 Mwanaisha Seugendo1
Mwanaisha Seugendo1 Iryna Janssen2Vanessa Lang2Irene Hasibuan2Wolfgang Bohne2Paul Cooper3
Iryna Janssen2Vanessa Lang2Irene Hasibuan2Wolfgang Bohne2Paul Cooper3 Rolf Daniel4Katrin Gunka2R. L. Kusumawati5
Rolf Daniel4Katrin Gunka2R. L. Kusumawati5 Stephen E. Mshana6Lutz von Müller7Benard Okamo6Jan R. Ortlepp8
Stephen E. Mshana6Lutz von Müller7Benard Okamo6Jan R. Ortlepp8 Jörg Overmann9
Jörg Overmann9 Thomas Riedel9
Thomas Riedel9 Maja Rupnik10,11Ortrud Zimmermann2
Maja Rupnik10,11Ortrud Zimmermann2 Uwe Groß2*
Uwe Groß2*- 1Department of Pediatrics and Child Health, Catholic University of Health and Allied Sciences, Mwanza, Tanzania
- 2Institute of Medical Microbiology, University Medical Center Göttingen, Göttingen, Germany
- 3St. Martin de Porres Hospital, Eikwe, Ghana
- 4Department of Genomic and Applied Microbiology, University of Göttingen, Göttingen, Germany
- 5Department of Microbiology, Faculty of Medicine, Universitas Sumatera Utara, Medan, Indonesia
- 6Department of Medical Microbiology, Catholic University of Health and Allied Sciences, Mwanza, Tanzania
- 7Institute of Medical Microbiology, Saarland University, Homburg, Germany
- 8Asklepios Kliniken Schildautal, Seesen, Germany
- 9Department Microbial Ecology and Diversity Research, Leibniz Institute DSMZ, Braunschweig, Germany
- 10Institute of Public Health Maribor, Maribor, Slovenia
- 11Faculty of Medicine, University of Maribor, Maribor, Slovenia
Clostridioides (Clostridium) difficile infections (CDI) are considered worldwide as emerging health threat. Uptake of C. difficile spores may result in asymptomatic carrier status or lead to CDI that could range from mild diarrhea, eventually developing into pseudomembranous colitis up to a toxic megacolon that often results in high mortality. Most epidemiological studies to date have been performed in middle- and high income countries. Beside others, the use of antibiotics and the composition of the microbiome have been identified as major risk factors for the development of CDI. We therefore postulate that prevalence rates of CDI and the distribution of C. difficile strains differ between geographical regions depending on the regional use of antibiotics and food habits. A total of 593 healthy control individuals and 608 patients suffering from diarrhea in communities in Germany, Ghana, Tanzania and Indonesia were selected for a comparative multi-center cross-sectional study. The study populations were screened for the presence of C. difficile in stool samples. Cultured C. difficile strains (n = 84) were further subtyped and characterized using PCR-ribotyping, determination of toxin production, and antibiotic susceptibility testing. Prevalence rates of C. difficile varied widely between the countries. Whereas high prevalence rates were observed in symptomatic patients living in Germany and Indonesia (24.0 and 14.7%), patients from Ghana and Tanzania showed low detection rates (4.5 and 6.4%). Differences were also obvious for ribotype distribution and toxin repertoires. Toxin A+/B+ ribotypes 001/072 and 078 predominated in Germany, whereas most strains isolated from Indonesian patients belonged to toxin A+/B+ ribotype SLO160 and toxin A-/B+ ribotype 017. With 42.9–73.3%, non-toxigenic strains were most abundant in Africa, but were also found in Indonesia at a rate of 18.2%. All isolates were susceptible to vancomycin and metronidazole. Mirroring the antibiotic use, however, moxifloxacin resistance was absent in African C. difficile isolates but present in Indonesian (24.2%) and German ones (65.5%). This study showed that CDI is a global health threat with geographically different prevalence rates which might reflect distinct use of antibiotics. Significant differences for distributions of ribotypes, toxin production, and antibiotic susceptibilities were observed.
Introduction
Clostridioides (Clostridium) difficile infections (CDI) have become an emerging health threat; more than 450,000 cases with approximately 30,000 deaths have been estimated to occur every year in the USA alone (Lessa et al., 2015). Infections with this pathogen may stay asymptomatic or range from mild diarrhea up to pseudomembranous colitis or even develop into life-threatening toxic megacolon (Rupnik et al., 2009). Based on its impact on health systems, C. difficile has been prioritized as pathogen of the highest priority group for surveillance and epidemiological research (Balabanova et al., 2011). It is generally believed that only toxigenic strains cause disease with toxin B (TcdB) being most important for virulence. The majority of virulent strains produce toxin A (TcdA) and toxin B (TcdB) simultaneously. Some strains also produce a binary toxin (CDT), either together with TcdA and TcdB or alone (Eckert et al., 2015). Strains with modifications in the toxin A and B coding region, the so-called pathogenicity locus (PaLoc), compared to the well-characterized reference strain VPI 10463, are defined as variant strains. They can be differentiated by toxinotyping, a PCR-restriction fragment length polymorphism (RFLP)-based method (Rupnik and Janezic, 2016). However, for epidemiological purposes, classification of C. difficile strains is currently mainly achieved by PCR ribotyping (Wilcox, 2012). Based on phylogenetic analysis eight clades are currently distinguished, and comprise non-toxigenic (PaLoc absent) strains and clades with representative ribotypes for each (Knight et al., 2015). Most epidemiological studies to date have been performed in middle- and high income countries, especially in North-America, Europe, Australia, and to a lesser extend in Asia (Burke and Lamont, 2014). Only very limited data are available from Africa. We therefore previously performed prospective cross-sectional studies in Ghana and Tanzania, which indicated a high prevalence of non-toxigenic strains in sub-Saharan Africa (Seugendo et al., 2015; Janssen et al., 2016). Using the identical study design we also investigated prevalence rates of C. difficile-positive individuals in Medan/Indonesia and Seesen/Germany in the similar time period as in Ghana and Tanzania and performed further characterization of the obtained isolates. The aim of this article is to compare the data obtained from Indonesia and Germany with the previously published data from Ghana and Tanzania and to present this multi-center prospective study as a whole in order to compare prevalence rates, strain distribution and characterization of C. difficile in these four distinct geographical regions.
Materials and Methods
Study Design
The four studies to be compared here were performed during the time period of September 2013 to October 2014 in the St. Martin de Porres Hospital in Eikwe/rural Ghana (Janssen et al., 2016), the Bugando Medical Center and Sekou Toure Regional Hospital in Mwanza/urban Tanzania (Seugendo et al., 2015), the Adam Malik Hospital and Pematang Siantar Hospital in Medan/urban Indonesia, and the Asklepios Hospital Schildautal in Seesen/rural Germany. This study was carried out in accordance with the recommendations of the guidelines set by the University Medical Center Göttingen. The protocol was approved by the Ethical Committees responsible for the participating hospitals and the University Medical Center, Göttingen, Germany (29/3/11). All subjects gave written informed consent in accordance with the Declaration of Helsinki. The participants were classified into two groups; those with diarrhea (symptomatic group) and a non-diarrheic control group, consisting of patients, relatives of the patients without diarrhea or employees of the respective hospitals. Following informed consent, all participants of the study submitted a stool sample that was directly examined for the presence of C. difficile at the local laboratory. All examiners were trained beforehand in bacterial identification at the Institute of Medical Microbiology of the University Medical Center Göttingen, Germany.
Microbiological Analysis
Stool samples were cultured on C. difficile selective agar (bioMérieux, Marcy-l’Étoile, France) or chromogenic agar (CHROMagar, Paris, France) and incubated for up to 48 h in an anaerobic jar, using anaerobic packs (bioMérieux). At least five grown C. difficile colonies were isolated on COS Columbia blood agar, enriched with 5% sheep blood (bioMérieux) and stored in a microbank system (bestbion dx GmbH, Cologne, Germany) until further analysis (e.g., identification by MALDI-TOF mass spectrometry, toxin and sensitivity test) in Göttingen, Germany.
Clostridium difficile identification was verified by MALDI-TOF mass spectrometry (Biotyper, Bruker Daltonics, Bremen, Germany) with score values ≥ 2000. Susceptibility of C. difficile isolates to macrolides (erythromycin or clarithromycin), moxifloxacin, metronidazole, and vancomycin was determined with Etest® (bioMérieux) according to standard protocols. Briefly, bacterial isolates were cultured in BHI broth (BD Difco Fraser Broth Supplement, Heidelberg, Germany), adjusted with 0.5% yeast extract and 0.03% L-cysteine and incubated in an anaerobic chamber (Coy Laboratory Products, Michigan, United States) with an atmosphere of 5% CO2, 5% H2, and 90% N2. Bacterial cells were diluted using 0.9% saline to McFarland standard 1 and streaked onto Mueller-Hinton agar supplemented with 5% horse blood + 20 mg/l β-NAD+ (bioMérieux). Reproducibility was ensured by inclusion of the control strains C. difficile 630 (DSMZ-27543, Leibniz Institute DSMZ, Braunschweig, Germany) and C. difficile R 20291 (DSM-27147, Leibniz Institute DSMZ, Braunschweig, Germany). After two days of incubation with Etest® strips (bioMérieux), the minimal inhibitory concentrations (MIC) were determined. Toxin production was investigated using the Serazym® C. difficile toxin A+B immunoassay (Seramun Dianostica GmbH, Heidesee, Germany) or Quik Chek Complete (Alere Techlab, Blacksburg, VA, United States). Furthermore, isolates were specified by multiplex PCR to detect toxin gene profiles (Stahlmann et al., 2014) and PCR ribotyped by agarose (isolates from Ghana and Indonesia) or capillary gel electrophoresis (isolates from Germany and Tanzania) according to consensus protocols (CDRN, ECDIS-Net) as previously described (Janezic and Rupnik, 2010; Fawley et al., 2016; van Dorp et al., 2016; Berger et al., 2018).
Results
Prevalence Rates of C. difficile Carriage
This multi-center, cross-sectional study covers a total of 1,201 participants, 608 inpatients with diarrhea and 593 controls. Prevalence rates of C. difficile carriage were highest in the participants from the German and the Indonesian study sites compared with the two African study sites (Table 1).
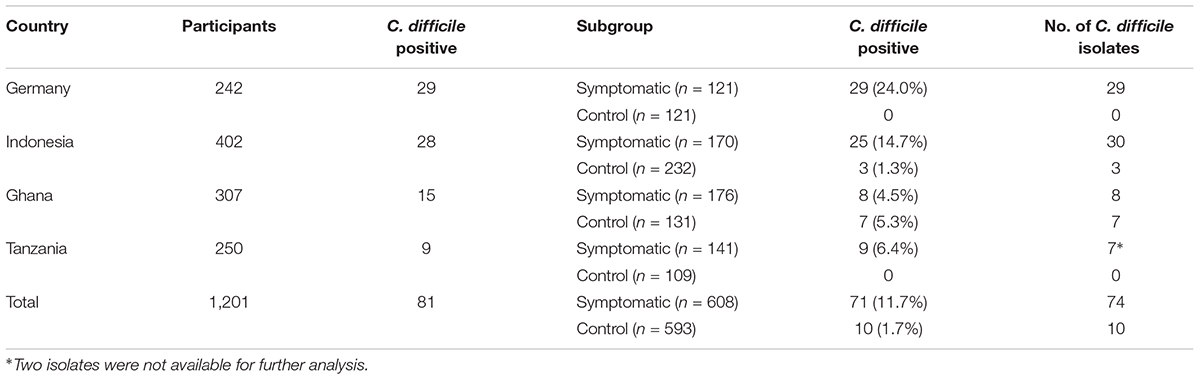
TABLE 1. Prevalence rates of C. difficile in the different study sites.
In fact, C. difficile was only found in symptomatic patients but not in asymptomatic controls in the German study site. The mean age of C. difficile-positive patients was 73.5 years in comparison to 68.7 years in the C. difficile-negative group. Similarly, C. difficile was nearly exclusively recovered only from symptomatic patients in Indonesia. In contrast to the situation in Germany, 50% of C. difficile-positive and 21.4% of C. difficile-negative participants in Indonesia were children younger than 6 years of age.
Like in Seesen/Germany, C. difficile was only found in symptomatic patients in the Tanzanian study site but not in the healthy control group. 48.9% of Tanzanian patients with diarrhea were children 12 years of age or younger and five out of seven C. difficile isolates were recovered from children (Seugendo et al., 2015). Whereas a clear difference in prevalence rates between symptomatic patients and healthy controls was found in the above-mentioned three study sites, nearly equal colonization rates were found in symptomatic and asymptomatic participants from the Ghanaian study site. Here, the majority of C. difficile-positive asymptomatic controls were children aged 0–5 years, whereas the majority of C. difficile-positive symptomatic patients aged 16–45 years (Janssen et al., 2016).
Ribotypes of C. difficile Isolates
Further characterization of bacterial isolates revealed the presence of mixed infections with at least two different C. difficile strains only in symptomatic patients from the Indonesian study site, but not in any of the other three study sites. A total of six different ribotypes were present amongst the German C. difficile isolates with ribotype 001/072 dominating (62.1%, n = 18/29). In contrast, a broad variation of 14 different ribotypes was identified in Indonesia with SLO160 (27.3%, n = 9/33) and ribotype 017 (18.2%, n = 6/33) being most prevalent (Figure 1). In the Ghanaian study site, ribotype 084 was most prevalent (40.0%, n = 6/15) and several new ribotypes were identified amongst the total number of nine ribotypes (Janssen et al., 2016). In contrast, only three different ribotypes were present in the Tanzanian C. difficile isolates (Seugendo et al., 2015; Figure 1).
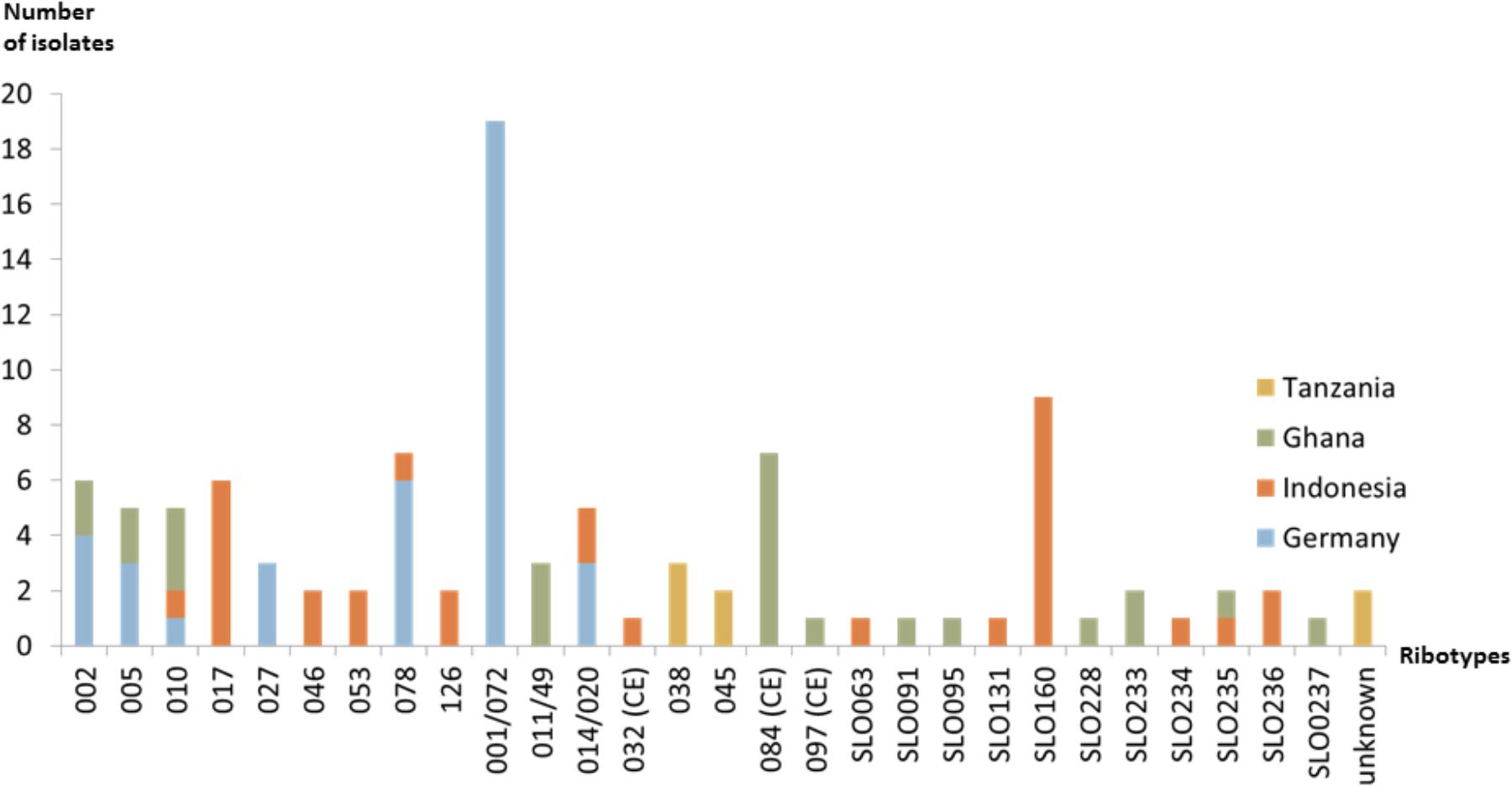
FIGURE 1. Ribotype distribution of C. difficile in the different study sites.
Characterization of Toxinotypes
As expected, all C. difficile isolates recovered from German patients either produced the two major toxins alone (TcdA+/TcdB+; 86.2%, n = 25/29) or together with the binary toxin CDT (TcdA+/TcdB+/CDT+; 13.8%, n = 4/29). Like in Germany, the majority of C. difficile from Indonesia (63.6%, n = 21/33) was TcdA+/TcdB+; all six ribotype 017 isolates (18.2%) were TcdA-/TcdB+, and the remaining six isolates (18.2%) were non-toxigenic (Figure 2). In contrast to the situation in Germany and Indonesia, a rather large ratio of African C. difficile isolates were non-toxigenic; 73.3% (n = 11/15) of the strains isolated in Ghanaian study participants and 42.9% (n = 3/7) of the strains recovered from Tanzanian patients (Seugendo et al., 2015; Janssen et al., 2016). In addition, one isolate from Ghana was only positive for CDT (TcdA-/TcdB-/CDT+) and two isolates from Tanzania expressed all toxins (TcdA+/TcdB+/CDT+, Figure 2).
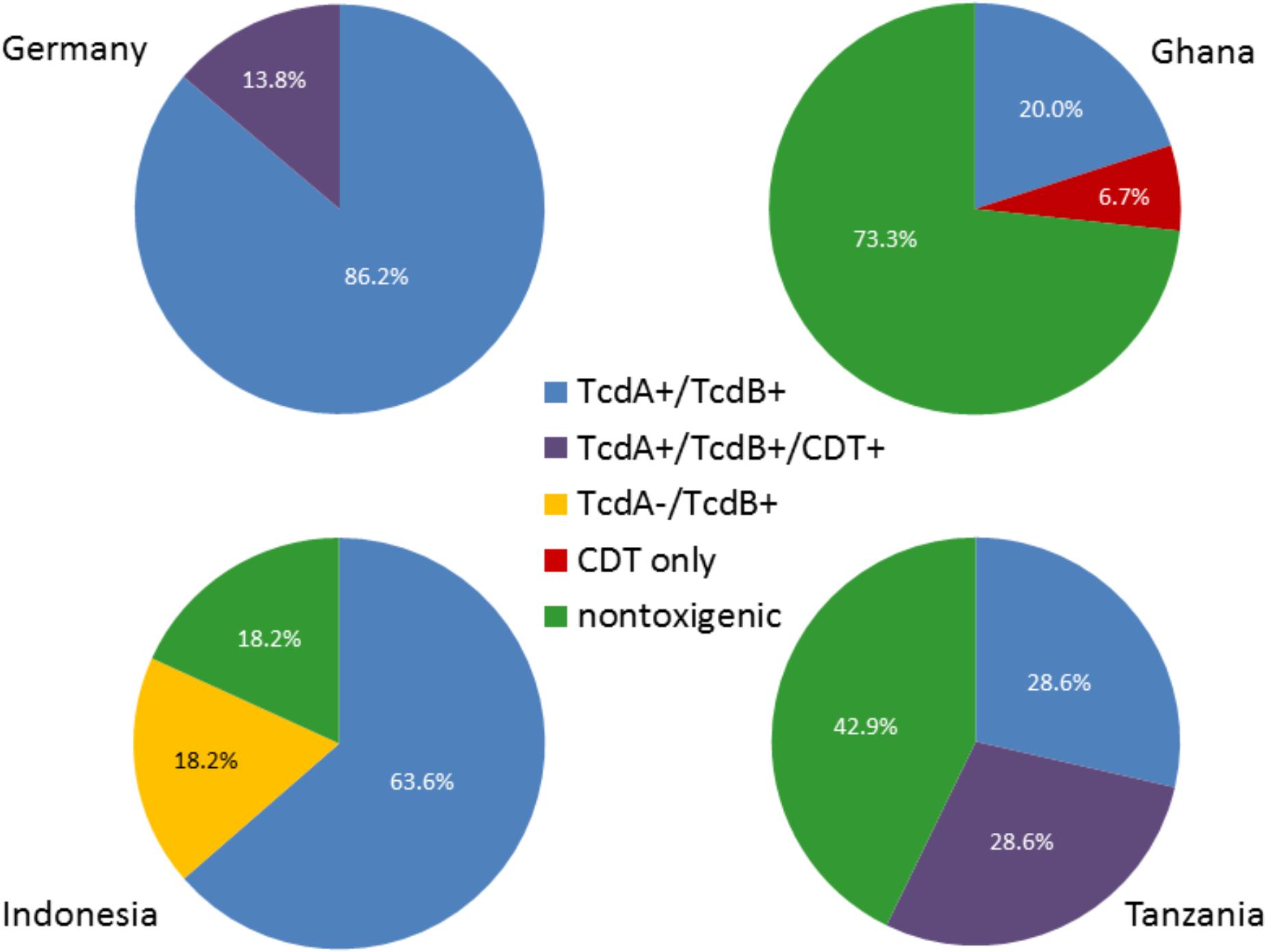
FIGURE 2. Distribution of toxinotypes in the four study sites. Percent of total numbers for the different toxinotypes in the study regions are shown. Note that rounding of percentages given for isolates from Tanzania resulted in > 100%.
Antibiotic Susceptibility
All isolates were susceptible to metronidazole and vancomycin. The majority of 75.9% (n = 22/29) of C. difficile isolates from German patients was resistant against the macrolide erythromycin and belonged to ribotypes 001/072 (n = 17/18), 027 (n = 1/1), and 078 (n = 3/3). In contrast, only 15.2% (n = 5/33) of the isolates from Indonesia and 8/15 (53.3%) isolates from Ghana were resistant against erythromycin, including all isolates of ribotype 084 and with nearly equal distribution between symptomatic patients and asymptomatic controls (Table 2; Janssen et al., 2016). With 42.9% (n = 3/7), a similar resistance rate against the macrolide clarithromycin was found in Tanzania (Seugendo et al., 2015). With 65.5% (n = 19/29), an unexpectedly high percentage of the isolates from the German study site was resistant against moxifloxacin consisting of strains belonging to 001/072 (n = 15/18), 027 (n = 1/1), and 078 (n = 3/3). In Indonesia, only 24.2% (n = 8/33) of the isolates showed moxifloxacin resistance consisting mainly of ribotype 017 strains (n = 5/6). Moxifloxacin resistance was neither identified in Ghana nor in Tanzania.
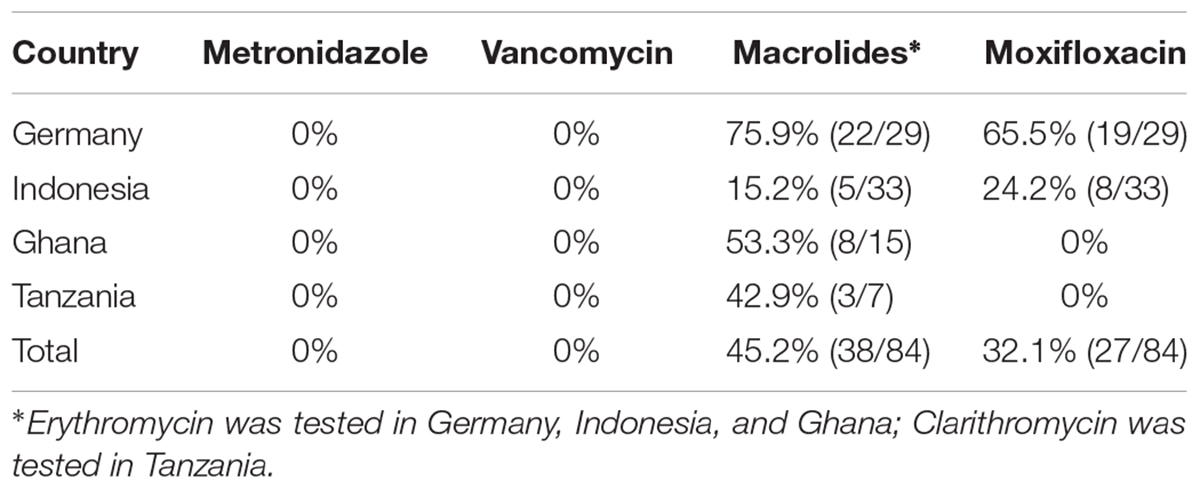
TABLE 2. Antimicrobial resistance rates of C. difficile isolated in the different study sites.
Discussion
Analysing a total of 1,201 inpatients with diarrhea (n = 608) and a control group without diarrhea (n = 593) in this cross-sectional multi-center study performed in a rural area of Germany and an urban area in Indonesia, and including the recently published results from a rural area of Ghana and an urban area of Tanzania (Seugendo et al., 2015; Janssen et al., 2016), we identified C. difficile as a likely cause of diarrhea at varying prevalence rates. Whereas C. difficile was present in 24 and 15% of patients suffering from diarrhea in Germany and Indonesia, respectively, this rate was significantly lower in African patients (5–6%). In addition, 1 and 5% of asymptomatic control participants from Indonesia and Ghana, respectively, were also colonized. Although age has been identified as important risk factor for colonization, C. difficile could neither be detected in asymptomatic control participants from Germany nor from Tanzania although most study participants from Germany were significantly older than those in Tanzania. Likewise, in contrast to the three other study sites more diarrheal patients from Germany underwent complex medical treatments and might have been prone to get hospital-acquired complications such as antibiotic-associated diarrhea caused by C. difficile.
Other studies revealed asymptomatic carriage rates ranging from 5–51%, which was only present in the Ghanaian, but also not in the Indonesian asymptomatic control groups (Ryan et al., 2010; Arvand et al., 2012; Alasmari et al., 2014; Galdys et al., 2014). In the Ghanaian control group, nearly all C. difficile-positive individuals (6/7) were colonized with non-toxigenic bacteria, which to date are considered to be non-pathogenic. On one hand, the finding that colonization was absent or a rather rare finding in our four cohorts could be attributed to the fact that our sample size was relatively small and hence the asymptomatic carriage might be underestimated. On the other hand the genesis of asymptomatic carriage remains still unclear. The different prevalence rates could also be attributed to patient-related factors, e.g., antibiotic consumption, the intestinal microbiome or nutritional habits. Recent data from Switzerland support the suggestion that asymptomatic carriage seems not to play an important role in nosocomial transmission (Pires et al., 2016).
The average age of the symptomatic C. difficile-positive patients varied significantly between the study sites and partly contradicted previous studies. It is widely known that advanced age and its consecutive comorbidities is one of the most important risk factors for CDI (Rupnik et al., 2009; Bauer et al., 2011; Leffler and Lamont, 2015). Indeed, in both Germany and Ghana the majority of C. difficile-positive patients were adults. In contrast, most patients were at child age in both Indonesia and Tanzania. A sampling bias seems to be a rather unlikely explanation for our finding because the study design, time of sampling, and microbiological methodology was identical at all study sites. Nutrition status or habits as main explanation for the age difference is unlikely, because age between C. difficile-positive patients differs significantly between the two African study sites. Whether C. difficile is affecting adults more in rural (German and Ghanaian study sites) and children more in urban environments (Indonesian and Tanzanian study sites) awaits further investigation. Data from a European surveillance study make this explanation unlikely (Bauer et al., 2011).
As it has been shown by others, the most frequently isolated ribotype in Germany was 001/072 followed by 078 (Freeman et al., 2015). In contrast, ribotype 017 was most frequently recovered from C. difficile-positive symptomatic patients in Indonesia. This ribotype has also been shown previously to be the most prevalent one in several Asian countries (Burke and Lamont, 2014; Knight et al., 2015). The fact that ribotype 017 C. difficile strains produce only TcdB has a direct impact on diagnosis of travelers or migrants from Asian countries because a false-negative status would result from toxin tests that exclusively detect TcdA only. The same is true for non-toxigenic C. difficile isolates; whereas 18.2% of isolates from Indonesian participants were non-toxigenic, the majority of C. difficile isolates from Ghanaian and Tanzanian patients and control participants were non-toxigenic. Although pathogenicity of C. difficile currently relies on the presence of toxins, the high prevalence of non-toxigenic isolates in Ghana, Tanzania, as well as in Indonesia awaits further investigation. Hypervirulent ribotypes 027 and 078 were only identified in a small number of patients from Germany and one patient from Indonesia, indicating that they seem to play no distinct role in our cohort of patients.
Our finding of metronidazole and vancomycin susceptibility of all C. difficile isolates, irrespective of origin are in line with the results of other studies, such as e.g., the European Surveillance Study (Freeman et al., 2015). In contrast to this European Surveillance Study with a moxifloxacin resistance of 48.8% for C. difficile strains from Germany, however, we found a high rate of moxifloxacin resistant strains (65.5%, mostly of the epidemic ribotype 001/072). This is in the range of an investigation of 34 C. difficile strains from Southern Germany that revealed a moxifloxacin resistance rate of 67.6% including 80% of tested ribotype 001/072 strains (Reil et al., 2012). The fact that the rate of moxifloxacin-resistant C. difficile isolates in Indonesia was significantly lower and resistance against this fluoroquinolone was even absent in the African study sites might mirror antibiotic consumption; whereas moxifloxacin has been introduced in Germany in 1999 and much later in Indonesia, it is still not available at the two African study sites (Brunner, 1999).
Conclusion
This international multi-center study indicates that CDI and C. difficile colonization is a global health threat with geographically different prevalence rates that might reflect distinct use of antibiotics. Diagnosis should rely on glutamate-dehydrogenase testing to identify the presence of C. difficile and a test for determining at least TcdB production to identify toxigenic isolates.
Author Contributions
UG had the initial idea which was developed in a project together with PC, RLK, SM, JRO, and OZ. MS, IJ, VL, IH, KG, and BO collected the samples and performed the microbiological analyses and together with OZ, WB, and UG interpreted the results. LM and MR determined ribotypes and toxinotypes. All authors wrote the manuscript and read and approved the final version.
Funding
This work was funded by the Federal State of Lower Saxony, Niedersächsisches Vorab (VWZN2889/3215). The Open Access Support Program of the Deutsche Forschungsgemeinschaft and the publication fund of the Georg-August-Universität Göttingen funded publication of this paper.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We thank the patients and healthy control individuals for their participation in this study.
References
Alasmari, F., Seiler, S. M., Hink, T., Burnham, C. A. D., and Dubberke, E. R. (2014). Prevalence and risk factors for asymptomatic Clostridium difficile carriage. Clin. Infect. Dis. 59, 216–222. doi: 10.1093/cid/ciu258
Arvand, M., Moser, V., Schwehn, C., Bettge-Weller, G., Hensgens, M. P., and Kuijper, E. J. (2012). High prevalence of Clostridium difficile colonization among nursing home residents in Hesse. Germany. PLoS One 7:e30183. doi: 10.1371/journal.pone.0030183
Balabanova, Y., Gilsdorf, A., Buda, S., Burger, R., Eckmanns, T., Gärtner, B., et al. (2011). Communicable diseases prioritized for surveillance and epidemiological research: results of a standardized prioritization procedure in Germany, 2011. PLoS One 6:e25691. doi: 10.1371/journal.pone.0025691
Bauer, M. P., Notermans, D. W., van Benthem, B. H. B., Brazier, J. S., Wilcox, M. H., Rupnik, M., et al. (2011). Clostridium difficile infection in Europe: a hospital-based survey. Lancet 377, 63–73. doi: 10.1016/S0140-6736(10)61266-4
Berger, F. K., Rasheed, S. S., Araj, G. F., Mahfouz, R., Rimmani, H. H., Karaoui, W. R., et al. (2018). Molecular characterization, toxin detection and resistance testing of human clinical Clostridium difficile isolates from Lebanon. Int. J. Med. Microbiol. 308, 358–363. doi: 10.1016/j.ijmm.2018.01.004
Brunner, U. (1999). Moxifloxacin ab September auf dem Markt. Pharmazeutische Zeitung online 34/1999 (accessed 30 May 2018).
Burke, K. E., and Lamont, J. T. (2014). Clostridium difficile infection: a worldwide disease. Gut Liver 8, 1–6. doi: 10.5009/gnl.2014.8.1.1
Eckert, C., Emirian, A., Le Monnier, A., Cathala, L., De Montclos, H., Goret, J., et al. (2015). Prevalence and pathogenicity of binary toxin–positive Clostridium difficile strains that do not produce toxins A and B. New Microbes New Infect. 3, 12–17. doi: 10.1016/j.nmni.2014.10.003
Fawley, W. N., Davies, K. A., Morris, T., Parnell, P., Howe, R., and Wilcox, M. H. (2016). Enhanced surveillance of Clostridium difficile infection occurring outside hospital, England, 2011 to 2013. Euro Surveill. 21:30295. doi: 10.2807/1560-7917.ES.2016.21.29.30295
Freeman, J., Vernon, J., Morris, K., Nicholson, S., Todhunter, S., Longshaw, C., et al. (2015). Pan-European longitudinal surveillance of antibiotic resistance among prevalent Clostridium difficile ribotypes. Clin. Microbiol. Infect. 21, 248.e9–248.e16. doi: 10.1016/j.cmi.2014.09.017
Galdys, A. L., Nelson, J. S., Shutt, K. A., Schlackman, J. L., Pakstis, D. L., Pasculle, A. W., et al. (2014). Prevalence and duration of asymptomatic Clostridium difficile carriage among healthy subjects in Pittsburgh, Pennsylvania. J. Clin. Microbiol. 52, 2406–2409. doi: 10.1128/JCM.00222-14
Janezic, S., and Rupnik, M. (2010). Molecular typing methods for Clostridium difficile: pulsed-field gel electrophoresis and PCR ribotyping. Methods Mol. Biol. 646, 55–65. doi: 10.1007/978-1-60327-365-7_4
Janssen, I., Cooper, P., Gunka, K., Rupnik, M., Wetzel, D., Zimmermann, O., et al. (2016). High prevalence of nontoxigenic Clostridium difficile isolated from hospitalized and non-hospitalized individuals in rural Ghana. Int. J. Med. Microbiol. 306, 652–656. doi: 10.1016/j.ijmm.2016.09.004
Knight, D. R., Elliott, B., Chang, B. J., Perkins, T. T., and Riley, T. V. (2015). Diversity and evolution in the genome of Clostridium difficile. Clin. Microbiol. Rev. 28, 721–741. doi: 10.1128/CMR.00127-14
Leffler, D. A., and Lamont, J. T. (2015). Clostridium difficile infection. N. Engl. J. Med. 372, 1539–1548. doi: 10.1056/NEJMra1403772
Leesa, F. C., Mu, Y., Bamberg, W. M., Beldavs, Z. G., Dumyati, G. K., Dunn, J. R., et al. (2015). Burden of Clostridium difficile infection in the United States. N. Engl. J. Med. 372, 825–834. doi: 10.1056/NEJMoa1408913
Pires, D., Prendki, V., Renzi, G., Fankhauser, C., Sauvan, V., Huttner, B., et al. (2016). Low frequency of asymptomatic carriage of toxigenic Clostridium difficile in an acute care geriatric hospital: prospective cohort study in Switzerland. Antimicrob. Resist. Infect. Control 5:24. doi: 10.1186/s13756-016-0123-6
Reil, M., Hensgens, M. P. M., Kuijper, E. J., Jakobiak, T., Gruber, H., Kist, M., et al. (2012). Seasonality of Clostridium difficile infections in Southern Germany. Epidemiol. Infect. 140, 1787–1793. doi: 10.1017/S0950268811002627
Rupnik, M., and Janezic, S. (2016). An update on Clostridium difficile toxinotyping. J. Clin. Microbiol. 54, 13–18. doi: 10.1128/JCM.02083-15
Rupnik, M., Wilcox, M. H., and Gerding, D. N. (2009). Clostridium difficile infection: new developments in epidemiology and pathogenesis. Nat. Rev. Microbiol. 7, 526–536. doi: 10.1038/nrmicro2164
Ryan, J., Murphy, C., Twomey, C., Paul Ross, R., Rea, M. C., MacSharry, J., et al. (2010). Asymptomatic carriage of Clostridium difficile in an Irish continuing care institution for the elderly: prevalence and characteristics. Ir. J. Med. Sci. 179, 245–250. doi: 10.1007/s11845-009-0361-1
Seugendo, M., Mshana, S. E., Hokororo, A., Okamo, B., Mirambo, M. M., von Müller, L., et al. (2015). Clostridium difficile infections among adults and children in Mwanza/Tanzania: is it an underappreciated pathogen among immunocompromised patients in sub-Saharan Africa? New Microbes New Infect. 8, 99–102. doi: 10.1016/j.nmni.2015.09.016
Stahlmann, J., Schönberg, M., Herrmann, M., and von Müller, L. (2014). Detection of nosocomial Clostridium difficile infections with toxigenic strains despite negative toxin A and B testing on stool samples. Clin. Microbiol. Infect. 20, 590–592. doi: 10.1111/1469-0691.12558
van Dorp, S. M., Kinross, P., Gastmeier, P., Behnke, M., Kola, A., Delmée, M., et al. (2016). Standardised surveillance of Clostridium difficile infection in European acute care hospitals: a pilot study, 2013. Euro Surveill. 21:30293. doi: 10.2807/1560-7917.ES.2016.21.29.30293
Keywords: Clostridioides difficile, epidemiology, Germany, Indonesia, Africa, multi-center study, ribotype, toxinotype
Citation: Seugendo M, Janssen I, Lang V, Hasibuan I, Bohne W, Cooper P, Daniel R, Gunka K, Kusumawati RL, Mshana SE, von Müller L, Okamo B, Ortlepp JR, Overmann J, Riedel T, Rupnik M, Zimmermann O and Groß U (2018) Prevalence and Strain Characterization of Clostridioides (Clostridium) difficile in Representative Regions of Germany, Ghana, Tanzania and Indonesia – A Comparative Multi-Center Cross-Sectional Study. Front. Microbiol. 9:1843. doi: 10.3389/fmicb.2018.01843
Received: 31 May 2018; Accepted: 24 July 2018;
Published: 07 August 2018.
Edited by:
George Grant, University of Aberdeen, United KingdomReviewed by:
Richard Vernon Goering, Creighton University School of Medicine, United StatesThandavarayan Ramamurthy, Translational Health Science and Technology Institute, India
Copyright © 2018 Seugendo, Janssen, Lang, Hasibuan, Bohne, Cooper, Daniel, Gunka, Kusumawati, Mshana, von Müller, Okamo, Ortlepp, Overmann, Riedel, Rupnik, Zimmermann and Groß. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Uwe Groß, dWdyb3NzQGd3ZGcuZGU=