 Axel S. Merseburger
Axel S. Merseburger Götz Geiges2
Götz Geiges2- 1Department of Urology, University Hospital Schleswig-Holstein, Lübeck, Germany
- 2Arztpraxis für Urologie, Berlin, Germany
- 3Urologie Bayenthal, Köln, Germany
- 4Department of Internal Medicine I, University Hospital St. Poelten, Karl Landsteiner, University of Health Sciences, St. Poelten, Austria
Lipegfilgrastim is a long-acting glycopegylated granulocyte-colony stimulating factor (G-CSF) approved for the management of chemotherapy-induced neutropenia. In general, there is little information on the use of any G-CSFs specifically in patients with urological malignancies receiving chemotherapy. This report combines information from two prospective non-interventional studies on the prophylactic use of lipegfilgrastim in urological cancer patients receiving chemotherapy in the real-world setting. Data were derived from two phase IV studies (NADIR and LEOS) with similar protocols conducted in nine European countries. Analysis included 228 patients (142 prostate, 50 testicular, 27 bladder, and 9 other urological cancers). Chemotherapy-induced febrile neutropenia risk was classified as high (43.0%), intermediate (49.1%), or low (7.5%). Lipegfilgrastim was administered as primary (n=180, 78.9%) or secondary (n=29, 12.7%) prophylaxis. The incidence of febrile neutropenia over all chemotherapy cycles (n=998) and first cycles (n=228) for which lipegfilgrastim was administered for prophylaxis was 2.6% and 1.3%, respectively. Corresponding results for Grade 3/4 neutropenia were 2.2% and 0.9%, respectively. Adverse drug reactions occurred in 24 patients (10.5%): those in more than one patient were bone pain (n=6, 2.6%) and pyrexia (n=3, 1.3%). The use of lipegfilgrastim for the prophylaxis of chemotherapy-induced neutropenia was effective and well tolerated in patients with urological malignancies in the real-world setting.
Introduction
Chemotherapy-induced neutropenia is a common, and the most serious, hematological adverse event (AE) in cancer patients treated with myelosuppressive chemotherapies (1, 2). It frequently results in chemotherapy-dose delay or reduction, which can reduce dose intensity sufficiently to compromise optimal treatment response and survival (1, 3). Fever is frequently the first symptom of infection in cancer patients with chemotherapy-induced neutropenia and patients exhibiting febrile neutropenia usually require aggressive treatment including systemic antimicrobial treatment that necessitates hospitalization (1). Risk factors for the development of febrile neutropenia include intensive chemotherapy regimens and patient-related factors such as advanced age, advanced disease stage, previous episodes of febrile neutropenia, and comorbid conditions (4, 5).
Recombinant N-methionyl human granulocyte-colony stimulating factors (r-metHuG-CSFs, hereafter G-CSFs) are effective agents in cancer patients, reducing the duration and incidence of chemotherapy-induced neutropenia and febrile neutropenia by stimulating the release of neutrophils and neutrophil proliferation from bone marrow (6, 7). G-CSFs should be instituted for the prophylactic prevention of febrile neutropenia in high-risk patients (≥20% risk), and those at intermediate risk (10–20%) in the presence of other factors such as advanced age, advanced disease, previous febrile neutropenia, and no antimicrobial prophylaxis according to current treatment guidelines (4, 5, 8, 9).
G-CSFs have undergone considerable development and refinement since their initial introduction more than 25 years ago. The first agent to become available, filgrastim, has a relatively short half-life, which necessitated repeated daily subcutaneous administration for a mean of 10–11 days (10, 11) and up to 14 days per chemotherapy cycle (6, 7) to provide adequate absolute neutrophil count (ANC) recovery in clinical trials. However, a recent review of real-world observational studies showed that the mean duration of filgrastim treatment was considerably shorter at 3.7–7.5 days (12). This, combined with a delay in starting filgrastim in clinical practice, appears to contribute to reduced efficacy (13–17). The half-life of filgrastim was prolonged sufficiently by pegylation to allow the effective administration of a fixed dose of pegfilgrastim once per chemotherapy cycle (18). Single-dose pegfilgrastim was as effective as filgrastim administered daily for 10–14 days per cycle for prophylaxis of febrile neutropenia according to meta-analyses of randomized controlled trials (16, 17, 19, 20). However, observational studies suggest pegfilgrastim is more effective for the prevention of severe neutropenia and febrile neutropenia than filgrastim in a real-world setting (14, 21–23) and more convenient to administer.
Lipegfilgrastim (Lonquex®, Teva Pharmaceuticals Industries Ltd, Petach Tikva, Israel) is approved by the European Medicines Agency for the management of chemotherapy-induced neutropenia (24). It is a glycopegylated G-CSF with a prolonged half-life compared with the same dose of pegfilgrastim and produces a more sustained ANC increase (25–27). Lipegfilgrastim was at least as effective and as well tolerated compared to the same dose of pegfilgrastim in a phase III clinical trial among breast cancer patients receiving doxorubicin/docetaxel (28); subsequent analysis of secondary endpoints revealed a favorable response with lipegfilgrastim for some endpoints (e.g. time to ANC recovery, incidence of severe neutropenia, depth of ANC nadir) (26, 29). Glycopegylation as applied for lipegfilgrastim is the most specific pegylation method available to date, selectively adding one molecule of methoxyPEG (mPEG) to a sugar-activated threonine (threonine134) in filgrastim. In addition to this defined glycopegylation pattern, the position of the methoxypegylation site is also worthy of mention and could be the basis for hypothesis generation, as one particular aspect of the PEG modification in lipegfilgrastim is shielding the protein from enzymatic degradation and protection from recognition by the immune system. A centrally positioned mPEG-chain, as in lipegfilgrastim, might be favorable over an N-terminal-positioned PEG-chain as in pegfilgrastim (26).
There are no published reports on the effectiveness or safety of lipegfilgrastim specifically in patients with urological malignancies such as prostate, testicular, kidney, or bladder cancer. Patients with testicular cancer are usually young and are treated with highly myelosuppressive chemotherapy regimens where the goal is to cure the disease and, consequently, it is highly important to maintain dose intensity. Many cisplatin-based chemotherapy regimens for testicular cancer have a high risk, e.g., VelP (vinblastine, ifosfamide, cisplatin), VIP (etoposide, ifosfamide, cisplatin), BEP (bleomycin, etoposide, cisplatin), TIP (paclitaxel, ifosfamide, cisplatin) (30–33), or intermediate risk for febrile neutropenia, e.g., etoposide/cisplatin (34). Dose-dense MVAC (methotrexate, vinblastine, cyclophosphamide, cisplatin) in bladder cancer (35) presents a high risk for febrile neutropenia. Cabazitaxel plus prednisone presents an intermediate risk for febrile neutropenia in castration-resistant prostate cancer (36). Many of the patients with an intermediate risk of developing febrile neutropenia have additional factors that increase their risk, e.g. advanced age and comorbidities, making them candidates for G-CSF treatment. Here, we report pooled data from two non-interventional studies of lipegfilgrastim conducted in urological cancer patients with chemotherapy-induced neutropenia.
Methods
Data were derived from two (NADIR and LEOS) prospective, multicenter, phase IV, observational cohort studies with similar protocols, which were conducted from 8 January 2014 to 16 January 2017 in nine European countries (Austria, Belgium, Czech Republic, Germany, Italy, Poland, Slovakia, Spain, and The Netherlands). Neither study had any influence on an individual’s course of treatment. The study protocols were approved by ethical review boards at all their respective study centers and written informed consent was obtained from patients prior to inclusion. The studies followed the principles of the Declaration of Helsinki and guidelines of the International Conference on Harmonization of Good Clinical Practice. Full details of the methods and results of NADIR have been published for all 2,489 evaluable patients with various cancers (37). Interim results of the LEOS study have been reported for 621 patients with various cancers (38).
Patients and Treatment
Patients were male or female adults (≥18 years) with solid urological tumors receiving cytotoxic chemotherapy in whom their treating physician had decided to institute lipegfilgrastim for primary or secondary prophylaxis of neutropenia. Pregnant or lactating women were excluded.
The treating physician determined the cancer therapy appropriate for each patient, which followed the standard clinical practice for the relevant country. Lipegfilgrastim 6 mg was administered subcutaneously approximately 24 h after cytotoxic chemotherapy and continued for up to six cycles according to standard clinical practice and within approved marketing authorization (37).
Assessments
The following baseline demographic and clinical characteristics were recorded during screening: age, gender, height, weight, ethnicity, Eastern Cooperative Oncology Group (ECOG) performance status score, primary disease/tumor history, nutritional deficiency, details of previous and current chemotherapy, history of febrile neutropenia, concurrent diseases and medications, and blood counts. Baseline individual patient-related risk factors for febrile neutropenia (4) and intended use of lipegfilgrastim (primary or secondary prophylaxis) were determined. Patients were followed from initiation of lipegfilgrastim until 6–8 weeks after the last dose of lipegfilgrastim. Efficacy endpoints included incidence of severe (Grade 3/4) neutropenia, febrile neutropenia, use of antimicrobial agents, hospitalization, and chemotherapy dose modifications.
Safety
AEs and adverse drug reactions (ADRs) potentially related to lipegfilgrastim (yes/no) were coded by Medical Dictionary for Regulatory Affairs v20.0 and graded by National Cancer Institute Common Terminology Criteria for Adverse Events v4.03. Serious AEs and serious ADRs were reported in an expedited manner and coded/graded in the same manner. Highly prevalent chemotherapy-derived AEs (e.g., nausea, vomiting) were excluded from being recorded in one study (LEOS).
Statistics
Data are reported using descriptive statistics with continuous variables as mean ± standard deviation (SD) and median (range), and different categories of discrete variables as frequencies (%). Statistical analyses were performed using IBM® SPSS Statistics (v21.0 or higher) and StatXact® (v6.0), with missing values not being replaced or extrapolated.
Results
Demographics and Clinical Characteristics
The study included a total of 228 patients who had received ≥2 cycles of chemotherapy with at least one dose of lipegfilgrastim, which constituted the safety and efficacy populations. The demographic and clinical characteristics of the entire study population (N=228) as well as the three major subpopulations with prostate (n=142), testicular (n=50), and bladder (n=27) cancer are summarized in Table 1. Age and tumor stage were lower in the subpopulation with testicular cancer.
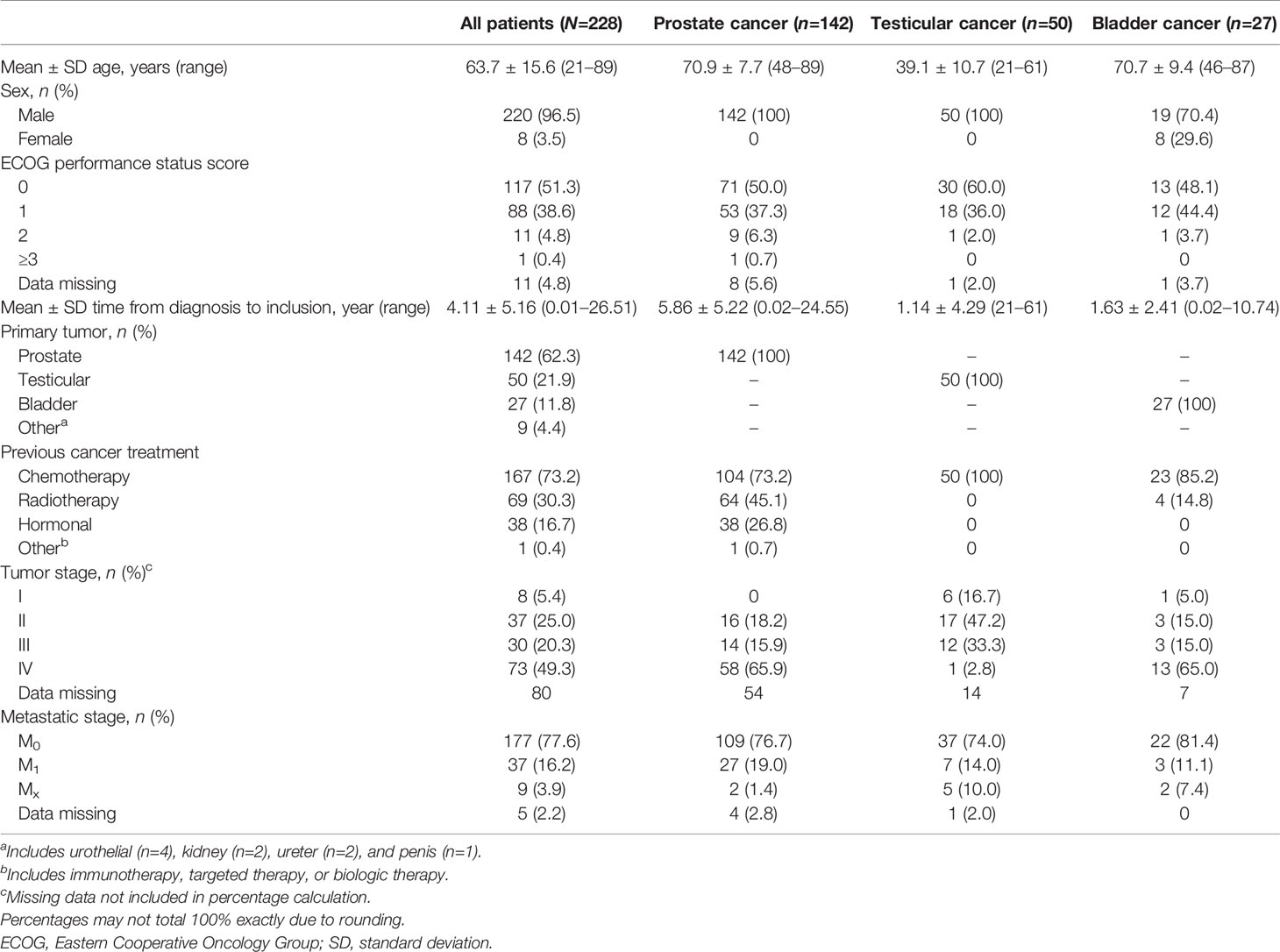
Table 1 Demographics and clinical characteristics.
Overall, ~60% of the patients had ≥1 comorbidity, with 25.6% having 1, 20.7% having 2, 10.1% having 3, and 2.6% having ≥4 concurrent comorbidities (Table 2). The mean number of comorbidities per patient was 1.09 ± 1.15, overall, but was considerably lower at 0.54 ± 0.73 in the subgroup with testicular cancer.
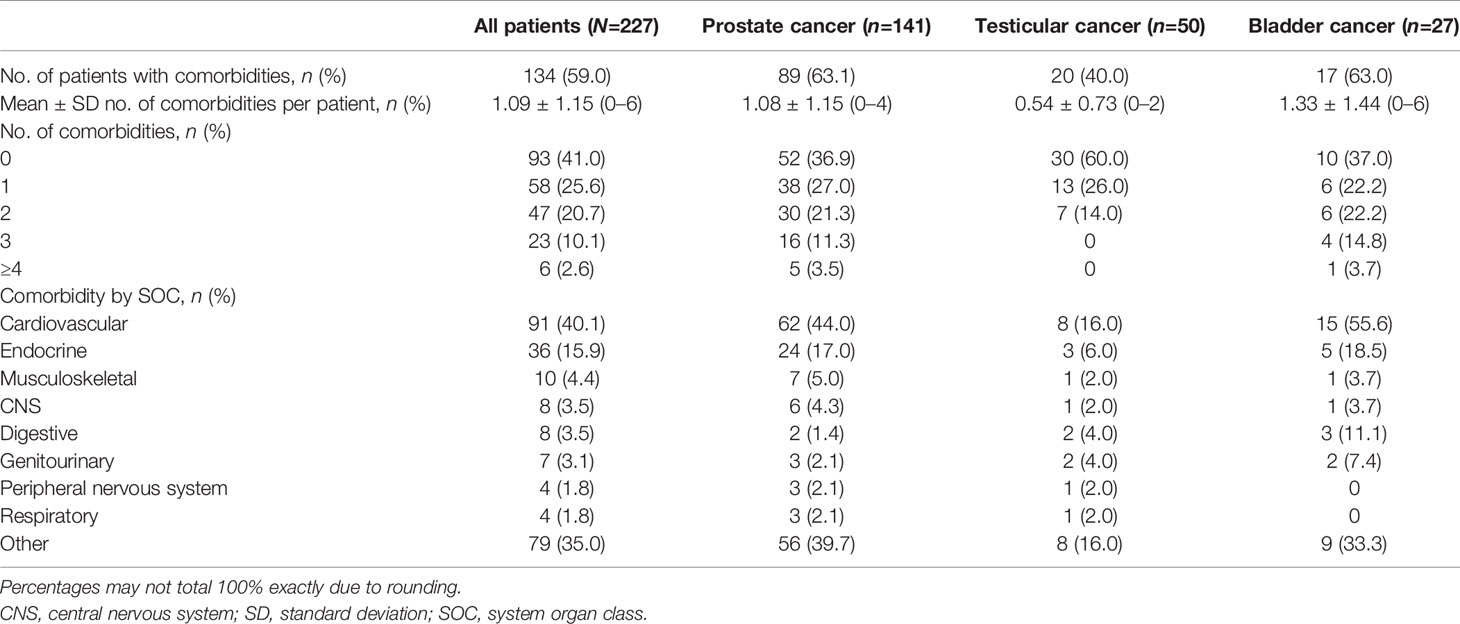
Table 2 Comorbidities.
Details of neutropenic risk, chemotherapies, and prophylaxis type are summarized in Table 3 (35, 36, 39–50). Overall, the mean number of patient-related risk factors for febrile neutropenia for the entire population was 1.36 ± 0.96; age >65 years (n=136, 59.6%), prior febrile neutropenia (n=116, 50.9%), and hemoglobin <12 g/dL (n=42, 18.4%) accounted for nearly all of the risk factors for febrile neutropenia. Chemotherapy-induced febrile neutropenia risk was intermediate (49.1%) or high (43.0%) in nearly all patients, with 7.5% having low risk. The chemotherapy setting was usually palliative (58.3%) or metastatic (18.4%), which would appear to be related to the high prevalence of patients with prostate cancer in the total cohort. The subpopulation with testicular cancer had a lower mean number of risk factors for febrile neutropenia (0.40 ± 0.61), more frequently had a high risk of chemotherapy febrile neutropenia (64.0%), and more frequently had a curative (26.0%), adjuvant (20.0%), or adjuvant/induction setting (24.0%) relative to palliative (22.0%) or metastatic settings (8.0%). Lipegfilgrastim was administered as primary prophylaxis in 180 patients (78.9%) and secondary prophylaxis in 29 (12.7%), with missing data in 19 (8.3%): there was a similar distribution across the three cancer subpopulations.
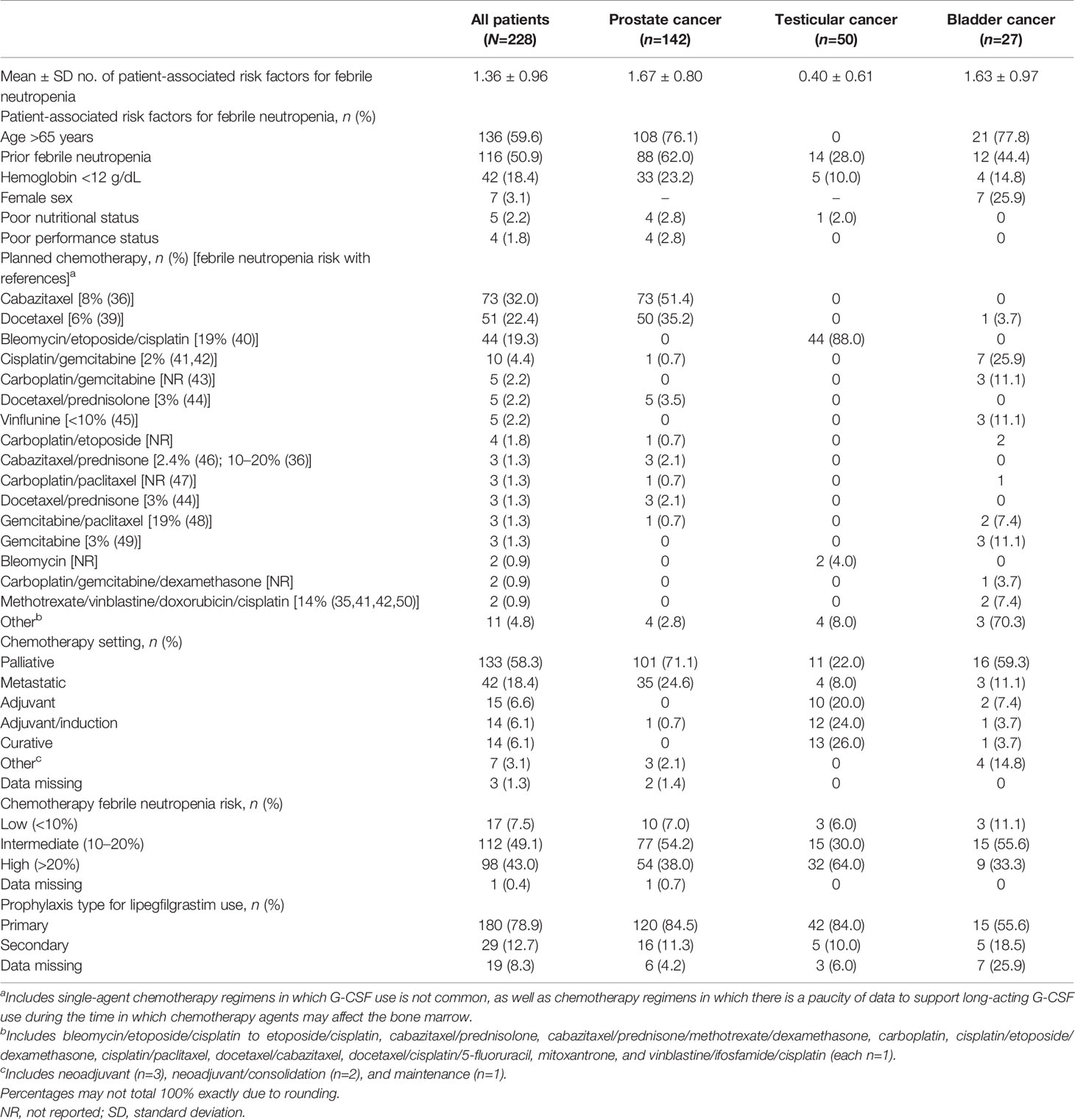
Table 3 Neutropenic risk, chemotherapies, and prophylaxis type.
Effectiveness
The incidence of febrile neutropenia over all cycles (n=998) and first cycles (n=228) that lipegfilgrastim was administered for prophylaxis was 2.6% and 1.3%, respectively (Table 4). The incidence of febrile neutropenia over all cycles and first cycles, respectively, was lower among those who received primary prophylaxis (1.7% and 0.6%) compared to those who received secondary prophylaxis (6.9% and 3.4%). The incidence of Grade 3/4 neutropenia over all cycles and first cycles of lipegfilgrastim was 2.2% and 1.3%, respectively, with lower incidences during primary prophylaxis (2.2% and 1.1%, respectively) compared to secondary prophylaxis (3.4% and 3.4%, respectively).

Table 4 Incidence of febrile neutropenia and neutropenia over all cycles and in the first cycle according to intention of lipegfilgrastim treatment.
Anti-infective drug use was evaluable over 834 of 998 cycles (83.8%) during which lipegfilgrastim was administered as prophylaxis. Anti-infective agents were used in 15 patients (6.6%) overall, including 11 (6.1%) during primary prophylaxis and four (13.8%) during secondary prophylaxis. The route of anti-infective drug administration was oral (n=11) or intravenous (n=4). The reasons for anti-infective drug use were prophylaxis (n=7), cystitis (n=1), fever without neutropenia (n=1), hematuria (n=1), pharyngitis (n=1), pharyngo-laryngitis (n=1), and unknown (n=3). No antimycotic agents were used.
Safety
Fifty ADRs (12.5%) occurred in 24 patients (10.5%). The most frequent ADRs (occurring in >1% of patients) were bone pain (n=6, 2.6%) and pyrexia (n=3, 1.3%). The full list of ADRs is reported in Table 5. Lipegfilgrastim was discontinued because of an ADR in one patient (0.4%). Fourteen serious ADRs (6.1%) were recorded in nine patients (3.9%). The most frequent serious ADRs (occurring in >1 patient) were fever and hematuria (each n=2, 0.9%). Overall, 12 serious AEs were categorized as deaths occurring in nine patients (3.95%), none of which were considered related to lipegfilgrastim. The events leading to death in the nine patients were reported as prostate cancer with metastasis and general physical health deterioration, sepsis, general physical health deterioration and neoplasm, general physical health deterioration and anemia, renal failure, Clostridium difficile colitis, neoplasm recurrence, pneumonia, and death.
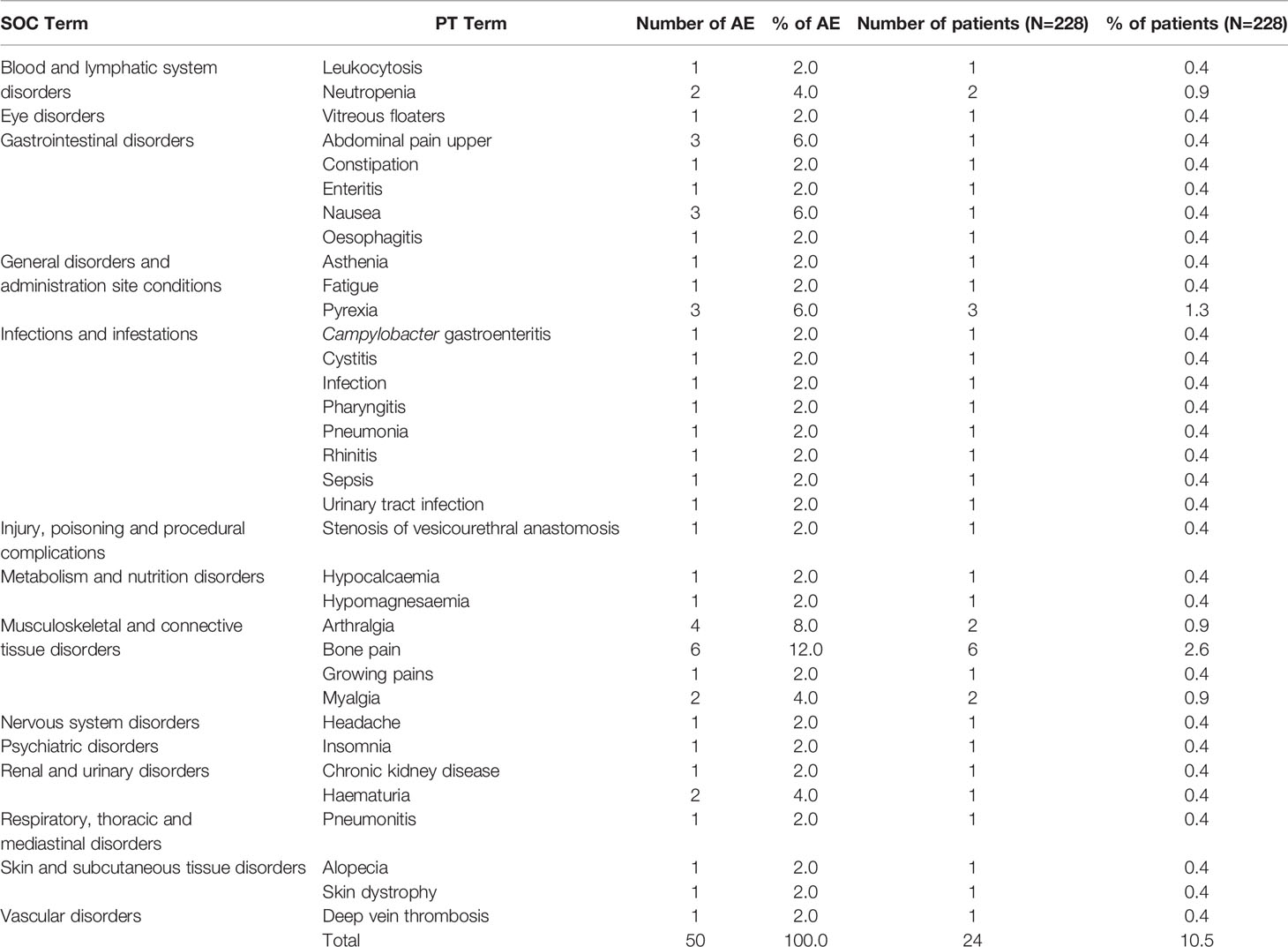
Table 5 Adverse reactions coded in System Organ Classes and Preferred Terms.
Discussion
The incidence of febrile neutropenia and Grade 3/4 neutropenia was 2.6% and 2.2%, respectively, over all cycles (n=998) of chemotherapy when lipegfilgrastim was administered as prophylaxis for neutropenia in a cohort of 228 patients with various urological malignancies (predominantly prostate, testicular, and bladder cancers). The corresponding incidence of febrile neutropenia and Grade 3/4 neutropenia was 1.3% and 0.9%, respectively, when analysis was restricted to the first cycle of chemotherapy. The incidence of febrile neutropenia was lower at 1.7% over all cycles, and even lower at 0.6% over the first cycle, when analysis was restricted to those patients who received lipegfilgrastim as primary prophylaxis. Final results from the full NADIR study using lipegfilgrastim in ~2500 patients with a range of cancers (predominantly breast cancer, lung cancer, and non-Hodgkin lymphoma) showed an almost identical incidence of febrile neutropenia (2.7%), while the incidence of Grade 3/4 neutropenia was considerably higher at 26.8% (37).
Lipegfilgrastim and pegfilgrastim (each 6 mg per cycle) have been compared directly in a prospective, randomized, controlled trial in 188 patients with breast cancer receiving up to 4 cycles of high-risk chemotherapy (28). None of the lipegfilgrastim recipients experienced febrile neutropenia during cycle 1 compared with 3.2% of pegfilgrastim recipients and the incidence of severe (Grade 4) neutropenia was 43.6% and 51.1% (p=0.3409), respectively, during cycle 1. Lipegfilgrastim 6 mg and placebo have also been compared in a prospective, randomized, controlled trial in ~375 patients with non-small cell lung cancer receiving up to 4 cycles of high-risk chemotherapy (51). The incidence of febrile neutropenia was 2.4% and 5.6% with lipegfilgrastim and placebo, respectively, during cycle 1.
The incidence of febrile neutropenia has been reported in a number of observational studies of pegfilgrastim: 3% (52), 4.4% (51, 52), 5.7% (53), and 5.6–6.3% (54). These observational studies rarely included any patients with urological malignancies and none reported results specifically in this subpopulation. Pegfilgrastim and filgrastim have been compared in many observational studies but such studies did not include patients with urological malignancies and several did not report the incidence of febrile neutropenia or severe neutropenia. Morrison and colleagues (21) reported a lower incidence of febrile neutropenia comparing pegfilgrastim and filgrastim in 2,863 US patients (4.7% vs 6.5%, p=0.044), and Almenar Cubells and colleagues (14) reported respective incidences for febrile neutropenia (6.7% vs 13.3%) and Grade 3/4 neutropenia (28.3% vs 49.3%) among 391 Spanish patients. A recent review of real-world comparative effectiveness studies found that the risk of febrile neutropenia was generally lower for prophylaxis with pegfilgrastim compared with that with short-acting G-CSFs (12).
It should be noted that 43.0% of the study population of patients with urological malignancies had a high risk (>20%) of febrile neutropenia from the chemotherapy compared to 49.1% with an intermediate risk (10–20%) and 7.5% with a low risk (<10%). Almost 80% of patients received lipegfilgrastim as primary prophylaxis. This would generally appear to be in line with current treatment guidelines which recommend primary G-CSF prophylaxis should be given to patients at high risk and to those at intermediate risk in the presence of other risk factors such as advanced age, advanced disease stage, prior febrile neutropenia, and/or concurrent comorbid conditions (4, 5, 8, 9). Most patients had additional risk factors [including age >65 years (59.6%), prior febrile neutropenia (50.9%), and hemoglobin >12 g/dL (18.4%)], at least one comorbidity (59.0%), and stage III/IV disease (69.6%), which would account for the use of lipegfilgrastim in those patients who received intermediate- or low-risk chemotherapy regimens.
With respect to safety, any grade ADRs occurred in 15.4% of patients, with bone pain (2.6%) and pyrexia (1.3%) occurring in >1% of patients. The ADR profile was similar to that previously reported for lipegfilgrastim in other cancers and compared to other long- and short-acting G-CSFs (28, 55).
The study was limited by the relatively low numbers of patients evaluated, although this is the first study to our knowledge that has specifically examined the efficacy and safety of lipegfilgrastim in patients with urological malignancies. The number of patients receiving lipegfilgrastim as secondary prophylaxis in the study was too low to allow any meaningful or reliable conclusions with respect to effectiveness. The study was, furthermore, limited by the relatively large proportion of patients with missing data. Another limitation of the investigation is the use of reduced Cabazitaxel dose to 20 mg/kg, which is mainly carried out in the USA. However, in real-life clinical scenarios Cabazitaxel is also often dose reduced so that there are fewer side effects whilst maintaining similar efficacy, as shown in recent publications (56).
Conclusion
In conclusion, lipegfilgrastim was effective and well tolerated for the prophylaxis of chemotherapy-induced neutropenia in patients with urological malignancies in the real-world setting. The use of lipegfilgrastim in these patients generally appeared to comply with current treatment recommendations and guidelines.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Author Contributions
All authors contributed to the article and approved the submitted version.
Funding
This work was sponsored by Teva Pharmaceuticals Europe B.V. (Amsterdam, The Netherlands).
Conflict of Interest
GG was employed by Arztpraxis für Urologie. AM declares receiving lecture or speaker fees, or honoraria from AstraZeneca, Bristol-Myers Squibb, Eisai, Ipsen, MSD, Merck Serono, Janssen, Takeda, Teva, Astellas, Novartis, Pfizer, and Roche; has acted as a consultant for AstraZeneca, Astellas, Bristol-Myers Squibb, Ipsen, Janssen, EUSAPharm, MSD, Merck Serono, Novartis, Takeda, Teva, Pfizer, and Roche; and has conducted research or clinical trials for AstraZeneca, Astellas, Bristol-Myers Squibb, Ipsen, Janssen, EUSAPharm, MSD, Merck Serono, Novartis, Takeda, Teva, Pfizer, and Roche.
The authors declare that this study received funding from Teva Pharmaceuticals Europe B.V. (Amsterdam, The Netherlands). The funder had the following involvement in the study: study design, conduct, and data analysis.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We would like to extend our thanks to Robert Scheuerlein (Scheuerlein Consulting, Leipzig, Germany) for editorial review and assistance. Thanks is also extended to Jacques Bruhwyler (ECSOR, Linkebeek, Belgium) for his expertise and assistance with the pooling and analysis of the data. Medical editorial assistance was provided by Peter Todd PhD (Tajut Ltd, Kaiapoi, New Zealand), which was funded by Teva (Amsterdam, The Netherlands).
References
1. Crawford J, Dale DC, Lyman GH. Chemotherapy-Induced Neutropenia: Risks, Consequences, and New Directions for its Management. Cancer (2004) 100:228–37. doi: 10.1002/cncr.11882
2. Lyman GH. Impact of Chemotherapy Dose Intensity on Cancer Patient Outcomes. J Natl Compr Canc Netw (2009) 7:99–108. doi: 10.6004/jnccn.2009.0009
3. Bonadonna G, Valagussa P. Dose-Response Effect of Adjuvant Chemotherapy in Breast Cancer. N Engl J Med (1981) 304:10–5. doi: 10.1056/NEJM198101013040103
4. Aapro MS, Bohlius J, Cameron DA, Dal Lago L, Donnelly JP, Kearney N, et al. European Organisation for Research and Treatment of Cancer. 2010 Update of EORTC Guidelines for the Use of Granulocyte-Colony Stimulating Factor to Reduce the Incidence of Chemotherapy-Induced Febrile Neutropenia in Adult Patients With Lymphoproliferative Disorders and Solid Tumours. Eur J Cancer (2011) 47:8–32. doi: 10.1016/j.ejca.2010.10.013
5. National Comprehensive Cancer Network (NCCN). NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines): Hematopoietic Growth Factors, Version 2.2019 (2019). Available at: https://www.nccn.org/professionals/physician_gls/pdf/growthfactors.pdf.
6. Crawford J, Ozer H, Stoller R, Johnson D, Lyman G, Tabbara I, et al. Reduction by Granulocyte Colony-Stimulating Factor of Fever and Neutropenia Induced by Chemotherapy in Patients With Small-Cell Lung Cancer. N Engl J Med (1991) 325:164–70. doi: 10.1056/NEJM199107183250305
7. Trillet-Lenoir V, Green J, Manegold C, Von Pawel J, Gatzemeier U, Lebeau B, et al. Recombinant Granulocyte Colony Stimulating Factor Reduces the Infectious Complications of Cytotoxic Chemotherapy. Eur J Cancer (1993) 29:319–24. doi: 10.1016/0959-8049(93)90376-Q
8. Crawford J, Caserta C, Roila F, ESMO Guidelines Working Group. Hematopoietic Growth Factors. ESMO Clinical Practice Guidelines for the Applications. Ann Oncol (2010) 21(Suppl 5):v248–51. doi: 10.1093/annonc/mdq195
9. Smith TJ, Bohlke K, Lyman GH, Carson KR, Crawford J, Cross SJ, et al. American Society of Clinical Oncology. Recommendations for the Use of WBC Growth Factors: American Society of Clinical Oncology Clinical Practice Guideline Update. J Clin Oncol (2015) 33:3199–212. doi: 10.1200/JCO.2015.62.3488
10. Holmes FA, O’Shaughnessy JA, Vukelja S, Jones SE, Shogan J, Savin M, et al. Blinded, Randomized, Multicenter Study to Evaluate Single Administration Pegfilgrastim Once Per Cycle Versus Daily Filgrastim as an Adjunct to Chemotherapy in Patients With High-Risk Stage II or Stage III/IV Breast Cancer. J Clin Oncol (2002) 20:727–31. doi: 10.1200/JCO.2002.20.3.727
11. Green MD, Koelbl H, Baselga J, Galid A, Guillem V, Gascon P, et al. International Pegfilgrastim 749 Study Group. A Randomized Double-Blind Multicenter Phase III Study of Fixed-Dose Single-Administration Pegfilgrastim Versus Daily Filgrastim in Patients Receiving Myelosuppressive Chemotherapy. Ann Oncol (2003) 14:29–35. doi: 10.1093/annonc/mdg019
12. Mitchell S, Li X, Woods M, Garcia J, Hebard-Massey K, Barron R, et al. Comparative Effectiveness of Granulocyte Colony-Stimulating Factors to Prevent Febrile Neutropenia and Related Complications in Cancer Patients in Clinical Practice: A Systematic Review. J Oncol Pharm Pract (2016) 22:702–16. doi: 10.1177/1078155215625459
13. Weycker D, Hackett J, Edelsberg JS, Oster G, Glass AG. Are Shorter Courses of Filgrastim Prophylaxis Associated With Increased Risk of Hospitalization? Ann Pharmacother (2006) 40:402–7. doi: 10.1345/aph.1G516
14. Almenar Cubells D, Bosch Roig C, Jiménez Orozco E, Álvarez R, Cuervo JM, Díaz Fernández N, et al. Learn II Study Group. Effectiveness of Daily Versus non-Daily Granulocyte Colony-Stimulating Factors in Patients With Solid Tumours Undergoing Chemotherapy: A Multivariate Analysis of Data From Current Practice. Eur J Cancer Care (Engl) (2013) 22:400–12. doi: 10.1111/ecc.12043
15. Wright JD, Neugut AI, Ananth CV, Lewin SN, Wilde ET, Lu YS, et al. Deviations From Guideline-Based Therapy for Febrile Neutropenia in Cancer Patients and Their Effect on Outcomes. JAMA Intern Med (2013) 173:559–68. doi: 10.1001/jamainternmed.2013.2921
16. Pfeil AM, Allcott K, Pettengell R, von Minckwitz G, Schwenkglenks M, Szabo Z. Efficacy, Effectiveness and Safety of Long-Acting Granulocyte Colony-Stimulating Factors for Prophylaxis of Chemotherapy-Induced Neutropenia in Patients With Cancer: A Systematic Review. Support Care Cancer (2015) 23:525–45. doi: 10.1007/s00520-014-2457-z
17. Wang L, Baser O, Kutikova L, Page JH, Barron R. The Impact of Primary Prophylaxis With Granulocyte Colony-Stimulating Factors on Febrile Neutropenia During Chemotherapy: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Support Care Cancer (2015) 23:3131–40. doi: 10.1007/s00520-015-2686-9
18. Yang BB, Kido A. Pharmacokinetics and Pharmacodynamics of Pegfilgrastim. Clin Pharmacokinet (2011) 50:295–306. doi: 10.2165/11586040-000000000-00000
19. Pinto L, Liu Z, Doan Q, Bernal M, Dubois R, Lyman G. Comparison of Pegfilgrastim With Filgrastim on Febrile Neutropenia, Grade IV Neutropenia and Bone Pain: A Meta-Analysis of Randomized Controlled Trials. Curr Med Res Opin (2007) 23:2283–95. doi: 10.1185/030079907X219599
20. Cooper KL, Madan J, Whyte S, Stevenson MD, Akehurst RL. Granulocyte Colony-Stimulating Factors for Febrile neutropenia prophylaxis Following Chemotherapy: Systematic Review and Meta-Analysis. BMC Cancer (2011) 11:404. doi: 10.1186/1471-2407-11-404
21. Morrison VA, Wong M, Hershman D, Campos LT, Ding B, Malin J. Observational Study of the Prevalence of Febrile neutropenia in Patients Who Received Filgrastim or Pegfilgrastim Associated With 3–4 Week Chemotherapy Regimens in Community Oncology Practices. J Manag Care Pharm (2007) 13:337–48. doi: 10.18553/jmcp.2007.13.4.337
22. Almenar D, Mayans J, Juan O, Bueno JM, Lopez JI, Frau A, et al. Pegfilgrastim and Daily Granulocyte Colony-Stimulating Factor: Patterns of Use and Neutropenia-Related Outcomes in Cancer Patients in Spain – Results of the LEARN Study. Eur J Cancer Care (Engl) (2009) 18:280–6. doi: 10.1111/j.1365-2354.2008.00959.x
23. Tan H, Tomic K, Hurley D, Daniel G, Barron R, Malin J. Comparative Effectiveness of Colony-Stimulating Factors for Febrile Neutropenia: A Retrospective Study. Curr Med Res Opin (2011) 27:79–86. doi: 10.1185/03007995.2010.536527
24. Guariglia R, Martorelli MC, Lerose R, Telesca D, Milella MR, Musto P. Lipegfilgrastim in the Management of Chemotherapy-Induced Neutropenia of Cancer Patients. Biologics (2016) 10:1–8. doi: 10.2147/BTT.S58597
25. Buchner A, Lammerich A, Abdolzade-Bavil A, Müller U, Bias P. Lipegfilgrastim: Pharmacodynamics and Pharmacokinetics for Body-Weight-Adjusted and 6 mg Fixed Doses in Two Randomized Studies in Healthy Volunteers. Curr Med Res Opin (2014) 30:2523–33. doi: 10.1185/03007995.2014.962131
26. Zündorf I, Dingermann T. Pegylation: A Well-Proven Strategy for the Improvement of Recombinant Drugs. Pharmazie (2014) 69:323–6.
27. Abdolzade-Bavil A, von Kerczek A, Cooksey BA, Kaufman T, Krasney PA, Pukac L, et al. Differential Sensitivity of Lipegfilgrastim and Pegfilgrastim to Neutrophil Elastase Correlates With Differences in Clinical Pharmacokinetic Profile. J Clin Pharmacol (2016) 56:186–94. doi: 10.1002/jcph.578
28. Bondarenko I, Gladkov OA, Elsaesser R, Buchner A, Bias P. Efficacy and Safety of Lipegfilgrastim Versus Pegfilgrastim: A Randomized, Multicenter, Active-Control Phase 3 Trial in Patients With Breast Cancer Receiving Doxorubicin/Docetaxel Chemotherapy. BMC Cancer (2013) 13:386. doi: 10.1186/1471-2407-13-386
29. Gladkov OA, Buchner A, Bias P, Müller U, Elsässer R. Chemotherapy-Associated Treatment Burden in Breast Cancer Patients Receiving Lipegfilgrastim or Pegfilgrastim: Secondary Efficacy Data From a Phase III Study. Support Care Cancer (2016) 24:395–400. doi: 10.1007/s00520-015-2803-9
30. Miller KD, Loehrer PJ, Gonin R, Einhorn LH. Salvage Chemotherapy With Vinblastine, Ifosfamide, and Cisplatin in Recurrent Seminoma. J Clin Oncol (1997) 15:1427–31. doi: 10.1200/JCO.1997.15.4.1427
31. Nichols CR, Catalano PJ, Crawford ED, Vogelzang NJ, Einhorn LH, Loehrer PJ. Randomized Comparison of Cisplatin and Etoposide and Either Bleomycin or Ifosfamide in Treatment of Advanced Disseminated Germ Cell Tumors: An Eastern Cooperative Oncology Group, Southwest Oncology Group, and Cancer and Leukemia Group B Study. J Clin Oncol (1998) 16:1287–93. doi: 10.1200/JCO.1998.16.4.1287
32. Kondagunta GV, Bacik J, Donadio A, Bajorin D, Marion S, Sheinfeld J, et al. Combination of Paclitaxel, Ifosfamide, and Cisplatin is an Effective Second-Line Therapy for Patients With Relapsed Testicular Germ Cell Tumors. J Clin Oncol (2005) 23:6549–55. doi: 10.1200/JCO.2005.19.638
33. Motzer RJ, Nichols CJ, Margolin KA, Bacik J, Richardson PG, Vogelzang NJ, et al. Phase III Randomized Trial of Conventional-Dose Chemotherapy With or Without High-Dose Chemotherapy and Autologous Hematopoietic Stem-Cell Rescue as First-Line Treatment for Patients With Poor-Prognosis Metastatic Germ Cell Tumors. J Clin Oncol (2007) 25:247–56. doi: 10.1200/JCO.2005.05.4528
34. Motzer RJ, Sheinfeld J, Mazumdar M, Bajorin DF, Bosl GJ, Herr H, et al. Etoposide and Cisplatin Adjuvant Therapy for Patients With Pathologic Stage II Germ Cell Tumors. J Clin Oncol (1995) 13:2700–4. doi: 10.1200/JCO.1995.13.11.2700
35. Sternberg CN, de Mulder PH, Schornagel JH, Théodore C, Fossa SD, van Oosterom AT, et al. European Organization for Research and Treatment of Cancer Genitourinary Tract Cancer Cooperative Group. Randomized Phase III Trial of High-Dose-Intensity Methotrexate, Vinblastine, Doxorubicin, and Cisplatin (MVAC) Chemotherapy and Recombinant Human Granulocyte Colony-Stimulating Factor Versus Classic MVAC in Advanced Urothelial Tract Tumors: European Organization for Research and Treatment of Cancer Protocol No. 30924. J Clin Oncol (2001) 19:2638–46. doi: 10.1200/JCO.2001.19.10.2638
36. de Bono JS, Oudard S, Ozguroglu M, Hansen S, Machiels JP, Kocak I, et al. Tropic Investigators. Prednisone Plus Cabazitaxel or Mitoxantrone for Metastatic Castration-Resistant Prostate Cancer Progressing After Docetaxel Treatment: A Randomised Open-Label Trial. Lancet (2010) 376:1147–54. doi: 10.1016/S0140-6736(10)61389-X
37. Fietz T, Lück A, Schulz H, Harde J, Losem C, Grebhardt S, et al. Prophylaxis of Chemotherapy-Induced Neutropenia and Febrile Neutropenia With Lipegfilgrastim in 2489 Cancer Patients: Final Results From the non-Interventional Study NADIR. Curr Med Res Opin (2019) 35:1127–38. doi: 10.1080/03007995.2018.1560200
38. Steger G, Pilcher P, Airoldi M, Mazza P, Fontaine C, Timmer Bonte J, et al. Poster Display Session: Breast Cancer - Early Stage, Locally Advanced & Metastatic, CNS Tumours, Developmental Therapeutics, Genitourinary Tumours - Prostate & non-Prostate, Palliative Care, Psycho-oncology, Public Health Policy, Sarcoma, Supportive Care. Ann Oncol (2018) 29(suppl_8):viii603–viii640.
39. Sweeney CJ, Chen YH, Carducci M, Liu G, Jarrard DF, Eisenberger M, et al. Chemohormonal Therapy in Metastatic Hormone-Sensitive Prostate Cancer. N Engl J Med (2015) 373:737–46. doi: 10.1056/NEJMoa1503747
40. Culine S, Kramar A, Théodore C, Geoffrois L, Chevreau C, Biron P, et al. Genito-Urinary Group of the French Federation of Cancer Centers Trial T93m. Randomized Trial Comparing Bleomycin/Etoposide/Cisplatin With Alternating Cisplatin/Cyclophosphamide/Doxorubicin and Vinblastine/Bleomycin Regimens of Chemotherapy for Patients With Intermediate- and Poor-Risk Metastatic Nonseminomatous Germ Cell Tumors: Genito-Urinary Group of the French Federation of Cancer Centers Trial T93mp. J Clin Oncol (2008) 26:421–7. doi: 10.1200/JCO.2007.13.8461
41. von der Maase H, Hansen SW, Roberts JT, Dogliotti L, Oliver T, Moore MJ, et al. Gemcitabine and Cisplatin Versus Methotrexate, Vinblastine, Doxorubicin, and Cisplatin in Advanced or Metastatic Bladder Cancer: Results of a Large, Randomized, Multinational, Multicenter, Phase III Study. J Clin Oncol (2000) 18:3068–77. doi: 10.1200/JCO.2000.18.17.3068
42. von der Maase H, Sengelov L, Roberts JT, Ricci S, Dogliotti L, Oliver T, et al. Long-Term Survival Results of a Randomized Trial Comparing Gemcitabine Plus Cisplatin, With Methotrexate, Vinblastine, Doxorubicin, Plus Cisplatin in Patients With Bladder Cancer. J Clin Oncol (2005) 23:4602–8. doi: 10.1200/JCO.2005.07.757
43. Dogliotti L, Cartenì G, Siena S, Bertetto O, Martoni A, Bono A, et al. Gemcitabine Plus Cisplatin Versus Gemcitabine Plus Carboplatin as First-Line Chemotherapy in Advanced Transitional Cell Carcinoma of the Urothelium: Results of a Randomized Phase 2 Trial. Eur Urol (2007) 52:134–41. doi: 10.1016/j.eururo.2006.12.029
44. Tannock IF, de Wit R, Berry WR, Horti J, Pluzanska A, Chi KN, et al. Tax 327 Investigators. Docetaxel Plus Prednisone or Mitoxantrone Plus Prednisone for Advanced Prostate Cancer. N Engl J Med (2004) 351:1502–12. doi: 10.1056/NEJMoa040720
45. Bellmunt J, Orsola A, Leow JJ, Wiegel T, De Santis M, Horwich A. Esmo Guidelines Working Group. Bladder Cancer: ESMO Practice Guidelines for Diagnosis, Treatment and Follow-Up. Ann Oncol (2014) 25(Suppl 3):iii40–8. doi: 10.1093/annonc/mdu223
46. Oudard S. TROPIC: Phase III Trial of Cabazitaxel for the Treatment of Metastatic Castration-Resistant Prostate Cancer. Future Oncol (2011) 7:497–506. doi: 10.2217/fon.11.23
47. Vaughn DJ, Manola J, Dreicer R, See W, Levitt R, Wilding G. Phase II Study of Paclitaxel Plus Carboplatin in Patients With Advanced Carcinoma of the Urothelium and Renal Dysfunction (E2896): A Trial of the Eastern Cooperative Oncology Group. Cancer (2002) 95:1022–7. doi: 10.1002/cncr.10782
48. Meluch AA, Greco FA, Burris HA3, O’Rourke T, Ortega G, Steis RG, et al. Paclitaxel and Gemcitabine Chemotherapy for Advanced Transitional-Cell Carcinoma of the Urothelial Tract: A Phase II Trial of the Minnie Pearl Cancer Research Network. J Clin Oncol (2001) 19:3018–24. doi: 10.1200/JCO.2001.19.12.3018
49. Stadler WM, Kuzel T, Roth B, Raghavan D, Dorr FA. Phase II Study of Single-Agent Gemcitabine in Previously Untreated Patients With Metastatic Urothelial Cancer. J Clin Oncol (1997) 15:3394–8. doi: 10.1200/JCO.1997.15.11.3394
50. Sternberg CN, Yagoda A, Scher HI, Watson RC, Herr HW, Morse MJ, et al. Methotrexate, Vinblastine, Doxorubicin, and Cisplatin for Advanced Transitional Cell Carcinoma of the Urothelium. Efficacy and Patterns of Response and Relapse. Cancer (1989) 64:2448–58. doi: 10.1002/1097-0142(19891215)64:12<2448::AID-CNCR2820641209>3.0.CO;2-7
52. Jurczak W, Kalinka-Warzocha E, Chmielowska E, Duchnowska R, Wojciechowska-Lampka E, Wieruszewska K. Multicentre, Prospective Observational Study of Pegfilgrastim Primary Prophylaxis in Patients At High Risk of Febrile Neutropenia in Poland: Profil Study. Contemp Oncol (Pozn) (2015) 19:214–9. doi: 10.5114/wo.2015.52657
53. Fiegl M, Steger GG, Studnicka M, Eisterer W, Jaeger C, Willenbacher W. Pegfilgrastim Prophylaxis in Patients At Different Levels of Risk for Chemotherapy-Associated Febrile Neutropenia: An Observational Study. Curr Med Res Opin (2013) 29:505–15. doi: 10.1185/03007995.2013.781018
54. Madry R, Poplawska L, Haslbauer F, Šafanda M, Ghizdavescu D, Benkovicova J, et al. Results of a Prospective Dose Intensity and Neutropenia Prophylaxis Evaluation Programme (DIEPP) in Cancer Patients At Risk of Febrile Neutropenia Due to Myelosuppressive Chemotherapy. Wien Klin Wochenschr (2016) 128:238–47. doi: 10.1007/s00508-015-0917-1
55. Volovat C, Bondarenko IM, Gladkov OA, Elsässer R, Buchner A, Bias P, et al. Randomized, Double-Blind, Placebo-Controlled, Multicenter Study of Lipegfilgrastim in Patients With non-Small Cell Lung Cancer Receiving Myelosuppressive Therapy. Springerplus (2015) 4:316. doi: 10.1186/s40064-015-1067-7
Keywords: lipegfilgrastim, prostate, testicular, bladder, cancer, neutropenia, efficacy and safety
Citation: Merseburger AS, Geiges G, Klier J, Wiesholzer M and Pichler P (2021) Pooled Analysis on the Effectiveness and Safety of Lipegfilgrastim in Patients With Urological Malignancies in the Real-World Setting. Front. Oncol. 11:655355. doi: 10.3389/fonc.2021.655355
Received: 18 January 2021; Accepted: 21 April 2021;
Published: 28 May 2021.
Edited by:
Viktor Grünwald, Universitätsklinikum Essen, GermanyReviewed by:
Kouji Izumi, Kanazawa University, JapanMehmet Asim Bilen, Emory University, United States
Thomas Hilser, Essen University Hospital, Germany
Copyright © 2021 Merseburger, Geiges, Klier, Wiesholzer and Pichler. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Axel S. Merseburger, YXhlbC5tZXJzZWJ1cmdlckB1a3NoLmRl