 Jingru Ren1†
Jingru Ren1† Chenxi Pan1
Chenxi Pan1 Yuqian Li1
Yuqian Li1 Lanting Li1Ping Hua1Ligang Xu1
Lanting Li1Ping Hua1Ligang Xu1 Li Zhang2
Li Zhang2 Wenbin Zhang3
Wenbin Zhang3 Pingyi Xu4
Pingyi Xu4 Weiguo Liu1*
Weiguo Liu1*- 1Department of Neurology, The Affiliated Brain Hospital of Nanjing Medical University, Nanjing, China
- 2Department of Geriatrics, The Affiliated Brain Hospital of Nanjing Medical University, Nanjing, China
- 3Department of Neurosurgery, The Affiliated Brain Hospital of Nanjing Medical University, Nanjing, China
- 4Department of Neurology, First Affiliated Hospital of Guangzhou Medical University, Guangzhou, China
Objective: Patients with Parkinson’s disease (PD) are commonly classified into subtypes based on motor symptoms. The aims of the present study were to determine the consistency between PD motor subtypes, to assess the stability of PD motor subtypes over time, and to explore the variables influencing PD motor subtype stability.
Methods: This study was part of a longitudinal study of de novo PD patients at a single center. Based on three different motor subtype classification systems proposed by Jankovic, Schiess, and Kang, patients were respectively categorized as tremor-dominant/indeterminate/postural instability and gait difficulty (TD/indeterminate/PIGD), TDS/mixedS/akinetic-rigidS (ARS), or TDK/mixedK/ARK at baseline evaluation and then re-assessed 1 month later. Demographic and clinical characteristics were recorded at each evaluation. The consistency between subtypes at baseline evaluation was assessed using Cohen’s kappa coefficient (κ). Additional variables were compared between PD subtype groups using the two-sample t-test, Mann–Whitney U-test or Chi-squared test.
Results: Of 283 newly diagnosed, untreated PD patients, 79 were followed up at 1 month. There was fair agreement between the Jankovic, Schiess, and Kang classification systems (κS = 0.383 ± 0.044, κK = 0.360 ± 0.042, κSK = 0.368 ± 0.038). Among the three classification systems, the Schiess classification was the most stable and the Jankovic classification was the most unstable. The non-motor symptoms questionnaire (NMSQuest) scores differed significantly between PD patients with stable and unstable subtypes based on the Jankovic classification (p = 0.008), and patients with a consistent subtype had more severe NMSQuest scores than patients with an inconsistent subtype.
Conclusion: Fair consistency was observed between the Jankovic, Schiess, and Kang classification systems. For the first time, non-motor symptoms (NMSs) scores were found to influence the stability of the TD/indeterminate/PIGD classification. Our findings support combining NMSs with motor symptoms to increase the effectiveness of PD subtypes.
Introduction
The clinical presentations of Parkinson’s disease (PD) are considerably heterogeneous (Armstrong and Okun, 2020). It is difficult to delineate if such variability between PD patients reflects the various manifestations of a unitary disease or represents different disease subtypes driven by underlying pathological and pathophysiological distinctions (Calne, 1989). The solution to this problem is generally thought to be through the use of PD subtypes.
Classification of PD subtypes is based on empirical clinical observations of prominent motor symptoms. At present, the recognized PD motor subtype classifications, including tremor-dominant/indeterminate/postural instability and gait difficulty (TD/indeterminate/PIGD) put forward by Jankovic and two classifications of the TD/mixed/akinetic-rigid (AR) classification system proposed by Schiess and Kang (Jankovic et al., 1990; Schiess et al., 2000; Kang et al., 2005), are widely used (Guan et al., 2017; Choi et al., 2018; Erro et al., 2019; Lian et al., 2019; Polychronis et al., 2019; Ren et al.,2020a,b). Although numerous additional subtypes based on data-driven approaches have been subsequently proposed (Graham and Sagar, 1999; van Rooden et al., 2010; Fereshtehnejad et al., 2015), the above three classifications occupy a dominant position in clinical practice and scientific research and have entered the conventional lexicon of clinicians.
Accurately subtyping patients is an indispensable step for research on disease mechanisms, for prodromal and clinical trial design and, in particular, for the development of tailored treatments. However, the terminology used to describe PD motor subtypes has overlapping boundaries, which can result in confusion and lead to an extensively inaccurate literature (Kotagal, 2016). A recent study found that the consistency between the Jankovic classification and Schiess classification is poor (Erro et al., 2019). In addition, temporal instability of these two classifications in de novo PD patients has been reported (Simuni et al., 2016; Erro et al., 2019).
To our knowledge, studies of the consistency of the Kang, Jankovic, and Schiess classifications, or of the stability of the Kang classification alone, have not been performed. It is also unknown whether factors besides the disease course influence the stability of motor subtypes (Simuni et al., 2016; Eisinger et al., 2017, 2020). To address these gaps, this study aimed to examine the consistency between the TD/indeterminate/PIGD (Jankovic classification) and two TD/mixed/AR classification systems (Schiess and Kang classification) in 283 de novo PD patients at baseline and then determine the stability of the three classification systems over 1-month follow-up in a subgroup of 79 patients. In addition, we aimed to identify variables that affected the stability of the motor subtypes.
Methods
Participants
This study was part of a longitudinal study of de novo PD patients conducted at the Department of Neurology, Affiliated Brain Hospital of Nanjing Medical University from January 2012 to October 2020. All patients who came to the clinic were examined by a movement disorder specialist. A total of 283 de novo PD patients fulfilled all the study inclusion and exclusion criteria, of which 27.9% had evaluation data for the first month of follow-up. The inclusion criteria were: (1) the presence of bradykinesia plus an additional clinical motor sign, namely resting tremor, rigidity, or postural instability; (2) be newly diagnosed with PD based on the United Kingdom Parkinson’s Disease Society Brain Bank clinical diagnostic criteria (Gibb and Lees, 1988); (3) be untreated; (4) have early- or middle-stage PD (modified H-Y stage ≤3); (5) have more than a 30% improvement rate in the Unified Parkinson’s Disease Rating Scale (UPDRS) part III scores by the standard acute levodopa challenge test; (6) receive follow-up through hospital visits for at least 1 year, especially for motor symptoms assessment; and (7) have detailed clinical evaluation information available. The exclusion criteria were: (1) the presence of atypical or secondary Parkinsonism disorders; (2) previous brain magnetic resonance imaging (MRI) scans with obvious clinically significant lesions; and (3) severe chronic diseases.
This study was approved by the Medical Ethics Committee of the Affiliated Brain Hospital of Nanjing Medical University (2011-KY003, 2015-KY030, and 2019-KY019-01) and conducted in accordance with the ethical standards outlined in the Helsinki Declaration of 1964. All subjects provided written informed consent before participating in this study.
Clinical Evaluation
All baseline clinical evaluations were performed before initiation of dopaminergic replacement therapy (DRT), which includes levodopa (L-DOPA) and dopamine receptor agonists (DAs). After starting DRT, 1-month follow-up evaluations were performed in the “practically defined OFF state” (Langston et al., 1992) and the levodopa equivalent daily dose (LEDD) was calculated (Tomlinson et al., 2010). Patients’ demographic and clinical characteristics were recorded at the baseline and 1-month follow-up visits. Demographic data included age, gender, formal education in years, age at onset, and years of PD symptom onset duration. Motor dysfunction and disease severity were assessed by the UPDRS part II, III and the modified Hoehn and Yahr (H-Y) stages, respectively. General cognition, mood and sleep were measured using the Mini-Mental State Examination (MMSE), Montreal Cognitive Assessment (MoCA), Hamilton Depression Scale (HAMD), Hamilton Anxiety Scale (HAMA), and the Parkinson Disease Sleep Scale (PDSS), respectively. Non-motor symptoms (NMSs) were assessed using the non-motor symptoms questionnaire (NMSQuest) (Chaudhuri et al., 2006).
Subtype Classification
UPDRS items selected according to a published formula were used to classify patients as TD/indeterminate/PIGD or TD/mixed/AR motor subtypes (Table 1; Jankovic et al., 1990; Schiess et al., 2000; Kang et al., 2005). For clarity, TDS/mixedS/ARS refers to the classification proposed by Schiess whereas TDK/mixedK/ARK refers to the classification proposed by Kang.
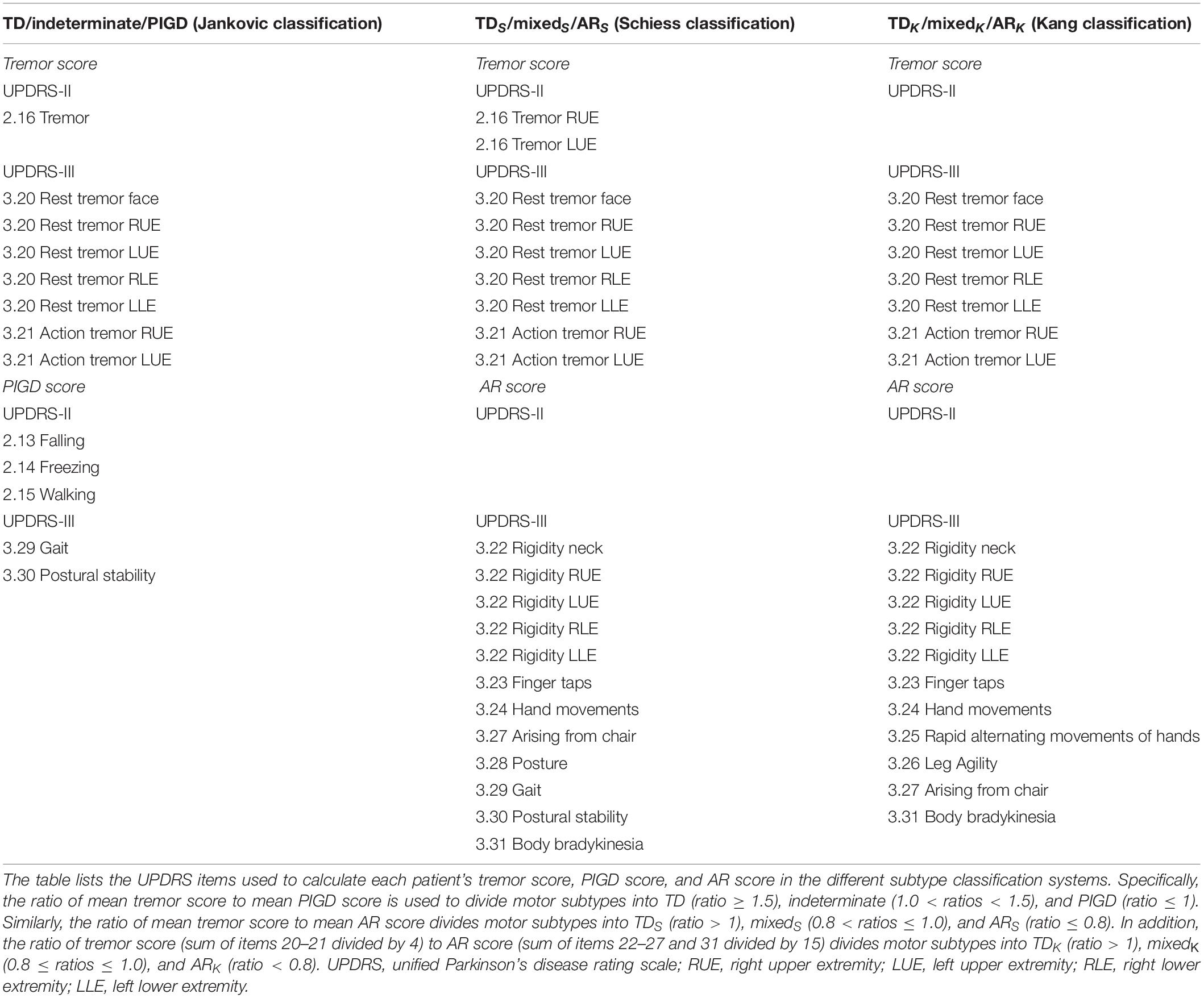
Table 1. Items used for the tremor-dominant/indeterminate/postural instability and gait difficulty (TD/indeterminate/PIGD) and TD/mixed/akinetic-rigid (AR) classifications.
Statistical Analysis
Statistical analysis was conducted using IBM SPSS software version 25.0. The level of statistical significance was P < 0.05. The Kolmogorov-Smirnov test was used to assess the normality of the data. Differences in gender between groups were assessed using the chi-square test. Differences in baseline demographic and clinical variables other than gender between patients with and without 1-month follow-up assessment and between patients with stable and unstable subtypes in the TD/indeterminate/PIGD classification system were assessed using the two-sample t-test when the data were normally distributed; otherwise, the Mann–Whitney U-test was used. Cohen’s kappa coefficient (κ) was used to analyze agreement between the Jankovic, Schiess, and Kang classification systems at baseline. A κ value < 0.00 represents poor agreement, 0.00–0.20 represents slight agreement, 0.21–0.40 represents fair agreement, 0.41–0.60 represents moderate agreement, 0.61–0.80 represents substantial agreement and 0.81–1.00 represents almost perfect agreement (Landis and Koch, 1977).
Results
Demographic and Clinical Characteristics
Table 2 presents patients’ baseline demographic and clinical characteristics. Of the 283 PD patients enrolled in this study, clinical evaluation data at 1-month follow-up were available for 79 (27.9%). There were no significant differences in terms of demographic characteristics (age, gender, education, age at PD onset, and duration of symptom onset), motor symptoms (UPDRS part II, UPDRS part III, and modified H-Y stage), or NMSs (MMSE, MoCA, HAMD, HAMA, PDSS, and NMSQuest) between patients with and without 1-month follow-up data, indicating that the high drop-out rate did not affect the results. In addition, the demographic and clinical characteristics of the 79 PD patients at 1-month follow-up are provided in Supplementary Table 1. At 1-month follow-up, LEDD for 79 patients was 74.5 ± 4.2 mg.
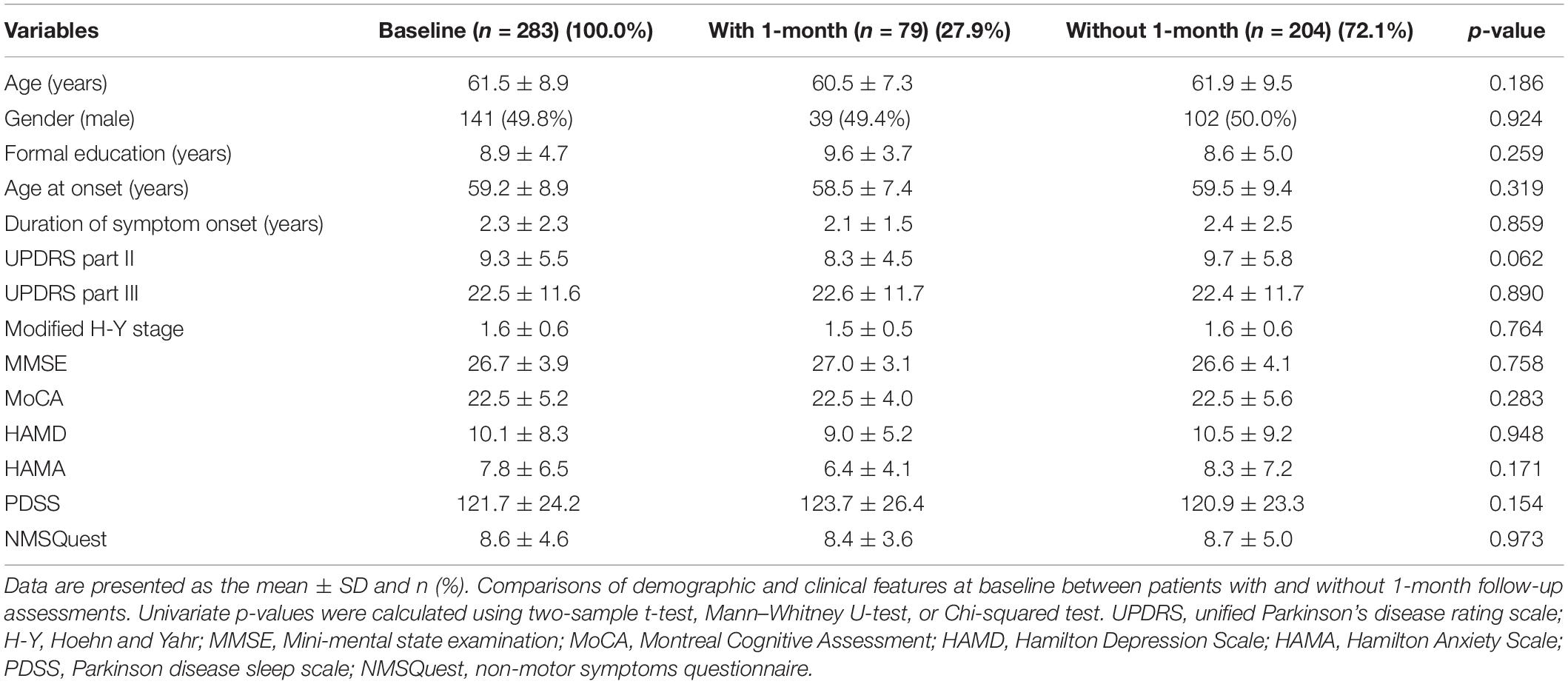
Table 2. Baseline demographic and clinical characteristics.
Baseline Consistency Between the Jankovic, Schiess, and Kang Classification Systems
At baseline, 83 (29.3%) patients were classified as TD, 159 (56.2%) as PIGD and 41 (14.5%) as indeterminate in TD/indeterminate/PIGD subtypes of the Jankovic classification. Schiess and Kang have each proposed method for categorizing patients into TD/mixed/AR subtypes. Using the Schiess classification, the majority subtype was ARS with 213 cases (75.3%), followed by 49 (17.3%) TDS cases and 21 (7.4%) mixedS cases. Using the classification proposed by Kang, there were 124 (43.8%) TDK cases, 135 (47.7%) ARK cases, and 24 (8.5%) mixedK cases. There was fair agreement between the Jankovic, Schiess, and Kang classification systems (κS = 0.383 ± 0.044, κK = 0.360 ± 0.042, κSK = 0.368 ± 0.038) (Table 3).
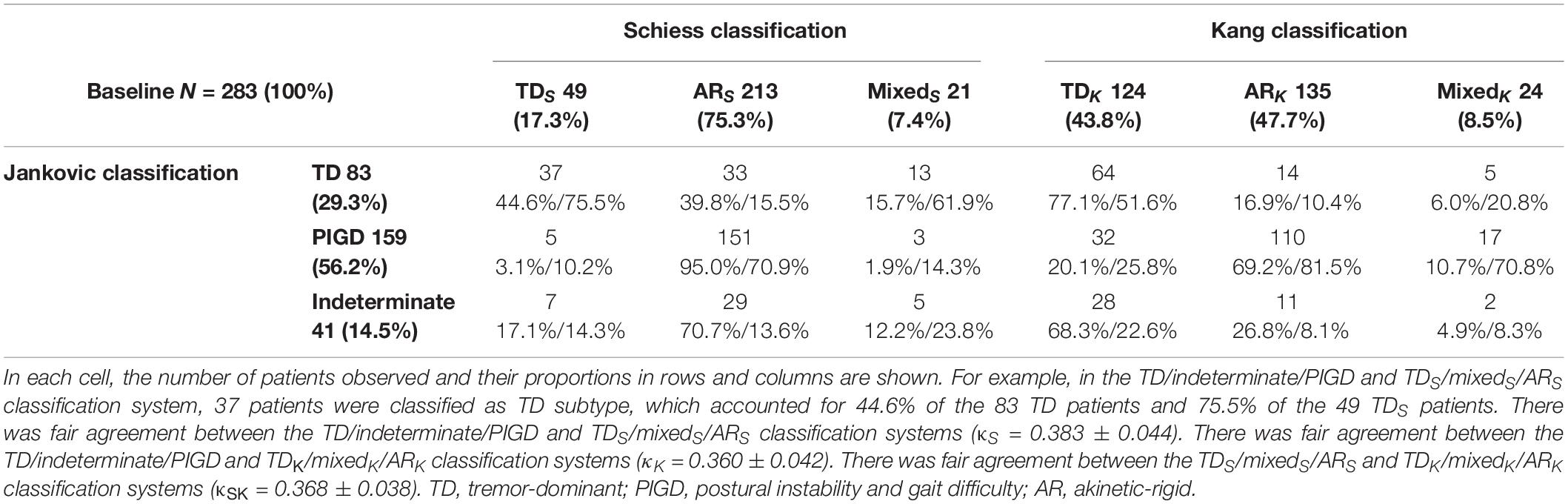
Table 3. Baseline consistency between the Jankovic, Schiess, and Kang classification systems.
Stability of the Jankovic, Schiess, and Kang Classification Systems
Changes in the Jankovic, Schiess, and Kang classification systems from baseline to 1-month follow-up among the 79 patients with longitudinal data are presented in Table 4. Using the Jankovic classification, 12 (54.5%) of the initially classified TD subtype cases and 37 (72.5%) of the initially classified PIGD subtype cases remained stable at 1-month follow-up. Using the Schiess classification, all of the initially classified TDS subtype cases and 54 (83.1%) of the ARS subtype cases were consistent at 1-month follow-up. Using the Kang classification, 15 (75.0%) of the initially classified TDK cases and 35 (68.6%) of the initially classified ARK cases were stable at 1-month follow-up. Among the three motor subtype classification systems, in the Schiess classification, the number of PD patients with stable motor subtypes from baseline to 1-month follow-up (65 cases in total, including 11 cases of TDS subtype and 54 cases of ARS subtype) was the largest, while in the Jankovic classification, the number of PD patients with stable motor subtypes (49 cases in total, including 12 cases of TD subtype and 37 cases of PIGD subtype) was the smallest. Therefore, the Schiess classification was the most stable and thus might be the most valid motor classification system, whereas the Jankovic classification was the most unstable.
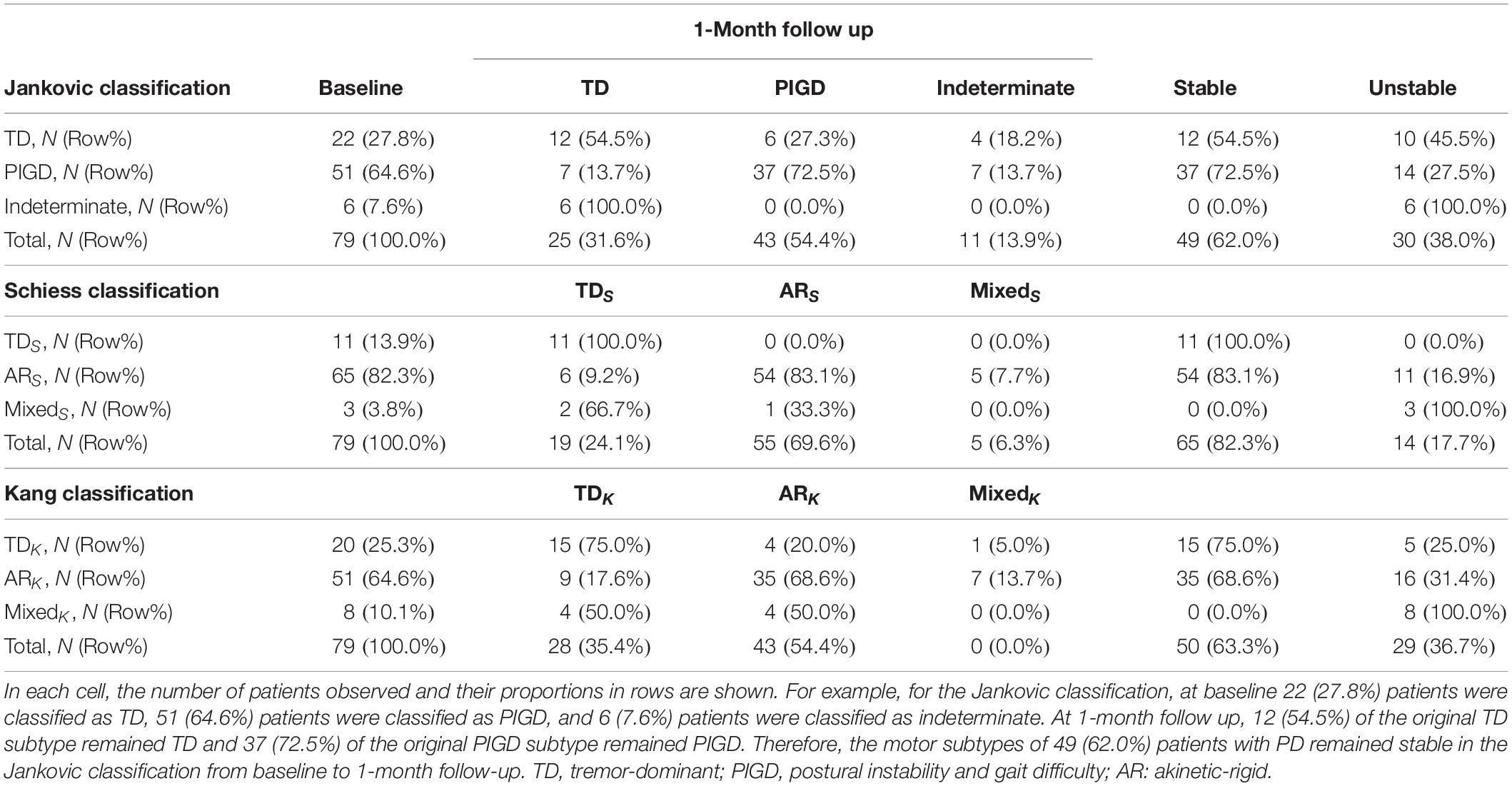
Table 4. Stability of the Jankovic, Schiess, and Kang classification systems from baseline to 1-month follow-up.
As the TD/indeterminate/PIGD classification system proposed by Jankovic was the most unstable, the baseline demographics and clinical characteristics of patients with stable and unstable subtypes were compared in this classification system to further analyze potential factors affecting the stability of PD motor subtypes. No significant differences in demographic or clinical characteristics between patients with stable and unstable subtypes, other than NMSQuest scores (p = 0.008), were observed. Patients with consistent subtypes had more severe NMSQuest scores than patients with inconsistent subtypes (Table 5).
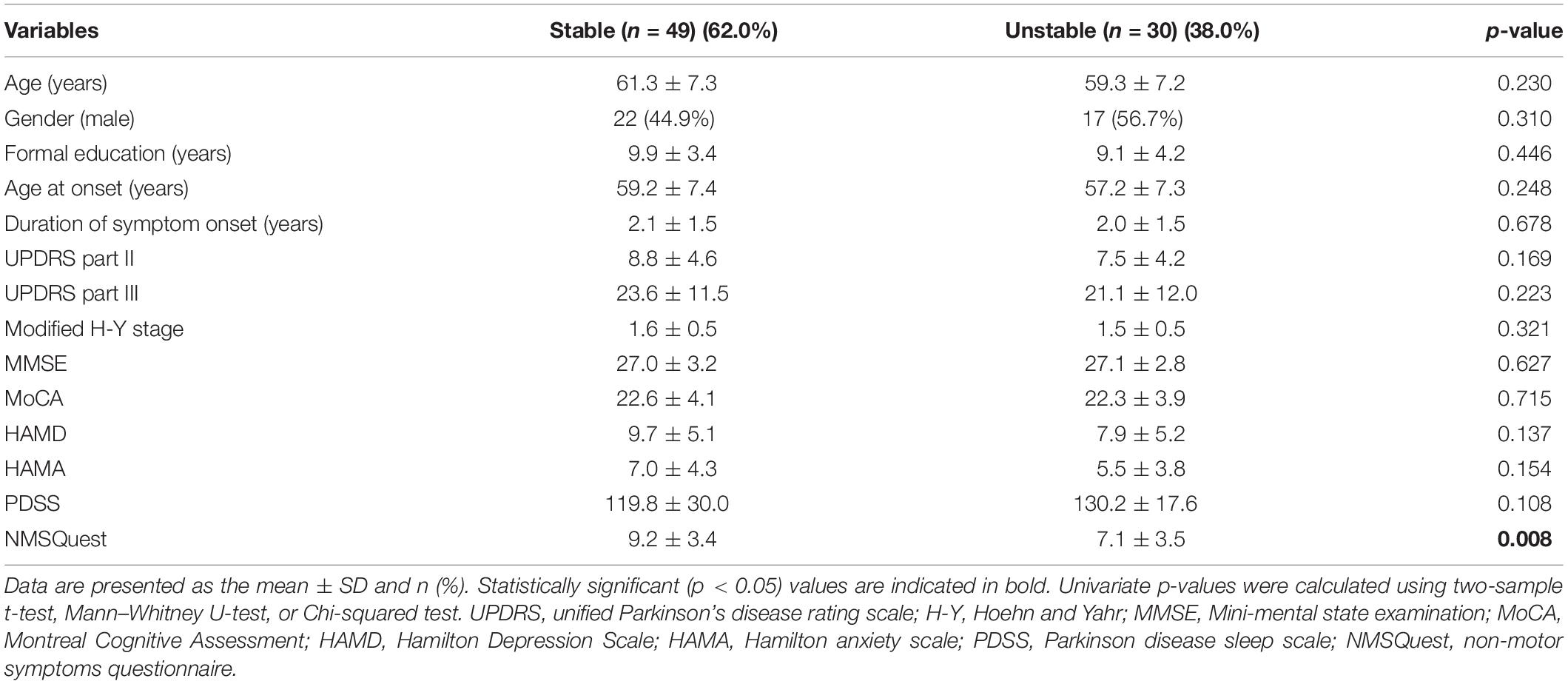
Table 5. Comparisons of baseline demographic and clinical characteristics between patients with stable and unstable subtypes in the Jankovic classification.
Discussion
To the best of our knowledge, this is the first study to assess the consistency and stability of the Jankovic, Schiess, and Kang classification systems (TD/indeterminate/PIGD and TD/mixed/AR, respectively) in de novo PD patients at a single center. We found that the TD/indeterminate/PIGD and the two TD/mixed/AR classifications have fair consistency, suggesting that a patient may be categorized as one subtype based on one classification system, but not according to another classification system. In addition, changes in subtype classification from baseline to 1-month follow-up indicated that there are other factors influencing the stability of motor subtype classification besides the course of the disease. Further, this is the first study to report that NMSs strongly affect the stability of the TD/indeterminate/PIGD classification.
Parkinson’s disease (PD) subtype identification is recognized as an essential research focus, as it may provide better paths for subtype-specific biomarkers and clinical trial designs, especially in terms of long-term prognosis (Sieber et al., 2014; Fereshtehnejad and Postuma, 2017). If PD subtypes predict a unique clinical course and are mutually independent and exclusive, they are prognostically relevant (Kotagal, 2016; Espay et al., 2017). However, due to the lack of reliable and effective subtype definition criteria, the PD motor subtype classifications lack these key elements. In the absence of these characteristics, it is not difficult to understand the inconsistency between PD motor subtype classification taxonomy and instability. Motor subtype classification systems follow a similar principle, classifying PD patients based on the ratio of two UPDRS subscores. However, different motor subtype classification systems use different UPDRS items and cutoff rates to define subtypes, suggesting that patients may be classified as tremor subtypes according to one motor subtype classification method but PIGD or AR subtypes according to another method. As a result, the consistency between different motor subtypes is fair. In a previous study, the Jankovic and Schiess classifications were found to poorly overlap in 103 de novo PD patients (Erro et al., 2019). By contrast, in the present study of 283 patients with de novo PD, we found that the Jankovic classification is fairly consistent with the two motor subtype classifications of TD/mixed/AR. Although differences in terms of sample size may lead to slightly different results, the overall consistency between different subtypes requires improvement. In addition, the instability of PD motor subtypes has been previously demonstrated (Simuni et al., 2016; Erro et al., 2019). The Parkinson’s Progression Biomarker Initiative (PPMI) consortium has decided to subdivide PD patients into TD and non-TD (PIGD and indeterminate) subtypes in order to reduce instability of the motor subtypes (Simuni et al., 2016). However, based on the Jankovic classification of similar cohorts of de novo PD patients, the prevalence of the TD phenotype varies from 29.3% as reported in the present study to 44.6% in an ongoing prospective research project (Erro et al., 2019) to 55.1% in the Deprenyl and Tocopherol Antioxidative Therapy of Parkinsonism (DATATOP) (Jankovic et al., 1990) cohort to 71.3% of the PPMI cohort (Simuni et al., 2016). Considering the large difference in the prevalence of TD subtypes, although stratification based solely on the variable of tremors will slightly increase stability, it may also increase the inconsistency of subtypes to a certain extent and generate confusion. Therefore, the consistency and stability of PD subtypes still need to be resolved, and powerful and validated criteria for PD subtype definition may be one of the most effective methods to achieve this.
The influence of DRT on the instability of PD motor subtypes warrants careful consideration. Although ‘practically defined OFF state’ is the conventional method for measuring the baseline degree of motor disability (Langston et al., 1992), the effect of DRT may be longer than the standard overnight flushing effect (Anderson and Nutt, 2011). In addition, its treatment effect on bradykinesia and rigidity is better than its effect on tremors. Therefore, a certain proportion of PIGD or AR patients were shifted into the TD group at 1-month follow-up. However, this does not explain the transfer of TD patients to other subtypes, which indicates that the instability of the motor subtype classification system does not depend mainly on DRT, which is consistent with previous reports (Simuni et al., 2016; Erro et al., 2019). There may be other potential factors explaining the observed instability. UPDRS provides operating standards for assessing the severity of symptoms; however, to some extent, it still depends on the evaluators. In addition, the TD subscores involved in defining motor subtypes in PD patients may fluctuate significantly at evaluations due to emotions such as worry and embarrassment. These factors may partially explain the observed instability of PD motor subtypes and the differences between studies.
Importantly, the stability of motor subtype classifications obtained through empirical clinical observation is greatly affected by disease duration. Recent studies have reported high variability in motor subtypes over 1, 2, and 4 years of follow-up in de novo PD cohorts (Simuni et al., 2016; Erro et al., 2019). Additionally, prospective and retrospective research of empirical motor subtype classification has shown that, over 8 years of follow-up, most TD subtypes eventually become the PIGD subtype (Alves et al., 2006; Josephs et al., 2006; Selikhova et al., 2009). However, a recent review suggested that disease course is insufficient to explain the shifts in motor subtypes (Nutt, 2016). In this context, the present study chose to reassess patients at one month to minimize the influence of disease duration so as to identify other potential variables that affect the stability of PD motor subtypes. Since the TD/indeterminate/PIGD classification had the worst stability among the three classifications, this classification was selected for further analysis of the factors influencing stability. Ultimately, we demonstrated that NMSs affect the stability of the TD/indeterminate/PIGD classification. Although PD motor subtype classification systems based on a single taxonomic factor ignore the non-motor features of PD, a longitudinal study confirmed that NMSs are significant indicators of prognosis and crucial characteristics of the definitions of PD subtypes (de Lau et al., 2014). Thus, inclusion of NMSs in the classification systems may result in more stable subtypes (Marras and Chaudhuri, 2016; Qian and Huang, 2019). Recently, novel PD clinical subtypes were identified using three critical NMSs (mild cognitive impairment, orthostatic hypotension, and rapid eye movement behavior disorder) and motor severity as key determinants in prospective cohorts (Fereshtehnejad et al., 2015), and then validated in the PPMI cohort with de novo PD patients (Fereshtehnejad et al., 2017). In light of the increasing importance of NMSs and the discovery of the novel subtype classification system, it may be time to redefine the entire motor subtype classification system of PD and its nomenclature.
When interpreting our findings, several limitations must be considered. First, our participants were de novo PD patients selected from a single center study. Thus, our cohort does not represent the entire PD patient population and our results may not be generalizable. However, differences in prevalence of TD subtypes were found in the similarly designed studies described above, which suggests that the type of recruitment may have a small influence on the results. Additionally, the sample size of this study is sufficiently large. Second, because the initial study design of the de novo PD cohort was based on annual follow-up to define biomarkers of PD diagnosis and progression, and the first month of follow-up data was collected due to increased attention to the instability of PD motor subtypes in recent years, there was a high drop-out rate for evaluation. However, there were no significant differences in baseline demographic and clinical features between patients with and without 1-month follow-up, suggesting that drop-out did not greatly affect the results. Third, although we compared demographic and clinical characteristics of patients with consistent and inconsistent subtypes, we did not account for variables such as genetics, environment, or other disease attributes. Fourth, de novo PD patients may still be mixed with patients with atypical parkinsonisms. Therefore, it is necessary to extend the longitudinal follow-up time to distinguish atypical parkinsonisms from PD.
Conclusion
Fair consistency was observed between TD/indeterminate/PIGD and the two TD/mixed/AR classifications, indicating that patients may be divided into one subtype according to one classification system but not according to another classification system. Furthermore, for the first time, NMSs were found to influence the stability of TD/indeterminate/PIGD classification. Our findings strongly suggest that combining non-motor and conventional motor symptoms will improve the value of PD subtypes.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Ethics Statement
The studies involving human participants were reviewed and approved by Ethics Committee of the Affiliated Brain Hospital of Nanjing Medical University. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
All authors listed have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
Funding
This work was supported by the National Key Research and Development Program of China, Grant/Award Numbers: 2017YFC1310302 and 2016YFC1306600, General Program of National Natural Science Foundation of China, Grant/Award Number: 81571348, Science and Technology Program of Jiangsu Province, Grant/Award Number: BE2019611, and General Program of Jiangsu Provincial Natural Science Foundation of China, Grant/Award Number: BK20151077.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We would like to thank the patients for their participation and their families for their support and cooperation.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnins.2021.637896/full#supplementary-material
References
Alves, G., Larsen, J. P., Emre, M., Wentzel-Larsen, T., and Aarsland, D. (2006). Changes in motor subtype and risk for incident dementia in Parkinson’s disease. Mov. Disord. 21, 1123–1130. doi: 10.1002/mds.20897
Anderson, E., and Nutt, J. (2011). The long-duration response to levodopa: phenomenology, potential mechanisms and clinical implications. Parkinsonism Relat. Disord. 17, 587–592. doi: 10.1016/j.parkreldis.2011.03.014
Armstrong, M. J., and Okun, M. S. (2020). Diagnosis and treatment of Parkinson disease: a review. JAMA 323, 548–560. doi: 10.1001/jama.2019.22360
Calne, D. B. (1989). Is “Parkinson’s disease” one disease? J. Neurol. Neurosurg. Psychiatry 52(Suppl), 18–21. doi: 10.1136/jnnp.52.suppl.18
Chaudhuri, K. R., Martinez-Martin, P., Schapira, A. H., Stocchi, F., Sethi, K., Odin, P., et al. (2006). International multicenter pilot study of the first comprehensive self-completed nonmotor symptoms questionnaire for Parkinson’s disease: the NMSQuest study. Mov. Disord. 21, 916–923. doi: 10.1002/mds.20844
Choi, S. M., Kim, B. C., Cho, B. H., Kang, K. W., Choi, K. H., Kim, J. T., et al. (2018). Comparison of two motor subtype classifications in de novo Parkinson’s disease. Parkinsonism Relat. Disord. 54, 74–78. doi: 10.1016/j.parkreldis.2018.04.021
de Lau, L. M., Verbaan, D., van Rooden, S. M., Marinus, J., and van Hilten, J. J. (2014). Relation of clinical subtypes in Parkinson’s disease with survival. Mov. Disord. 29, 150–151. doi: 10.1002/mds.25652
Eisinger, R. S., Hess, C. W., Martinez-Ramirez, D., Almeida, L., Foote, K. D., Okun, M. S., et al. (2017). Motor subtype changes in early Parkinson’s disease. Parkinsonism Relat. Disord. 43, 67–72. doi: 10.1016/j.parkreldis.2017.07.018
Eisinger, R. S., Martinez-Ramirez, D., Ramirez-Zamora, A., Hess, C. W., Almeida, L., Okun, M. S., et al. (2020). Parkinson’s disease motor subtype changes during 20 years of follow-up. Parkinsonism Relat. Disord. 76, 104–107. doi: 10.1016/j.parkreldis.2019.05.024
Erro, R., Picillo, M., Amboni, M., Savastano, R., Scannapieco, S., Cuoco, S., et al. (2019). Comparing postural instability and gait disorder and akinetic-rigid subtyping of Parkinson disease and their stability over time. Eur. J. Neurol. 26, 1212–1218. doi: 10.1111/ene.13968
Espay, A. J., Schwarzschild, M. A., Tanner, C. M., Fernandez, H. H., Simon, D. K., Leverenz, J. B., et al. (2017). Biomarker-driven phenotyping in Parkinson’s disease: a translational missing link in disease-modifying clinical trials. Mov. Disord. 32, 319–324. doi: 10.1002/mds.26913
Fereshtehnejad, S. M., and Postuma, R. B. (2017). Subtypes of Parkinson’s disease: what do they tell us about disease progression? Curr. Neurol. Neurosci. Rep. 17:34. doi: 10.1007/s11910-017-0738-x
Fereshtehnejad, S. M., Romenets, S. R., Anang, J. B., Latreille, V., Gagnon, J. F., and Postuma, R. B. (2015). New clinical subtypes of Parkinson disease and their longitudinal progression: a prospective cohort comparison with other phenotypes. JAMA Neurol. 72, 863–873. doi: 10.1001/jamaneurol.2015.0703
Fereshtehnejad, S. M., Zeighami, Y., Dagher, A., and Postuma, R. B. (2017). Clinical criteria for subtyping Parkinson’s disease: biomarkers and longitudinal progression. Brain 140, 1959–1976. doi: 10.1093/brain/awx118
Gibb, W. R., and Lees, A. J. (1988). The relevance of the Lewy body to the pathogenesis of idiopathic Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 51, 745–752. doi: 10.1136/jnnp.51.6.745
Graham, J. M., and Sagar, H. J. (1999). A data-driven approach to the study of heterogeneity in idiopathic Parkinson’s disease: identification of three distinct subtypes. Mov. Disord. 14, 10–20. doi: 10.1002/1531-8257(199901)14:1<10::aid-mds1005<3.0.co;2-4
Guan, X., Zeng, Q., Guo, T., Wang, J., Xuan, M., Gu, Q., et al. (2017). Disrupted functional connectivity of basal ganglia across tremor-dominant and akinetic/rigid-dominant Parkinson’s disease. Front. Aging Neurosci. 9:360. doi: 10.3389/fnagi.2017.00360
Jankovic, J., McDermott, M., Carter, J., Gauthier, S., Goetz, C., Golbe, L., et al. (1990). Variable expression of Parkinson’s disease: a base-line analysis of the DATATOP cohort. the Parkinson study group. Neurology 40, 1529–1534. doi: 10.1212/wnl.40.10.1529
Josephs, K. A., Matsumoto, J. Y., and Ahlskog, J. E. (2006). Benign tremulous parkinsonism. Arch. Neurol. 63, 354–357. doi: 10.1001/archneur.63.3.354
Kang, G. A., Bronstein, J. M., Masterman, D. L., Redelings, M., Crum, J. A., and Ritz, B. (2005). Clinical characteristics in early Parkinson’s disease in a central California population-based study. Mov. Disord. 20, 1133–1142. doi: 10.1002/mds.20513
Kotagal, V. (2016). Is PIGD a legitimate motor subtype in Parkinson disease? Ann. Clin. Transl. Neurol. 3, 473–477. doi: 10.1002/acn3.312
Landis, J. R., and Koch, G. G. (1977). The measurement of observer agreement for categorical data. Biometrics 33, 159–174. doi: 10.2307/2529310
Langston, J. W., Widner, H., Goetz, C. G., Brooks, D., Fahn, S., Freeman, T., et al. (1992). Core assessment program for intracerebral transplantations (CAPIT). Mov. Disord. 7, 2–13. doi: 10.1002/mds.870070103
Lian, T. H., Guo, P., Zuo, L. J., Hu, Y., Yu, S. Y., Yu, Q. J., et al. (2019). Tremor-dominant in Parkinson disease: the relevance to iron metabolism and inflammation. Front. Neurosci. 13:255. doi: 10.3389/fnins.2019.00255
Marras, C., and Chaudhuri, K. R. (2016). Nonmotor features of Parkinson’s disease subtypes. Mov. Disord. 31, 1095–1102. doi: 10.1002/mds.26510
Nutt, J. G. (2016). Motor subtype in Parkinson’s disease: different disorders or different stages of disease? Mov. Disord. 31, 957–961. doi: 10.1002/mds.26657
Polychronis, S., Niccolini, F., Pagano, G., Yousaf, T., and Politis, M. (2019). Speech difficulties in early de novo patients with Parkinson’s disease. Parkinsonism Relat. Disord. 64, 256–261. doi: 10.1016/j.parkreldis.2019.04.026
Qian, E., and Huang, Y. (2019). Subtyping of Parkinson’s disease – where are we up to? Aging Dis. 10, 1130–1139. doi: 10.14336/ad.2019.0112
Ren, J., Hua, P., Li, Y., Pan, C., Yan, L., Yu, C., et al. (2020a). Comparison of three motor subtype classifications in de novo Parkinson’s disease patients. Front. Neurol. 11:601225. doi: 10.3389/fneur.2020.601225
Ren, J., Hua, P., Pan, C., Li, Y., Zhang, L., Zhang, W., et al. (2020b). Non-motor symptoms of the postural instability and gait difficulty subtype in de novo Parkinson’s disease patients: a cross-sectional study in a single center. Neuropsychiatr. Dis. Treat. 16, 2605–2612. doi: 10.2147/ndt.S280960
Schiess, M. C., Zheng, H., Soukup, V. M., Bonnen, J. G., and Nauta, H. J. (2000). Parkinson’s disease subtypes: clinical classification and ventricular cerebrospinal fluid analysis. Parkinsonism Relat. Disord. 6, 69–76. doi: 10.1016/s1353-8020(99)00051-6
Selikhova, M., Williams, D. R., Kempster, P. A., Holton, J. L., Revesz, T., and Lees, A. J. (2009). A clinico-pathological study of subtypes in Parkinson’s disease. Brain 132(Pt 11), 2947–2957. doi: 10.1093/brain/awp234
Sieber, B. A., Landis, S., Koroshetz, W., Bateman, R., Siderowf, A., Galpern, W. R., et al. (2014). Prioritized research recommendations from the National institute of neurological disorders and stroke Parkinson’s disease 2014 conference. Ann. Neurol. 76, 469–472. doi: 10.1002/ana.24261
Simuni, T., Caspell-Garcia, C., Coffey, C., Lasch, S., Tanner, C., and Marek, K. (2016). How stable are Parkinson’s disease subtypes in de novo patients: analysis of the PPMI cohort? Parkinsonism Relat. Disord. 28, 62–67. doi: 10.1016/j.parkreldis.2016.04.027
Tomlinson, C. L., Stowe, R., Patel, S., Rick, C., Gray, R., and Clarke, C. E. (2010). Systematic review of levodopa dose equivalency reporting in Parkinson’s disease. Mov. Disord. 25, 2649–2653. doi: 10.1002/mds.23429
Keywords: de novo Parkinson’s disease, motor subtypes, non-motor symptoms, tremor-dominant, postural instability and gait difficulty, akinetic-rigid
Citation: Ren J, Pan C, Li Y, Li L, Hua P, Xu L, Zhang L, Zhang W, Xu P and Liu W (2021) Consistency and Stability of Motor Subtype Classifications in Patients With de novo Parkinson’s Disease. Front. Neurosci. 15:637896. doi: 10.3389/fnins.2021.637896
Received: 04 December 2020; Accepted: 02 February 2021;
Published: 01 March 2021.
Edited by:
Gianfranco Spalletta, Santa Lucia Foundation (IRCCS), ItalyReviewed by:
Louis Tan, National Neuroscience Institute (NNI), SingaporeFrancesca Assogna, Santa Lucia Foundation (IRCCS), Italy
Copyright © 2021 Ren, Pan, Li, Li, Hua, Xu, Zhang, Zhang, Xu and Liu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Weiguo Liu, d2dsaXVuYmhAc2luYS5jb20=
†ORCID: Jingru Ren, orcid.org/0000-0002-9186-6621