 Hombamane Christelle Simfele1
Hombamane Christelle Simfele1 Gnatoulma Katawa1*
Gnatoulma Katawa1* Kathrin Arndts2,3
Kathrin Arndts2,3 Christèle Nguepou Tchopba1
Christèle Nguepou Tchopba1 Oukoe Marthe Amessoudji1
Oukoe Marthe Amessoudji1 Edlom Pélagie Tchadie1
Edlom Pélagie Tchadie1 Simplice Damintoti Karou1
Simplice Damintoti Karou1 Yaovi Ameyapoh1Achim Hoerauf2,3,4Malewe Kolou5Laura Layland-Heni2
Yaovi Ameyapoh1Achim Hoerauf2,3,4Malewe Kolou5Laura Layland-Heni2 Manuel Ritter2,3*
Manuel Ritter2,3*- 1Unité de Recherche en Immunologie et Immunomodulation (UR2IM)/Laboratoire de Microbiologie et de Contrôle de Qualité des Denrées Alimentaires (LAMICODA)/Ecole Supérieure des Techniques Biologiques et Alimentaires (ESTBA), Université de Lomé, Lomé, Togo
- 2Institute for Medical Microbiology, Immunology and Parasitology (IMMIP), University Hospital Bonn (UKB), Bonn, Germany
- 3German-West African Centre for Global Health and Pandemic Prevention (G-WAC), Partner Site Bonn, Bonn, Germany
- 4German Center for Infection Research (DZIF), Partner Site Bonn-Cologne, Bonn, Germany
- 5Faculté des Sciences de la Santé, Université de Lomé, Lomé, Togo
Background: The world health organization (WHO) introduced the mass drug administration (MDA) strategy in order to reduce the prevalence of soil-transmitted helminths (STHs) and Schistosoma mansoni in endemic areas. However, this strategy is not implemented in adult population in Togo. Thus, the question arose if the present MDA strategy contributes to the reduction of transmission rates. The present study aimed to monitor the prevalence of STHs and S. mansoni among adult’s, between 2017 and 2022, in the central region of Togo.
Methods: Two cross-sectional studies were conducted in six villages in the central region of Togo in 2017 and 2022. Stool samples were collected from adults over the age of 18 years. To assess STHs and S. mansoni infections, real-time multiplex qPCR and Kato-Katz techniques were performed. Data were analysed using SPSS software version 21 and GraphPad PRISM version 9.2.0. A p-value less than 0.05 was considered statistically significant.
Results: A total of 210 and 289 individuals were recruited in 2017 and 2022, respectively. We detected significant increase in the prevalence of STHs and S. mansoni from 7.61% to 24.56% (p=0.0008) and from 27.62% to 46.36% (p=0.0014) by Kato-Katz and RT-qPCR, respectively. The prevalence of Ancylostoma duodenale infection was the highest with an increase from 7.14% to 23.53% by Kato-Katz and 9.09% to 40.0% by RT-qPCR.
Conclusion: The prevalence of STHs and S. mansoni increased in the adult population in the central region of Togo from 2017 to 2022, despite the implementation of MDA in school-aged children. Hence, there is an urgent need to include adult individuals and adapt the MDA programme in the central region of Togo.
1 Introduction
Soil-transmitted helminths (STHs) and schistosomiasis are the most common parasitic worms in the world (1). These infections, disproportionately affect people and most of them in the underprivileged areas of Sub-Saharan Africa (2). In total, an estimated 1.5 billion people are infected with STHs (3) and about 250 million people are infected with schistosomiasis, 80% of whom live in Sub-Saharan Africa (4). STH infections are propagated by oral uptake of eggs that are excreted in the stool by people infected with STHs such as hookworm (Ancylostoma duodenale and Necator americanus), Ascaris lumbricoides, and Trichuris trichiura, whereas Schistosoma mansoni is transmitted through the penetration by the skin by cercariae which reside in fresh water (5, 6). STH infections can cause intestinal damage, loss of appetite, weakness, anaemia, and impaired physical and cognitive development (7); intestinal schistosomiasis can lead to abdominal pain, diarrhoea and blood in the stool causing severe public health problems in endemic regions (8). Children and pregnant women have been identified as the population at risk of STHs and schistosomiasis, with a high burden of disease for over 3.3 million and 1.8 million disability-adjusted life years (DALYs) respectively (9).
In order to control these infections, a global strategy programme based on preventive chemotherapy was introduced by the World Health Organisation (WHO) since 2006 (10). This programme consisted of mass drug administration (MDA) with praziquantel and albendazole for schistosomiasis and STH, respectively, mainly given to school-aged children (5 to 14 years old) (10, 11). Since then, several programmes in endemic countries, such as Togo, implemented periodic MDA according to WHO guidelines (12). Since 2010, this programme contributed to a decline in the prevalence of STHs from 31.5% to 11.6% and 23.5% to 5% for schistosomiasis in school-aged children between 2009 and 2015 (13). Similarly, in Ghana, a decrease in the prevalence of schistosomiasis from 23.8% to 3.6% and hookworm from 8.6% to 3.1% was observed (14) and also in other endemic countries such as Cameroon and Nigeria (15–17).
Despite the recent revision of WHO guidelines on the control of STHs and schistosomiasis, MDA is not effectively implemented in people over the age of 15 years (18) and therefore, the monitoring of STHs and schistosomiasis prevalence is less undertaken in this group. This could contribute to the failure of MDA programme, since this group is also exposed to infections. In the present study, we aim to monitor the prevalence of STHs and schistosomiasis between 2017 and 2022 in the Mô prefecture of the central region of Togo. Our findings contribute to improve WHO preventive chemotherapy programme and help countries health stakeholders to improve community policies to control and prevent STHs.
2 Methods
2.1 Study design and period
The present study based on two cross-sectional studies conducted in July 2017 and in August 2022. The frequencies of MDA were evaluated according to the national NTDs programme (Programme National de lutte contre les maladies tropicales négligées) guidelines. Their records from 2017 to 2021 were used.
2.2 Study area
This study was carried out in six villages of the Mô prefecture, namely Bato, Takadè, Kouida, Tchatchakou, Tchatoun-koura and Banda. The Mô prefecture is located in the central region of Togo close to the Ghanaian border (Figure 1). This area was chosen with reference to data provided by the National Programme for the Control of Neglected Tropical Diseases (NTDs) in Togo (Programme National de Lutte contre les Maladies Tropicales Négligées au Togo; PNLMTN) on areas of high prevalence of helminthiasis (20).
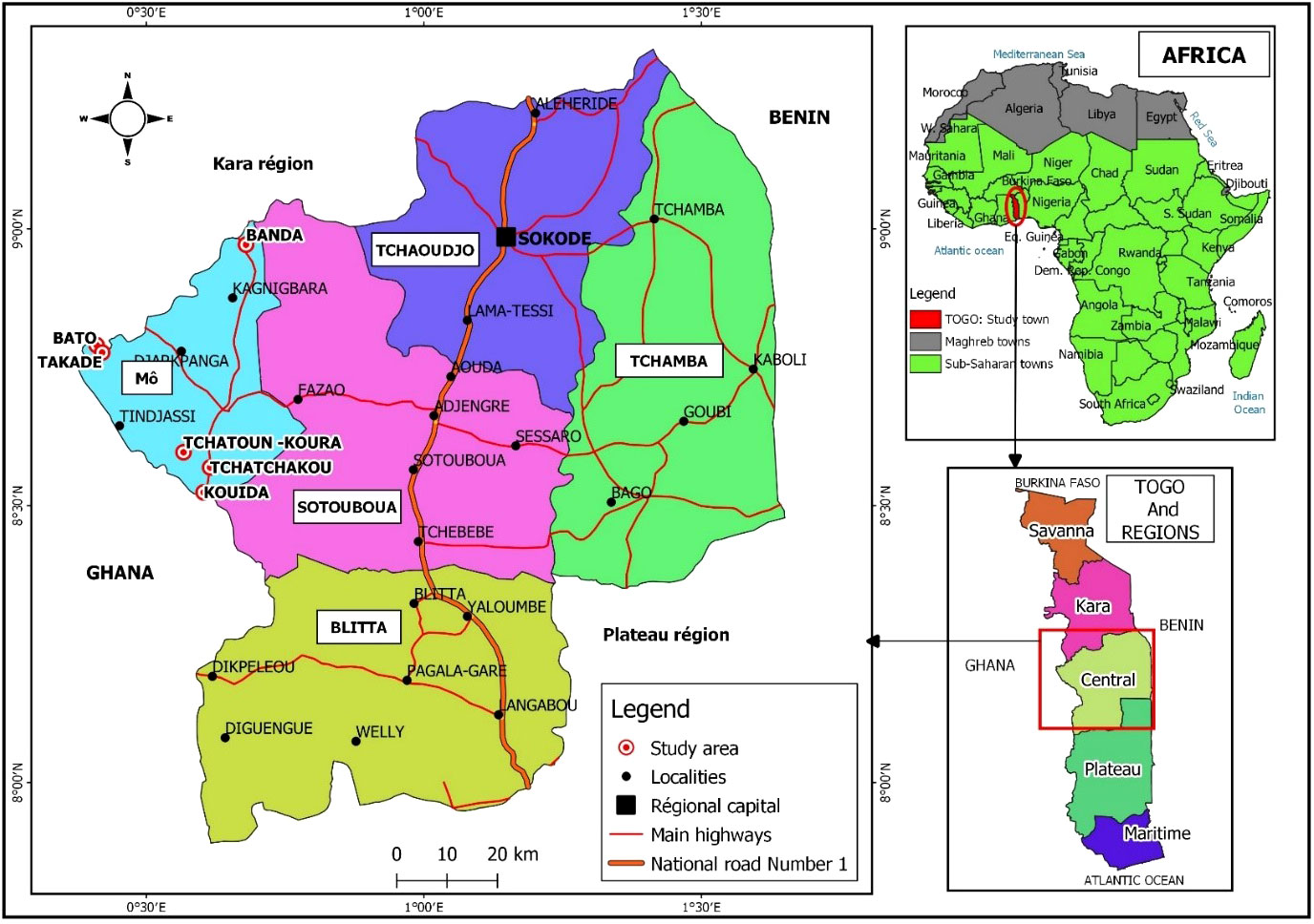
Figure 1 Map of Togo showing the Mô prefecture and the different study areas (created by our team during a previous study) (19).
2.3 Study population and sample size determination
The target population consists of male and female individuals over the age of 18 years, living in the study area for 10 years. The sample size was calculated according to the SCHWARTZ formula n= Z2 P (1-P)/d2 with Z, the accepted risk error at 1.96; d, the precision at 0.05; P, the prevalence of STHs estimated at 31.5% (12) and 11.6% (13) according to a previous study conducted in 2012 and 2018 in Togo respectively. Therefore, the estimated minimum sample size was 312 participants for the first study conducted in 2017 and 158 participants for that conducted in 2022.
2.4 Sample collection
The study was explained to the village communities during a meeting. Thereafter, stool containers (Quantum Biomedicals, Chennai, India) were distributed to participants to collect samples in the early morning. A semi-structured questionnaire was used to collect socio-demographic data. The questionnaire was validated in 2017 during a pilot study and was used for both studies. All information received from the participants was anonymised by assigning a code.
2.5 Parasitological diagnosis
The Kato-Katz (KK) technique was used to detect eggs of hookworm, A. lumbricoides, S. mansoni, T. trichiura and intestinal protozoan (21). The samples were processed in each locality on the same day at the sampling site or at the laboratory of the “Centre Hospitalier Préfectoral” (CHP) of Djarkpanga, where a team of qualified technicians evaluated the KK smears. The stool samples were then preserved in 1 mL of sterile eNAT medium (Copan, Brescia, Italy) and stored at -20°C for subsequent molecular analyses.
2.6 Molecular diagnosis of STHs and Schistosoma mansoni
2.6.1 DNA extraction
Previously stored stool samples were thawed and genomic DNA extracted using the Qiagen QIAmp Fast Stool Mini Kit (QIAGEN, Hilden, Germany) following the manufacturer’s instructions. Briefly, approximately 180 mg of stool was weighed into a 2 mL tube (Eppendorf, Hamburg, Germany) and placed on ice. The stool samples were then heated to 70°C in a water bath for 10 minutes and stool particles were crushed by centrifugation for one minute at 14,000 RPM (MIKRO 200, Berverly, USA). Following, 15 µL of proteinase K and 200 µL of lysis buffer (AL buffer) were added to 200 µL of stool supernatant and the mixture was incubated at 70°C for 15 minutes. The resulting lysate was mixed with 200 µL of 95% ethanol (Alcoford, Lomé, Togo) and inverted on the column (QIAamp spin) for centrifugation at 14,000 RPM for one minute. To remove any other stool debris, columns were washed twice with 500 µL of buffer 1 (AW1 buffer) and buffer 2 (AW2 buffer) at 14,000 RPM for one minute and 3 minutes respectively. Finally, the DNA was eluted with 200 µL of elution buffer (ATE buffer) onto the QIAamp membrane in 1.5 ml tubes after 5 minutes of incubation. Once elution was completed, DNA quantification was performed from each extract using the RG-3000 Rotor-gene thermal cycler (Corbett Research, Sydney, Australia). For that purpose, a solution of DNA extract of known concentration was used as the standard, then four successive dilutions were made to plot the standard curve. Then, a total reaction volume of 20 µL of the DNA extracts were added into each reaction well and a 16 minutes run was performed on the RG-3000 Rotor-gene thermal cycler. The DNA concentration measurement analysis operates by relating the fluorescence (A.FAM) level to a concentration values. DNA samples were stored at -20°C for subsequent RT-qPCR.
2.6.2 Real-time quantitative polymerase chain reaction (RT-qPCR) assays
RT-qPCR was performed on a Rotor-Gene 3000 system (Corbett Research) in a total reaction volume of 20 μL for the detection of STHs. Multiplex RT-qPCR was performed to detect A. duodenale, N. americanus, A. lumbricoides and S. mansoni using the iQ Multiplex Powermix (Bio-Rad Laboratories, Hercules, CA, USA) and species-specific primers (22). The reaction mixture consisted of: 1) 2 µL template (DNA template/plasmid) at a concentration of 20 ng/µL; 2) 10 µL iQ Multiplex Powermix; 3) a subtotal volume of 1 µL (Forward primer + Reverse primer + Probe) for each species tested, i.e., a total volume of 4 µL, as we have 4 species; 4) 4 µL H2O (Dnase Rnase free). The run consisted of an initial hold step of 95°C for 2 minutes, followed by 45 cycles of 95°C for 30 seconds and 53°C for 60 seconds. All species quenchers were acquired on last cycle of 53°C for 60 seconds.
All RT-qPCR runs included a positive control (plasmid) specific to each species of interest as well as a negative control consisting only of the master mix. All samples and controls were blinded and analysed in duplicate. Results were only considered positive when both duplicate samples were amplified with a cycle threshold below 40 (Ct <40) (23). Primers and probes used in the RT-qPCR are shown in Supplementary Data 1.
2.7 Sensitivity and specificity of RT-qPCR and Kato-Katz
The sensitivities and specificities of RT-qPCR and KK were calculated for STH species and S. mansoni. KK and PCR were used as a reference test (Gold standard). The 95% confidence intervals (95% CI), and percentage values were calculated using Microsoft Excel 2013. The formula used to calculate the sensitivity and specificity is summarised in Table 1 (24).
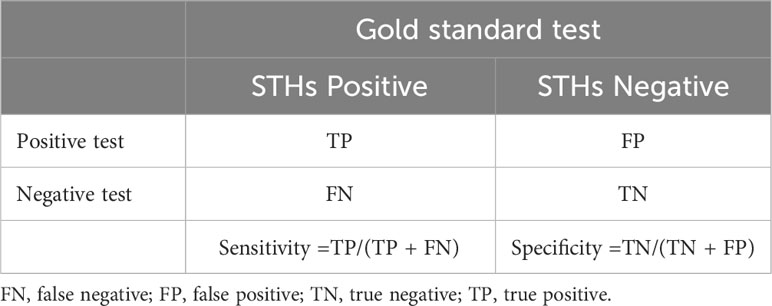
Table 1 Sensitivity and specificity calculation.
2.8 Statistical analysis
Statistical analysis was performed using SPSS software (IBM SPSS Statistics 21, Armonk, NY). Figures were generated using GraphPad PRISM version 9.2.0 software for Windows (GraphPad Software, San Diego California, USA). The Chi-square (χ2) test or Fisher’s exact test was used for percentage comparison. A p-value less than 0.05 was considered statistically significant.
2.9 Ethics approval and consent to participate
The study protocol was reviewed and approved by the ethical board of the Ministry of Health of Togo, “Comité de Bioéthique pour la Recherche en Santé” (CBRS), under the registration numbers 043/2016/MSPS/CAB/SG/DPLET/CBRS February 05th, 2016 and 029/2021/MSPS/CAB/SG/DPLET/CBRS June 25th, 2021 respectively in 2017 and 2022. All participants were informed about the study and provided written consent.
3 Results
3.1 Socio-demographic characteristics of the study population
A total of 210 subjects were recruited in the study area in 2017 and 289 subjects in 2022. The mean age of the participants was 37.15± 11.79 years and 42.01± 14.70 years in 2017 and 2022 respectively. The age ranges of 35-47 and 48-75 years were the most represented with 64 (30.5%) and 122 (42.2%) in 2017 and 2022 respectively. The mean lifetime in the study area was 24.43 years ± 13.66 in 2017 and 22.97 years ± 15.44 in 2022. Males were most represented with 121(57.6%) and 152(52.6%) in 2017 and 2022, respectively. The majority of the population were farmers with 147 (70.0%) and 240 (83.0%) in 2017 and 2022, respectively (Table 2).
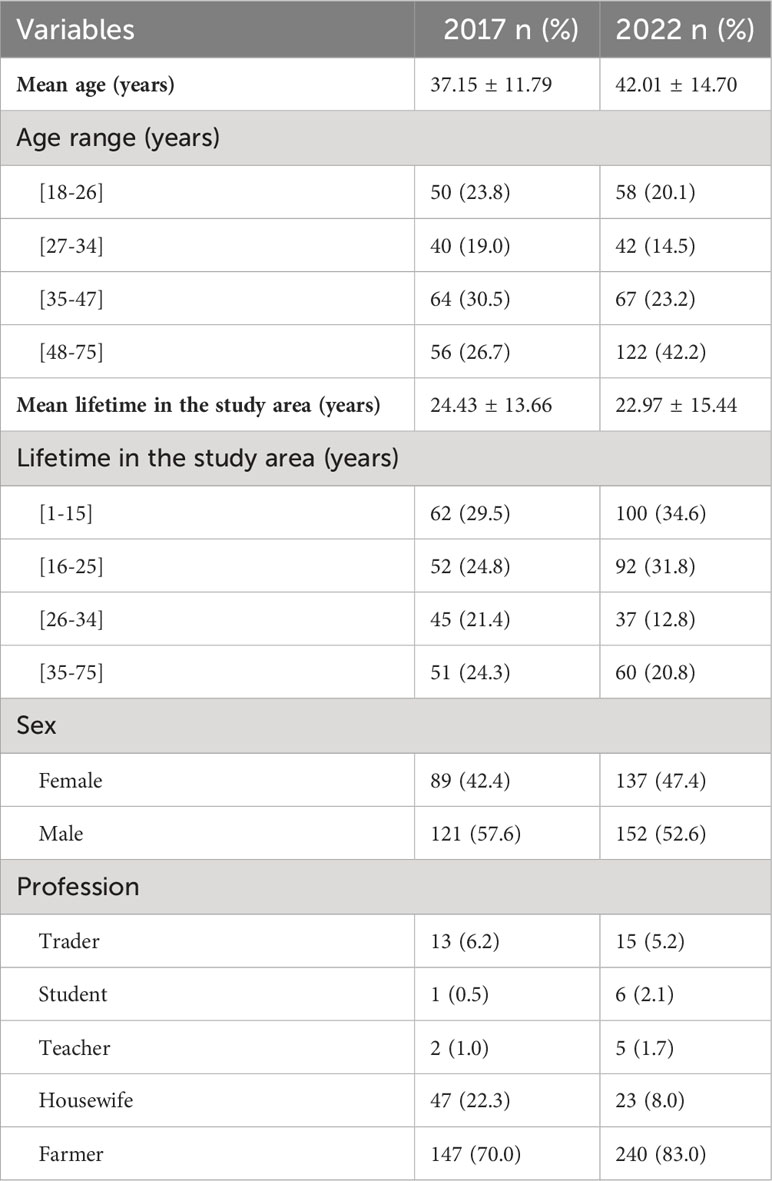
Table 2 Socio-demographic characteristics of the study population.
3.2 Status of deworming in the study area
The data in Tables 3, 4 provide an overview about the MDA with albendazole and praziquantel treatment strategies in the study area from 2017 and 2021. The population for treatment, included only school-aged children 5 to 14 years of age.
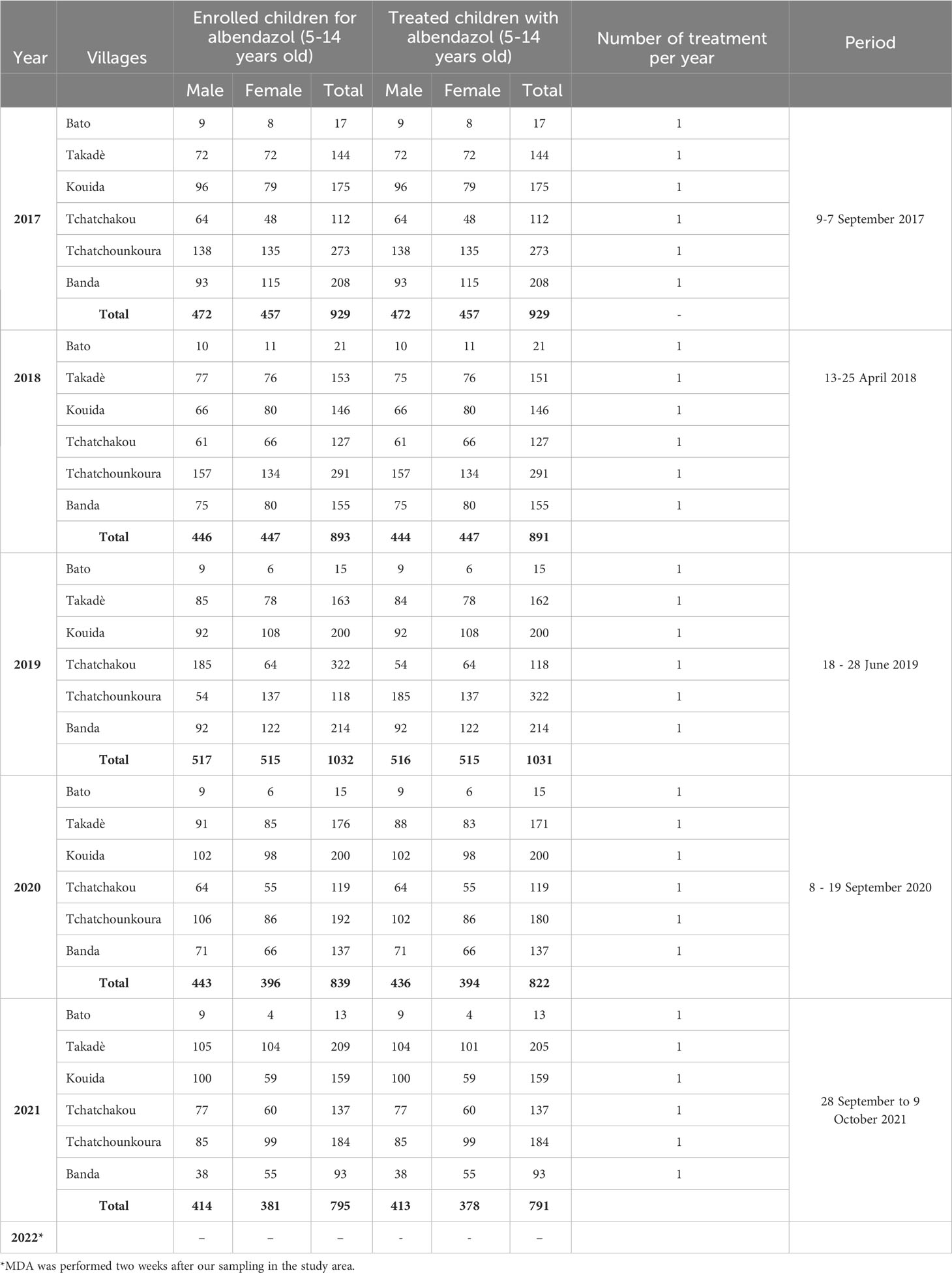
Table 3 Mass drug administration with albendazole in the study area.
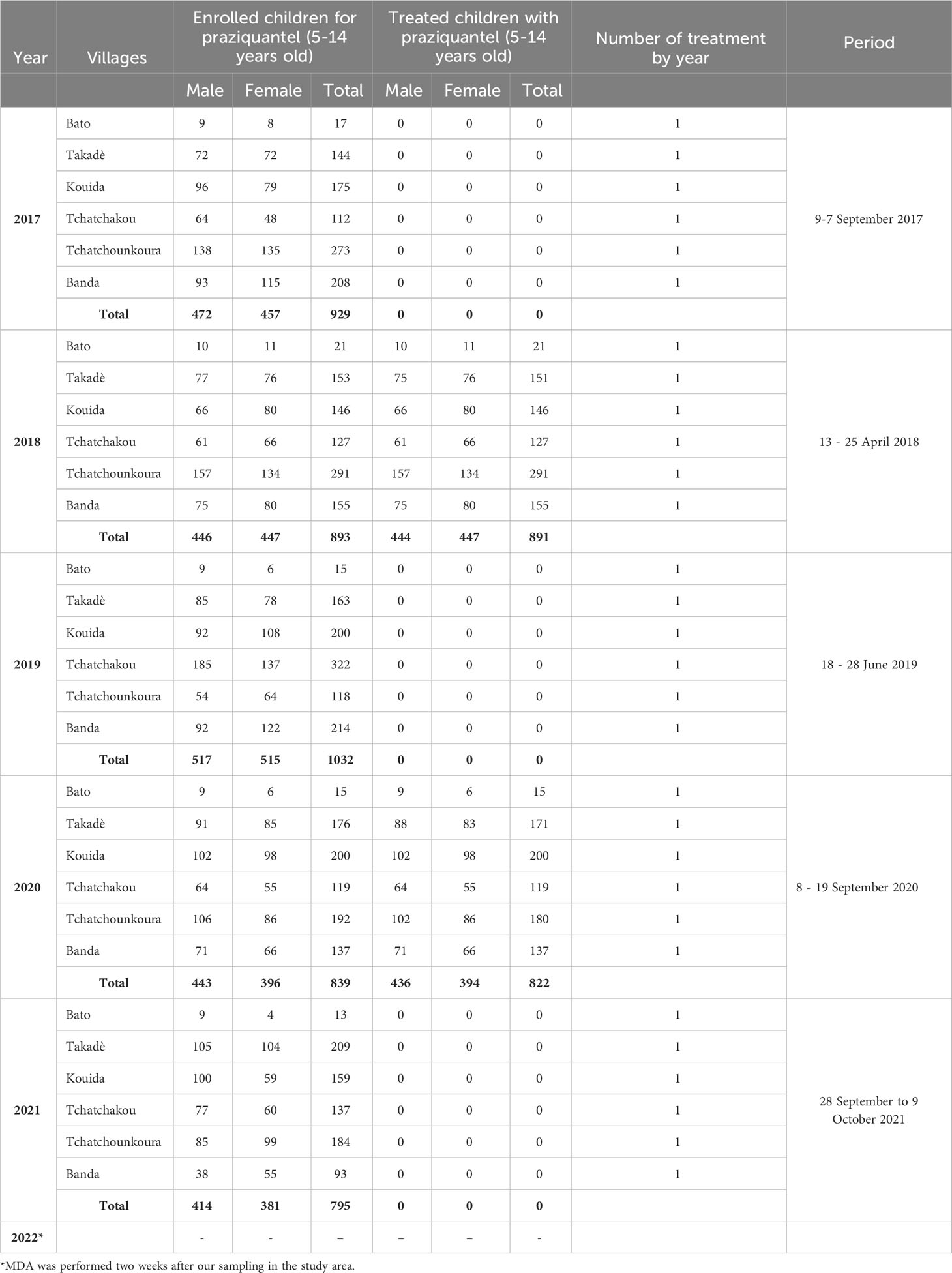
Table 4 Mass drug administration with praziquantel in the study area.
The deworming programmes were carried out once a year with albendazole and the treatment coverage was > 97% from 2017 to 2021 (Table 3). However, for praziquantel, the treatment is given every two years in the same age group and the treatment coverage was 99.78% in 2018 and 97.97% in 2020. There was no treatment in 2017, 2019 and 2021 (Table 4). Adolescents and adults (15 years and older) were not included into the MDA programme.
3.3 Sensitivity and specificity of RT-qPCR and Kato-Katz
In order to determine the performance of the RT-qPCR and KK approaches, sensitivities and specificities were calculated. For A. duodenale, the sensitivity of RT-qPCR related to KK was 100% in 2017 and 2022, while that of KK related to RT-qPCR was 45.45% and 57.63% in 2017 and 2022, respectively. The sensitivity of the KK and RT-qPCR tests was undetectable for A. lumbricoides, N. americanus and S. mansoni, due to the absence of double-positive subjects to both tests. However, in 2022 the sensitivity of RT-qPCR related to KK was 100% and 40% for KK related to RT-qPCR for S. mansoni. The specificity of KK related to RT-qPCR was elevated than RT-qPCR related KK for all species (Table 5). Absolute values obtained in the diagnostic assays are shown in Supplementary Data 2.
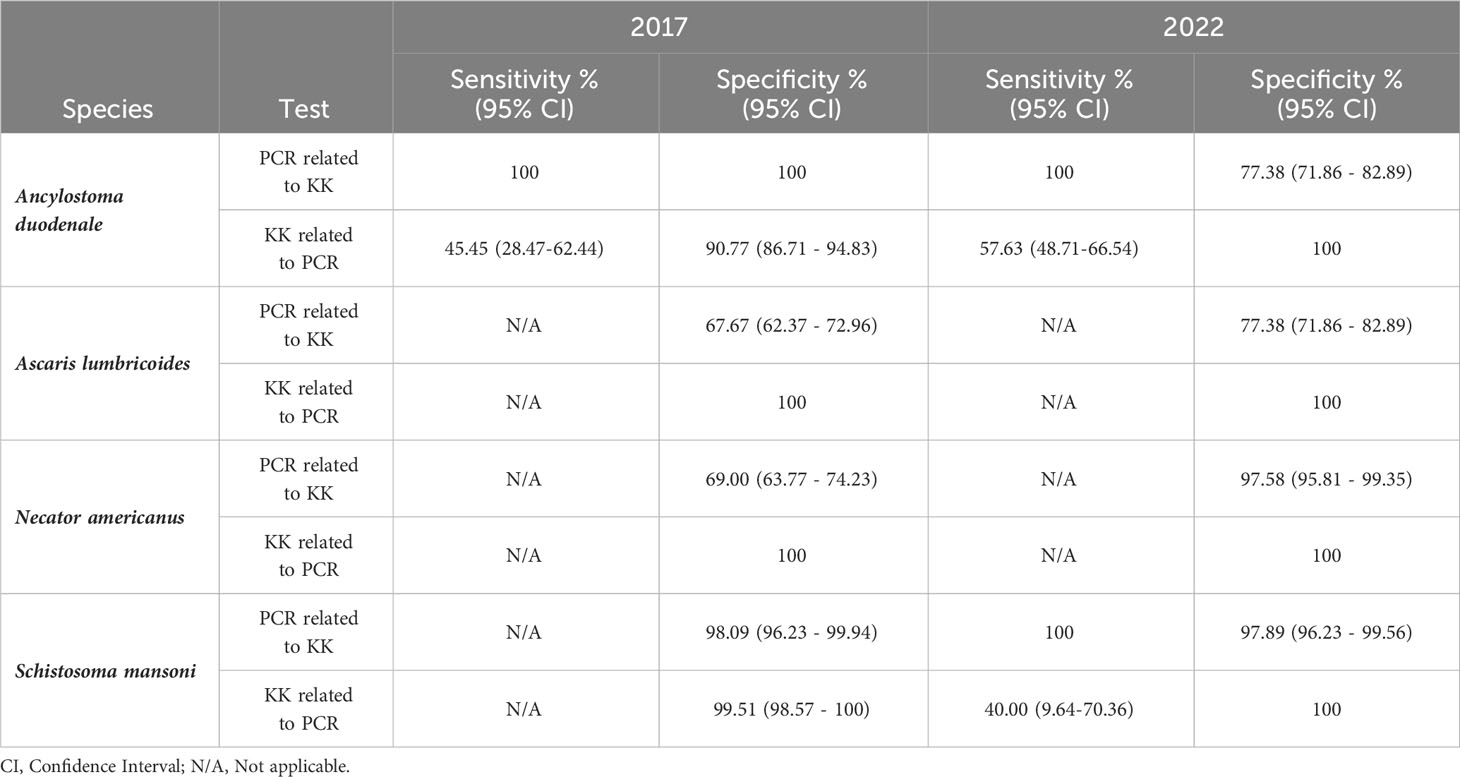
Table 5 Sensitivity and specificity of RT-qPCR and Kato-Katz for the different helminth species.
3.4 Increased STHs and S. mansoni prevalence from 2017 to 2022
From 2017 to 2022, the overall prevalence of STHs had significantly increased from 7.61% in 2017 to 24.56% in 2022 determined with the KK method (Figure 2A) and from 27.62% to 46.36% with the RT-qPCR method (Figure 2B). STHs were only detected in 5/6 villages by KK technique, whereas infected individuals were found in all of the villages using RT-qPCR. However, for all of the villages except Bato, we observed a general increase in the prevalence from 2017 to 2022. We found no cases of infection using the KK method in both 2017 and 2022 (Figure 2C) at Bato village, although RT-qPCR revealed 29.6% infection of helminths in 2017 and 28.6% in 2022 (Figure 2D). A. duodenale was the most prevalent helminth, with a significantly higher prevalence in 2022 than in 2017 analysed by KK (Figure 2E) and also by RT-qPCR (Figure 2F). With the KK technique we did not detect any infections with N. americanus and A. lumbricoides (Figure 2E), while RT-qPCR showed prevalence of 1.43% and 2.42% for N. americanus and 3.33% to 7.27% for A. lumbricoides (Figure 2F). S. mansoni prevalence increased from 0.48% to 1.38% by KK and from 2.38% to 3.46% by RT-qPCR although the difference was not statistically significant (Figures 2E, F).
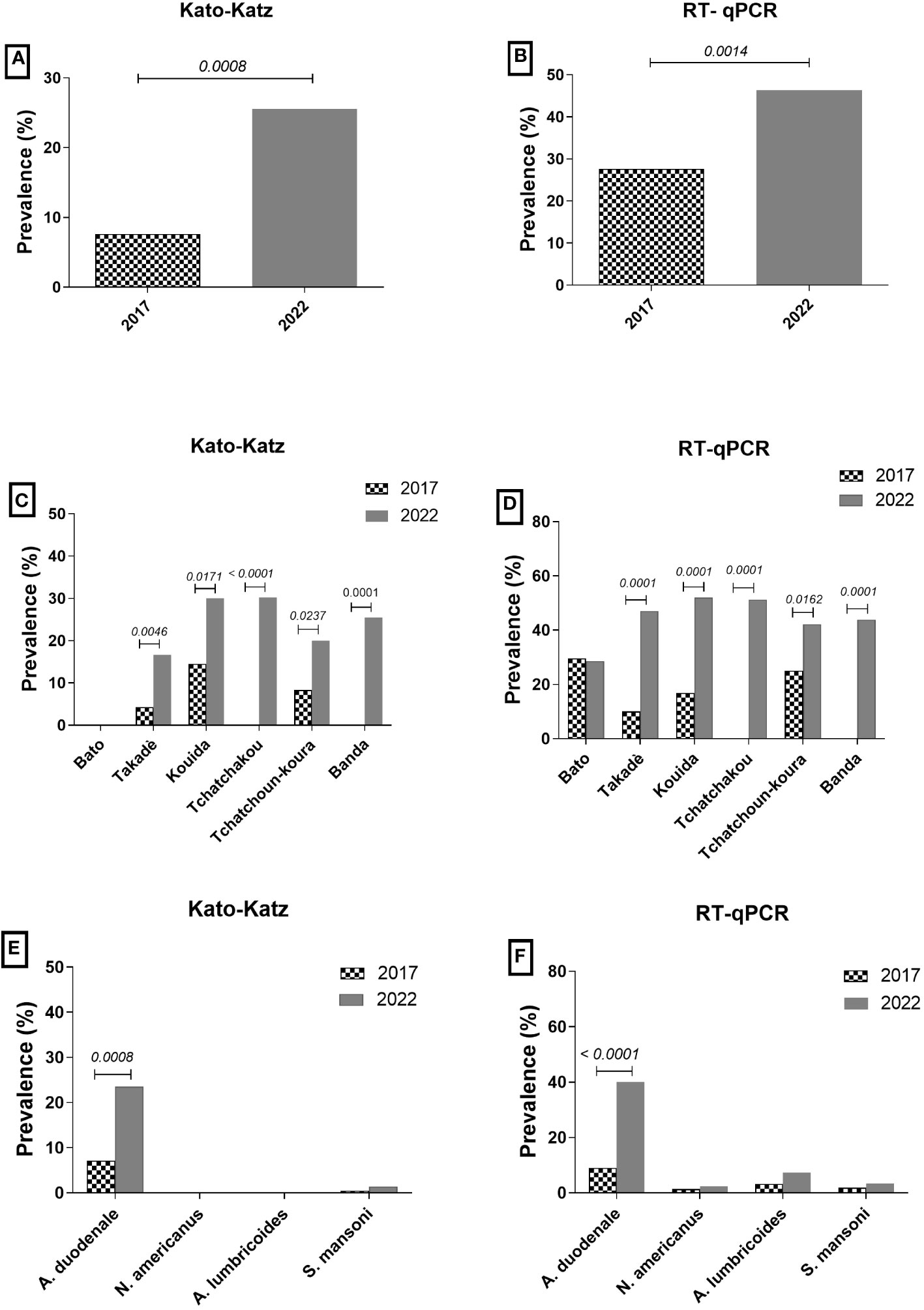
Figure 2 Prevalences of STHs and S. mansoni. Bars show the prevalence of infected people. (A) represents the total prevalence of STHs determined by KK and (B) by RT-qPCR in 2017 (n=210) and 2022 (n=289). (C) depicts the prevalence for individual villages using KK and (D) RT-qPCR. (E) shows the prevalence of the individual species studied by KK and (F) by RT-qPCR. For the comparison of percentages, a Fisher’s exact test was performed, significant differences of p<0.05 are indicated in the figures.
3.5 Despite MDA in school-aged children there was increase of STHs and S. mansoni infections in adults
The treatment coverage in school-aged children was 100% and 99.5% in 2017 and 2021 respectively. However, the prevalences of STHs and S. mansoni, among adults increased between 2017 and 2022, from 7.61% to 27.62% by Kato-Katz and from 24.56% to 46.36% by RT-qPCR (Table 6). Overall, these data show that despite the large coverage of MDA, in school-aged children, prevalence of STHs and S. mansoni increased from 2017 to 2022.

Table 6 Comparative table of MDA coverage in school-aged children and prevalence in adult.
4 Discussion
STHs and schistosomiasis remain public health problems despite efforts by the mass drug administration programmes to control these infections (25). The present study reported the prevalence of STHs among adults and revealed an overall increase in the prevalence of STHs and schistosomiasis from 2017 to 2022 in the six villages of the Mô prefecture in the central region of Togo. The MDA strategy in this area, which only includes children school-aged (5 to 14 years old) in the treatment of STHs and schistosomiasis (Table 4), may be a cause of increase in these infections in the adult population. It should be noted that the last deworming in the study area took place more than six months before the data collection in 2017 and 2022. However, due to the helminths endemic nature, even among people who receive treatment, reinfection may occur at any time of the year (26). For instance, a study on the effectiveness of MDA against STHs and schistosomiasis performed in 2018 in Togo, revealed a resurgence of hookworm infections in children who did not received albendazole in the previous 6 months (13). These parameters should be taken into account in future MDA strategies in the particular region but also in other endemic areas.
Among STH species assessed, A. duodenale was the most prevalent species in 2017 (7.14%) and 2022 (23.53%). Neither N. americanus nor A. lumbricoides cases were found. Similarly, during our previous study in 2020 in the central region of Togo we found that, among adult women (18 to 56 years old), hookworm was also the most prevalent parasitic infection with a prevalence of 95.34% (27). Moreover, according to a survey conducted in Togo in 2018, hookworm was the most frequent STH among school children in the central region of the country (15.2%), whereas A. lumbricoides and Trichuris trichiura were rare (28). As the prevalence of hookworm is as high in adults as in school-aged children, this could indicate the possibility of resistance of this species to drugs in this endemic area. Although most studies have focused on the prevalence of STH infections in school-aged children (29–32), it has been demonstrated that infections increase with age and peak in adults (33, 34). Thus our data is similar to that found in Tanzania where hookworm prevalence was highest (21.7%) followed by S. mansoni (12.4%) (35). STH infections can affect all age groups, and in view of the transmission cycle of the disease, we think that it is important to include adults in the MDA strategy to reach the elimination goals and protect vulnerable populations, such as children and pregnant women (5). The increase in prevalence observed in this study could continue if the control strategy is not reviewed, and this could slow down the WHO objective in the STHs and schistosomiasis elimination as a public health problem by 2030 (36). Interestingly, we did not detect Strongyloides infections, but the implemented Kato Katz method using a single stool sample is not suitable to accurately detect Strongyloides larvae. Thus, upcoming studies should use faecal culture methods and serological approaches to assess Strongyloides infections more in detail.
Our data showed that the prevalence of STHs and S. mansoni by KK microscopy was lower than that obtained by RT-qPCR method. The superiority of RT-qPCR to KK for diagnosing intestinal parasites has been described for 10 years now (37–39). This is also in accordance with findings from the area of Bato, since we observed an increase of prevalence from 0% to nearly 30% in 2017 and 2022. Similarly, Eindra et al. revealed that KK negative samples were positive using a RT-qPCR (40). Additionally, a study in the Philippines showed that RT-qPCR detected more STH infections than the KK method in school children (41). In addition, parasitological diagnosis such as microscopy is the most commonly method used in the surveillance of helminthiasis (42) since it is cost effective and does not require laboratory infrastructure. Nevertheless, it would be advantageous to include RT-qPCR diagnosis of helminths in epidemiological surveillance in Africa, especially in low-prevalence countries, whenever possible.
We noted that despite the large coverage of albendazole treatment, the prevalence of STHs increased between 2017 and 2022 in adults. This would be due to the exclusion of adults from the MDA programme. Our data are consistent with those found in Zambia where, the S. mansoni prevalence was elevated with 13.9% and 12.7% for both A. lumbricoides and hookworm, despite children in the same area were treated (43), which was also seen in Malawi (44). These treated children could be re-infected, due to the absence of parasite immunity, since they live in the same locality with infected adults, thus helping to maintain the transmission chain of the infection (45). However, this study has some limitations. As the study was cross-sectional, it was not possible to follow the included individuals over time to see whether they had been treated as children and inferable effect are not permitted due to the cross-sectional design of the study. However, given the mean age of the study population (37.15 ± 11.79 in 2017 and 42.01 ± 14.70 in 2022), most would not have had the chance to be included in the programme, since the deworming programme only began in Togo in 2010 (12).
In summary, we recommend that, as part of the implementation of the WHO roadmap for 2030, which targets that 90% fewer people require interventions against NTDs, 75% fewer NTD-related disability-adjusted life years and 100 countries achieving elimination of at least 1 NTD, more sensitive tests, such as PCR or circulating anodic antigen (CAA) recommended by the WHO should be used to confirm prevalence of less than 1% during epidemiological surveillance. Given that the prevalence of STHs has increased in the study area, it would be advisable to carry out an additional series of MDA, ideally also targeting adults. Moreover, surveys should be implemented each year to strengthen collaboration with handwashing (WASH) and sanitation partners, which have already proved their effectiveness in the fight against NTDs in Togo (28). In addition, a programme to provide an MDA coverage trend for each region should be established to guide intervention, which should be also connected to the Togo’s National Programme for the Control of Neglected Tropical Diseases (PNLMTNT). Indeed, the burden of STHs and schistosomiasis varies considerably from one region to another due to differences in the nature of the, as well as environmental disease (particular schistosomiasis, which demands fresh water and snails for the transmission), social, cultural and economic conditions (46). Thus, regional programmes should implement for mapping, monitoring and controlling/eliminating zoonotic diseases and conduct operational research to inform policy on the factors affecting the transmission, morbidity and control of STHs and schistosomiasis. Finally, regular evaluations of the epidemiological impact of interventions through regular assessment of disease prevalence should be established.
5 Conclusion
This study showed that the prevalence of STHs (especially hookworm infection) and Schistosoma mansoni, was increased in 2022 compared to 2017 in adults, although MDA programmes are implemented in school-aged children. Collectively, this study suggests that MDA programmes in school-aged children do not reduce STHs and schistosomiasis prevalence in adults in Togo. Therefore, deworming and testing programmes need to be expanded to adults especially in highly endemic areas to reach the goal of elimination of helminth infections as a public health problem in Togo.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding authors.
Ethics statement
The studies involving humans were approved by ethical board of the Ministry of Health of Togo, “Comité de Bioéthique pour la Recherche en Santé” (CBRS). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
HS: Conceptualization, Formal analysis, Methodology, Writing – original draft, Writing – review & editing. GK: Conceptualization, Data curation, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Writing – review & editing. KA: Validation, Visualization, Writing – review & editing. CN: Formal analysis, Methodology, Writing – review & editing. MA: Methodology, Writing – review & editing. ET: Methodology, Writing – review & editing. SK: Validation, Writing – review & editing. AY: Validation, Writing – review & editing. AH: Funding acquisition, Writing – review & editing. MK: Validation, Writing – review & editing. LL-H: Data curation, Funding acquisition, Supervision, Writing – review & editing. MR: Conceptualization, Project administration, Resources, Supervision, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was supported by the German Research Foundation (DFG) within the German-African Projects in Infectiology [LA 2746/1-1 and LA 2746/1-2] and AH was supported under Germany’s Excellence Strategy – EXC2151 – 390873048. The funders have no role in the publication of this manuscript.
Acknowledgments
We would like to thank all the villagers of the Mô prefecture of Togo who agreed to collaborate and participate in this study. The “National Programme for the Control of Neglected Tropical Diseases in Togo” which provided us MDA data for the study area.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fitd.2024.1283532/full#supplementary-material
References
1. King CH. Helminthiasis epidemiology and control: Scoring successes and meeting the remaining challenges. Adv Parasitol (2019) 103:11–30. doi: 10.1016/bs.apar.2018.08.001
2. Gebreyesus TD, Tadele T, Mekete K, Barry A, Gashaw H, Degefe W, et al. Prevalence, intensity, and correlates of schistosomiasis and soil-transmitted helminth infections after five rounds of preventive chemotherapy among school children in Southern Ethiopia. Pathogens (2020) 9(11):920. doi: 10.3390/pathogens9110920
3. WHO. Available at: Soil-transmitted helminth infections. (2023). https://www.who.int/news-room/fact-sheets/detail/soil-transmitted-helminth-infections.
4. Kjetland EF, Gundersen SG, Zulu SG, Taylor M. Prevalence and intensity of neglected tropical diseases (schistosomiasis and soil-transmitted helminths) amongst rural female pupils in Ugu district, KwaZulu-Natal, South Africa. S Afr J Infect Dis (2020) 35(1):1–7. doi: 10.4102/sajid.v35i1.123
5. Jourdan PM, Lamberton PH, Fenwick A, Addiss DG. Soil-transmitted helminth infections. Lancet (2018) 391(10117):252–65. doi: 10.1016/S0140-6736(17)31930-X
6. Braun L, Hazell L, Webb AJ, Allan F, Emery AM, Templeton MR. Determining the viability of Schistosoma mansoni cercariae using fluorescence assays: An application for water treatment. PLoS Negl Trop Dis (2020) 14(3):. doi: 10.1371/journal.pntd.0008176
7. Pullan RL, Smith JL, Jasrasaria R, Brooker S. Global numbers of infection and disease burden of soil transmitted helminth infections in 2010. Parasites Vectors (2014) 7(1):1–19. doi: 10.1186/1756-3305-7-37
8. Organisation WH. Soil-transmitted helminth infections 2022 . Available at: https://www.who.int/news-room/fact-sheets/detail/soil-transmitted-helminth-infections.
9. Bartlett AW, Sousa-Figueiredo JC, van Goor RC, Monaghan P, Lancaster W, Mugizi R, et al. Burden and factors associated with schistosomiasis and soil-transmitted helminth infections among school-age children in Huambo, Uige and Zaire provinces, Angola. Infect Dis Poverty (2022) 11(1):1–15. doi: 10.1186/s40249-022-00975-z
10. WHO Expert Committee. Prevention and control of schistosomiasis and soil-transmitted helminthiasis. World Health Organ Tech Rep Ser (2002) 912:1–57.
11. OMS. Lutte contre les helminthiases chez les enfants d’âge scolaire Deuxième édition Guide à l’intention des responsables des programmes de lutte. (2011). Available at: https://iris.who.int/bitstream/handle/10665/77959/?sequence=1.
12. Dorkenoo A, Bronzan R, Ayena K, Anthony G, Agbo Y, Sognikin K, et al. Nationwide integrated mapping of three neglected tropical diseases in Togo: countrywide implementation of a novel approach. Trop Med Int Health (2012) 17(7):896–903. doi: 10.1111/j.1365-3156.2012.03004.x
13. Bronzan RN, Dorkenoo AM, Agbo YM, Halatoko W, Layibo Y, Adjeloh P, et al. Impact of community-based integrated mass drug administration on schistosomiasis and soil-transmitted helminth prevalence in Togo. PLoS Negl Trop Dis (2018) 12(8). doi: 10.1371/journal.pntd.0006551
14. Kulinkina AV, Farnham A, Biritwum N-K, Utzinger J, Walz Y. How do disease control measures impact spatial predictions of schistosomiasis and hookworm? The example of predicting school-based prevalence before and after preventive chemotherapy in Ghana. PLoS Negl Trop Dis (2023) 17(6). doi: 10.1371/journal.pntd.0011424
15. Chelkeba L, Mekonnen Z, Emana D, Jimma W, Melaku T. Prevalence of soil-transmitted helminths infections among preschool and school-age children in Ethiopia: a systematic review and meta-analysis. Glob Health Res Policy (2022) 7(1):1–23. doi: 10.1186/s41256-022-00239-1
16. Nkengni SMM, Zoumabo ATC, Soppa NPS, Sizono ABN, Vignoles P, Tchuenté L-AT, et al. Current decline in schistosome and soil-transmitted helminth infections among school children at Loum, Littoral region, Cameroon. Pan Afr Med J (2019) 33. doi: 10.11604/pamj.2019.33.94.18265
17. Karshima S. Prevalence and distribution of soil-transmitted helminth infections in Nigerian children: a systematic review and meta-analysis. Infect Dis Poverty (2018) 7(04):1–14. doi: 10.1186/s40249-018-0451-2
18. Lo NC, Bezerra FSM, Colley DG, Fleming FM, Homeida M, Kabatereine N, et al. Review of 2022 WHO guidelines on the control and elimination of schistosomiasis. Lancet Infect Dis (2022) 22(11):e327–35. doi: 10.1016/S1473-3099(22)00221-3
19. Katawa G, Ataba E, Ritter M, Amessoudji OM, Awesso ER, TChadié PE, et al. Anti-Th17 and anti-Th2 responses effects of hydro-ethanolic extracts of Aframomum melegueta, Khaya Senegalensis and Xylopia aethiopica in hyperreactive onchocerciasis individuals’ peripheral blood mononuclear cells. PLoS Negl Trop Dis (2022) 16(4). doi: 10.1371/journal.pntd.0010341
20. Plan Directeur National de Lutte Intégrée contre les Maladies Tropicales Négligées (2016-2020). Available at: https://espen.afro.who.int/system/files/content/resources/TOGO_NTD_Master_Plan_2016_2020.pdf.
21. Katz N, Chaves A, Pellegrino J. A simple, device for quantita tive stool thick-smear technique in schistosomiasis mansoni. Rev Inst Med Trop Sao Paulo (1972) 14(6):397–400.
22. Hassan N, Noor Badi F, Mohd-Shaharuddin N, Wan Yusoff W, Lim Y, Chua K, et al. RESEARCH ARTICLE A conventional multiplex PCR for the detection of four common soil-transmitted nematodes in human feces: development and validation. Trop Biomed (2022) 39(1):135–43. doi: 10.47665/tb.39.1.016
23. Sturt AS, Webb EL, Patterson C, Phiri CR, Mweene T, Kjetland EF, et al. Cervicovaginal immune activation in Zambian women with female genital schistosomiasis. Front Immunol (2021) 12:620657. doi: 10.3389/fimmu.2021.620657
24. Fuss A, Mazigo HD, Tappe D, Kasang C, Mueller A. Comparison of sensitivity and specificity of three diagnostic tests to detect Schistosoma mansoni infections in school children in Mwanza region, Tanzania. PLoS ONE (2018) 13(8). doi: 10.1371/journal.pone.0202499
25. Rujeni N, Morona D, Ruberanziza E, Mazigo HD. Schistosomiasis and soil-transmitted helminthiasis in Rwanda: an update on their epidemiology and control. Infect Dis Poverty (2017) 6(1):1–11. doi: 10.1186/s40249-016-0212-z
26. Al-Mekhlafi MH, Surin J, Atiya A, Ariffin W, Mahdy AM, Abdullah HC. Pattern and predictors of soil-transmitted helminth reinfection among aboriginal schoolchildren in rural Peninsular Malaysia. Acta Trop (2008) 107(2):200–4. doi: 10.1016/j.actatropica.2008.05.022
27. Holali Ameyapoh A, Katawa G, Ritter M, Tchopba CN, TChadie PE, Arndts K, et al. Hookworm infections and sociodemographic factors associated with female reproductive tract infections in rural areas of the central region of Togo. Front Microbiol (2021) 12:738894. doi: 10.3389/fmicb.2021.738894
28. Baker JM, Trinies V, Bronzan RN, Dorkenoo AM, Garn JV, Sognikin S, et al. The associations between water and sanitation and hookworm infection using cross-sectional data from Togo’s national deworming program. PLoS Negl Trop Dis (2018) 12(3). doi: 10.1371/journal.pntd.0006374
29. Belay DG, Kibret AA, Diress M, Gela YY, Sinamaw D, Simegn W, et al. Deworming among preschool age children in sub-Saharan Africa: pooled prevalence and multi-level analysis. Trop Med Health (2022) 50(1):1–10. doi: 10.1186/s41182-022-00465-w
30. Ouédraogo JCRP, Jatta JW, Tabiri D, Nitiema M, Belemlilga MB. School-age children’S knowledge and perceptions concerning Soil-transmitted Helminthiases and Targeted Preventive Chemotherapy in Ghana’s Oti Region. Med Trop Sante Int (2022) 2(2):1–15. doi: 10.48327/mtsi.v2i2.2022.236
31. Hailegebriel T, Nibret E, Munshea A. Treatment. Prevalence of Soil-transmitted helminth infection among school-aged children of Ethiopia: a systematic review and meta-analysis. Infect Dis (Auckl) (2020) 13:1178633720962812. doi: 10.1177/1178633720962812
32. Rajan VXC, Sivamani M, Appalaraju B. Prevalence and the factors influencing soil-transmitted helminths among school age children (5–14 years age) in a rural area of Coimbatore district. Trop Parasitol (2020) 10(2):74. doi: 10.4103/tp.TP_33_19
33. Hotez PJ, Brooker S, Bethony JM, Bottazzi ME, Loukas A, Xiao S. Hookworm infection. N Engl J Med (2004) 351(8):799–807. doi: 10.1056/NEJMra032492
34. Forrer A, Vounatsou P, Sayasone S, Vonghachack Y, Bouakhasith D, Utzinger J, et al. Risk profiling of hookworm infection and intensity in southern Lao People’s Democratic Republic using Bayesian models. PLoS Negl Trop Dis (2015) 9(3). doi: 10.1371/journal.pntd.0003486
35. Siza JE, Kaatano GM, Chai J-Y, Eom KS, Rim H-J, Yong T-S, et al. Prevalence of schistosomes and soil-transmitted helminths and morbidity associated with schistosomiasis among adult population in Lake Victoria Basin, Tanzania. Korean J Parasitol (2015) 53(5):525. doi: 10.3347/kjp.2015.53.5.525
36. WHO. Ending the neglect to attain the Sustainable Development Goals: A road map for neglected tropical diseases 2021–2030. (2021), 2021–30. Available at: https://www.who.int/publications/i/item/9789240010352.
37. Mejia R, Vicuna Y, Broncano N, Sandoval C, Vaca M, Chico M, et al. A novel, multi-parallel, real-time polymerase chain reaction approach for eight gastrointestinal parasites provides improved diagnostic capabilities to resource-limited at-risk populations. Am J Trop Med Hyg (2013) 88(6):1041. doi: 10.4269/ajtmh.12-0726
38. Dunn JC, Papaiakovou M, Han KT, Chooneea D, Bettis AA, Wyine NY, et al. The increased sensitivity of qPCR in comparison to Kato-Katz is required for the accurate assessment of the prevalence of soil-transmitted helminth infection in settings that have received multiple rounds of mass drug administration. Parasites Vectors (2020) 13:1–11. doi: 10.1186/s13071-020-04197-w
39. Adisakwattana P, Yoonuan T, Phuphisut O, Poodeepiyasawat A, Homsuwan N, Gordon CA, et al. Clinical helminthiases in Thailand border regions show elevated prevalence levels using qPCR diagnostics combined with traditional microscopic methods. Parasites Vectors (2020) 13(1):1–10. doi: 10.1186/s13071-020-04290-0
40. Aung E, Han KT, Gordon CA, Hlaing NN, Aye MM, Htun MW, et al. High prevalence of soil-transmitted helminth infections in Myanmar schoolchildren. Infect Dis Poverty (2022) 11(1):1–12. doi: 10.1186/s40249-022-00952-6
41. Mationg MLS, Gordon CA, Tallo VL, Olveda RM, Alday PP, Reñosa MDC, et al. Status of soil-transmitted helminth infections in schoolchildren in Laguna Province, the Philippines: Determined by parasitological and molecular diagnostic techniques. PLoS Negl Trop Dis (2017) 11(11). doi: 10.1371/journal.pntd.0006022
42. Adu-Gyasi D, Asante KP, Frempong MT, Gyasi DK, Iddrisu LF, Ankrah L, et al. Epidemiology of soil transmitted Helminth infections in the middle-belt of Ghana, Africa. Parasite Epidemiol Control (2018) 3(3). doi: 10.1016/j.parepi.2018.e00071
43. Halwindi H, Magnussen P, Olsen A, Lisulo M. Potential contribution of adult populations to the maintenance of schistosomiasis and soil-transmitted helminth infections in the Siavonga and Mazabuka districts of Zambia. J Biosoc Sci (2017) 49(2):265–75. doi: 10.1017/S0021932016000201
44. Poole H, Terlouw DJ, Naunje A, Mzembe K, Stanton M, Betson M, et al. Schistosomiasis in pre-school-age children and their mothers in Chikhwawa district, Malawi with notes on characterization of schistosomes and snails. Parasites Vectors (2014) 7:1–12. doi: 10.1186/1756-3305-7-153
45. Means AR, Werkman M, Walson J. Prospects for elimination of soil-transmitted helminths. Curr Opin Infect Dis (2017) 30(5):482. doi: 10.1097/QCO.0000000000000395
Keywords: soil-transmitted helminths, S. mansoni, adults, MDA programme, school-aged children
Citation: Simfele HC, Katawa G, Arndts K, Tchopba CN, Amessoudji OM, Tchadie EP, Karou SD, Ameyapoh Y, Hoerauf A, Kolou M, Layland-Heni L and Ritter M (2024) Is a mass drug administration deworming programme for school-aged children enough to reduce the prevalence of soil-transmitted helminths and Schistosoma mansoni in adults: a cross-sectional study from Togo. Front. Trop. Dis 5:1283532. doi: 10.3389/fitd.2024.1283532
Received: 26 August 2023; Accepted: 23 January 2024;
Published: 13 February 2024.
Edited by:
Catherine A. Gordon, The University of Queensland, AustraliaReviewed by:
James Lee Crainey, Oswaldo Cruz Foundation (Fiocruz), BrazilIvan Mueller, University of Basel, Switzerland
Copyright © 2024 Simfele, Katawa, Arndts, Tchopba, Amessoudji, Tchadie, Karou, Ameyapoh, Hoerauf, Kolou, Layland-Heni and Ritter. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Gnatoulma Katawa, bWFoa2F0YXdhQHlhaG9vLmZy; Manuel Ritter, bWFudWVsLnJpdHRlckB1a2Jvbm4uZGU=