 Ndeye M. Kane1
Ndeye M. Kane1 Khadime Sylla2
Khadime Sylla2 Ngayo Sy3Boubacar Diop4Rose Monteil5Malang Mané5Daouda Gueye1Momadou L. Samb1
Ngayo Sy3Boubacar Diop4Rose Monteil5Malang Mané5Daouda Gueye1Momadou L. Samb1 Babacar Banda Diallo5
Babacar Banda Diallo5 Madeline Woo6
Madeline Woo6 Julie Ritter6Darin Evans7
Julie Ritter6Darin Evans7 Anna Phillips6*
Anna Phillips6*- 1Programme National de lutte contre les Maladies Tropicales Négligées (MTN), Ministère de la Santé et de l’Action Sociale, Dakar, Senegal
- 2Université Cheikh Anta Dio, Service Département parasitologie, Dakar, Senegal
- 3Service de Lutte Antiparasitaire de Thiès, Thiès, Senegal
- 4Ministère de la Santé et de l’Action Sociale, Dakar, Senegal
- 5Family Health International (FHI) 360, Dakar, Senegal
- 6Family Health International (FHI) 360, Washington, DC, United States
- 7US Agency for International Development (USAID), Washington, DC, United States
Introduction: Schistosomiasis has been a major public health concern in Senegal for almost 40 years. Mass drug administration (MDA) is the primary control strategy for treating schistosomiasis, however, there is a global limited availability of praziquantel therefore not all at-risk groups can be adequately treated. For settings in Senegal where there are numerous permanent bodies of water and persistent water contact, reducing prevalence and maintaining progress is challenging as reinfection occurs rapidly and can quickly return to pre-treatment levels.
Methods: In this paper we compare schistosomiasis prevalence following nearly 10 rounds of MDA. We also explore the impact of shifting decision-making from district-level prevalence to sub-district level prevalence on endemicity categorization and drug needs.
Results: Using mapping survey data from baseline (1996-2013) to the most recent impact assessment (2022-2024) we found that schistosomiasis prevalence declined significantly from 19.3% to 14.4%. Analysis of changes in endemicity categorization by district and sub-district level prevalence found that a larger percentage of sub-districts were classified as non-endemic, and a lower percentage of sub-districts were low or moderate/high endemicity compared to using district-level prevalence.
Conclusion: These differences suggest that shifting from treating entire districts to targeting sub-districts may yield similar outcomes to current strategies while offering economic and drug resource allocation benefits. This information is valuable for governments, donors, and implementation partners involved in the planning and execution of MDA programs in these regions.
1 Introduction
Schistosomiasis, commonly known as bilharzia, is a neglected tropical disease (NTD) affecting an estimated 251.4 million people worldwide across 51 countries, of which over 90% of cases are in Africa (1, 2). The schistosomiasis infection rate is particularly high in settings with poor sanitation and limited access to safe water (3). Schistosomiasis is an acute and chronic parasitic disease caused by blood flukes (trematode worms) of the genus Schistosoma. The two most common species in Africa are Schistosoma mansoni and S. haematobium, causing intestinal and urogenital schistosomiasis, respectively.
The mainstay control strategy is to periodically treat at least 75% of all school-aged children (SAC) who are at risk of morbidity from schistosomiasis through mass drug administration (MDA) with praziquantel (4–6). In 2022, the World Health Organization (WHO) released new treatment guidelines that recommend annual MDA in endemic communities with a prevalence of Schistosoma spp. infection ≥ 10% among all age groups at risk above 2 years of age, including pregnant women after the first trimester and lactating women (7). In communities with a prevalence of Schistosoma spp. infection < 10%, the WHO suggests one of the following two approaches based on programmatic objectives and resources: (i) where there has been a program of regular preventive chemotherapy, continue the intervention at the same or reduced frequency towards interruption of transmission; or (ii) where there has not been a program of regular preventive chemotherapy, to use a clinical approach of test and-treat, instead of MDA (7). There is, however, a global limited availability of donated praziquantel and not enough drugs to treat all at-risk groups. As a result, there is a simultaneous shift from mass treatment at the district to the sub-district level, but prevalence data often do not exist at this level.
Numerous research studies conducted in the 1980s found that schistosomiasis is a major public health problem in Senegal, which was exacerbated further by the construction of agricultural dams (8–13). As a result, an intergovernmental organization (Organisation pour la mise en Valeur du fleuve du Sénégal or OMVS) was established by the World Bank in 1995 around the Diama Dam in the Saint-Louis region (14). In 1999, the Senegalese Ministry of Health launched the National Schistosomiasis Control Program (PNLB) with funding from the World Bank. Baseline schistosomiasis mapping was conducted between 1996 and 2013 in two phases. In the first phase, 102 villages in 24 districts were mapped between 1996 and 2003. Based on these results, MDA started in 2009 and 2010 in 14 districts, focusing on SAC and adults at risk. Then, in 2012, with the support from the U.S. Agency for International Development (USAID), and in 2013, with funding from the Schistosomiasis Control Initiative (SCI), the PNLB conducted a final mapping of the central and southern regions of Senegal in a further 27 districts.
Along the Senegal river basin, treatment with praziquantel has proved effective at reducing schistosomiasis but the prevalence remains high in some areas due to the abundance of permanent water bodies and persistent water contact that maintains transmission of the disease throughout the year (15). Therefore, in such settings, despite repeated MDA, the control of schistosomiasis transmission is difficult as reinfection occurs rapidly, and the prevalence can return to pre-treatment levels quickly (16–18). The third MDA was implemented in 2014, and, by 2016, nationwide treatment had been scaled up. As per the WHO guidelines, after four to five rounds of MDA, impact evaluations were conducted between 2016 and 2020 in the Senegal Basin River to assess the impact of treatment and review the treatment strategy (19–22). As part of optimizing schistosomiasis treatment and eliminating it as a public health problem, the WHO shifted its recommendations and encouraged countries to update schistosomiasis endemicity at the sub-district level (rather than district) to better target populations requiring chemoprevention with praziquantel. It is in this context that the national schistosomiasis control program conducted an analysis of the first impact assessment data in collaboration with the WHO/Expanded Special Project for the Elimination of Neglected Tropical Diseases (ESPEN) to categorize sub-district schistosomiasis endemicity across the country in 2021. This exercise highlighted the evidence gap in the number of sub-districts without prevalence information (23). As a result, between 2022 and 2024, Senegal started to scale up sub-district level surveys not only to evaluate the impact of MDA and reassess the burden of schistosomiasis after 5 years of MDA, but also to enable a paradigm shift in implementation strategy (23). Here, we present the prevalence of schistosomiasis among SAC in Senegal from baseline to 2024, following up to 10 rounds of preventive chemotherapy.
2 Methods
There have been three major schistosomiasis surveys conducted in Senegal. The first baseline evaluation was carried out between 1996 and 2013, followed by a post-MDA evaluation between 2016 and 2020, and, more recently, a second reassessment in 2022–2024 (see Table 1). Simultaneously, there has been a change in focus by WHO over the last 15 years (from district to sub-district implementation) and donors with different budget priorities, both of which have had an impact on the consistency of study design over time.
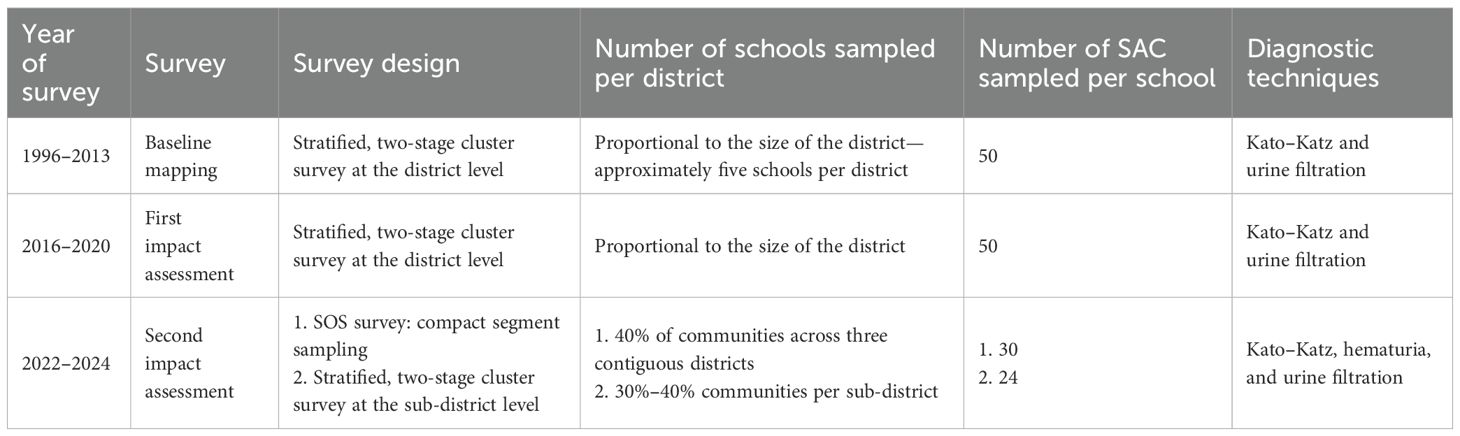
Table 1. Summary of schistosomiasis surveys from baseline mapping to the most recent surveys.
2.1 Baseline mapping (1996–2013)
Baseline disease mapping of schistosomiasis was conducted between 1996 and 2013 whereby the sample size was calculated to give the same spatial density of schools used in similar surveys from neighboring West African countries, which equated to approximately five schools sampled per district (24, 25). In brief, 50 SAC aged 5–14 years stratified equally by sex (25 girls and 25 boys) were selected using systematic random sampling of class lists in each school in accordance with WHO mapping guidelines. All selected SAC were asked to provide a stool sample that was examined microscopically using duplicate Kato–Katz for the eggs of STH (Ascaris lumbricoides, Trichuris trichiura, and hookworms) and S. mansoni (4). Average eggs across two slides were used to calculate the eggs per gram (epg) of stool for each organism and the threshold for heavy-intensity infections was ≥400 epg of stool (4, 26). Each child also provided a urine sample where up to 10 mL was filtered through polycarbonate filters with a pore size of 8–30 μm and the number of eggs of S. haematobium was counted and expressed as eggs per 10 mL of urine (4). Infection was categorized according to WHO guidelines, where heavy infections were defined as ≥50 eggs per 10 ml of urine (4). Urogenital schistosomiasis infection was defined as having the presence of hematuria and/or S. haematobium eggs in the urine (4, 27).
2.2 First schistosomiasis impact assessment (2016–2020)
By 2016, schistosomiasis treatment in all endemic districts had been achieved, and after 5 years of MDA implementation, the WHO recommends an impact evaluation of MDA on schistosomiasis prevalence (4). The same survey method was used as a baseline, with the selection of schools proportional to the size of the district, which resulted in approximately five schools sampled per district. The assessments were rolled out systematically with 11 districts surveyed in 2016, nine districts in 2017, six districts in 2018, eight districts in 2019, and finally five districts in 2020 (19–22). Like at baseline, 50 SAC were chosen using systematic random sampling of class lists by age and sex in each school using duplicate Kato–Katz for STH and S. mansoni diagnosis and urine filtration for S. haematobium (4).
2.3 Second schistosomiasis impact assessment (2022–2024)
Due to the shift from district to sub-district implementation and the evidence gap to enable the change in approach, sub-district level schistosomiasis assessments were rolled out, starting with eight districts (94 sub-districts) surveyed in 2022, 13 districts (167 sub-districts) in 2023, and 22 districts (195 sub-districts) in 2024.
The survey method has been published elsewhere, but to summarize, a stratified, two-stage cluster survey design was used whereby the first selection was a simple random sample of sites (schools) in each sub-district, and the second selection was SAC in schools (28, 29). The survey sample size was decided based on precision-based sample size calculations. In brief, since the survey aimed to estimate the prevalence at the sub-district level, which is probably less ecologically heterogeneous than the district, an estimated intra-cluster correlation coefficient (ICC) of 0.041 was used (28). Villages were selected proportional to sub-district size (approximately 30%–40% of communities). In each selected village, a school was selected. Sample size calculations were performed to find a two-stage cluster survey design that would be capable of estimating 50% prevalence with a 10-percentage-point margin of error on the 95% confidence interval, using calculations from Lohr (30). This led to a recommended sample size of 15–20 schools per district (dependent on the size of the district) and 2–3 schools per sub-district, with 24 children aged 5–14 years sampled per school (12 girls and 12 boys) (29). In a selected school, students from the first six primary schools were recruited into the study. In each class, the students were assembled in separate lines—one line of boys and one line of girls. Two boys and two girls were subsequently selected randomly. A list of the students who were selected for the study was given to the school authority for their records. The respondents were interviewed with a semi-structured questionnaire using the ESPEN Collect with global positioning system (GPS) coordinates for each school and water, sanitation, and hygiene (WASH) data were recorded (31).
Laboratories were set up in schools or health posts to ensure samples were examined immediately after they were produced. Upon collection in the field, each urine sample was visually assessed, and the results were recorded as clear, turbid, or bloody. The samples were tested immediately at the school using a urine dipstick (Haemastix®) according to the manufacturer’s instructions for examining the presence of blood, as a proxy measure for S. haematobium. The Haemastix® results were graded as “negative”, “trace not haemolysed”, “trace haemolysed”, “+”, “++”, and “+++”, respectively. All hematuria-positive samples were then processed using the filtration technique and the slide was microscopically examined for S. haematobium eggs (27). Single stool samples were examined for the presence of STH and S. mansoni using the Kato–Katz technique on duplicate slides and the results were read by a laboratory technician using standard procedures (26).
2.4 Statistical analysis
In all survey years, each child had a unique ID number allocated to them for anonymous analysis of their parasitological results. In the baseline mapping and first impact assessment, individual-level data were collected on paper and then double-entered into Microsoft Excel (Microsoft Corporation, Bellevue, WA). In the second impact assessment, data were collected on Android tablets using ESPEN Collect (31). The analysis utilized current geography to compare prevalence over time and included an analysis of aggregated prevalence at the regional level across survey years. Data were analyzed in STATA 16.1 (StataCorp, College Station, TX) with figures generated utilizing multiple packages in R (v4.3.3; R Core Team 2024, Vienna, Austria). Disease prevalence estimates using baseline and most recent survey data were calculated and 95% confidence intervals were determined using negative binomial regression. Prevalence estimates between the baseline data and the most recent survey data were compared using a two-sample test of proportions. The significance threshold for all statistical tests was set at 0.05. Missing data were excluded from estimates of prevalence. Only aggregated school-level data were available for the baseline; however, individual-level data were available for the first and second impact assessments but are not presented here due to a lack of historical comparison data. The maps were generated utilizing Python (Python Software Foundation, version 3.13.1. Available at http://www.python.org) to join the prevalence tables with the shapefiles and ArcGIS Pro to visualize the data and create the maps. Population data was from the national census compiled by the National Agency of Statistics and Demography of Senegal (ANSD).
3 Results
Baseline schistosomiasis mapping was conducted in a total of 48 districts, with 218 schools and 17,865 SAC sampled. Overall schistosomiasis prevalence across all the schools sampled between 1996 and 2013 was 13.2%, with the district-level prevalence ranging from 0% to 91.2%. Following several rounds of treatment, a schistosomiasis impact assessment was then carried out between 2016 and 2020 across 32 districts, with 145 schools and 8,345 SAC sampled. Overall prevalence in all the schools sampled was 22.5%, with district-level prevalence ranging from 0% to 94.8%. More recently, a second impact evaluation, this time powered to estimate prevalence at the sub-district rather than the district level, was carried out between 2022 and 2024. In total, 29 districts (456 sub-districts), 727 schools, and 18,884 SAC were sampled. Overall schistosomiasis prevalence across all the schools surveyed in this time frame was 14.7%, with the district-level prevalence ranging from 0% to 47.3% (Table 2). In summary, when considering overall national prevalence at each time point, there was no statistically significant change in prevalence between baseline (13.2%) and current (14.7%; p=0.06). Considering regional prevalence, however, there was a statistically significant reduction in most regions (Table 2; Supplementary Tables 1, 2).
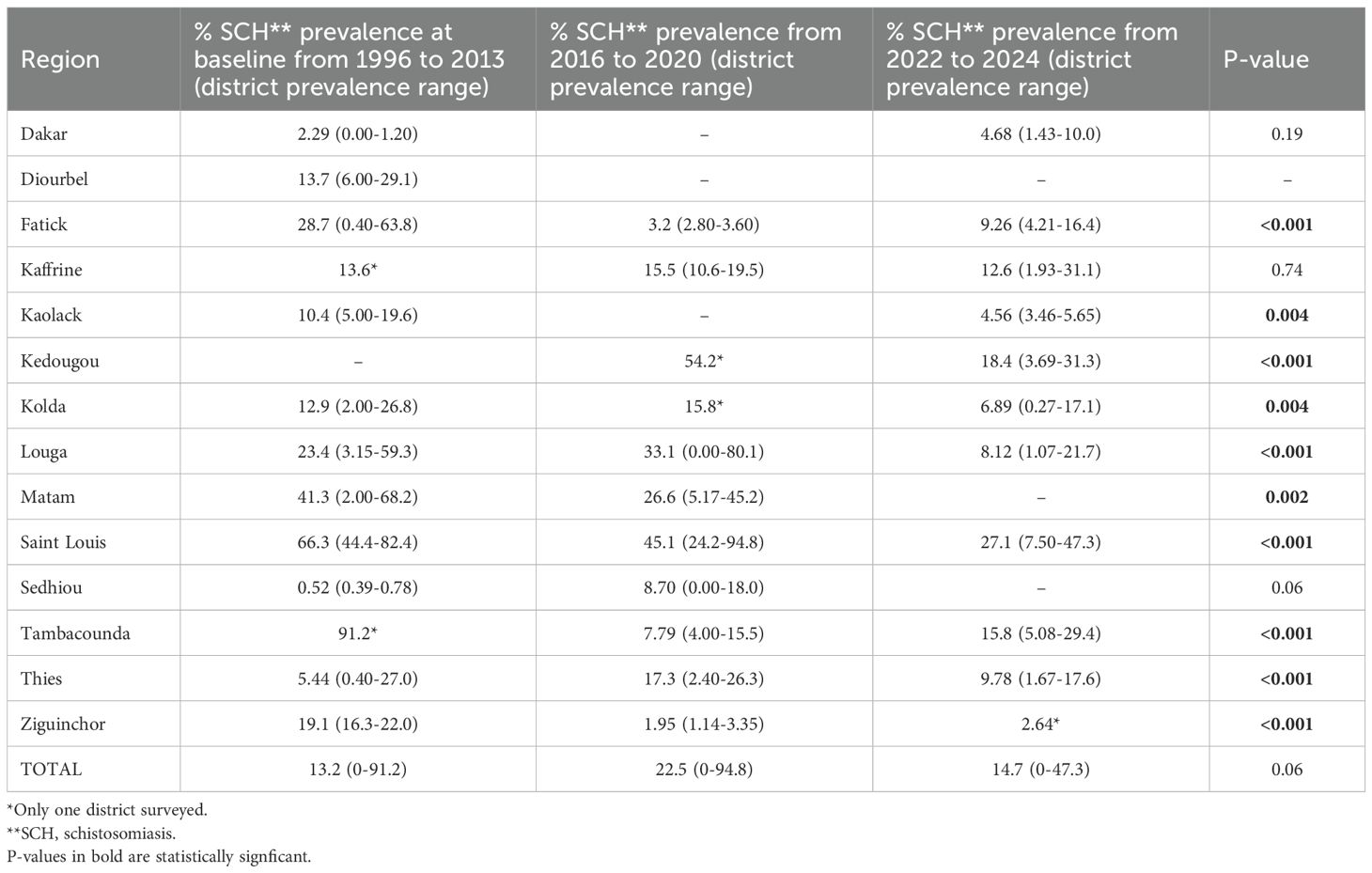
Table 2. Summary of schistosomiasis prevalence across all regions over time. .
Since different districts were surveyed at each time point, the prevalence in the subset of districts that were assessed both at baseline and the most recent survey was analyzed (Table 3 and Figure 1). Overall, schistosomiasis prevalence has decreased significantly from the start of the program (19.3%) to the most recent survey (14.4%), both in S. mansoni (0.01% to 0.002%) and S. haematobium infection (21.5% to 15.0%), the more predominant species (p<0.001).

Table 3. Schistosomiasis prevalence at baseline compared with the most recent (2022–2024) survey in a subset of districts assessed at both time points only (N=26).
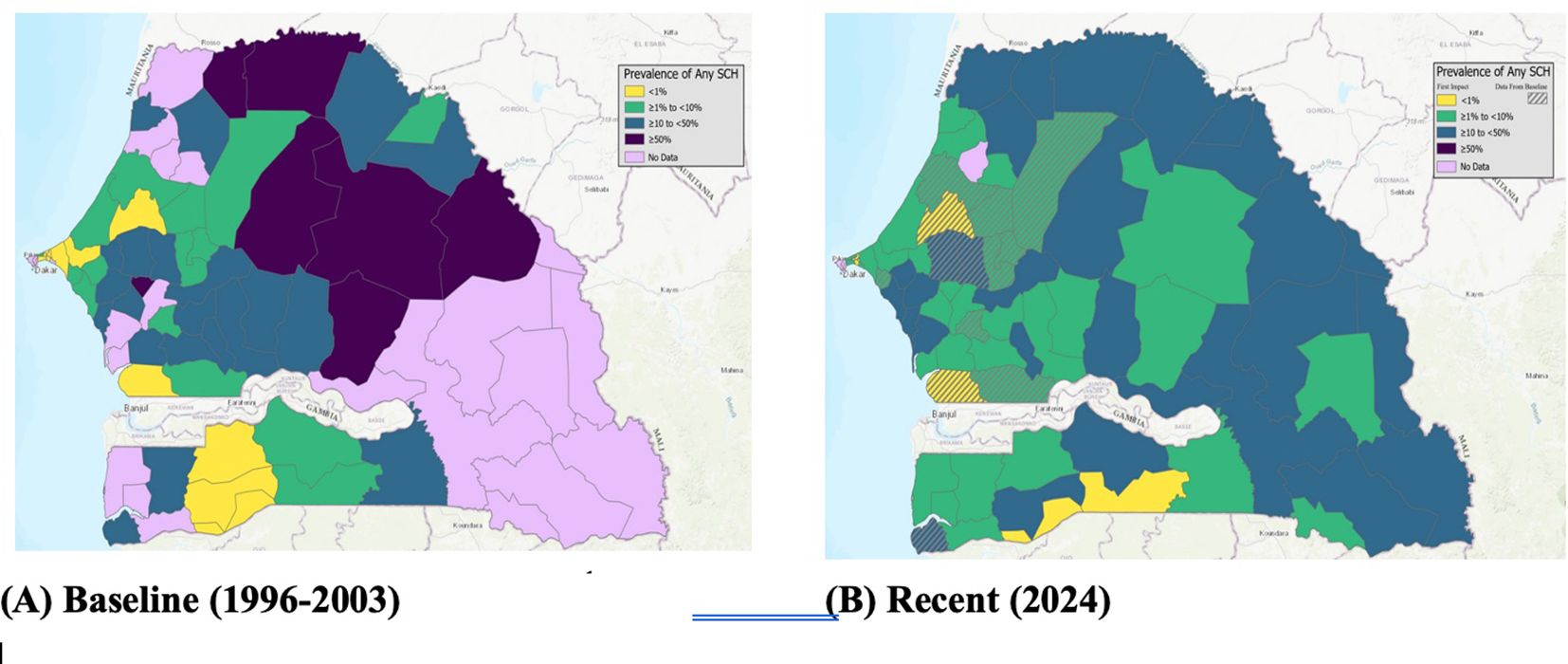
Figure 1. District-level baseline (1996–2003) and recent (2022–2024) schistosomiasis mapping.
3.1 Changes in endemicity from district to sub-district implementation
Figure 2 illustrates how the endemicity category changes when considering the prevalence in the recent survey at the district level vs. the sub-district level. Overall, 8.5% of the districts (95% CI: 6.2%–12.0%) were classified as non-endemic, yet at the sub-district level, 18.7% (95% CI: 16.4%–21.4%) were non-endemic, i.e., the prevalence was <%, which was statistically significant (p<0.001). The proportion of low endemic districts was higher at 48.5% (95% CI: 41.3%–46.3%) compared with the proportion of sub-districts at 42.3% (95% CI: 40.1%–45.1%). Finally, the number of moderate to high (i.e., greater than 10%) implementation units (IUs) that were eligible for community-wide treatment was higher at the district-level with 42.9% (95% CI: 40.6%–45.6%) compared to 39.0% of the sub-districts (95% CI: 36.7%–41.0%).
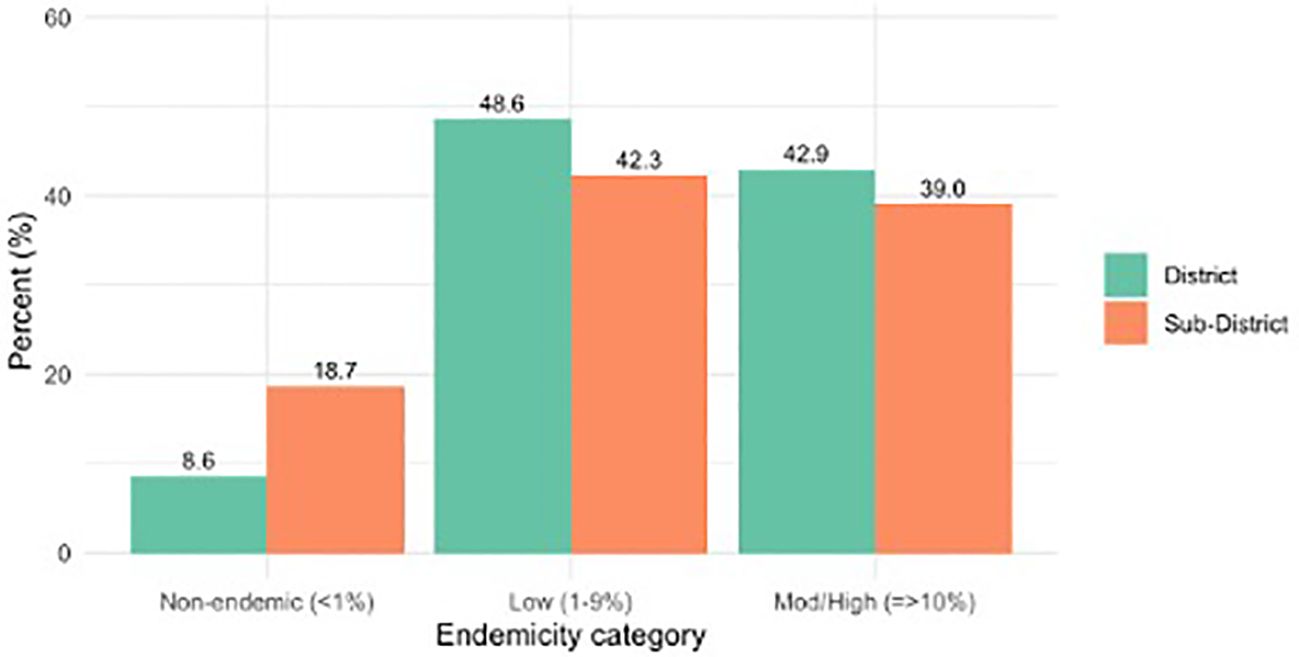
Figure 2. Comparison of endemicity by district and sub-district (2003–2024); N=70 for districts and N=1,519 for subdistricts.
Figure 3 visualizes the average sub-district prevalence at baseline with respect to the most recent surveys conducted. At baseline, there was very little prevalence data at the sub-district level due to inefficient sample size (five sites sampled per district) and despite the intensive surveying conducted between 2022 and 2024, there remains a current gap in prevalence information at the sub-district level. Furthermore, when analyzing the most recent district prevalence map (Figure 1), it is possible to see how high infection pockets at the sub-district level (Figure 3) are masked by the average district prevalence.
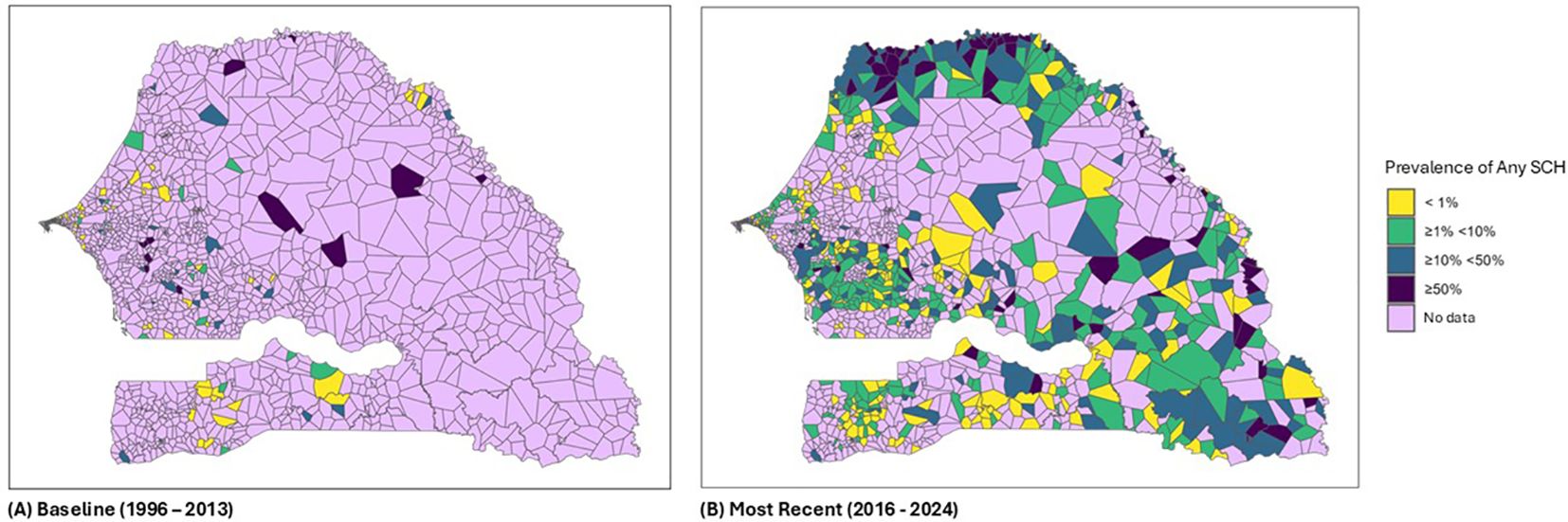
Figure 3. Sub-district-level baseline (1996–2003) and recent (2022–2024) schistosomiasis mapping.
3.1.1 The impact of implementation unit level on drug needs
The higher proportion of non-endemic sub-districts and lower proportion of low and moderate-high endemic sub-districts indicate that if Senegal conducts treatment at the sub-district level, there should be less drug need than at the district level. Table 4 provides the total treatment numbers calculated at the district and sub-district levels by endemicity using the recent WHO recommendations, i.e., no treatment if prevalence <1%, biennial MDA if prevalence is low (1%–9%), and community-wide annual treatment where prevalence is ≥10% (7). There is a stark difference in the treatment need when calculating the prevalence at the district level, with an estimated 14.7 million praziquantel pills needed vs. 12.7 million per year if calculating drug need at the sub-district level (see Table 4).

Table 4. Total treatment numbers calculated at the district and sub-district levels by endemicity based on the 2022 WHO recommendations.
3.2 Discussion
There have been multiple schistosomiasis surveys conducted in Senegal over the last 25 years, all of which have demonstrated the high rate of schistosomiasis transmission across the country (8–14, 19–22). To support the Ministry of Health in collating this wealth of data, the Act to End NTDs West Africa project created a schistosomiasis disease tracker that the Senegal NTD program populated with historical survey data. This enabled the analysis of change in prevalence over time, which is complex to track as both different districts and survey methods have been used over the years. Nevertheless, this tool was able to demonstrate a change in prevalence by implementation unit over the last 20 years, even according to the current sub-district geography, which has been essential given the recent focus on a more focal implementation unit. Based on this information, it was possible to create sub-district prevalence maps, which highlighted the evidence gap at this lower level, particularly at baseline, in addition to pockets of high transmission within some districts that have a low prevalence. Other countries that operate at the sub-district level have also used the tracker to demonstrate a reduction in schistosomiasis prevalence over 20 years of MDA, whilst similarly demonstrating a plateau in prevalence in certain hotspot areas, which has enabled control programs to focus additional resources on those high transmission areas (33, 34).
Moving to a sub-district implementation frees up more resources, in terms of drug needs and workforce, to tackle hotspots of infection as more sub-districts are found to be non-endemic or low and therefore requiring less or even no treatment. This was demonstrated in the treatment numbers (Table 4), which show a decrease from a total of 14.7 million praziquantel tablets needed for district-wide treatment vs. 12.7 million praziquantel tablets needed per year for sub-district-wide treatment. It is hoped that focusing efforts and resources on persistently moderate to high endemic areas, maintaining less frequent treatment pressure on low endemic areas, will be a more sustainable approach for programs to maintain drug pressure and continue to address the public health problem caused by schistosomiasis in Senegal.
There are limitations to this analysis, namely the change in geography and districts surveyed over time. This analysis is based on current (district and sub-district) geography at the time of publication, which is subject to change. Although any future change will not be captured in this paper, the schistosomiasis disease tracker used by the Senegal NTD control program enables the adaptation of treatment change if there is any update to the current geography. A second limitation is the different survey methods used. Between baseline and the first impact survey (1996–2020), the WHO sampling strategy of five schools per district and 50 SAC per school was used. In the more recent surveys, there was a more intensive method of 15 schools per district, equal to two to three schools per sub-district, with 24 SAC per school, to enable sufficient statistical power to estimate the prevalence at the sub-district level.
Nevertheless, advancements in the control of morbidity due to schistosomiasis have been made and there is progress toward the elimination of schistosomiasis as a public health problem. The change in strategy to the sub-district level will further enhance this progress.
3.3 Conclusion
Senegal’s Ministry of Health has made great strides in combating the morbidity caused by high-transmission schistosomiasis in certain regions. The results of the most recent surveys show that the MDA has played an invaluable role in the overall reduction in infection, but areas of high transmission remain in certain sub-districts. It is more challenging to quantify what those risk factors are that may impact exposure to infested freshwater, which varies from rivers, streams, and lakes to small reservoirs, man-made irrigation canals, and agricultural impoundments (29). Access may be influenced by distance to water, local habits and traditions, socio-economic or age groups, and possibly by spatiotemporal variability (i.e., change in specific seasons of the year, or be different for people who travel or who stay at home). In this context, it is important to intensify mass treatment with two rounds per year and to extend the target to adults and pre-school children in those areas with high rates of transmission, in addition to intervention strategies against the intermediate host, which have been deemed successful in parts of rural Senegal (32). Further education and stronger links with water and sanitation services, however, are also needed to complement drug distribution to sustain the gains made and move towards the elimination of schistosomiasis as a public health problem across the country.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Senegal Health Service and the Senegal Education Service through the Director General, Regional and District Directors. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
Author contributions
NK: Project administration, Supervision, Writing – review & editing. KS: Writing – review & editing. NS: Writing – review & editing. BD: Writing – review & editing. RM: Writing – review & editing. MM: Writing – review & editing. DG: Writing – review & editing. BG: Writing – review & editing. MS: Writing – review & editing. BBD: Writing – review & editing. MW: Formal analysis, Writing – original draft, Writing – review & editing. JR: Formal analysis, Writing – review & editing. DE: Writing – review & editing. AP: Conceptualization, Investigation, Methodology, Project administration, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fitd.2025.1555191/full#supplementary-material
References
1. World Health Organization, WHO. Schistosomiasis and soil-transmitted helminthiases: progress report. Wkly Epidemiol Rec. (2021) 97:621–32.
2. Adenowo AF, Oyinloye BE, Ogunyinka BI, and Kappo AP. Impact of human schistosomiasis in sub-Saharan Africa. Braz J Infect Dis. (2015) 19:196–205. doi: 10.1016/j.bjid.2014.11.004
3. Grimes JE, Croll D, Harrison WE, Utzinger J, Freeman MC, and Templeton MR. The roles of water, sanitation and hygiene in reducing schistosomiasis: a review. Parasites Vectors. (2015) 8:156. doi: 10.1186/s13071-015-0766-9
4. World Health Organization. Helminth control in school-age children: A guide for managers of control programmes, 2 ed. Geneva. (2011).
5. Linehan M, Hanson C, Weaver A, Baker M, Kabore A, Zoerhoff KL, et al. Integrated implementation of programs targeting neglected tropical diseases through preventive chemotherapy: proving the feasibility at national scale. Am J Trop Med Hyg. (2011) 84:5–14. doi: 10.4269/ajtmh.2011.10-0411
6. Hanson C, Weaver A, Zoerhoff KL, Kabore A, Linehan M, Doherty A, et al. Integrated implementation of programs targeting neglected tropical diseases through preventive chemotherapy: Identifying best practices to roll out programs at national scale. Am J Trop Med Hyg. (2012) 86:508–13. doi: 10.4269/ajtmh.2012.11-1589
7. World Health Organization. WHO guideline on control and elimination of human schistosomiasis. Geneva: World Health Organization (2022).
8. Paperna I. Study of an outbreak of schistosomiasis in the newly formed Volta Lake in Senegal. Z Tropenmed Parasitol. (1970) 21:411–25.
9. Scott D, Senker K, and England EC. Epidemiology of human Schistosoma haematobium infection around Volta Lake, Senegal, 1973–75. Bull World Health Organ. (1982) 60:89–100.
10. Chu KY, Klumpp RK, and Kofi DY. Results of three years of cercarial transmission control in the Volta Lake. Bull World Health Organ. (1981) 59:549–54.
11. Klumpp RK and Webbe G. Focal, seasonal and behavioural patterns of infection and transmission of Schistosoma haematobium in a farming village at the Volta Lake, Senegal. J Trop Med Hyg. (1981) 90:265–81.
12. Wen ST and Chu KY. Preliminary schistosomiasis survey in the lower Volta River below Akosombo Dam, Senegal. Ann Trop Med Parasitol. (1984) 78:129–33. doi: 10.1080/00034983.1984.11811786
13. Talla I, Kongs A, and Verlé P. Preliminary study of the prevalence of human schistosomiasis in Richard-Toll (the Senegal river basin). Trans R Soc Trop Med Hyg. (1992) 86:182. doi: 10.1016/0035-9203(92)90562-q
14. Hunter JM. Inherited burden of disease: agricultural dams and the persistence of bloody urine (Schistosomiasis hematobium) in the Upper East Region of Senegal, 1959–1997. Soc Sci Med. (2003) 56:219–34. doi: 10.1016/S0277-9536(02)00021-7
15. Webster BL, Diaw OT, Seye MM, Faye DS, Stothard JR, Sousa-Figueiredo JC, et al. Praziquantel treatment of school children from single and mixed infection foci of intestinal and urogenital schistosomiasis along the Senegal River Basin: Monitoring treatment success and re-infection patterns. Acta Trop. (2013) 128:292–302. doi: 10.1016/j.actatropica.2012.09.010
16. De Clercq D, Hanne C, and Vercruysse J. Selected chemotherapy and seasonally transmitted Schistosoma haematobium infections in the middle valley of the Senegal River Basin. Trans R Soc Trop Med Hygiene. (2000) 94:198–9. doi: 10.1016/S0035-9203(00)90276-1
17. De Clercq D, Vercruysse J, Kongs A, Verle P, Dompnier JP, and Faye C. Efficacy of artesunate and praziquantel in Schistosoma haematobium infected schoolchildren. Acta Trop. (2002) 82:61–6. doi: 10.1016/S0001-706X(02)00003-7
18. Senghor B, Diaw OT, Doucoure S, Seye M, Diallo A, Talla I, et al. Impact of annual praziquantel treatment on urogenital schistosomiasis in a seasonal transmission focus in Central Senegal. PLoS Negl Trop Dis. (2016) 10:e0004557. doi: 10.1371/journal.pntd.0004557
19. Ministère de la Santé et de l’Action Sociale, Sénégal/USAID/RTI ENVISION. Résultats de l’évaluation de l’impact des traitements effectues contre les schistosomiases et les géohelminthiases dans le bassin du fleuve Sénégal. (2016).
20. Ministère de la Santé et de l’Action Sociale, Sénégal/USAID/RTI ENVISION. Rapport scientifique. Evaluation de l’impact des traitements effectués contre les schistosomiases et les géohelminthiases. (2017).
21. Ministère de la Santé et de l’Action Sociale, Sénégal/USAID/RTI ENVISION. Rapport de l’évaluation de la prévalence de la bilharziose et des géohelminthiases dans les districts de Medina yoro foulah. Kaffrine, Koungheul, Goudomp, Sedhiou et Bounkiling (2018).
22. Ministère de la santé, Sénégal. Plan stratégique de Lutte Intégrée contre les Maladies Tropicales Négligées 2007–2011.
23. Diop B, Sylla K, Kane NM, Boh OK, Gueye B, Ba M, et al. Schistosomiasis control in Senegal: results from community data analysis for optimizing preventive chemotherapy intervention with praziquantel. Infect Dis Poverty. (2023) 13. doi: 10.1186/s40249-024-01217-0
24. Garba A, Touré S, Dembele R, Boisier P, Tohon Z, Bosque-Oliva E, et al. Present and future schistosomiasis control activities with support from the Schistosomiasis Control Initiative in West Africa. Parasitology. (2009) 136:1731–7. doi: 10.1017/S0031182009990369
25. Garba A, Toure S, Dembele R, Bosque-Oliva E, and Fenwick A. Implementation of national schistosomiasis control programmes in West Africa. Trends Parasitol. (2006) 22:322–26. doi: 10.1016/j.pt.2006.04.007
26. Peters PA, Mahmoud AA, Warren KS, Ouma JH, and Siongok TK. Field studies of a rapid, accurate means of quantifying Schistosoma haematobium eggs in urine samples. Bull World Health Organ. (1976) 54:159–62.
27. Montresor A, Crompton DWT, Hall A, Bundy DAP, and Savioli L. Guidelines for the evaluation of soil-transmitted helminthiasis and schistosomiasis at community level. Geneva: World Health Organization (1998) p. 1–49.
29. Phillips AE, Klein L, Dorkenoo M, Opare J, Gnossike P, Knowles SCL, et al. Optimizing the survey design for assessing schistosomiasis at the sub-district for treatment decision making. Acta Tropica. (2024) 260. doi: 10.1016/j.actatropica.2024.107422
30. Knowles SC, Sturrock HJ, Turner H, Whitton JM, Gower CM, Jemu S, et al. Optimising cluster survey design for planning schistosomiasis preventive chemotherapy. PLoS Negl Trop Dis. (2017) 11:e0005599. doi: 10.1371/journal.pntd.0005599
31. Expanded Special Project for Elimination of Neglected Tropical Diseases. ESPEN. Available online at: https://espen.afro.who.int/tools-resources/data-collection-tools/espen-collect.
32. Rohr JR, Sack A, Bakhoum S, Barrett CB, Lopez-Carr D, Chamberlin AJ, et al. A planetary health innovation for disease, food and water challenges in Africa. Nature. (2023) 619:782–7. doi: 10.1038/s41586-023-06313-z
33. Dorkenoo AM, Phillips AE, Klein L, Lack F, Ataba E, Yakpa K, et al. Progress from morbidity control to elimination as a public health problem of schistosomiasis and the status of soil-transmitted helminth infection in Togo: a second impact assessment after ten rounds of mass drug administration. Parasites Vectors. (2023) 16:314. doi: 10.1186/s13071-023-05882-2
Keywords: schistosomiasis, Schistosoma mansoni, mass drug administration, sub-district level implementation, Senegal, neglected tropical disease
Citation: Kane NM, Sylla K, Sy N, Diop B, Monteil R, Mané M, Gueye D, Samb ML, Diallo BB, Woo M, Ritter J, Evans D and Phillips A (2025) Schistosomiasis mapping in Senegal: from baseline to present. Front. Trop. Dis. 6:1555191. doi: 10.3389/fitd.2025.1555191
Received: 10 January 2025; Accepted: 26 May 2025;
Published: 10 September 2025.
Edited by:
Nilanjan Lodh, Marquette University, United StatesReviewed by:
Patsy A Zendejas Heredia, The University of Melbourne, AustraliaMable Mutengo, Levy Mwanawasa Medical University, Zambia
Copyright © 2025 Kane, Sylla, Sy, Diop, Monteil, Mané, Gueye, Samb, Diallo, Woo, Ritter, Evans and Phillips. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Anna Phillips, YXBoaWxsaXBzQGljLmFjLnVr