilherme LevíTres, Heitor Filipe Surlo, Helena da Silva Corona, Isabella Vargas de Souza Lima, Isac Ribeiro Moulaz, João Gabriel Leão Sperancini Amaral, João Pedro Sarcinelli Chagas, JA, Jonathan Willian Da Silva Rodrigues, José Geraldo Mill, JR, Julia Fagundes Fracasso, JB, Juliana Ribeiro de Oliveira, KLT, KLB, KM, KS, Laís Pizzol Pasti, Laissa Fiorotti Albertino, LD, Laura Gonçalves Rodrigues Aguiar, Leonardo Barbosa da Silva, Leonardo Rodrigues Campos, Lucélia Paula Cabral Schmidt, Ludmila Arrebola Rubin de Celis Mori, Luigi Marangão Calil, Luiza Helena Coutinho Ribeiro, Luiza Lorenzoni Grillo, Lunara Baptista Ferreira, Maisa Brito Nunes, MP, Marcos Mavignier Sousa Dias, MB, MD, Maria da Penha Gomes Gouvea, Mariana de Oliveira Macabú, MF, Marina Deorce de Lima, Mittermayer Barreto Santiago, Nadja Maria Santiago de Mattos, NR, NS, Natália Seixas de Melo, Nicole Pamplona Bueno de Andrade, Nilzio Antonio da Silva, OM, OM-F, Paula dos Santos Athayde, Pedro Matos, Pietra Zava Lorencini, Pollyana Vitoria Thomaz da Costa, PD, Rafaela Cavalheiro do Espírito Santo, Ranielly Correêa Lube Santos Brum, RL, Rebeca Silva Moreira da Fraga, Regiane Lima, RR, Renata Henriques de Azevedo, RX, Roberta Beatriz Nazareth Alagia, Rodrigo Cutrim Gaudio, RP, Rosely Holanda da Silva Sanches, Russian Teixeira Rebello, Sabrina de Souza Ramos, Samira Tatiyama Miyamoto, SE, TS, TK, Thaisa de Moraes Ribeiro Espirito Santo, Valderilio Feijó Azevedo, Valéria Bezerra da Silva, VV, VO, Vanessa Hax, VP-M, VD, Vinícius de Pádua Sanders Medeiros, VAC, Viviane Angelina de Souza, Yasmin Gurtler Pinheiro de Oliveira. We also thank all the patients who participated in this study and the nurses for their support with patient care and sample collection.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Generative AI statement
The author(s) declare that Generative AI was used in the creation of this manuscript. For grammatical support.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2025.1655917/full#supplementary-material
References
1. Eder L, Croxford R, Drucker AM, Mendel A, Kuriya B, Touma Z, et al. COVID-19 hospitalizations, intensive care unit stays, ventilation, and death among patients with immune-mediated inflammatory diseases compared to controls. J Rheumatol. (2022) 49:523–30. doi: 10.3899/jrheum.211012
2. Kroon FPB, Najm A, Alunno A, Schoones JW, Landewé RBM, MaChado PM, et al. Risk and prognosis of SARS-CoV-2 infection and vaccination against SARS-CoV-2 in rheumatic and musculoskeletal diseases: a systematic literature review to inform EULAR recommendations. Ann Rheum Dis. (2022) 81:422–32. doi: 10.1136/annrheumdis-2021-221575
3. Santos CS, Morales CM, Álvarez ED, Castro CÁ, Robles AL, and Sandoval TP. Determinants of COVID-19 disease severity in patients with underlying rheumatic disease. Clin Rheumatol. (2020) 39:2789–96. doi: 10.1007/s10067-020-05301-2
4. Marques CDL, Kakehasi AM, Pinheiro MM, Mota LMH, Albuquerque CP, Silva CR, et al. High levels of immunosuppression are related to unfavourable outcomes in hospitalised patients with rheumatic diseases and COVID-19: First results of ReumaCoV Brasil registry. RMD Open. (2021) 7:e001461. doi: 10.1136/rmdopen-2020-001461corr1
5. Gomides APM, de Albuquerque CP, da Mota LMH, Devidé G, Dias LH, Duarte ALBP, et al. Factors associated with hospitalizations for Covid-19 in patients with rheumatoid arthritis: data from the Reumacov Brazil registry. Adv Rheumatol. (2022) 62:13. doi: 10.1186/s42358-022-00244-5
6. Ugarte-Gil MF, Alarcón GS, Izadi Z, Duarte-García A, Reátegui-Sokolova C, Clarke AE, et al. Characteristics associated with poor COVID-19 outcomes in individuals with systemic lupus erythematosus: data from the COVID-19 Global Rheumatology Alliance. Ann Rheum Dis. (2022) 81:970–8. doi: 10.1136/annrheumdis-2021-221636
7. Hoff LS, Ravichandran N, Shinjo SK, Day J, Sen P, Junior JG, et al. COVID-19 severity and vaccine breakthrough infections in idiopathic inflammatory myopathies, other systemic autoimmune and inflammatory diseases, and healthy controls: a multicenter cross-sectional study from the COVID-19 Vaccination in Autoimmune Diseases (COVAD) survey. Rheumatol Int. (2023) 43:47–58. doi: 10.1007/s00296-022-05229-7
8. Rutherford MA, Scott J, Karabayas M, Antonelou M, Gopaluni S, Gray D, et al. Risk factors for severe outcomes in patients with systemic vasculitis and COVID-19: A binational, registry-based cohort study. Arthritis Rheumatol. (2021) 73:1713–9. doi: 10.1002/art.41728
9. Samanta J, Naidu G, Deo P, Mittal S, Prasad CB, Das D, et al. Managing ANCA-associated vasculitis during COVID-19 pandemic: a single-center cross-sectional study. Rheumatol Int. (2022) 42:2159–66. doi: 10.1007/s00296-022-05177-2
10. Antovic A, Bruchfeld A, Ekland J, Lövström B, Hugelius A, Börjesson O, et al. Risks and treatment related aspects of COVID-19 infection in patients with ANCA-associated vasculitis. Scand J Rheumatol. (2023) 52:418–23. doi: 10.1080/03009742.2022.2109337
11. Sattui SE, Conway R, Putman MS, Seet AM, GianFrancesco MA, Beins K, et al. Outcomes of COVID-19 in patients with primary systemic vasculitis or polymyalgia rheumatica from the COVID-19 Global Rheumatology Alliance physician registry: a retrospective cohort study. Lancet Rheumatol. (2021) 3:e855–64.
12. Watts RA and Robson J. Introduction, epidemiology and classification of vasculitis. Best Pract Res Clin Rheumatol. (2018) 32:3–20. doi: 10.1016/j.berh.2018.10.003
13. de Souza AWS, Zarur EB, Pimentel-Quiroz VR, Sanchez-Torres A, Ugarte-Gil MF, and Sato EI. Different epidemiologic profiles of systemic vasculitis between Brazil and Peru-preliminary results in two referral centers from both countries. Clin Rheumatol. (2022) 41:635–9. doi: 10.1007/s10067-021-06032-8
14. Vieira M, Ochtrop MLG, Sztajnbok F, Souto Oliveira Elias C, Verztman JF, Bica BERG, et al. The epidemiology of takayasu arteritis in Rio de Janeiro, Brazil: A large population-based study. J Clin Rheumatol. (2023) 29:E100–3. doi: 10.1097/RHU.0000000000001964
15. Pearce FA, Craven A, Merkel PA, Luqmani RA, and Watts RA. Global ethnic and geographic differences in the clinical presentations of anti-neutrophil cytoplasm antibody-associated vasculitis. Rheumatol (Oxford). (2017) 56:1962–9. doi: 10.1093/rheumatology/kex293
16. Watts RA, Hatemi G, Burns JC, and Mohammad AJ. Global epidemiology of vasculitis. Nat Rev Rheumatol. (2022) 18:22–34. doi: 10.1038/s41584-021-00718-8
17. Garen T, Lerang K, Hoffmann-Vold AM, Andersson H, Midtvedt Ø, Brunborg C, et al. Mortality and causes of death across the systemic connective tissue diseases and the primary systemic vasculitides. Rheumatol (Oxford). (2019) 58:313–20. doi: 10.1093/rheumatology/key285
18. Phillip R and Luqmani R. Mortality in systemic vasculitis: a systematic review. Clin Exp Rheumatol. (2008) 26:S94–104.
19. Tavares ACFMG, de Melo AKG, Cruz VA, de Souza VA, de Carvalho JS, MaChado KLLL, et al. Guidelines on COVID-19 vaccination in patients with immune-mediated rheumatic diseases: a Brazilian Society of Rheumatology task force. Adv Rheumatol. (2022) 62:3. doi: 10.1186/s42358-022-00234-7
20. Yamana TK, Galanti M, Pei S, Di Fusco M, Angulo FJ, Moran MM, et al. The impact of COVID-19 vaccination in the US: Averted burden of SARS-COV-2-related cases, hospitalizations and deaths. PloS One. (2023) 18:e0275699. doi: 10.1371/journal.pone.0275699
21. Kirwan PD, Charlett A, Birrell P, Elgohari S, Hope R, Mandal S, et al. Trends in COVID-19 hospital outcomes in England before and after vaccine introduction, a cohort study. Nat Commun. (2022) 13:4834. doi: 10.1038/s41467-022-32458-y
22. Suthar AB, Wang J, Seffren V, Wiegand RE, Griffing S, and Zell E. Public health impact of covid-19 vaccines in the US: observational study. BMJ. (2022) 377:e069317. doi: 10.1136/bmj-2021-069317
23. Tu W, Zhang P, Roberts A, Allen KS, Williams J, Embi P, et al. SARS-CoV-2 infection, hospitalization, and death in vaccinated and infected individuals by age groups in Indiana, 2021–2022. Am J Public Health. (2023) 113:96–104. doi: 10.2105/AJPH.2022.307112
24. Tharwat S, Abdelsalam HA, Abdelsalam A, and Nassar MK. COVID-19 vaccination intention and vaccine hesitancy among patients with autoimmune and autoinflammatory rheumatological diseases: A survey. Int J Clin Pract. (2022) 2022:1–10. doi: 10.1155/2022/5931506
25. Chen J, Cai W, Liu T, Zhou Y, Jin Y, Yang Y, et al. The COVID-19 vaccine: Attitudes and vaccination in patients with autoimmune inflammatory rheumatic diseases. Rheumatol Autoimmun. (2022) 2:82–91. doi: 10.1002/rai2.12028
26. Vieira Rezende RP, Braz AS, Guimarães MFB, Ribeiro SLE, Abreu Vieira RMR, Bica BE, et al. Characteristics associated with COVID-19 vaccine hesitancy: A nationwide survey of 1000 patients with immune-mediated inflammatory diseases. Vaccine. (2021) 39:6454–9. doi: 10.1016/j.vaccine.2021.09.057
27. Butt IN, van Eeden C, Kovacs Burns K, Saxinger L, Clifford A, Redmond D, et al. Understanding COVID-19 vaccine hesitancy in vasculitis patients. Front Public Health. (2023) 11. doi: 10.3389/fpubh.2023.1301492
28. Kong X, Dai X, Ma L, Wang J, Sun Y, and Jiang L. COVID-19 vaccine uptake, hesitancy and clinical effects on patients with Takayasu’s arteritis: A web-based questionnaire survey from a large cohort. Front Immunol. (2023) 14. doi: 10.3389/fimmu.2023.1030810
29. Baier E, Olgemöller U, Biggemann L, Buck C, and Tampe B. Dual-positive MPO- and PR3-ANCA-associated vasculitis following SARS-CoV-2 mRNA booster vaccination: A case report and systematic review. Vaccines (Basel). (2022) 10:653.
30. Miskovic R, Radovic S, Arandjelovic S, Plavsic A, Reljic V, Peric J, et al. Onset of leukocytoclastic vasculitis following covid-19 vaccination: case based comprehensive review. Rheumatol Int. (2024) 44:2621–35. doi: 10.1007/s00296-024-05718-x
31. Sanker V, Mylavarapu M, Gupta P, Syed N, Shah M, and Dondapati VVK. Post COVID-19 vaccination medium vessel vasculitis: a systematic review of case reports. Infection. (2024) 52:1207–13. doi: 10.1007/s15010-024-02217-w
32. Mettler C, Terrier B, Treluyer JM, and Chouchana L. Risk of systemic vasculitis following mRNA COVID-19 vaccination: a pharmacovigilance study. Rheumatology. (2022) 61:e363–5. doi: 10.1093/rheumatology/keac323/6596033
33. Jarrot PA, Mirouse A, Ottaviani S, Cadiou S, Salmon JH, Liozon E, et al. Polymyalgia rheumatica and giant cell arteritis following COVID-19 vaccination: Results from a nationwide survey. Hum Vaccin Immunother. (2024) 20:2334084. doi: 10.1080/21645515.2024.2334084
34. Ramdani Y, Largeau B, Jonville-Bera AP, Maillot F, and Audemard-Verger A. COVID-19 vaccination as a trigger of IgA vasculitis: A global pharmacovigilance study. J Rheumatol. (2023) 50:564–7. doi: 10.3899/jrheum.220629
35. MaChado PM, Lawson-Tovey S, Strangfeld A, Mateus EF, Hyrich KL, Gossec L, et al. Safety of vaccination against SARS-CoV-2 in people with rheumatic and musculoskeletal diseases: results from the EULAR Coronavirus Vaccine (COVAX) physician-reported registry. Ann Rheum Dis. (2022) 81:695–709. doi: 10.1136/annrheumdis-2021-221490
36. Mageau A, Ferré VM, Goulenok T, Charpentier C, Delory N, Francois C, et al. Severely impaired humoral response against SARS-CoV-2 variants of concern following two doses of BNT162b2 vaccine in patients with systemic lupus erythematosus (SLE). Ann Rheumatic Dis. (2022) 81:1194–6. doi: 10.1136/annrheumdis-2022-222498
37. Krasselt M, Wagner U, Nguyen P, Pietsch C, Boldt A, Baerwald C, et al. Humoral and cellular response to COVID-19 vaccination in patients with autoimmune inflammatory rheumatic diseases under real-life conditions. Rheumatology. (2022) 61:SI180–8. doi: 10.1093/rheumatology/keac089
38. Tang W, Gartshteyn Y, Ricker E, Inzerillo S, Murray S, Khalili L, et al. The use of COVID-19 vaccines in patients with SLE. Curr Rheumatol Rep. (2021) 23:79. doi: 10.1007/s11926-021-01046-2
39. Sieiro Santos C, Calleja Antolin S, Moriano Morales C, Garcia Herrero J, Diez Alvarez E, Ramos Ortega F, et al. Immune responses to mRNA vaccines against SARS-CoV-2 in patients with immune-mediated inflammatory rheumatic diseases. RMD Open. (2022) 8:e001898. doi: 10.1136/lupus-2022-elm2022.188
40. Cruz VA, Guimarães C, Rêgo J, MaChado KLLL, Miyamoto ST, Burian APN, et al. Safety of CoronaVac and ChAdOx1 vaccines against SARS-CoV-2 in patients with rheumatoid arthritis: data from the Brazilian multicentric study safer. Adv Rheumatol. (2024) 64:1–8. doi: 10.1186/s42358-024-00397-5
41. Calderaro DC, Valim V, Ferreira GA, MaChado KLLL, Ribeiro PDC, Ribeiro SLE, et al. Predictors of hospitalization in breakthrough COVID-19 among fully vaccinated individuals with immune-mediated rheumatic diseases: data from SAFER-study. Vaccines. (2024) 12:1031.
42. MaChado KLLL, Burian APN, Martins-Filho OA, Mill JG, Ferreira LB, Tapia KRL, et al. Immunogenicity and safety according to immunosuppressive drugs and different COVID-19 vaccine platforms in immune-mediated disease: data from SAFER cohort. Vaccines. (2024) 12:1367.
43. Sartori NS, MaChado KLLL, Miyamoto ST, Pretti FZ, Gouveia M da PG, de Oliveira YGP, et al. Immunogenicity of SARS-CoV-2 vaccination schedules including a booster dose in patients with systemic lupus erythematosus: data from a prospective multicenter study. Vaccines (Basel). (2025) 13:127. doi: 10.3390/vaccines13020127
44. Teles C, Borges A, Magalhães A, Barra C, Silva I, Tomé P, et al. Effectiveness and immunogenicity of SARS-CoV-2 booster vaccine in immunosuppressed systemic autoimmune disease patients: A prospective study. Med Clin (Barc). (2025) 164:106920. doi: 10.1016/j.medcli.2025.106920
45. Speer C, Töllner M, Benning L, Klein K, Bartenschlager M, Nusshag C, et al. Third COVID-19 vaccine dose with BNT162b2 in patients with ANCA-associated vasculitis. Ann rheumatic Dis. (2022) 81:593–5.
46. Kant S, Azar A, and Geetha D. Antibody response to COVID-19 booster vaccine in rituximab-treated patients with anti–neutrophil cytoplasmic antibody–associated vasculitis. Kidney Int. (2022) 101:414–5. doi: 10.1016/j.kint.2021.11.012
47. Pereira RMR, Dagostin MA, Caparbo VF, Sales LP, Pasoto SG, Silva CA, et al. Anti-SARS-CoV-2 inactivated vaccine in patients with ANCA-associated vasculitis: Immunogenicity, safety, antibody decay and the booster dose. Clinics. (2023) 78:100150. doi: 10.1016/j.clinsp.2022.100150
48. Egri N, Calderón H, Martinez R, Vazquez M, Gómez-Caverzaschi V, Pascal M, et al. Cellular and humoral responses after second and third SARS-CoV-2 vaccinations in patients with autoimmune diseases treated with rituximab: specific T cell immunity remains longer and plays a protective role against SARS-CoV-2 reinfections. Front Immunol. (2023) 14. doi: 10.3389/fimmu.2023.1146841
49. Marty PK, Van Keulen VP, Erskine CL, Shah M, Hummel A, Stachowitz M, et al. Antigen specific humoral and cellular immunity following SARS-CoV-2 vaccination in ANCA-associated vasculitis patients receiving B-cell depleting therapy. Front Immunol. (2022) 13. doi: 10.3389/fimmu.2022.834981
50. Carruthers JE, Wells J, Gupta A, Kallon D, Cox A, Pina N, et al. Response to vaccination against SARS-CoV-2 in patients with antineutrophil cytoplasmic antibody-associated vasculitis with renal involvement. Front Med (Lausanne). (2022) 8. doi: 10.3389/fmed.2021.817845
51. Floyd L, Elsayed ME, Seibt T, von Bergwelt-Baildon A, Seo P, Antiochos B, et al. SARS-CoV-2 vaccine response in patients with antineutrophil cytoplasmic autoantibody-associated vasculitis. Kidney Int Rep. (2022) 7:629–32. doi: 10.1016/j.ekir.2021.12.004
52. Furer V, Eviatar T, Zisman D, Peleg H, Paran D, Levartovsky D, et al. Immunogenicity and safety of the BNT162b2 mRNA COVID-19 vaccine in adult patients with autoimmune inflammatory rheumatic diseases and in the general population: A multicentre study. Ann Rheum Dis. (2021) 80:1330–8. doi: 10.1136/annrheumdis-2021-220647
53. Ozdede A, Nohut OK, Atli Z, Tok YT, Guner S, Yilmaz E, et al. Higher antibody responses after mRNA-based vaccine compared to inactivated vaccine against SARS-CoV-2 in Behcet’s syndrome. Rheumatol Int. (2022) 42:1741–50. doi: 10.1007/s00296-022-05164-7
54. Ozdede A, Guner S, Ozcifci G, Yurttas B, Toker Dincer Z, Atli Z, et al. Safety of SARS-CoV-2 vaccination in patients with Behcet’s syndrome and familial Mediterranean fever: a cross-sectional comparative study on the effects of M-RNA based and inactivated vaccine. Rheumatol Int. (2022) 42:973–87. doi: 10.1007/s00296-022-05119-y
55. Apaydin H, Erden A, Güven SC, Armağan B, Konak HE, Polat B, et al. Effects of anti-SARS-CoV-2 vaccination on safety and disease exacerbation in patients with Behçet syndrome in a monocentric cohort. Int J Rheum Dis. (2022) 25:1068–77. doi: 10.1111/1756-185X.14387
56. Monti S, Fornara C, Delvino P, Bartoletti A, Bergami F, Comolli G, et al. Immunosuppressive treatments selectively affect the humoral and cellular response to SARS-CoV-2 in vaccinated patients with vasculitis. Rheumatol (Oxford). (2023) 62:726–34. doi: 10.1093/rheumatology/keac365
57. Delvino P, Bozzalla-Cassione E, Biglia A, Quadrelli VS, Bartoletti A, Montecucco C, et al. Safety of BNT162b2 mRNA COVID-19 vaccine in a cohort of elderly, immunocompromised patients with systemic vasculitis. Clin Exp Rheumatol. (2022) 40:853. doi: 10.55563/clinexprheumatol/xj2pqk
58. Bartoletti A, Fornara C, Delvino P, Franchi G, Ferrari A, Baldanti FP, et al. Humoral and T-cell immune response following three doses of SARS-CoV-2 mRNA vaccine in giant cell arteritis: analysis of a prospective cohort. Clin Exp Rheumatol. (2024) 42:942. doi: 10.55563/clinexprheumatol/mlatyf
59. van Sleen Y, van der Geest KSM, Buisman AM, Sandovici M, van Baarle D, and Brouwer E. Humoral SARS-CoV-2 vaccine responses in patients with giant cell arteritis and polymyalgia rheumatica: decay after primary vaccination and effects of the booster. Arthritis Care Res (Hoboken). (2024) 76:105–10. doi: 10.1002/acr.25173
60. Karakaş A, Yüce İnel T, Önen F, and Sari İ. The effect of COVID-19 pandemic in a large series of patients with Takayasu arteritis. Turk J Med Sci. (2022) 52:565–70. doi: 10.55730/1300-0144.5347
61. Visentini M, Gragnani L, Santini SA, Urraro T, Villa A, Monti M, et al. Flares of mixed cryoglobulinaemia vasculitis after vaccination against SARS-CoV-2. Ann rheumatic Dis. (2022) 81:441–3. doi: 10.1136/annrheumdis-2021-221248
62. Vacchi C, Testoni S, Visentini M, Zani R, Lauletta G, Gragnani L, et al. COVID-19 vaccination rate and safety profile in a multicentre Italian population affected by mixed cryoglobulinaemic vasculitis. Clin Exp Rheumatol. (2023) 41:787–91. doi: 10.55563/clinexprheumatol/ldv88a
63. Zan J, Ma J, Man Q, Liu X, Yu D, Zhang Y, et al. Safety evaluation of COVID-19 vaccine in patients with IgA nephropathy or IgA vasculitis nephritis. Kidney Int Rep. (2022) 7:1435–6. Available online at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8977377/.
64. Turner D, Luxton G, Yong K, and Sammel A. The impact of coronavirus-19 vaccination on anti-nuclear cytoplasmic antibody vasculitis hospitalisations in a Sydney health network. Intern Med J. (2024) 54:483–7. doi: 10.1111/imj.16343
65. Bakasis AD, Mavragani CP, Voulgari PV, Gerolymatou N, Argyropoulou OD, Vlachoyiannopoulos PG, et al. COVID-19: Clinical features and outcomes in unvaccinated 2-dose and 3-dose vaccinated against SARS-CoV-2 patients with systemic autoimmune and autoinflammatory rheumatic diseases. J Autoimmun. (2022) 131:102846. doi: 10.1016/j.jaut.2022.102846
66. Arend WP, Michel BA, Bloch DA, Hunder GG, Calabrese LH, Edworthy SM, et al. The American College of Rheumatology 1990 criteria for the classification of takayasu arteritis. Arthritis Rheum. (2010) 33:1129–34. doi: 10.1002/art.1780330811
67. International Study Group for Behçet’s Disease. Criteria for diagnosis of Behcet’s disease. Lancet. (1990) 335:1078–80.
68. Jennette JC, Falk RJ, Bacon PA, Basu N, Cid MC, Ferrario F, et al. 2012 Revised International Chapel Hill consensus conference nomenclature of vasculitides. Arthritis Rheum. (2013) 65:1–11. doi: 10.1002/art.37715
69. Watts R, Lane S, Hanslik T, Hauser T, Hellmich B, Koldingsnes W, et al. Development and validation of a consensus methodology for the classification of the ANCA-associated vasculitides and polyarteritis nodosa for epidemiological studies. Ann Rheum Dis. (2007) 66:222–7. doi: 10.1136/ard.2006.054593
70. Quartuccio L, Isola M, Corazza L, Ramos-Casals M, Retamozo S, Ragab GM, et al. Validation of the classification criteria for cryoglobulinaemic vasculitis. Rheumatology. (2014) 53:2209–13. doi: 10.1093/rheumatology/keu271
71. Mills JA, Michel BA, Bloch DA, Calabrese LH, Hunder GG, Arend WP, et al. The American College of Rheumatology 1990 criteria for the classification of henoch-schönlein purpura. Arthritis Rheum. (2010) 33:1114–21. doi: 10.1002/art.1780330809
72. Hunder GG, Bloch DA, Michel BA, Stevens MB, Arend WP, Calabrese LH, et al. The American College of Rheumatology 1990 criteria for the classification of giant cell arteritis. Arthritis Rheum. (2010) 33:1122–8. doi: 10.1002/art.1780330810
73. Shionoya S. Diagnostic criteria of Buerger’s disease. Int J Cardiol. (1998) 66 Suppl 1:S243–5. doi: 10.1016/S0167-5273(98)00175-2
74. Calabrese LH and Mallek JA. Primary angiitis of the central nervous system: Report of 8 new cases, review of the literature, and proposal for diagnostic criteria. Med (United States). (1988) 67:20–39. doi: 10.1097/00005792-198801000-00002
75. Pileggi GS, Da Mota LMH, Kakehasi AM, De Souza AW, Rocha A, de Melo AKG, et al. Brazilian recommendations on the safety and effectiveness of the yellow fever vaccination in patients with chronic immune-mediated inflammatory diseases. Adv Rheumatol. (2019) 59:17. doi: 10.1186/s42358-019-0056-x
76. Brenol CV, da Mota LMH, Cruz BA, Pileggi GS, Pereira IA, Rezende LS, et al. Consenso 2012 da Sociedade Brasileira de Reumatologia sobre vacinação em pacientes com artrite reumatoide. Rev Bras Reumatol. (2013) 53:13–23.
77. Zhao J, Yuan Q, Wang H, Liu W, Liao X, Su Y, et al. Antibody responses to SARS-CoV-2 in patients with novel coronavirus disease 2019. Clin Infect Dis. (2020) 71:2027–34. doi: 10.1093/cid/ciaa344
78. Mukhtyar C, Lee R, Brown D, Carruthers D, Dasgupta B, Dubey S, et al. Modification and validation of the Birmingham vasculitis activity score (version 3). Ann Rheum Dis. (2009) 68:1827–32. doi: 10.1136/ard.2008.101279
79. Neves F de S, Caldas CAM, de Medeiros DM, de Moraes JCB, and Gonçalves CR. Adaptação transcultural da versão simplificada (s) do Behçet’s Disease Current Activity Form (BDCAF) e compara_̧tiao do desempenho das versões Brasileiras dos dois instrumentos de avaliação da atividade da Doença de Behçet: BR-BDCAF e BR-BDCAF(s). Rev Bras Reumatol. (2009) 49:20–31. doi: 10.1590/S0482-50042009000100003
80. Kerr GS, Hallahan CW, Giordano J, Leavitt RY, Fauci AS, Rottem M, et al. Takayasu arteritis. Ann Intern Med. (1994) 120:919–29. doi: 10.7326/0003-4819-120-11-199406010-00004
81. Assawasaksakul T, Lertussavavivat T, Sathitratanacheewin S, Oudomying N, Vichaiwattana P, Wanlapakorn N, et al. Comparison of immunogenicity and safety of inactivated, adenovirus-vectored, and heterologous adenovirus-vectored/mRNA vaccines in patients with systemic lupus erythematosus and rheumatoid arthritis: A prospective cohort study. Vaccines (Basel). (2022) 10:853. doi: 10.3390/vaccines10060853
82. Herring MK, Romine JK, Wesley MG, Ellingson KD, Yoon SK, Caban-Martinez AJ, et al. Severe acute respiratory syndrome coronavirus 2 infection history and antibody response to 3 Coronavirus disease 2019 messenger RNA vaccine doses. Clin Infect Dis. (2023) 76:1822–31. doi: 10.1093/cid/ciac976
83. García-Pérez J, Bermejo M, Ramírez-García A, de la Torre-Tarazona HE, Cascajero A, Castillo de la Osa M, et al. Longer intervals between SARS-CoV-2 infection and mRNA-1273 doses improve the neutralization of different variants of concern. J Med Virol. (2023) 95:e28679. doi: 10.1002/jmv.28679
84. Frodlund M, Nived P, Chatzidionysiou K, Södergren A, Klingberg E, Hansson M, et al. The serological immunogenicity of the third and fourth doses of COVID-19 vaccine in patients with inflammatory rheumatic diseases on different biologic or targeted DMARDs: a Swedish nationwide study (COVID-19-REUMA). Microbiol Spectr. (2024) 12:e0298123. doi: 10.1128/spectrum.02981-23
85. Chu C, Schönbrunn A, Fischer D, Liu Y, Hocher JG, Weinerth J, et al. Immune response of heterologous versus homologous prime-boost regimens with adenoviral vectored and mRNA COVID-19 vaccines in immunocompromised patients. Front Immunol. (2023) 14. doi: 10.3389/fimmu.2023.1187880
86. Honfi D, Gémes N, Szabó E, Neuperger P, Balog J, Nagy LI, et al. Comparison of homologous and heterologous booster SARS-CoV-2 vaccination in autoimmune rheumatic and musculoskeletal patients. Int J Mol Sci. (2022) 23:11411. doi: 10.3390/ijms231911411
87. Nangsue C, Srisurapanont K, and Sudjaritruk T. A Comparison of the Immunogenicity and Safety of an Additional Heterologous versus Homologous COVID-19 Vaccination among Non-Seroconverted Immunocompromised Patients after a Two-Dose Primary Series of mRNA Vaccination: A Systematic Review and Meta-Analysis. Vaccines (Basel). (2024) 12:468. doi: 10.3390/vaccines12050468
88. Gallardo-Nelson MJ, Cruces M, Gómez YM, Fuenzalida C, Silva J, Aravena-Traipi L, et al. 4th booster-dose SARS-CoV-2 heterologous and homologous vaccination in rheumatological patients. Front Immunol. (2024) 15. doi: 10.3389/fimmu.2024.1427501
89. Isnardi CA, Alpizar-Rodriguez D, Calderaro DC, Marques CDL, Pons-Estel GJ, Xavier RM, et al. Factors associated with mortality in patients with immune-mediated rheumatic diseases and COVID-19 from Latin America: data from Argentina, Mexico, and Brazil. J Clin Rheumatol. (2024) 30:E9–17. doi: 10.1097/RHU.0000000000002038
90. Liew J, GianFrancesco M, Harrison C, Izadi Z, Rush S, Lawson-Tovey S, et al. SARS-CoV-2 breakthrough infections among vaccinated individuals with rheumatic disease: results from the COVID-19 Global Rheumatology Alliance provider registry. RMD Open. (2022) 8:e002187.
91. Araujo CSR, Medeiros-Ribeiro AC, Saad CGS, Bonfiglioli KR, Domiciano DS, Shimabuco AY, et al. Two-week methotrexate discontinuation in patients with rheumatoid arthritis vaccinated with inactivated SARS-CoV-2 vaccine: a randomised clinical trial. Ann Rheum Dis. (2022) 81:889–97. doi: 10.1136/annrheumdis-2021-221916
92. Medeiros-Ribeiro AC, Bonfiglioli KR, Domiciano DS, Shimabuco AY, Da Silva HC, Saad CGS, et al. Distinct impact of DMARD combination and monotherapy in immunogenicity of an inactivated SARS-CoV-2 vaccine in rheumatoid arthritis. Ann Rheum Dis. (2022) 81:710–9. doi: 10.1136/annrheumdis-2021-221735
93. De Santis M, Motta F, Isailovic N, Clementi M, Criscuolo E, Clementi N, et al. Dose-dependent impairment of the immune response to the moderna-1273 mRNA vaccine by mycophenolate mofetil in patients with rheumatic and autoimmune liver diseases. Vaccines (Basel). (2022) 10:801. doi: 10.3390/vaccines10050801
94. Kashiwado Y, Kimoto Y, Ohshima S, Sawabe T, Irino K, Nakano S, et al. Immunosuppressive therapy and humoral response to third mRNA COVID-19 vaccination with a six-month interval in rheumatic disease patients. Rheumatol (Oxford). (2024) 63:725–33. doi: 10.1093/rheumatology/kead275
95. Furer V, Eviatar T, Zisman D, Peleg H, Braun-Moscovici Y, Balbir-Gurman A, et al. Predictors of immunogenic response to the BNT162b2 mRNA COVID-19 vaccination in patients with autoimmune inflammatory rheumatic diseases treated with rituximab. Vaccines (Basel). (2022) 10:901.
96. Ferri C, Ursini F, Gragnani L, Raimondo V, Giuggioli D, Foti R, et al. Impaired immunogenicity to COVID-19 vaccines in autoimmune systemic diseases. High prevalence of non-response in different patients’ subgroups. J Autoimmun. (2021) 125:102744. doi: 10.1016/j.jaut.2021.102744
97. Jena A, Mishra S, Deepak P, Kumar-M P, Sharma A, Patel YI, et al. Response to SARS-CoV-2 vaccination in immune mediated inflammatory diseases: Systematic review and meta-analysis. Autoimmun Rev. (2022) 21:102927. doi: 10.1016/j.autrev.2021.102927
98. Braun-Moscovici Y, Kaplan M, Braun M, Markovits D, Giryes S, Toledano K, et al. Disease activity and humoral response in patients with inflammatory rheumatic diseases after two doses of the Pfizer mRNA vaccine against SARS-CoV-2. Ann Rheum Dis. (2021) 80:1317–21. doi: 10.1136/annrheumdis-2021-220503
99. Tomelleri A, Sartorelli S, Campochiaro C, Baldissera EM, and Dagna L. Impact of COVID-19 pandemic on patients with large-vessel vasculitis in Italy: a monocentric survey. Ann Rheum Dis. (2020) 79:1252–3. doi: 10.1136/annrheumdis-2020-217600
100. Comarmond C, Leclercq M, Leroux G, Marques C, Le Joncour A, Domont F, et al. Correspondence on ‘Impact of COVID-19 pandemic on patients with large-vessels vasculitis in Italy: a monocentric survey.’. Ann Rheum Dis. (2023) 82:e30–0.
101. Curtis JR, Johnson SR, Anthony DD, Arasaratnam RJ, Baden LR, Bass AR, et al. American college of rheumatology guidance for COVID-19 vaccination in patients with rheumatic and musculoskeletal diseases: version 3. Arthritis Rheumatol. (2021) 73:e60–75.
102. Simoncelli E, Conticini E, ColaFrancesco S, Gattamelata A, Spinelli FR, Garufi C, et al. Multicentre case-control study evaluating the safety of anti-SARS-CoV-2 vaccines in a cohort of patients with systemic vasculitis. Clin Exp Rheumatol. (2023) 41:922–7. doi: 10.55563/clinexprheumatol/if8nka
Keywords: vasculitis, vaccination, COVID-19, Behçet’s disease, ANCA-associated vasculitis, Takayasu arteritis, SARS-CoV-2 vaccination
Citation: Biegelmeyer E, de Freitas Aguiar M, Dias Cardoso Ribeiro P, Machado KLLL, Paiva França Telles CM, Euzébio Ribeiro SL, Sarzi Sartori N, Poubel Vieira de Rezende R, Guedes de Melo AK, Alves Cruz V, Rodrigues de Abreu Vieira RM, Kakehasi AM, Dias Corrêa MC, Azevedo VF, Martins-Filho OA, Matos Melo Campos Peixoto FM, de Oliveira Magalhães V, Gomes Gouveia MdP, Karnopp TE, Lino Baptista K, Santos Melo T, Rêgo J, Rodrigues Vieira AS, Faria Moreira Gomes Tavares AC, Dornelas Paz Carvalho V, Peruhype-Magalhães V, Dias LH, Lima de Lima R, da Silva Gonçalves KR, Rodrigues Querido Fortes N, Marques Veghini D, Amorim JA, Tuão RC, Lallemand Tapia KR, Kayser C, Castro CHdM, Barbosa Beloni Lirio M, Bühring J, Xavier RM, Teixeira-Carvalho A, Angelina de Souza V, Monticielo OA, Ferreira GA, Pinheiro MdM, Torres dos Reis Neto E, Sato EI, Valim V, Pileggi GS and de Souza AWS (2025) Immunogenicity and safety to SARS-Cov-2 vaccination in patients with systemic vasculitis. Front. Immunol. 16:1655917. doi: 10.3389/fimmu.2025.1655917
Received: 28 June 2025; Accepted: 27 October 2025;
Published: 17 November 2025.
Edited by:
Sebastian Dolff, University Duisburg-Essen, GermanyReviewed by:
Emanuele Bizzi, Vita-Salute San Raffaele University, ItalyYannick van Sleen, University Medical Center Groningen, Netherlands
Copyright © 2025 Biegelmeyer, de Freitas Aguiar, Dias Cardoso Ribeiro, Machado, Paiva França Telles, Euzébio Ribeiro, Sarzi Sartori, Poubel Vieira de Rezende, Guedes de Melo, Alves Cruz, Rodrigues de Abreu Vieira, Kakehasi, Dias Corrêa, Azevedo, Martins-Filho, Matos Melo Campos Peixoto, de Oliveira Magalhães, Gomes Gouveia, Karnopp, Lino Baptista, Santos Melo, Rêgo, Rodrigues Vieira, Faria Moreira Gomes Tavares, Dornelas Paz Carvalho, Peruhype-Magalhães, Dias, Lima de Lima, da Silva Gonçalves, Rodrigues Querido Fortes, Marques Veghini, Amorim, Tuão, Lallemand Tapia, Kayser, Castro, Barbosa Beloni Lirio, Bühring, Xavier, Teixeira-Carvalho, Angelina de Souza, Monticielo, Ferreira, Pinheiro, Torres dos Reis Neto, Sato, Valim, Pileggi and de Souza. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alexandre Wagner Silva de Souza, YWxleGFuZHJlX3dhZ25lckB1b2wuY29tLmJy