 Silvia Escribano-Serrat1,2*
Silvia Escribano-Serrat1,2* María Queralt Salas3
María Queralt Salas3 Cristina Pascual-Izquierdo4
Cristina Pascual-Izquierdo4 Manuel Fernández Villalobos4
Manuel Fernández Villalobos4 Inés Gómez-Seguí5Teresa Fidalgo6Marta Fernández Docampo7Jorge Martínez Nieto8
Inés Gómez-Seguí5Teresa Fidalgo6Marta Fernández Docampo7Jorge Martínez Nieto8 Óscar Lamas5
Óscar Lamas5 Miquel Lozano9
Miquel Lozano9 Joan Cid9Paola Charry9Marc Pino1Patricia Molina1
Joan Cid9Paola Charry9Marc Pino1Patricia Molina1 Blanca De Moner1,2,10Álex Ramos1,2
Blanca De Moner1,2,10Álex Ramos1,2 Ana Belén Moreno-Castaño1,2Julia Martinez-Sanchez1,2
Ana Belén Moreno-Castaño1,2Julia Martinez-Sanchez1,2 Ginés Escolar1,2
Ginés Escolar1,2 Maribel Díaz-Ricart1,2 on behalf of the Spanish Apheresis Group
Maribel Díaz-Ricart1,2 on behalf of the Spanish Apheresis Group- 1Laboratory of Hemostasis and Erythropathology, Hematopathology, Pathology Department, CDB, Hospital Clínic de Barcelona, Barcelona, Spain
- 2Instituto de Investigaciones Biomédicas August Pi i Sunyer (IDIBAPS), Barcelona, Spain
- 3Hematopoietic Transplantation Unit, Hospital Clínic de Barcelona, ICAMS, Barcelona, Spain
- 4Hematology Department, Hospital Universitario Gregorio Marañón, Instituto de Investigación Gregorio Marañón, Madrid, Spain
- 5Hematology Department, Hospital Universitario La Fe, Valencia, Spain
- 6Centro Hospitalar Universitário de Coimbra, Coimbra, Portugal
- 7Área de Gestión Integrada de A Coruña, Instituto de investigación Biomédica de A Coruña (INIBIC), A Coruña, Spain
- 8Hospital Clínico San Carlos, Madrid, Spain
- 9Apheresis and Cellular Therapy Unit, Department of Hemotherapy and Hemostasis, ICAMS, Hospital Clínic de Barcelona, Barcelona, Spain
- 10Josep Carreras Leukaemia Research Institute, Hospital Clínic de Barcelona, Barcelona, Spain
Introduction: Immune-mediated thrombotic thrombocytopenic purpura (iTTP) is a life-threatening thrombotic microangiopathy resulting from severe ADAMTS13 deficiency. Caplacizumab accelerates platelet recovery, but ~15% of patients remain refractory, and endothelial/microvascular injury or low ADAMTS13 activity may persist despite remission, highlighting the need for biomarkers. We evaluated the Endothelial Activation and Stress Index (EASIX), an endothelial dysfunction surrogate, dynamics and ability to predict refractoriness and mortality in iTTP.
Methods: Fifty-five adults receiving ≥2 therapies (corticosteroids, plasma exchange, rituximab, and/or caplacizumab) were studied. Clinical and laboratory data were collected at baseline, days 1–2, 7, 14, 21, 28, 35, and at treatment discontinuation, including clinical or ADAMTS13 relapses. EASIX was calculated at each time point; logistic regression and ROC analyses evaluated its predictive performance for refractoriness and mortality.
Results: Median age was 47 years; 13% were refractory, and 7% died. In responders, EASIX dropped below 1 by day 7, earlier than ADAMTS13 recovery (day 21). Clinical relapses showed EASIX spikes (median 13.2), unlike ADAMTS13-only relapses. Baseline EASIX was higher in refractory patients (752 vs. 91; p=0.007), remaining elevated at days 7 and 14. Higher pre-treatment EASIX predicted refractoriness (OR = 1.003; p=0.021; AUC = 0.811; sensitivity 100%; specificity 58.7%) and mortality (OR = 1.004; p=0.027).
Discussion: EASIX may help predict refractoriness and death, improving monitoring in iTTP.
Introduction
Thrombotic microangiopathy (TMA) is a distinct pathological entity characterized by widespread endothelial injury, leading to the formation of platelet-rich thrombi that occlude the microvascular lumen, and result in ischemia, thrombocytopenia, and microangiopathic hemolytic anemia (1, 2). Thrombotic thrombocytopenic purpura (TTP), a rare but potentially fatal TMA, has an estimated incidence of 1.5–6 cases per million adults per year and is defined by severe deficiency of ADAMTS13 (<10%), either congenital or immune-mediated (iTTP) (1–4). This deficiency leads to the accumulation of ultra-large von Willebrand factor (vWF) multimers and uncontrolled platelet aggregation, causing widespread microvascular thrombi (1, 4).
Without treatment, TTP has a mortality rate exceeding 90%. Current therapeutic strategies have reduced mortality to below 10% in specialized centers, although 10-15% of patients remain refractory to initial therapies (4, 5). Despite these advances, early recognition and prompt initiation of treatment remain critical (2, 4, 5). First-line treatment for iTTP consists of daily therapeutic plasma exchange (TPE), corticosteroids (CS) and rituximab (2, 5–7). More recently, the addition of caplacizumab, an anti-vWF antibody, has significantly improved clinical outcomes by accelerating platelet recovery and reducing the risk of disease exacerbation (2, 5, 8–12). Platelet count and lactate dehydrogenase (LDH) remain essential biomarkers for assessing disease activity and treatment response. However, the rapid normalization of platelet counts with caplacizumab highlights the need for dynamic and individualized monitoring strategies, particularly in the early stages of therapy (4, 5, 13).
The Endothelial Activation and Stress Index (EASIX), initially developed in the setting of allogeneic stem cell transplantation to predict treatment response and survivorship in patients with graft-versus-host disease, has emerged as a surrogate marker of endothelial dysfunction and a predictor of clinical outcomes and vascular complications, including transplant-associated TMA and sinusoidal obstruction syndrome. Its utility has subsequently been validated across diverse clinical contexts, such as hematologic malignancies, CAR-T cell therapy, sepsis, and COVID-19 (14–27).
Given the central role of endothelial damage in iTTP, this study aimed to determine the dynamic behavior of EASIX in patients with iTTP and explore its potential as a predictive marker of refractoriness and mortality.
Methods
Patient selection
This was an international, multicenter retrospective cohort study involving 6 institutions from Spain and Portugal (Hospital Clínic de Barcelona, Hospital Universitario Gregorio Marañón, Hospital Universitario de la Fe, Centro Hospitalar e Universitário de Coimbra, Complejo Hospitalario Universitario de A Coruña, and Hospital Clínico San Carlos). All patients ≥18 years olddiagnosed with iTTP between 2015 and 2024, defined by ADAMTS13 activity <10% with detectable anti-ADAMTS13 antibodies, who received at least two of the following treatments at onset: CS, TPE, rituximab, or caplacizumab, were included.
This study was approved by the Ethics Committee of Hospital Gregorio Marañón (COAG-PTT-2021-01) and Hospital Clinic de Barcelona (HCB/2022/0073), and was conducted in accordance with the principles outlined in the Declaration of Helsinki.
Clinical and laboratory data
Demographic and clinical data were collected retrospectively and updated in May 2025, including patients’ vital status (alive or deceased). Laboratory variables were collected at the following predefined time points: at onset (day 0), during debut follow-up (on days 1-2, 7, 14, 21, 28, and 35 after the start of targeted treatment) and on the day of discontinuation of the last targeted therapy agent. If clinical or ADAMTS13 relapse, or isolated ADAMTS13 activity decline occurred, laboratory data were also collected on the first day of the event.
Complete blood counts were assessed using automated analyzers in each center. ADAMTS13 activity was measured using fluorescence resonance energy transfer (FRETS) assay or ELISA methods, depending on the center. Following internal validation of the FRETS assay, determinations were performed in parallel in the absence and presence of a bilirubin inhibitor (bilirubin oxidase, Sigma-Aldrich, Spain), to prevent potential interference from bilirubin. Anti-ADAMTS13 antibodies were assessed using ELISA methods.
EASIX was calculated using the following formula: creatinine (mg/dL)*LDH (U/L)/platelets (x109/L). If clinical or ADAMTS13 relapses, or an isolated ADAMTS13 activity decline occurred, EASIX was also calculated on the first day of the event.
Main definitions
Targeted treatment was defined as the administration of TPE, rituximab, and/or caplacizumab. Clinical and ADAMTS13 remission, exacerbations, and clinical and ADAMTS13 relapses were defined according to the criteria established by Cuker et al. (13, 28). Isolated ADAMTS13 decline refers to a single drop in ADAMTS13 activity below 20%, not confirmed on subsequent testing and not associated with any clinical signs or symptoms. Refractoriness, as defined by Scully et al., was characterized by persistent thrombocytopenia (< 50×109/L) and persistently elevated LDH despite at least five sessions of TPE plus CE, with or without rituximab (28). For those receiving caplacizumab, refractoriness was defined by any of the following: 1) death attributable to iTTP, 2) failure to achieve clinical remission within five days, characterized by a platelet count ≥150x109/L along with normalization of LDH levels or resolution of organ damage, 3) emergence of new signs of organ injury despite ongoing treatment.
Statistical analysis
Descriptive statistics were reported as medians with interquartile ranges (IQR) for continuous variables, and as counts with percentages for categorical variables. Wilcoxon rank sum test was used to evaluate the association between continuous variables.
To assess the correlation between EASIX values and clinical outcomes, a logistic regression analysis was conducted, including EASIX as a continuous independent variable. Results are reported as odds ratios (OR) with 95% confidence intervals (CI) and corresponding p-values.
To further explore the predictive accuracy of EASIX at day 0 and day 1, receiver operating characteristic (ROC) curve analyses were performed. Additionally, to determine whether it provides prognostic information beyond its individual components, separate analyses were conducted using platelet count and LDH levels at days 0 and 1.
For mortality prediction analyses, only deaths directly attributable to iTTP were considered, in order to ensure disease-specific prognostic evaluation.
All P-values were two-tailed, and p-values <0.05 were considered statistically significant. Statistical analyses were performed using R version 4.3.2 (R Foundation for Statistical Computing, Vienna, Austria, https://www.R-project.org/) with the “gtsummary” and “pROC” packages.
Results
Clinical data
A total of 55 patients were included. Baseline characteristics are detailed in Table 1. The median age at iTTP onset was 47 years (range: 21–77), and 34 (62%) patients were females. At diagnosis, all patients presented with thrombocytopenia and 53 (96%) with anemia. The most common clinical manifestations were neurologic (56%) and gastrointestinal (23%) symptoms.

Table 1. Clinical data.
Regarding treatment, 54 patients (98%) received CS, 53 (96%) TPE, 43 (78%) rituximab, and 41 (75%) caplacizumab. The combination of CS, TPE, rituximab, and caplacizumab was the most frequently administered regimen (n=33, 60%). One patient did not receive CSdue to a prior history of CS-induced psychosis. Notably, two patients did not receive TPE as they were treated within the context of a clinical trial where TPE was not included in the treatment protocol.
Complications at debut were observed in 19 patients (35%), predominantly of infectious origin (14%). Refractoriness occurred in 7 patients (13%), of whom five had received caplacizumab. Clinical relapse was documented in 13 patients (24%) and ADAMTS13 relapse in 6 patients (11%). Four (7%) patients died.
Laboratory data and EASIX dynamics
Laboratory findings for the entire cohort are summarized in Table 2. At diagnosis, median ADAMTS13 activity was 0% (IQR 0.0–0.7), and anti-ADAMTS13 antibody levels were 63 U/mL (IQR 38-83). A progressive increase in ADAMTS13 activity was observed from day 14, surpassing 20% by day 21 (Figure 1).

Table 2. Laboratory data (n=55).

Figure 1. EASIX and ADAMTS13 activity dynamics at debut, clinical relapse, ADAMTS13 relapse, and isolated ADAMTS13 decline.
At onset, the median EASIX was 103.7 (IQR 41.1-290.9). Following treatment initiation, EASIX values declined rapidly, reaching values below 1 by day 7 (Figure 1). Similarly, creatinine, LDH, and platelets counts normalized by day 7; however, substantial inter-individual variability was observed in these parameters compared to EASIX values (Table 2 and Supplementary Figure S1).
During follow-up, clinical relapses, ADAMTS13 relapses, and isolated ADAMTS13 declines were all associated with ADAMTS13 activities below 10%. Notably, EASIX values remained consistently below one after initial recovery, except during clinical relapses, where a marked elevation was observed, with a peak median value of 13.2 (IQR 5.0-27.5).
EASIX and refractoriness
The study cohort was divided into two groups based on refractoriness to first-line treatment: non-refractory (n=48) and refractory (n=7; Figure 2). Refractory patients were slightly older (median age: 58 vs. 47 years), and included a lower proportion of females (57% vs. 63%). Four of the seven refractory patients presented neurological symptoms at diagnosis, while none exhibited gastrointestinal manifestations. Regarding treatment, 5/7 refractory patients received CS, TPE, rituximab, and caplacizumab; whereas the remaining two were treated with CS, TPE, and rituximab. At presentation, two patients developed infectious complications, one had cardiac complications, and two experienced hemorrhagic complications.

Figure 2. EASIX dynamics in non-refractory vs. refractory patients.
Median EASIX values were significantly higher in refractory patients at day 0 (91 vs. 752, p=0.007), day 7 (1 vs. 45, p<0.001), and day 14 (0.4 vs. 1.6, p=0.003). At day 1, a non-significant trend toward higher EASIX values was also observed in the refractory group (19 vs. 63, p=0.069).
Based on these findings, logistic regression models were used to evaluate the association between EASIX and refractoriness. Higher EASIX values at day 0 were significantly associated with an increased risk of refractoriness (β=0.003, SE = 0.001, p = 0.021), corresponding to an odds ratio (OR) of 1.003 (95% CI: 1.001–1.005). Similar analyses for subsequent time points revealed statistically significant associations for day 1 (OR = 1.009, 95% CI: 1.002–1.020, p = 0.041) and day 14 (OR = 45.6, 95% CI: 2.62–7765.2, p = 0.042), with a borderline result for day 7 (OR = 1.322, 95% CI: 1.042–1.860, p = 0.070).
To explore the predictive performance of early EASIX values, ROC curve analyses were conducted focusing on days 0 and 1, given their clinical relevance for early risk stratification. The area under the ROC curve (AUC) was 0.811 at day 0, with an optimal cut-off value of 129.1 yielding 100% sensitivity (SS) and 58.7% specificity (SP). At day 1, the AUC was 0.718, with a SS of 71.4% and SP of 72.1% at a cut-off value of 42.9 (Figure 3).

Figure 3. EASIX day 0 and day 1 ROC curves.
To determine whether EASIX adds prognostic value beyond its individual components, logistic regressions were also conducted for platelet count and LDH at days 0 and 1 (Supplementary Figure S2). These parameters were analyzed separately as they are commonly used for clinical monitoring, unlike creatinine. Platelet counts showed no significant association with refractoriness (day 0: OR = 0.827, 95% CI: 0.627–0.974, p=0.097; day 1: OR = 0.987, 95% CI: 0.952–1.007, p=0.355). In contrast, higher LDH levels were significantly associated with refractoriness at both time points (day 0: OR = 1.001, 95% CI: 1.000–1.001, p=0.036; day 1: OR = 1.002, 95% CI: 1.000–1.003, p=0.017).
ROC analyses confirmed moderate predictive ability of LDH alone, with AUCs of 0.714 (day 0, SS 85.7% and SP 58.7%) and 0.764 (day 1, SS 71.4% and SP 71.4%), at thresholds markedly exceeding the normal reference values (1343 U/L and 1100 U/L, respectively; Supplementary Figure S3).
EASIX and mortality
The cohort was divided based on mortality risk during the first year of diagnosis into survivors (n = 52) and non-survivors (n = 3). Among the deceased, causes of death included two cases related to refractoriness and one due to myocarditis. One patient who died after one year from diagnosis due to causes unrelated to iTTP was included in the 1-year survivors. Logistic regression analyses showed that EASIX measured at day 0 was significantly associated with mortality risk (β=0.004, SE = 0.002, p=0.027), with an OR of 1.004 (95% CI: 1.001–1.009). EASIX at day 1 showed a non-significant trend towards association with mortality (β=0.027, SE = 0.016, p=0.103; OR = 1.027, 95% CI: 1.008–1.099), Figure 4.
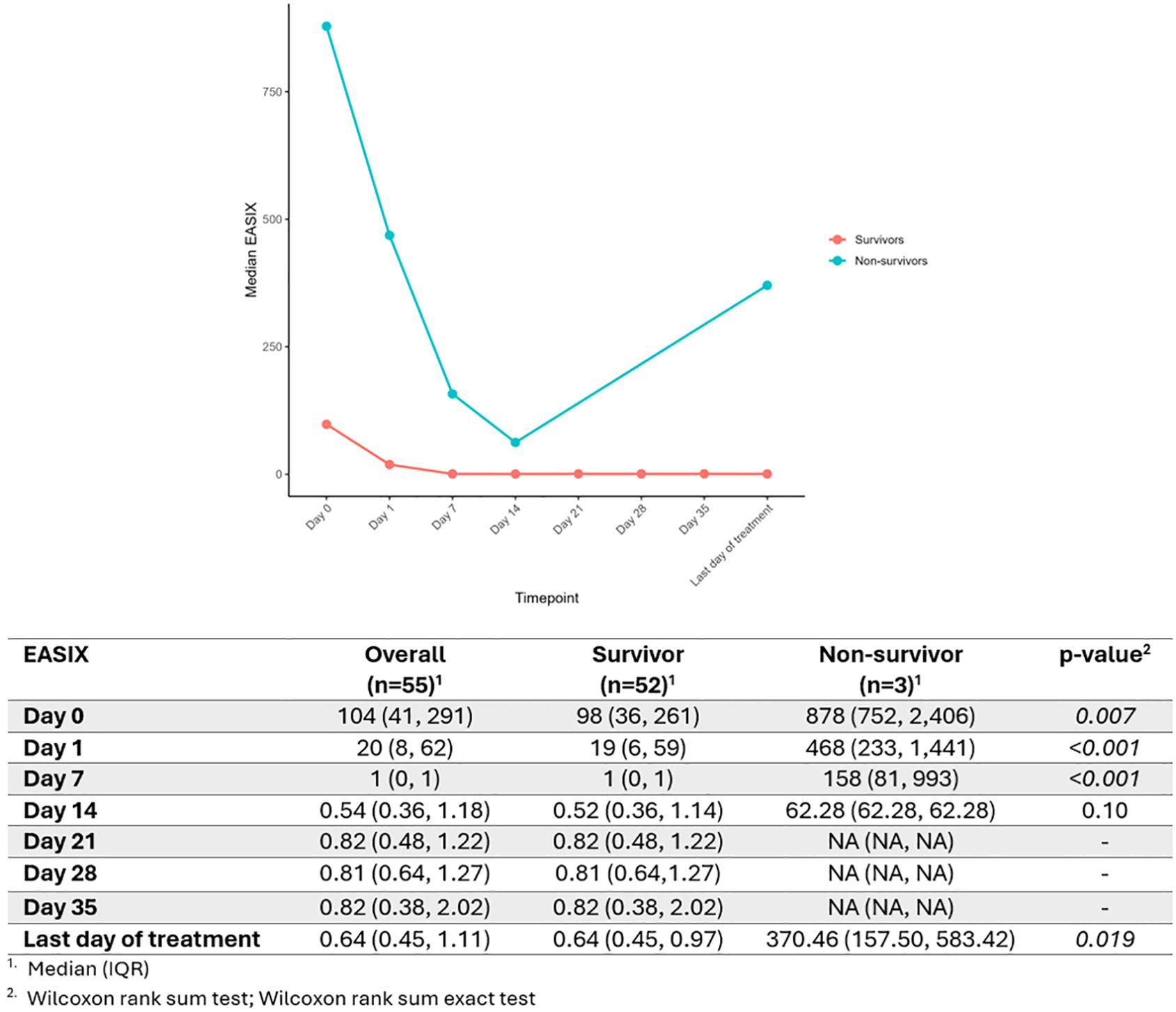
Figure 4. EASIX dynamics in survivors vs. non-survivors.
To evaluate whether the individual components of EASIX were also associated with mortality, additional logistic regression analyses were performed for platelet count and LDH at days 0 and 1. Platelet count showed no significant association with mortality (day 0: OR = 0.762, 95% CI: 0.432–0.990, p = 0.204; day 1: OR = 0.958, 95% CI: 0.842–1.007, p = 0.329). In contrast, higher LDH levels at day 0 were significantly associated with mortality risk (day 0: OR = 1.001, 95% CI: 1.000–1.002, p = 0.017; day 1: OR = 1.184, 95% CI: 0–1017, p = 0.998).
Discussion
This study offers novel insights into the clinical utility of EASIX as an indirect biomarker of endothelial activation in the context of iTTP. Our analysis describes the evolving behavior of EASIX throughout the clinical course of iTTP and demonstrates its predictive capacity for refractoriness and mortality in this setting. Its early and pronounced response to therapy, along with its sharp increase during relapses, highlights its potential role as a real-time biomarker for risk stratification and therapeutic guidance.
The introduction of caplacizumab into the iTTP treatment landscape, owing to its ability to accelerate platelet recovery, has prompted a redefinition of response criteria and patient monitoring strategies (13). In this evolving context, ADAMTS13 activity has gained attention as a key biomarker for follow-up (2, 4, 5, 13). However, complete ADAMTS13 responses are not consistently achieved, and maintained low activity levels do not invariably lead to relapse (2, 29–31). Moreover, ADAMTS13 testing remains time-consuming, and is limited to specialized laboratories.
In this context, EASIX emerges as a promising biomarker. Originally developed to predict outcomes and endothelial complications after allogeneic stem cell transplantation, it has since been validated in multiple disease settings characterized by endothelial injury, such as multiple myeloma, lymphoma, myelodysplastic syndromes, COVID-19, and in patients treated with CAR-T cell therapies (14–27). These precedents reinforce the biological plausibility of its use in iTTP, a condition in which endothelial activation and microvascular thrombosis are central pathophysiological components. In contrast to ADAMTS13, EASIX relies exclusively on standard, widely available laboratory tests, offering a fast, inexpensive, and reproducible alternative with potential for broader clinical applicability. The cost-effectiveness and operational simplicity of EASIX make it particularly suitable for settings where access to ADAMTS13 testing is limited, delayed, or where rapid clinical decisions are required.
In our study, EASIX normalization occurred at day 7, preceding the restoration of ADAMTS13 activity (day 21), and showed less inter-patient variability than LDH and platelet count, a potential misleading variable in the era of caplacizumab, suggesting it may be a more reliable marker for early treatment monitoring.
Higher baseline EASIX values were strongly associated with refractoriness. Refractory patients exhibited significantly higher EASIX values at day 0 and maintained elevated values at days 1, 7, and 14, reflecting sustained endothelial stress. EASIX outperformed LDH and platelet count in predicting refractoriness. The platelet count showed no significant association, while LDH was significant but only moderately predictive, with AUCs of 0.714 and 0.764 at days 0 and 1, respectively. However, it required abnormally high thresholds, limiting its standalone clinical utility. In contrast, EASIX, by integrating multiple clinically relevant parameters, provides a more comprehensive assessment of endothelial dysfunction and global disease severity. ROC analyses of EASIX showed excellent discriminatory power at day 0 (AUC 0.81, 100% sensitivity), suggesting its potential role in early risk stratification and guiding therapeutic escalation.
Notably, EASIX also demonstrated value in relapse monitoring. It rose markedly in clinical relapses, but remained low in ADAMTS13 relapses and isolated ADAMTS13 declines, providing a helpful distinction between clinically relevant and subclinical events. Importantly, iTTP is a chronic disease with a high risk of relapse, which requires long-term, structured follow-up. Regular assessment of ADAMTS13 activity and EASIX should be considered part of post-remission surveillance, especially during situations that may trigger clinical relapse, such as infections, pregnancy, or systemic inflammatory episodes. Incorporating EASIX into routine follow-up could enhance early detection of endothelial stress and facilitate timely therapeutic intervention.
Beyond relapse monitoring, EASIX also showed a potential association with mortality. In our cohort, higher baseline EASIX values at day 0 were significantly linked to an increased risk of death, and LDH at day 0 demonstrated a similar trend, suggesting that both may reflect severe endothelial injury and global disease burden. However, since most deaths in our series were related to refractoriness, these findings should be interpreted with caution and warrant confirmation in larger, independent studies.
Nevertheless, this study has limitations that should be recognized, including its retrospective design and small sample size. In addition, the heterogeneity observed in treatment regimens and ADAMTS13 assay methodology across centers may introduce variability among results.
In conclusion, EASIX emerges as a sensitive and accessible biomarker of endothelial injury in iTTP, outperforming traditional markers. By integrating LDH, creatinine, and platelet count over time, EASIX allows dynamic monitoring of disease activity, evaluation of treatment response, and, most importantly, early detection of clinical relapses. Moreover, its capacity to predict refractoriness, and, potentially, mortality, further underscores its value for risk stratification, and treatment guidance, including decisions on therapy intensification or early implementation of targeted approaches. Although prospective validation is warranted, these findings support the integration of EASIX into future risk-adapted therapeutic algorithms for iTTP.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Ethics statement
This study was approved by the Ethics Committee of Hospital Gregorio Marañón (COAG-PTT-2021-01) and Hospital Clinic de Barcelona (HCB/2022/0073), and was conducted in accordance with the principles outlined in the Declaration of Helsinki. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
SE-S: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. MQS: Conceptualization, Investigation, Methodology, Project administration, Supervision, Validation, Writing – review & editing. CP-I: Data curation, Writing – review & editing. MFV: Data curation, Writing – review & editing. IG-S: Data curation, Writing – review & editing. TF: Data curation, Writing – review & editing. MFD: Data curation, Writing – review & editing. JMN: Data curation, Writing – review & editing. ÓL: Data curation, Writing – review & editing. ML: Data curation, Writing – review & editing. JC: Data curation, Writing – review & editing. PC: Data curation, Writing – review & editing. MP: Data curation, Resources, Writing – review & editing. PM: Data curation, Resources, Writing – review & editing. BD: Data curation, Resources, Writing – review & editing. ÁR: Data curation, Resources, Writing – review & editing. AM-C: Data curation, Writing – review & editing. JM-S: Data curation, Writing – review & editing. GE: Funding acquisition, Investigation, Project administration, Resources, Supervision, Writing – review & editing. MD-R: Conceptualization, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research and/or publication of this article. Study partially supported by Departament de Recerca i Universitats de la Generalitat de Catalunya (2021-SGR-01118).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2025.1700907/full#supplementary-material
References
1. Tsai HM. Autoimmune thrombotic microangiopathy: advances in pathogenesis, diagnosis, and management. Semin Thromb Hemost. (2012) 38:469–82. doi: 10.1055/s-0032-1306431, PMID: 22473663
2. Sukumar S, Lämmle B, and Cataland SR. Thrombotic thrombocytopenic purpura: pathophysiology, diagnosis, and management. J Clin Med. (2021) 10:536. doi: 10.3390/jcm10030536, PMID: 33540569
3. Pascual-Izquierdo C, Del Rio-Garma J, De La Rubia J, Viejo A, Mingot E, Cid J, et al. Incidence, diagnosis, and outcome of immune-mediated thrombotic thrombocytopenic purpura: A nationwide survey by the Spanish registry of thrombotic thrombocytopenic purpura. J Clin Apheresis. (2021) 36:563–73. doi: 10.1002/jca.21894, PMID: 33780553
4. Selvakumar S, Liu A, and Chaturvedi S. Immune thrombotic thrombocytopenic purpura: Spotlight on long-term outcomes and survivorship. Front Med. (2023) 10:1137019. doi: 10.3389/fmed.2023.1137019, PMID: 36926315
5. Mingot Castellano ME, Pascual Izquierdo C, González A, Viejo Llorente A, Valcarcel Ferreiras D, Sebastián E, et al. Recomendaciones para el abordaje clínico de pacientes con púrpura trombocitopénica trombótica. Med Clínica. (2022) 158:630.e1–630.e14. doi: 10.1016/j.medcli.2021.03.040, PMID: 34266669
6. Cataland SR, Coppo P, Scully M, and Lämmle B. Thrombotic thrombocytopenic purpura: 100 years of research on Moschcowitz syndrome. Blood. (2024) 144:1143–52. doi: 10.1182/blood.2023022277, PMID: 38958481
7. Zheng XL, Vesely SK, Cataland SR, Coppo P, Geldziler B, Iorio A, et al. ISTH guidelines for treatment of thrombotic thrombocytopenic purpura. J Thromb Haemost JTH. (2020) 18:2496–502. doi: 10.1111/jth.15010, PMID: 32914526
8. Coppo P, Bubenheim M, Azoulay E, Galicier L, Malot S, Bigé N, et al. A regimen with caplacizumab, immunosuppression, and plasma exchange prevents unfavorable outcomes in immune-mediated TTP. Blood. (2021) 137:733–42. doi: 10.1182/blood.2020008021, PMID: 33150928
9. Scully M, Howells L, and Lester WA. Impact of new medications on the treatment of immune TTP. Blood. (2025) 145:1353–7. doi: 10.1182/blood.2024026390, PMID: 39912777
10. Mingot-Castellano ME, Izquierdo CP, and Del Rio Garma J. Spanish registry of thrombotic thrombocytopenic purpura (REPTT): Data evidence and new developments. Transfus Apher Sci. (2023) 62:103725. doi: 10.1016/j.transci.2023.103725, PMID: 37202322
11. Scully M, Cataland SR, Peyvandi F, Coppo P, Knöbl P, Kremer Hovinga JA, et al. Caplacizumab treatment for acquired thrombotic thrombocytopenic purpura. N Engl J Med. (2019) 380:335–46. doi: 10.1056/NEJMoa1806311, PMID: 30625070
12. Peyvandi F, Cataland S, Scully M, Coppo P, Knoebl P, Kremer Hovinga JA, et al. Caplacizumab prevents refractoriness and mortality in acquired thrombotic thrombocytopenic purpura: integrated analysis. Blood Adv. (2021) 5:2137–41. doi: 10.1182/bloodadvances.2020001834, PMID: 33881463
13. Cuker A, Cataland SR, Coppo P, De La Rubia J, Friedman KD, George JN, et al. Redefining outcomes in immune TTP: an international working group consensus report. Blood. (2021) 137:1855–61. doi: 10.1182/blood.2020009150, PMID: 33529333
14. Luft T, Benner A, Jodele S, Dandoy CE, Storb R, Gooley T, et al. EASIX in patients with acute graft-versus-host disease: a retrospective cohort analysis. Lancet Haematol. (2017) 4:e414–23. doi: 10.1016/S2352-3026(17)30108-4, PMID: 28733186
15. Luft T, Benner A, Terzer T, Jodele S, Dandoy CE, Storb R, et al. EASIX and mortality after allogeneic stem cell transplantation. Bone Marrow Transplant. (2020) 55:553–61. doi: 10.1038/s41409-019-0703-1, PMID: 31558788
16. Escribano Serrat S, Charry P, Rodríguez-Lobato LG, Moreno-Castaño AB, Suárez-Lledó M, Martínez-Cibrian N, et al. Easix application in adults undergoing allogeneic hematopoietic cell transplantation with post-transplant cyclophosphamide-based prophylaxis. Blood. (2022) 140:7616–8. doi: 10.1182/blood-2022-167051
17. Greenbaum U, Strati P, Saliba RM, Torres J, Rondon G, Nieto Y, et al. CRP and ferritin in addition to the EASIX score predict CAR-T–related toxicity. Blood Adv. (2021) 5:2799–806. doi: 10.1182/bloodadvances.2021004575, PMID: 34264268
18. Kalicińska E, Biernat M, Rybka J, Zińczuk A, Janocha-Litwin J, Rosiek-Biegus M, et al. Endothelial activation and stress index (EASIX) as an early predictor for mortality and overall survival in hematological and non-hematological patients with COVID-19: multicenter cohort study. J Clin Med. (2021) 10:4373. doi: 10.3390/jcm10194373, PMID: 34640390
19. Pedraza A, Salas MQ, Rodríguez-Lobato LG, Escribano-Serrat S, Suárez-Lledo M, Martínez-Cebrian N, et al. Easix score correlates with endothelial dysfunction biomarkers and predicts risk of acute graft-versus-host disease after allogeneic transplantation. Transplant Cell Ther. (2024) 30:187.e1–187.e12. doi: 10.1016/j.jtct.2023.11.016, PMID: 38000709
20. Pennisi M, Sanchez-Escamilla M, Flynn JR, Shouval R, Alarcon Tomas A, Silverberg ML, et al. Modified EASIX predicts severe cytokine release syndrome and neurotoxicity after chimeric antigen receptor T cells. Blood Adv. (2021) 5:3397–406. doi: 10.1182/bloodadvances.2020003885, PMID: 34432870
21. Peña M, Salas MQ, Mussetti A, Moreno-Gonzalez G, Bosch A, Patiño B, et al. Pretransplantation EASIX predicts intensive care unit admission in allogeneic hematopoietic cell transplantation. Blood Adv. (2021) 5:3418–26. doi: 10.1182/bloodadvances.2021004812, PMID: 34495311
22. Dai H, Penack O, Radujkovic A, Schult D, Majer-Lauterbach J, Blau IW, et al. Early bilirubinemia after allogeneic stem cell transplantation—an endothelial complication. Bone Marrow Transplant. (2021) 56:1573–83. doi: 10.1038/s41409-020-01186-6, PMID: 33517355
23. Jiang S, Penack O, Terzer T, Schult D, Majer-Lauterbach J, Radujkovic A, et al. Predicting sinusoidal obstruction syndrome after allogeneic stem cell transplantation with the EASIX biomarker panel. Haematologica. (2020) 106:446–53. doi: 10.3324/haematol.2019.238790, PMID: 31974195
24. Song GY, Jung SH, Kim K, Kim SJ, Yoon SE, Lee HS, et al. Endothelial activation and stress index (EASIX) is a reliable predictor for overall survival in patients with multiple myeloma. BMC Cancer. (2020) 20:803. doi: 10.1186/s12885-020-07317-y, PMID: 32831058
25. Varma A, Rondon G, Srour SA, Chen J, Ledesma C, Champlin RE, et al. Endothelial activation and stress index (EASIX) at admission predicts fluid overload in recipients of allogeneic stem cell transplantation. Biol Blood Marrow Transplant. (2020) 26:1013–20. doi: 10.1016/j.bbmt.2020.01.028, PMID: 32045652
26. Park S, Go SI, and Lee GW. The Endothelial Activation and Stress Index (EASIX) score is an independent prognostic factor in patients with diffuse large B-cell lymphoma. BMC Cancer. (2022) 22:816. doi: 10.1186/s12885-022-09915-4, PMID: 35879680
27. Merz A, Germing U, Kobbe G, Kaivers J, Jauch A, Radujkovic A, et al. EASIX for prediction of survival in lower-risk myelodysplastic syndromes. Blood Cancer J. (2019) 9:85. doi: 10.1038/s41408-019-0247-z, PMID: 31712595
28. Scully M, Cataland S, Coppo P, De La Rubia J, Friedman KD, Kremer Hovinga J, et al. Consensus on the standardization of terminology in thrombotic thrombocytopenic purpura and related thrombotic microangiopathies. J Thromb Haemost. (2017) 15:312–22. doi: 10.1111/jth.13571, PMID: 27868334
29. Jin M, Casper TC, Cataland SR, Kennedy MS, Lin S, Li YJ, et al. Relationship between ADAMTS13 activity in clinical remission and the risk of TTP relapse. Br J Haematol. (2008) 141:651–8. doi: 10.1111/j.1365-2141.2008.07107.x, PMID: 18397340
30. Peyvandi F, Lavoretano S, Palla R, Feys HB, Vanhoorelbeke K, Battaglioli T, et al. ADAMTS13 and anti-ADAMTS13 antibodies as markers for recurrence of acquired thrombotic thrombocytopenic purpura during remission. Haematologica. (2008) 93:232–9. doi: 10.3324/haematol.11739, PMID: 18223285
Keywords: ITTP, EASIX, ADAMTS13 activity, biomarker, endothelial dysfunction
Citation: Escribano-Serrat S, Salas MQ, Pascual-Izquierdo C, Fernández Villalobos M, Gómez-Seguí I, Fidalgo T, Fernández Docampo M, Martínez Nieto J, Lamas Ó, Lozano M, Cid J, Charry P, Pino M, Molina P, De Moner B, Ramos Á, Moreno-Castaño AB, Martinez-Sanchez J, Escolar G and Díaz-Ricart M (2025) EASIX, a new tool to predict response and refractoriness in immune-mediated thrombotic thrombocytopenic purpura. Front. Immunol. 16:1700907. doi: 10.3389/fimmu.2025.1700907
Received: 07 September 2025; Accepted: 29 October 2025;
Published: 17 November 2025.
Edited by:
Yudong Liu, Beijing Hospital/National Center of Gerontology, ChinaReviewed by:
Konstantine Halkidis, University of Kansas Medical Center, United StatesChristopher Graham, University of Minnesota Health Sciences and University of Minnesota Medical Center, United States
Copyright © 2025 Escribano-Serrat, Salas, Pascual-Izquierdo, Fernández Villalobos, Gómez-Seguí, Fidalgo, Fernández Docampo, Martínez Nieto, Lamas, Lozano, Cid, Charry, Pino, Molina, De Moner, Ramos, Moreno-Castaño, Martinez-Sanchez, Escolar and Díaz-Ricart. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Silvia Escribano-Serrat, c2lsdmlhLmVzY3JpYmFuby5zZXJyYXRAZ21haWwuY29t