 Michal Yalon1†
Michal Yalon1† Ruty Mehrian-Shai
Ruty Mehrian-Shai- 1Pediatric Hemato-Oncology, Edmond and Lilly Safra Children's Hospital and Cancer Research Center, Sheba Medical Center, Ramat Gan, Israel
- 2The Sackler School of Medicine, Tel-Aviv University, Tel Aviv, Israel
- 3Department of Pediatric Neurosurgery, Dana Children's Hospital, Tel-Aviv-Sourasky Medical Center, Tel Aviv, Israel
Pediatric brain tumors are the most common solid tumor type and the leading cause of cancer-related death in children. The immune system plays an important role in cancer pathogenesis and in the response to immunotherapy treatments. T lymphocytes are key elements for the response of the immune system to cancer cells and have been associated with prognosis of different cancers. Neutrophils on the other hand, which secrete pro-angiogenic and anti-apoptotic factors, enhance the ability of tumor cells to grow and develop into metastases. We conducted a retrospective study of 120 pediatric brain cancer patients and 171 elective pediatric patients hospitalized in Dana Children's Hospital and Sheba Medical Center. Data on age, sex, treatment, lymphocyte, neutrophil, and monocyte count were collected from routinely performed preoperative blood tests. Neutrophil-to-lymphocyte ratio (NLR), and the lymphocyte-to-monocyte ratio (LMR) were calculated and significance was determined by paired T test. p < 0.05 was considered as statistically significant. NLR was significantly higher in the pediatric brain cancer patients. The high NLR in pediatric brain cancer patients is the result of a combination of low lymphocytes and high neutrophils. Both of these factors can have a role in cancer development and propagation and also in response to therapy.
Introduction
Pediatric brain tumors are the most common solid tumor type and the leading cause of cancer-related deaths in children aged 0–14 years (1). There is increasing evidence that malfunction of immune system may contribute to tumor development. Failure to eliminate tumor cells or keeping the tumor cells in a dormant state by the immune system are included in the “hallmarks of cancer” (2). Understanding these underlying mechanisms has provided a basis for the development of new immunotherapies against tumors.
Lymphocytes have, among others, an anti-tumor effect (3). T lymphocytes are key elements to eliminate cancer cells and their dysfunction have been associated with development of cancer (4) and prognosis for several cancer types.
Neutrophils and monocytes on the other hand, may promote tumor progression (5). Neutrophils which secrete pro-angiogenic and anti-apoptotic factors, enhance the ability of tumor cells to grow and develop into metastases (6). Elevated numbers of neutrophils in the peripheral blood is associated with poor outcome in several types of cancers (7). Tumor-associated neutrophils can acquire a pro-tumor phenotype, supporting tumor growth, and suppressing the antitumor immune response (8). Myeloid-derived suppressor cells (MDSC) which are closely related to neutrophils and monocytes (9) play a major role in suppression of T cells (10, 11). Not only are levels of MDSC increased in the blood of patients with cancer, MDSC frequencies correlate to clinical cancer stage in several cancers including bladder cancer (12) and breast cancer (13).
Neutrophils, lymphocytes and monocytes have prognostic value in patients with a variety of common solid tumors (14). These patients are characterized by an increase in circulating neutrophil levels accompanied by a fall in circulating lymphocyte levels thus the neutrophil to lymphocyte ratio (NLR) is increased. In general, the blood NLR is high in patients with more advanced or aggressive cancers (15) and correlates with poor survival of patients with many solid tumors (16, 17).
Lymphocyte-to-monocyte ratio (LMR) has been suggested to be an important factor for predicting prognosis in patients with lung cancer, colon cancer and hematologic malignancies (18, 19). In a meta-analysis of adult solid tumors it was concluded that low pre-treatment LMR is an unfavorable prognostic factor (20).
In this study we investigated NLR and LMR in pediatric brain cancer patients on day of diagnosis before any treatment administration.
Methods
Clinical data from pediatric brain cancer patients (M = malignant group) and elective pediatric patients hospitalized for hernia repair were retrospectively analyzed. Exclusion criteria were steroid treatment before the blood test and a history of concomitant diseases. Age, Sex, treatment, blood count plus differential were collected from blood tests performed before surgery in both groups. NLR, and the LMR were calculated and significance was determined by paired T-test. p < 0.05 was considered as statistically significant. ANOVA test was used to compare mean of NLR value in different brain tumor types.
Results
Clinical data from 120 pediatric brain cancer patients and 171 elective pediatric patients hospitalized for hernia repair were retrospectively analyzed. The study was approved by the ethical review boards of both Sheba and Tel Aviv Sourasky Medical Centers and was consistent with the declaration of Helsinki. Cancer patients who received dexacort before the blood test were excluded. Children from the elective hernia surgery control group with known background diseases were also excluded. Ninety-nine cancer and 62 control patients that met the inclusion criteria and had all the data in the medical records were included in the analysis. Brain cancer patients consisted of 37 astrocytoma patients, 27 medulloblastoma patients, 25 patients with pilocytic astrocytoma, and 10 glioblastoma patients. Age, Sex, treatment, lymphocyte, Neutrophil count, and monocyte count were collected from routinely performed preoperative blood tests. NLR and the LMR were calculated and significance was determined by paired T-test. P < 0.05 was considered as statistically significant.
Male/female ratios in the study and control group were 64%/36% and 61%/29%, respectively. Mean age was 10.26 and 8.7 years old, respectively. No significant NLR and LMR differences were found between males and females in the patient group. Table 1 summarizes the blood count results, differential, NLR, and LMR in both groups.
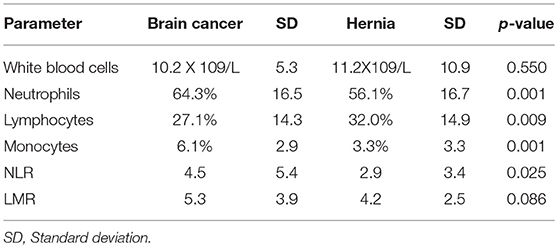
Table 1. Blood count results, differential, NLR, and LMR in brain cancer and hernia groups.
The mean percentage of neutrophils was higher in the patient group (64.3%) compared to the control group (56.11%) p = 0.001. In contrast, the mean percentage of lymphocytes was significantly higher in the control group (32.08%) compared to the patient group (27.11%) p = 0.009. As a result, the NLR was significantly higher in the patient group (4.59) compared to the control group (2.96) p = 0.025. Although the mean percentage of monocytes was higher in the patient group (6.1%) compared to the control group (3.3%) p = 0.001, there was no significant difference in LMR between the patient group (5.3) compared to the control group (4.2) (p = 0.08).
Table 2 summarizes the mean NLR results in different brain tumor types in children. Although NLR values of astrocytoma and pilocytic astrocytoma are lower than glioblastoma and medulloblastoma, no significant difference was found between the mean of NLR value in different tumor types by ANOVA test {F = 3.75, p = 0.13}.
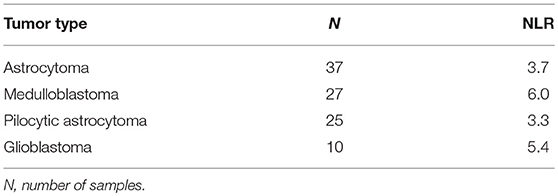
Table 2. NLR value results in different brain tumor types in children.
Discussion
Pediatric cancers and especially solid tumors can have devastating effects on young lives and their families. There is increasing evidence that failures of the immune system may contribute to tumor development. Lymphocytes have an important role in tumor cells elimination. Neutrophils and monocytes on the other hand, may promote tumor progression. In fact, suppression of the immune response to cancer cells is one of the impediments to develop effective immunotherapeutic approaches for glioma patients (21). Overcoming the suppression can be done by blocking the inhibitory signals of the immune system by anti CTLA4 and anti PD1/PDL1 therapy (22). On the other hand, persisting response of the inflammatory milieu paves the way to cancer (23). Neutrophils trigger and sustain a state of chronic inflammation (6) and high systematic immune-inflammation is significantly associated with a lower overall survival rate of patients with colon cancer (24), lung cancer (25), and breast cancer (26). Suppressing this arm of the immune response is necessary to limit proliferative signaling, angiogenesis, migration and invasion processes (2). Inhibitors of inflammatory pathways have been successful in pre-clinical tumor models and early clinical trials (27).
It has been shown that elevated NLR is predictive of poorer overall survival in patients with hepatocellular/ squamous cell carcinoma, GBM (28–30), pancreatic ductal adenocarcinoma (31), ovarian cancer (32) and pediatric sarcoma (33). In addition, preoperative elevated NLR reflects a systemic inflammatory response and is a predictor of poor survival in gastric cancer (16). Finally, high NLR is associated with poorer outcomes in patients receiving immune checkpoint inhibitors (34). In our study, pediatric brain cancer patients' blood samples present both increased neutrophil count and decreased lymphocyte count resulting in significantly higher NLR. Moreover, although no significant difference was found between the mean of NLR value in different tumor types in children, NLR values of astrocytoma and pilocytic astrocytoma are lower than glioblastoma and medulloblastoma. It is important to note that pediatric astrocytoma and pilocytic astrocytoma are with a more favorable prognosis compared to glioblastoma and medulloblastoma.
Using the body's own immune system to fight cancer is increasingly desirable treatment for cancer because of its' potential to specifically target the tumor while limiting damage to normal tissue. Because lymphocytes account for only 20–40% of the total WBC count, low levels of T cells may go unnoticed when WBC count is checked without a differential count of CD4+ (helper) T cells/CD8+ (suppressor) T cells/B cells. Reduced lymphocyte numbers may contribute to cancer development and may affect treatment, especially the current promising treatment of immunotherapy. Furthermore, the success of immunotherapy in tumors of the central nervous system depends on the immune microenvironment and lymphocyte tracking through the blood-brain barrier (BBB) into the central nervous system (35). The brain is presumably an immune-privileged organ due to the BBB (36). During gliomagenesis, the BBB is broken and circulating immune cells including T cells, B cells, macrophages, and MDSC cross the BBB (37). The resulting bi-directional communication between immune cells and glioma cells create an immunosuppressed microenvironment that promotes tumor survival and growth (38). Glioma-associated microglia and macrophages are attracted to the tumor (39) and can be polarized into M2 becoming tumor-supportive and immunosuppressive cells (40). The glioma immunosuppressive environment is further enhanced by elevated numbers of regulatory T cells (41). Immunophenotyping of pediatric brain tumors reveal immunosuppressive phenotype in higher grade tumors with more regulatory T cells present in these tumor types (42). Interestingly, it has been shown recently that intracranial tumors like GBM may cause depletion of mature T cells (43). The tumor imposed depletion of Sphingosine-1-phosphate receptor 1 from the T cell surface prevents their trafficking from lymphoid organs into the circulation. It may well be that in pediatric brain cancer patients the T cells are sequestered in the lymph nodes and can inversely be released to fight cancer by manipulations yet to be discovered. Thus, Immunotherapy via adoptive cell transfer, especially with T cells engineered to express chimeric antigen receptors, represents a promising approach (44). Recent evidence has demonstrated that systemic therapy for brain tumors is not limited by the BBB (45). Cellular therapy as well as reversing immune-suppression through immune checkpoint blockade are showing promising results for GBM (46). In light of these findings the prognostic as well as treatment response prediction value of the NLR warrants prospective validation in large cohorts of children with CNS tumors.
Ethics Statement
The study was retrospective study of clinical files. Clinical data from 120 pediatric brain cancer patients and 171 elective pediatric patients hospitalized for hernia repair were retrospectively analyzed. The study was approved by the ethical review boards of both Sheba and Tel Aviv Sourasky Medical Centers and was consistent with the declaration of Helsinki.
Author Contributions
RM-S and DJ contributed to implementation, analysis, and interpretation of the data. RM-S, DJ, MY, AT, EF, and SC were involved in experimental design, in the writing of the manuscript, and have read and approved the final version.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Grob ST, Levy JMM. Improving diagnostic and therapeutic outcomes in pediatric brain tumors. Mol Diagn Ther. (2018) 22:25–39. doi: 10.1007/s40291-017-0299-3
2. Hanahan D, Weinberg RA. Hallmarks of cancer: the next generation. Cell. (2011) 144:646–74. doi: 10.1016/j.cell.2011.02.013
3. Lee HJ, Hong CY, Kim MH, Lee YK, Nguyen-Pham TN, Park BC, et al. In vitro induction of anterior gradient-2-specific cytotoxic T lymphocytes by dendritic cells transduced with recombinant adenoviruses as a potential therapy for colorectal cancer. Exp Mol Med. (2012) 44:60–7. doi: 10.3858/emm.2012.44.1.006
4. Thommen DS, Schumacher TN. T Cell dysfunction in cancer. Cancer Cell. (2018) 33:547–62. doi: 10.1016/j.ccell.2018.03.012
6. Rosales C. Neutrophil: a cell with many roles in inflammation or several cell types? Front Physiol. (2018) 9:113. doi: 10.3389/fphys.2018.00113
7. Schmidt H, Bastholt L, Geertsen P, Christensen IJ, Larsen S, Gehl J, et al. Elevated neutrophil and monocyte counts in peripheral blood are associated with poor survival in patients with metastatic melanoma: a prognostic model. Br J Cancer. (2005) 93:273–8. doi: 10.1038/sj.bjc.6602702
8. Fridlender ZG, Albelda SM. Tumor-associated neutrophils: friend or foe? Carcinogenesis. (2012) 33:949–55. doi: 10.1093/carcin/bgs123
9. Aarts CEM, Kuijpers TW. Neutrophils as myeloid-derived suppressor cells. Eur J Clin Invest. (2018) 48 (Suppl 2):e12989. doi: 10.1111/eci.12989
10. Bronte V, Zanovello P. Regulation of immune responses by L-arginine metabolism. Nat Rev Immunol. (2005) 5:641–54. doi: 10.1038/nri1668
11. Habibi D, Jalili RB, Forouzandeh F, Ong CJ, Ghahary A. High expression of IMPACT protein promotes resistance to indoleamine 2,3-dioxygenase-induced cell death. J Cell Physiol. (2010) 225:196–205. doi: 10.1002/jcp.22220
12. Yuan XK, Zhao XK, Xia YC, Zhu X, Xiao P. Increased circulating immunosuppressive CD14(+)HLA-DR(-/low) cells correlate with clinical cancer stage and pathological grade in patients with bladder carcinoma. J Int Med Res. (2011) 39:1381–91. doi: 10.1177/147323001103900424
13. Diaz-Montero CM, Salem ML, Nishimura MI, Garrett-Mayer E, Cole DJ, Montero AJ. Increased circulating myeloid-derived suppressor cells correlate with clinical cancer stage, metastatic tumor burden, and doxorubicin-cyclophosphamide chemotherapy. Cancer Immunol Immunother. (2009) 58:49–59. doi: 10.1007/s00262-008-0523-4
14. Leitch EF, Chakrabarti M, Crozier JE, McKee RF, Anderson JH, Horgan PG, et al. Comparison of the prognostic value of selected markers of the systemic inflammatory response in patients with colorectal cancer. Br J Cancer. (2007) 97:1266–70. doi: 10.1038/sj.bjc.6604027
15. Guthrie GJ, Charles KA, Roxburgh CS, Horgan PG, McMillan DC, Clarke SJ. The systemic inflammation-based neutrophil-lymphocyte ratio: experience in patients with cancer. Crit Rev Oncol Hematol. (2013) 88:218–30. doi: 10.1016/j.critrevonc.2013.03.010
16. Paramanathan A, Saxena A, Morris DL. A systematic review and meta-analysis on the impact of pre-operative neutrophil lymphocyte ratio on long term outcomes after curative intent resection of solid tumours. Surg Oncol. (2014) 23:31–9. doi: 10.1016/j.suronc.2013.12.001
17. Templeton AJ, McNamara MG, Seruga B, Vera-Badillo FE, Aneja P, Ocaña A, et al. Prognostic role of neutrophil-to-lymphocyte ratio in solid tumors: a systematic review and meta-analysis. J Natl Cancer Inst. (2014) 106:dju124. doi: 10.1093/jnci/dju124
18. Hu P, Shen H, Wang G, Zhang P, Liu Q, Du J. Prognostic significance of systemic inflammation-based lymphocyte- monocyte ratio in patients with lung cancer: based on a large cohort study. PLoS ONE. (2014) 9:e108062. doi: 10.1371/journal.pone.0108062
19. Peng J, Li H, Ou Q, Lin J, Wu X, Lu Z, et al. Preoperative lymphocyte-to-monocyte ratio represents a superior predictor compared with neutrophil-to-lymphocyte and platelet-to-lymphocyte ratios for colorectal liver-only metastases survival. Onco Targets Ther. (2017) 10:3789–99. doi: 10.2147/OTT.S140872
20. Nishijima TF, Muss HB, Shachar SS, Tamura K, Takamatsu Y. Prognostic value of lymphocyte-to-monocyte ratio in patients with solid tumors: a systematic review and meta-analysis. Cancer Treat Rev. (2015) 41:971–8. doi: 10.1016/j.ctrv.2015.10.003
21. Grauer OM, Nierkens S, Bennink E, Toonen LW, Boon L, Wesseling P, et al. CD4+FoxP3+ regulatory T cells gradually accumulate in gliomas during tumor growth and efficiently suppress antiglioma immune responses in vivo. Int J Cancer. (2007) 121:95–105. doi: 10.1002/ijc.22607
22. Fan Y, Zhang C, Jin S, Gao Z, Cao J, Wang A, et al. Progress of immune checkpoint therapy in the clinic (Review). Oncol Rep. (2019) 41:3–14. doi: 10.3892/or.2018.6819
24. Tao MY, Wang ZH, Zhang MH, Ma TH, Yang XZ, Wu SN, et al. Prognostic value of the systematic immune-inflammation index among patients with operable colon cancer: a retrospective study. Medicine. (2018) 97:e13156. doi: 10.1097/MD.0000000000013156
25. Gao Y, Zhang H, Li Y, Wang D, Ma Y, Chen Q. Preoperative increased systemic immune-inflammation index predicts poor prognosis in patients with operable non-small cell lung cancer. Clin Chim Acta. (2018) 484:272–7. doi: 10.1016/j.cca.2018.05.059
26. Qian Y, Tao J, Li X, Chen H, Lu Q, Yang J, et al. Peripheral inflammation/immune indicators of chemosensitivity and prognosis in breast cancer patients treated with neoadjuvant chemotherapy. Onco Targets Ther. (2018) 11:1423–32. doi: 10.2147/OTT.S148496
27. Marelli G, Sica A, Vannucci L, Allavena P. Inflammation as target in cancer therapy. Curr Opin Pharmacol. (2017) 35:57–65. doi: 10.1016/j.coph.2017.05.007
28. Mascarella MA, Mannard E, Silva SD, Zeitouni A. Neutrophil-to-lymphocyte ratio in head and neck cancer prognosis: a systematic review and meta-analysis. Head Neck. (2018) 40:1091–100. doi: 10.1002/hed.25075
29. Lopes M, Carvalho B, Vaz R, Linhares P. Influence of neutrophil-lymphocyte ratio in prognosis of glioblastoma multiforme. J Neurooncol. (2018) 136:173–80. doi: 10.1007/s11060-017-2641-3
30. Najjar M, Agrawal S, Emond JC, Halazun KJ. Pretreatment neutrophil-lymphocyte ratio: useful prognostic biomarker in hepatocellular carcinoma. J Hepatocell Carcinoma. (2018) 5:17–28. doi: 10.2147/JHC.S86792
31. Abe T, Nakata K, Kibe S, Mori Y, Miyasaka Y, Ohuchida K, et al. Prognostic value of preoperative nutritional and immunological factors in patients with pancreatic ductal adenocarcinoma. Ann Surg Oncol. (2018) 25:3996–4003. doi: 10.1245/s10434-018-6761-6
32. Yang Z, Gu JH, Guo CS, Li XH, Yang WC. Preoperative neutrophil-to-lymphocyte ratio is a predictor of survival of epithelial ovarian cancer: a systematic review and meta-analysis of observational studies. Oncotarget. (2017) 8:46414–24. doi: 10.18632/oncotarget.16793
33. Vasquez L, Leon E, Beltran B, Maza I, Oscanoa M, Geronimo J. Pretreatment neutrophil-to-lymphocyte ratio and lymphocyte recovery: independent prognostic factors for survival in pediatric sarcomas. J Pediatr Hematol Oncol. (2017) 39:538–46. doi: 10.1097/MPH.0000000000000911
34. Sacdalan DB, Lucero JA, Sacdalan DL. Prognostic utility of baseline neutrophil-to-lymphocyte ratio in patients receiving immune checkpoint inhibitors: a review and meta-analysis. Onco Targets Ther. (2018) 11:955–65. doi: 10.2147/OTT.S153290
35. Ameratunga M, Coleman N, Welsh L, Saran F, Lopez J. CNS cancer immunity cycle and strategies to target this for glioblastoma. Oncotarget. (2018) 9:22802–16. doi: 10.18632/oncotarget.24896
36. Wilson EH, Weninger W, Hunter CA. Trafficking of immune cells in the central nervous system. J Clin Invest. (2010) 120:1368–79. doi: 10.1172/JCI41911
37. Gieryng A, Pszczolkowska D, Walentynowicz KA, Rajan WD, Kaminska B. Immune microenvironment of gliomas. Lab Invest. (2017) 97:498–518. doi: 10.1038/labinvest.2017.19
38. Galvao RP, Zong H. Inflammation and gliomagenesis: bi-directional communication at early and late stages of tumor progression. Curr Pathobiol Rep. (2013) 1:19–28. doi: 10.1007/s40139-012-0006-3
39. Okada M, Saio M, Kito Y, Ohe N, Yano H, Yoshimura S, et al. Tumor-associated macrophage/microglia infiltration in human gliomas is correlated with MCP-3, but not MCP-1. Int J Oncol. (2009) 34:1621–7. doi: 10.3892/ijo_00000292
40. Wu SY, Watabe K. The roles of microglia/macrophages in tumor progression of brain cancer and metastatic disease. Front Biosci. (2017) 22:1805–29. doi: 10.2741/4573
41. El Andaloussi A, Lesniak MS. CD4+ CD25+ FoxP3+ T-cell infiltration and heme oxygenase-1 expression correlate with tumor grade in human gliomas. J Neurooncol. (2007) 83:145–52. doi: 10.1007/s11060-006-9314-y
42. Plant AS, Koyama S, Sinai C, Solomon IH, Griffin GK, Ligon KL, et al. Immunophenotyping of pediatric brain tumors: correlating immune infiltrate with histology, mutational load, and survival and assessing clonal T cell response. J Neurooncol. (2018) 137:269–78. doi: 10.1007/s11060-017-2737-9
43. Chongsathidkiet P, Jackson C, Koyama S, Loebel F, Cui X, Farber SH, et al. Sequestration of T cells in bone marrow in the setting of glioblastoma and other intracranial tumors. Nat Med. (2018) 24:1459–68. doi: 10.1038/s41591-018-0135-2
44. Choi BD, Maus MV, June CH, Sampson JH. Immunotherapy for glioblastoma: adoptive T-cell strategies. Clin Cancer Res. (2019). 25:2042–8. doi: 10.1158/1078-0432.CCR-18-1625
45. Zhang I, Formenti SC, Knisely JPS. Immunotherapy plus stereotactic radiosurgery: building on the promise of precision medicine for CNS malignancies-PART 1: principles of combined treatment. Oncology. (2018) 32:e28–e32. Online available at: https://www.cancernetwork.com/oncology-journal/immunotherapy-plus-stereotactic-radiosurgery-building-promise-precision-medicine-cns-malignancies
Keywords: pediatric brain cancer, neutrophils, lymphocytes, NLR, LMR
Citation: Yalon M, Toren A, Jabarin D, Fadida E, Constantini S and Mehrian-Shai R (2019) Elevated NLR May Be a Feature of Pediatric Brain Cancer Patients. Front. Oncol. 9:327. doi: 10.3389/fonc.2019.00327
Received: 05 February 2019; Accepted: 11 April 2019;
Published: 30 April 2019.
Edited by:
Andrea Carai, Bambino Gesù Children Hospital (IRCCS), ItalyReviewed by:
Joseph Louis Lasky, Cure 4 The Kids, United StatesUte Katharina Bartels, Hospital for Sick Children, Canada
Copyright © 2019 Yalon, Toren, Jabarin, Fadida, Constantini and Mehrian-Shai. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ruty Mehrian-Shai, cnV0eS5zaGFpQHNoZWJhLmhlYWx0aC5nb3YuaWw=
†These authors have contributed equally to this work