 Fabian Weykamp1,2,3Rami A. El Shafie1,2,3Laila König1,2,3Katharina Seidensaal1,2,3Tobias Forster1,2,3Nathalie Arians1,2,3Sebastian Regnery1,2,3Philipp Hoegen1,2,3Thomas M. Deutsch4Andreas Schneeweiss3Jürgen Debus1,2,3,5,6,7Juliane Hörner-Rieber1,2,3,6*
Fabian Weykamp1,2,3Rami A. El Shafie1,2,3Laila König1,2,3Katharina Seidensaal1,2,3Tobias Forster1,2,3Nathalie Arians1,2,3Sebastian Regnery1,2,3Philipp Hoegen1,2,3Thomas M. Deutsch4Andreas Schneeweiss3Jürgen Debus1,2,3,5,6,7Juliane Hörner-Rieber1,2,3,6*- 1Department of Radiation Oncology, Heidelberg University Hospital, Heidelberg, Germany
- 2Heidelberg Institute of Radiation Oncology (HIRO), Heidelberg, Germany
- 3Department of Obstetrics and Gynecology, Heidelberg University Hospital, Heidelberg, Germany
- 4National Center for Tumor Diseases (NCT), Heidelberg, Germany
- 5Department of Radiation Oncology, Heidelberg Ion-Beam Therapy Center (HIT), Heidelberg University Hospital, Heidelberg, Germany
- 6Clinical Cooperation Unit Radiation Oncology, German Cancer Research Center (DKFZ), Heidelberg, Germany
- 7German Cancer Consortium (DKTK), Partner Site Heidelberg, Heidelberg, Germany
Purpose: Several prognostic indexes for overall survival (OS) after radiotherapy of brain metastases in breast cancer patients exist but are mainly validated for whole-brain radiotherapy or not specifically for breast cancer patients. To date, no such index provides information beyond mere OS.
Methods: We retrospectively analyzed 95 breast cancer patients treated with stereotactic radiosurgery for 203 brain metastases. The Kaplan–Meier method with log-rank test was used to assess OS, local control (LC), distant cranial control (DCC), and extracranial control (EC). Cox regression was applied to detect prognostic outcome factors. A point scoring system was designed to stratify patients based on outcome. Nine established prognostic indexes were analyzed using the concordance index (c-index).
Results: Two out of nine analyzed prognostic indexes for OS showed a significant c-index, the breast graded prognostic assessment (bGPA; 0.631; 95% CI, 0.514–0.748; p = 0.037) and the modified bGPA (mod-bGPA; 0.662; 95% CI, 0.547–0.777; p = 0.010). Significant results from multivariate analysis (Karnofsky Performance Score, Her2/neu receptor status, extracranial control) were used to generate a new point system: the breast cancer stereotactic radiotherapy score (bSRS), which discriminated three significantly different prognostic groups, for LC, DCC, EC, and OS, respectively. However, the c-index was only significant for OS (0.689; 95% CI, 0.577–0.802; p = 0.003).
Conclusions: The new bSRS score was superior to the bGPA and mod-bGPA scores for prognosis of OS. The bSRS is easy to use and the first tool, which might also provide outcome assessment beyond mere OS. Future studies need to validate these findings.
Background and Purpose
In autopsy studies, central nervous system metastases were detected in up to 30% of breast cancer patients (1). Brain metastases represent a major limiting survival factor for breast cancer patients (2). Stereotactic radiosurgery (SRS) is the recommended treatment for limited brain metastases (3–6).
One of the oldest scoring tools to solely estimate overall survival (OS) in patients with brain metastases is the Graded Prognostic Assessment (GPA) index, which consists of age, Karnofsky performance status (KPS), number of brain metastases, and presence of extracranial metastases. This prognostic tool was developed through analysis of several RTOG studies (7–11). All of the mentioned studies mainly took place in the pre-Her2/neu receptor status era, only a small proportion of breast cancer patients were included, and no patient received SRS without concomitant whole-brain radiotherapy (WBRT). Sperduto et al. then developed the breast GPA (bGPA) for OS prediction in the year 2012, which specifically addressed breast cancer patients. This score includes age, KPS, and Her2/neu as well as hormone receptor status. The respective validation study comprised 400 breast cancer patients, 115 of which received SRS only. Interestingly, unlike the original GPA, the number of brain metastases and whether extracranial metastases were present were left out in the scoring system. Subsequently, Subbiah et al. developed a modified bGPA (mod-bGPA) for OS assessment by reintegrating the number of brain metastases into the scoring system. The respective study cohort comprised 1,552 breast cancer patients; however, only 164 of which (11%) received SRS alone (5). Furthermore, Sperduto et al. updated their bGPA (u-bGPA) and reintegrated the number of brain metastases and the presence of extracranial metastases (12). Table 1 illustrates an overview including several additional prognostic tools.
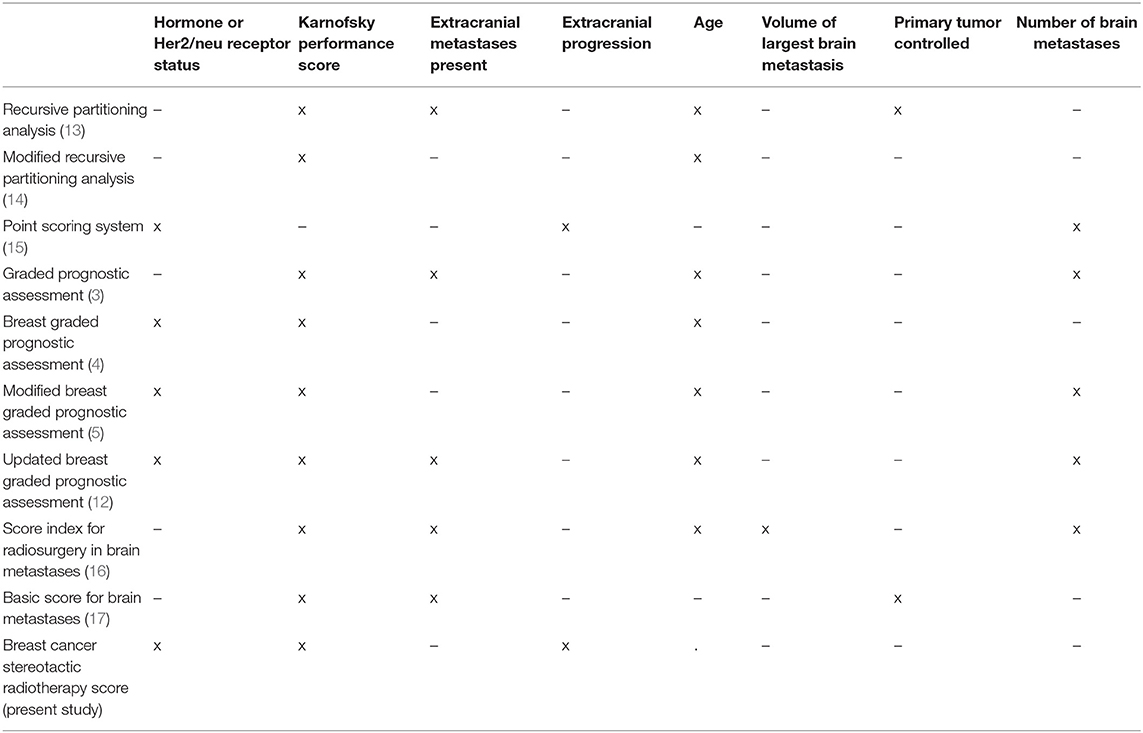
Table 1. Overview of prognostic scoring indexes for radiotherapy in brain metastases (x marks included factors).
Recent studies investigated prognostic factors for OS in breast cancer patients treated with SRS only. However, these studies did not analyze or compare the prognostic validity of the scoring tools in this particular setting. Instead, only a plane description of the number of patients in the respective prognostic group was performed (6, 18).
To our best knowledge, there is no available prognostic tool for breast cancer patients with brain metastases, which exceeds the assessment of mere OS. However, it is of high importance to also estimate local control (LC), distant cranial control (DCC), and extracranial control (EC) when discussing different treatment options and their optimal timing in an interdisciplinary tumor board, including SRS, WBRT, and intensification of systemic therapy.
On top of validating different OS scoring tools for SRS in cerebral metastasized breast cancer patients, we therefore sought to develop a new score, which comprises prognostic assessment of LC, DCC, EC, and OS altogether.
Methods
Patients and Treatment Characteristics
We retrospectively analyzed female breast cancer patients treated with SRS for brain metastases in the Department of Radiation Oncology at Heidelberg University Hospital from 05/2005 to 10/2019. Until 2016, patients were treated with a conventional linear accelerator (Siemens Mevatron, Erlangen, Germany, or Elekta Versa HD, Stockholm, Sweden), while from 2016 on, the CyberKnife M6 (Accuray Inc., Sunnyvale California, USA) was primarily used for radiosurgery.
All patients received an individual scotch cast or thermoplastic mask for head fixation. A computed tomography (CT) scan as well as a magnetic resonance imaging (MRI) scan of the head was performed for treatment planning. The gross tumor volume (GTV) of each brain metastasis was delineated on both contrast-enhanced CT and MRI. The addition of a safety margin (1–3 mm, isotropic) resulted in the planning target volume (PTV). For conventional linac-based radiosurgery, a PTV margin of 3 mm was applied to account for geometry uncertainty, while for robotic radiosurgery, a PTV margin of only 1 mm was used. The radiation dose was prescribed according to current German (19) and European (20) guidelines, depending on the size of the respective metastasis. Most patients received 20 or 18 Gy, prescribed to the 70% isodose and covering at least 98% of the PTV.
The biologically effective dose (BED) was calculated using the linear–quadratic model (21). An α/β ratio of 10 was assumed for brain metastases.
Ethics approval for the study and a waiver of written informed consent were granted by the Heidelberg University ethics committee on April 12, 2018 (#S-172/2018). Patient confidentiality was maintained by anonymizing patient data to remove any identifying information.
Endpoints and Statistical Methods
LC, DCC, EC, and OS were calculated starting from the last day of SRS. In this study, LC refers to the high-dose area surrounding the respective irradiated metastasis. Recurrences in the brain outside the high-dose area were defined as distant cranial failure. LC was calculated for each individual lesion. DCC, EC, and OS were calculated per patient. Toxicity was evaluated using the Common Terminology Criteria for Adverse Events (CTCAE v. 5.0).
The first follow-up MRI scan of the head was performed 6–8 weeks after completion of the SRS. Further follow-up was done according to German guidelines and regularly included a contrast-enhanced MRI scan of the head every 3 months.
LC, DCC, EC, and OS were estimated using the Kaplan–Meier method. Survival curves were compared applying the log-rank test. Cox regression was used for univariate analysis. Multivariate cox models were calculated including all variables with p ≤ 0.1 from univariate analysis.
The prognostic value of the nine investigated different prognostic scoring tools, shown in Table 1, was assessed by the concordance index (c-index), where a value of 1.0 represents a perfect prognostic scoring tool. A p < 0.05 was considered statistically significant.
Results from multivariate analysis (Table 2) were used to generate a new, all-encompassing index, which we refer to as the breast cancer stereotactic radiotherapy score (bSRS; Table 3). It encompasses the Her2/neu receptor status (independently significant for OS), the KPS (independently significant for OS and DCC), and the diagnosis of extracranial progression prior to SRS (borderline significant for OS and independently significant for LC and EC). We then attributed respective points proportionally to their hazard ratio in multivariate analysis (Table 2), with a higher score representing a more favorable outcome in terms of LC, DCC, EC, and OS. A positive Her2/neu receptor status (HR 0.8) resulted in 1 point, reflecting the independently better OS. A KPS of at least 80% (HR 0.4) led to 2 points accordingly, representing twice the effect of the Her2/neu receptor status. However, since the bSRS was designed as a multidimensional tool, we needed to modify the scoring process. Optimal results for LC, DCC, EC, and OS altogether were obtained, if the aforementioned 2 points were attributed only to patients with a KPS of at least 90% and 1 point in case of a KPS of 80%. The same accounted for patients with extracranial progression in terms of LC (HR 4.8). Best results were obtained for all four study endpoints, if 4 points were attributed to patients with extracranial control, reflecting a more favorable outcome. Thus, the maximum of seven points was achieved by patients who were in excellent clinical condition (KPS at least 90%), had stable or absent extracranial disease, and had a positive Her2/neu receptor status. Afterward, patients were allocated to three subgroups according to their respective points (0–4, 5, and 6–7), where 0–4 points represent the poor prognosis subgroup and 6–7 points stand for the subgroup with excellent prognosis in terms of LC, DCC, EC, and OS altogether. All statistical analyses were performed with SPSS software (IBM SPSS Version 24.0).
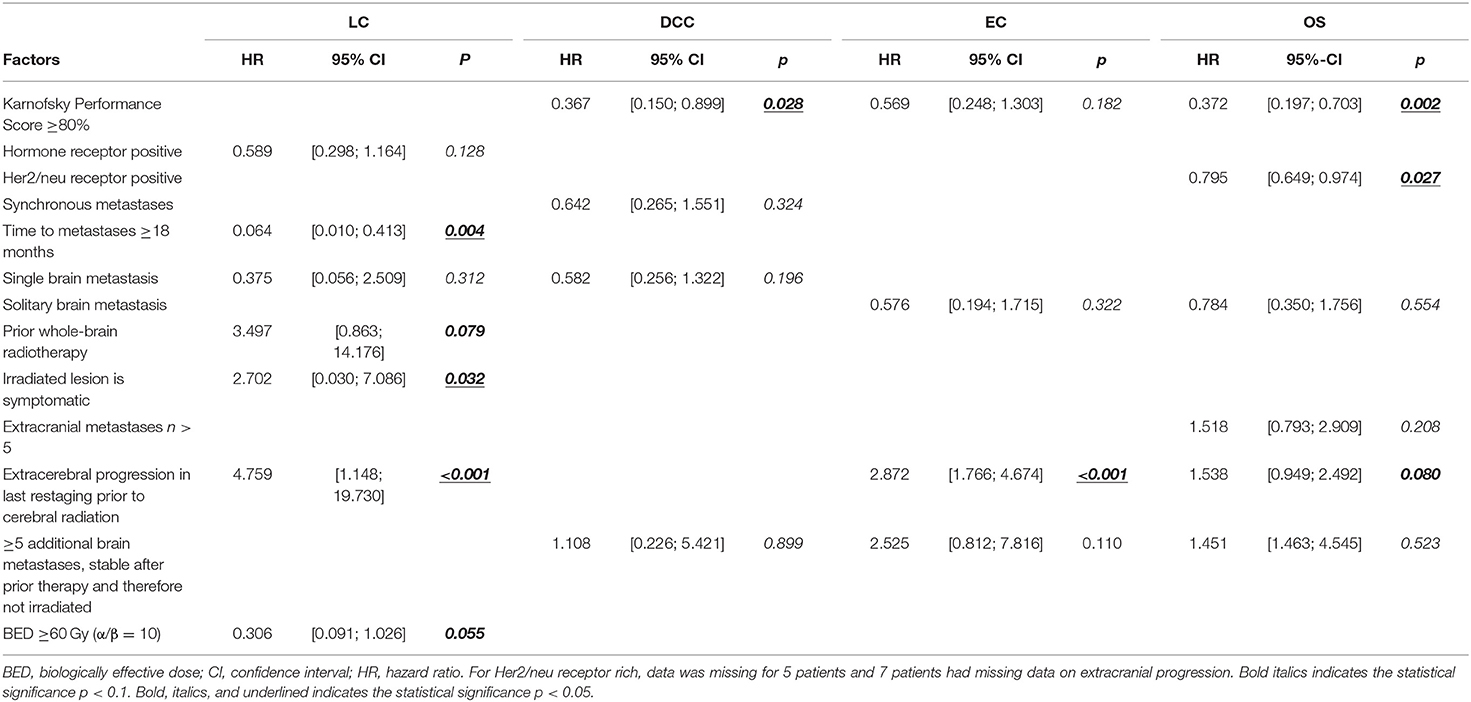
Table 2. Multivariate analysis of prognostic factors influencing local control (LC), distant cranial control (DCC), extracranial control (EC), and overall survival (OS).
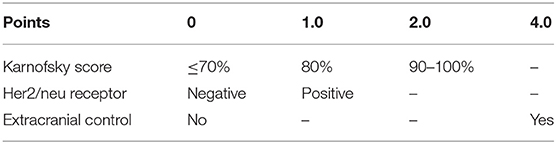
Table 3. Breast cancer scoring tool for radiosurgery (bSRS).
Results
Median age was 57 years (range 31–83 years) with a median KPS of 80%. Most patients suffered from additional extracranial metastases (62.2%). About a third (31.6%) had already been treated with WBRT for prior brain metastases. At radiosurgery, all patients were diagnosed with a controlled primary tumor. Further patient characteristics are illustrated in Table 4. Table 5 shows characteristics of the SRS treatment. Most patients received treatment of a single lesion (51.6%) with a maximum of seven irradiated brain metastases.
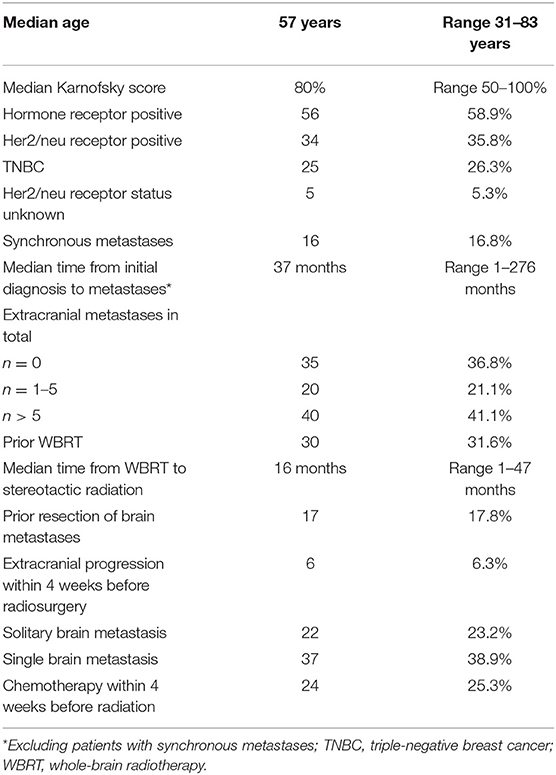
Table 4. Patient characteristics (n = 95).
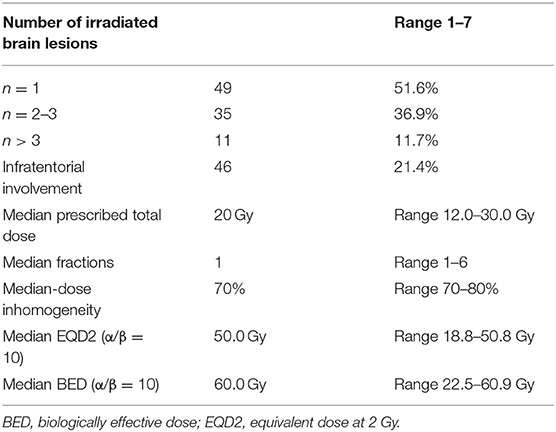
Table 5. Treatment characteristics (n = 203).
Seventeen (17.9%) grade I acute toxicities were described at first follow-up (mainly mild headache, nausea, or dizziness) and 3 (3.2%) grade II toxicities were documented (nausea, cerebral edema, and headache). In six patients, radiation induced blood–brain barrier disruptions were detected, of whom two underwent surgery, which confirmed radionecrosis and no tumor recurrence. Median imaging follow-up was 11.9 months (range 0.8–105.3).
Local Control
Local control, defined as a stable or regressive contrast enhancement in the T1-weighted MRI, was 90.6% at 12 months and 71.6% at 24 months.
Univariate analysis (Table 6) showed hormone receptor positivity (HR = 0.626, CI [0.407; 0.961], p = 0.032), time to metastases of any kind ≥18 months (HR = 0.239, CI [0.090; 0.634], p = 0.004), and a BED ≥60 Gy (HR = 0.378, CI [0.160; 0.894], p = 0.027) as positive prognostic factors, whereas symptomatic brain lesions were associated with worse LC (HR = 2.702, CI [0.030; 7.086], p = 0.043) as well as extracerebral progression within 4 weeks prior to SRS (HR = 5.265, CI [2.534; 10.940], p < 0.001). In multivariate analysis, time to metastases ≥18 months (HR = 0.064, CI [0.010; 0.413], p = 0.004) was identified as an independent positive prognostic factor, whereas symptomatic brain lesions (HR = 2.702, CI [0.030; 7.086], p = 0.032) and extracerebral progression within 4 weeks prior to SRS (HR = 4.759, CI [1.148; 19.730], p < 0.001) were found to be negative prognostic factors for LC (Table 2).
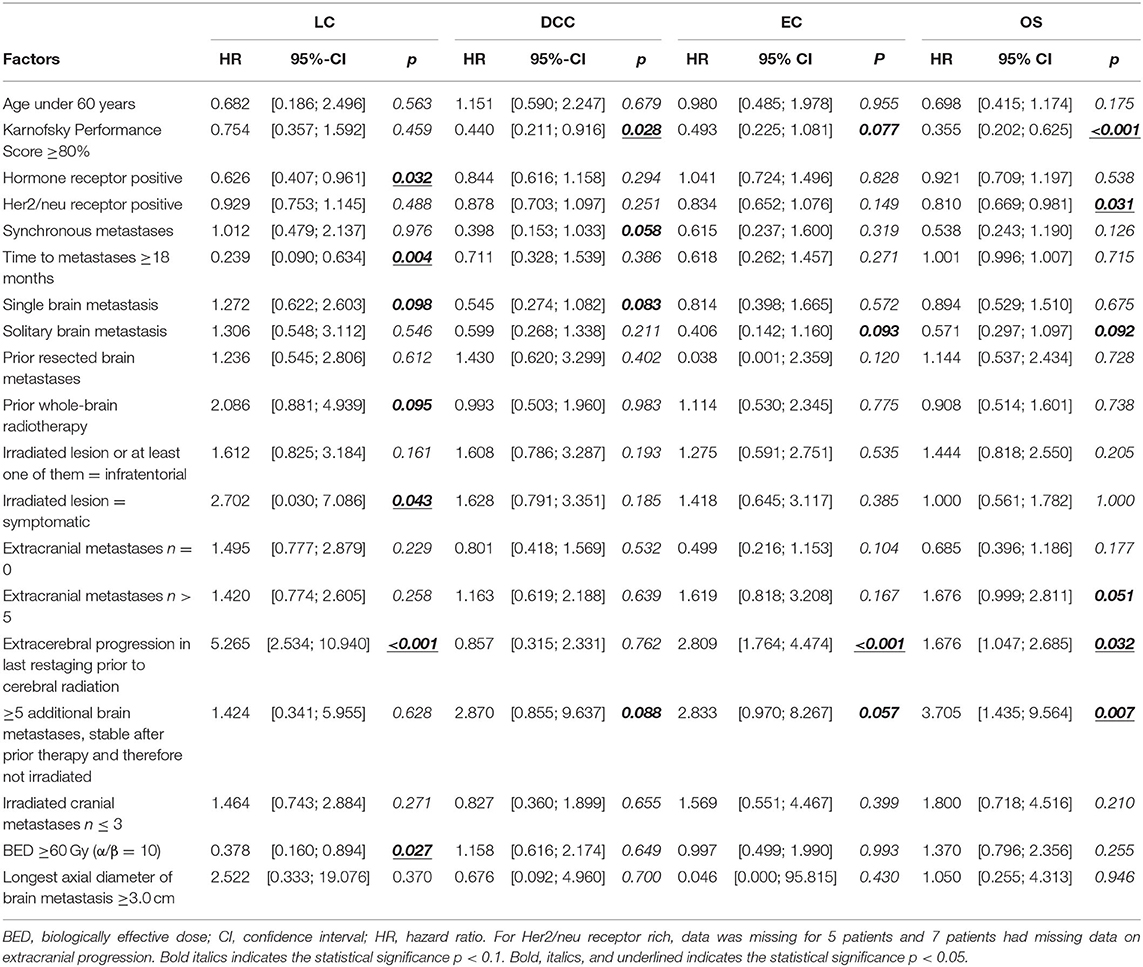
Table 6. Univariate analysis of prognostic factors influencing local control (LC), distant cranial control (DCC), extracranial control (EC), and overall survival (OS).
Distant Intracranial Control
Forty out of 95 patients (42.1%) were diagnosed with cerebral progression distant to the SRS lesion during follow-up. One- and two-year DCC rates were 65.3 and 36.7%. KPS (HR = 0.440, CI [0.211; 0.916], p = 0.028) was revealed as a significant favorable prognostic factor in univariate analysis (Table 6), with synchronous diagnosis of metastases (HR = 0.398, CI [0.153; 1.033] p = 0.058) and single brain metastasis (HR = 0.545, CI [0.274; 1.082], p = 0.083) at borderline significance level. If patients had presence of ≥5 additional brain metastases, which were stable form prior therapy and therefore not irradiated, it was found to be a borderline significant negative factor associated with worse DCC (HR = 2.870, CI [0.855; 9.637], p = 0.088). After adjusting for potential confounding variables on multivariate analysis, none of the aforementioned factors remained significant (Table 2).
Extracranial Control
During follow-up, 31 of 88 patients developed extracranial progression (35.2%). Estimated 1- and 2-year EC rates were 57.5 and 46.5%.
Extracerebral progression within 4 weeks prior to SRS (HR = 2.809, CI [1.764; 4.474], p < 0.001) was identified as an independent prognostic factor for further extracerebral progression after SRS (Table 2).
Overall Survival
Sixty patients (62.1%) died during follow-up time. One- and two-year OS were 60.9 and 37.8%, respectively. Univariate analysis revealed a KPS ≥80% (HR = 0.355, CI [0.202; 0.625], p < 0.001) and Her2/neu positivity (HR = 0.810, CI [0.669; 0.981], p = 0.031) as significant factors for superior OS, with a solitary brain metastasis (HR = 0.571, CI [0.297; 1.097], p = 0.092) at borderline significance level (Table 6). Five or more not irradiated brain metastases (HR = 3.705, CI [1.435; 9.564], p = 0.007) were significantly associated with inferior OS, with extracranial metastases n > 5 (HR = 1.676, CI [0.999; 2.811], p = 0.051) and extracerebral progression in last restaging prior to cerebral radiation (HR = 1.676, CI [1.047; 2.685], p = 0.032) at borderline significance level. In multivariate analysis, a KPS ≥80% (HR = 0.355, CI [0.202; 0.625], p < 0.001) and Her2/neu positivity (HR = 0.810, CI [0.669; 0.974], p = 0.027) were independently associated with improved OS (Table 2), with extracranial progression at borderline significance level (HR = 1.538, CI [0.949; 2.492], p = 0.080).
Validation of Nine Different Prognostic Grading Indexes
Two out of nine tested prognostic grading indexes shown in Table 1 provided a reliable ranking of survival groups according to their significant c-index, namely, the bGPA (c-index 0.631; 95% CI, 0.514–0.748; p = 0.037) and the mod-bGPA (c-index 0.662; 95% CI, 0.547–0.777; p = 0.010). Kaplan–Meier curves, median overall survival, and estimates of 1- and 2-year OS are shown in Figures 1, 2. The other, unsuccessfully tested prognostic scores had insignificant c-indexes, namely, the original GPA (c-index 0.531; 95% CI, 0.407–0.655; p = 0.615), the u-bGPA (c-index 0.583; 95% CI, 0.460–0.705; p = 0.188), the BSBM (c-index 0.579; 95% CI, 0.462–0.696; p = 0.197), the RPA (c-index 0.470; 95% CI, 0.351–0.590; p = 0.629), the SIR (c-index 0.566; 95% CI, 0.447–0.686; p = 0.279), the PSS (c-index 0.620; 95% CI, 0.502–0.793; p = 0.055), and the mRPA (c-index 0.512; 95% CI, 0.394–0.631; p = 0.845).
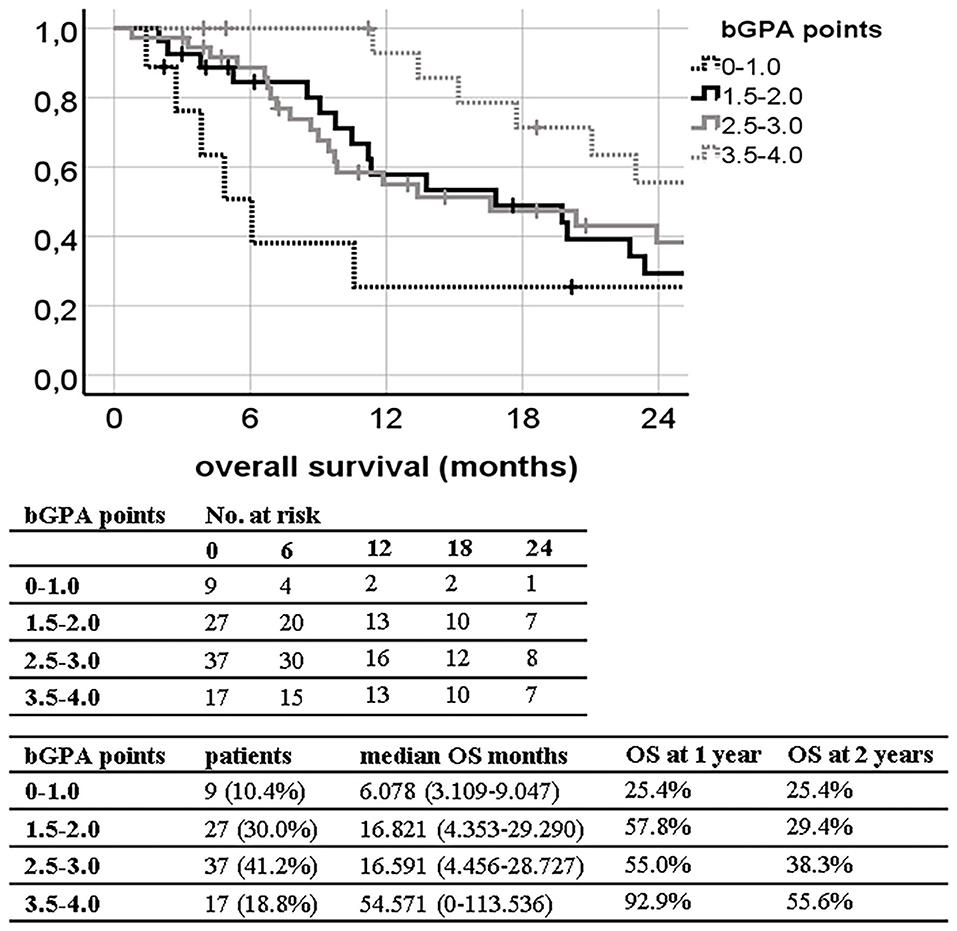
Figure 1. Kaplan–Meier curves for overall survival (OS) divided by the breast graded prognostic assessment (bGPA) in our patient population (log-rank p = 0.030; concordance index 0.631; 95% CI, 0.514–0.748; p = 0.037) with median OS and 1- and 2-year OS estimates.
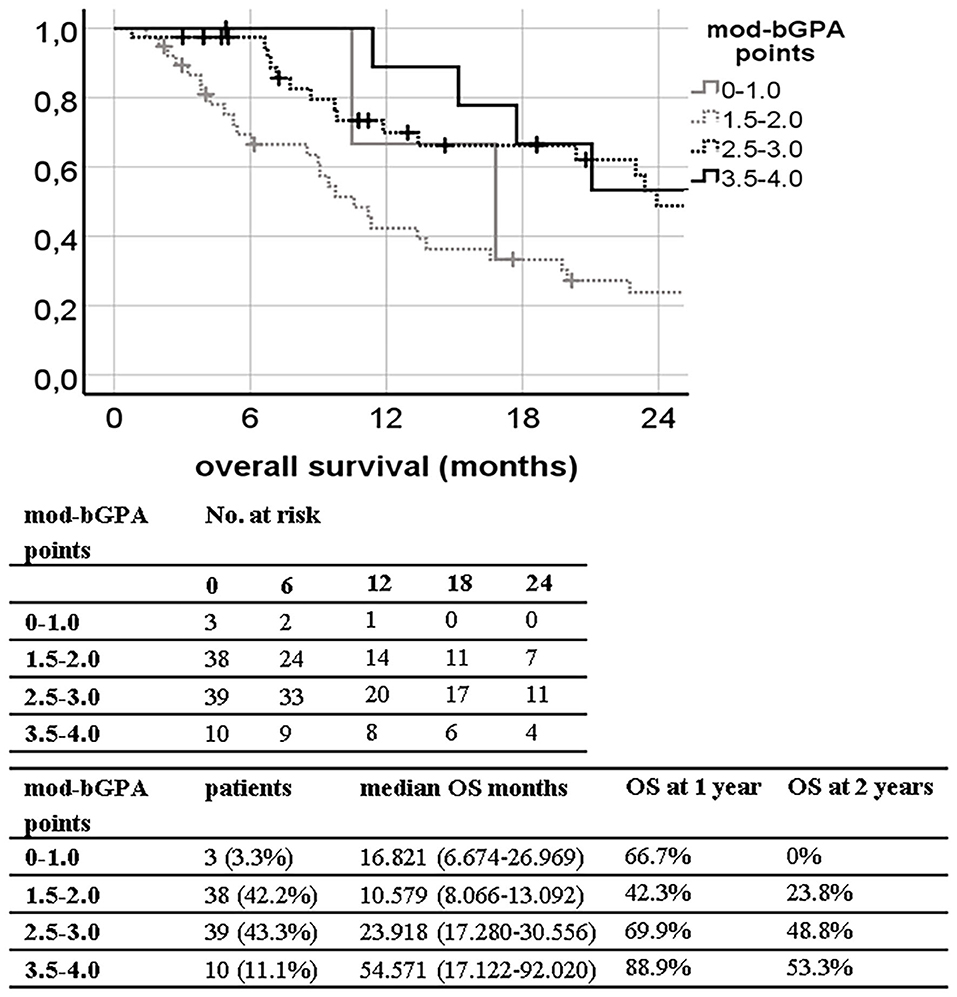
Figure 2. Kaplan–Meier curves for overall survival (OS) divided by the modified breast graded prognostic assessment (mod-bGPA) in our patient population (log-rank p = 0.003; concordance index 0.662; 95% CI, 0.547–0.777; p = 0.010) with median OS and 1- and 2-year OS estimates.
Breast Cancer Stereotactic Radiotherapy Score (bSRS)
The bSRS did significantly classify patients into three different prognostic subgroups for all outcome variables including LC, DCC, EC, and OS. The c-index was significant for OS (0.689; 95% CI, 0.577–0.802; p = 0.003), but not for LC, DCC, and EC. The c-index of the bSRS was superior to those of the bGPA or the mod-bGPA (0.689 vs. 0.631 vs. 0.662). The Kaplan–Meier curves and respective OS, LC, DCC, and EC estimates are shown in Figures 3–6.
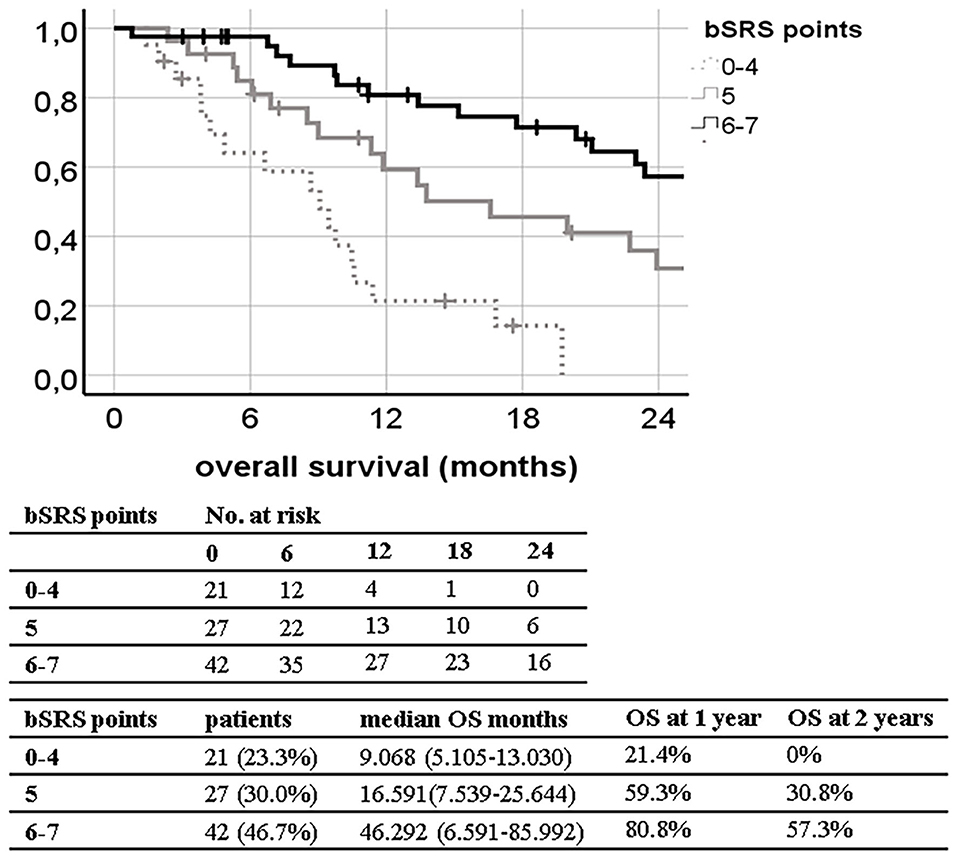
Figure 3. Kaplan–Meier curves for overall survival (OS; n = 90) divided by the breast scoring tool for stereotactic therapy (bSRS) in our patient population (log-rank p < 0.001; concordance index 0.689; 95% CI, 0.577–0.802; p = 0.003) with 1- and 2-year OS estimates.
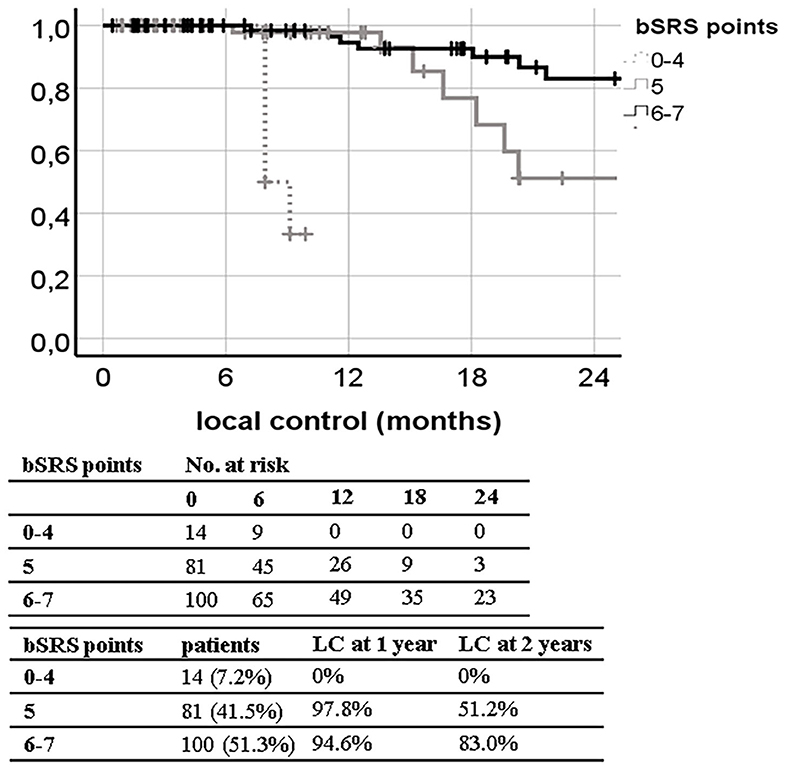
Figure 4. Kaplan–Meier curves for local control (LC; n = 195) of the irradiated lesions (n = 195) divided by the breast scoring tool for stereotactic therapy (bSRS) in our patient population (log-rank p < 0.001; concordance index 0.607; 95% CI, 0.462–0.751; p = 0.118) with 1- and 2-year LC estimates.
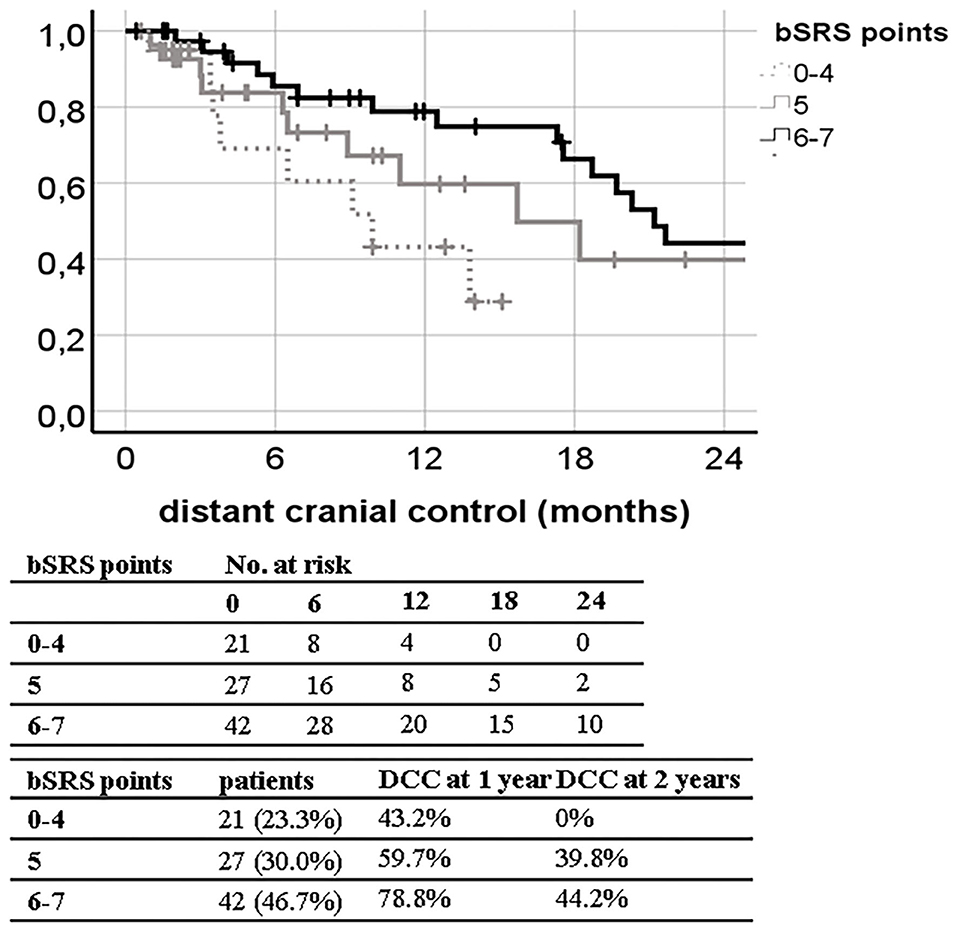
Figure 5. Kaplan–Meier curves for distant cranial control (DCC; n = 90) divided by the breast scoring tool for stereotactic therapy (bSRS) in our patient population (log-rank p = 0.036; concordance index 0.482; 95% CI, 0.359–0.604; p = 0.771) with 1- and 2-year DCC estimates.
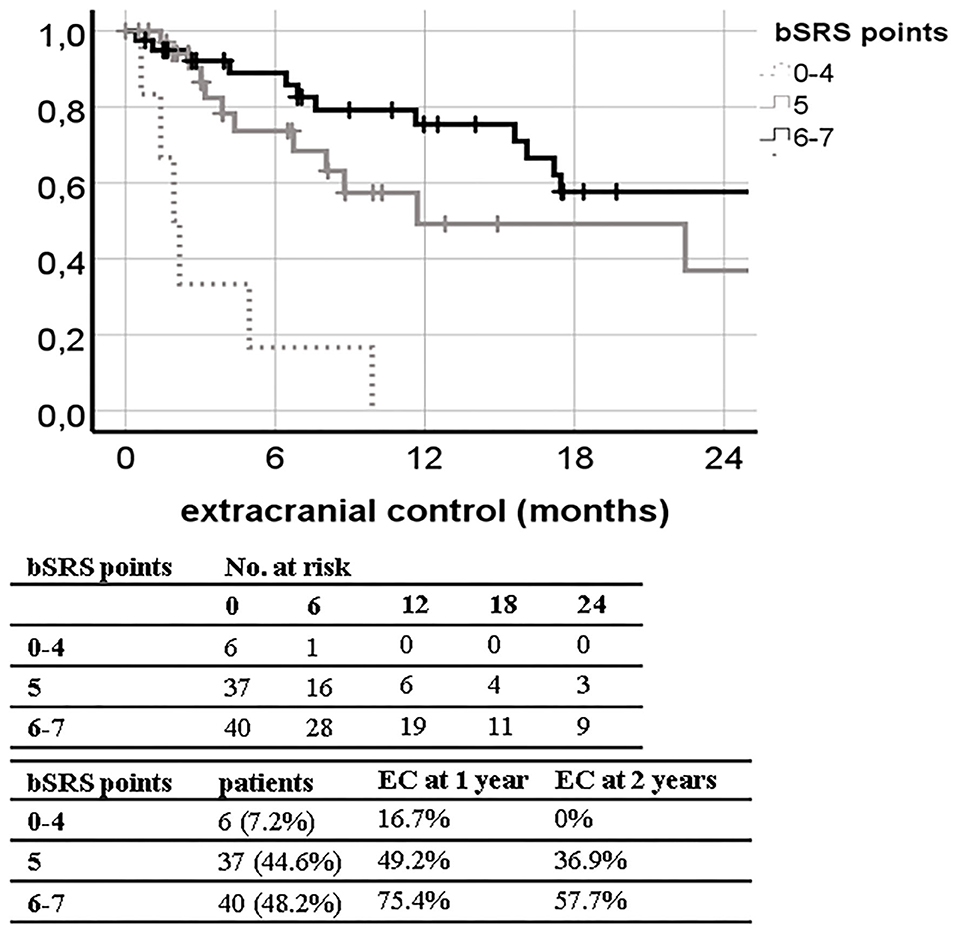
Figure 6. Kaplan–Meier curves for extracranial control (EC; n = 83) divided by the breast scoring tool for stereotactic therapy (bSRS) in our patient population (log-rank p < 0.001; concordance index 0.596; 95% CI, 0.465–0.728; p = 0.143) with 1- and 2-year EC estimates.
Discussion
In this retrospective study consisting of 95 breast cancer patients who received SRS for in total 203 brain metastases, two out of nine prognostic scoring indexes could be validated for OS assessment. Furthermore, we generated a new scoring index based on prior identified prognostic factors, which was superior for OS prognosis and was also applicable for LC, DCC, and EC assessment following radiosurgery.
Our study population matches with other studies on SRS for brain metastases in breast cancer patients in terms of epidemiology, radiotherapy protocols, LC, DCC, and OS (Table 7). The tendency of higher OS in the most recent studies suggests improved systemic therapy (6, 15).
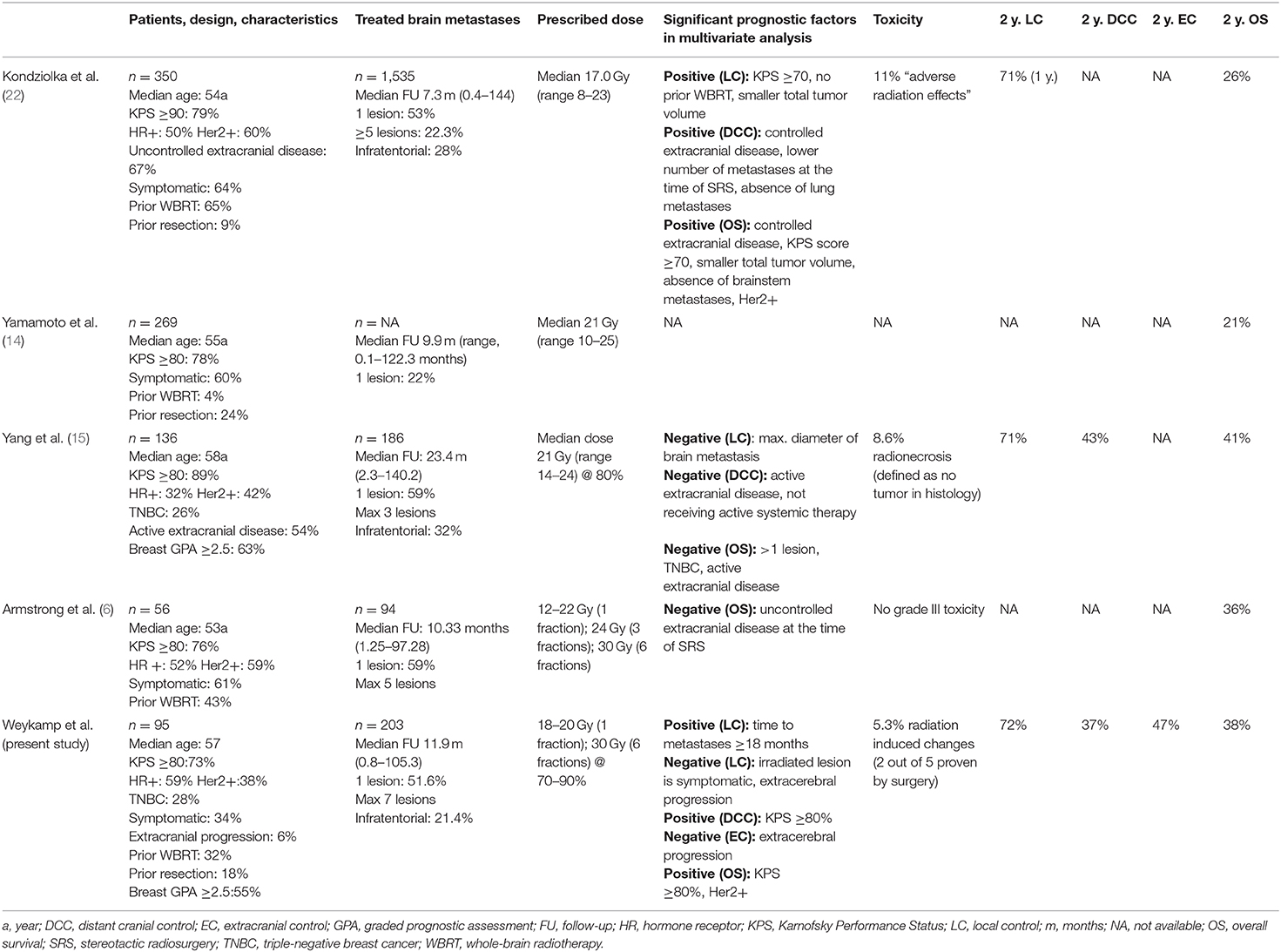
Table 7. Larger recent studies on radiosurgery only for brain metastases in female breast cancer patients.
Seven out of nine examined, well-established scoring indexes for radiotherapy of brain metastasis patients failed to yield significantly different prognostic groups in our study population, which may be caused by the different composition of the respective prognostic scoring indexes.
The PSS could not separate our patient cohort in different prognostic subgroups, although it was specifically designed for breast cancer patients with brain metastases receiving SRS (15). Nonetheless, it does not include the KPS (Table 1), even though this was reported to be one of the most important prognostic factors as shown previously (4, 5) and in our analysis. Thus, the KPS was also included in our bSRS. The mRPA, which also showed no prognostic relevance in our study cohort, was as well specifically designed for breast cancer patients with brain metastases receiving SRS. However, it is only a modification of the old RPA and therefore does not include the hormone or Her2/neu receptor status (14), which might explain the inferior results.
Only the bGPA and the mod-bGPA were confirmed as reliable prognostic tools in our study population as measured by the c-index (Figures 1, 2). A major reason for this finding might be that these two prognostic tools take into account the histological peculiarity of breast cancer patients, especially the Her2/neu receptor status (4, 5). Several studies have confirmed an independent positive impact of Her2/neu receptor positivity on OS in breast cancer patients after radiation of brain metastases (15, 22, 23). This was also demonstrated in our multivariate analysis (Table 2), which led to the inclusion of the Her2/neu receptor status into our bSRS. One of the reasons why Her2/neu receptor positivity improves OS is thought to be the anti Her2/neu therapy agents acting as a radiosensitizer (24).
In our analysis, both bGPA and mod-bGPA have their weakness in discriminating the second and third most favorable prognostic groups during the first 24 months of follow-up as illustrated in Figures 1, 2. This is probably caused by the fact that especially the most unfavorable prognostic group of the mod-bGPA is unproportionally small (n = 3; 3%; Figure 2) compared to the respective validation study by Subbiah et al. (5) (21%). However, this can be explained by the mod-bGPA being predominantly validated for WBRT. Only 11% of the validation study population was to receive SRS alone, since 42% of the patients had more than five brain metastases (5). In our SRS-only study population, 88% patients had a maximum of three brain metastases. Consequently, attributing a higher score to patients with only up to three brain metastases, like the mod-bGPA, grants artificial scoring points to nearly the entire study population. This results into a smaller subgroup of patients with only few total scoring points. Nonetheless, the mod-bGPA yields a higher c-index, indicating to be more suitable for differentiating prognostic OS subgroups than the bGPA (Figures 1, 2). The mod-bGPA includes a modified scoring system for age discrimination. Patients with older age are less disadvantaged than with the bGPA. This might improve prognostic reliability considering that older age could not be identified as an independent risk factor for inferior survival, neither in the present study nor in the recent comparable studies (6, 15, 22).
In 2014, Yamamoto et al. demonstrated that OS was non-inferior for patients treated with radiosurgery for 5–10 brain metastases compared to those who received SRS for only 2–4 cerebral metastases (25). This led to a change in treatment practice in the radiooncology community with an increasing number of centers offering radiosurgery for more than 4 brain metastases for selected patients. Hence, today the prognostic quality of several of the investigated scoring indexes, which are at least partly based on the number of brain metastases, like the mod-bGPA, is impaired. These indexes do no longer reflect current treatment approaches emphasizing again the necessity for a modern prognostic score. It remains unclear why the u-bGPA could not be successfully validated in our study population although being the latest bGPA scoring tool to date (12). Possibly, this is due to the fact that the prognostic factor “presence of extracranial metastases” was reintegrated into the u-bGPA (Table 1), like it was originally used in the old, not breast cancer-specific GPA (3). However, for the u-bGPA, Sperduto et al. only used the sole status of extracranial metastases without any quantitative measurement of the metastatic burden (e.g., dissemination) (12). Furthermore, no information on extracranial disease progression was provided, although it was described as an important independent factor for OS prognosis and is therefore also part of our bSRS (6, 15, 22). Since systemic therapies in breast cancer have improved during the last years, but often still do not penetrate the blood–brain barrier or even increase the risk of radiation-induced changes when combined with SRS, extracranial progression is a highly conflicting circumstance (26, 27). In general, patients with controlled extracranial disease may benefit the most from upfront definitive SRS alone, as shown in our study. However, in patients with progressive extracranial disease, SRS might offer the benefit of minimal systemic treatment interruption compared to WBRT and hereby enabling medical oncologists to continuously pursue optimal extracranial disease control with systemic treatments.
Our developed bSRS index consists of well-known prognostic factors for contemporary patients including the KPS, the Her2/neu status, and the status of extracranial progression as discussed above. The bSRS index could successfully divide patients into three significantly different subgroups in terms of LC, DCC, EC, and OS altogether. However, the c-index was only found to be significant for OS, and not for LC, DCC, and EC. This might be due to the main limitations of the presented study, namely, its retrospective and single-center design, leading to a rather small sample size. Furthermore, extracranial progression was much less frequent in the present study (6%) compared to other studies in the field with up to 67% (15, 22). This circumstance reflects a more conservative utilization of SRS in our patient cohort and thus hinders the development of an all-encompassing prognostic index, since extracranial progression was the only independent factor, both negatively influencing LC and EC to be identified (Table 2). Nonetheless, the bSRS was superior in differentiating prognostic OS subgroups compared to all other indexes as indicated by the higher c-index and the properly separated Kaplan–Meier curves (Figures 1–3), since it reflects the latest knowledge of prognostic OS factors in treatment of limited brain metastases in breast cancer patients, namely, KPS, Her2/neu positivity, and extracranial control (Tables 1, 7).
Conclusion
This retrospective single-center study could validate the bGPA and mod-bGPA as prognostic tools for OS in 95 breast cancer patients receiving SRS for in total 203 brain metastases. Furthermore, we developed the bSRS, a modern risk score for assessing not only OS but also LC, DCC, and EC following radiosurgery for breast cancer patients. Larger studies or post-hoc analyses of trials with a higher proportion of extracranial progressive patients are required to externally validate our generated score index.
Data Availability Statement
The datasets generated for this study are available on request to the corresponding author.
Ethics Statement
The studies involving human participants were reviewed and approved by Heidelberg University ethics committee on April 12th, 2018 (#S-172/2018). Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author Contributions
FW carried out the data collection, performed the statistical analysis, and drafted the manuscript. RE, LK, KS, TF, PH, SR, and NA helped with data collection as well as figure and table preparation. RE, FW, LK, KS, NA, and JH-R were involved in patient treatment. TD and AS contributed to the gynecological knowledge of the manuscript and were involved in pre-radiotherapy treatment. JH-R and JD participated in the study design and helped to draft the manuscript. All the authors were responsible for data interpretation, participated in manuscript revisions, and approved the final manuscript.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Tsukada Y, Fouad A, Pickren JW, Lane WW. Central nervous system metastasis from breast carcinoma autopsy study. Cancer. (1983) 52:2349–54. doi: 10.1002/1097-0142(19831215)52:12<2349::AID-CNCR2820521231>3.0.CO;2-B
2. Ou D, Cao L, Xu C, Kirova Y, Chen JY. Upfront brain radiotherapy may improve survival for unfavorable prognostic breast cancer brain metastasis patients with Breast-GPA 0-2.0. Breast J. (2019) 25:1134–42. doi: 10.1111/tbj.13426
3. Sperduto P, Sneed P, Bhatt A, Schwer A, Fiveash J, Chiang V, et al. A multi-institutional validation study of a new prognostic index (graded prognostic assessment, GPA) for patients with brain metastases. Int J Radiat Oncol Biol Phys. (2008) 72:S51. doi: 10.1016/j.ijrobp.2008.06.881
4. Sperduto PW, Kased N, Roberge D, Xu Z, Shanley R, Luo X, et al. Effect of tumor subtype on survival and the graded prognostic assessment for patients with breast cancer and brain metastases. Int J Radiat Oncol Biol Phys. (2012) 82:2111–7. doi: 10.1016/j.ijrobp.2011.02.027
5. Subbiah IM, Lei X, Weinberg JS, Sulman EP, Chavez-MacGregor M, Tripathy D, et al. Validation and development of a modified breast graded prognostic assessment as a tool for survival in patients with breast cancer and brain metastases. J Clin Oncol. (2015) 33:2239–45. doi: 10.1200/JCO.2014.58.8517
6. Armstrong K, Ward J, Dunne M, Rock L, Westrup J, Mascott CR, et al. Linac-based radiosurgery for patients with brain oligometastases from a breast primary, in the Trastuzumab era-impact of tumor phenotype and prescribed SRS dose. Front Oncol. (2019) 9:377. doi: 10.3389/fonc.2019.00377
7. Coia LR. The role of radiation therapy in the treatment of brain metastases. Int J Radiat Oncol Biol Phys. (1992) 23:229–38. doi: 10.1016/0360-3016(92)90567-2
8. Murray KJ, Scott C, Greenberg HM, Emami B, Seider M, Vora NL, et al. A randomized phase III study of accelerated hyperfractionation versus standard in patients with unresected brain metastases: a report of the Radiation Therapy Oncology Group (RTOG) 9104. Int J Radiat Oncol Biol Phys. (1997) 39:571–4. doi: 10.1016/S0360-3016(97)00341-6
9. Komarnicky LT, Phillips TL, Martz K, Asbell S, Isaacson S, Urtasun R. A randomized phase III protocol for the evaluation of misonidazole combined with radiation in the treatment of patients with brain metastases (RTOG-7916). Int J Radiat Oncol Biol Phys. (1991) 20:53–8. doi: 10.1016/0360-3016(91)90137-S
10. Phillips TL, Scott CB, Leibel SA, Rotman M, Weigensberg IJ. Results of a randomized comparison of radiotherapy and bromodeoxyuridine with radiotherapy alone for brain metastases: report of RTOG trial 89-05. Int J Radiat Oncol Biol Phys. (1995) 33:339–48. doi: 10.1016/0360-3016(95)00168-X
11. Andrews DW, Scott CB, Sperduto PW, Flanders AE, Gaspar LE, Schell MC, et al. Whole brain radiation therapy with or without stereotactic radiosurgery boost for patients with one to three brain metastases: phase III results of the RTOG 9508 randomised trial. Lancet. (2004) 363:1665–72. doi: 10.1016/S0140-6736(04)16250-8
12. Sperduto PW, Mesko S, Li J, Cagney D, Aizer A, Lin NU, et al. Beyond an updated graded prognostic assessment (breast GPA): a prognostic index and trends in treatment and survival in breast cancer brain metastases from 1985 to today. Int J Radiat Oncol Biol Phys. (2020) 107:334–43. doi: 10.1016/j.ijrobp.2020.01.051
13. Gaspar L, Scott C, Rotman M, Asbell S, Phillips T, Wasserman T, et al. Recursive partitioning analysis (RPA) of prognostic factors in three radiation therapy oncology group (RTOG) brain metastases trials. Int J Radiat Oncol Biol Phys. (1997) 37:745–51. doi: 10.1016/S0360-3016(96)00619-0
14. Yamamoto M, Kawabe T, Higuchi Y, Sato Y, Barfod BE, Kasuya H, et al. Validity of three recently proposed prognostic grading indexes for breast cancer patients with radiosurgically treated brain metastases. Int J Radiat Oncol Biol Phys. (2012) 84:1110–5. doi: 10.1016/j.ijrobp.2012.02.040
15. Yang TJ, Oh JH, Folkert MR, Gupta G, Shi W, Zhang Z, et al. Outcomes and prognostic factors in women with 1 to 3 breast cancer brain metastases treated with definitive stereotactic radiosurgery. Int J Radiat Oncol Biol Phys. (2014) 90:518–25. doi: 10.1016/j.ijrobp.2014.06.063
16. Weltman E, Salvajoli JV, Brandt RA, de Morais Hanriot R, Prisco FE, Cruz JC, et al. Radiosurgery for brain metastases: a score index for predicting prognosis. Int J Radiat Oncol Biol Phys. (2000) 46:1155–61. doi: 10.1016/S0360-3016(99)00549-0
17. Lorenzoni J, Devriendt D, Massager N, David P, Ruíz S, Vanderlinden B, et al. Radiosurgery for treatment of brain metastases: estimation of patient eligibility using three stratification systems. Int J Radiat Oncol Biol Phys. (2004) 60:218–24. doi: 10.1016/j.ijrobp.2004.02.017
18. Wilson T, Robinson T, MacFarlane C, Spencer T, Herbert C, Wade L, et al. Treating brain metastases from breast cancer: outcomes after stereotactic radiosurgery. Clin Oncol. (2020) 32:390–6. doi: 10.1016/j.clon.2020.02.007
19. Kocher M, Wittig A, Piroth MD, Treuer H, Seegenschmiedt H, Ruge M, et al. Stereotactic radiosurgery for treatment of brain metastases. Strahlenther Onkol. (2014) 190:521–32. doi: 10.1007/s00066-014-0648-7
20. Soffietti R, Abacioglu U, Baumert B, Combs SE, Kinhult S, Kros JM, et al. Diagnosis and treatment of brain metastases from solid tumors: guidelines from the European Association of Neuro-Oncology (EANO). Neuro Oncol. (2017) 19:162–74. doi: 10.1093/neuonc/now241
21. Park C, Papiez L, Zhang S, Story M, Timmerman RD. Universal survival curve and single fraction equivalent dose: useful tools in understanding potency of ablative radiotherapy. Int J Radiat Oncol Biol Phys. (2008) 70:847–52. doi: 10.1016/j.ijrobp.2007.10.059
22. Kondziolka D, Kano H, Harrison GL, Yang H-c, Liew DN, Niranjan A, et al. Stereotactic radiosurgery as primary and salvage treatment for brain metastases from breast cancer. J Neurosurg. (2011) 114:792–800. doi: 10.3171/2010.8.JNS10461
23. Shenker RF, Hughes RT, McTyre ER, Lanier C, Lo H-W, Metheny-Barlow L, et al. Potential prognostic markers for survival and neurologic death in patients with breast cancer brain metastases who receive upfront SRS alone. J Radiosurg SBRT. (2018) 5:277. doi: 10.1016/j.ijrobp.2018.07.926
24. Liang K, Lu Y, Jin W, Ang KK, Milas L, Fan Z. Sensitization of breast cancer cells to radiation by trastuzumab. Mol Cancer Ther. (2003) 2:1113−20.
25. Yamamoto M, Serizawa T, Shuto T, Akabane A, Higuchi Y, Kawagishi J, et al. Stereotactic radiosurgery for patients with multiple brain metastases (JLGK0901): a multi-institutional prospective observational study. Lancet Oncol. (2014) 15:387–95. doi: 10.1016/S1470-2045(14)70221-9
26. Chamberlain MC, Baik CS, Gadi VK, Bhatia S, Chow LQM. Systemic therapy of brain metastases: non–small cell lung cancer, breast cancer, and melanoma. Neuro Oncol. (2016) 19:i1–24. doi: 10.1093/neuonc/now197
Keywords: stereotactic radiosurgery, breast cancer, brain metastases, prognostic tool, breast graded prognostic assessment, prognostic grading index, overall survival
Citation: Weykamp F, El Shafie RA, König L, Seidensaal K, Forster T, Arians N, Regnery S, Hoegen P, Deutsch TM, Schneeweiss A, Debus J and Hörner-Rieber J (2020) Validation of Nine Different Prognostic Grading Indexes for Radiosurgery of Brain Metastases in Breast Cancer Patients and Development of an All-Encompassing Prognostic Tool. Front. Oncol. 10:1557. doi: 10.3389/fonc.2020.01557
Received: 30 May 2020; Accepted: 20 July 2020;
Published: 02 September 2020.
Edited by:
Brian Timothy Collins, Georgetown University, School of Medicine, United StatesReviewed by:
Young Kwok, University of Maryland Medical Center, United StatesElvira V. Grigorieva, Institute of Molecular Biology and Biophysics (RAS), Russia
Copyright © 2020 Weykamp, El Shafie, König, Seidensaal, Forster, Arians, Regnery, Hoegen, Deutsch, Schneeweiss, Debus and Hörner-Rieber. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Juliane Hörner-Rieber, anVsaWFuZS5ob2VybmVyLXJpZWJlckBtZWQudW5pLWhlaWRlbGJlcmcuZGU=