 Maria Gisele Gonçalves*
Maria Gisele Gonçalves* Lucila Okuyama Fukasawa
Lucila Okuyama Fukasawa Karoline Rodrigues Campos
Karoline Rodrigues Campos Fábio Takenori Higa
Fábio Takenori Higa Adele Caterino-de-Araujo*
Adele Caterino-de-Araujo*- Centro de Imunologia, Instituto Adolfo Lutz, Coordenadoria de Controle de Doenças, Secretaria de Estado da Saúde de São Paulo, São Paulo, Brazil
Brazil currently has the highest number of individuals infected with human T-lymphotropic virus 1- and 2- (HTLV-1 and HTLV-2) globally. At present, neither molecular protocols nor commercial assays are available for HTLV-1/-2 diagnosis or validated by the Brazilian Ministry of Health regulatory agency (ANVISA). We developed and validated two in-house multiplex quantitative real-time PCR for HTLV-1/-2 (mqPCR_HTLV) assays, targeting the pol and tax genes, for the simultaneous identification of HTLV-1, HTLV-2, and the albumin reference gene. The robustness of the assays was evaluated on two platforms using seven commercial master mix formulations. The reactions employed double plasmids (pHTLV1-Alb and pHTLV2-Alb) for the standard curve’s construction and for expressing the detection limit of the assays. They were able to detect 10 and 10 copies of HTLV-1 and 10 and 70 copies of HTLV-2 for the tax and pol targets, respectively. High efficiency was obtained using both the platforms and all the reagents evaluated and were successfully reproduced by other analysts. DNA samples from HTLV-1/-2-infected and non-infected patients and from HIV/HTLV-coinfected patients were evaluated to determine the feasibility of their use in routine diagnosis. The mqPCR_HTLV (pol and tax) assays demonstrated an overall specificity of 100% and a sensitivity of 97.4% when testing samples from patients without HIV infection, and sensitivities of 77.1% (pol) and 74.6% (tax) in samples from HIV/HTLV-coinfected patients. In addition, they resolved the issue of HTLV western blotting (WB) indeterminate and WB-untyped results in 45.5 and 66.7% of cases, respectively. The developed mqPCR_HTLV (pol and tax) assays indicated their feasibility for efficient and reliable HTLV diagnosis in various core facility laboratories under different conditions and supplies.
Introduction
Human T-lymphotropic virus 1 and 2 (HTLV-1 and HTLV-2) are endemic to Brazil and their distribution varies according to the ethnic background of individuals and geographic regions (CGIST/DDCI/SVS et al., 2020). Brazil has the highest number of HTLV-1/2-infected individuals in Latin America and worldwide (Gessain and Cassar, 2012; CGIST/DDCI/SVS et al., 2020). Although the majority of the individuals remain asymptomatic, many people living with HTLV may develop one or more of a range of related diseases (Haziot et al., 2019; Rosadas et al., 2021a). At least two diseases of high morbidity and mortality rates are associated with HTLV-1, including HTLV-1-associated myelopathy (HAM) and adult T-cell leukemia/lymphoma (ATL), while HTLV-2 is rarely associated with a disease (Paiva and Casseb, 2015; Rosadas et al., 2021a). Thus, it is important to perform confirmatory and discriminatory diagnosis of HTLV-1/2 infections. There is no curative treatment available for these infections, therefore preventive measures, which include correct diagnosis, are the only means to eliminate HTLV transmission (Rosadas et al., 2021b).
The laboratory diagnosis of HTLV-1 and -2 is performed on blood samples from patients using screening tests followed by confirmatory tests. The screening tests detect antibodies against HTLV-1/2 in plasma/serum samples; they have high sensitivities, and negative results exclude HTLV-1/2 infection (da Silva Brito et al., 2018; Caterino-de-Araujo et al., 2021). The most common screening tests are the particle agglutination (PA), enzyme immunoassays (EIA or ELISA), and chemiluminescence immunoassays (CLIA) (Okuma et al., 2020; Caterino-de-Araujo et al., 2021; Rosadas et al., 2021a). Confirmatory serologic tests identify antibodies specific for HTLV-1 and -2 antigens in plasma/serum samples, and the most common types of these tests are western blotting (WB) and the line immunoassay (LIA). Both these serologic confirmatory assays help in diagnosis, but in some cases, inconclusive results may occur (HTLV untyped and indeterminate), especially when samples obtained from patients with HTLV-2 infection and those from patients coinfected with HIV, and/or HBV, and/or HCV (Campos et al., 2017a,b, 2020; Caterino-de-Araujo et al., 2021) are tested. LIA has a greater accuracy in comparison to WB for the confirmation of HTLV-1 and -2 infection (Campos et al., 2020; Okuma et al., 2020), but in cases of LIA- or WB-indeterminate and untyped results, molecular assays that amplify segments of the proviral DNA present in the HTLV-infected cells samples, must be conducted (Caterino-de-Araujo et al., 2021; Rosadas et al., 2021a). These molecular tests are based on polymerase chain reaction (PCR) in various formats: nested PCR (n-PCR), PCR followed by restriction fragment polymorphism analysis (PCR-RFLP), real-time quantitative PCR (qPCR), and loop-mediated isothermal amplification (LAMP) (Gomes et al., 2020; Caterino-de-Araujo et al., 2021; Rosadas et al., 2021a).
The HTLV Brazilian Protocol for Sexually Transmitted Infections 2020 recommends performing WB or LIA as the first confirmatory assay, and in case of inconclusive results conducting a PCR for confirmation (Rosadas et al., 2021a). However, at present, neither molecular protocols nor commercial molecular assays for HTLV-1/-2 diagnosis are commercially available in Brazil or validated by the Brazilian Ministry of Health regulatory agency (ANVISA). The molecular tests used in Brazil have been developed in-house and most of them have not been validated. This makes the implementation of routine molecular testing and the comparison of results from different laboratories difficult.
Since 1992, the Instituto Adolfo Lutz (IAL) Central Public Health Laboratory in São Paulo, Brazil, has been conducting studies on HTLV-1 and -2 infections, and has performed HTLV serology routinely since 1998. At this laboratory, we searched for the best assays and algorithms that could be used for testing in São Paulo and Brazil in general, based on performance and cost-effectiveness. During these years we had the opportunity to use WB (several trademarks and versions), LIA, n-PCR (env, tax, LTR), PCR-RFLP (env, tax), and qPCR (pol) as confirmatory assays (de-Araujo et al., 1994; Caterino-de-Araujo et al., 1998, 2014, 2015; Jacob et al., 2007, 2008; Morimoto et al., 2007; Costa et al., 2011; Campos et al., 2017a,b, 2020), and it was concluded that laboratories without appropriate infrastructure for molecular biology studies could confirm infection using LIA instead of WB (Campos et al., 2020). For laboratories that had the appropriate infrastructure and supplies to perform both the confirmatory tests (serological and molecular), molecular tests should be first-line test used, considering the better cost/benefit ratio (Caterino-de-Araujo et al., 2021). Of all the molecular confirmatory assays, qPCR has the advantage of quantifying the HTLV-1/2 proviral load (PVL), and consequently, stratifying the risk of HTLV-1-associated disease development (Haziot et al., 2019; Rosadas et al., 2021a).
A study of the literature published regarding the molecular assays for the diagnosis of HTLV-1/2, particularly in Brazil, revealed the differences in PCR protocols among laboratories, regions of the proviral DNA amplification, primer pairs and probes, PCR platforms and reagents, and criteria of positivity (Caterino-de-Araujo and Gonçalves, 2021).
In light of this scenario, and considering the exorbitant expenses on reagents, the shortage of clinical specimens, the different qPCR platforms, and the supplies available in each Central Public Health Laboratory in Brazil, we decided to develop and validate two in-house multiplex quantitative real-time PCR assays (mqPCR_HTLV), targeting the pol and tax genes, for the simultaneous identification of HTLV-1, HTLV-2, and the human albumin reference gene using double plasmids (pHTLV1-Alb and pHTLV2-Alb) for the standard curve construction. We used two platforms and seven commercial master mix formulations simulating the various core facility laboratories in Brazil and their different conditions and supplies.
Materials and Methods
Samples
Blood samples obtained from patients tested for HTLV-1/-2 specific antibodies which were infected and not infected with HIV-1, HBV and HCV were distributed in the following groups: Group 1, 37 patients infected with HTLV-1 alone confirmed by WB; Group 2, 152 patients infected with HIV-1 and reactive of HTLV-1/2 infection by screening assays; Group 3, 30 patients not infected with HTLV but infected with HIV-1 and/or HBV and/or HCV.
Briefly, samples of Group 1 belonged to blood donors from Recife, Pernambuco (Northeast Brazil), tested positive for HTLV-1 during the years 2012–2017, and sent to IAL for HTLV-1 subtype characterization (LTR, env and tax sequencing) using DNA extracted from peripheral blood mononuclear cells (PBMCs) isolated by Ficoll-Paque Plus density gradient centrifugation (GE Healthcare, Uppsala, Sweden). The HTLV-1 sequences from Recife were deposited in GenBank (Accession Numbers LTR: MF178246.1 to MF178269.1; tax: KY928553.1 to KY928577.1; env: KY928459.1 to KY928480.1), and the remaining DNA samples were tested for mqPCR_HTLV assays.
Samples from Group 2 and Group 3 belonged to patients infected with HIV/AIDS attending AIDS Reference Centers in São Paulo, and were sent to IAL during the years 2015–2018 (n = 2,991) for HTLV-1/2 diagnosis. The samples were used to detect the prevalence of HTLV-1 and HTLV-2 in HIV-1 infected patients from São Paulo, for HTLV-1/2 subtype surveillance, and for searching markers of diagnostic and prognostic values in retroviruses coinfection. The data of such research were published elsewhere (Caterino-de-Araujo et al., 2015; Campos et al., 2017a,b, 2020). Blood samples were collected in tubes containing EDTA, and the plasma and peripheral blood leukocytes (PBLs) were separated by centrifugation at 800 g for 10 min. Plasma samples were first tested for HTLV-1/2 specific antibodies using two immunoenzymatic assays (Gold ELISA HTLV I+II, REM Industria e Comercio Ltda, São Paulo, Brazil and Murex HTLV I+II, Diasorin, United Kingdom), and subsequently by WB (HTLV Blot 2.4, MP Biomedicals, Asia Pacific Pte. Ltd.), which is considered the reference method for confirming and differentiating between HTLV-1 from HTLV-2 infections in a majority of laboratories in Brazil and elsewhere. The PBL were stored at −20°C for further DNA extraction and qualitative qPCR analysis.
In some of the HTLV-1/-2-infected patients (Group 2) in clinical and laboratory follow-up tests (n = 16), PBMCs were isolated by Ficoll-Paque Plus density gradient centrifugation (GE Healthcare, Uppsala, Sweden), washed twice in phosphate buffered saline, and 106 cells pellets stored at −20°C for further qPCR quantitative analysis.
All samples refer to the routine diagnosis and projects on HTLV-1/2 approved by the Ethics Committee for Research of IAL (Ministry of Health protocol numbers CAAE #55837316.0.0000.0059 and #52493316.1.0000.0059).
DNA Extraction
Genomic DNA was extracted and purified from PBL and PBMC samples using Roche MagNA Pure® LC Robot Instrument, (Mannheim, Germany), with the LC MagNA Pure Nucleic Acid Isolation kit I from Roche Diagnostics, (Mannheim, Germany), according to the manufacturer’s instructions, and eluted with 100 μL of PCR-grade water. The extracted DNA was aliquoted into 4 vials for subsequent analysis and thawed only once.
Primers and Probes
Table 1 presents the sequences of primers and probes used in the mqPCR_HTLV (pol and tax) assays for HTLV-1 and HTLV-2 detection, their position in the genomic prototypes (ATK HTLV-1 infected cell line; GenBank accession number J02029.1), MoT (HTLV-2 infected cell line; GenBank accession number M10060.1), human albumin (GenBank accession number M12523.1), amplicon size, and the authors’ reference. The oligonucleotide concentrations were optimized using different concentrations of primers and probes in the range of 0.2–0.9 and 0.1–0.3 μM, respectively.
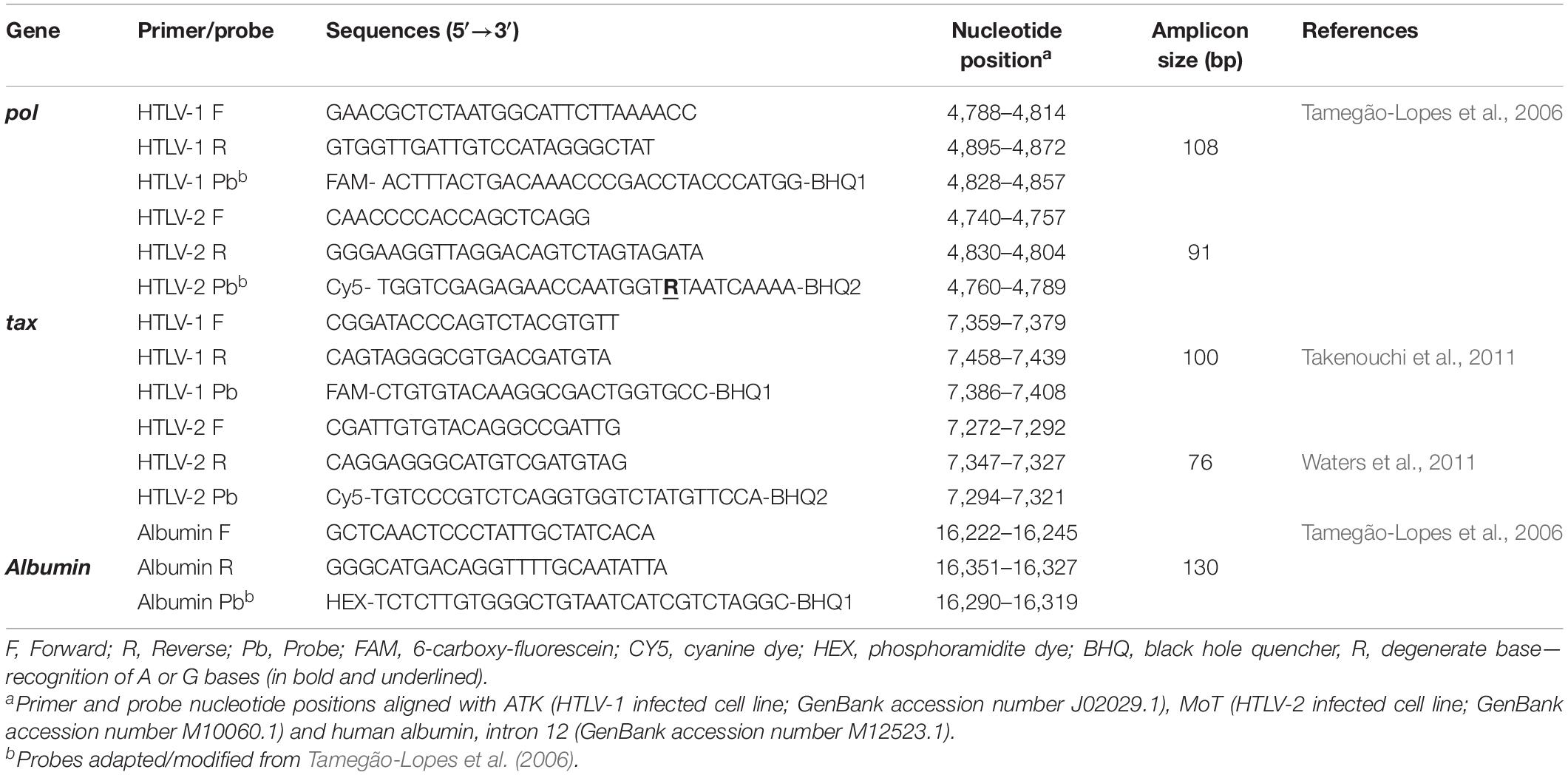
Table 1. Primers and probes employed in two multiplex qPCR_HTLV assays (pol and tax) for detecting HTLV-1 and HTLV-2.
Comparative analysis of sequences of HTLV-1 and HTLV-2 isolates from Brazil and abroad using the Basic Local Alignment Search Tool of the National Center for Biotechnology Information (NCBI) website,1 showed a mismatch (A and G) among some HTLV-2 Brazilian isolates at position 4,780 of the pol target region. Thus, to overcome this problem, a degenerate base (R) was included in the probe design (see Table 1, in bold and underlined).
Plasmids
Double recombinants plasmids of HTLV-1- and HTLV-2-albumin for both the gene targets (pol and tax) were employed as positive controls for standard curves construction.
The double recombinant plasmid of the pol target gene of HTLV-1 and the human albumin (pHTLV1pol-Alb) was kindly provided by Jorge Casseb from the Instituto de Medicina Tropical, São Paulo, and it was constructed by cloning a segment of 246 bp of the pol region of HTLV-1 (nucleotide position range from 4,708 to 4,953) and a 1,183 bp segment (nucleotide position range from 15,758 to 16,940) of intron 12 of the human albumin gene, according to Dehée et al. (2002). The pHTLV2pol-Alb double plasmid was kindly provided and designed by Marina Lobato Martins from the Fundação HEMOMINAS, Belo Horizonte, Minas Gerais, and consisted of a synthetic DNA of 321 bp, cloned into the vector pENO8H, containing a 138 bp fragment of the pol gene of HTLV-2 (nucleotide position range from 4,723 to 4,860) and a 170 bp fragment of the human albumin gene (nucleotide position range from 16,202 to 16,371).
The double recombinant plasmids for the tax target genes were designed at IAL and synthesized by Invitrogen GeneArt Gene Synthesis (Thermo Scientific, Waltham, United States). The pHTLV1tax-Alb plasmid consisted of a 321 bp synthetic DNA sequence (nucleotide position range from 7,339 to 7,488), and the pHTLV2tax-Alb plasmid consisted of a 297 bp fragment (nucleotide position 7,252–7,377), and both the plasmids contained a 170 bp fragment of the human albumin gene (nucleotide position range from 16,202 to 16,371). The plasmids containing the HTLV-1 or HTLV-2 tax and albumin target genes were expanded in E. coli cells in Luria Bertani (LB) medium containing 0.2 mg/mL ampicillin, and subsequently extracted and purified using the QIAprep Spin up Miniprep kit (Qiagen, Hilden, Germany). The sequences of the cloned inserts were determined and confirmed by performing a sequencing reaction on ABI 3130xl equipment and subsequently compared with reference sequences in GenBank (Accession Numbers J02029.1, M12523.1, and M10060.1).
The plasmid concentrations (ng/μL) were determined using the NanoDrop 2000 spectrophotometer (Thermo Fisher Scientific, Waltham, United States), and the Avogadro’s constant was used to convert it to the number of copies per microliter.
To determine the performance of the plasmids in mqPCR_HTLV assays, their standard curves and the limit of detection (LOD) were obtained by amplification of 10-fold dilutions of the plasmids containing 106 to 1 copy/5 μL in Tris-EDTA solution (10 mM Tris, 1 mM EDTA) and pH 8.0, in duplicate. The cycle quantification (Cq) values obtained were plotted against the logarithm of copy number.
Since HTLV-2 is known to have fewer copy numbers in relation to HTLV-1 (Lee et al., 2004; Murphy et al., 2004; Montanheiro et al., 2008), the LOD for HTLV-2 (pol) assay with concentrations of plasmids varying from 100 to 10 copies was tested in six replicates among the range of 100–15 copies and in 12 replicates for 10 copies.
The efficiencies of the assays were calculated according to the formula E = 10(–1/slope) −1 (Kubista et al., 2006; Raymaekers et al., 2009); the parameters for a singleplex assay were: efficiency 90–110% (slope between −3.6 and −3.1) and R2 ≥ 0.99; those for a multiplex assay were: efficiency 80–120% (slope between –3.9 and –2.9) and R2 ≥ 0.98 (Broeders et al., 2014).
Standardization of Multiplex Quantitative Real-Time PCR for HTLV-1/-2 Assays
The serial dilution of plasmids were utilized in mqPCR_HTLV using the Roche LightCycler 480II (Roche Diagnostics, Indianapolis, Indiana) and the 7.500 Applied Biosystems—ABI (Applied Biosystems) platforms. Each mqPCR_HTLV reaction was 25 μL in volume and contained: 5 μL of DNA template, 12.5 μL of master mix reagent, 0.2 μM of each set of oligonucleotides, except for the tax probe, which was used at 0.1 μM. Passive reference dye (ROX) was added to the reaction mix when using the ABI platform, according to the manufacturer’s instructions. PCR thermocycler conditions for amplification were as follows: 1 cycle at 50°C for 2 min, 1 cycle at 95°C for 10 min, 50 cycles at 90°C for 50 s, and 1 cycle at 60°C for 1 min (Tamegão-Lopes et al., 2006; Costa et al., 2011). The reactions were conducted in duplicate and considered positive if the amplification curves displayed the shape/slope and characteristics of an amplification reaction with a Cq value ≤ 40, according to the LOD of assays.
Seven different commercial master mix brands for hydrolysis probes were analyzed in the mqPCR_HTLV assays, using the ABI/Roche platforms: LightCycler Probes Master (Roche), Platinum®Quantitative PCR SuperMix-UDG (Invitrogen), GoTaq®Probe qPCR Master Mix (Promega), PerfeCTa qPCR ToughMix (Quantabio); Sso Advanced™ Universal Probes Supermix (Bio-Rad), Kapa Probe Fast qPCR Kit Master Mix (2X) Universal (Kapa Biosystems) and LuminoCt® qPCR ReadyMix™ (Merck/Sigma).
Validation of Multiplex Quantitative Real-Time PCR for HTLV-1/-2 Assays
To validate the multiplex qPCR format using plasmids, we compared the performance of multiplex and singleplex reactions in detecting HTLV-1 and HTLV-2 (pol and tax) at six points along the standard curves.
The LOD and efficiency of the mqPCR_HTLV assays were evaluated simultaneously on ABI and ROCHE platforms using serial dilutions of the double plasmids. The same LOD protocol was followed for conducting the reactions with different master mix formulations, as well as for analyzing the reproducibility of the assay by three different analysts and that of the robotic workstation for high-precision dilution setup of PCR-QIAgility (Qiagen). These professionals reproduced the reactions without previous knowledge of the mqPCR_HTLV results, having received only the initial concentration of the plasmids and the LOD protocol.
Performance of Multiplex Quantitative Real-Time PCR for HTLV-1/-2 Assays in Diagnosis
For calculating the efficiency of analytical performance of mqPCR_HTLV assays (pol and tax), we employed genomic DNA samples obtained from patients who were HTLV seropositive in screening assays, and for calculating the sensitivity and specificity of assays we considered the WB results. In case of divergent results, we observed the results of another confirmatory serological assay (LIA, INNOLIA HTLV-I/II, Fujirebio, Europe N.V., Belgium) and/or the PCR-RFLP (tax) assay, as previously described (Tuke et al., 1992; Campos et al., 2017b).
The sensitivity of the assays was evaluated in DNA samples obtained from PBL or PBMC of 37 patients infected with HTLV-1 alone (Group 1) and 152 patients infected with HIV and suspected of HTLV-1/-2 coinfection (Group 2). The specificity of assays was evaluated using genomic DNA samples of 30 HTLV-1/-2-seronegative patients infected with HIV-1 (Group 3), which included 22 HIV-monoinfected, 2 HIV/HBV-coinfected, 3 HIV/HCV-coinfected, and 3 HIV/HBV/HCV-coinfected.
The precision of mqPCR_HTLV (pol and tax) assays (reproducibility intra- and inter-assays) was assessed in DNA samples of patients that had different positive Cq values (profiles): Cq ≤ 30 (high); Cq from 31 to 35 (median); Cq from 36 to 37 (low); Cq from 38 to 40 (scarce). Eight clinical DNA samples were processed (4 HTLV-1 and 4 HTLV-2) in duplicate and the experiments were conducted daily across 4 consecutive days.
In addition to the qualitative use of the assays, we evaluated their possible use in PVL quantification. Unfortunately, due to the low volume of the remaining DNA samples, this analysis could not be performed for all the mqPCR_HTLV assays, but only mqPCR_HTLV (pol), which was conducted in duplicate using the ABI equipment. Using 5 μL of the 100 μL of DNA samples extracted from 1 × 106 PBMCs of 16 HTLV-1/2-infected patients in follow-up (Group 2), we inferred that the Cq value obtained corresponds to 0.5 × 105 cells. Thus, for calculating the number of copies of HTLV-1 and HTLV-2 in 105 cells, we plotted the Cq value obtained in the standard curve and multiplied the number of copies by 2.
Statistical Analysis
The mqPCR_HTLV assay data were analyzed by descriptive statistics using 2 × 2 contingency tables and the Microsoft Excel 2016 software. 95% confidence interval (CI) and the Kappa index were calculated. The Grubbs test was employed for the comparison of the methods and the creation of the linearity graphs.
The intra- and inter-assay reproducibility were calculated in percentage using the mean Cq, standard deviation (SD) values, and coefficient of variation (CV) (CV = 100 × standard deviation / mean, %). CV of Cq values of intra- and inter-assay reproducibility of 3 and 10%, respectively, are considered acceptable according to Dehée et al. (2002), and Estes and Sevall (2003).
Results
Multiplex Quantitative Real-Time PCR for HTLV-1/-2 (pol and tax) Assays Optimization
After testing several concentrations of primers (0.2–0.9 μM), and probes (0.1–0.3 μM), the mqPCR_HTLV (pol and tax) assays were optimized using 0.2 μM primers and probes, except for the tax probe which performed better at a concentration of 0.1 μM.
Comparative Efficiency of Singleplex and Multiplex qPCR_HTLV Assays
Figure 1 represents the comparative efficiency of singleplex and multiplex qPCR_HTLV in detecting HTLV-1/-2 pol (Figures 1A,B) and tax (Figures 1C,D) target genes using serial plasmid dilutions and linear regression graphics analyses. Six synthetic DNA concentrations were detected in both the assays, with R2 values > 0.99 or 0.98 and at least 90 or 80% efficiency as acceptable values for the two detection assays, respectively.
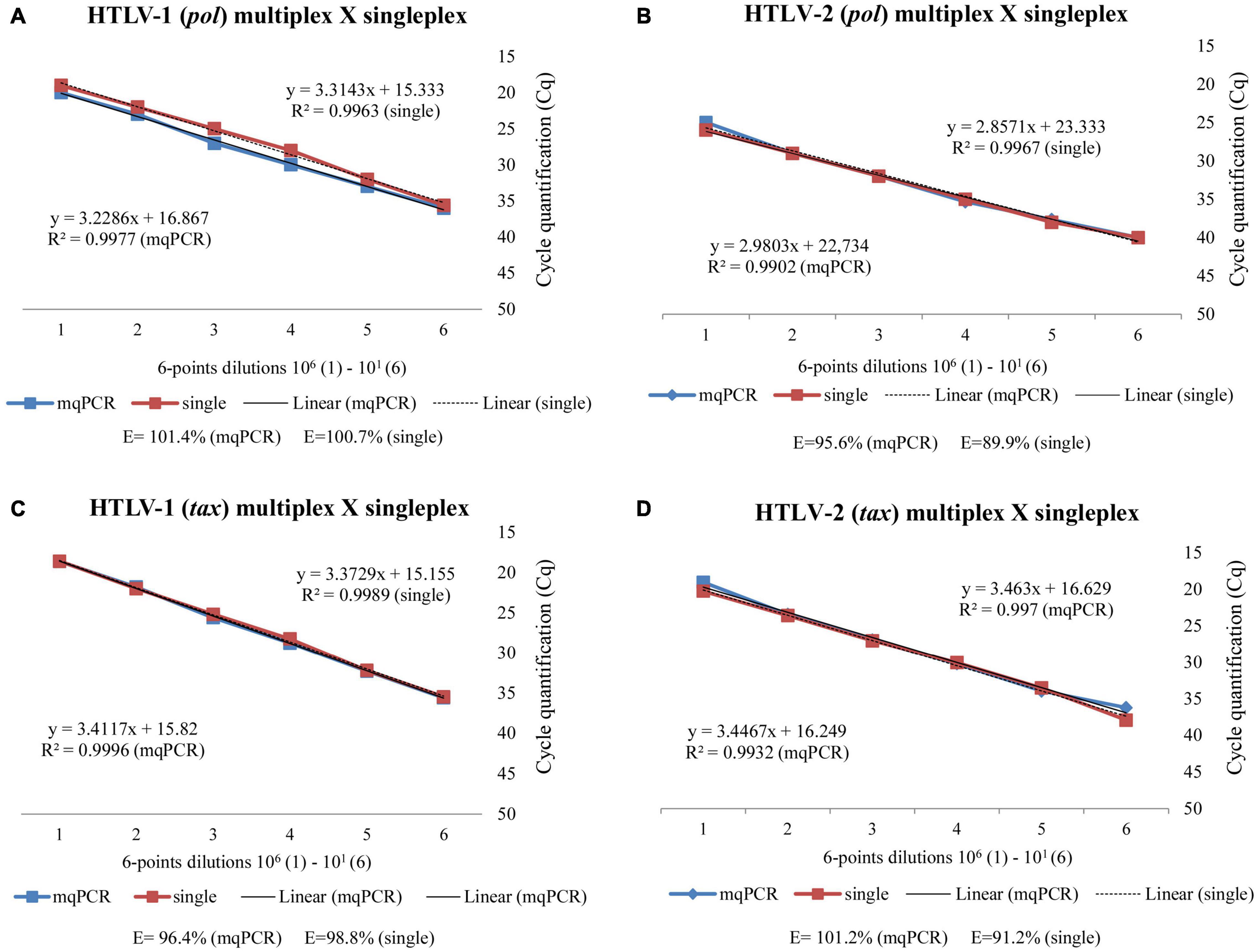
Figure 1. Comparative efficiency of the singleplex and multiplex qPCR_HTLV in detecting HTLV-1/-2 pol (A,B) and tax (C,D) target genes using serial plasmid dilutions and linear regression analyses, conducted in ROCHE platform.
Efficiency and Limit of Detection of the Multiplex Quantitative Real-Time PCR for HTLV-1/-2 Assays With Respect to Plasmids Dilutions and Different Platforms
The efficiencies and LODs of mqPCR_HTLV (pol and tax) assays analyzed using the ABI and Roche’s equipment are shown in Table 2. Independent of the equipment utilized, the best LODs were set for detecting HTLV-1 and the tax target gene.
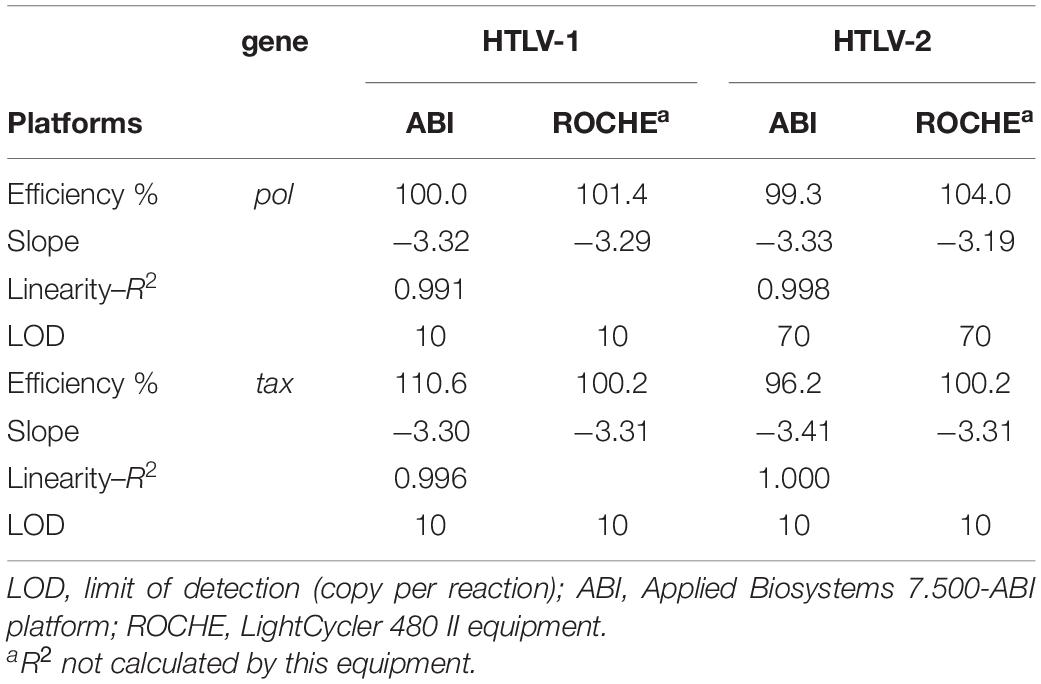
Table 2. Efficiency of the mqPCR_HTLV (pol and tax), slope and correlation coefficients (R2) for detecting HTLV-1 and HTLV-2 using two platform/equipment.
All results obtained (pol, tax and Albumin) agree with the acceptance performance parameters for mqPCR assays, but because the LOD for HTLV-2 pol ranged from 10 to 100 copies per reaction, it was decided to conduct additional evaluations in this range of plasmid dilutions to determine the best final LOD using intra-assay reproducibility analyses (Table 3). The reactions were conducted in 6 replicates for concentrations ranging between 15 to 100 plasmid copy number, and in 12 replicates for 10 plasmid copy number. The results obtained disclosed 100% consistent detections (6/6) for 70 copies, 66% (4/6) for 50 copies, and 50% (3/6) for 20 copies (Table 3). Thus, we decided to consider 70 copies as the LOD for HTLV-2 (pol).
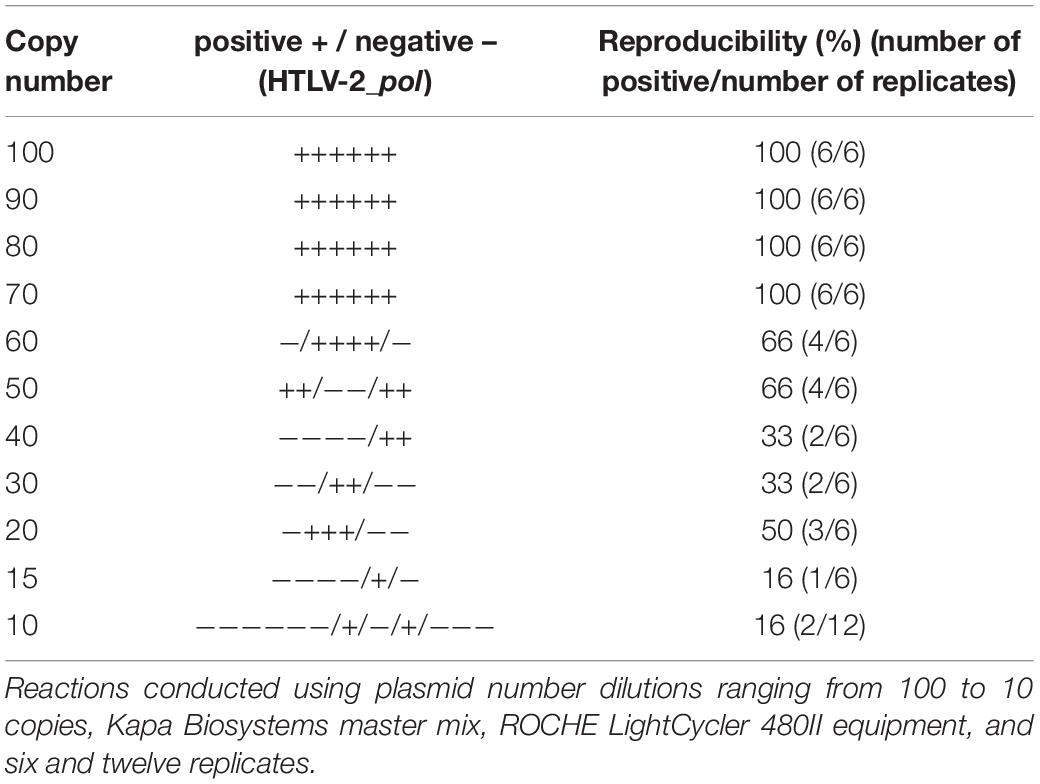
Table 3. Limit of detection and intra-assay reproducibility of the mqPCR_HTLV (pol) for detecting HTLV-2.
Sensitivity and Efficiency of the Multiplex Quantitative Real-Time PCR for HTLV-1/-2 Assays Using Several Master Mix Formulations
We assessed the feasibility and performance of seven different commercial master mix reagents, available in the Brazilian market, for mqPCR assays for HTLV-1 and HTLV-2 provirus detection using the LOD protocol for pol and tax target genes. The results obtained are shown in Figures 2, 3. All commercial reagents exhibited the parameters required of the mqPCR assays, displaying good performance in the reactions, with the lowest efficiency being over 90% (Table 4), confirming the flexibility of use of master mix formulations in these assays.
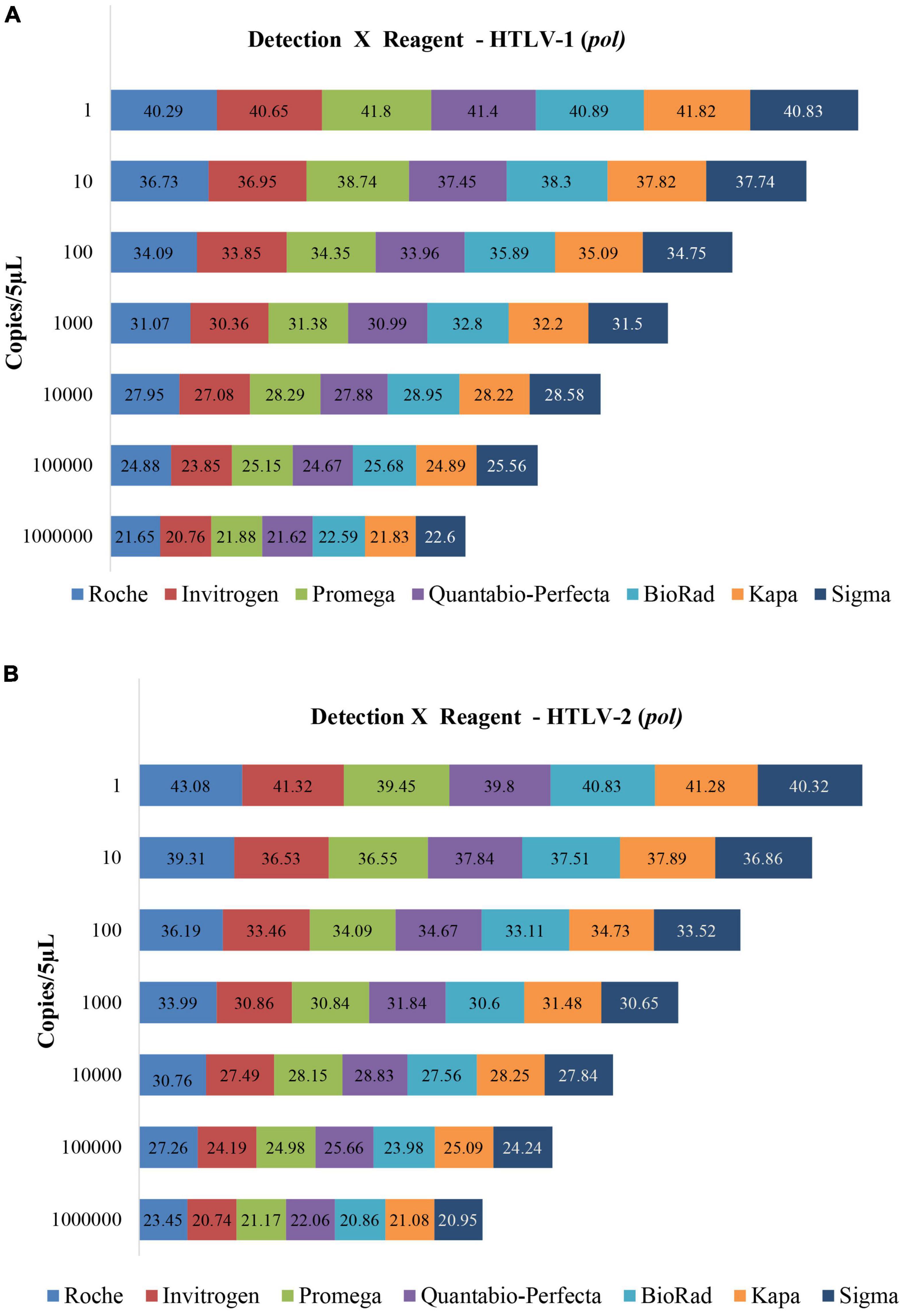
Figure 2. Limit of copy number detection of the mqPCR_HTLV assay (pol) for detecting HTLV-1 (A) and HTLV-2 (B) using plasmids and seven different master mix trademarks, and ROCHE LightCycler 480II equipment. The Cq values are disclosed inside the rectangles.
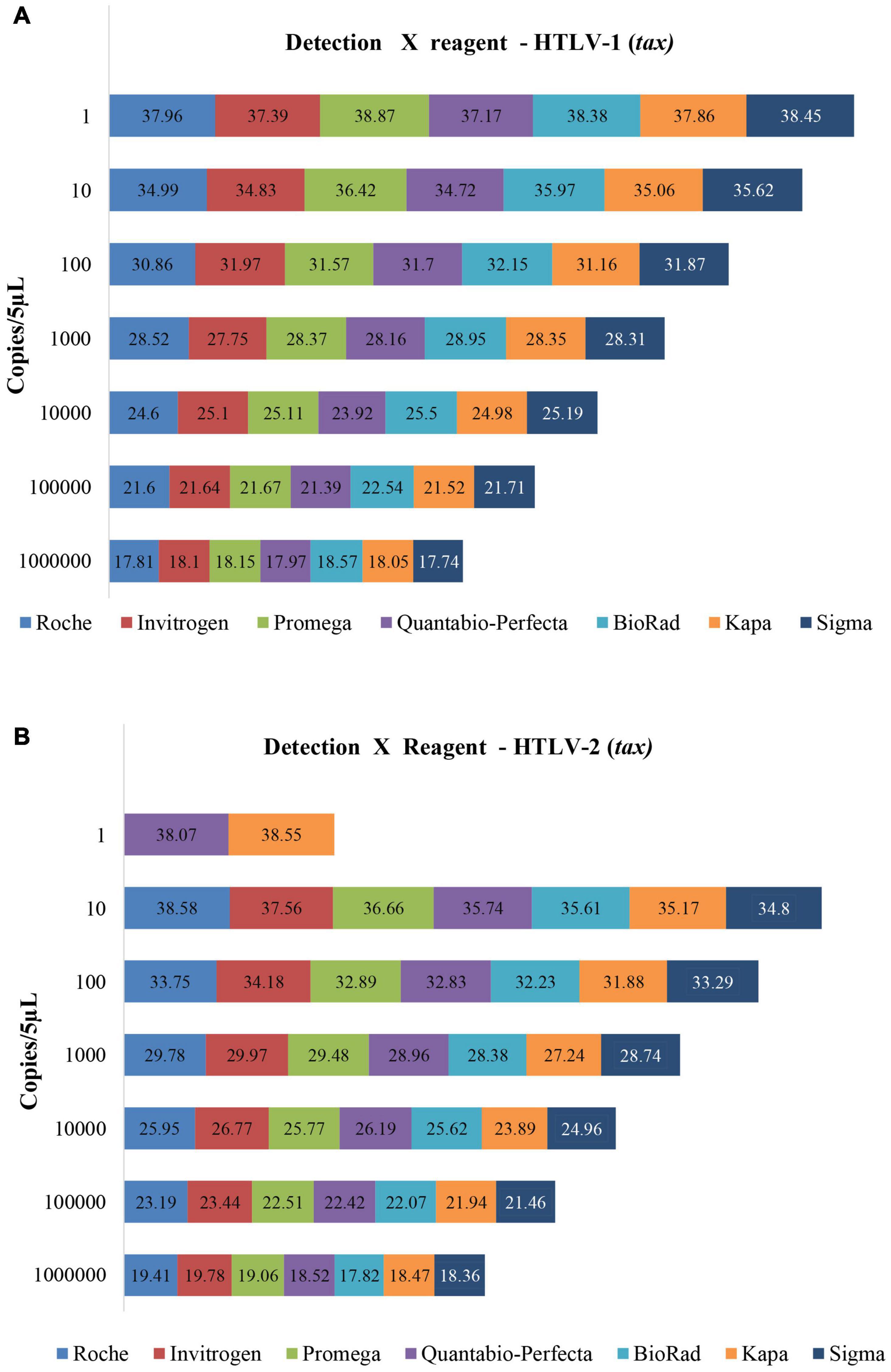
Figure 3. Limit of copy number detection of the mqPCR_HTLV assay (tax) for detecting HTLV-1 (A) and HTLV-2 (B) using plasmids and seven different master mix trademarks, and ABI 7.500 equipment. The Cq values are disclosed inside the rectangles.
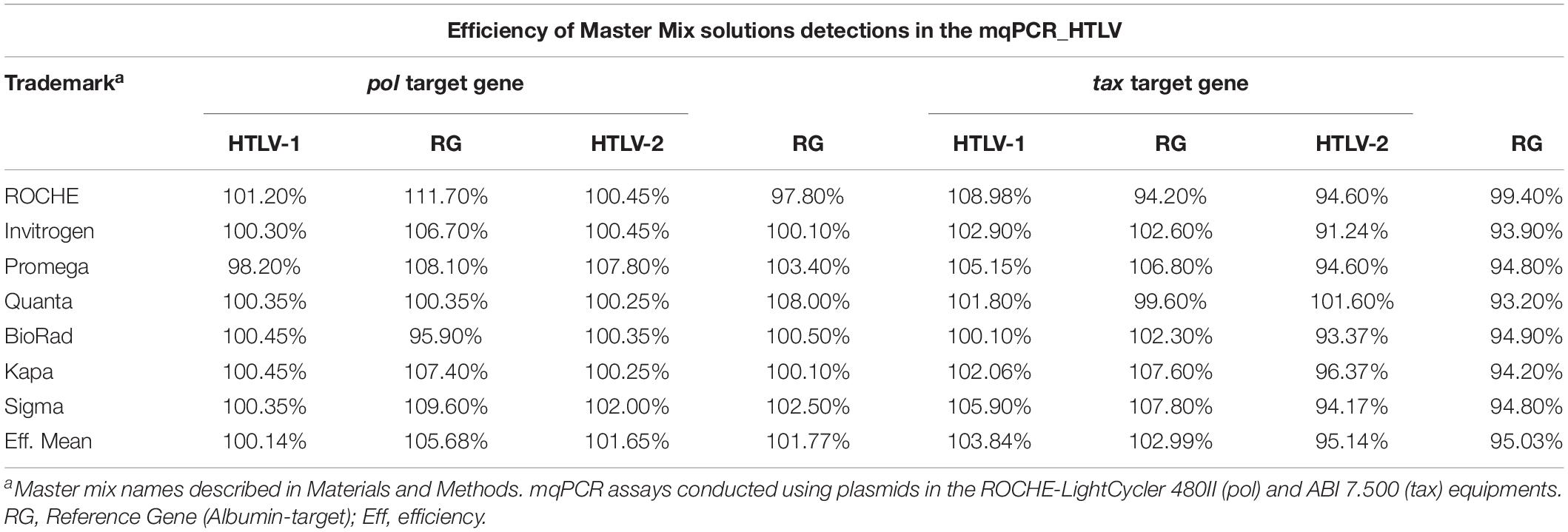
Table 4. Efficiency values of the mqPCR_HTLV assays for detecting HTLV-1 and HTLV-2 (pol and tax) and the reference gene (human albumin gene), using seven commercial master mix reagents.
Precision of Multiplex Quantitative Real-Time PCR for HTLV-1/-2 Assays
The intra- and inter-assay reproducibility results of the mqPCR_HTLV (pol and tax) assays conducted with respect to the plasmid dilutions prepared by the three analysts, and those prepared by the robotic workstation for high-precision PCR, are presented in Table 5. The data analysis showed no substantial differences among the professionals in reproducing the assays, with acceptable values of CV for all. All of them were able to detect at least 10 copies of HTLV-1 in both the mqPCR_HTLV (pol and tax) assays, 10 copies of HTLV-2 in mqPCR_HTLV (tax) assay, and approximately 10–100 copies of HTLV-2 in mqPCR_HTLV (pol) assay, thereby corroborating previous results.
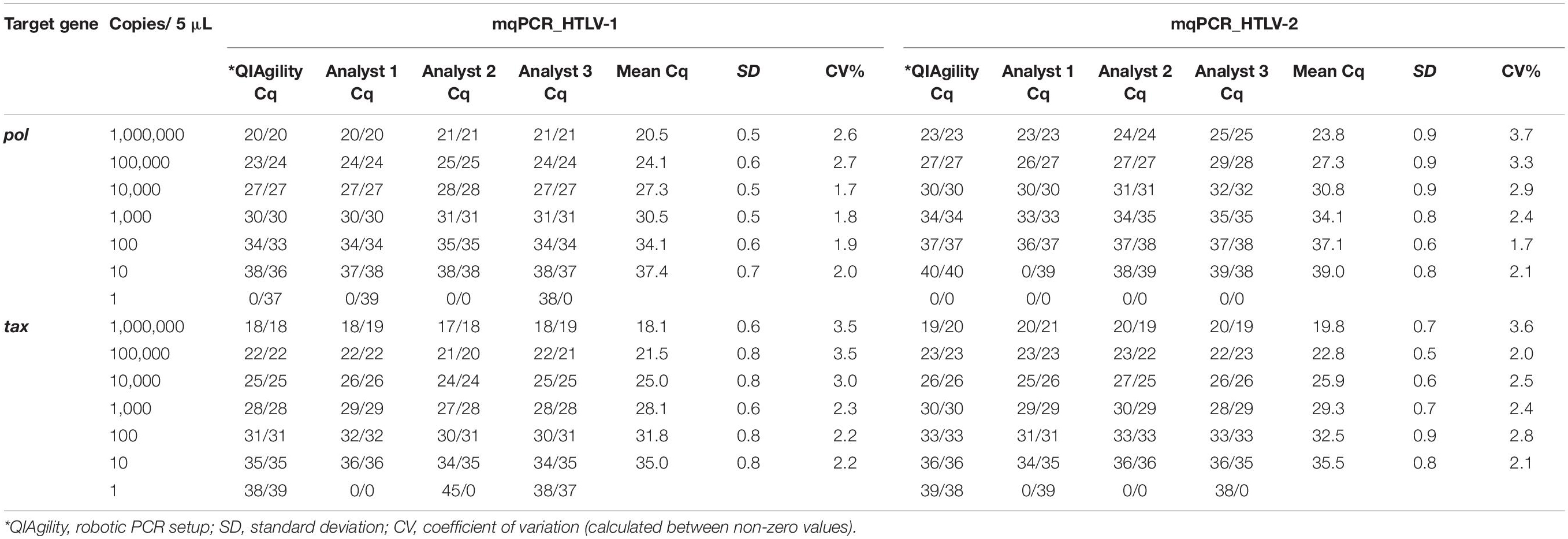
Table 5. Intra- and inter-assay reproducibility of mqPCR_HTLV (pol and tax) for detecting HTLV-1 and HTLV-2 using serial plasmid dilutions prepared by three analysts and a robot, conducted in duplicate using the ABI equipment.
Performance of the Multiplex Quantitative Real-Time PCR for HTLV-1/-2 Assays in Diagnosis (Sensitivity and Specificity)
To calculate the sensitivity of the mqPCR_HTLV (pol and tax) assays we compared the WB results. Of the 37 DNA samples from patients infected with HTLV-1 alone analyzed by WB (Group 1), 36 were positive in both mqPCR_HTLV (pol and tax) assays (97.3%; CI 95% 76.9–84.6). The single mqPCR_HTLV negative sample showed discordant results on screening (data not shown).
The testing of 152 DNA samples from HIV-infected patients that were HTLV reactive on screening (Group 2) using the mqPCR_HTLV pol and tax assays showed different and interesting results (Table 6). Per WB results, 118 out of the 152 samples were HTLV positive (77.6%, 95% CI 76.9–84.6): 77 HTLV-1, 29 HTLV-2, 3 HTLV-1+2, 9 HTLV untyped, 22 indeterminate, and 12 negative. Per the mqPCR_HTLV (pol) assay, 101 out of the 152 samples were positive (66.4%, 95% CI 57–75.4), and as per the mqPCR_HTLV (tax) assay, 95 out of the 152 samples were positive (62.5%, 95% CI 52.7–72.2). The mqPCR_HTLV (pol) assay was able to detect more cases of HTLV-2 than the mqPCR_HTLV (tax) assay and WB (Table 6).

Table 6. Results of HTLV-1/2 confirmatory tests (WB, mqPCR_HTLV pol and tax) when employed in HIV-infected individuals suspected of HTLV-1/2 infection by screening assays (Group 2).
Among the 22 WB-indeterminate samples, the mqPCR_HTLV (pol) assay identified ten as positive (45.5%): nine as HTLV-2 (Patients N. 14, 20, 29, 35, 83, 116,144, 146, and 148), and one as HTLV-1 (Patient N. 7). By the mqPCR (tax) assay, seven were positive (31.8%): six were HTLV-2 (Patient N. 14, 29, 35, 83, 144, and 146) and one was HTLV-1 (Patient N. 7). Regarding the nine WB HTLV untyped samples, six (66.7%) were identified as positive: three HTLV-1 (Patient N. 31, 88, and 120) and one HTLV-2 (Patient N. 84), using both the mqPCR (pol and tax) assays, one HTLV-2 using mqPCR pol (Patient N. 129) and one HTLV-1 by mqPCR tax (Patient N. 108) (Table 7).
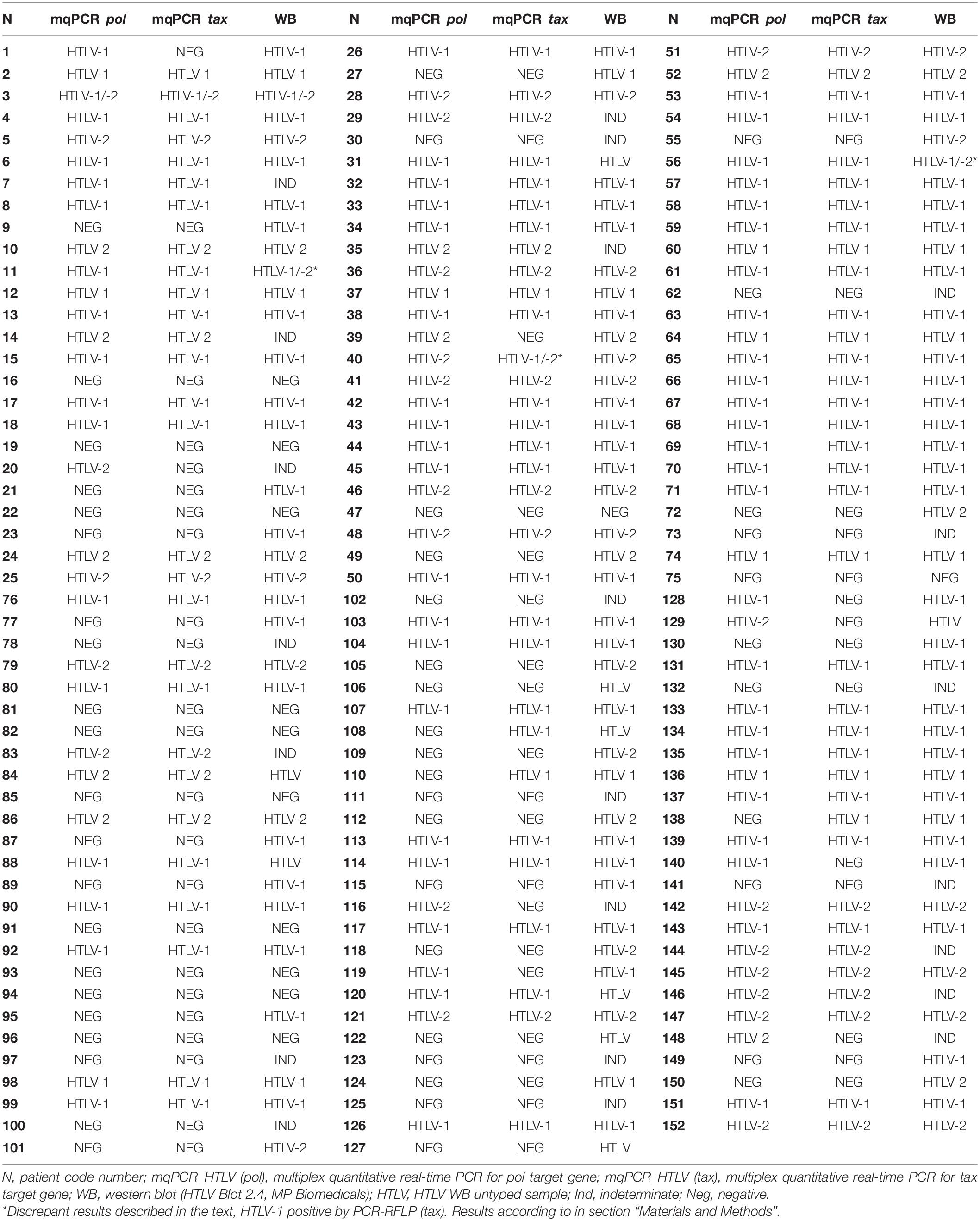
Table 7. Final results of HTLV-1/2 confirmatory tests (mqPCR_HTLV pol and tax, WB when employed in 152 HIV-infected individuals suspected of HTLV-1/2 infection by screening assays (Group 2).
Furthermore, three discrepant results were observed among the confirmatory assays, one sample confirmed HTLV-2 infection in three tests (WB, LIA and mqPCR_HTLV pol), and was repeatedly detected positive for HTLV-1 and HTLV-2 by mqPCR-tax and for HTLV-1 by PCR-RFLP (tax) (Patient N. 40, Table 7), data published elsewhere (Campos et al., 2017b). The other two samples were confirmed HTLV-1 and HTLV-2 by WB analysis but were only HTLV-1 positive by mqPCR_HTLV (pol and tax) assays (Patients N. 11 and 56). In one of these samples the LIA was indeterminate.
Thus, the relative sensitivity of the mqPCR_HTLV (pol and tax) assays compared to that of WB in HTLV-1 monoinfected patients was 97.4%; in HIV/HTLV-coinfected was 77.1%, Kappa index—0.405 (95% CI 0.238–0.575) (mqPCR_HTLV pol) and 74.6%, Kappa index—0.435 (95% CI 0.277–0.593) (mqPCR_HTLV tax). No sample from Group 3 (HIV- and/or HBV- and/or HCV-infected) and or samples negative per WB and LIA assays from Group 2 were positive in mqPCR_HTLV assays. Additionally, all samples tested negative for HTLV-1 and HTLV-2 in molecular assays were positive for the reference gene (Albumin).
Table 8 shows the intra- and inter-assay reproducibility for detecting HTLV-1 and -2 using the mqPCR_HTLV assays (pol and tax). The DNA samples from eight individuals with different positive Cq profiles were tested in duplicates across four consecutive days. The mean Cq and CV values were determined and the results showed minor variation and good reproducibility of results in samples with low DNA concentrations (Cq > 36). Although the same input volume of DNA was used for both the assays to detect HTLV-2, a difference around 3 Cq was detected, the greater value being for pol target gene detection. Despite the fact that the mqPCR_HTLV tax presented lower Cq values in relation to the mqPCR_HTLV pol, the tax target gene was more difficult to detect in samples with scarce DNA copy number, corroborating previous findings of assays standardization.
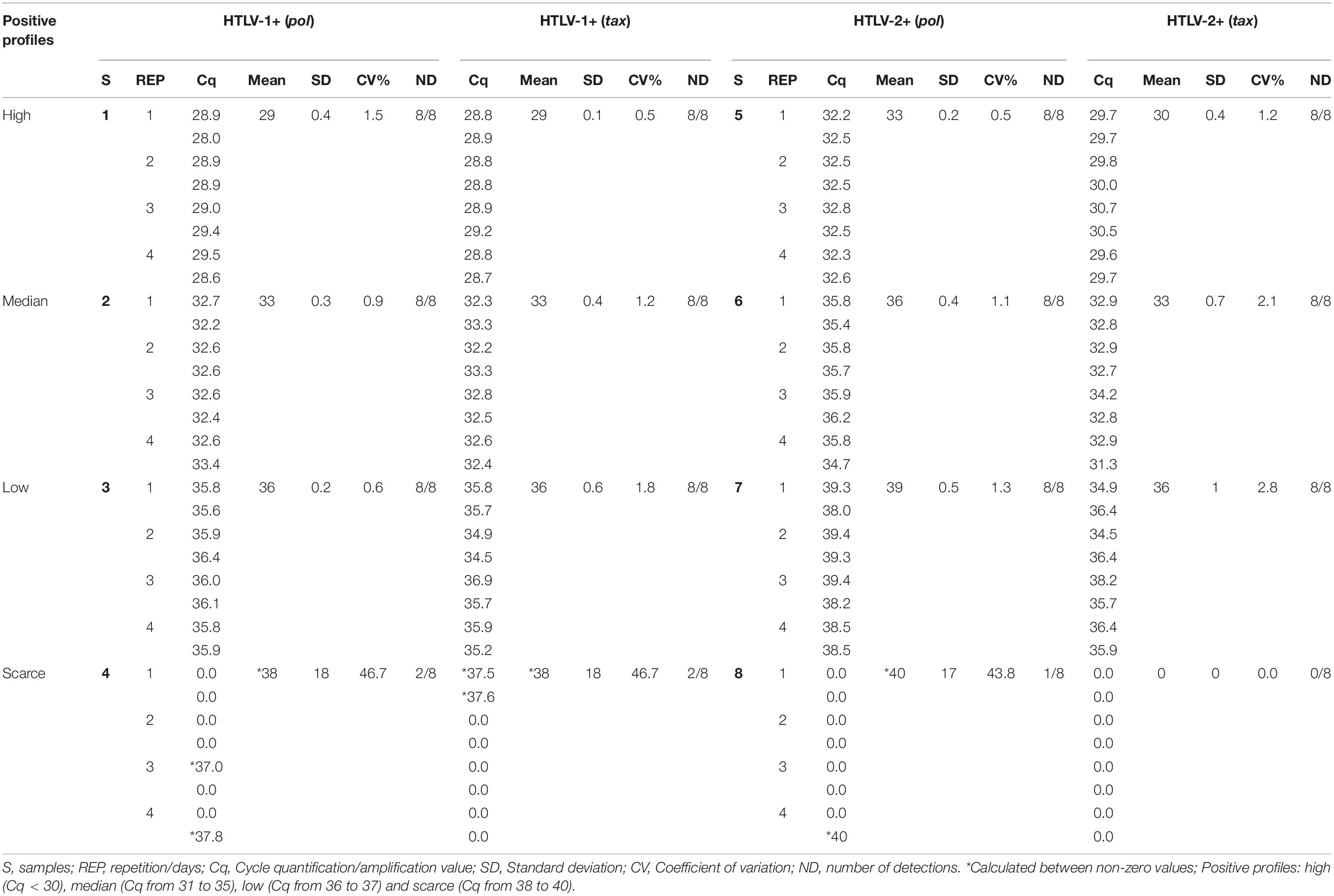
Table 8. Intra- and inter-assay reproducibility of mqPCR_HTLV assays (pol and tax) for detecting HTLV-1 and HTLV-2 using DNA samples from eight individuals with different positive Cq profiles, in duplicate and in four consecutive days of analysis.
Application of Multiplex Quantitative Real-Time PCR for HTLV-1/-2 Assays for Proviral Load Measurement
Sixteen DNA samples from patients of Group 2 in clinical and laboratory follow-ups were analyzed for PVL quantification using the mqPCR_HTLV (pol). Four (25%) were negative, seven (43.7%) were HTLV-1 positive, and five (31.3%) were HTLV-2 positive. The results of provirus copy number calculated as described in section “Materials and Methods” are presented as Supplementary Table 1. Additionally, all samples that were negative for HTLV-1 and HTLV-2 in mqPCR_HTLV assays had DNA of good quality and quantity, indicated by the positive results of the albumin reference target gene.
Discussion
Molecular confirmatory assays, mostly qPCR, are important tools for HTLV-1/2 diagnosis, for avoiding vertical transmission in children born to HTLV-1/2-infected mothers, and for monitoring HTLV-1/2 PVLs and disease development (Rosadas et al., 2021b). Serological confirmatory assays for HTLV-1 and HTLV-2 (WB and LIA) are expensive and prone to delivering inconclusive results (indeterminate or HTLV untyped results) (Campos et al., 2020; Caterino-de-Araujo et al., 2021). In Brazil, all molecular assays for HTLV diagnosis are developed in-house but only a few of them were validated (Andrade et al., 2010; Waters et al., 2011; Furtado et al., 2012; Ribeiro et al., 2012; Rosadas et al., 2013; Caterino-de-Araujo and Gonçalves, 2021). The aim of the present study was to develop and validate two multiplex qPCR_HTLV assays capable of simultaneously detecting the presence of HTLV-1 and HTLV-2 target genes and the albumin reference gene, using different PCR platforms and master mix formulations. This design and validation aimed to solve problems related to time constraints, cost, low quantity of biological specimens, and the diversity of PCR platforms and reagents available in the Public Health Laboratories in Brazil.
We used four double synthetic plasmids for standard curve construction (two of which were customized by us), since this kind of reference material is stable, provides reproducible results, and could be used for absolute PVL quantification (Dehée et al., 2002; Kamihira et al., 2010; Abad-Fernández et al., 2014; Bandeira et al., 2020). Bandeira et al. (2020) identified the potential of using synthetic oligonucleotides to prepare a standard curve for HTLV-1 PVL quantification based on the linearity, qPCR efficiency, and equivalent results of such references when compared with a validated qPCR assay using a conventional TARL-2 cell standard curve, as constructed by Rosadas et al. (2013). In addition, these authors highlighted that procuring and maintaining such reference material is less expensive than using DNA obtained from cells lineages infected with HTLV-1 and -2 (Bandeira et al., 2020).
We selected two segments of the proviral genome of HTLV-1 and -2 to standardize these assays, pol, and tax, and utilized probes labeled with FAM (HTLV-1), CY5 (HTLV-2) and HEX (albumin). We used two assays employing different target genes to avert possible false negative results due to the presence of point mutations in primers and probes binding regions or the presence of defective provirus particles (absence of such genes) in HTLV-1 and -2 infected individuals (Tamiya et al., 1996; Ramirez et al., 2003; Takenouchi et al., 2011; Kuramitsu et al., 2017; Campos and Caterino-de-Araujo, 2020; Blanco et al., 2021; Caterino-de-Araujo and Campos, 2021). We evaluated theses assays in two Platforms (ROCHE and ABI) and with seven master mix formulations.
Comparative performance analysis of the plasmid standard curves construction and sensitivities in singleplex and multiplex assays showed no difference, which indicates that there is no interference of one labeled probe with another labeled probe in the multiplex qPCR_HTLV assays. The comparative analyses of the standard curves showed similar efficiency, and the overall sensitivities (LOD) of assays were 10 and 10 copies for HTLV-1 and 10 and 70 copies for HTLV-2 using tax and pol target genes, respectively, with efficiencies above 90%.
Although previous studies of mqPCRs disclosed greater sensitivities for detect and quantify HTLV-1/2 compared to the present study, they are restricted to equipment and reagents, with trademark exclusivity. For instance, Moens et al. (2009) developed a triplex qPCR for simultaneous detections of 1 copy of HTLV-1 (FAM), HTLV-2 (JOE), and HTLV-3 (CY5) using tax specific target primers and human β-globin as reference gene (NED). However, the reference gene to quantify cells number was detected separately and the dye NED is exclusive to the ABI platform.
Lee et al. (2004) developed one biplex qPCR assay using a primer pair that amplifies a segment of tax gene common to HTLV-1 and HTLV-2, and as reference gene another single qPCR for HLA-DQ alpha; both assays employed the Sybr Green dye. Thus, although these qPCR showed high sensitivity (1 copy per reaction), and could be employed in different PCR platforms, the biplex qPCR does not distinguish HTLV-1 from HTLV-2. Estes and Sevall (2003) described another biplex qPCR that utilizes the tax segment of HTLV-1 and a segment of the 5′ LTR of HTLV-2 as targets and the singleplex assay for human β-globin for PVL quantification. In these assays, the ABI equipment and supplies were utilized and a LOD of ∼60 copies were detected for both HTLV-1 and HTLV-2.
Besson and Kazanji (2009) developed a fourplex qPCR to detect HTLV-1, HTLV-2, HTLV-3, and human albumin. The authors used primer pairs for the pX regions of HTLV with LOD of 1 copy for HTLV-1 and 10 copies for HTLV-2. Nevertheless, the probe used for HTLV-1 pX detection was labeled with ROX. Since this dye is a passive reference that the ABI platform needs to normalize the fluorescence data, this component does not allow the use of such fourplex qPCR for quantitative analyses in this equipment, as well as commercial reagents that have ROX or similar passive reference in their formulation.
Waters et al. (2011) developed and validated a triplex qPCR for detecting the segments pol of HTLV-1, tax of HTLV-2, and the human albumin as reference. They used the labeled probes HTLV-1 (JOE), HTLV-2 (FAM) and Albumin (NED) and detected sensitivities varying from 1 to 10 copies for all target genes but solely using the ABI platform. Thus, considering the previous information, the present mqPCR_HTLV assays have the advantage of being used in two different platforms, representative of the PCR platforms available in Public Health Laboratories in Brazil.
Furthermore, the present mqPCR_HTLV showed similar sensitivity (LOD) using seven different master mix formulations, solving the problem of using varied brands of master mix depending on availability and cost.
The concern reported around the LOD (more sensitivity) in the previous qPCR assays compared with the present mqPCR_HTLV assays, is that the discordant results could be partially explained by the target choice. When we used the pol as target gene, differences in sensitivity (LOD) of assays were detected. In contrast, when we used the tax target gene a significant LOD was detected, corroborating with previous descriptions. The majority of mqPCR assays above employed the tax gene for HTLV-1/2 detection. We do not know the cause of these results, but despite the lower LOD of the mqPCR pol, this assay was able to detect 1 copy of HTLV-1 and 10 copies of HTLV-2, but without consistent reproducibility. In this regard, according to the Poisson’s distribution, LOD < 3 copies, and the detections of 1 copy of DNA are considered only hypothetical to qPCR assays (Bustin et al., 2009), and needed to define the dynamic range of the method and the PCR characteristics (Raymaekers et al., 2009). Detection below the LOD IC 95% could be obtained in DNA samples from pathogens, but with less accuracy (Kralik and Ricchi, 2017), corroborating the present results. Although the LOD = 1 copy is possible when conducted usually with plasmids, in clinical samples they will be incredibly rare, except for digital-PCR.
Curiously, although Cq values > 40 were obtained in mqPCR_HTLV (pol) assay using plasmids, when this assay was employed in clinical DNA samples, no sample showed Cq values > 40. Thus, we could suggest in the future, after gaining experience from testing many samples, to reduce the number of cycles repetition from 50 to 45, and consider the Cq value ≤ 40 for positive samples.
Another important fact that emerged from this study was the greater diagnostic sensitivity of mqPCR_HTLV (pol) for detecting samples infected with HTLV-2, which seems contradictory with the fact that this assay has a lower LOD compared to mqPCR_HTLV (tax). HTLV-2 is more difficult to be confirmed by serological and molecular confirmatory assays, as HTLV-2 accounts for more indeterminate WB results (Morimoto et al., 2007; Costa et al., 2011; Caterino-de-Araujo et al., 2014, 2015; Campos et al., 2017b,2020) and has a low PVL (Lee et al., 2004; Murphy et al., 2004; Montanheiro et al., 2008).
The relative sensitivity of 97.4% detected in samples from patients monoinfected with HTLV-1 in both mqPCR assays of the present study is in accordance with a series of studies reported in a review of molecular assays for HTLV-1/2 diagnosis (Caterino-de-Araujo and Gonçalves, 2021); the unique sample that resulted negative on these assays presented discordant results in serologic screening, which could be due to low PVL (under the detection limit of assays) and consequently low levels of antibodies production, and/or the presence of provirus mutations or defective particles circulating in this patient.
Among samples of HIV/HTLV-coinfected patients, relative sensitivities of 77.1% (mqPCR-HTLV pol) and 74.6% (mqPCR_HTLV tax) were detected and the negative results could be due to: (i) provirus mutations and defective HTLV particles circulating in HIV/HTLV-coinfected patients (Campos and Caterino-de-Araujo, 2020; Caterino-de-Araujo and Campos, 2021), (ii) fluctuations in HTLV-1/-2 PVL in patients under antiretroviral therapy (Machuca and Soriano, 2000), (iii) use of highly active antiretroviral therapy (HAART) for long periods of time by the patients (Costa et al., 2011; Caterino-de-Araujo et al., 2015), and (iv) low PVL, mostly of HTLV-2 (Lee et al., 2004; Murphy et al., 2004; Montanheiro et al., 2008). Despite these limitations, the present mqPCR_HTLV were able to confirm and distinguish HTLV-1 and HTLV-2 infections in HIV-infected patients that resulted WB-indeterminate or HTLV untyped, as occurred in the past using the singleplex qPCR assays (Costa et al., 2011; Caterino-de-Araujo et al., 2015). As expected, no complete agreement of results was detected between mqPCR assays and WB (Kappa index = 0.4), since they are designed for different targets (proviral DNA and antibodies, respectively).
Notably, both mqPCR_HTLV assays disclosed 100% specificity when applied in samples of patients infected with HIV, and/or HBV, and/or HCV. In patients with HIV infection, the correct diagnosis of HTLV-1 and HTLV-2 coinfection has predictive value, since they impact in HIV disease progression to AIDS: HTLV-1 accelerates HIV disease progression while HTLV-2 has been pointed to delay progression to AIDS (Beilke, 2012).
Concerning the use of present assays for PVL quantification, although only the mqPCR_HTLV (pol) could be evaluated, the results obtained support its use for monitoring infection and stratifying the risk for HTLV-1-associated disease development (Haziot et al., 2019; Rosadas et al., 2021a).
Finally, although the present study had some limitations regarding: (i) limited volume of biological samples to conduct all comparative experiments, (ii) absence of samples of patients infected only with HTLV-2, (iii) possible low PVL in HIV-infected patients on HAART treatment, (iv) insufficient volume of samples for validate PVL quantification for both target genes (pol and tax), and (v) no inter-labs comparative analysis, the present mqPCR_HTLV assays were validated for routine diagnosis considering the parameters previously described for qualitative assays (standard curves, efficiencies, R2 values), without false positive results.
In conclusion, the present mqPCR_HTLV (pol and tax) assays displayed feasibility in diagnosing HTLV-1 and HTLV-2 in different core facilities laboratory, conditions, and supplies.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
Ethics Statement
The studies involving human participants were reviewed and approved by Research Ethics Committee of Instituto Adolfo Lutz. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
MG designed the work, performed all the experiments, figures and tables, analyzed the results, and wrote the manuscript. LF designed and expanded the plasmids, conducted some experiments, analyzed the results, and wrote the manuscript. FH conducted the experiments of reproducibility. KC conducted experiments that supported to determine the diagnostic performance of the new assays. ACA conceived and administrated the project, acquired funding, supervised the experiments, analyzed the results, and wrote the manuscript. All authors read and approved the submitted version.
Funding
This study was supported by grants from Fundação de Amparo a Pesquisa do Estado de São Paulo (FAPESP #16/03654-0).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We thank Jorge Casseb from the Instituto de Medicina Tropical de São Paulo and Marina Lobato Martins from the Fundação HEMOMINAS de Belo Horizonte for providing the pol-Alb plasmids, Patricia Moura from Universidade Federal de Pernambuco for consenting to use the remaining DNA samples of blood donors infected with HTLV-1 in mqPCR_HTLV analysis, and Wong Kuen Alencar (in memoriam) from Centro de Referência e Treinamento em DST/AIDS de São Paulo for take care patients. We are also indebted to Cláudio Tavares Sacchi for review the medical records of patients, Maristela Marques Salgado for conducting the LOD reproduction assay and supporting the preliminary samples procedure, Terezinha Pereira de Araujo, Alonso Fernandes and Vanessa Cristina Barbosa for their technical assistance, and Ricardo Ishak/CNPq for supporting the publication fee.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmicb.2022.831594/full#supplementary-material
Footnotes
References
Abad-Fernández, M., Cabrera, C., García, E., and Vallejo, A. (2014). Transient increment of HTLV-2 proviral load in HIV-1-co-infected patients during treatment intensification with raltegravir. J. Clin. Virol. 59, 204–207. doi: 10.1016/j.jcv.2013.12.010
Andrade, R. G., Ribeiro, M. A., Namen-Lopes, M. S. S., Silva, S. M. N., Basques, F. V., Ribas, J. G., et al. (2010). Evaluation of the use of real-time PCR for human T cell Lymphotropic virus 1 and 2 as a confirmatory test in screening for blood donors. Rev. Soc. Bras. Med. Trop. 43, 111–115. doi: 10.1590/S0037-86822010000200001
Bandeira, L. M., Puga, M. A. M., de Paula, V. S., Demarchi, L. H. F., Licks, G. G. C., Domingos, J. A., et al. (2020). Use of synthetic oligonucleotides for determination of HTLV-1 proviral load by real-time PCR: a helpful alternative approach in the clinical management. J. Appl. Microbiol. 129, 768–774. doi: 10.1111/jam.14646
Beilke, M. A. (2012). Retroviral coinfections: HIV and HTLV: taking stock of more than a quarter century of research. AIDS Res. Hum. Retroviruses 28, 139–147. doi: 10.1089/AID.2011.0342
Besson, J., and Kazanji, M. (2009). One-Step, multiplex, real-time PCR assay with molecular beacon probes for simultaneous detection, differentiation, and quantification of human T-cell leukemia virus types 1, 2, and 3. J. Clin. Virol. 47, 1129–1135. doi: 10.1128/JCM.02006-08
Blanco, S., Frutos, M. C., Balangero, M. C., and Gallego, S. V. (2021). Human T-lymphotropic virus type 1 infection in absence of tax gene: a challenge for molecular diagnosis. Infect. Gen. Evol. 90:104765. doi: 10.1016/j.meegid.2021.104765
Broeders, S., Huber, I., Grohmann, L., Berben, G., Taverniers, I., Mazzara, M., et al. (2014). Guidelines for validation of qualitative real-time PCR methods. Trends Food Sci. Technol. 37, 115–126. doi: 10.1016/j.tifs.2014.03.008
Bustin, S. A., Benes, V., Garson, J. A., Hellemans, J., Huggett, J., Kubista, M., et al. (2009). The MIQE guidelines: minimum information for publication of quantitative real-time PCR experiments. Clin. Chem. 55, 611–622. doi: 10.1373/clinchem.2008.112797
Campos, K. R., and Caterino-de-Araujo, A. (2020). Provirus mutations of human T-lymphotropic virus 1 and 2 (HTLV-1 and HTLV-2) in HIV-1-coinfected individuals. mSphere 30:e00923–20. doi: 10.1128/mSphere.00923-20
Campos, K. R., Gonçalves, M. G., and Caterino-de-Araujo, A. (2017a). Failures in detecting HTLV-1 and HTLV-2 in patients infected with HIV-1. AIDS Res. Hum. Retroviruses 33, 382–385, 2017. doi: 10.1089/AID.2016.0191
Campos, K. R., Gonçalves, M. G., Costa, N. A., and Caterino-de-Araujo, A. (2017b). Comparative performances of serologic and molecular assays for detecting HTLV-1 and HTLV-2 in patients infected with HIV-1. Brazilian J. Infect. Dis. 21, 297–305. doi: 10.1016/j.bjid.2017.02.005
Campos, K. R., Santos, F. L. N., Brito, V. S., Gonçalves, N. L. S., Araujo, T. H. A., Galvão-Castro, B., et al. (2020). Line immunoassay for confirmation and discrimination of human T-cell lymphotropic virus infections in inconclusive Western blot serum samples from Brazil. J. Clin. Microbiol. 58:e01384–19. doi: 10.1128/JCM.01384-19
Caterino-de-Araujo, A., and Campos, K. R. (2021). Defective particles of human T-lymphotropic virus and negative results in molecular assays. Infect. Gen. Evol. 96:105141. doi: 10.1016/j.meegid.2021.105141
Caterino-de-Araujo, A., and Gonçalves, M. G. (2021). Diagnóstico molecular de vírus T-linfotrópico humano (HTLV): histórico e estado da arte. Molecular diagnosis of human T-lymphotropic virus (HTLV): history and state of the art. BEPA Boletim Epidemiol. Paulista 18, 14–62.
Caterino-de-Araujo, A., Barbosa-Stancioli, E. F., Alonso Neto, J. B., Aragón, M. G., Galvão-Castro, B., Ishak, R., et al. (2021). Laboratory diagnosis of HTLV in Brazil: assays, flowcharts, challenges and perspectives. Rev. Soc. Bras. Med. Trop. 54, e0175–e2021. doi: 10.1590/0037-8682-0175-2021
Caterino-de-Araujo, A., Magri, M. C., Sato, N. S., Morimoto, H. K., Brigido, L. F. M., and Morimoto, A. A. (2014). Inability to detect HTLV-2-specific antibodies in a patient coinfected with HIV-1, HTLV-1, HTLV-2, and hepatitis C virus. AIDS Res. Hum. Retroviruses 30, 97–101. doi: 10.1089/AID.2013.0158
Caterino-de-Araujo, A., Sacchi, C. T., Gonçalves, M. G., Campos, K. R., Magri, M. C., Alencar, W. K., et al. (2015). Current prevalence and risk factors associated with HTLV-1 and HTLV-2 infections among HIV/AIDS patients in São Paulo, Brazil. AIDS Res. Hum. Retroviruses 31, 543–549. doi: 10.1089/AID.2014.0287
Caterino-de-Araujo, A., Santos-Fortuna, E., Zandoná-Meleiro, M. C., Suleiman, J., Calabrò, M. L., Favero, A., et al. (1998). Sensitivity of two ELISA tests in relation to western blot in detecting HTLV-I and HTLV-II infections among HIV-1-infected patients from São Paulo, Brazil. Diagn. Microbiol. Infect. Dis. 30, 173–182. doi: 10.1016/s0732-8893(97)00236-8
CGIST/DDCI/SVS, de V das 1ST, C.-G., Rosadas, C., Espinosa Miranda, A., Utsch Gonçalves, D., Caterino-de-Araujo, A., et al. (2020). Prevalência da Infecção por HTLV-1/2 no Brasil. Bol. Epidemiol. 51, 25–33.
Costa, E. A. S., Magri, M. C., and Caterino-de-Araujo, A. (2011). The best algorithm to confirm the diagnosis of HTLV-1 and HTLV-2 in at-risk individuals from São Paulo, Brazil. J. Virol. Meth. 173, 280–286. doi: 10.1016/j.jviromet.2011.02.018
da Silva Brito, V. S., Santos, F. L. N., Gonçalves, N. L. S., Araujo, T. H. A., Nascimento, D. S. V., Pereira, F. M., et al. (2018). Performance of commercially available serological screening tests for human T-cell lymphotropic virus infection in Brazil. J. Clin. Microbiol. 56:e00961–18. doi: 10.1128/JCM.00961-18
de-Araujo, A. C., Casseb, J. S. R., Xavier Neitzert, E., De Souza, M. L., Mammano, F., Del Mistro, A., et al. (1994). HTLV-I and HTLV-II infections among HIV-1 seropositive patients in São Paulo, Brazil. Eur. J. Epidemiol. 10, 165–171. doi: 10.1007/BF01730366
Dehée, A., Césaire, R., Desiré, N., Lézin, A., Bourdonné, O., Béra, O., et al. (2002). Quantitation of HTLV-I proviral load by a TaqMan real-time PCR assay. J. Virol. Methods 102, 37–51. doi: 10.1016/s0166-0934(01)00445-1
Estes, M. C., and Sevall, J. S. (2003). Multiplex PCR using real time DNA amplification for the rapid detection and quantitation of HTLV I or II. Mol. Cell. Probes 17, 59–68. doi: 10.1016/s0890-8508(03)00002-1
Furtado, M. S. B. S., Andrade, R. G., Romanelli, L. C. F., Ribeiro, M. A., Gabriel Ribas, J. G., Torres, B. E., et al. (2012). Monitoring the HTLV-1 proviral load in the peripheral blood of asymptomatic carriers and patients with HTLV-associated myelopathy/tropical spastic paraparesis from a Brazilian cohort: ROC curve analysis to establish the threshold for risk disease. J. Med. Virol. 84, 664–671. doi: 10.1002/jmv.23227
Gessain, A., and Cassar, O. (2012). Epidemiological aspects and world distribution of HTLV-1 infection. Front. Microbiol. 3:388. doi: 10.3389/fmicb.2012.00388
Gomes, Y., Caterino-de-Araujo, A., Campos, K., Gonçalves, M. G., Leite, A. C., Lima, M. A., et al. (2020). Loop-mediated isothermal amplification (LAMP) assay for rapid and accurate confirmatory diagnosis of HTLV-1/2 infection. Viruses 12:981. doi: 10.3390/v12090981
Haziot, M. E., Gascon, M. R., Assone, T., Fonseca, L. A. M., Luiz, O. C., Smid, J., et al. (2019). Detection of clinical and neurological signs in apparently asymptomatic HTLV-1 infected carriers: association with high proviral load. PLoS Negl. Trop. Dis. 13:e0006967. doi: 10.1371/journal.pntd.0006967
Jacob, F., Santos-Fortuna, E., Azevedo, R. S., and Caterino-de-Araujo, A. (2007). Performance of HTLV serological tests in diagnosing HTLV infection in high-risk of São Paulo, Brazil. Rev. Inst. Med. Trop. Sao Paulo 49, 361–364. doi: 10.1590/s0036-46652007000600005
Jacob, F., Santos-Fortuna, E., Azevedo, R. S., and Caterino-de-Araujo, A. (2008). Serological patterns for HTLV-I/II and its temporal trend in high-risk populations attended at Public Health Units of São Paulo, Brazil. J. Clin. Virol. 42, 149–155. doi: 10.1016/j.jcv.2008.01.017
Kamihira, S., Yamano, Y., Iwanaga, M., Sasaki, D., Satake, M., Okayama, A., et al. (2010). Intra- and inter-laboratory variability in human T-cell leukemia virus type-1 proviral load quantification using real-time polymerase chain reaction assays: a multi-center study. Cancer Sci. 101, 2361–2367. doi: 10.1111/j.1349-7006.2010.01720.x
Kralik, P., and Ricchi, M. (2017). A basic guide to real time PCR in microbial diagnostics: definitions, parameters, and everything. Front. Microbiol. 8:108. doi: 10.3389/fmicb.2017.00108
Kubista, M., Andrade, J. M., Bengtsson, M., Forootan, A., Jonák, J., Lind, K., et al. (2006). The real-time polymerase chain reaction. Mol. Aspects Med. 27, 95–125. doi: 10.1016/j.mam.2005.12.007
Kuramitsu, M., Sekizuka, T., Yamochi, T., Firouzi, S., Sato, T., Umeki, K., et al. (2017). Proviral features of human T cell leukemia virus type 1 in carriers with indeterminate Western blot analysis results. J. Clin. Microbiol. 55, 2838–2849. doi: 10.1128/JCM.00659-17
Lee, T. H., Chafets, D. M., Busch, M. P., and Murphy, E. L. (2004). Quantitation of HTLV-I and II proviral load using real-time quantitative PCR with SYBR Green chemistry. J. Clin. Virol. 31, 275–282. doi: 10.1016/j.jcv.2004.05.016
Machuca, A., and Soriano, V. (2000). In vivo fluctuation of HTLV-I and HTLV-II proviral load in patients receiving antiretroviral drugs. J. Acquir. Immune Defic. Syndr. 24, 189–193. doi: 10.1097/00126334-200006010-00017
Moens, B., Lopez, G., Adaui, V., Gonzalez, E., Kerremans, L., Clark, D., et al. (2009). Development and validation of a multiplex real-time PCR assay for simultaneous genotyping and human T lymphotropic virus type 1, 2, and 3 proviral load determination. J. Clin. Microbiol. 47, 3682–3691. doi: 10.1128/JCM.00781-09
Montanheiro, P., Olah, I., Fukumori, L. M. I., Smid, J., Oliveira, A. C. P., Kanzaki, L. I. B., et al. (2008). Low DNA HTLV-2 proviral load among women in São Paulo City. Virus Res. 135, 22–25. doi: 10.1016/j.virusres.2008.01.015
Morimoto, H. K., Morimoto, A. A., Reiche, E. M. V., Ueda, L. T., Matsuo, T., Reiche, F. V., et al. (2007). Difficulties in the diagnosis of HTLV-2 infection in HIV/AIDS patients from Brazil: comparative performances of serologic and molecular assays, and detection of HTLV-2b subtype. Rev. Inst. Med. Trop. Sao Paulo 49, 225–230. doi: 10.1590/s0036-46652007000400006
Murphy, E. L., Lee, T. H., Chafets, D., Nass, C. C., Wang, B., Loughlin, K., et al. (2004). Higher human T lymphotropic virus (HTLV) provirus load is associated with HTLV-I versus HTLV-II, with HTLV-II subtype A versus B, and with male sex and a history of blood transfusion. J. Infect. Dis. 190, 504–510. doi: 10.1086/422398
Okuma, K., Kuramitsu, M., Niwa, T., Taniguchi, T., Masaki, Y., Ueda, G., et al. (2020). Establishment of a novel diagnostic test algorithm for human T-cell leukemia virus type 1 infection with line immunoassay replacement of western blotting: a collaborative study for performance evaluation of diagnostic assays in Japan. Retrovirology 17:26. doi: 10.1186/s12977-020-00534-0
Paiva, A., and Casseb, J. (2015). Origin and prevalence of human T-lymphotropic virus type 1 (HTLV-1) and type 2 (HTLV-2) among indigenous populations in the Americas. Rev. Inst. Med. Trop. Sao Paulo 57, 1–13. doi: 10.1590/S0036-46652015000100001
Ramirez, E., Fernandez, J., Cartier, L., Villota, C., and Rios, M. (2003). Defective human T-cell lymphotropic virus type I (HTLV-I) provirus in seronegative tropical spastic paraparesis/HTLV-I-associated myelopathy (TSP/HAM) patients. Virus Res. 91, 231–239. doi: 10.1016/s0168-1702(02)00276-9
Raymaekers, M., Smets, R., Maes, B., and Cartuyvels, R. (2009). Checklist for optimization and validation of real-time PCR assays. J. Clin. Lab. Anal. 23, 145–151. doi: 10.1002/jcla.20307
Ribeiro, M. A., Martins, M. L., Teixeira, C., Ladeira, R., Oliveira, M. F., Januário, J. H., et al. (2012). Blocking vertical transmission of human T cell lymphotropic virus type 1 and 2 through breastfeeding interruption. Pediatr. Infect. Dis. J. 31, 1139–1143. doi: 10.1097/INF.0b013e318263215e
Rosadas, C., Cabral-Castro, M. J., Vicente, A. C. P., Peralta, J. M., and Puccioni-Sohler, M. (2013). Validation of a quantitative real-time PCR assay for HTLV-1 proviral load in peripheral blood mononuclear cells. J. Virol. Methods 193, 536–541. doi: 10.1016/j.jviromet.2013.07.040
Rosadas, C., Brites, C., Arakaki-Sanchez, D., Casseb, J., and Ishak, R. (2021a). Brazilian Protocol for Sexually Transmitted Infections 2020: human T-cell lymphotropic virus (HTLV) infection. Rev. Soc. Bras. Med. Trop. 54(Suppl I):e2020605. doi: 10.1590/0037-8682-605-2020
Rosadas, C., Menezes, M. L. B., Galvão-Castro, B., Assone, T., Miranda, A. E., Aragon, M., et al. (2021b). Blocking HTLV-1/2 silent transmission in Brazil: current public health policies and proposal of additional strategies. PLoS Negl. Trop. Dis. 15:e0009717. doi: 10.1371/journal.pntd.0009717
Takenouchi, H., Umeki, K., Sasaki, D., Yamamoto, I., Nomura, H., Takajo, I., et al. (2011). Defective human T-lymphotropic virus type 1 provirus in asymptomatic carriers. Int. J. Cancer 128, 1335–1343. doi: 10.1002/ijc.25450
Tamegão-Lopes, B. P., Rezende, P. R., Maradei-Pereira, L. M. C., and Lemos, J. A. R. (2006). HTLV-1 and HTLV-2 proviral load: a simple method using quantitative real-time PCR. Rev. Soc. Bras. Med. Trop. 39, 548–552. doi: 10.1590/s0037-86822006000600007
Tamiya, S., Matsuoka, M., Etoh, K.-I., Watanabe, T., Kamihira, S., Yamaguchi, K., et al. (1996). Two types of defective human T-lymphotropic virus type I provirus in Adult T-cell Leukemia. Blood 88, 3065–3073.
Tuke, P. W., Luton, P., and Garson, J. A. (1992). Differential diagnosis of HTLV-I and HTLV-II infections by restriction enzyme analysis of “nested” PCR products. J. Virol. Methods 40, 163–173. doi: 10.1016/0166-0934(92)90065-l
Waters, A., Oliveira, A. L. A., Coughlan, S., Venecia, C., Schor, D., Leite, A. C., et al. (2011). Multiplex real-time PCR for the detection and quantitation of HTLV-1 and HTLV-2 proviral load: addressing the issue of indeterminate HTLV results. J. Clin. Virol. 52, 38–44. doi: 10.1016/j.jcv.2011.05.022
Keywords: HTLV-1, HTLV-2, multiplex qPCR, pol, tax
Citation: Gonçalves MG, Fukasawa LO, Campos KR, Higa FT and Caterino-de-Araujo A (2022) Development and Validation of Multiplex Quantitative Real-Time PCR Assays for Simultaneous Detection and Differentiation of HTLV-1 and HTLV-2, Using Different PCR Platforms and Reagent Brands. Front. Microbiol. 13:831594. doi: 10.3389/fmicb.2022.831594
Received: 08 December 2021; Accepted: 26 January 2022;
Published: 15 March 2022.
Edited by:
Antonio C. R. Vallinoto, Federal University of Pará, BrazilReviewed by:
Maria Alice Freitas Queiroz, Federal University of Pará, BrazilCarlos Alberto M. Carvalho, Universidade do Estado do Pará, Brazil
Eurico Arruda, University of São Paulo Ribeirão Preto, Brazil
Copyright © 2022 Gonçalves, Fukasawa, Campos, Higa and Caterino-de-Araujo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Maria Gisele Gonçalves, bWFyaWEuZ29uY2FsdmVzQGlhbC5zcC5nb3YuYnI=; Adele Caterino-de-Araujo, YWRlbGUuY2F0ZXJpbm9AaWFsLnNwLmdvdi5icg==