 Lionel Butry1*
Lionel Butry1* Johanna Thomä1
Johanna Thomä1 Sigrid Elsenbruch2,3Adriane Icenhour4Robert Rehmann1
Sigrid Elsenbruch2,3Adriane Icenhour4Robert Rehmann1 Elena Enax-Krumova1†
Elena Enax-Krumova1† Lara Schlaffke1,5,6,7†
Lara Schlaffke1,5,6,7†- 1Department of Neurology, BG University Hospital Bergmannsheil, Ruhr University Bochum, Bochum, Germany
- 2Department of Medical Psychology and Medical Sociology, Medical Faculty, Ruhr University Bochum, Bochum, Germany
- 3Department of Neurology, Center for Translational Neuro- and Behavioral Sciences, University Hospital Essen, University of Duisburg-Essen, Essen, Germany
- 4Department of Affective Neuroscience, Medical Faculty, Ruhr University Bochum, Bochum, Germany
- 5BG University Hospital Bergmannsheil, Heimer Institute for Muscle Research, Bochum, Germany
- 6Department of Medical Engineering, FH Dortmund, University of Applied Sciences and Arts, Dortmund, Germany
- 7Ruhr University Bochum, University Hospital of Pediatrics and Adolescent Medicine, Bochum, Germany
Introduction: Identifying brain topology alterations in chronic pain is a crucial step in understanding its pathophysiology. The primary objective of this systematic review and meta-analysis was to assess alterations in resting-state functional and structural global network properties in patients with chronic pain.
Methods: Following the preregistration (PROSPERO CRD42024542390), databases were searched for studies comparing connectivity-based whole-brain global network properties between patients with chronic pain and healthy controls. Risk of bias was assessed using an adapted Newcastle-Ottawa scale. Random-effect meta-analyses were conducted for each global network property separately.
Results: A total of 32 functional topology studies and 17 structural topology studies were included in the qualitative review, with 27 functional topology studies and 17 structural topology studies eligible for meta-analysis across nine unique structural and functional global network properties. The number of participants per meta-analysis ranged from 178 to 1,592. There was low-certainty evidence that chronic pain patients showed impairments in local efficiency of resting-state functional whole-brain topology (SMD: −0.50, 95%-CI: −0.81 to −0.19, 95%-PI: −1.38 to 0.38), and low to very low-certainty evidence that structural whole-brain topology was not altered in chronic pain across nine global network properties. The heterogeneity was high in the majority of functional (I2: 1–76%) and structural (I2: 68–97%) topology studies. Most functional (50%) and structural (65%) topology studies showed some concern regarding the risk of bias.
Discussion: The meta-analyses indicate that functional but not structural whole-brain topological reorganisation is involved in the pathophysiology of chronic pain.
1 Introduction
Chronic pain imposes a significant personal and economic burden, affecting over 30% of the global population (Cohen et al., 2021). Unlike acute pain, which serves an adaptive function, chronic pain represents not just a prolonged form of pain but is associated with altered structural and functional neural plasticity across widespread brain regions (Kuner and Flor, 2016; Brandl et al., 2022). However, the role of these alterations is not fully understood. Investigating the underlying neuropathophysiology of chronic pain is crucial to facilitate innovations in the management of chronic pain disorders.
Advances in neuroimaging techniques and the growing adoption of network neuroscience have led to an increased focus on brain network topology in chronic pain research. Brain network topology refers to both the functional and structural organisation of the brain. The topology of a network is decisive for its function, as the principles of its information transfer capability naturally arise from its organisation (Moon et al., 2015). This is reflected in different brain topological alterations across neurological and psychological disorders such as depression, Parkinson’s disease, epilepsy, and traumatic brain injury (Kambeitz et al., 2016; Farahani et al., 2019; Xu et al., 2021; Slinger et al., 2022; Zuo et al., 2023). This raises the question whether brain topology can exhibit alterations characteristic of chronic pain.
Graph theory provides a robust mathematical framework for quantifying brain network topology (Farahani et al., 2019). In this approach, the brain network is modelled as a graph, composed of nodes connected by edges. Nodes represent predefined brain regions, and edges reflect the physical connection (structural connectivity) or synchronous neural activity (functional connectivity) between nodes (Bullmore and Sporns, 2009). Edges are defined by connectivity strength measures such as streamline count or fractional anisotropy (FA) in structural connectomes, or correlation coefficients in functional connectomes (Bullmore and Sporns, 2009). Graph theoretical metrics can be computed on a global network level, quantifying the topology of the entire brain network into a single value regarding its properties, such as integration, segregation, centrality, resilience, or small-worldness (Rubinov and Sporns, 2010). For a brief description of common global network properties, please refer to Table 1.
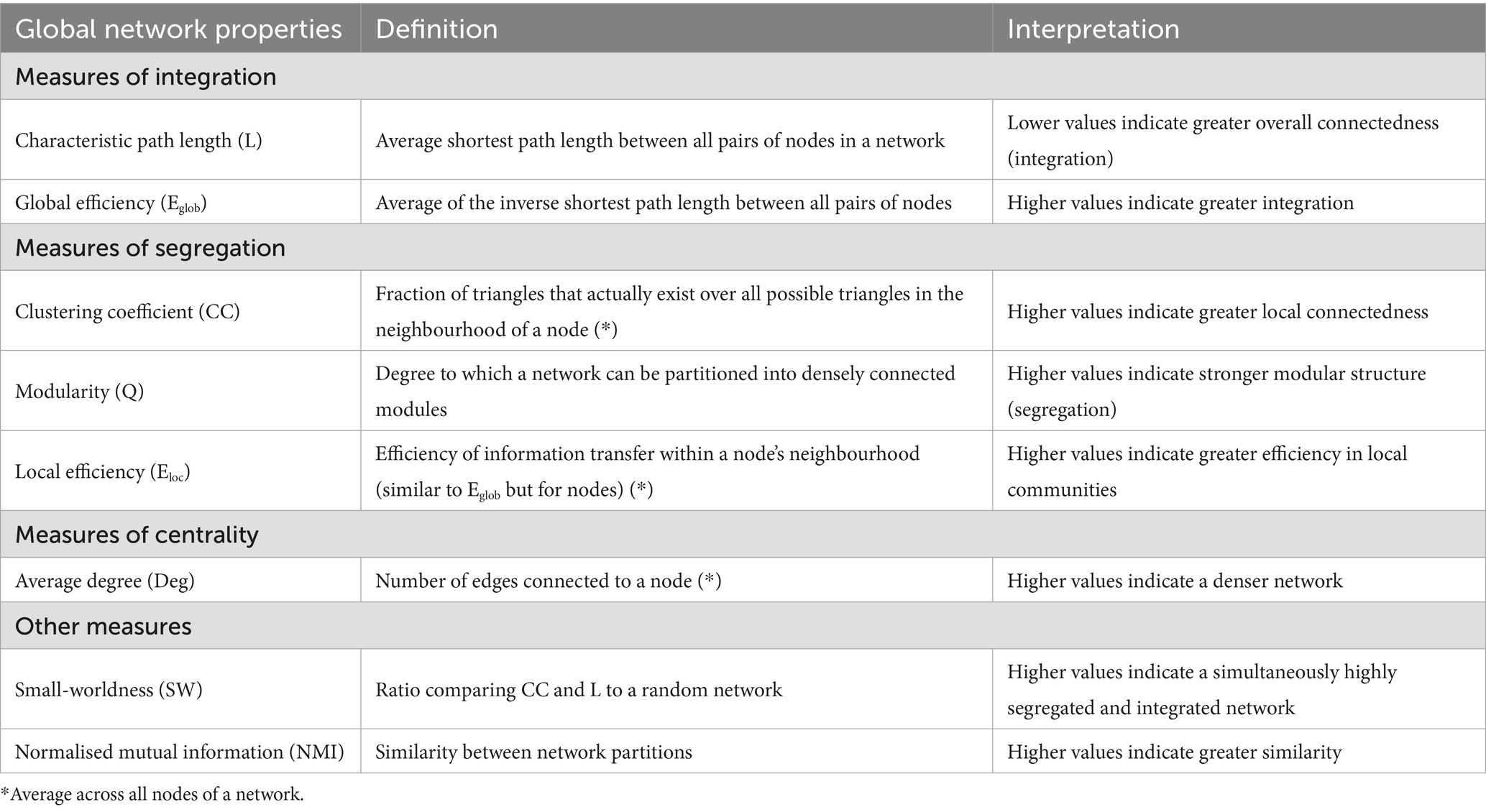
Table 1. Description of common global network properties.
Previous qualitative aggregation efforts reported alterations in global brain network topology in chronic pain patients compared to healthy individuals (Lenoir et al., 2021; Xin et al., 2024). Still, the certainty of evidence remains unknown as a plethora of new studies have been published, and no quantitative synthesis has been conducted so far.
The primary objective of this study was to assess differences in functional and structural connectivity-based global network properties between chronic pain patients and healthy controls. Secondarily, we examined whether these alterations varied by chronic pain type, distinguishing between chronic primary pain and chronic secondary pain. The ICD-11 defines chronic primary pain as a disease in its own right, whereas chronic secondary pain arises as a symptom of an underlying disease (Treede et al., 2019). Additionally, the influence of psychological comorbidities was explored. By synthesising existing evidence, our findings refine the current understanding of brain network topology in chronic pain.
2 Methods
The review was preregistered with PROSPERO (CRD42024542390), and the reporting used the PRISMA 2020 checklist.
2.1 Search strategy
An electronic database search of MEDLINE via PubMed, Web of Science, PsychInfo via EBSCO, CINAHL via EBSCO and Scopus was conducted. The search string had three domains (chronic pain, brain connectivity, graph analysis) combined by ‘AND’, containing MeSH categories and simple search terms (Appendix 1). The ‘Polyglot Search Translater’ was utilised to translate the search strings across databases (Clark et al., 2020). The initial search was completed from inception to April 29, 2024 and was updated on February 20, 2025. Additionally, articles which have been included in two a priori identified relevant systematic reviews (Lenoir et al., 2021; Xin et al., 2024) were added to the screening. The ‘Deduplicator’ software was used to remove article duplicates before screening (Forbes et al., 2024).
2.2 Eligibility criteria
Inclusion criteria followed the population, interventions, comparators, outcomes and study design (PICOS) framework.
Population. The population group of interest was adults (>18 years) with chronic pain, including chronic primary pain (i.e., chronic widespread, complex regional pain syndrome, headache or orofacial, visceral, musculoskeletal) and chronic secondary pain (i.e., cancer-related, postsurgical or posttraumatic, musculoskeletal, visceral, neuropathic, headache or orofacial) diagnoses. Chronic pain was defined as pain that persists or recurs for more than 3 months, following the ICD-11 (Treede et al., 2019). Pain duration of >3 months had to be reported in the sample eligibility criteria, sample characteristics or the diagnosis criteria. Articles investigating diseases associated with chronic secondary pain had to report the existence of pain in their population, either defined in the participants’ inclusion criteria or reported as a pain-specific measure.
Intervention. Studies had to assess resting-state functional connectivity of grey matter or structural connectivity of white matter using neuroimaging techniques such as resting-state functional MRI (rs-fMRI), rs-EEG, rs-MEG or diffusion-weighted MRI (dMRI). Functional connectivity had to be computed as a form of correlation between neural activity measures of brain regions at rest, irrespective of neuroimaging technique. Structural connectivity had to be computed based on diffusion MRI fibre tractography, irrespective of the diffusion tensor model used.
Comparator. The chronic pain group had to be compared with a healthy control group without chronic pain.
Outcome. Included studies had to examine graph-theoretical global network metrics of whole-brain functional or structural connectivity. Structural covariance networks based on T1-weighted MRI data and articles solely reporting region-of-interest or subnetwork analysis were excluded.
Study design. Any study with a comparative design of chronic pain and healthy controls that was published in a peer-reviewed journal in English or German was included. Longitudinal studies were included if baseline comparison was reported.
The synthesis was conducted separately for functional and structural topology.
2.3 Screening
Each record was assessed by two independent reviewers (LB and one of AI, LS, RR or SE) using the Systematic Review Facility (SyRF; Bahor et al., 2021). First, the title/abstract was screened, then the full text was screened to assess eligibility. Disagreements were resolved by EEK and by discussion between the assessors in the title/abstract phase and full text phase, respectively.
2.4 Data extraction
Data extraction was performed independently by two reviewers (LB, JT). The following information was extracted from the full texts of eligible articles: Relevant publication information (author, title, year), study demographics (sample size, sex ratio, age, pain duration, pain intensity), pain diagnosis, type of chronic pain (primary, secondary, both), assessment of psychological comorbidities, neuroimaging information (imaging modality, MRI field strength, voxel size, number of channels, frequency bandwidth, number of diffusion-gradient directions, b-value, tractography type), connectivity matrix information (type of connectivity, parcellation scheme, type and metric of edges, network thresholding, software used for global network property computation), main results (mean and standard deviation of connectivity-based global network metrics or p-value). Conflicts were resolved by discussion. In longitudinal studies, only baseline data were extracted. If studies reported multiple values of an outcome across different network thresholding levels or dynamic functional connectivity states, the data were pooled. In cases where data was reported as median and interquartile range, the mean and standard deviation were estimated using a widely used formula (Appendix 2; Wan et al., 2014). If outcome measures were reported solely in figures, WebPlotDigitizer v5.2 was utilised to extract the data. Although a standardised extraction protocol was employed to minimise plot digitalisation errors (Appendix 2), small variability in the digitalised plot data was expected. Therefore, this data was pooled across the two independent extractors. If outcome data could not be extracted, the corresponding author was contacted two times within 4 weeks.
2.5 Risk of bias and certainty in evidence assessment
There is no gold standard in assessing risk of bias in cross-sectional studies (Kelly et al., 2024). This review utilised an adapted Newcastle-Ottawa Scale for case–control studies (Stang, 2010), which has been employed in previous systematic reviews of global network properties (Lenoir et al., 2021; Slinger et al., 2022; Gao et al., 2023). It assesses the following domains: participant selection (max. 4 points), group comparability (max. 2 points) and outcome (max. 3 points; Appendix 2). A study can score between 0 and 9 points, with a higher score indicating a lower risk of bias. The points were converted to percentages and grouped into low risk of bias (71.6–100%), some concerns (28.6–71.5%) and high risk of bias (0–28.5%). The grouping thresholds ensure that only studies with relatively minor or major methodological issues are considered low or high risk of bias, respectively. Each included study was assessed by two independent assessors (LB, JT), and conflicts were resolved by discussion.
The certainty in evidence was assessed using the GRADE approach (very low-certainty to high-certainty). Risk of bias, inconsistency, imprecision and publication bias were considered to determine the certainty in each meta-analysis. A detailed description of the rating is presented in Appendix 2.
2.6 Statistical analysis
All analyses were performed in R v4.4.1 with the meta v8.0–2 R package (Balduzzi et al., 2019). Each global network property with at least three included studies was analysed separately for structural and functional brain topology, comparing the chronic pain group with the healthy control group. Subgroup analysis was conducted by segregating the chronic pain group into chronic primary pain and chronic secondary pain to explore sources of heterogeneity. In functional topology meta-analyses, only studies examining low-frequency fluctuations (≤ 0.1 Hz) were included to ensure comparability among the studies. To account for expected heterogeneity in study characteristics, random-effects meta-analyses with a restricted maximum-likelihood approach were performed using sample-bias corrected standardised mean difference (SMD; Hedges’g) and standard error (Viechtbauer, 2005). The 95% confidence intervals (CIs) for the random effects estimates were computed using the Hartung-Knapp method with adhoc variance correction (IQWiG6; Knapp and Hartung, 2003; IQWiG, 2022). The Hartung-Knapp-Partlett-Riley method with ad hoc variance correction was applied to estimate the 95% prediction intervals (PIs) if at least four studies were included in the meta-analysis (Partlett and Riley, 2017). Hedge’s g was calculated using the R package esc v0.5.1 (Lüdecke, 2019), based on the mean, standard deviation (SD) and sample size. When SDs or other measures of uncertainty were unavailable, and the authors were non-responsive, we imputed the SD by using the pooled coefficient of variation from other studies on the same outcome and converting it back to an SD. For studies that only reported p-values, Hedge’s g was estimated from the t- or F-statistic. In cases where non-significant p-values were reported without sufficient information to determine the direction of the effect, Hedge’s g was set to zero (Van Aert et al., 2016). This approach avoids making arbitrary assumptions about the effect size direction while ensuring that such studies contribute to the overall analysis through their standard error. When a study compared healthy controls to two or more chronic pain groups, the data were pooled to avoid sample overlap (Higgins et al., 2019). Heterogeneity was assessed using the I2 statistic (Higgins et al., 2019). Publication bias was assessed by funnel plot asymmetry, tested with an adapted Egger’s test (Pustejovsky and Rodgers, 2019). Sensitivity analysis was performed by removing statistical outliers and by removing studies with p-value-based imputed SMDs. The alpha level for statistical significance for all analyses was set to p < 0.05. The results of each meta-analysis were visualised in a forest plot and an overview plot containing the pooled SMD and PI of each meta-analysis.
2.7 Deviations from the study protocol
We intended to perform multilevel random-effects meta-analyses with neuroimaging information and connectivity matrix information included as covariates. Due to substantial missing data in study characteristics, we opted to forgo the multilevel meta-regression approach in favour of random-effect meta-analyses. Additionally, we intended to conduct subgroup analyses based on pain duration and psychological comorbidities, but this was not feasible due to the same reason.
3 Results
3.1 Study selection and characteristics
Overall, 1,185 articles were screened at the title/abstract phase, and 130 full texts were assessed (Figure 1). Finally, 47 studies were included in qualitative synthesis (Balenzuela et al., 2010; Liu et al., 2011, 2012, 2013, 2017, 2018; Zhang et al., 2014, 2017; Zhang et al., 2022b; Zhang et al., 2022a; Mansour et al., 2016; Pijnenburg et al., 2016; Wu et al., 2016, 2020; Li et al., 2017; Wada et al., 2017; Huang et al., 2019, 2021; Kaplan et al., 2019; Shi et al., 2019, 2020; Ta Dinh et al., 2019; Tu et al., 2019, 2023; De Pauw et al., 2020; Nieboer et al., 2020; Barroso et al., 2021; Dai et al., 2021; Duan et al., 2021; Fauchon et al., 2021; Kurokawa et al., 2021; Larkin et al., 2021; Silvestro et al., 2021; Chao et al., 2022; Lin et al., 2022; Wang et al., 2022, 2024; Lee et al., 2023; Qiu et al., 2023; Yang et al., 2023, 2024, 2025; Kang et al., 2024; Mao et al., 2024; Matoso et al., 2024; Mei et al., 2024; Zhou et al., 2024). Excluded studies with the reason for exclusion are provided in Appendix 3. Two studies examined both functional and structural topology (Zhang et al., 2022a; Yang et al., 2024).
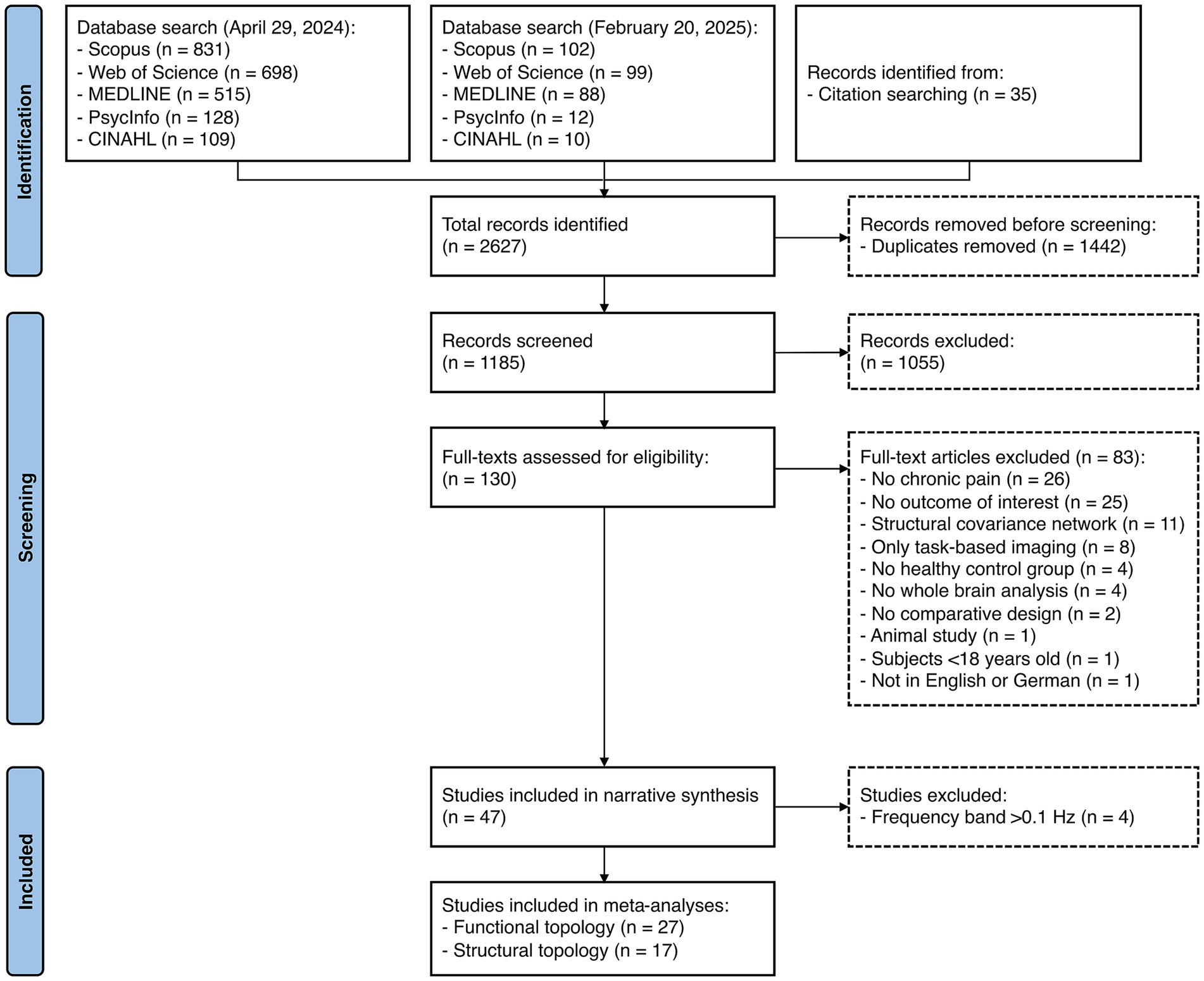
Figure 1. PRISMA-flowchart of study selection.
3.1.1 Functional topology studies
Overall, 32 studies examined functional brain topology. A qualitative summary of the included functional topology studies is provided in Table 2. Notably, a considerable number of studies did not report basic population characteristics such as sex, exact pain duration or pain intensity. Twenty-eight studies used rs-fMRI, three used rs-MEG, and one used rs-EEG. Of the 27 studies using an atlas-based parcellation approach, 15 (56%) chose a version of the AAL atlas. The existence of psychological comorbidities was an exclusion criterion in 20 (63%) studies, 15 (47%) studies assessed psychological comorbidities using patient-reported outcome measures (eight [25%] studies only in the chronic pain group), and eight (25%) studies did not report them at all. A detailed overview of all functional topology studies is presented in Appendix 4.
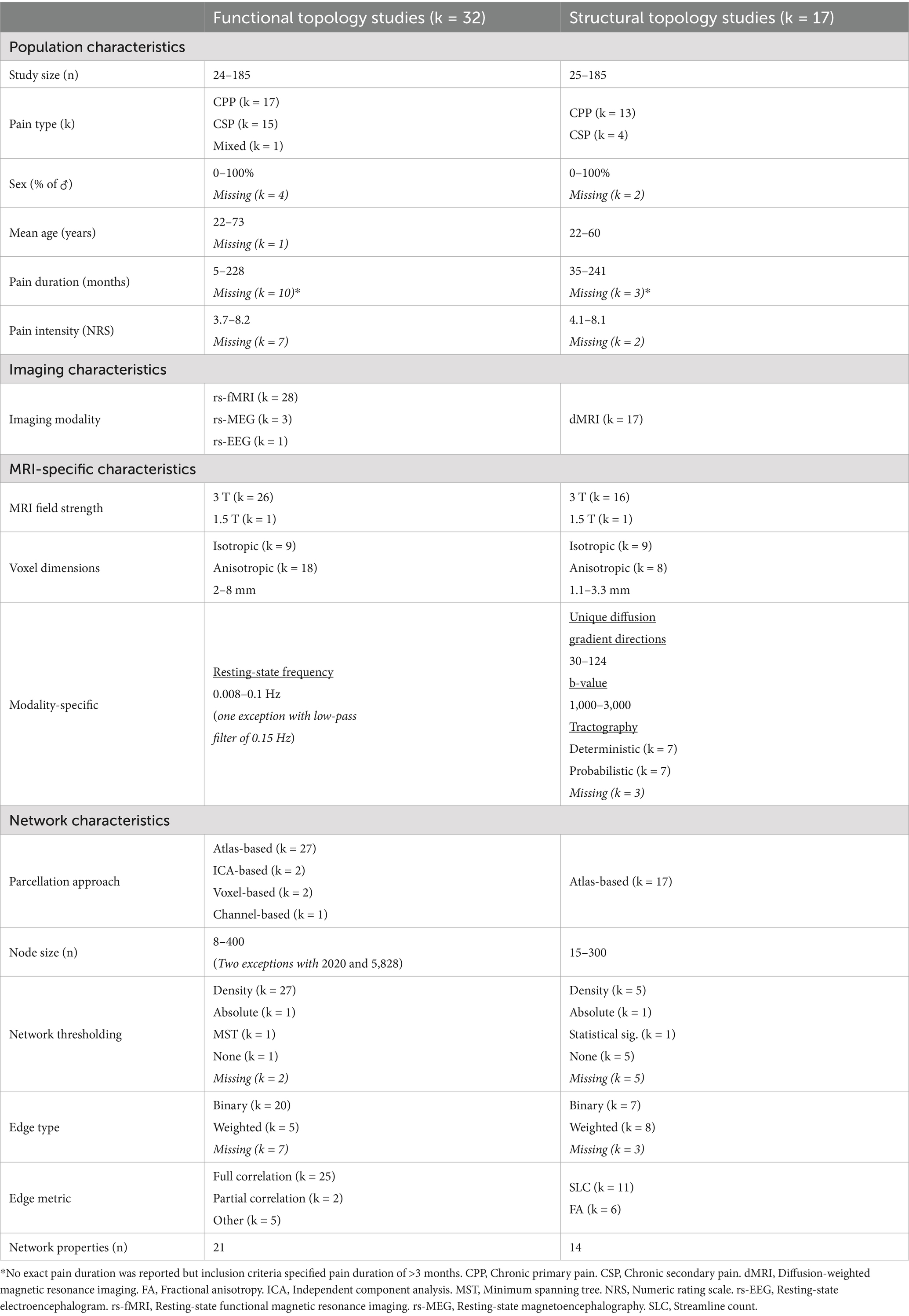
Table 2. Summary of study characteristics.
3.1.2 Structural topology studies
Structural brain topology was investigated by 17 studies. A qualitative summary of the included structural topology studies is provided in Table 1. Notably, a considerable number of studies did not report basic population characteristics such as sex, exact pain duration or pain intensity. Twelve (71%) studies employed a version of the AAL atlas. A single-shell dMRI acquisition protocol was used in 15 (88%) of included studies. The existence of psychological comorbidities was an exclusion criterion in six (35%) studies, seven (41%) studies assessed psychological comorbidities using patient-reported outcome measures (five [29%] only in the chronic pain group), and seven (41%) studies did not report psychological comorbidities at all. A detailed overview of all structural topology studies is presented in Appendix 4.
3.1.3 Risk of bias
The results of the risk of bias assessment are illustrated in Figure 2. Among the 32 studies that assessed functional brain topology, 11 (34%) were deemed to have low risk of bias, 16 (50%) had some concerns, and five (16%) were classified as having a high risk of bias. Of the 17 studies that examined structural brain topology, five (29%) scored low risk of bias, 11 (65%) had some concerns, and one (6%) had high risk of bias. When examining domain-specific risk of bias, 14 (44%) and 10 (59%) of functional and structural topology studies exhibited a high risk of bias in participant selection.
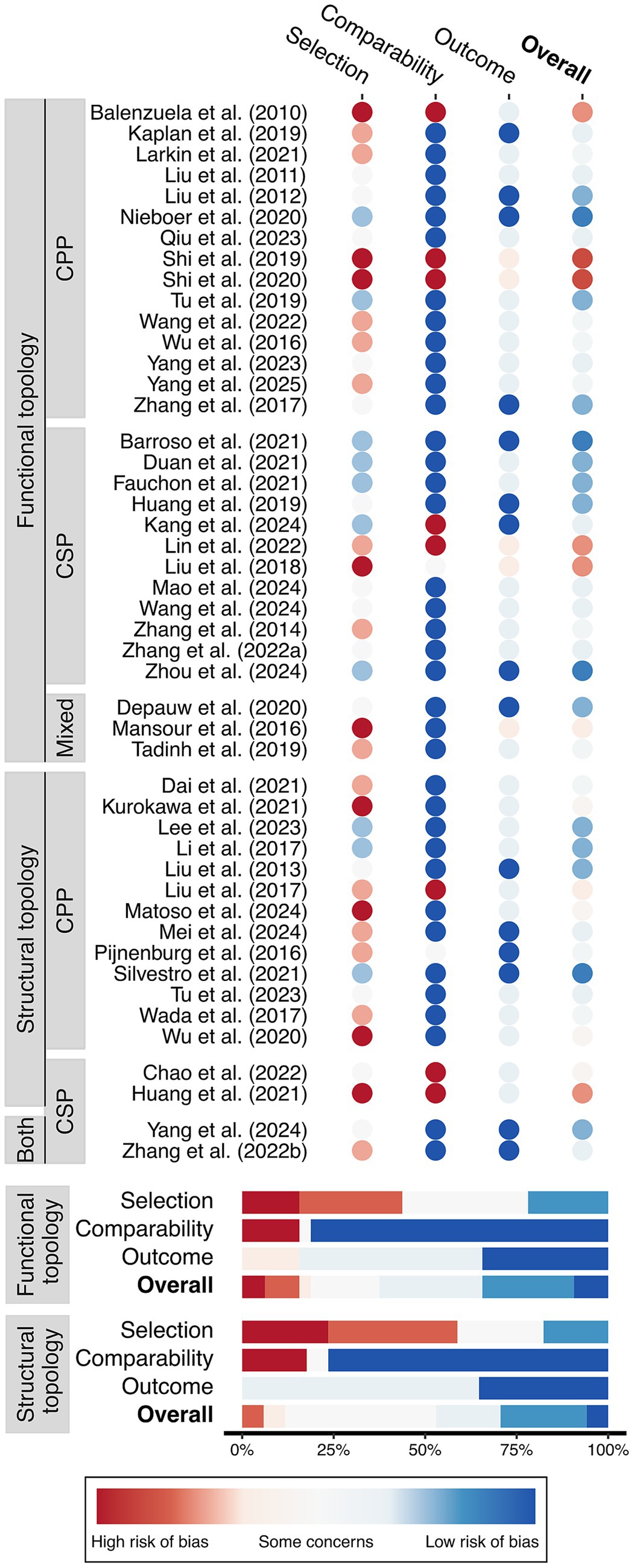
Figure 2. Risk of bias assessment grouped by functional and structural topology, chronic primary pain (CPP), and chronic secondary pain (CSP).
3.2 Meta-analysis
3.2.1 Data handling
For at least one outcome, the mean and standard deviation were extracted directly in 16 studies (Zhang et al., 2014; Liu et al., 2017, 2018; Kaplan et al., 2019; Wu et al., 2020; Dai et al., 2021; Fauchon et al., 2021; Huang et al., 2021; Kurokawa et al., 2021; Chao et al., 2022; Wang et al., 2022, 2024; Lee et al., 2023; Yang et al., 2023, 2024; Mao et al., 2024) WebPlotDigitizer was used in 24 studies (Balenzuela et al., 2010; Liu et al., 2011, 2012, 2013; Mansour et al., 2016; Pijnenburg et al., 2016; Li et al., 2017; Zhang et al., 2017, 2022a,b; Huang et al., 2019; Shi et al., 2019; De Pauw et al., 2020; Barroso et al., 2021; Duan et al., 2021; Fauchon et al., 2021; Larkin et al., 2021; Lin et al., 2022; Tu et al., 2023; Kang et al., 2024; Matoso et al., 2024; Mei et al., 2024; Zhou et al., 2024; Yang et al., 2025), and the standard deviation was imputed in five studies (Balenzuela et al., 2010; Shi et al., 2019; Silvestro et al., 2021; Zhang et al., 2022b; Kang et al., 2024). Pooling of multiple groups was performed in 10 studies (Liu et al., 2011; Mansour et al., 2016; De Pauw et al., 2020; Wu et al., 2020; Dai et al., 2021; Duan et al., 2021; Fauchon et al., 2021; Mei et al., 2024; Yang et al., 2024; Zhou et al., 2024). Two of these studies included both a chronic primary and secondary pain group, which were handled separately for the subgroup analysis (De Pauw et al., 2020; Mansour et al., 2016). In 40 studies, the SMD was computed based on the mean and standard deviation for at least one outcome (Balenzuela et al., 2010; Liu et al., 2011, 2012, 2013, 2017, 2018; Zhang et al., 2014, 2017, 2022a,b;Mansour et al., 2016; Pijnenburg et al., 2016; Li et al., 2017; Huang et al., 2019, 2021; Kaplan et al., 2019; Shi et al., 2019; De Pauw et al., 2020; Wu et al., 2020; Barroso et al., 2021; Dai et al., 2021; Duan et al., 2021; Fauchon et al., 2021; Kurokawa et al., 2021; Larkin et al., 2021; Silvestro et al., 2021; Chao et al., 2022; Lin et al., 2022; Wang et al., 2022, 2024; Lee et al., 2023; Tu et al., 2023; Yang et al., 2023, 2024, 2025; Kang et al., 2024; Mao et al., 2024; Matoso et al., 2024; Mei et al., 2024; Zhou et al., 2024). In four studies, the SMD was estimated based on the p-value (Wada et al., 2017; Shi et al., 2019; Silvestro et al., 2021; Tu et al., 2023), and in one study, the F-value was used (Tu et al., 2019). The SMD could not be estimated for at least one outcome in four studies due to insufficient reporting (Balenzuela et al., 2010; Shi et al., 2020; Barroso et al., 2021; Lin et al., 2022). The authors were contacted in 12 cases, with a response rate of 8% (n = 1).
3.2.2 Functional topology
Meta-analysis was eligible for nine unique global network properties of functional topology (across 27 rs-fMRI studies). A qualitative synthesis of studies excluded from the meta-analysis is presented in Appendix 5. There was low-certainty evidence that chronic pain patients showed lower local efficiency in functional whole-brain topology (Figure 3). Additionally, there was low to very low-certainty evidence that chronic pain patients exhibited no difference in functional whole-brain topology assessed by clustering coefficient, normalised clustering coefficient, global efficiency, characteristic path length, normalised characteristic path length, normalised mutual information, modularity and small-worldness (Figure 3). The heterogeneity in overall chronic pain meta-analysis was high, ranging from 67 to 76%, except for the normalised characteristic path length, with 1%. Subgroup analysis showed similar results, with low-certainty evidence of lower local efficiency in chronic primary pain and chronic secondary pain compared to healthy controls (Figure 3). All accompanying forest plots are presented in Appendix 6. The results were robust to outlier removal sensitivity analysis (Appendix 6). When removing studies with p-value-based imputed SMDs, the significant difference in local efficiency between chronic primary pain and healthy controls disappeared (SMD, −0.51; 95%-CI: −1.47, 0.45; Appendix 6). All other results were robust to this sensitivity analysis (Appendix 6).
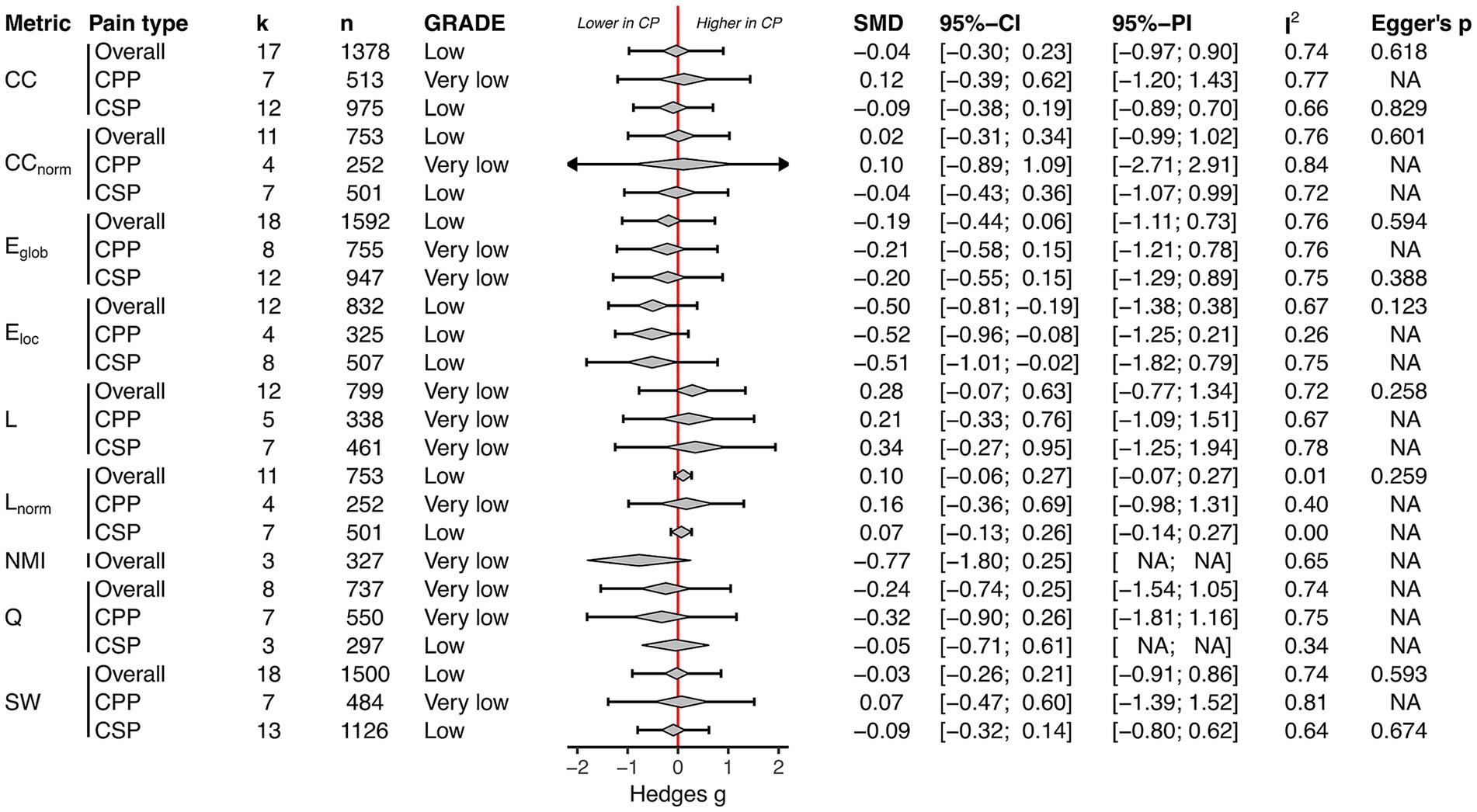
Figure 3. Functional topology: Summary of all meta-analyses ordered by global network property (clustering coefficient [CC]; normalised clustering coefficient [CCnorm]; global efficiency [Eglob]; local efficiency [Eloc]; characteristic path length [L]; normalised characteristic path length [Lnorm]; normalised mutual information [NMI]; modularity [Q]; small-worldness [SW]) and pain type (overall; chronic primary pain [CPP]; chronic secondary pain [CSP]). The diamond depicts the pooled SMD and the error bar its 95% prediction interval; CP, Chronic pain.
3.2.3 Structural topology
Meta-analysis was eligible for nine unique global network properties of structural topology (across 17 dMRI studies). There was low to very low-certainty evidence that chronic pain patients showed no difference in structural whole-brain topology assessed by average degree, clustering coefficient, normalised clustering coefficient, global efficiency, local efficiency, characteristic path length, normalised characteristic path length, modularity, and small-worldness (Figure 4). The heterogeneity in chronic pain overall meta-analyses was substantial, ranging from 68 to 97%. Subgroup analysis also revealed no alterations in structural brain topology in chronic primary and secondary pain (Figure 4). In outlier-removal-sensitivity analysis, the results remained non-significant (Appendix 7). The results were robust when removing studies with p-value-based imputed SMDs (Appendix 7).
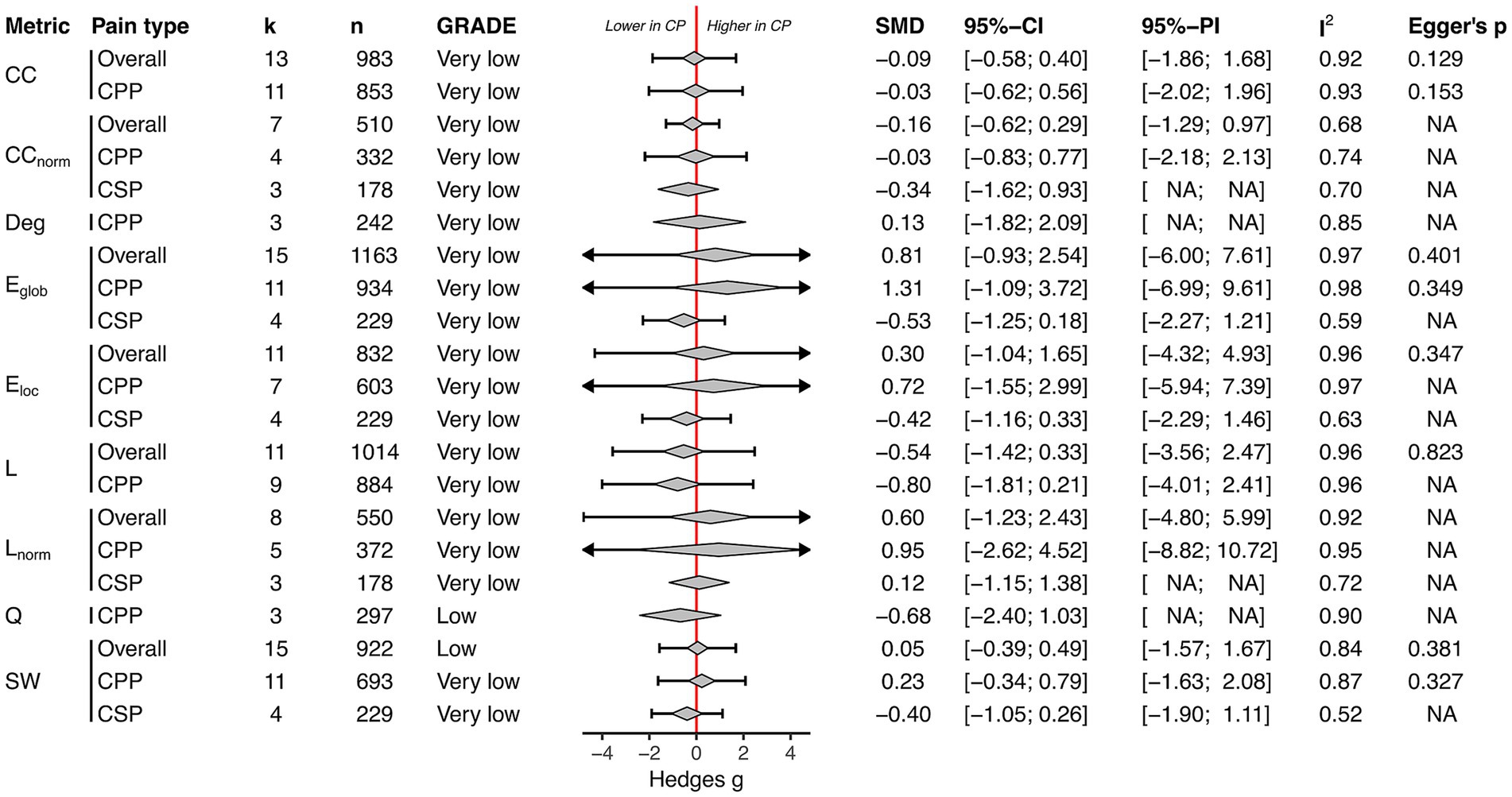
Figure 4. Structural topology: Summary of all meta-analyses ordered by global network property (clustering coefficient [CC]; normalised clustering coefficient [CCnorm]; degree [deg]; global efficiency [Eglob]; local efficiency [Eloc]; characteristic path length [L]; normalised characteristic path length [Lnorm]; modularity [Q]; small-worldness [SW]) and pain type (Overall, chronic primary pain [CPP], chronic secondary pain [CSP]). The diamond depicts the pooled SMD and the error bar its 95% prediction interval; CP, Chronic pain.
4 Discussion
The primary aim of this study was to quantitatively synthesise alterations in functional and structural connectivity-based global network properties of whole-brain topology in chronic pain. There was low-certainty evidence that chronic pain patients showed impairments in local efficiency of resting-state functional whole-brain topology, and low to very low-certainty evidence that structural whole-brain topology was not altered in chronic pain.
4.1 Lower local efficiency in resting-state functional network in chronic pain
Local efficiency quantifies how effectively information is transferred within local neighbourhoods of a network (Figure 5). It is therefore a measure of segregation, reflecting the brain’s capacity for specialised processing within densely interconnected groups of brain regions (Rubinov and Sporns, 2010). Patients with chronic pain showed lower local efficiency in their resting-state functional network, indicating reduced local specialisation and suggesting a shift towards greater global integration. Both chronic primary pain and chronic secondary pain exhibited impairments in local efficiency, suggesting that chronic pain, regardless of its origin, is associated with similar reorganisation of functional whole-brain topology.
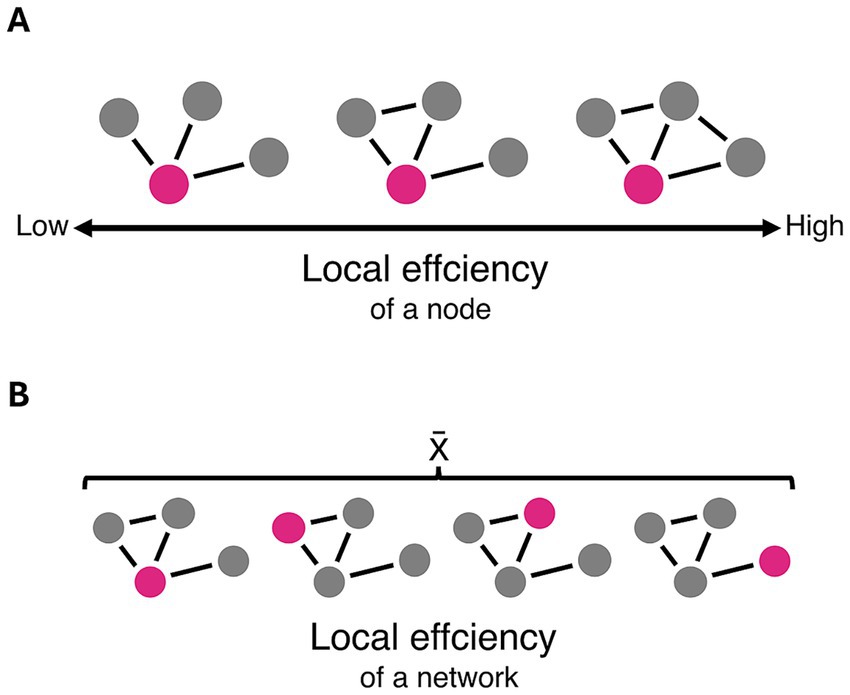
Figure 5. Schematic representation of local efficiency. (A) Local efficiency of a node is increased as the number of connections between its neighbouring nodes increases. (B) Local efficiency as a global network property is determined by the average local efficiency of all nodes within a given network.
In healthy individuals, the resting state is dominated by activity in the default mode network (DMN), associated with self-referential thought. A recent meta-analysis of resting-state fMRI studies concluded that patients with chronic pain exhibit altered intra-DMN connectivity and increased connectivity between DMN and somatosensory regions (Fiúza-Fernandes et al., 2025). This pattern further supports a shift towards global integration through stronger interconnectedness of self-referential processes and pain processing.
Impairments in local efficiency of the functional whole-brain network have also been reported in a meta-analysis of patients with depression (Xu et al., 2021), a common comorbidity in chronic pain (De La Rosa et al., 2024). Due to inconsistent reporting of psychological comorbidities in the included studies, we were unable to determine their influence on functional topology alterations in chronic pain. Therefore, it is unclear whether local efficiency impairments are characteristic of chronic pain, are conditional on the presence of psychological comorbidities such as depression, or are a shared neural principle across conditions.
4.2 No structural whole-brain topology alterations in chronic pain
Our meta-analyses concluded that the structural whole-brain topology remains unaltered in chronic pain. This contrasts with neurological diseases with substantial anatomical changes, such as epilepsy, Parkinson’s disease, or traumatic brain injury, which have demonstrated impairments in structural whole-brain topology (Imms et al., 2019; Slinger et al., 2022; Zuo et al., 2023). Interestingly, dMRI-based alterations of various white matter bundles have been documented in chronic pain, including the corpus callosum, thalamic radiations, internal capsule and corona radiata (Bautin et al., 2025). However, these microstructural changes do not necessarily affect the global organisation of the structural connectome, suggesting preserved large-scale brain architecture despite local white matter disruptions.
4.3 Heterogeneity and risk of bias
The heterogeneity was with I2 values of more than 50% in most meta-analyses, and wide prediction intervals, considered to be high. Although no meta-regression was performed to evaluate heterogeneity, the qualitative synthesis showed a wide range in population and methodological characteristics of the included studies. For example, included studies investigated different chronic pain syndromes, including headache, orofacial pain, visceral pain, musculoskeletal pain, widespread pain, complex regional pain syndromes and neuropathic pain. Notably, half of the structural topology studies and about one-third of functional topology studies examined migraine, indicating a bias in the meta-analyses.
The methodological characteristics of the included studies reflect the current lack of a gold standard in graph-theoretical brain network analysis (Fornito et al., 2013; Bahrami et al., 2023). Differences in parcellation scheme, network thresholding, and edge definition may have influenced the results of our meta-analysis. While several global network properties remain robust across different parcellation schemes at a consistent resolution (number of nodes), altering the parcellation resolution significantly impacts these global metrics (Zalesky et al., 2010). Since the number of nodes (84–264) of most studies was on a similar scale, parcellation was less likely to influence the results. However, it must be noted that in functional networks, larger parcellation units yield smoother, less specific time courses, which in turn reduce the specificity of the resulting network topology (De Reus and Van Den Heuvel, 2013). Different thresholding methods are applied to networks to account for spurious connections, but they introduce specific limitations (van Wijk et al., 2010). Although most included studies employed density-based thresholding, which retains a specific percentage of the strongest connections, the range of the used thresholds varied widely, adding heterogeneity to the meta-analyses as the choice of a density threshold influences the graph measures (van Wijk et al., 2010). Additionally, structural topology studies showed higher heterogeneity in network binarisation and edge metric, adding further variability, while functional topology studies showed higher concordance in these characteristics. Many rs-fMRI and some dMRI studies acquired anisotropic voxels, potentially introducing anatomical inaccuracies, partial volume effects, and other directional biases (Mulder et al., 2019). Most structural topology studies used the simple DTI model with a one-shell diffusion acquisition scheme with 30 to 64 directions, yielding high residuals in the tensor model. Future studies should embrace the advancements made in dMRI acquisition and processing over the last 15 years by utilising multi-shell acquisitions, which enable state-of-the-art dMRI analysis (Bautin et al., 2025).
The risk of bias assessment of this review indicates a considerable risk in the selection of study participants, a common pitfall of cross-sectional studies. Future studies should improve this by clearly defining their control group and by investigating more representative study samples. Strikingly, many studies showed poor reporting, missing basic population and methodological information such as sex, exact pain duration, pain intensity, edge type, network thresholding or tractography algorithm. Additionally, some studies lacked sufficient outcome data for cross-study pooling. Overall, the methodological heterogeneity and concerning reporting quality complicate the interpretation of cross-study comparisons of global network properties and call for standardisation in graph theoretical analysis of brain networks.
4.4 Limitations
The findings of this review should be considered with several methodological limitations in mind. First, as the meta-analyses only included functional topology studies investigating low-frequency fluctuations (≤ 0.1 Hz), no quantitative statement about other frequency bands (investigated in four studies) can be made. Second, four studies were excluded from the meta-analyses because their results could not be extracted due to poor reporting. As their results showed no alterations in brain topology, they would likely not alter the overall results of this review. Third, not all reported global network properties could be pooled due to limitations in the number of studies investigating them, as not all studies reported all metrics. Fourth, the review excluded studies investigating structural covariance networks as they do not analyse white matter topology but analyse structural topology based on the correlation of morphology parameters of grey matter regions. It remains unclear whether this approach can identify structural whole-brain topology alterations in chronic pain. Additionally, systematic differences in brain topology alteration may exist among different pain diagnoses. Pooling data across all diagnoses may have introduced sufficient variance to obscure any difference between healthy controls and chronic pain patients.
4.5 Implications for clinic and research
Our meta-analysis showed that impairments in local efficiency within the resting-state whole-brain network are associated with both chronic primary and secondary pain diagnoses. However, it remains unclear whether the functional topology reorganisation is a consequence of chronic pain or if it contributes to its development. Future studies may focus on determining the time course of functional topology reorganisation, its modulation by therapeutic interventions and consider psychological comorbidities as a possible influencing factor.
While the whole-brain approach captures essential characteristics of the entire macroscale brain organisation, it may lack sensitivity to detect subtle disease-related changes in network topology. Investigations of subnetworks such as large-scale brain networks (Uddin et al., 2019), or the ‘pain matrix’ (Legrain et al., 2011) could reveal structural and functional topology alterations confined to specific subnetworks previously masked by the whole-brain approach. Additionally, future studies could use further global network properties such as the hub disruption index, which captures changes at the nodal level, shows high reliability and sensitivity (Termenon et al., 2016), and has already been used in some pain studies (Huang et al., 2019; De Pauw et al., 2020; Barroso et al., 2021).
5 Conclusion
This is the first study to quantitatively synthesise connectivity-based global network properties of functional and structural brain topology in chronic pain. There was low-certainty evidence that chronic pain patients showed impairments in local efficiency of resting-state functional whole-brain topology, and low to very low-certainty evidence that structural whole-brain topology was not altered in chronic pain. This indicates that functional but not anatomical whole-brain topological reorganisation is involved in the pathophysiology of chronic pain. This review highlights the need for standardisation in graph-theoretical brain network analyses and reporting of methods and results. Additionally, future studies should consider psychological comorbidities and expand the analyses to specific subnetworks when investigating brain topology in chronic pain.
Author’s note
This work is part of the PhD project of L. Butry.
Data availability statement
Publicly available datasets were analysed in this study. This data can be found at: https://osf.io/y27qc/.
Author contributions
LB: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Software, Visualization, Writing – original draft. JT: Investigation, Writing – review & editing. SE: Conceptualization, Investigation, Writing – review & editing. AI: Conceptualization, Investigation, Writing – review & editing. RR: Investigation, Writing – review & editing. EE-K: Conceptualization, Investigation, Resources, Supervision, Validation, Writing – review & editing. LS: Conceptualization, Investigation, Resources, Supervision, Validation, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
We thank Ryo Kurokawa for providing additional data upon request.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnins.2025.1672542/full#supplementary-material
References
Bahor, Z., Liao, J., Currie, G., Ayder, C., Macleod, M., Mccann, S. K., et al. (2021). Development and uptake of an online systematic review platform: the early years of the CAMARADES systematic review facility (SyRF). BMJ Open Sci. 5:e100103. doi: 10.1136/bmjos-2020-100103
Bahrami, M., Laurienti, P. J., Shappell, H. M., and Simpson, S. L. (2023). Brain network analysis: A review on multivariate analytical methods. Brain Connect. 13, 64–79. doi: 10.1089/brain.2022.0007
Balduzzi, S., Rücker, G., and Schwarzer, G. (2019). How to perform a meta-analysis with R: a practical tutorial. Evid. Based Ment. Health 22, 153–160. doi: 10.1136/ebmental-2019-300117
Balenzuela, P., Chernomoretz, A., Fraiman, D., Cifre, I., Sitges, C., and Montoya, P. (2010). Modular organization of brain resting state networks in chronic back pain patients. Front. Neuroinform. 4:116. doi: 10.3389/fninf.2010.00116
Barroso, J., Wakaizumi, K., Reis, A. M., Baliki, M., Schnitzer, T. J., and Galhardo, V. (2021). Reorganization of functional brain network architecture in chronic osteoarthritis pain. Hum. Brain Mapp. 42, 1206–1222. doi: 10.1002/hbm.25287
Bautin, P., Fortier, M.-A., Sean, M., Little, G., Martel, M., and Descoteaux, M. (2025). What has brain diffusion magnetic resonance imaging taught us about chronic primary pain: a narrative review. Pain 166, 243–261. doi: 10.1097/j.pain.0000000000003345
Brandl, F., Weise, B., Mulej Bratec, S., Jassim, N., Hoffmann Ayala, D., and Bertram, T. (2022). Common and specific large-scale brain changes in major depressive disorder, anxiety disorders, and chronic pain: a transdiagnostic multimodal meta-analysis of structural and functional MRI studies. Neuropsychopharmacol. 47, 1071–1080. doi: 10.1038/s41386-022-01271-y
Bullmore, E., and Sporns, O. (2009). Complex brain networks: graph theoretical analysis of structural and functional systems. Nat. Rev. Neurosci. 10, 186–198. doi: 10.1038/nrn2575
Chao, C.-C., Hsieh, P.-C., Janice Lin, C.-H., Huang, S.-L., Hsieh, S.-T., and Chiang, M.-C. (2022). Impaired brain network architecture as neuroimaging evidence of pain in diabetic neuropathy. Diabetes Res. Clin. Pract. 186:109833. doi: 10.1016/j.diabres.2022.109833
Clark, J. M., Sanders, S., Carter, M., Honeyman, D., Cleo, G., and Auld, Y. (2020). Improving the translation of search strategies using the polyglot search translator: a randomized controlled trial. J. Med. Libr. Assoc. 108, 195–207. doi: 10.5195/jmla.2020.834
Cohen, S. P., Vase, L., and Hooten, W. M. (2021). Chronic pain: an update on burden, best practices, and new advances. Lancet 397, 2082–2097. doi: 10.1016/S0140-6736(21)00393-7
Dai, L., Zheng, Q., Chen, X., Wang, J., Peng, Y., and Hu, C. (2021). Altered brain structural topological properties and its correlations with clinical characteristics in episodic migraine without aura. Neuroradiology 63, 2099–2109. doi: 10.1007/s00234-021-02716-9
De La Rosa, J. S., Brady, B. R., Ibrahim, M. M., Herder, K. E., Wallace, J. S., Padilla, A. R., et al. (2024). Co-occurrence of chronic pain and anxiety/depression symptoms in U.S. adults: prevalence, functional impacts, and opportunities. Pain 165, 666–673. doi: 10.1097/j.pain.0000000000003056
De Pauw, R., Aerts, H., Siugzdaite, R., Meeus, M., Coppieters, I., Caeyenberghs, K., et al. (2020). Hub disruption in patients with chronic neck pain: a graph analytical approach. Pain 161, 729–741. doi: 10.1097/j.pain.0000000000001762
De Reus, M. A., and Van Den Heuvel, M. P. (2013). The parcellation-based connectome: limitations and extensions. NeuroImage 80, 397–404. doi: 10.1016/j.neuroimage.2013.03.053
Duan, S., Liu, L., Li, G., Wang, J., Hu, Y., and Zhang, W. (2021). Altered functional connectivity within and between salience and sensorimotor networks in patients with functional constipation. Front. Neurosci. 15:628880. doi: 10.3389/fnins.2021.628880
Farahani, F. V., Karwowski, W., and Lighthall, N. R. (2019). Application of graph theory for identifying connectivity patterns in human brain networks: A systematic review. Front. Neurosci. 13:585. doi: 10.3389/fnins.2019.00585
Fauchon, C., Meunier, D., Rogachov, A., Hemington, K. S., Cheng, J. C., and Bosma, R. L. (2021). Sex differences in brain modular organization in chronic pain. Pain 162, 1188–1200. doi: 10.1097/j.pain.0000000000002104
Fiúza-Fernandes, J., Pereira-Mendes, J., Esteves, M., Radua, J., Picó-Pérez, M., and Leite-Almeida, H. (2025). Common neural correlates of chronic pain – A systematic review and meta-analysis of resting-state fMRI studies. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 138:111326. doi: 10.1016/j.pnpbp.2025.111326
Forbes, C., Greenwood, H., Carter, M., and Clark, J. (2024). Automation of duplicate record detection for systematic reviews: Deduplicator. Syst. Rev. 13:206. doi: 10.1186/s13643-024-02619-9
Fornito, A., Zalesky, A., and Breakspear, M. (2013). Graph analysis of the human connectome: promise, progress, and pitfalls. NeuroImage 80, 426–444. doi: 10.1016/j.neuroimage.2013.04.087
Gao, M., Wong, N. M. L., Lin, C., Huang, C.-M., Liu, H.-L., Toh, C.-H., et al. (2023). Multimodal brain connectome-based prediction of suicide risk in people with late-life depression. Nat. Ment. Health 1, 100–113. doi: 10.1038/s44220-022-00007-7
Higgins, J., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M., et al. (2019). Cochrane handbook for systematic reviews of interventions. 2nd Edn. Chichester (UK): John Wiley & Sons.
Huang, X., Chen, J., Liu, S., Gong, Q., Liu, T., and Lu, C. (2021). Impaired frontal-parietal control network in chronic prostatitis/chronic pelvic pain syndrome revealed by graph theoretical analysis: A DTI study. Eur. J. Neurosci. 53, 1060–1071. doi: 10.1111/ejn.14962
Huang, S., Wakaizumi, K., Wu, B., Shen, B., Wu, B., and Fan, L. (2019). Whole-brain functional network disruption in chronic pain with disk herniation. Pain 160, 2829–2840. doi: 10.1097/j.pain.0000000000001674
Imms, P., Clemente, A., Cook, M., D’Souza, W., Wilson, P. H., and Jones, D. K. (2019). The structural connectome in traumatic brain injury: A meta-analysis of graph metrics. Neurosci. Biobehav. Rev. 99, 128–137. doi: 10.1016/j.neubiorev.2019.01.002
Kambeitz, J., Kambeitz-Ilankovic, L., Cabral, C., Dwyer, D. B., Calhoun, V. D., and van den Heuvel, M. P. (2016). Aberrant functional whole-brain network architecture in patients with schizophrenia: A Meta-analysis. Schizophr. Bull. 42, S13–S21. doi: 10.1093/schbul/sbv174
Kang, B., Ma, J., Shen, J., Zhao, C., Hua, X., and Qiu, G. (2024). Hemisphere lateralization of graph theoretical network in end-stage knee osteoarthritis patients. Brain Res. Bull. 213:110976. doi: 10.1016/j.brainresbull.2024.110976
Kaplan, C. M., Schrepf, A., Vatansever, D., Larkin, T. E., Mawla, I., and Ichesco, E. (2019). Functional and neurochemical disruptions of brain hub topology in chronic pain. Pain 160, 973–983. doi: 10.1097/j.pain.0000000000001480
Kelly, S. E., Brooks, S. P. J., Benkhedda, K., MacFarlane, A. J., Greene-Finestone, L. S., and Skidmore, B. (2024). A scoping review shows that no single existing risk of bias assessment tool considers all sources of bias for cross-sectional studies. J. Clin. Epidemiol. 172:111408. doi: 10.1016/j.jclinepi.2024.111408
Knapp, G., and Hartung, J. (2003). Improved tests for a random effects meta-regression with a single covariate. Stat. Med. 22, 2693–2710. doi: 10.1002/sim.1482
Kuner, R., and Flor, H. (2016). Structural plasticity and reorganisation in chronic pain. Nat. Rev. Neurosci. 18, 20–30. doi: 10.1038/nrn.2016.162
Kurokawa, R., Kamiya, K., Inui, S., Kato, S., Suzuki, F., and Amemiya, S. (2021). Structural connectivity changes in the cerebral pain matrix in burning mouth syndrome: a multi-shell, multi-tissue-constrained spherical deconvolution model analysis. Neuroradiology 63, 2005–2012. doi: 10.1007/s00234-021-02732-9
Larkin, T. E., Kaplan, C. M., Schrepf, A., Ichesco, E., Mawla, I., and Harte, S. E. (2021). Altered network architecture of functional brain communities in chronic nociplastic pain. NeuroImage 226:117504. doi: 10.1016/j.neuroimage.2020.117504
Lee, D. A., Kim, H. C., Lee, H.-J., and Park, K. M. (2023). Predicting Sumatriptan responsiveness based on structural connectivity in patients newly diagnosed with migraine. J. Clin. Neurol. (Seoul, Korea) 19, 573–580. doi: 10.3988/jcn.2022.0479
Legrain, V., Iannetti, G. D., Plaghki, L., and Mouraux, A. (2011). The pain matrix reloaded: A salience detection system for the body. Prog. Neurobiol. 93, 111–124. doi: 10.1016/j.pneurobio.2010.10.005
Lenoir, D., Cagnie, B., Verhelst, H., and De Pauw, R. (2021). Graph measure based connectivity in chronic pain patients: a systematic review. Pain Physician 24, E1037–E1058. Available online at: https://www.painphysicianjournal.com/linkout?issn=&vol=24&page=E1037
Li, K., Liu, L., Yin, Q., Dun, W., Xu, X., and Liu, J. (2017). Abnormal rich club organization and impaired correlation between structural and functional connectivity in migraine sufferers. Brain Imaging Behav. 11, 526–540. doi: 10.1007/s11682-016-9533-6
Lin, G., Lan, F., Wu, D., Cao, G., Li, Z., and Qi, Z. (2022). Resting-state functional connectivity alteration in elderly patients with knee osteoarthritis and declined cognition: an observational study. Front. Aging Neurosci. 14:1002642. doi: 10.3389/fnagi.2022.1002642
Liu, J., Ma, S., Mu, J., Chen, T., Xu, Q., and Dun, W. (2017). Integration of white matter network is associated with interindividual differences in psychologically mediated placebo response in migraine patients. Hum. Brain Mapp. 38, 5250–5259. doi: 10.1002/hbm.23729
Liu, J., Qin, W., Nan, J., Li, J., Yuan, K., and Zhao, L. (2011). Gender-related differences in the dysfunctional resting networks of migraine suffers. PLoS One 6:e27049. doi: 10.1371/journal.pone.0027049
Liu, J., Zhang, F., Liu, X., Zhuo, Z., Wei, J., Du, M., et al. (2018). Altered small-world, functional brain networks in patients with lower back pain. Sci. China Life Sci. 61, 1420–1424. doi: 10.1007/s11427-017-9108-6
Liu, J., Zhao, L., Li, G., Xiong, S., Nan, J., and Li, J. (2012). Hierarchical alteration of brain structural and functional networks in female migraine sufferers. PLoS One 7:e51250. doi: 10.1371/journal.pone.0051250
Liu, J., Zhao, L., Nan, J., Li, G., Xiong, S., Von Deneen, K. M., et al. (2013). The trade-off between wiring cost and network topology in white matter structural networks in health and migraine. Exp. Neurol. 248, 196–204. doi: 10.1016/j.expneurol.2013.04.012
Lüdecke, D. (2019). Esc: effect size computation for Meta analysis (version 0.5.1). Available online at: https://CRAN.R-project.org/package=esc (Accessed March 20, 2025).
Mansour, A., Baria, A. T., Tetreault, P., Vachon-Presseau, E., Chang, P.-C., Huang, L., et al. (2016). Global disruption of degree rank order: a hallmark of chronic pain. Sci. Rep. 6:34853. doi: 10.1038/srep34853
Mao, C., Yang, H., Dong, T., Wang, S., Shi, Z., Guo, R., et al. (2024). Thalamocortical dysconnectivity is associated with pain in patients with knee osteoarthritis. Eur. J. Neurosci. 60, 5831–5848. doi: 10.1111/ejn.16531
Matoso, A., Fouto, A. R., Esteves, I., Ruiz-Tagle, A., Caetano, G., da Silva, N. A., et al. (2024). Involvement of the cerebellum in structural connectivity enhancement in episodic migraine. J. Headache Pain 25:1–11. doi: 10.1186/s10194-024-01854-8
Mei, Y., Qiu, D., Xiong, Z., Li, X., Zhang, P., Zhang, M., et al. (2024). Disrupted topologic efficiency of white matter structural connectome in migraine: a graph-based connectomics study. J. Headache Pain 25:204. doi: 10.1186/s10194-024-01919-8
Moon, J.-Y., Lee, U., Blain-Moraes, S., and Mashour, G. A. (2015). General relationship of global topology, local dynamics, and directionality in large-scale brain networks. PLoS Comput. Biol. 11:e1004225. doi: 10.1371/journal.pcbi.1004225
Mulder, M. J., Keuken, M. C., Bazin, P.-L., Alkemade, A., and Forstmann, B. U. (2019). Size and shape matter: the impact of voxel geometry on the identification of small nuclei. PLoS One 14:e0215382. doi: 10.1371/journal.pone.0215382
Nieboer, D., Sorrentino, P., Hillebrand, A., Heymans, M. W., Twisk, J. W. R., and Stam, C. J. (2020). Brain network integration in patients with migraine: A magnetoencephalography study. Brain Connect. 10, 224–235. doi: 10.1089/brain.2019.0705
Partlett, C., and Riley, R. D. (2017). Random effects meta-analysis: coverage performance of 95% confidence and prediction intervals following REML estimation. Stat. Med. 36, 301–317. doi: 10.1002/sim.7140
Pijnenburg, M., Hosseini, S. M. H., Brumagne, S., Janssens, L., Goossens, N., and Caeyenberghs, K. (2016). Structural brain connectivity and the sit-to-stand-to-sit performance in individuals with nonspecific low Back pain: A diffusion magnetic resonance imaging-based network analysis. Brain Connect. 6, 795–803. doi: 10.1089/brain.2015.0401
Pustejovsky, J. E., and Rodgers, M. A. (2019). Testing for funnel plot asymmetry of standardized mean differences. Res. Synth. Methods 10, 57–71. doi: 10.1002/jrsm.1332
Qiu, D., Ge, Z., Mei, Y., Wang, W., Xiong, Z., and Li, X. (2023). Mapping brain functional networks topological characteristics in new daily persistent headache: a magnetoencephalography study. J. Headache Pain 24:161. doi: 10.1186/s10194-023-01695-x
Rubinov, M., and Sporns, O. (2010). Complex network measures of brain connectivity: uses and interpretations. NeuroImage 52, 1059–1069. doi: 10.1016/j.neuroimage.2009.10.003
Shi, M., Yang, D. D., Zhou, Y., Zhao, H., and Fang, Y. (2019). Analysis of migraine induced monitoring imaging data by multilayer mixed cluster detection. J. Med. Imaging Health Inform. 9, 1278–1283. doi: 10.1166/jmihi.2019.2729
Shi, Y., Zeng, W., Nie, W., and Yang, J. (2020). Multi-channel hierarchy functional integration analysis between large-scale brain networks for migraine: an fMRI study. NeuroImage. Clinical 28:102462. doi: 10.1016/j.nicl.2020.102462
Silvestro, M., Tessitore, A., Caiazzo, G., Scotto Di Clemente, F., Trojsi, F., Cirillo, M., et al. (2021). Disconnectome of the migraine brain: a “connectopathy” model. J. Headache Pain 22:102. doi: 10.1186/s10194-021-01315-6
Slinger, G., Otte, W. M., Braun, K. P. J., and van Diessen, E. (2022). An updated systematic review and meta-analysis of brain network organization in focal epilepsy: looking back and forth. Neurosci. Biobehav. Rev. 132, 211–223. doi: 10.1016/j.neubiorev.2021.11.028
Stang, A. (2010). Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 25, 603–605. doi: 10.1007/s10654-010-9491-z
Ta Dinh, S., Nickel, M. M., Tiemann, L., May, E. S., Heitmann, H., and Hohn, V. D. (2019). Brain dysfunction in chronic pain patients assessed by resting-state electroencephalography. Pain 160, 2751–2765. doi: 10.1097/j.pain.0000000000001666
Termenon, M., Achard, S., Jaillard, A., and Delon-Martin, C. (2016). The “hub disruption index,” a reliable index sensitive to the brain networks reorganization. A study of the Contralesional hemisphere in stroke. Front. Comput. Neurosci. 10:84. doi: 10.3389/fncom.2016.00084
Treede, R.-D., Rief, W., Barke, A., Aziz, Q., Bennett, M. I., and Benoliel, R. (2019). Chronic pain as a symptom or a disease: the IASP classification of chronic pain for the international classification of diseases (ICD-11). Pain 160, 19–27. doi: 10.1097/j.pain.0000000000001384
Tu, Y., Jung, M., Gollub, R. L., Napadow, V., Gerber, J., and Ortiz, A. (2019). Abnormal medial prefrontal cortex functional connectivity and its association with clinical symptoms in chronic low back pain. Pain 160, 1308–1318. doi: 10.1097/j.pain.0000000000001507
Tu, Y., Wang, J., Li, Z., Xiong, F., and Gao, F. (2023). Topological alterations in white matter structural networks in fibromyalgia. Neuroradiology 65, 1737–1747. doi: 10.1007/s00234-023-03225-7
Uddin, L. Q., Yeo, B. T. T., and Spreng, R. N. (2019). Towards a universal taxonomy of macro-scale functional human brain networks. Brain Topogr. 32, 926–942. doi: 10.1007/s10548-019-00744-6
Van Aert, R. C. M., Wicherts, J. M., and Van Assen, M. A. L. M. (2016). Conducting Meta-analyses based on p values: reservations and recommendations for applying p-uniform and p-curve. Perspect. Psychol. Sci. 11, 713–729. doi: 10.1177/1745691616650874
Wijk, B. C. M.van, Stam, C. J., and Daffertshofer, A. (2010). Comparing brain networks of different size and connectivity density using graph theory. PLoS One 5:e13701. doi: 10.1371/journal.pone.0013701
Viechtbauer, W. (2005). Bias and efficiency of meta-analytic variance estimators in the random-effects model. J. Educ. Behav. Stat. 30, 261–293. doi: 10.3102/10769986030003261
Wada, A., Shizukuishi, T., Kikuta, J., Yamada, H., Watanabe, Y., Imamura, Y., et al. (2017). Altered structural connectivity of pain-related brain network in burning mouth syndrome—investigation by graph analysis of probabilistic tractography. Neuroradiology 59, 525–532. doi: 10.1007/s00234-017-1830-2
Wan, X., Wang, W., Liu, J., and Tong, T. (2014). Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 14:135. doi: 10.1186/1471-2288-14-135
Wang, H., Labus, J. S., Griffin, F., Gupta, A., Bhatt, R. R., and Sauk, J. S. (2022). Functional brain rewiring and altered cortical stability in ulcerative colitis. Mol. Psychiatry 27, 1792–1804. doi: 10.1038/s41380-021-01421-6
Wang, H., Yan, X., Zhang, Q., Wu, Q., Qiu, L., and Zhou, J. (2024). Altered small-world and disrupted topological properties of functional connectivity networks in patients with nonarteritic anterior ischemic optic neuropathy. Clin. Neurol. Neurosurg. 236:108101. doi: 10.1016/j.clineuro.2023.108101
Wu, M., Jiang, X., Qiu, J., Fu, X., and Niu, C. (2020). Gray and white matter abnormalities in primary trigeminal neuralgia with and without neurovascular compression. J. Headache Pain 21:136. doi: 10.1186/s10194-020-01205-3
Wu, D., Zhou, Y., Xiang, J., Tang, L., Liu, H., Huang, S., et al. (2016). Multi-frequency analysis of brain connectivity networks in migraineurs: a magnetoencephalography study. J. Headache Pain 17, 1–10. doi: 10.1186/s10194-016-0636-7
Xin, H., Yang, B., Jia, Y., Qi, Q., Wang, Y., and Wang, L. (2024). Graph metrics reveal brain network topological property in neuropathic pain patients: A systematic review. J. Pain Res. 17, 3277–3286. doi: 10.2147/JPR.S483466
Xu, S., Deng, W., Qu, Y., Lai, W., Huang, T., and Rong, H. (2021). The integrated understanding of structural and functional connectomes in depression: A multimodal meta-analysis of graph metrics. J. Affect. Disord. 295, 759–770. doi: 10.1016/j.jad.2021.08.120
Yang, P.-L., Kamp, K. J., Burr, R. L., Tang, H.-Y. J., Dobra, A., Shulman, R. J., et al. (2023). Age differences in core symptoms and symptom relationships in patients with irritable bowel syndrome: a network analysis. Am. J. Gastroenterol. 118, 1648–1655. doi: 10.14309/ajg.0000000000002280
Yang, B., Xin, H., Wang, L., Qi, Q., Wang, Y., and Jia, Y. (2024). Distinct brain network patterns in complete and incomplete spinal cord injury patients based on graph theory analysis. CNS Neurosci. Ther. 30:e14910. doi: 10.1111/cns.14910
Yang, J., Yue, K., Sun, J., Pan, C., Wu, X., and Cheng, Y. (2025). Altered functional network topology properties to detect anxiety and depression caused by Crohn’s disease and disease severity. Brain Res. Bull. 221:111187. doi: 10.1016/j.brainresbull.2024.111187
Zalesky, A., Fornito, A., Harding, I. H., Cocchi, L., Yücel, M., and Pantelis, C. (2010). Whole-brain anatomical networks: does the choice of nodes matter? NeuroImage 50, 970–983. doi: 10.1016/j.neuroimage.2009.12.027
Zhang, Y.-P., Hong, G.-H., and Zhang, C.-Y. (2022b). Brain network changes in lumbar disc herniation induced chronic nerve roots compression syndromes. Neural Plast. 2022, 1–10. doi: 10.1155/2022/7912410
Zhang, Y., Liu, J., Li, L., Du, M., Fang, W., Wang, D., et al. (2014). A study on small-world brain functional networks altered by postherpetic neuralgia. Magn. Reson. Imaging 32, 359–365. doi: 10.1016/j.mri.2013.12.016
Zhang, J., Su, J., Wang, M., Zhao, Y., Zhang, Q.-T., and Yao, Q. (2017). The posterior insula shows disrupted brain functional connectivity in female Migraineurs without Aura based on Brainnetome atlas. Sci. Rep. 7:16868. doi: 10.1038/s41598-017-17069-8
Zhang, P., Wan, X., Ai, K., Zheng, W., Liu, G., and Wang, J. (2022a). Rich-club reorganization and related network disruptions are associated with the symptoms and severity in classic trigeminal neuralgia patients. NeuroImage: Clin. 36:103160. doi: 10.1016/j.nicl.2022.103160
Zhou, X., Wu, S., Wang, K., Chen, L., Hong, S., and Tian, Y. (2024). Default mode network and dorsal attentional network connectivity changes as neural markers of spinal manipulative therapy in lumbar disc herniation. Sci. Rep. 14:29541. doi: 10.1038/s41598-024-81126-2
Keywords: functional connectivity, structural connectivity, graph theory, brain topology, network analysis, chronic pain
Citation: Butry L, Thomä J, Elsenbruch S, Icenhour A, Rehmann R, Enax-Krumova E and Schlaffke L (2025) Brain network properties in chronic pain—a systematic review and meta-analysis of graph-based connectivity metrics. Front. Neurosci. 19:1672542. doi: 10.3389/fnins.2025.1672542
Edited by:
Lester Melie-Garcia, University of Basel, SwitzerlandReviewed by:
Xiang Liu, Michigan State University, United StatesSilke Kreitz, University of Erlangen Nuremberg, Germany
Copyright © 2025 Butry, Thomä, Elsenbruch, Icenhour, Rehmann, Enax-Krumova and Schlaffke. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lionel Butry, bGlvbmVsYnV0cnlAZ21haWwuY29t
†These authors have contributed equally to this work and share last authorship