 Marton König1,2*
Marton König1,2* Terje Osnes2,3*Øyvind Bruland2,4Kirsten Sundby Hall4Åse Bratland4
Terje Osnes2,3*Øyvind Bruland2,4Kirsten Sundby Hall4Åse Bratland4 Torstein R. Meling5,6
Torstein R. Meling5,6- 1Department of Neurosurgery, Oslo University Hospital, Oslo, Norway
- 2Faculty of Medicine, Institute of Clinical Medicine, University of Oslo, Oslo, Norway
- 3Department of Otorhinolaryngology, Head and Neck Surgery, Oslo University Hospital, Oslo, Norway
- 4Department of Oncology, Oslo University Hospital, Oslo, Norway
- 5Service de Neurochirurgie, Département des Neurosciences Cliniques, Hôpitaux Universitaires de Genève, Geneva, Switzerland
- 6Faculty of Medicine, University of Geneva, Geneva, Switzerland
Background: Tumors originating from the craniofacial region usually present in a locally advanced stage with frequent involvement of adjacent sites and have a strong tendency for local recurrence in the absence of adjuvant therapy, even when the original surgical resection was presumed to be radical. In the past decades, several advances in the radiological diagnosis and treatment of craniofacial malignancies have been introduced. There are, however, no randomized trials that define the optimal multimodal treatment of these tumors because of their rarity as well as heterogeneity in both histology and site of origin. The aim of this study was to conduct a critical review of the role of adjuvant therapy in the treatment of craniofacial malignancy.
Method: We conducted a critical review of the past and contemporary literature available, focusing on adjuvant oncological treatments of the most common craniofacial malignancies.
Results: Preoperative radiotherapy can have a documented role in the treatment of olfactory neuroblastoma and soft tissue sarcoma, while preoperative chemotherapy can be advocated in the treatment of sinonasal undifferentiated carcinoma, neuroendocrine carcinoma, olfactory neuroblastoma, and craniofacial sarcoma (both soft-tissue and high-grade osteosarcoma). Postoperative radiotherapy has a well-established role in the treatment of most craniofacial malignancies. The role of postoperative chemotherapy is unclear in most histologies, but is commonly used during the treatment of well-selected cases of paranasal sinus carcinoma, olfactory neuroblastoma, mucosal melanoma, soft tissue sarcoma and high-grade craniofacial osteosarcoma.
Discussion: Alongside developments in surgery, there have also been improvements in diagnostics, radiotherapy, and chemotherapy. Implementation of novel radiation techniques allows delivery of higher radiation doses while minimizing irradiation-related morbidity. Better understanding of tumor biology allows the construction of more complex treatment strategies, incorporating adjuvant chemotherapy either pre- or postoperatively. In the era of personalized targeted therapy, rapid strides are being made to identify specific tumor-targets for use of novel biologic agents, with the potential to change current management paradigms.
Introduction
The craniofacial region consists of several complex anatomic areas, closely related to the skull base, which pose surgical challenges for neurosurgeons and otorhinolaryngologists alike. Tumors originating from this region usually present in a locally advanced stage at diagnosis due to innocuous presenting symptoms and with frequent involvement of adjacent sites. In addition, there is a strong tendency for local recurrence in the absence of adjuvant therapy, even when the original surgical resection was presumed to be radical.
In the past decades, several advances in the radiological diagnosis and treatment of craniofacial malignancies have been introduced. Surgery in these locations may have dramatic functional and life-threatening consequences that sometimes prohibit radical surgical resections. However, novel surgical procedures and adjuvant modalities have made treatment feasible for malignancies previously considered impossible (1). There are no randomized trials that define the optimal multimodal treatment of malignancies of the craniofacial region because of the rarity of these tumors as well as their heterogeneity in both histology and site of origin.
This study aims to provide a critical review of the role of adjuvant therapy in the treatment of craniofacial malignancy.
Craniofacial Malignancies
The term “craniofacial” refers to the parts of the head enclosing the brain and the face from the upper part of the maxilla, largely corresponding to the suprastructure. This anatomical region is affected by a variety of tumors with clinical, etiological, pathological, and genetic features distinct from other tumors in the head and neck. The skull base forms the floor of the cranial cavity and separates the brain from other facial structures. It can be subdivided into three regions: the anterior, middle, and posterior cranial fossae. The most important anatomic structure above the sinonasal region is the anterior skull base. This part of the skull base is aberrant to other regions of the cranial skeleton as it displays a unique configuration of an osseous cranial vault with depressions, ridges, and septa. The anterior skull base stretches between the posterior wall of the frontal sinus anteriorly, to the roof of the sphenoid sinus marked by the anterior clinoid processes and the planum sphenoidale, posteriorly. The lateral boundaries are formed by the frontal bone. The anatomical connection between the midface and neurocranium is formed by the maxilla, the nasoethmoidal complex, the palatal and vomerine bone, and the pterygoid process of the sphenoid. The jaw is constituted by two main parts: the maxilla (upper part) and the mandibula (lower part).
Although these tumors may have similar anatomical locations, they can have considerably different characteristics and clinical behavior. In addition, there is no universally accepted grading and staging system available for these tumors.
Malignancies in this region are rare and encompass a variety of cancers arising from different sites. While emphasizing their rarity, the most common and representative of these malignancies are sinonasal carcinoma, olfactory neuroblastoma, mucosal melanoma, soft-tissue sarcoma, malignant meningioma and malignant tumors of the bone and cartilage, such as osteosarcoma, chondrosarcoma, and chordoma.
Adjuvant Therapies
Adjuvant therapies might be indicated when their efficacy—alone or in combination—is greater than their cumulative toxicity, depending on both patient-related and treatment-related factors (Table 1). They are usually administered with the intent of improving loco-regional control (i.e., enhancing the effect of surgery) with an impact on overall survival. Most commonly, these therapies include radiotherapy and/or chemotherapy administered pre and/or postoperatively (neoadjuvant and adjuvant therapy, respectively). In addition, novel therapies are currently being investigated, including agents selectively targeting extra- and intracellular signaling pathways, i.e., immune, hormone- and targeted therapies. At present, however, these therapies are mostly limited to therapy for overt metastatic disease (i.e., not as an adjuvant therapy), without primary surgical treatment.
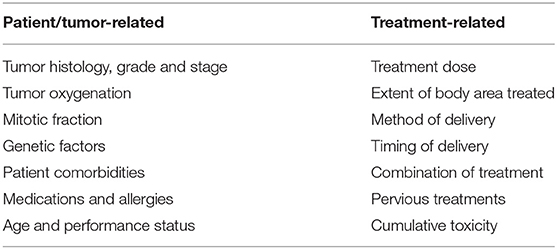
Table 1. Factors influencing the efficacy of adjuvant therapies.
Adjuvant therapies can be administered as a local or systemic treatment against the tumor (primary or recurrent), the resection site, local or regional lymph nodes, or to combat assumed distant subclinical/micrometastases.
Radiotherapy is used to achieve disease control at the tumor or lymph node site, and can be delivered using either using photons (X-rays) or heavy particles (proton beams or carbon ions). Fractionation is a commonly used process during the treatment of craniofacial malignancies, allowing maximal tumor cell death and minimal damage of nearby organs at risk (e.g., cranial nerves, eyes, brain).
When used as an adjuvant treatment, chemotherapy can be given as a radiosensitizer (i.e., rendering tumor cells more sensitive to radiation therapy by counteracting the radio-protective effect of tumor hypoxia). The two most commonly used agents are the cytotoxic agent cisplatin and the hypoxic modifier nimorazole.
However, chemotherapy can also be given as induction therapy or to minimize the subsequent risk of developing distant metastasis. For craniofacial malignancies, chemotherapy is usually administered as a part of a standardized regimen, and often as part of study protocols. The dosage is challenging; too low a dosage might be ineffective against the tumor, whereas too high dosage can lead to excessive—and sometimes intolerable—toxicity. All chemotherapy regimens require that the recipient is actually capable of undergoing treatment.
Targeted therapy interferes with specific molecules needed for carcinogenesis and tumor growth by targeting and blocking extracellular signals, rather than by blocking intracellular signals and interfering with all rapidly dividing cells (as traditional chemotherapy does) (2). A variety of molecular targets may be therapeutically relevant in some malignancies of the craniofacial region. In addition, identification of specific tumor markers may provide prognostic information that can be used to guide decision making and the selection of additional therapy. In some cases, participation in clinical trials that investigate immunotherapy and other novel approaches may be considered for patients with residual, recurrent, or metastatic disease (3–12).
Toxicity in Oncological Treatment
Toxicity is influenced by patient-, treatment-, tumor- and physician-related factors (Table 2). Toxicity can also be treatment specific (Table 3). Radiation therapy may lead to several local and site-specific complications in the craniofacial region affecting the skin of the head, the eyes, and the brain. Such complications include epithelial surface damage, swelling, fibrosis, dryness, and cognitive decline. Chemotherapy, on the other hand, may lead to systemic complications such as immunosuppression, myelosuppression, gastrointestinal distress, organ damage, and fatigue. Both radiation therapy and chemotherapy may cause nausea and vomiting, hair loss, ototoxicity and neuropathy. In addition, secondary neoplasm is a possible long-term complication of both modalities. Toxicities might be cumulative through life, and the administration of adequate doses of adjuvant therapies might not be possible for the treatment of a secondary neoplasm, or—in the worst case—the therapy might not be available at all.
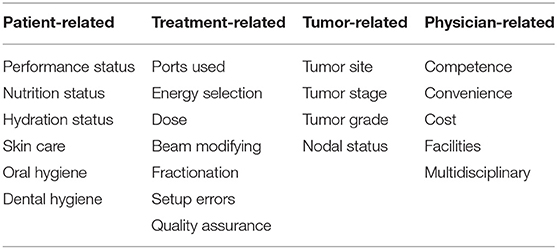
Table 2. Factors influencing the toxicity of adjuvant therapies.
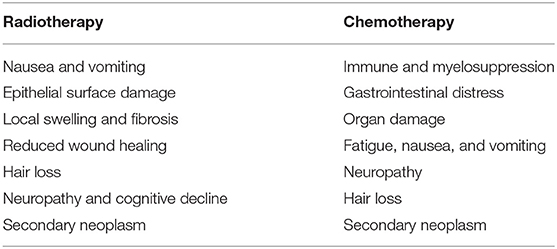
Table 3. Treatment-specific toxicities.
Timing of Adjuvant Therapies
Adjuvant therapy administered preoperatively (neoadjuvant) may shrink the primary tumor at the same time as instituting a treatment to avoid lymph node and/or visceral micrometastases developing into over metastases. Tumors with a low mitotic fraction experience a weaker response to radiation; in such cases, tumor control is often defined as lack of growth (and/or reduced cell density) rather than diminished size (13). In addition, preoperative therapy makes response-evaluation of the primary tumor feasible prior to surgery (i.e., induction chemotherapy). It is also advantageous that the blood supply to the tumor remains, i.e., not altered by surgery. However, neoadjuvant therapy may change both tumor and recipient characteristics, leading to difficulties regarding surgical treatment (Table 4).
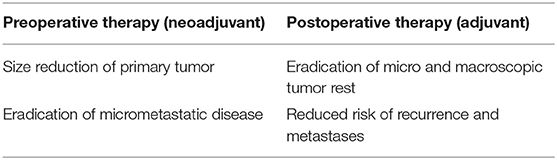
Table 4. Potential benefits of adjuvant therapies pre and postoperatively.
Postoperative adjuvant treatment has the potential to eradicate micro- or macroscopic tumor cells to improve survival, and to reduce the risk of both recurrence and metastases. In addition, features not available prior to surgery, such as complete histological evaluation, resection grade, and postoperative clinical status help further individualization of treatment, potentially increasing its efficacy and long-term survival for the patient (Table 4).
The Role of Adjuvant Therapies
Defining the role of adjuvant therapies for craniofacial malignancies is challenging. The rarity and varied pathology of lesions in this anatomical region make it difficult to accrue large series of patients with uniform pathologies, and to date there are no randomized clinical trials to guide the treatment of patients with these malignancies. With only a few multi-institutional studies published, most reports in the literature are single-center series with limited numbers of patients and often short follow-up times, making results difficult to interpret and compare. In addition, treatment outcomes over long time-periods may be biased by medical and surgical developments. Selected publications providing relevant outcome measures are illustrated in Table 5.
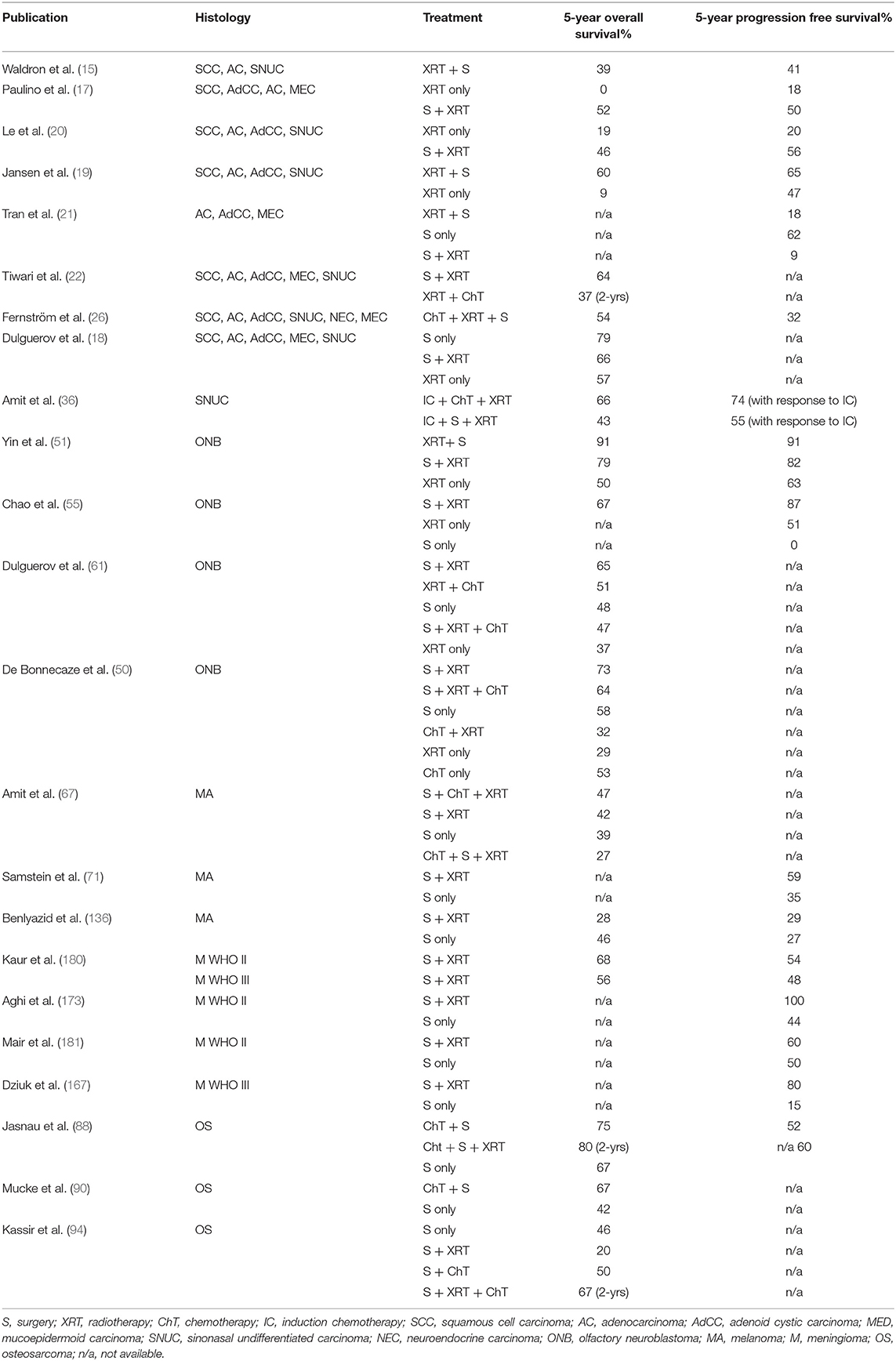
Table 5. Selected publications reporting outcome measures after multimodal treatment of craniofacial malignancies.
Preoperative Therapy
Paranasal Sinus Carcinoma
The role of preoperative radiotherapy is generally limited in patients with squamous cell carcinoma and adenocarcinoma of the paranasal sinuses as primary surgery provides a higher probability of radicality, lower complication rates, and also offers a precise histology with subsequent adjustment of postoperative radiation (14–17). Survival and local control in patients with advanced loco-regional tumors remain modest, with a meta-analysis showing an average 5-year survival of 51% (18). Radiation therapy alone or prior to salvage surgery should only be used when surgical resection is not feasible or is associated with unacceptable sequelae. Survival in such patients managed with primary radiation therapy with or without salvage surgery remains dismal (9–39%) (15, 17, 19, 20). If preoperative radiotherapy is used, a response-evaluation should be undertaken after 6–10 weeks to consider surgical resection of the tumor (14, 15, 17, 19–22).
The need to improve local control, increase survival and preserve organ function has prompted some centers to explore the addition of chemotherapy to standard treatment (23–26). Preoperative or induction chemotherapy can help to achieve operability in high-stage tumors, and can make radiation possible with less toxicity (23, 26, 27). The literature reports on a wide range of outcomes, and there are no definitive conclusions (28–30). Preoperative chemotherapy is usually not advised. There are concerns regarding possible disease progression during the treatment, and acquired cumulative toxicity leading patients being medically unfit for surgery (27). It can, however be considered in carefully selected cases where the tumor burden is so heavy that surgical resection or radiation is not possible without significant toxicity (27–29).
Sinonasal undifferentiated carcinoma and single-cell neuroendocrine carcinoma pose a unique therapeutic challenge to clinicians because of their aggressive biologic behavior, with a propensity (40–50%) for early invasion of vital structures such as the orbit, skull base, and brain, as well as a high risk of distant metastasis (20–30%) (31–35). In addition, these tumors are more chemo sensitive than other carcinomas in the same anatomical location (36, 37). Studies have documented the effect of platinum-based chemotherapy in these tumors, and intensive multimodal therapy is usually indicated, as oncological outcomes after open surgery remain poor (27, 36, 38, 39).
Patients with NUT-midline carcinoma—demonstrating loss of the ubiquitously expressed protein Integrase Interactor 1 (INI1; SMARCB1) —tend to present with large and locally advanced tumors; indeed, based on the previously reported series, most INI1-deficient sinonasal carcinomas are staged as T4 at the time of diagnosis. Experience suggests that these tumors respond well to neoadjuvant chemo-radiation (e.g., using a platinum based alkylating-like agent followed by radiation therapy) (40–45). Future treatments with agents that target the epigenetic machinery such as inhibitors against Enhancer of Zeste homolog 2 (EZH2) or histone deactylase may prove even more effective (46, 47).
Olfactory Neuroblastoma
The benefit of radical surgical resection in terms of survival is well–documented (27, 48–50), however, the role of preoperative radiotherapy is unclear. According to Yin et al. (51) preoperative radiation therapy can provide a valuable complement to surgery. Experience from University of Virginia shows that patients who responded to preoperative adjuvant therapy (radiotherapy for low-stage tumor and chemotherapy plus radiotherapy for high-stage tumors, respectively), had significantly lower rates of disease-related mortality (52, 53). Although there is no clear evidence supporting the administration of preoperative adjuvant therapy for all patients, preoperative platinum-based chemotherapy can be advocated for patients with locally advanced disease (e.g., with intracranial and/or orbital invasion) (54–65).
While radical surgery followed by postoperative radiation is considered the standard of care in adults, a similar approach in children can lead to significant long-term morbidity. Preoperative chemotherapy based multimodal approach should be considered in children with advanced stage disease, as pediatric olfactory neuroblastoma is considered a chemosensitive disease. Radiation therapy is effective for local control but lower doses should be considered in children (66).
Mucosal Melanoma
Preoperative radio-chemotherapy is generally not advocated for mucosal melanoma. However, radiotherapy may have a role when surgery is not appropriate or feasible (i.e., with palliative intent) (67–72).
Soft-Tissue Sarcoma
Preoperative radiotherapy may allow some patients with soft-tissue sarcoma to undergo potentially less mutilating surgery, and can also contribute to a higher rate of local control in groups of patients with a dismal prognosis. Preoperative treatment may also permit lower radiation doses and smaller target volumes than postoperative radiotherapy (73–76).
Preoperative chemotherapy is usually recommended for most patients with rhabdomyosarcoma, whereas its role in the management of other histological soft-tissue sarcoma subtypes is unclear at present (74–80).
Atypical and Malignant Meningioma
The use of radiotherapy or chemotherapy as a primary therapy with or without surgery is generally limited to patients medically unsuited for surgery or to those who have unresectable disease (81).
Malignant Tumors of Bone and Cartilage
Although osteosarcoma is generally resistant to radiotherapy, proton-beam therapy may be useful in the treatment of chondrosarcomas and osteosarcomas that involve the skull base (82, 83). It can be particularly difficult to deliver sufficient radiation doses in cases of chondrosarcoma and chordoma due to nearby organs being at risk. Preoperative radiation therapy in these cases is generally not utilized (84–87).
Modern treatment regimens for classic osteosarcoma include preoperative chemotherapy to eradicate micrometastatic disease. Although its benefit in craniofacial osteosarcoma (CFOS) is controversial, preoperative chemotherapy has been associated with improved survival in patients with high-grade CFOS (88–97). Preoperative chemotherapy is not advocated in cases of chondrosarcoma and chordoma as these tumors are resistant (84, 86, 87).
Postoperative Therapy
Paranasal Sinus Carcinoma
Achieving radical resection in this anatomical location is challenging, and paranasal sinus carcinomas have a high tendency for local recurrence in the absence of postoperative radiotherapy (98). In general, adenocarcinoma (salivary gland type) is less sensitive to radiation therapy than squamous cell carcinoma. Salvage surgery may be warranted in recurrent cases, even when only close resection margins may be achieved. Postoperative radiotherapy is generally advised after non-radical surgery, or when radicality is questionable (14, 99–102). Adjuvant radiotherapy is widely used for stage T3 and T4 tumors, and has been effective in decreasing the incidence of local recurrence. However, there are no randomized trials or prospective comparisons, and the data in retrospective analyses are often based on older techniques (103–108). Commonly used conformal techniques include three-dimensional conformal radiotherapy (3D-CRT) and intensity-modulated radiotherapy (IMRT). Charged particle therapy may offer additional advantages for delivering maximal tumor doses while minimizing radiation to the retina and brain (104–106).
The role of postoperative radiotherapy in cases of stage T2 tumors is unclear, while some studies show no benefit, others show higher recurrence rates in the absence of radiotherapy, especially in cases of high-risk tumors, such as adenoid cystic carcinoma and undifferentiated carcinoma (108–111). In cases of squamous cell carcinoma with macroscopic or microscopic tumors after surgical treatment, concomitant hypoxic modification with the radiosensitizer nimorazol should be used (112).
Postoperative chemotherapy has been incorporated as a component of the multimodal therapy of paranasal sinus carcinoma in a variety of ways. Concomitant platinum-based chemotherapy (cisplatin and 5-FU) seems to have a positive effect on local control and survival and may have an additional benefit in cases of non-radical surgery, advanced-stage disease, and extracapsular tumor extension (24, 27–29, 108, 113–118).
The prognosis of patients with recurrent or metastatic head and neck squamous cell cancer is generally poor. Carefully selected patients with a good performance status and locally recurrent disease may benefit from salvage surgery and/or re-irradiation (119, 120).
Systemic therapy is indicated for most patients with metastatic or advanced recurrent squamous cell carcinoma of the head and neck. The choice of systemic regimen—preferably administered as a part of a study protocol—is influenced by multiple clinical factors, including patient comorbidities, performance status, previous therapy, and pathologic features (i.e., programmed death-ligand 1 [PD-L1] expression status). Treatment options include immunotherapy with PD-L1 checkpoint inhibitors (e.g., pembrolizumab and nivolumab), conventional cytotoxic chemotherapy (e.g., cisplatin and carboplatin) and molecularly targeted agents (e.g., epidermal growth factor receptor [EGFR] inhibitors cetuximab and panatimumab) (6–8, 121–130).
Olfactory Neuroblastoma
Surgical resection followed by radiation therapy is the most widely used approach in cases of olfactory neuroblastoma. The results with this approach are illustrated by Dulguerov et al. who conducted a literature review and meta-analysis that included 390 patients from 26 studies published between 1990 and 2000 (61). For the 169 patients treated with a combination of surgery and radiation therapy, the reported 5-year survival rate was 65%. The reported 5-year survival rates for the 87 patients treated with surgery alone and the 49 patients treated with radiation alone were 48 and 37%, respectively. A similar added benefit of radiotherapy over surgery alone was shown for high-grade tumors in a Surveillance, Epidemiology, and End Results (SEER) study of 281 patients treated from 1973 to 2010 (65).
Several studies have documented that even patients with locally invasive tumors can achieve favorable long-term survival when surgical resection is followed by radiation (48, 54, 58–64, 131). The use of a combined-modality approach is particularly important for patients in whom disease extends beyond the paranasal sinuses or in whom surgical resection margins are positive (54, 59, 62).
The role of postoperative chemotherapy for olfactory neuroblastoma is unclear. Although several studies have shown improved results, the reason for these results (i.e., whether it is surgery, radiation, or chemotherapy) is unclear (37, 50, 53, 132–135). In general, adjuvant chemotherapy with cisplatin and etoposid is advocated in all cases of sinonasal cancer with small cell histology (27, 50).
The rarity of olfactory neuroblastoma, combined with the favorable prognosis following aggressive local and regional therapy, has resulted in only very limited experience for patients with disseminated disease. Chemotherapy appears to have activity in some patients (particularly cisplatin and etoposide), and newer molecularly targeted approaches (e.g., using sunitinib or by activating the sonic hedgehog pathway), may become an option as the biology of these tumors is better understood (10, 11).
Mucosal Melanoma
Local recurrence occurs in 29–79% of cases with mucosal melanoma, despite aggressive surgery. Several series have reported an improvement in loco-regional control with postoperative radiotherapy; however, there is no verified impact on long-term survival and its role has not been established (68–72, 136–140).
There is only limited data available regarding the role and efficacy of postoperative chemotherapy in mucosal melanomas. A Phase II randomized trial of interferon vs. chemotherapy in Chinese patients with resected mucosal melanoma showed a superior effect of temozolamide and cisplatin, but these results require replication in a broader patient-population before postoperative chemotherapy can be considered a standard-of-care treatment for Western patients (141).
An understanding of the molecular pathogenesis of mucosal melanoma has provided important insights that are leading to the development of targeted therapies for specific subsets of patients with metastatic disease. Approximately 10% of mucosal melanomas harbor activating mutations in the BRAF gene and another 25% have somatic mutations or amplification of the tyrosine-protein kinase KIT (12, 142, 143). Several studies have reported durable tumor responses to KIT inhibition by imatinib, nilotimib, sorafenib, dasatinib, and sunitinib in patients with melanoma harboring KIT mutations (142, 144–148). In addition, checkpoint inhibitor immunotherapy (e.g., anti-CTLA4 and anti-PD-1 immunotherapy) has been shown to significantly prolong survival in some patients with cutaneous melanoma; however, additional investigation is necessary to clarify the role of these therapies in patients with mucosal melanoma (149, 150).
Soft-Tissue Sarcoma
The benefit of postoperative radiation therapy for most histologic subtypes of soft-tissue sarcoma of the craniofacial region is controversial. Experience from the literature argues in favor of radiotherapy in cases of large tumors, high-grade tumors, and low-grade tumors with positive or close (<1 mm) resection margins (78, 151–158). Although radiotherapy for adults is commonly delivered through external beam radiation, for children with small, critically located tumors in the head and neck, intracavitary or interstitial implants (brachytherapy) may be an option (154, 159).
The indication for postoperative chemotherapy in soft-tissue sarcoma has to be determined individually and is only established in certain histotypes and high-grade sarcomas (77–79).
Given the limited efficacy of conventional cytotoxic chemotherapy, soft-tissue sarcoma remains fertile ground for the field of drug development. Clinical trials in a number of areas have shown promise in metastatic soft-tissue sarcoma, either as single agents or in combination with chemotherapy (160, 161).
Atypical and Malignant Meningioma
Postoperative radiotherapy is advocated for all malignant meningiomas and subtotally resected atypical meningiomas of the craniofacial regions as complete surgical resection is generally difficult to achieve, and there is a high rate of both local recurrence and increased disease-specific mortality after non-radical surgery (81, 162–165). Data suggest that malignant meningiomas are associated with a recurrence rate 5 years after surgery of ~60–90% and a 5-year overall survival of 20–50% (164–169). Adjuvant radiotherapy appears to decrease the recurrence rate by approximately half and may increase 5-year survival to >50%. For patients who undergo incomplete resection or biopsy of an atypical meningioma, the rate of recurrence or progression ranges from 60 to 100% (170, 171). Adjuvant radiotherapy improves local control, aims to prevent further neurologic morbidity related to growth of the residual tumor, and may improve survival (172).
The role of adjuvant radiotherapy is unclear in atypical meningiomas with an apparent gross total resection. The potential benefits of radiotherapy are more closely balanced with its risks and side effects, and it is particularly important to assess individual patient preferences and tolerance for risk (162, 170, 173–179). Based on contemporary series, the reported recurrence rate after imaging-confirmed gross total resection in patients not treated with adjuvant radiotherapy is ~30–50% at a median of 5 years or less, with rates of failure trending higher with longer follow-up (173–175, 177). Most but not all observational studies suggest that adjuvant radiation therapy improves local control and progression-free survival after complete resection of an atypical meningioma (170–172, 177, 178, 180, 181). The impact of radiotherapy on overall survival is less clear, however, and most studies have included insufficient numbers of patients or length of follow-up to adequately assess this outcome. The potential benefits of radiation therapy should be weighed against the short- and long-term side effects and risks of this treatment method. Factors that increase the risk of side effects or delayed toxicities of radiation therapy include advanced age, low functional status, large treatment volume, and proximity of the radiation field to critical structures such as the optic pathways or pituitary gland.
The role of adjuvant postoperative chemotherapy for atypical and malignant meningiomas is unclear. Current guidelines of the National Comprehensive Cancer Network (NCCN) recommend three agents to treat patients with refractory and high-grade meningiomas: hydroxyurea, interferon-2B and sandostatin (long-acting release) (182, 183).
Malignant Tumors of Bone and Cartilage
Postoperative radiotherapy is generally not advocated after radical, en bloc excision of CFOS. After non-radical surgery, re-excision should be performed. Radiotherapy (together with chemotherapy) is normally used for patients who are not candidates for re-excision or where the surgical margins remain positive after this attempt (83, 89, 184–186). In contrast, postoperative radiotherapy is suggested for most patients with chondrosarcomas and chordomas as complete resection of the tumor is difficult and recurrent tumors are associated with poorer prognosis (84, 85). Proton-beam therapy may be particularly useful as photon therapy is associated with a high rate of local failure and carries a significant risk of brainstem and cranial nerve damage (187–189).
Modern treatment regimens for osteosarcomas at non-head and neck sites generally include systemic cisplatin-based chemotherapy to eradicate occult micrometastatic disease. While chemotherapy (given either postoperatively or preoperatively) improves the prognosis of extremity osteosarcoma dramatically, its benefit in osteosarcoma of the head and neck is controversial.
Postoperative combination chemotherapy has a clear role in the management of high-grade CFOS; however, prospective data to support a benefit from adjuvant chemotherapy in head and neck osteosarcomas are lacking. In uncontrolled case series, the use of adjuvant or neoadjuvant chemotherapy has been associated with improved survival in patients with head and neck osteosarcomas in some (88, 90–93) but not all series (89, 190). Two meta-analyses on this subject reported conflicting conclusions, possibly due to incomplete information on the influence of surgical margin status (94, 95).
Whether patients with low-grade osteosarcomas benefit from chemotherapy is unclear. Most low-grade jaw osteosarcomas may be adequately treated with surgery alone, as long as clear margins can be achieved (191). The decision whether to pursue chemotherapy for very small high-grade and very large low-grade tumors must be individualized and made on a case-by-case basis (88, 89, 91–93, 95).
Postoperative chemotherapy has no role in the treatment of chondrosarcomas and chordomas, and it is hoped that novel therapeutics like targeted therapy will benefit these patients (2, 86, 87, 192–195). The relative lack of efficacy of conventional chemotherapy and the discovery of novel signaling pathways in several histologic subtypes of chondrosarcoma have prompted interest in molecular-targeted therapies (e.g., imatinib, dasatinib, sirolimus), particularly for chemotherapy-refractory non-operable or metastatic tumors (196–198). A variety of molecular targets may be relevant therapeutically in chordoma, including platelet-derived growth factor receptor (PDGFR), epidermal growth factor receptor (EGFR), vascular endothelial growth factor receptor (VEGFR), mammalian target of rapamycin (mTOR), and the INI1 gene (2, 86, 87).
Management of the Neck in Sinonasal Cancer
Postoperative irradiation (or lymph node dissection) of the neck is advocated for all patients with cervical lymph node involvement, while elective prophylactic treatment (in node negative patients) is controversial, and the optimal management in these cases is uncertain (54, 61, 65, 103, 199, 200). Radiotherapy is usually not necessary if there is N1 disease without extranodal extension, and neck dissection has been completed (201–203).
Discussion
Alongside developments in surgery, there have also been improvements in diagnostics, radiotherapy, and chemotherapy. Implementation of routine 3D treatment planning and IMRT allows delivery of higher radiation doses to the tumor while minimizing morbidity caused by irradiation of normal structures. At the same time, a better understanding of tumor biology allows the construction of more complex treatment strategies that incorporate adjuvant chemotherapy either pre or postoperatively. In the era of personalized targeted therapy, rapid strides are being made to identify specific tumor targets for the use of novel biologic agents, with the potential to change current management paradigms.
Management decisions are complicated by the rarity of these entities and the resulting lack of consensus regarding the optimal treatment regimen. Most studies suffer from a small number of patients and inconsistent treatment strategies. Although there is agreement that multimodal therapy is needed, the optimal sequence and combination of treatment modalities are not known. Inclusion bias is common upon assessment on treatment outcomes, as patients with higher stage tumors are prone to be selected for combination therapy rather than surgery alone. In addition, reporting of survival function in the literature is not uniform, leading to difficulties with the comparison of results. In general, malignancies of the craniofacial region have a high tendency for local recurrence in the absence of adjuvant (postoperative) radiotherapy, even when the original resection was thought to be radical. Although there are no randomized trials, adjuvant radiotherapy is widely used and has been effective in decreasing the incidence of local recurrence (103). The effect of radiotherapy depends on tumor histology and is greatest in olfactory neuroblastoma, squamous cell carcinoma, and rhabdomyosarcoma, whereas the effect is less clear in adenocarcinoma and chondrosarcoma (204). Arguments for postoperative administration of radiotherapy (rather than preoperative) are as follows: a probably higher chance for local radicality; more precise evaluation of tumor volume and tumor margins; histology at primary surgery; and the possibility of more focused radiotherapy to reduce the danger of the dose affecting nearby organs at risk (205, 206). The use of radiotherapy alone or in combination with chemotherapy is generally limited to those who are medically unsuited for surgery or to patients with unresectable disease (207).
Advances in radiotherapy techniques have led to the development of highly conformal techniques that permit the delivery of therapeutic doses to the skull base while minimizing the dose to uninvolved vital structures (e.g., nerves, vessels, eyes). The most frequently used conformal techniques are 3D-CRT and IMRT (104, 208, 209). Charged particle irradiation (by proton beam or carbon ion) irradiation may offer additional advantages for delivering maximal tumor doses, while minimizing radiation to the retina and brain compared with photon-based therapy (105, 106, 210).
The role of chemotherapy in the treatment of craniofacial malignancies is unclear. Chemotherapy has been incorporated as a component of multimodality therapy with radiotherapy and/or surgery in a variety of ways; however, as there are no randomized trials, no definitive conclusions can be drawn about the impact of chemotherapy on outcomes.
A possible advantage of giving chemotherapy before loco-regional treatment (neoadjuvant) is more optimal drug delivery, permitting higher chemotherapy doses and dose intensities compared with chemotherapy given during or after local therapy. Possible disadvantages include a slow recovery from toxicity and, when the interplay between different modalities is less than optimal, delay of loco-regional treatment (still is the cornerstone of the intervention) may be fatally counterproductive (27).
Adjuvant chemoradiotherapy has been less studied. Craniofacial and sinonasal malignancies have generally not been included in trials evaluating the impact of chemotherapy as a radiosensitizer, and only limited experience has been gained from retrospective analyses (27).
This review shows that preoperative radiotherapy can have a documented role in the treatment of olfactory neuroblastoma and soft-tissue sarcoma, while preoperative chemotherapy can be advocated in the treatment of sinonasal undifferentiated carcinoma, neuroendocrine carcinoma, olfactory neuroblastoma, and craniofacial sarcoma (both soft-tissue and high-grade osteosarcoma). Postoperative radiotherapy has a well-established role in the treatment of most craniofacial malignancies, apart from mucosal melanoma. The role of postoperative chemotherapy is unclear in most histologies but is commonly used during the treatment of well-selected cases of paranasal sinus carcinoma, olfactory neuroblastoma, mucosal melanoma, soft-tissue sarcoma, and high-grade craniofacial osteosarcoma (Figure 1).
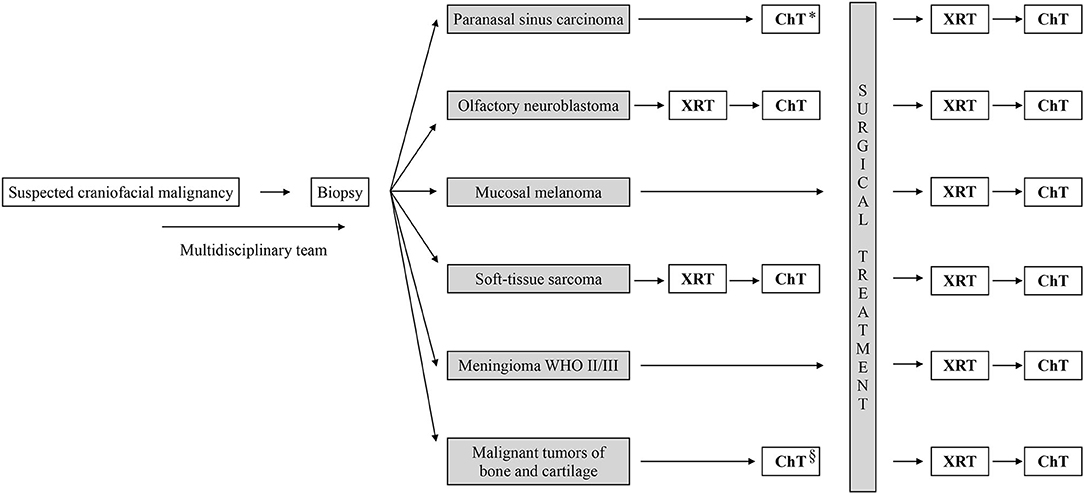
Figure 1. Summary work flow diagram for adjuvant treatment of craniofacial malignancies. *Sinonasal undifferentiated carcinoma, neuroendocrine carcinoma and NUT-midline carcinoma. §High-grade osteosarcoma. XRT, radiotherpy; ChT, chemotherpy.
Author Contributions
MK has conceived of the idea of the presented review, carried out a critical review of the literature, and wrote the manuscript. TM has supervised the review process. ØB, KS, ÅB, and TM have contributed to the final version of the manuscript with critical evaluation, suggestions, and expertise. All authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Konig M, Osnes T, Jebsen P, Meling TR. Craniofacial resection of malignant tumors of the anterior skull base: a case series and a systematic review. Acta Neurochir. (2018) 160:2339–48. doi: 10.1007/s00701-018-3716-4
2. Lebellec L, Chauffert B, Blay JY, Le Cesne A, Chevreau C, Bompas E, et al. Advanced chordoma treated by first-line molecular targeted therapies: outcomes and prognostic factors. A retrospective study of the French sarcoma group (GSF/GETO) and the association des neuro-oncologues d'expression francaise (ANOCEF). Eur J Cancer. (2017) 79:119–28. doi: 10.1016/j.ejca.2017.03.037
3. Gill CM, Fowkes M, Shrivastava RK. Emerging therapeutic targets in chordomas: a review of the literature in the genomic era. Neurosurgery. (2020) 86:E118–23. doi: 10.1093/neuros/nyaa008
4. Frezza AM, Botta L, Trama A, Dei Tos AP, Stacchiotti S. Chordoma: update on disease, epidemiology, biology and medical therapies. Curr Opin Oncol. (2019) 31:114–20. doi: 10.1097/CCO.0000000000000502
5. Zenonos GA, Fernandez-Miranda JC, Mukherjee D, Chang YF, Panayidou K, Snyderman CH, et al. Prospective validation of a molecular prognostication panel for clival chordoma. J Neurosurg. (2018). doi: 10.3171/2018.3.JNS172321. [Epub ahead of print].
6. Ferris RL, Blumenschein G Jr, Fayette J, Guigay J, Colevas AD, et al. Nivolumab for recurrent squamous-cell carcinoma of the head and neck. N Engl J Med. (2016) 375:1856–67. doi: 10.1056/NEJMoa1602252
7. Cohen EEW, Soulieres D, Le Tourneau C, Dinis J, Licitra L, Ahn MJ, et al. Pembrolizumab versus methotrexate, docetaxel, or cetuximab for recurrent or metastatic head-and-neck squamous cell carcinoma (KEYNOTE-040): a randomised, open-label, phase 3 study. Lancet. (2019) 393:156–67. doi: 10.1016/S0140-6736(18)31999-8
8. Mehra R, Seiwert TY, Gupta S, Weiss J, Gluck I, Eder JP, et al. Efficacy and safety of pembrolizumab in recurrent/metastatic head and neck squamous cell carcinoma: pooled analyses after long-term follow-up in KEYNOTE-012. Br J Cancer. (2018) 119:153–9. doi: 10.1038/s41416-018-0131-9
9. Wen PY, Quant E, Drappatz J, Beroukhim R, Norden AD. Medical therapies for meningiomas. J Neurooncol. (2010) 99:365–78. doi: 10.1007/s11060-010-0349-8
10. Preusser M, Hutterer M, Sohm M, Koperek O, Elandt K, Dieckmann K, et al. Disease stabilization of progressive olfactory neuroblastoma (esthesioneuroblastoma) under treatment with sunitinib mesylate. J Neurooncol. (2010) 97:305–8. doi: 10.1007/s11060-009-0027-x
11. Mao L, Xia YP, Zhou YN, Dai RL, Yang X, Wang YJ, et al. Activation of sonic hedgehog signaling pathway in olfactory neuroblastoma. Oncology. (2009) 77:231–43. doi: 10.1159/000236047
12. Carvajal RD, Antonescu CR, Wolchok JD, Chapman PB, Roman RA, Teitcher J, et al. KIT as a therapeutic target in metastatic melanoma. JAMA. (2011) 305:2327–34. doi: 10.1001/jama.2011.746
13. Debus J, Wuendrich M, Pirzkall A, Hoess A, Schlegel W, Zuna I, et al. High efficacy of fractionated stereotactic radiotherapy of large base-of-skull meningiomas: long-term results. J Clin Oncol. (2001) 19:3547–53. doi: 10.1200/JCO.2001.19.15.3547
14. Lund VJ, Clarke PM, Swift AC, McGarry GW, Kerawala C, Carnell D. Nose and paranasal sinus tumours: United Kingdom national multidisciplinary guidelines. J Laryngol Otol. (2016) 130:S111–8. doi: 10.1017/S0022215116000530
15. Waldron JN, O'Sullivan B, Warde P, Gullane P, Lui FF, Payne D, et al. Ethmoid sinus cancer: twenty-nine cases managed with primary radiation therapy. Int J Radiat Oncol Biol Phys. (1998) 41:361–9. doi: 10.1016/S0360-3016(98)00018-2
16. Waldron J, Witterick I. Paranasal sinus cancer: caveats and controversies. World J Surg. (2003) 27:849–55. doi: 10.1007/s00268-003-7111-8
17. Paulino AC, Marks JE, Bricker P, Melian E, Reddy SP, Emami B. Results of treatment of patients with maxillary sinus carcinoma. Cancer. (1998) 83:457–65. doi: 10.1002/(SICI)1097-0142(19980801)83:3<457::AID-CNCR14>3.0.CO;2-V
18. Dulguerov P, Jacobsen MS, Allal AS, Lehmann W, Calcaterra T. Nasal and paranasal sinus carcinoma: are we making progress? A series of 220 patients and a systematic review. Cancer. (2001) 92:3012–29. doi: 10.1002/1097-0142(20011215)92:12<3012::AID-CNCR10131>3.0.CO;2-E
19. Jansen EP, Keus RB, Hilgers FJ, Haas RL, Tan IB, Bartelink H. Does the combination of radiotherapy and debulking surgery favor survival in paranasal sinus carcinoma? Int J Radiat Oncol Biol Phys. (2000) 48:27–35. doi: 10.1016/S0360-3016(00)00594-0
20. Le QT, Fu KK, Kaplan M, Terris DJ, Fee WE, Goffinet DR. Treatment of maxillary sinus carcinoma: a comparison of the 1997 and (1977). Am joint committee cancer staging systems. Cancer. (1999) 86:1700–11. doi: 10.1002/(SICI)1097-0142(19991101)86:9<1700::AID-CNCR11>3.0.CO;2-4
21. Tran L, Sidrys J, Horton D, Sadeghi A, Parker RG. Malignant salivary gland tumors of the paranasal sinuses and nasal cavity. The UCLA experience. Am J Clin Oncol. (1989) 12:387–92. doi: 10.1097/00000421-198910000-00005
22. Tiwari R, Hardillo JA, Mehta D, Slotman B, Tobi H, Croonenburg E, et al. Squamous cell carcinoma of maxillary sinus. Head Neck. (2000) 22:164–9. doi: 10.1002/(SICI)1097-0347(200003)22:2<164::AID-HED8>3.0.CO;2-#
23. Hanna EY, Cardenas AD, DeMonte F, Roberts D, Kupferman M, Weber R, et al. Induction chemotherapy for advanced squamous cell carcinoma of the paranasal sinuses. Arch Otolaryngol Head Neck Surg. (2011) 137:78–81. doi: 10.1001/archoto.2010.231
24. Lee MM, Vokes EE, Rosen A, Witt ME, Weichselbaum RR, Haraf DJ. Multimodality therapy in advanced paranasal sinus carcinoma: superior long-term results. Cancer J Sci Am. (1999) 5:219–23.
25. McCary WS, Levine PA, Cantrell RW. Preservation of the eye in the treatment of sinonasal malignant neoplasms with orbital involvement. A confirmation of the original treatise. Arch Otolaryngol Head Neck Surg. (1996) 122:657–9. doi: 10.1001/archotol.1996.01890180063015
26. Fernström E, Nyman J, Hammerlid E, Holmberg E, Haugen-Cange H, Petruson K, et al. Results of preoperative chemoradiotherapy for patients with advanced cancer of the nasal cavity and paranasal sinuses. Acta Oto Laryngol. (2017) 137:1292–300. doi: 10.1080/00016489.2017.1357081
27. Bossi P, Saba NF, Vermorken JB, Strojan P, Pala L, de Bree R, et al. The role of systemic therapy in the management of sinonasal cancer: a critical review. Cancer Treat Rev. (2015) 41:836–43. doi: 10.1016/j.ctrv.2015.07.004
28. Pignon JP, le Maitre A, Maillard E, Bourhis J, Group M-NC. Meta-analysis of chemotherapy in head and neck cancer (MACH-NC): an update on 93 randomised trials and 17,346 patients. Radiother Oncol. (2009) 92:4–14. doi: 10.1016/j.radonc.2009.04.014
29. Blanchard P, Baujat B, Holostenco V, Bourredjem A, Baey C, Bourhis J, et al. Meta-analysis of chemotherapy in head and neck cancer (MACH-NC): a comprehensive analysis by tumour site. Radiother Oncol. (2011) 100:33–40. doi: 10.1016/j.radonc.2011.05.036
30. Dauzier E, Lacas B, Blanchard P, Le QT, Simon C, Wolf G, et al. Role of chemotherapy in 5000 patients with head and neck cancer treated by curative surgery: a subgroup analysis of the meta-analysis of chemotherapy in head and neck cancer. Oral Oncol. (2019) 95:106–14. doi: 10.1016/j.oraloncology.2019.06.001
31. Zielinski V, Laban S, Tribius S, Schafhausen P, Veldhoen S, Knecht R, et al. Management of sinonasal undifferentiated carcinoma with intracerebral invasion: clinical experience at a single institution and review of the literature. Ear Nose Throat J. (2016) 95:23–8.
32. Lopez F, Suarez V, Vivanco B, Suarez C, Llorente JL. Current management of sinonasal undifferentiated carcinoma. Rhinology. (2015) 53:212–20. doi: 10.4193/Rhin14.054
33. Chen AM, Daly ME, El-Sayed I, Garcia J, Lee NY, Bucci MK, et al. Patterns of failure after combined-modality approaches incorporating radiotherapy for sinonasal undifferentiated carcinoma of the head and neck. Int J Radiat Oncol Biol Phys. (2008) 70:338–43. doi: 10.1016/j.ijrobp.2007.06.057
34. Lin EM, Sparano A, Spalding A, Eisbruch A, Worden FP, Heth J, et al. Sinonasal undifferentiated carcinoma: a 13-year experience at a single institution. Skull Base. (2010) 20:61–7. doi: 10.1055/s-0029-1236165
35. Tanzler ED, Morris CG, Orlando CA, Werning JW, Mendenhall WM. Management of sinonasal undifferentiated carcinoma. Head Neck. (2008) 30:595–9. doi: 10.1002/hed.20748
36. Amit M, Abdelmeguid AS, Watcherporn T, Takahashi H, Tam S, Bell D, et al. Induction chemotherapy response as a guide for treatment optimization in sinonasal undifferentiated carcinoma. J Clin Oncol. (2019) 37:504–12. doi: 10.1200/JCO.18.00353
37. Fitzek MM, Thornton AF, Varvares M, Ancukiewicz M, McIntyre J, Adams J, et al. Neuroendocrine tumors of the sinonasal tract. Results of a prospective study incorporating chemotherapy, surgery, and combined proton-photon radiotherapy. Cancer. (2002) 94:2623–34. doi: 10.1002/cncr.10537
38. Ganly I, Patel SG, Singh B, Kraus DH, Bridger PG, Cantu G, et al. Craniofacial resection for malignant paranasal sinus tumors: report of an International collaborative study. Head Neck. (2005) 27:575–84. doi: 10.1002/hed.20165
39. Reiersen DA, Pahilan ME, Devaiah AK. Meta-analysis of treatment outcomes for sinonasal undifferentiated carcinoma. Otolaryngol Head Neck Surg. (2012) 147:7–14. doi: 10.1177/0194599812440932
40. Agaimy A, Hartmann A, Antonescu CR, Chiosea SI, El-Mofty SK, Geddert H, et al. SMARCB1 (INI-1)-deficient sinonasal carcinoma: a series of 39 cases expanding the morphologic and clinicopathologic spectrum of a recently described entity. Am J Surg Pathol. (2017) 41:458–71. doi: 10.1097/PAS.0000000000000797
41. Shah AA, Jain D, Ababneh E, Agaimy A, Hoschar AP, Griffith CC, et al. SMARCB1 (INI-1)-deficient adenocarcinoma of the sinonasal tract: a potentially under-recognized form of sinonasal adenocarcinoma with occasional yolk sac tumor-like features. Head Neck Pathol. (2020) 14:465–72. doi: 10.1007/s12105-019-01065-7
42. Allison DB, Bishop JA, Ali SZ. Cytopathologic characteristics of SMARCB1 (INI-1) deficient sinonasal carcinoma: a potential diagnostic pitfall. Diagn Cytopathol. (2016) 44:700–3. doi: 10.1002/dc.23503
43. Bishop JA, Antonescu CR, Westra WH. SMARCB1 (INI-1)-deficient carcinomas of the sinonasal tract. Am J Surg Pathol. (2014) 38:1282–9. doi: 10.1097/PAS.0000000000000285
44. Bell D, Hanna EY, Agaimy A, Weissferdt A. Reappraisal of sinonasal undifferentiated carcinoma: SMARCB1 (INI1)-deficient sinonasal carcinoma: a single-institution experience. Virchows Arch. (2015) 467:649–56. doi: 10.1007/s00428-015-1853-1
45. Wasserman JK, Dickson BC, Perez-Ordonez B, de Almeida JR, Irish JC, Weinreb I. INI1 (SMARCB1)-deficient sinonasal carcinoma: a clinicopathologic report of 2 cases. Head Neck Pathol. (2017) 11:256–61. doi: 10.1007/s12105-016-0752-3
46. Kuntz KW, Campbell JE, Keilhack H, Pollock RM, Knutson SK, Porter-Scott M, et al. The importance of being me: magic methyls, methyltransferase inhibitors, and the discovery of tazemetostat. J Med Chem. (2016) 59:1556–64. doi: 10.1021/acs.jmedchem.5b01501
47. Muscat A, Popovski D, Jayasekara WS, Rossello FJ, Ferguson M, Marini KD, et al. Low-dose histone deacetylase inhibitor treatment leads to tumor growth arrest and multi-lineage differentiation of malignant rhabdoid tumors. Clin Cancer Res. (2016) 22:3560–70. doi: 10.1158/1078-0432.CCR-15-2260
48. Konig M, Osnes T, Jebsen P, Evensen JF, Meling TR. Olfactory neuroblastoma: a single-center experience. Neurosurg Rev. (2017) 41:323–31. doi: 10.1007/s10143-017-0859-3
49. Castelnuovo P, Turri-Zanoni M, Battaglia P, Antognoni P, Bossi P, Locatelli D. Sinonasal malignancies of anterior skull base: histology-driven treatment strategies. Otolaryngol Clin North Am. (2016) 49:183–200. doi: 10.1016/j.otc.2015.09.012
50. De Bonnecaze G, Lepage B, Rimmer J, Al Hawat A, Vairel B, Serrano E, et al. Long-term carcinologic results of advanced esthesioneuroblastoma: a systematic review. Eur Arch Otorhinolaryngol. (2016) 273:21–6. doi: 10.1007/s00405-014-3320-z
51. Yin ZZ, Gao L, Luo JW, Yi JL, Huang XD, Qu Y, et al. Long-term outcomes of patients with esthesioneuroblastomas: a cohort from a single institution. Oral Oncol. (2016) 53:48–53. doi: 10.1016/j.oraloncology.2015.11.021
52. Polin RS, Sheehan JP, Chenelle AG, Munoz E, Larner J, Phillips CD, et al. The role of preoperative adjuvant treatment in the management of esthesioneuroblastoma: the university of virginia experience. Neurosurgery. (1998) 42:1029–37. doi: 10.1097/00006123-199805000-00045
53. Loy AH, Reibel JF, Read PW, Thomas CY, Newman SA, Jane JA, et al. Esthesioneuroblastoma: continued follow-up of a single institution's experience. Arch Otolaryngol Head Neck Surg. (2006) 132:134–8. doi: 10.1001/archotol.132.2.134
54. Ow TJ, Hanna EY, Roberts DB, Levine NB, El-Naggar AK, Rosenthal DI, et al. Optimization of long-term outcomes for patients with esthesioneuroblastoma. Head Neck. (2014) 36:524–30. doi: 10.1002/hed.23327
55. Chao KS, Kaplan C, Simpson JR, Haughey B, Spector GJ, Sessions DG, et al. Esthesioneuroblastoma: the impact of treatment modality. Head Neck. (2001) 23:749–57. doi: 10.1002/hed.1107
56. Kim DW, Jo YH, Kim JH, Wu HG, Rhee CS, Lee CH, et al. Neoadjuvant etoposide, ifosfamide, and cisplatin for the treatment of olfactory neuroblastoma. Cancer. (2004) 101:2257–60. doi: 10.1002/cncr.20648
57. El Kababri M, Habrand JL, Valteau-Couanet D, Gaspar N, Dufour C, Oberlin O. Esthesioneuroblastoma in children and adolescent: experience on 11 cases with literature review. J Pediatr Hematol Oncol. (2014) 36:91–5. doi: 10.1097/MPH.0000000000000095
58. Ward PD, Heth JA, Thompson BG, Marentette LJ. Esthesioneuroblastoma: results and outcomes of a single institution's experience. Skull Base. (2009) 19:133–40. doi: 10.1055/s-0028-1096195
59. Diaz EM Jr, Johnigan RH 3rd, Pero C, El-Naggar AK, Roberts DB, et al. Olfactory neuroblastoma: the 22-year experience at one comprehensive cancer center. Head Neck. (2005) 27:138–49. doi: 10.1002/hed.20127
60. Bachar G, Goldstein DP, Shah M, Tandon A, Ringash J, Pond G, et al. Esthesioneuroblastoma: the princess margaret hospital experience. Head Neck. (2008) 30:1607–14. doi: 10.1002/hed.20920
61. Dulguerov P, Allal AS, Calcaterra TC. Esthesioneuroblastoma: a meta-analysis and review. Lancet Oncol. (2001) 2:683–90. doi: 10.1016/S1470-2045(01)00558-7
62. Nichols AC, Chan AW, Curry WT, Barker FG, Deschler DG, Lin DT. Esthesioneuroblastoma: the massachusetts eye and ear infirmary and massachusetts general hospital experience with craniofacial resection, proton beam radiation, and chemotherapy. Skull Base. (2008) 18:327–37. doi: 10.1055/s-2008-1076098
63. Lund VJ, Howard D, Wei W, Spittle M. Olfactory neuroblastoma: past, present, and future? Laryngoscope. (2003) 113:502–7. doi: 10.1097/00005537-200303000-00020
64. Theilgaard SA, Buchwald C, Ingeholm P, Kornum Larsen S, Eriksen JG, Sand Hansen H. Esthesioneuroblastoma: a danish demographic study of 40 patients registered between 1978 and (2000). Acta Otolaryngol. (2003) 123:433–9. doi: 10.1080/00016480310001295
65. Tajudeen BA, Arshi A, Suh JD, St John M, Wang MB. Importance of tumor grade in esthesioneuroblastoma survival: a population-based analysis. JAMA Otolaryngol Head Neck Surg. (2014) 140:1124–9. doi: 10.1001/jamaoto.2014.2541
66. Venkatramani R, Pan H, Furman WL, Marron JM, Haduong J, Friedrich-Medina P, et al. Multimodality treatment of pediatric esthesioneuroblastoma. Pediatr Blood Cancer. (2016) 63:465–70. doi: 10.1002/pbc.25817
67. Amit M, Tam S, Abdelmeguid AS, Kupferman ME, Su SY, Raza SM, et al. Role of adjuvant treatment in sinonasal mucosal melanoma. J Neurol Surg B Skull Base. (2017) 78:512–8. doi: 10.1055/s-0037-1604350
68. Moreno MA, Roberts DB, Kupferman ME, DeMonte F, El-Naggar AK, Williams M, et al. Mucosal melanoma of the nose and paranasal sinuses, a contemporary experience from the M. D. Anderson cancer center. Cancer. (2010) 116:2215–23. doi: 10.1002/cncr.24976
69. Krengli M, Masini L, Kaanders JH, Maingon P, Oei SB, Zouhair A, et al. Radiotherapy in the treatment of mucosal melanoma of the upper aerodigestive tract: analysis of 74 cases. A rare cancer network study. Int J Radiat Oncol Biol Phys. (2006) 65:751–9. doi: 10.1016/j.ijrobp.2006.01.016
70. Bachar G, Loh KS, O'Sullivan B, Goldstein D, Wood S, Brown D, et al. Mucosal melanomas of the head and neck: experience of the princess margaret hospital. Head Neck. (2008) 30:1325–31. doi: 10.1002/hed.20878
71. Samstein RM, Carvajal RD, Postow MA, Callahan MK, Shoushtari AN, Patel SG, et al. Localized sinonasal mucosal melanoma: outcomes and associations with stage, radiotherapy, and positron emission tomography response. Head Neck. (2016) 38:1310–7. doi: 10.1002/hed.24435
72. Thompson LD, Wieneke JA, Miettinen M. Sinonasal tract and nasopharyngeal melanomas: a clinicopathologic study of 115 cases with a proposed staging system. Am J Surg Pathol. (2003) 27:594–611. doi: 10.1097/00000478-200305000-00004
73. O'Sullivan B, Gullane P, Irish J, Neligan P, Gentili F, Mahoney J, et al. Preoperative radiotherapy for adult head and neck soft tissue sarcoma: assessment of wound complication rates and cancer outcome in a prospective series. World J Surg. (2003) 27:875–83. doi: 10.1007/s00268-003-7115-4
74. Lahat G, Dhuka AR, Lahat S, Smith KD, Pollock RE, Hunt KK, et al. Outcome of locally recurrent and metastatic angiosarcoma. Ann Surg Oncol. (2009) 16:2502–9. doi: 10.1245/s10434-009-0569-3
75. Lahat G, Dhuka AR, Hallevi H, Xiao L, Zou C, Smith KD, et al. Angiosarcoma: clinical and molecular insights. Ann Surg. (2010) 251:1098–106. doi: 10.1097/SLA.0b013e3181dbb75a
76. DeMartelaere SL, Roberts D, Burgess MA, Morrison WH, Pisters PW, Sturgis EM, et al. Neoadjuvant chemotherapy-specific and overall treatment outcomes in patients with cutaneous angiosarcoma of the face with periorbital involvement. Head Neck. (2008) 30:639–46. doi: 10.1002/hed.20757
77. Raney RB, Anderson JR, Barr FG, Donaldson SS, Pappo AS, Qualman SJ, et al. Rhabdomyosarcoma and undifferentiated sarcoma in the first two decades of life: a selective review of intergroup rhabdomyosarcoma study group experience and rationale for intergroup rhabdomyosarcoma study V. J Pediatr Hematol Oncol. (2001) 23:215–20. doi: 10.1097/00043426-200105000-00008
78. Guadagnolo BA, Zagars GK, Araujo D, Ravi V, Shellenberger TD, Sturgis EM. Outcomes after definitive treatment for cutaneous angiosarcoma of the face and scalp. Head Neck. (2011) 33:661–7. doi: 10.1002/hed.21513
79. Young RJ, Brown NJ, Reed MW, Hughes D, Woll PJ. Angiosarcoma. Lancet Oncol. (2010) 11:983–91. doi: 10.1016/S1470-2045(10)70023-1
80. Meza JL, Anderson J, Pappo AS, Meyer WH, Children's Oncology G. Analysis of prognostic factors in patients with nonmetastatic rhabdomyosarcoma treated on intergroup rhabdomyosarcoma studies III and IV: the children's oncology group. J Clin Oncol. (2006) 24:3844–51. doi: 10.1200/JCO.2005.05.3801
81. Goldbrunner R, Minniti G, Preusser M, Jenkinson MD, Sallabanda K, Houdart E, et al. EANO guidelines for the diagnosis and treatment of meningiomas. Lancet Oncol. (2016) 17:e383–91. doi: 10.1016/S1470-2045(16)30321-7
82. Lee RJ, Arshi A, Schwartz HC, Christensen RE. Characteristics and prognostic factors of osteosarcoma of the jaws: a retrospective cohort study. JAMA Otolaryngol Head Neck Surg. (2015) 141:470–7. doi: 10.1001/jamaoto.2015.0340
83. DeLaney TF, Park L, Goldberg SI, Hug EB, Liebsch NJ, Munzenrider JE, et al. Radiotherapy for local control of osteosarcoma. Int J Radiat Oncol Biol Phys. (2005) 61:492–8. doi: 10.1016/j.ijrobp.2004.05.051
84. Stacchiotti S, Sommer J, Chordoma Global Consensus G. Building a global consensus approach to chordoma: a position paper from the medical and patient community. Lancet Oncol. (2015) 16:e71–83. doi: 10.1016/S1470-2045(14)71190-8
85. De Amorim Bernstein K, DeLaney T. Chordomas and chondrosarcomas-The role of radiation therapy. J Surg Oncol. (2016) 114:564–9. doi: 10.1002/jso.24368
86. Yamaguchi T, Imada H, Iida S, Szuhai K. Notochordal tumors: an update on molecular pathology with therapeutic implications. Surg Pathol Clin. (2017) 10:637–56. doi: 10.1016/j.path.2017.04.008
87. Colia V, Stacchiotti S. Medical treatment of advanced chordomas. Eur J Cancer. (2017) 83:220–8. doi: 10.1016/j.ejca.2017.06.038
88. Jasnau S, Meyer U, Potratz J, Jundt G, Kevric M, Joos UK, et al. Craniofacial osteosarcoma experience of the cooperative German-Austrian-Swiss osteosarcoma study group. Oral Oncol. (2008) 44:286–94. doi: 10.1016/j.oraloncology.2007.03.001
89. Laskar S, Basu A, Muckaden MA, D'Cruz A, Pai S, Jambhekar N, et al. Osteosarcoma of the head and neck region: lessons learned from a single-institution experience of 50 patients. Head Neck. (2008) 30:1020–6. doi: 10.1002/hed.20820
90. Mucke T, Mitchell DA, Tannapfel A, Wolff KD, Loeffelbein DJ, Kanatas A. Effect of neoadjuvant treatment in the management of osteosarcomas of the head and neck. J Cancer Res Clin Oncol. (2014) 140:127–31. doi: 10.1007/s00432-013-1550-x
91. Ferrari D, Codeca C, Battisti N, Broggio F, Crepaldi F, Violati M, et al. Multimodality treatment of osteosarcoma of the jaw: a single institution experience. Med Oncol. (2014) 31:171. doi: 10.1007/s12032-014-0171-9
92. Kammerer PW, Shabazfar N, Vorkhshori Makoie N, Moergel M, Al-Nawas B. Clinical, therapeutic and prognostic features of osteosarcoma of the jaws - experience of 36 cases. J Craniomaxillofac Surg. (2012) 40:541–8. doi: 10.1016/j.jcms.2011.10.001
93. Thiele OC, Freier K, Bacon C, Egerer G, Hofele CM. Interdisciplinary combined treatment of craniofacial osteosarcoma with neoadjuvant and adjuvant chemotherapy and excision of the tumour: a retrospective study. Br J Oral Maxillofac Surg. (2008) 46:533–6. doi: 10.1016/j.bjoms.2008.03.010
94. Kassir RR, Rassekh CH, Kinsella JB, Segas J, Carrau RL, Hokanson JA. Osteosarcoma of the head and neck: meta-analysis of nonrandomized studies. Laryngoscope. (1997) 107:56–61. doi: 10.1097/00005537-199701000-00013
95. Smeele LE, Kostense PJ, van der Waal I, Snow GB. Effect of chemotherapy on survival of craniofacial osteosarcoma: a systematic review of 201 patients. J Clin Oncol. (1997) 15:363–7. doi: 10.1200/JCO.1997.15.1.363
96. Konig M, Osnes TA, Lobmaier I, Bjerkehagen B, Bruland OS, Sundby Hall K, et al. Multimodal treatment of craniofacial osteosarcoma with high-grade histology. A single-center experience over 35 years. Neurosurg Rev. (2016) 40:449–60. doi: 10.1007/s10143-016-0802-z
97. Konig M, Mork J, Hall KS, Osnes T, Meling TR. Multimodal treatment of osteogenic sarcoma of the jaw. Skull Base. (2010) 20:207–12. doi: 10.1055/s-0029-1246221
98. Harbo G, Grau C, Bundgaard T, Overgaard M, Elbrond O, Sogaard H, et al. Cancer of the nasal cavity and paranasal sinuses. A clinico-pathological study of 277 patients. Acta Oncol. (1997) 36:45–50. doi: 10.3109/02841869709100731
99. Llorente JL, Lopez F, Suarez C, Hermsen MA. Sinonasal carcinoma: clinical, pathological, genetic and therapeutic advances. Nat Rev Clin Oncol. (2014) 11:460–72. doi: 10.1038/nrclinonc.2014.97
100. Wang K, Zanation AM, Chera BS. The role of radiation therapy in the management of sinonasal and ventral skull base malignancies. Otolaryngol Clin North Am. (2017) 50:419–32. doi: 10.1016/j.otc.2016.12.014
101. König M, Osnes T, Jebsen P, Meling T. Squamous cell carcinomas of the paranasal sinuses: a single-center experience. J Neurol Surg B Skull Base. (2020). doi: 10.1055/s-0039-1694967. [Epub ahead of print].
102. König M, Osnes T, Bratland A, Jebsen P, Meling T. Treatment of sinonasal adenocarcinoma: a population-based prospective cohort study. J Neurol Surg B Skull Base. (2020). doi: 10.1055/s-0039-1694050. [Epub ahead of print].
103. Robbins KT, Ferlito A, Silver CE, Takes RP, Strojan P, Snyderman CH, et al. Contemporary management of sinonasal cancer. Head Neck. (2011) 33:1352–65. doi: 10.1002/hed.21515
104. Brizel DM, Light K, Zhou SM, Marks LB. Conformal radiation therapy treatment planning reduces the dose to the optic structures for patients with tumors of the paranasal sinuses. Radiother Oncol. (1999) 51:215–8. doi: 10.1016/S0167-8140(99)00043-2
105. Patel SH, Wang Z, Wong WW, Murad MH, Buckey CR, Mohammed K, et al. Charged particle therapy versus photon therapy for paranasal sinus and nasal cavity malignant diseases: a systematic review and meta-analysis. Lancet Oncol. (2014) 15:1027–38. doi: 10.1016/S1470-2045(14)70268-2
106. Koto M, Demizu Y, Saitoh JI, Suefuji H, Tsuji H, Okimoto T, et al. Definitive carbon-ion radiation therapy for locally advanced sinonasal malignant tumors: subgroup analysis of a multicenter study by the Japan carbon-ion radiation oncology study group (J-CROS). Int J Radiat Oncol Biol Phys. (2018) 102:353–61. doi: 10.1016/j.ijrobp.2018.05.074
107. Lund VJ, Wei WI. Endoscopic surgery for malignant sinonasal tumours: an eighteen year experience. Rhinology. (2015) 53:204–11. doi: 10.4193/Rhin14.318
108. Cracchiolo JR, Patel K, Migliacci JC, Morris LT, Ganly I, Roman BR, et al. Factors associated with a primary surgical approach for sinonasal squamous cell carcinoma. J Surg Oncol. (2018) 117:756–64. doi: 10.1002/jso.24923
109. Mahmood U, Koshy M, Goloubeva O, Suntharalingam M. Adjuvant radiation therapy for high-grade and/or locally advanced major salivary gland tumors. Arch Otolaryngol Head Neck Surg. (2011) 137:1025–30. doi: 10.1001/archoto.2011.158
110. Gamez ME, Lal D, Halyard MY, Wong WW, Vargas C, Ma D, et al. Outcomes and patterns of failure for sinonasal undifferentiated carcinoma (SNUC): the mayo clinic experience. Head Neck. (2017) 39:1819–24. doi: 10.1002/hed.24834
111. Kashiwazaki R, Turner MT, Geltzeiler M, Fernandez-Miranda JC, Gardner PA, Snyderman CH, et al. The endoscopic endonasal approach for sinonasal and nasopharyngeal adenoid cystic carcinoma. Laryngoscope. (2019) 130:1414–21. doi: 10.1002/lary.28100
112. Overgaard J, Hansen HS, Overgaard M, Bastholt L, Berthelsen A, Specht L, et al. A randomized double-blind phase III study of nimorazole as a hypoxic radiosensitizer of primary radiotherapy in supraglottic larynx and pharynx carcinoma. Results of the danish head and neck cancer study (DAHANCA) protocol 5-85. Radiother Oncol. (1998) 46:135–46. doi: 10.1016/S0167-8140(97)00220-X
113. Michel J, Radulesco T, Penicaud M, Mancini J, Dessi P. Sinonasal adenocarcinoma: clinical outcomes and predictive factors. Int J Oral Maxillofac Surg. (2017) 46:422–7. doi: 10.1016/j.ijom.2016.11.018
114. Michel J, Fakhry N, Mancini J, Braustein D, Moreddu E, Giovanni A, et al. Sinonasal squamous cell carcinomas: clinical outcomes and predictive factors. Int J Oral Maxillofac Surg. (2014) 43:1–6. doi: 10.1016/j.ijom.2013.07.741
115. Airoldi M, Garzaro M, Valente G, Mamo C, Bena A, Giordano C, et al. Clinical and biological prognostic factors in 179 cases with sinonasal carcinoma treated in the Italian piedmont region. Oncology. (2009) 76:262–9. doi: 10.1159/000206140
116. Kuo P, Manes RP, Schwam ZG, Judson BL. Survival outcomes for combined modality therapy for sinonasal undifferentiated carcinoma. Otolaryngol Head Neck Surg. (2017) 156:132–6. doi: 10.1177/0194599816670146
117. Kuo P, Torabi SJ, Kraus D, Judson BL. Survival outcomes for induction vs adjuvant chemotherapy in squamous cell carcinoma of the maxillary sinus. Otolaryngol Head Neck Surg. (2019) 160:658–63. doi: 10.1177/0194599818804777
118. Kang JH, Cho SH, Kim JP, Kang KM, Cho KS, Kim W, et al. Treatment outcomes between concurrent chemoradiotherapy and combination of surgery, radiotherapy, and/or chemotherapy in stage III and IV maxillary sinus cancer: multi-institutional retrospective analysis. J Oral Maxillofac Surg. (2012) 70:1717–23. doi: 10.1016/j.joms.2011.06.221
119. Wong LY, Wei WI, Lam LK, Yuen AP. Salvage of recurrent head and neck squamous cell carcinoma after primary curative surgery. Head Neck. (2003) 25:953–9. doi: 10.1002/hed.10310
120. Arnold DJ, Goodwin WJ, Weed DT, Civantos FJ. Treatment of recurrent and advanced stage squamous cell carcinoma of the head and neck. Semin Radiat Oncol. (2004) 14:190–5. doi: 10.1053/j.semradonc.2004.03.001
121. Lokich J, Anderson N. Carboplatin versus cisplatin in solid tumors: an analysis of the literature. Ann Oncol. (1998) 9:13–21. doi: 10.1023/A:1008215213739
122. Go RS, Adjei AA. Review of the comparative pharmacology and clinical activity of cisplatin and carboplatin. J Clin Oncol. (1999) 17:409–22. doi: 10.1200/JCO.1999.17.1.409
123. Hong WK, Schaefer S, Issell B, Cummings C, Luedke D, Bromer R, et al. A prospective randomized trial of methotrexate versus cisplatin in the treatment of recurrent squamous cell carcinoma of the head and neck. Cancer. (1983) 52:206–10. doi: 10.1002/1097-0142(19830715)52:2<206::AID-CNCR2820520204>3.0.CO;2-J
124. A phase III randomised trial of cistplatinum methotrextate cisplatinum + methotrexate and cisplatinum + 5-FU in end stage squamous carcinoma of the head and neck. Liverpool head and neck oncology group. Br J Cancer. (1990) 61:311–5. doi: 10.1038/bjc.1990.59
125. Clavel M, Vermorken JB, Cognetti F, Cappelaere P, de Mulder PH, Schornagel JH, et al. Randomized comparison of cisplatin, methotrexate, bleomycin and vincristine (CABO) versus cisplatin and 5-fluorouracil (CF) versus cisplatin (C) in recurrent or metastatic squamous cell carcinoma of the head and neck. A phase III study of the EORTC head and neck cancer cooperative group. Ann Oncol. (1994) 5:521–6. doi: 10.1093/oxfordjournals.annonc.a058906
126. Veronesi A, Zagonel V, Tirelli U, Galligioni E, Tumolo S, Barzan L, et al. High-dose versus low-dose cisplatin in advanced head and neck squamous carcinoma: a randomized study. J Clin Oncol. (1985) 3:1105–8. doi: 10.1200/JCO.1985.3.8.1105
127. Forastiere AA, Takasugi BJ, Baker SR, Wolf GT, Kudla-Hatch V. High-dose cisplatin in advanced head and neck cancer. Cancer Chemother Pharmacol. (1987) 19:155–8. doi: 10.1007/BF00254569
128. Forastiere AA, Leong T, Rowinsky E, Murphy BA, Vlock DR, DeConti RC, et al. Phase III comparison of high-dose paclitaxel + cisplatin + granulocyte colony-stimulating factor versus low-dose paclitaxel + cisplatin in advanced head and neck cancer: eastern cooperative oncology group study E1393. J Clin Oncol. (2001) 19:1088–95. doi: 10.1200/JCO.2001.19.4.1088
129. Havlin KA, Kuhn JG, Myers JW, Ozols RF, Mattox DE, Clark GM, et al. High-dose cisplatin for locally advanced or metastatic head and neck cancer. A phase II pilot study. Cancer. (1989) 63:423–7. doi: 10.1002/1097-0142(19890201)63:3<423::AID-CNCR2820630304>3.0.CO;2-C
130. Vermorken JB, Trigo J, Hitt R, Koralewski P, Diaz-Rubio E, Rolland F, et al. Open-label, uncontrolled, multicenter phase II study to evaluate the efficacy and toxicity of cetuximab as a single agent in patients with recurrent and/or metastatic squamous cell carcinoma of the head and neck who failed to respond to platinum-based therapy. J Clin Oncol. (2007) 25:2171–7. doi: 10.1200/JCO.2006.06.7447
131. Konig MS, Osnes T, Meling TR. Treatment of esthesioneuroblastomas. Neurochirurgie. (2014) 60:151–7. doi: 10.1016/j.neuchi.2014.03.007
132. Sheehan JM, Sheehan JP, Jane JA Sr, Polin RS. Chemotherapy for esthesioneuroblastomas. Neurosurg Clin N Am. (2000) 11:693–701. doi: 10.1016/S1042-3680(18)30094-9
133. Eich HT, Hero B, Staar S, Micke O, Seegenschmiedt H, Mattke A, et al. Multimodality therapy including radiotherapy and chemotherapy improves event-free survival in stage C esthesioneuroblastoma. Strahlenther Onkol. (2003) 179:233–40. doi: 10.1007/s00066-003-1089-x
134. Zappia JJ, Carroll WR, Wolf GT, Thornton AF, Ho L, Krause CJ. Olfactory neuroblastoma: the results of modern treatment approaches at the university of michigan. Head Neck. (1993) 15:190–6. doi: 10.1002/hed.2880150303
135. Argiris A, Dutra J, Tseke P, Haines K. Esthesioneuroblastoma: the northwestern university experience. Laryngoscope. (2003) 113:155–60. doi: 10.1097/00005537-200301000-00029
136. Benlyazid A, Thariat J, Temam S, Malard O, Florescu C, Choussy O, et al. Postoperative radiotherapy in head and neck mucosal melanoma: a GETTEC study. Arch Otolaryngol Head Neck Surg. (2010) 136:1219–25. doi: 10.1001/archoto.2010.217
137. Patel SG, Prasad ML, Escrig M, Singh B, Shaha AR, Kraus DH, et al. Primary mucosal malignant melanoma of the head and neck. Head Neck. (2002) 24:247–57. doi: 10.1002/hed.10019
138. Temam S, Mamelle G, Marandas P, Wibault P, Avril MF, Janot F, et al. Postoperative radiotherapy for primary mucosal melanoma of the head and neck. Cancer. (2005) 103:313–9. doi: 10.1002/cncr.20775
139. Wu AJ, Gomez J, Zhung JE, Chan K, Gomez DR, Wolden SL, et al. Radiotherapy after surgical resection for head and neck mucosal melanoma. Am J Clin Oncol. (2010) 33:281–5. doi: 10.1097/COC.0b013e3181a879f5
140. Owens JM, Roberts DB, Myers JN. The role of postoperative adjuvant radiation therapy in the treatment of mucosal melanomas of the head and neck region. Arch Otolaryngol Head Neck Surg. (2003) 129:864–8. doi: 10.1001/archotol.129.8.864
141. Lian B, Si L, Cui C, Chi Z, Sheng X, Mao L, et al. Phase II randomized trial comparing high-dose IFN-alpha2b with temozolomide plus cisplatin as systemic adjuvant therapy for resected mucosal melanoma. Clin Cancer Res. (2013) 19:4488–98. doi: 10.1158/1078-0432.CCR-13-0739
142. Carvajal RD, Lawrence DP, Weber JS, Gajewski TF, Gonzalez R, Lutzky J, et al. Phase II study of nilotinib in melanoma harboring KIT alterations following progression to prior KIT inhibition. Clin Cancer Res. (2015) 21:2289–96. doi: 10.1158/1078-0432.CCR-14-1630
143. Curtin JA, Busam K, Pinkel D, Bastian BC. Somatic activation of KIT in distinct subtypes of melanoma. J Clin Oncol. (2006) 24:4340–6. doi: 10.1200/JCO.2006.06.2984
144. Hodi FS, Friedlander P, Corless CL, Heinrich MC, Mac Rae S, Kruse A, et al. Major response to imatinib mesylate in KIT-mutated melanoma. J Clin Oncol. (2008) 26:2046–51. doi: 10.1200/JCO.2007.14.0707
145. Lutzky J, Bauer J, Bastian BC. Dose-dependent, complete response to imatinib of a metastatic mucosal melanoma with a K642E KIT mutation. Pigment Cell Melanoma Res. (2008) 21:492–3. doi: 10.1111/j.1755-148X.2008.00475.x
146. Guo J, Si L, Kong Y, Flaherty KT, Xu X, Zhu Y, et al. Phase II, open-label, single-arm trial of imatinib mesylate in patients with metastatic melanoma harboring c-Kit mutation or amplification. J Clin Oncol. (2011) 29:2904–9. doi: 10.1200/JCO.2010.33.9275
147. Quintas-Cardama A, Lazar AJ, Woodman SE, Kim K, Ross M, Hwu P. Complete response of stage IV anal mucosal melanoma expressing KIT Val560Asp to the multikinase inhibitor sorafenib. Nat Clin Pract Oncol. (2008) 5:737–40. doi: 10.1038/ncponc1251
148. Kalinsky K, Lee S, Rubin KM, Lawrence DP, Iafrarte AJ, Borger DR, et al. A phase 2 trial of dasatinib in patients with locally advanced or stage IV mucosal, acral, or vulvovaginal melanoma: a trial of the ECOG-ACRIN cancer research group (E2607). Cancer. (2017) 123:2688–97. doi: 10.1002/cncr.30663
149. Del Vecchio M, Di Guardo L, Ascierto PA, Grimaldi AM, Sileni VC, Pigozzo J, et al. Efficacy and safety of ipilimumab 3mg/kg in patients with pretreated, metastatic, mucosal melanoma. Eur J Cancer. (2014) 50:121–7. doi: 10.1016/j.ejca.2013.09.007
150. D'Angelo SP, Larkin J, Sosman JA, Lebbe C, Brady B, Neyns B, et al. Efficacy and safety of nivolumab alone or in combination with ipilimumab in patients with mucosal melanoma: a pooled analysis. J Clin Oncol. (2017) 35:226–35. doi: 10.1200/JCO.2016.67.9258
151. Mendenhall WM, Mendenhall CM, Werning JW, Riggs CE, Mendenhall NP. Adult head and neck soft tissue sarcomas. Head Neck. (2005) 27:916–22. doi: 10.1002/hed.20249
152. Chang AE, Chai X, Pollack SM, Loggers E, Rodler E, Dillon J, et al. Analysis of clinical prognostic factors for adult patients with head and neck sarcomas. Otolaryngol Head Neck Surg. (2014) 151:976–83. doi: 10.1177/0194599814551539
153. Peng KA, Grogan T, Wang MB. Head and neck sarcomas: analysis of the SEER database. Otolaryngol Head Neck Surg. (2014) 151:627–33. doi: 10.1177/0194599814545747
154. Blank LE, Koedooder K, Pieters BR, van der Grient HN, van de Kar M, Buwalda J, et al. The AMORE protocol for advanced-stage and recurrent nonorbital rhabdomyosarcoma in the head-and-neck region of children: a radiation oncology view. Int J Radiat Oncol Biol Phys. (2009) 74:1555–62. doi: 10.1016/j.ijrobp.2008.10.029
155. Lydiatt WM, Shaha AR, Shah JP. Angiosarcoma of the head and neck. Am J Surg. (1994) 168:451–4. doi: 10.1016/S0002-9610(05)80097-2
156. Mark RJ, Tran LM, Sercarz J, Fu YS, Calcaterra TC, Juillard GF. Angiosarcoma of the head and neck. The UCLA experience 1955 through 1990. Arch Otolaryngol Head Neck Surg. (1993) 119:973–8. doi: 10.1001/archotol.1993.01880210061009
157. Morrison WH, Byers RM, Garden AS, Evans HL, Ang KK, Peters LJ. Cutaneous angiosarcoma of the head and neck. A therapeutic dilemma. Cancer. (1995) 76:319–27. doi: 10.1002/1097-0142(19950715)76:2<319::AID-CNCR2820760224>3.0.CO;2-8
158. Patel SH, Hayden RE, Hinni ML, Wong WW, Foote RL, Milani S, et al. Angiosarcoma of the scalp and face: the mayo clinic experience. JAMA Otolaryngol Head Neck Surg. (2015) 141:335–40. doi: 10.1001/jamaoto.2014.3584
159. Schouwenburg PF, Kupperman D, Bakker FP, Blank LE, de Boer HB, Voute TA. New combined treatment of surgery, radiotherapy, and reconstruction in head and neck rhabdomyosarcoma in children: the AMORE protocol. Head Neck. (1998) 20:283–92. doi: 10.1002/(SICI)1097-0347(199807)20:4<283::AID-HED1>3.0.CO;2-V
160. Agulnik M, Yarber JL, Okuno SH, von Mehren M, Jovanovic BD, Brockstein BE, et al. An open-label, multicenter, phase II study of bevacizumab for the treatment of angiosarcoma and epithelioid hemangioendotheliomas. Ann Oncol. (2013) 24:257–63. doi: 10.1093/annonc/mds237
161. Stacchiotti S, Tamborini E, Marrari A, Brich S, Rota SA, Orsenigo M, et al. Response to sunitinib malate in advanced alveolar soft part sarcoma. Clin Cancer Res. (2009) 15:1096–104. doi: 10.1158/1078-0432.CCR-08-2050
162. Rogers L, Gilbert M, Vogelbaum MA. Intracranial meningiomas of atypical (WHO grade II) histology. J Neurooncol. (2010) 99:393–405. doi: 10.1007/s11060-010-0343-1
163. Hanft S, Canoll P, Bruce JN. A review of malignant meningiomas: diagnosis, characteristics, and treatment. J Neurooncol. (2010) 99:433–43. doi: 10.1007/s11060-010-0348-9
164. Sughrue ME, Sanai N, Shangari G, Parsa AT, Berger MS, McDermott MW. Outcome and survival following primary and repeat surgery for world health organization grade III meningiomas. J Neurosurg. (2010) 113:202–9. doi: 10.3171/2010.1.JNS091114
165. Rosenberg LA, Prayson RA, Lee J, Reddy C, Chao ST, Barnett GH, et al. Long-term experience with world health organization grade III (malignant) meningiomas at a single institution. Int J Radiat Oncol Biol Phys. (2009) 74:427–32. doi: 10.1016/j.ijrobp.2008.08.018
166. Milosevic MF, Frost PJ, Laperriere NJ, Wong CS, Simpson WJ. Radiotherapy for atypical or malignant intracranial meningioma. Int J Radiat Oncol Biol Phys. (1996) 34:817–22. doi: 10.1016/0360-3016(95)02166-3
167. Dziuk TW, Woo S, Butler EB, Thornby J, Grossman R, Dennis WS, et al. Malignant meningioma: an indication for initial aggressive surgery and adjuvant radiotherapy. J Neurooncol. (1998) 37:177–88. doi: 10.1023/A:1005853720926
168. Perry A, Scheithauer BW, Stafford SL, Lohse CM, Wollan PC. Malignancy in meningiomas: a clinicopathologic study of 116 patients, with grading implications. Cancer. (1999) 85:2046–56. doi: 10.1002/(SICI)1097-0142(19990501)85:9<2046::AID-CNCR23>3.0.CO;2-M
169. Palma L, Celli P, Franco C, Cervoni L, Cantore G. Long-term prognosis for atypical and malignant meningiomas: a study of 71 surgical cases. Neurosurg Focus. (1997) 2:e3. doi: 10.3171/foc.1997.2.4.6
170. Park HJ, Kang HC, Kim IH, Park SH, Kim DG, Park CK, et al. The role of adjuvant radiotherapy in atypical meningioma. J Neurooncol. (2013) 115:241–7. doi: 10.1007/s11060-013-1219-y
171. Hardesty DA, Wolf AB, Brachman DG, McBride HL, Youssef E, Nakaji P, et al. The impact of adjuvant stereotactic radiosurgery on atypical meningioma recurrence following aggressive microsurgical resection. J Neurosurg. (2013) 119:475–81. doi: 10.3171/2012.12.JNS12414
172. Wang C, Kaprealian TB, Suh JH, Kubicky CD, Ciporen JN, Chen Y, et al. Overall survival benefit associated with adjuvant radiotherapy in WHO grade II meningioma. Neuro Oncol. (2017) 19:1263–70. doi: 10.1093/neuonc/nox007
173. Aghi MK, Carter BS, Cosgrove GR, Ojemann RG, Amin-Hanjani S, Martuza RL, et al. Long-term recurrence rates of atypical meningiomas after gross total resection with or without postoperative adjuvant radiation. Neurosurgery. (2009) 64:56–60. doi: 10.1227/01.NEU.0000330399.55586.63
174. Komotar RJ, Iorgulescu JB, Raper DM, Holland EC, Beal K, Bilsky MH, et al. The role of radiotherapy following gross-total resection of atypical meningiomas. J Neurosurg. (2012) 117:679–86. doi: 10.3171/2012.7.JNS112113
175. Adeberg S, Hartmann C, Welzel T, Rieken S, Habermehl D, von Deimling A, et al. Long-term outcome after radiotherapy in patients with atypical and malignant meningiomas–clinical results in 85 patients treated in a single institution leading to optimized guidelines for early radiation therapy. Int J Radiat Oncol Biol Phys. (2012) 83:859–64. doi: 10.1016/j.ijrobp.2011.08.010
176. Combs SE, Adeberg S, Dittmar JO, Welzel T, Rieken S, Habermehl D, et al. Skull base meningiomas: long-term results and patient self-reported outcome in 507 patients treated with fractionated stereotactic radiotherapy (FSRT) or intensity modulated radiotherapy (IMRT). Radiother Oncol. (2013) 106:186–91. doi: 10.1016/j.radonc.2012.07.008
177. Aizer AA, Arvold ND, Catalano P, Claus EB, Golby AJ, Johnson MD, et al. Adjuvant radiation therapy, local recurrence, and the need for salvage therapy in atypical meningioma. Neuro Oncol. (2014) 16:1547–53. doi: 10.1093/neuonc/nou098
178. Weber DC, Ares C, Villa S, Peerdeman SM, Renard L, Baumert BG, et al. Adjuvant postoperative high-dose radiotherapy for atypical and malignant meningioma: a phase-II parallel non-randomized and observation study (EORTC 22042-26042). Radiother Oncol. (2018) 128:260–5. doi: 10.1016/j.radonc.2018.06.018
179. Rogers L, Zhang P, Vogelbaum MA, Perry A, Ashby LS, Modi JM, et al. Intermediate-risk meningioma: initial outcomes from NRG oncology RTOG 0539. J Neurosurg. (2018) 129:35–47. doi: 10.3171/2016.11.JNS161170
180. Kaur G, Sayegh ET, Larson A, Bloch O, Madden M, Sun MZ, et al. Adjuvant radiotherapy for atypical and malignant meningiomas: a systematic review. Neuro Oncol. (2014) 16:628–36. doi: 10.1093/neuonc/nou025
181. Mair R, Morris K, Scott I, Carroll TA. Radiotherapy for atypical meningiomas. J Neurosurg. (2011) 115:811–9. doi: 10.3171/2011.5.JNS11112
182. Brem SS, Bierman PJ, Brem H, Butowski N, Chamberlain MC, Chiocca EA, et al. Central nervous system cancers. J Natl Compr Canc Netw. (2011) 9:352–400. doi: 10.6004/jnccn.2011.0036
183. Moazzam AA, Wagle N, Zada G. Recent developments in chemotherapy for meningiomas: a review. Neurosurg Focus. (2013) 35:E18. doi: 10.3171/2013.10.FOCUS13341
184. Guadagnolo BA, Zagars GK, Raymond AK, Benjamin RS, Sturgis EM. Osteosarcoma of the jaw/craniofacial region: outcomes after multimodality treatment. Cancer. (2009) 115:3262–70. doi: 10.1002/cncr.24297
185. Mark RJ, Sercarz JA, Tran L, Dodd LG, Selch M, Calcaterra TC. Osteogenic sarcoma of the head and neck. The UCLA experience. Arch Otolaryngol Head Neck Surg. (1991) 117:761–6. doi: 10.1001/archotol.1991.01870190073015
186. Canadian Society of O-H Neck Surgery Oncology Study G. Osteogenic sarcoma of the mandible and maxilla: a canadian review (1980-2000). J Otolaryngol. (2004) 33:139–44. doi: 10.2310/7070.2004.03013
187. Catton C, O'Sullivan B, Bell R, Laperriere N, Cummings B, Fornasier V, et al. Chordoma: long-term follow-up after radical photon irradiation. Radiother Oncol. (1996) 41:67–72. doi: 10.1016/S0167-8140(96)91805-8
188. Alahmari M, Temel Y. Skull base chordoma treated with proton therapy: a systematic review. Surg Neurol Int. (2019) 10:96. doi: 10.25259/SNI-213-2019
189. Zhou J, Yang B, Wang X, Jing Z. Comparison of the effectiveness of radiotherapy with photons and particles for chordoma after surgery: a meta-analysis. World Neurosurg. (2018) 117:46–53. doi: 10.1016/j.wneu.2018.05.209
190. Smith RB, Apostolakis LW, Karnell LH, Koch BB, Robinson RA, Zhen W, et al. National cancer data base report on osteosarcoma of the head and neck. Cancer. (2003) 98:1670–80. doi: 10.1002/cncr.11716
191. Huh WW, Holsinger FC, Levy A, Palla FS, Anderson PM. Osteosarcoma of the jaw in children and young adults. Head Neck. (2012) 34:981–4. doi: 10.1002/hed.21850
192. van Maldegem AM, Gelderblom H, Palmerini E, Dijkstra SD, Gambarotti M, Ruggieri P, et al. Outcome of advanced, unresectable conventional central chondrosarcoma. Cancer. (2014) 120:3159–64. doi: 10.1002/cncr.28845
193. Italiano A, Mir O, Cioffi A, Palmerini E, Piperno-Neumann S, Perrin C, et al. Advanced chondrosarcomas: role of chemotherapy and survival. Ann Oncol. (2013) 24:2916–22. doi: 10.1093/annonc/mdt374
194. Suijker J, Oosting J, Koornneef A, Struys EA, Salomons GS, Schaap FG, et al. Inhibition of mutant IDH1 decreases D-2-HG levels without affecting tumorigenic properties of chondrosarcoma cell lines. Oncotarget. (2015) 6:12505–19. doi: 10.18632/oncotarget.3723
195. Li L, Paz AC, Wilky BA, Johnson B, Galoian K, Rosenberg A, et al. Treatment with a small molecule mutant IDH1 inhibitor suppresses tumorigenic activity and decreases production of the oncometabolite 2-hydroxyglutarate in human chondrosarcoma cells. PLoS ONE. (2015) 10:e0133813. doi: 10.1371/journal.pone.0133813
196. Bovee JV, Hogendoorn PC, Wunder JS, Alman BA. Cartilage tumours and bone development: molecular pathology and possible therapeutic targets. Nat Rev Cancer. (2010) 10:481–8. doi: 10.1038/nrc2869
197. Grignani G, Palmerini E, Stacchiotti S, Boglione A, Ferraresi V, Frustaci S, et al. A phase 2 trial of imatinib mesylate in patients with recurrent nonresectable chondrosarcomas expressing platelet-derived growth factor receptor-alpha or -beta: an Italian sarcoma group study. Cancer. (2011) 117:826–31. doi: 10.1002/cncr.25632
198. Bernstein-Molho R, Kollender Y, Issakov J, Bickels J, Dadia S, Flusser G, et al. Clinical activity of mTOR inhibition in combination with cyclophosphamide in the treatment of recurrent unresectable chondrosarcomas. Cancer Chemother Pharmacol. (2012) 70:855–60. doi: 10.1007/s00280-012-1968-x
199. Abu-Ghanem S, Horowitz G, Abergel A, Yehuda M, Gutfeld O, Carmel NN, et al. Elective neck irradiation versus observation in squamous cell carcinoma of the maxillary sinus with N0 neck: a meta-analysis and review of the literature. Head Neck. (2015) 37:1823–8. doi: 10.1002/hed.23791
200. Nalavenkata SB, Sacks R, Adappa ND, Palmer JN, Purkey MT, Feldman MD, et al. Olfactory neuroblastoma: fate of the neck–a long-term multicenter retrospective study. Otolaryngol Head Neck Surg. (2016) 154:383–9. doi: 10.1177/0194599815620173
201. Cantu G, Bimbi G, Miceli R, Mariani L, Colombo S, Riccio S, et al. Lymph node metastases in malignant tumors of the paranasal sinuses: prognostic value and treatment. Arch Otolaryngol Head Neck Surg. (2008) 134:170–7. doi: 10.1001/archoto.2007.30
202. Dooley L, Shah J. Management of the neck in maxillary sinus carcinomas. Curr Opin Otolaryngol Head Neck Surg. (2015) 23:107–14. doi: 10.1097/MOO.0000000000000138
203. Brown JS, Bekiroglu F, Shaw RJ, Woolgar JA, Triantafyllou A, Rogers SN. First report of elective selective neck dissection in the management of squamous cell carcinoma of the maxillary sinus. Br J Oral Maxillofac Surg. (2013) 51:103–7. doi: 10.1016/j.bjoms.2012.04.004
204. Lund V, Howard DJ, Wei WI. Endoscopic resection of malignant tumors of the nose and sinuses. Am J Rhinol. (2007) 21:89–94. doi: 10.2500/ajr.2007.21.2957
205. Bhandare N, Monroe AT, Morris CG, Bhatti MT, Mendenhall WM. Does altered fractionation influence the risk of radiation-induced optic neuropathy? Int J Radiat Oncol Biol Phys. (2005) 62:1070–7. doi: 10.1016/j.ijrobp.2004.12.009
206. Monroe AT, Bhandare N, Morris CG, Mendenhall WM. Preventing radiation retinopathy with hyperfractionation. Int J Radiat Oncol Biol Phys. (2005) 61:856–64. doi: 10.1016/j.ijrobp.2004.07.664
207. Johnson J, Barani IJ. Radiotherapy for malignant tumors of the skull base. Neurosurg Clin North Am. (2013) 24:125–35. doi: 10.1016/j.nec.2012.08.011
208. Claus F, De Gersem W, De Wagter C, Van Severen R, Vanhoutte I, Duthoy W, et al. An implementation strategy for IMRT of ethmoid sinus cancer with bilateral sparing of the optic pathways. Int J Radiat Oncol Biol Phys. (2001) 51:318–31. doi: 10.1016/S0360-3016(01)01627-3
209. Madani I, Bonte K, Vakaet L, Boterberg T, De Neve W. Intensity-modulated radiotherapy for sinonasal tumors: ghent university hospital update. Int J Radiat Oncol Biol Phys. (2009) 73:424–32. doi: 10.1016/j.ijrobp.2008.04.037
Keywords: skull base malignancies, adjuvant therapies, sinonasal cancer, olfactory, neuroblastoma, mucosal melanoma, malignant meningioma, soft tissue sarcoma
Citation: König M, Osnes T, Bruland Ø, Sundby Hall K, Bratland Å and Meling TR (2020) The Role of Adjuvant Treatment in Craniofacial Malignancy: A Critical Review. Front. Oncol. 10:1402. doi: 10.3389/fonc.2020.01402
Received: 15 May 2020; Accepted: 02 July 2020;
Published: 07 August 2020.
Edited by:
Aviram Mizrachi, Rabin Medical Center, IsraelReviewed by:
Diana Bell, University of Texas MD Anderson Cancer Center, United StatesJames O'Hara, Newcastle upon Tyne NHS Hospitals, United Kingdom
Copyright © 2020 König, Osnes, Bruland, Sundby Hall, Bratland and Meling. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marton König, bWFrb25pQG91cy1oZi5ubw==; Terje Osnes, dG9zbmVzQG91cy1oZi5ubw==