 Michele Guida1*
Michele Guida1* Alessandro D'Alò1
Alessandro D'Alò1 Anita Mangia2
Anita Mangia2 Federica Di Pinto3Margherita Sonnessa4Anna Albano1Angela Sciacovelli1
Federica Di Pinto3Margherita Sonnessa4Anna Albano1Angela Sciacovelli1 Artor Niccoli Asabella5
Artor Niccoli Asabella5 Livia Fucci4
Livia Fucci4- 1Department of Medical Oncology, IRCCS Istituto Tumori “Giovanni Paolo II”, Bari, Italy
- 2Functional Biomorphology Laboratory, IRCCS Istituto Tumori “Giovanni Paolo II”, Bari, Italy
- 3Department of Pathology, Research Hospital, National Institute of Gastroenterology “S. De Bellis”, Castellana Grotte, Italy
- 4Department of Pathology, IRCCS Istituto Tumori “Giovanni Paolo II”, Bari, Italy
- 5Nuclear Medicine Unit, Department of Interdisciplinary Medicine, University of Bari Aldo Moro, Bari, Italy
Background: Merkel-cell carcinoma (MCC) is a rare, highly aggressive skin cancer typically involving elderly people. Surgery is usually the first treatment for primary tumor. In adjuvant setting, radiotherapy is effective in reducing local recurrence and in improving overall survival. Regarding advanced disease, systemic chemotherapy ended up disappointing results whereas antiPD1/antiPD-L1 immunotherapy recently gave relevant clinical benefits. Interestingly, about the half of MCC patients expresses high somatostatin receptors (SRs) to possibly represent a target for the therapeutic use of somatostatin analogs (SSAs). Nevertheless, SSAs have been little studied in MCC and cases treated with SSAs in association with checkpoint inhibitor immunotherapy have not been published yet.
Case Report: We report the case of a 73-year-old man affected by metastatic MCC of right arm previously treated with surgery and adjuvant radio and chemotherapy. Three years later the patient presented loco-regional relapse involving lateral-cervical, mediastinal, and submandibular lymph nodes with high value of chromogranin A and neuron specific enolase. Due to the high expression of SRs at octreoscan and immunoistochemistry, patient started octreotide 30 mg i.m. every 28 days with a good control of disease for about 2 years. A widespread progression of disease was reported afterwards. The patient started the antiPD-L1 avelumab immunotherapy, only recently available in Italy, while still taking SSA. The patient showed an impressive regression of the disease after only four cycles of avelumab until complete remission.
Conclusions: SSA could be a valid therapeutic option in patients with MCC with high SR expression. When combined with PD-1/PD-L1 immune-checkpoint inhibition, SSA is likely to enhance antiproliferative activity. Our case report provides the rationale to conduct a prospective trial and translational research to verify the efficacy and safety of combined SSA and checkpoint inhibitors for advanced MCC.
Introduction
Merkel-cell carcinoma (MCC) is a rare but highly aggressive skin cancer typically involving elderly people, although it has been also described in young adult and exceptionally in childhood (1).
Factors involved in the pathogenesis of MCC included age over 65 years, ultraviolet radiation exposure, immunosuppression, and infection by Merkel cell polyomavirus (MCPV) which is detected in almost 80% of MCC cases. Other primary cancers seem to increase the risk of MCC incidence, especially prior multiple myeloma, chronic lymphocytic leukemia, and malignant melanoma (2). Ultraviolet light exposure has been reported to induce an extremely high genome mutation rate, whereas MCPV-infected Merkel carcinoma cells show low rates of genome mutation (3).
MCC typically tends to grow locally, but soon it spreads to the locoregional lymph nodes and than through the blood circulation to distant organs, particularly to liver, lung, brain, and to bone (4).
Therapeutic management of MCC is controversial. Early diagnosis and adequate treatment of primary MCC are important prognostic factors. Surgery and radiotherapy are usually chosen in localized forms. Adjuvant radiotherapy showed effective in reducing the local recurrence and in increasing the overall survival (5).
Systemic chemotherapy has been used to treat advanced disease with disappointing results. First-line chemotherapy with platinum-based regimens produced high response rates of about 50–60%. The main therapeutic regimens included cis-platinum or carboplatin in association with etoposide or ifosfamide or anthracyclines. CAV regimen (cyclophosphamide + Adriamycin + Vincristine) was used in patients unfit for platinum-based regimens. Unfortunately, response duration was only a few months with PFS of 3–4 months. Moreover, treatment was associated to significant toxicity (6, 7).
Checkpoints inhibitors antiPD1/antiPD-L1 (Programmed Death Ligand1) immunotherapy have been recently investigated in the metastatic setting and positive results were reported (8–10). The antiPD-L1 avelumab was first tested in a multicentre phase 2 trial involving 88 patients with stage IV chemotherapy-refractory MCC. The response rate was 31.8%, including eight complete responses and 20 partial responses (8). Based on these results, the U.S. Food and Drug Administration granted accelerated approval of the antiPD-L1 avelumab to treat adults and children above 12 years with metastatic MCC.
Other two antiPD-1 antibodies have also been investigated in advanced MCC. Pembrolizumab was tested as first-line treatment in advanced MCC (9) whereas nivolumab was proposed as neoadjuvant therapy in patients with resectable MCC (10). In both studies, an objective response rate over 50% was reported. Of note, responses were observed in both patients with virus-positive tumors and those with virus-negative tumors (9–11).
Due to these new therapeutic options, chemotherapy is now indicated just for patients who are not candidates for immunotherapy or after immunotherapy failure.
About half of MCC expresses highly somatostatin receptors (SRs) that could represent a potential target for both imaging and treatment purposes (12). Somatostatin analogs (SSAs) have been used in the past with palliative intent for functioning neuro-endocrine tumors and remarkable results were reported. More recently, direct anti-proliferative effects of SSAs have also been demonstrated in neuroendocrine neoplasms (13). The use of SSA in MCC has been little studied (14) and cases of MCC treated with SSA in combination with checkpoint inhibitor immunotherapy have not been published yet.
We report for the first time the case of a metastatic MCC successfully treated first with SSA and then, when disease progressed, with SSA plus anti PD-L1 avelumab.
Case Report
A 73-year-old man affected by metastatic MCC on the right arm treated with surgery and adjuvant radio and chemotherapy came to our observation in December 2015. At the diagnosis, immunohistochemistry reported a Ki67 of 25% and a positivity for synaptophysin, chromogranin A, CK20, nuclear polyomavirus marker, and SSTR2A, whereas SSTR5A, PD-L1, and p63 (a transcription factor often associated with worse prognosis) were negative (Figure 1A). The tumor infiltrating lymphocytes (TILs) in the tumor microenvironment were moderate as was the infiltration of intra-tumor lymphocytes.
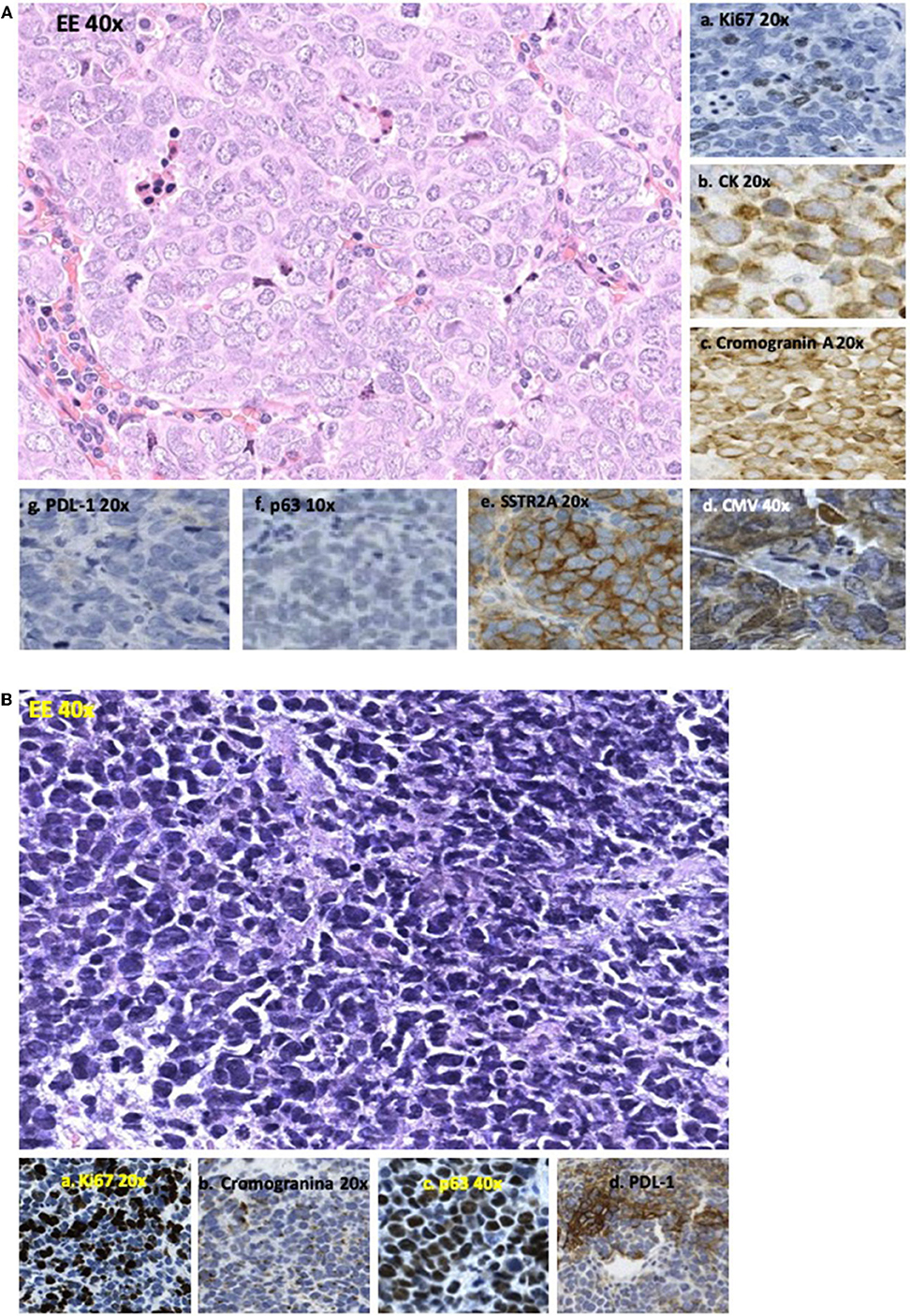
FIGURE 1. (A) Sample of lymph node metastasis performed before SSA therapy showing an epithelioid feature of cells with “salt and pepper” nuclei (EE40x). Immunohistochemistry showed (a) positivity for Ki67 in 25% of cells (20×); (b) positivity for CK20 with nuclear dot (20×); (c) positivity for chromogranin A with nuclear dot (20×); (d) nuclear positivity for poliomavirus Merkel cells carcinoma associated/CMV (40×); (e) diffuse and strong membranous positivity for somatostatin receptor 2A (SSTR2A) (20×); (f) negativity for p63 (10×); and (g) for PDL-1 (20×). (B) Sample of lymph node metastasis performed after disease progression to SSA therapy showing cells having smaller size than those of pre-treatment and a round shape with dark nuclei (40×). Immunohistochemistry showed (a) Ki67 positivity in 85% of cells (20×); (b) reduction of positivity for chromogranin (20×); (c) diffuse nuclear positivity for p63 (40×); (d) strong positivity for PDL-1 in 35% of neoplastic cells (10×).
Three years later the patient presented relapse involving loco-regional lymph nodes and the right lung with high value of chromogranin A (CgA) and neuron specific enolase (NSE).
Due to the high expression of SRs at octreoscan with 99mTc-EDDA/HYNIC-TOC (Figure 2) and at immunohistochemistry (Figure 1A), the patient started the SSA octreotide at the dose of 30 mg intramuscularly every 28 days obtaining a progressive decrease of serum markers and a partial regression of disease lasting over 2 years. After this long period, the patient presented disease progression in all known sites and new lesions at lung middle lobe and left adrenal gland. At this time, circulating CgA remained under normal value whereas NSE increased rapidly (Figure 4). A new lymph node biopsy was performed revealing a profound changing in the morphology of the neoplastic cells. Immunohistochemistry also showed a Ki67 of 85% compared to 25% of the first biopsy, whereas p63 and PD-L1 became strongly positive (Figure 1B). At this time, peritumoral TILs were very scarce and completely absent the intra-tumor lymphocytes component.
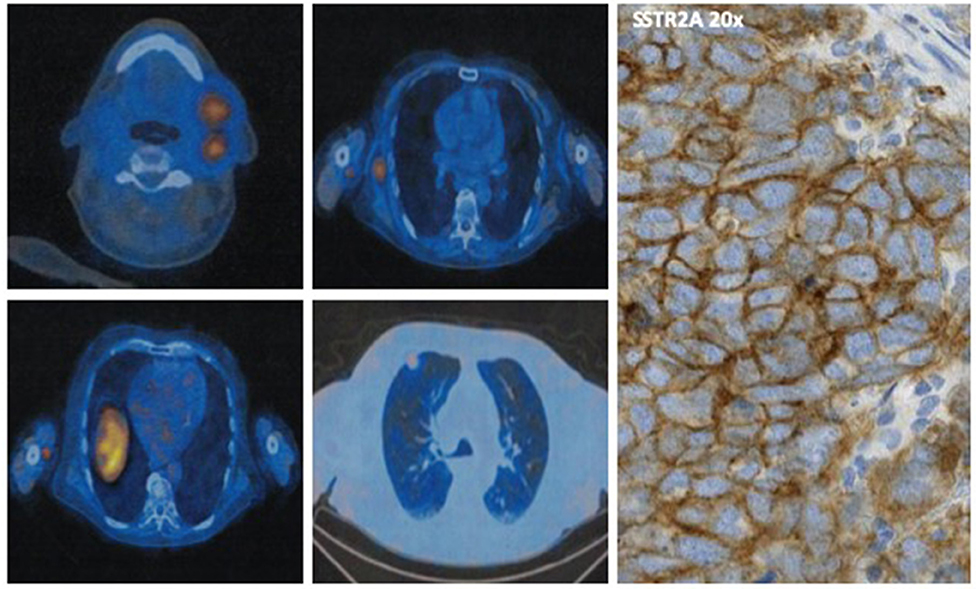
FIGURE 2. Octreoscan showing high uptake of 99mTc-EDDA/HYNIC-TOC in the right axillary and thoracic wall, in the left sub-mandibular and latero-cervical region, and at right superior pulmonary lobe in the sub-pleurical region. On the right is shown the membranous diffuse expression of SSTR2A on immunohistochemistry.
Considering the disease progression and the recent availability in Italy of the antiPD-L1 avelumab, the patient started this drug at the dose of 10 mg/kg intravenously every 2 weeks continuing octreotide at the same dose and timing. After four administrations of avelumab, an impressive response was observed until achieving a complete remission (Figures 3A,B). Also circulating NSE level progressively decreased until normal value (Figure 4).
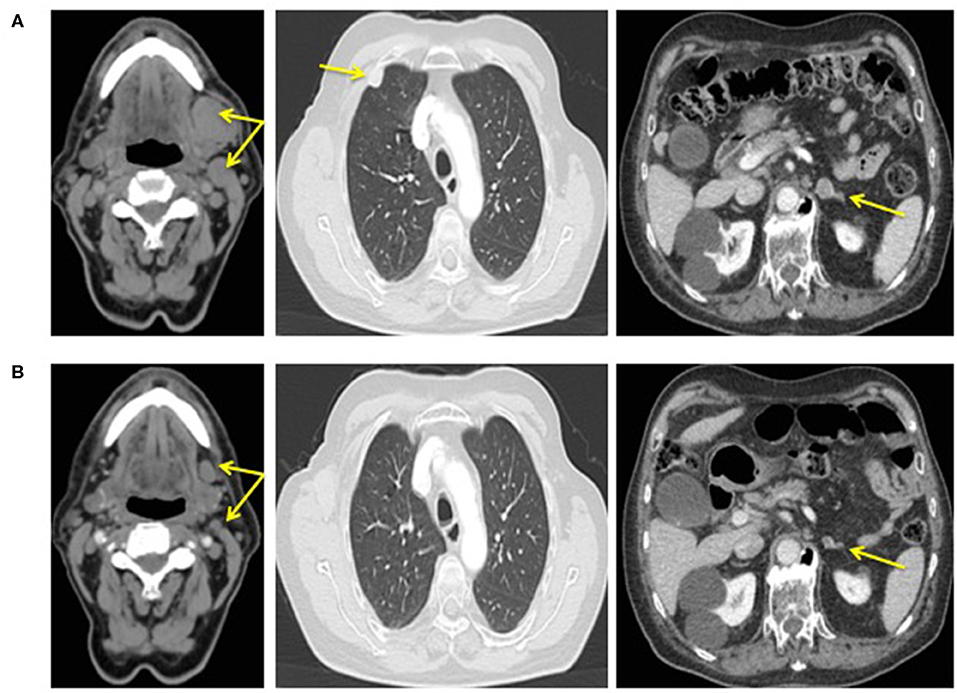
FIGURE 3. CT scan performed before therapy with the association octreotide plus avelumab (A) and after 10 months of therapy (B).
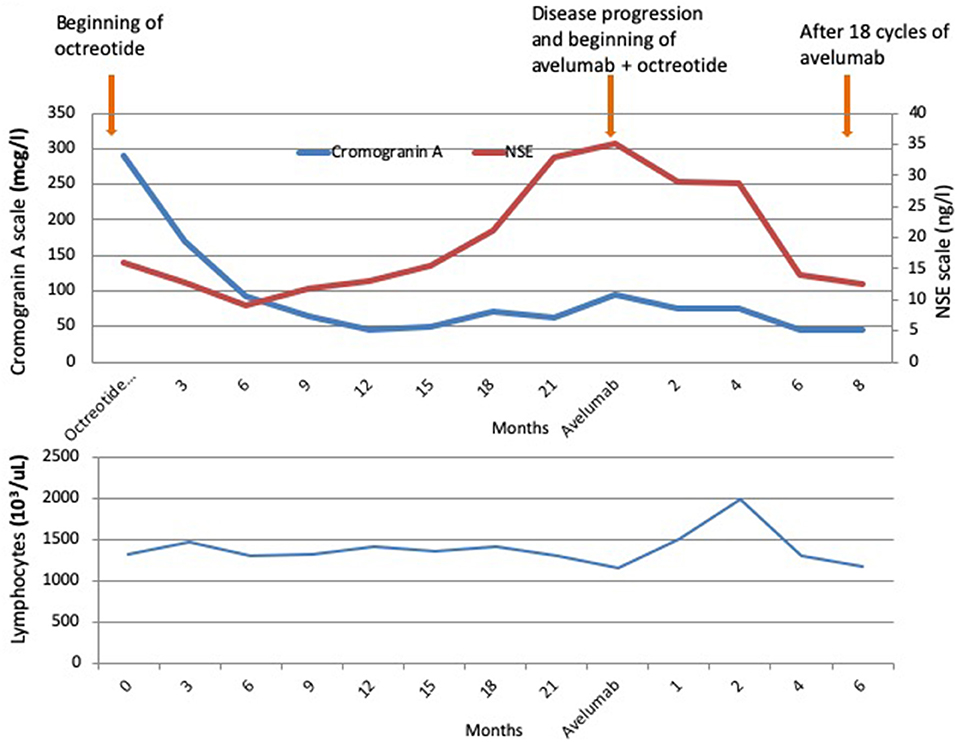
FIGURE 4. Behavior of chromogranin A (CgA), Neuron-Specific Enolase (NSE), and peripheral lymphocytes count during octreotide and then during the association of octreotide plus avelumab.
Peripheral lymphocytes remained quite under normal value during all SSA therapy period without significant variations. Nevertheless, when avelumab was started, a sudden and rapid increase just after the first administration of avelumab was noted reaching the maximum value at the second month of therapy. Then, lymphocytes progressively decreased until pre-treatment value (Figure 4).
Treatment was well tolerated by the patient with only mild hyposthenia reported.
At present, after 17 months of therapy, the patient is in good clinical status with complete remission of disease. He is continuing avelumab in combination with octreotide without remarkable side effects.
Discussion
Avelumab was the first-ever drug approved in advanced MCC after showing meaningful efficacy. In the second line setting after chemotherapy, the response rate reaches 33% with responses occurring on average after about 6 weeks of therapy. Early objective response to avelumab was associated with significant improved overall survival. Moreover, in patients who responded, about two-third remained relapse free after 2 years with half of patients and one-third of patients still alive at 1 and 2 years, respectively. When used in a first-line setting, PD-1/PD-L1 inhibitors including avelumab, pembrolizumab, and nivolumab are even more promising as objective responses were observed in ~50–70% of patients with a 2-year survival rate of about 70%. Due to these results, PD-1/PD-L1 inhibitors are considered the standard of care in advanced MCC and are currently being investigated in the adjuvant and neoadjuvant settings (9–11).
Somatostatin is a hormone with multiple actions such as endocrine, paracrine, and antiproliferative. The direct antiproliferative effects of somatostatin are mediated by its high affinity for somatostatin specific receptors (SRs) present on neuroendocrine neoplasms (15–17). Five sub-types of specific membrane receptors have been found in a lot of normal tissues as brain and leptomeningeal tissue, anterior pituitary gland, endocrine and exocrine pancreas, gastrointestinal mucosa, immune system cells (16, 17). Of note is that each type of tumor shows different sub-types of SRs and the amplitude of the antiproliferative activity of somatostatin analogs (SSAs) seems to correlate with the number of receptors present on the cellular surface (16, 17).
SSTR2A and 5 have been recently reported to be expressed in MCC in about 60 and 45%, respectively (12). Overall, at least one SR was expressed in 76.5% of cases and no association was found either with the severity of the disease, nor with clinical features, proliferative index of Ki 67, relapse-free survival, and overall survival. SRs expression between the primary skin tumor and the corresponding metastases was consistent in 43 and 86% for SRs 2A and SRs 5, respectively. The expression of SSTR2A but not SRs 5 was finally associated with MCPyV status (12).
Considering the expression of these receptors, this tumor may be candidate for SSAs therapy. To our knowledge, the use of SSAs in MCC has been little investigated with only three cases published in English literature and disappointing results were reported (14). No cases treated with SSAs plus checkpoints inhibitors have been published until now.
We obtained a good control of the disease for about 2 years using octreotide alone. Of note, when the patient presented a widespread progression of the disease, a radical change in terms of cell morphology and higher proliferative index were noted, whereas p63 and PD-L1 became strongly positive (Figure 1B). The behaviors of tumor markers also confirmed the biological switch of disease with CgA remaining within normal values and NSE slowly increased (Figure 4).
We obtained an impressive regression of the disease with avelumab in association with octreotide until complete remission lasting over 10 months without relevant side effects with only mild hyposthenia reported by our patient. Data from literature regarding the toxic profile of avelumab reported that this drug is associated with a very good toxicity profile. No treatment-related grade 4 adverse events or treatment-related deaths were reported. Moreover, grade 3 treatment-related adverse events occurred in only 6% of patients with lymphopenia, blood creatine phosphokinase increase, aminotransferase increase, and blood cholesterol increase being more common side effects. Finally, serious treatment-related adverse events included enterocolitis, infusion-related reaction, aminotransferases increased, chondrocalcinosis, synovitis, and interstitial nephritis. All side effects were effectively addressed with prompt recognition and appropriate management (8).
Interestingly, peripheral lymphocytes which showed no significant variation during SSA therapy, increased significantly after the first administrations of avelumab with the maximum value at the second month of therapy and then progressively decreased.
Although considerable therapeutic progress has been made in the MCC with the arrival of checkpoint inhibitors, about 50% of patients with advanced disease do not respond to immunotherapy. Unfortunately, no clear predictors of response are available yet. Regarding PD-L1, its prognostic value is controversial as well as its predictive role of response to checkpoint inhibitors. Although more remarkable responses have been reported in cancer overexpressing PD-L1 levels regardless of histology, as the case of our patient, even patients with low PD-L1 levels can have an important clinical benefit with immunotherapy. Our patient showed high expression of PD-L1 on tumoral cells before starting therapy with avelumab. Therefore, using PD-L1 as predictive factor is questionable for its weak and unreliable capability to discriminate responder from no-responder patients. Thus, PD-L1 could constitute one of the partners when associated with other finer and more specific parameters such as mutational load, tumor neoantigen burden, cytotoxic activity, and IFN gamma signature. It is urgent to identify new predictive factors of response to immunotherapy. It is thought that better understanding of tumor microenvironment and use of combined biomarkers are necessary to better identify patients who will benefit from PD-1/PD-L1 checkpoint blockade therapy. Moreover, new immunotherapeutic strategies are now being investigated both alone or in combinations to enhance the immune antitumoral response against (18, 19).
Our case demonstrates that SSA represents a valid therapeutic option in MCC patients expressing high SRs levels. When combined with check point inhibitors immunotherapy, SSA can safely enhance the anti-proliferative activity of immunotherapy with final strengthen results. Thus, it provides a rationale to conduct a prospective trial with an adequately powered sample to test the efficacy and safety of this combination and to optimize the schedule and timing of the two drugs. Furthermore, translational research is also recommended to better characterize the potential immune activation properties and the synergistic activity of SSA and to verify the predictive value of SRs to response to this therapeutic combination.
Data Availability Statement
All datasets generated for this study are included in the article/supplementary material.
Ethics Statement
Written informed consent was obtained from the patient for the publication of this case report.
Author Contributions
All authors listed have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Heath M, Jaimes N, Lemos B, Mostaghimi A, Wang LC, Peñas PF, et al. Clinical characteristics of Merkel cell carcinoma at diagnosis in 195 patients: the AEIOU features. J Am Acad Dermatol. (2008) 58:375–81. doi: 10.1016/j.jaad.2007.11.020
2. Howard RA, Dores GM, Curtis RE, Anderson WF, Travis LB. Merkel cell carcinoma and multiple primary cancers. Cancer Epidemiol Biomarkers Prev. (2006) 15:1545–9. doi: 10.1158/1055-9965.EPI-05-0895
3. Wong SQ, Waldeck K, Vergara IA, Schröder J, Madore J, Wilmott JS, et al. UV-associated mutations underlie the etiology of MCV-negative Merkel cell carcinomas. Cancer Res. (2015) 75:5228–34. doi: 10.1158/0008-5472.CAN-15-1877
4. Emge DA, Cardones AR. Updates on Merkel cell carcinoma. Dermatol Clin. (2019) 37:489–503. doi: 10.1016/j.det.2019.06.002
5. Hasan S, Liu L, Triplet J, Li Z, Mansur D. The role of postoperative radiation and chemoradiation in merkel cell carcinoma: a systematic review of the literature. Front Oncol. (2013) 3:276. doi: 10.3389/fonc.2013.00276
6. Tello TL, Coggshall K, Yom SS, Yu SS. Merkel cell carcinoma: an update and review: current and future therapy. J Am Acad Dermatol. (2018) 78:445–54. doi: 10.1016/j.jaad.2017.12.004
7. Nghiem P, Kaufman HL, Bharmal M, Mahnke L, Phatak H, Becker JC. Systematic literature review of efficacy, safety and tolerability outcomes of chemotherapy regimens in patients with metastatic Merkel cell carcinoma. Future Oncol. (2017) 13:1263–79. doi: 10.2217/fon-2017-0072
8. Kaufman HL, Russell J, Hamid O, Bhatia S, Terheyden P, D'Angelo SP, et al. Avelumab in patients with chemotherapy-refractory metastatic Merkel cell carcinoma: a multicentre, single-group, open-label, phase 2 trial. Lancet Oncol. (2016) 17:1374–85. doi: 10.1016/S1470-2045(16)30364-3
9. Nghiem P, Bhatia S, Lipson EJ, Sharfman WH, Kudchadkar RR, Brohl AS, et al. Durable tumor regression and overall survival in patients with advanced Merkel Cell Carcinoma receiving pembrolizumab as First-Line Therapy. J Clin Oncol. (2019) 37:693–702. doi: 10.1200/JCO.18.01896
10. Topalian SL, Bhatia S, Kudchadkar RR. Nivolumab as neoadjuvant therapy in patients with resectable Merkel cell carcinoma in CheckMate 358 [Abstract]. J Clin Oncol. (2018) 36:9505. doi: 10.1200/JCO.2018.36.15_suppl.9505
11. Samimi M. Immune checkpoint inhibitors and beyond: an overview of immune-based therapies in Merkel cell carcinoma. Am J Clin Dermat. (2019) 20:(3):391–407. doi: 10.1007/s40257-019-00427-9
12. Gardair C, Samimi M, Touzé A, Coursaget P, Lorette G, Caille A, et al. Somatostatin receptors 2A and 5 are expressed in Merkel Cell Carcinoma with no association with disease severity. Neuroendocrinology. (2015) 101:223–35. doi: 10.1159/000381062
13. Rinke A, Wittenberg M, Schade-Brittinger C, Aminossadati B, Ronicke E, Gress TM, et al. Placebo-controlled, double-blind, prospective, randomized study on the effect of octreotide LAR in the control of tumor growth in patients with metastatic neuroendocrine midgut tumors (PROMID): results of long-term survival. Neuroendocrinology. (2017) 104:26–32. doi: 10.1159/000443612
14. Slovacek L. Merckel cell carcinoma of the skin treated with somatostatin analogue and mTOR inhibitor exhausted after primary surgery, adjuvant radiotherapy and palliative chemotherapy. Bratisl Lek Listy. (2014) 115:663–5. doi: 10.4149/BLL_2014_128
15. Lamberts SW, Van der Lely AJ, de Herder WW, Hofland LJ. Octreotide. NEJM. (1996) 334:246–54. doi: 10.1056/NEJM199601253340408
16. Culler MD, Oberg K, Arnold R, Krenning EP, Sevilla I, Díaz JA. Somatostatin analogs for the treatment of neuroendocrine tumors. Cancer Metastasis Rev. (2011) 30(Suppl 1):9–17. doi: 10.1007/s10555-011-9293-0
17. Hofland LJ, van Koetsveld PM, Wouters N, Waaijers M, Reubi JC, Lamberts SW. Dissociation of antiproliferative and antihormonal effects of the somatostatin analog octreotide on 7315b pituitary tumor cells. Endocrinology. (1992) 131:571–7. doi: 10.1210/endo.131.2.1322274
18. Wang X, Teng F, Kong L, Yu J. PD-L1 expression in human cancers and its association with clinical outcomes. Onco Targets Ther. (2016) 9:5023–39. doi: 10.2147/OTT.S105862
Keywords: immunothearpy, somatostatin analog, Merkel cell carcinoma (MCC), Merkel carcinoma, somatostatin—receptor
Citation: Guida M, D'Alò A, Mangia A, Di Pinto F, Sonnessa M, Albano A, Sciacovelli A, Asabella AN and Fucci L (2020) Somatostatin Receptors in Merkel-Cell Carcinoma: A Therapeutic Opportunity Using Somatostatin Analog Alone or in Association With Checkpoint Inhibitors Immunotherapy. A Case Report. Front. Oncol. 10:1073. doi: 10.3389/fonc.2020.01073
Received: 18 October 2019; Accepted: 28 May 2020;
Published: 07 July 2020.
Edited by:
Nathalie Bonnefoy, Institut de Recherche en Cancérologie de Montpellier (IRCM), INSERM U1194, FranceReviewed by:
Bipulendu Jena, Independent Researcher, San Diego, United StatesMassimo Milione, Istituto Nazionale dei Tumori (IRCCS), Italy
Copyright © 2020 Guida, D'Alò, Mangia, Di Pinto, Sonnessa, Albano, Sciacovelli, Asabella and Fucci. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Michele Guida, bWljZ3VpZGE1N0BnbWFpbC5jb20=