 Paul Sargos1*
Paul Sargos1* Mame Daro Faye2Manon Bacci1
Mame Daro Faye2Manon Bacci1 Stéphane Supiot3
Stéphane Supiot3 Igor Latorzeff4
Igor Latorzeff4 David Azria5
David Azria5 Tamim M. Niazi2Te Vuong2
Tamim M. Niazi2Te Vuong2 Véronique Vendrely6Renaud de Crevoisier7
Véronique Vendrely6Renaud de Crevoisier7- 1Department of Radiation Oncology, Institut Bergonié, Bordeaux Cedex, France
- 2Department of Radiation Oncology, Jewish General Hospital, Montreal, QC, Canada
- 3Department of Radiation Oncology, Institut de Cancérologie de l’Ouest, Saint-Herblain, France
- 4Department of Radiation Oncology, Clinique Pasteur, Toulouse, France
- 5Department of Radiation Oncology, Institut de Cancérologie de Montpellier, Montpellier, France
- 6Department of Radiation Oncology, Bordeaux University Hospital, Bordeaux, France
- 7Department of Radiation Oncology, Centre Eugene Marquis, Rennes, France
Introduction: Late gastro-intestinal toxicities (LGIT) secondary to pelvic radiotherapy (RT) are well described in the literature. LGIT are mainly related to rectal or ano-rectal irradiation; however, involvement of the anal canal (AC) in the occurrence of LGIT remains poorly described and understood.
Materials and Methods: The aim of this work was to explore the potential role of the AC in the development of LGIT after prostate irradiation and identify predictive factors that could be optimized in order to limit these toxicities. This narrative literature review was realized using the Pubmed database. We identified original articles published between June 1997 and July 2019, relating to LGIT after RT for localized prostate cancer and for which AC was identified independently. Articles defining the AC as part of an anorectal or rectal volume only were excluded.
Results: A history of abdominal surgery or cardio-vascular risk, anticoagulant or tobacco use, and the occurrence of acute GIT during RT increases the risk of LGIT. A dose-effect relationship was identified between dose to the AC and development of LGIT. Identification and contouring of the AC and adjacent anatomical structures (muscles or nerves) are justified to apply specific dose constraints. As a limitation, our review mainly considered on 3DCRT which is no longer the standard of care nowadays; we did not identify any reports in the literature using moderately hypofractionated RT for the prostate and AC specific dosimetry.
Conclusion: These results suggest that the AC may have an important role in the development of LGIT after pelvic RT for prostate cancer. The individualization of the AC during planning should be recommended in prospective studies.
Introduction
Gastrointestinal toxicities (GIT), acute or late (LGIT), can occur after radiotherapy (RT) for localized prostate cancer, altering the quality of life of up to 50% of patients (1, 2). These LGIT include gastrointestinal bleeding, painful bowel movements, increased stool frequency, diarrhea or mucous in stool, fecal urgency, incontinence, as well as abdominal pain (3–5). Matta et al. (6) recently reported that grade >2 LGIT occur in 2% to 26% of patients treated with conventional fractionation prostate RT (dose level between 70 and 80 Gy), whereas for moderately hypofractionated RT, the rate of grade >2 LGIT is lower than 6% (6). In the case of ultra hypofractionated prostate RT (over 6 Gy per fraction), grade >2 LGIT rates are between 0% and 4% (6). Thus, it appears that evolving RT techniques allow for a better tolerance of dose escalation treatment regimens.
LGIT are often thought to be related to irradiation of organs at risk (OARs), such as the rectum, the ano-rectal volume, and/or the small bowel. However, there is no clear correlation between irradiation of the anal canal (AC) alone and the development of LGIT (7). Indeed, the long-term effects of pelvic RT on the function of the rectum or the ano-rectum have been largely studied, with a specific focus on GIT (8–13). However, these studies did not identify the AC independently despite it being often included in a non-specific OAR volume (8–13). Pelvic irradiation could lead to certain toxicities, some of which could be specific to the AC (14, 15).
The CTCAE classification is a descriptive scale for the severity of symptoms, graded from 1 to 5, which could arise from any treatment. In its fourth version (v4.0) (14), toxicities described for the AC include anal fistulas, anal hemorrhage, mucositis, ulceration, necrosis, stenosis, and anal pain. However, symptoms related to fecal incontinence, diarrhea, and hemorrhoids are not directly attributed to irradiation of the AC, but rather to the GI structures in general (14). The same observation can be made in other classification systems used to describe radiation-related gastrointestinal toxicities, such as the Radiation Therapy Oncology Group/European Organization for Research and Treatment of cancer (RTOG/EORTC) (16–18) or the subjective-objective-management-analytic–late effects of normal tissues (SOMA-LENT) (8, 19–24). This prompted us to do a literature review to assess the individual contribution of AC irradiation on the incidence of LGIT after prostate RT.
The objectives of this narrative critical literature review were to explore if LGIT could be potentially related to irradiation of the AC in the context of prostate cancer RT. We sought to analyze the extent to which the AC is involved in the development of radiation-related LGIT, to bring to light different predictive factors for the occurrence of LGIT and to show a potential dose-effect relationship between dose to the AC and the development of LGIT. The overall goal is to optimize the care and quality of life of patients undergoing prostate RT.
Materials and Methods
Literature Search
This narrative literature review was realized using the Pubmed database. Articles published in any language between June 1997 and July 2019 were included. The PICO research question was “Is irradiation of the anal canal as an individual structure related to the development of LGIT in prostate cancer patients treated with radiotherapy” (P: prostate cancer patients treated with radiotherapy; I: irradiation of the anal canal as an individual volume; C: none; O: LGIT). Keywords for the search included « anal canal », « anorectal » « prostate », « Prostatic Neoplasms/radiotherapy », « gastrointestinal », « toxicity », « NTCP » and « probability », used separately or in combination. Bibliographic references cited within eligible articles could be used as well. Eligible articles were ranked and prioritized based on quality of the publication starting with randomized control trials (RCTs), then prospective studies, and finally retrospective studies, but given the limited number of articles found, they were all considered in this review.
Inclusion and Exclusion Criteria
All selected articles discussed on the RT of localized prostate cancer with or without pelvic lymph nodes irradiation. All cases were biopsy-proven adenocarcinoma of the prostate, localized (T1-T4) and non-metastatic. We selected the articles where LGIT were clearly cited as a primary or secondary objective of the study. GIT were defined as late when they occurred more than 6 months after the end of RT. Selected articles also had to contain an analysis of the toxicities related to the AC, defined as a specific OAR, meaning that articles evaluating LGIT on a rectal or ano-rectal volume only were out of the scope of our review. Exclusion criteria were: articles on acute toxicities only, late GIT not specifically related to the AC, i.e., not specifically describing AC-related symptoms and/or grade, articles that did not specify the AC as a separate OAR, articles on late GIT related to pelvic irradiation but for other cancer histologies, letters to the editors, commentaries, and abstracts.
Articles Selection
Sixty-three articles were identified using the above search method. One abstract, one editorial, and two letters were excluded. Thirty additional articles were excluded based on their titles. The abstracts of the 30 remaining articles were read independently by two authors and those not specifically related to the AC-related late GIT or the AC as an OAR were excluded, leaving a total of nine articles for further analysis. Bibliographic references cited in these nine papers are also cited when contributory to the discussion or for background information.
Results of the Literature Search
The majority of the articles from our literature search were on LGIT after prostate RT, however only nine articles were specifically on the AC and met all our inclusion and exclusion criteria (16, 17, 23, 25–30).
Impact of Anal Canal Irradiation on Rectorrhagia in the Context of Pelvic Radiotherapy
After treatment of prostate cancer with RT, the risk of grade ≥ 2 rectorrhagia specifically related to irradiation of the AC is between 5% and 10% (31, 32). Identification of clinical and dosimetric predictive factors related to GI bleeding after prostate RT has been the subject of many publications (16, 17, 19–24, 27, 28, 33). These studies looked at patients that were specifically treated to the prostate with three-dimensional conformal radiation therapy (3D-CRT), at doses between 64 and 78 Gy. The studies that specifically defined the AC as an OAR are presented in Table 1.
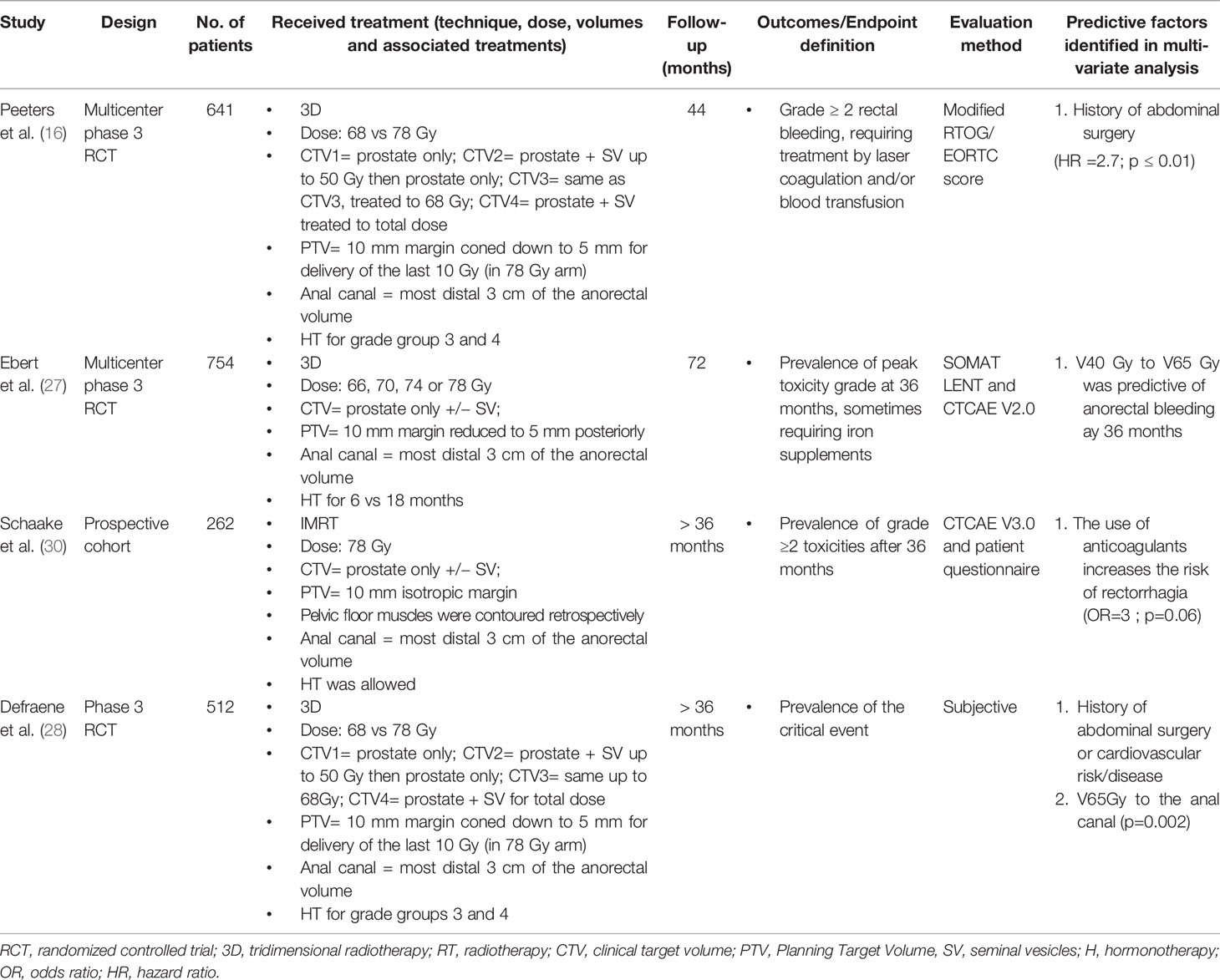
Table 1 Identification of predictive factors for rectorrhagia in patients with localized prostate cancer treated with pelvic radiotherapy.
Only one study, the TROG 03.04 RADAR trial that analyzed LGIT after prostate RT using the SOMA-LENT scale with a median follow-up of six years, showed the dose-effect relationship of moderate to high doses of RT to the AC (> 40 Gy) and rectorrhagia incidence at 36 months (27). In this study, V40 Gy to V65 Gy to the whole anorectum was predictive of anorectal bleeding whereas low-to-mid doses to the AC were predictive of rectorrhagia. Interestingly, the peak incidence of rectorrhagia attributed to the rectum peaked before 24 months whereas for the AC, it peaked at 36 months. Thus, the authors suggested an association of earlier bleeding with dose to the rectum and delayed bleeding with dose to the AC dose (27).
Peeters et al. (16) showed that rectorrhagia needing treatment correlated most strongly with anorectal V55–V65 Gy (p < 0.01), with the most significant parameter being V65 (p < 0.004). Interestingly, on multivariate analysis, rectal parameters were slightly less significant for rectorrhagia compared with the corresponding anorectal variables (16). Then, delineation of a separate AC subvolume in future prospective studies may help tease out the different contributions of the rectal and AC structures to late rectorrhagia (33, 34).
As for patient-related factors, it appears that a history of abdominal surgery (16, 19, 20, 28) increases the risks of rectorrhagia after pelvic irradiation. Peeters et al. (16) showed that RTOG/EORTC Grade ≥2 toxicities were significantly associated with low to intermediate dose anal parameters and anal Dmean. Importantly, adding the variables of abdominal surgery and pretreatment GI symptoms increased the level of significance of this association on multivariate analysis. The same authors showed that including a history of abdominal surgery to the Lyman Kutcher Burman (LKB) model, which also includes dose to the AC, improved its prediction capacity for late rectal bleeding (17). The TD50 (dose at which toxicity occurs in 50% of the population) was estimated at 81 Gy using the original LKB model. However, using their modified stratified model, TD50 was 85 Gy in patients without any past abdominal surgery history compared to 78 Gy for patients with a history of abdominal surgery (16, 17). These results were corroborated by Defraene et al. who also showed that cardiovascular history was predictive of LGIT (28).
Impact of Anal Canal Irradiation on Stool Frequency and Diarrhea in the Context of Pelvic Radiotherapy
The risk of developing grade ≥ 2 diarrhea and increased stool frequency after prostate RT varies between 4% and 19% (24). Table 2 summarizes the AC dosimetric data and patient-related factors that are predictive of increased stool frequency and diarrhea. The TROG 03.04 RADAR study, in which the AC was individually defined as an OAR, showed that low to moderate doses to the AC (4–38 Gy) were correlated with increased stool frequency (27). Interestingly, in another study, an increase in stool frequency was associated with dose to pelvic muscles such as the iliococcygeal muscle (V45) and the levator ani (V40) (30).
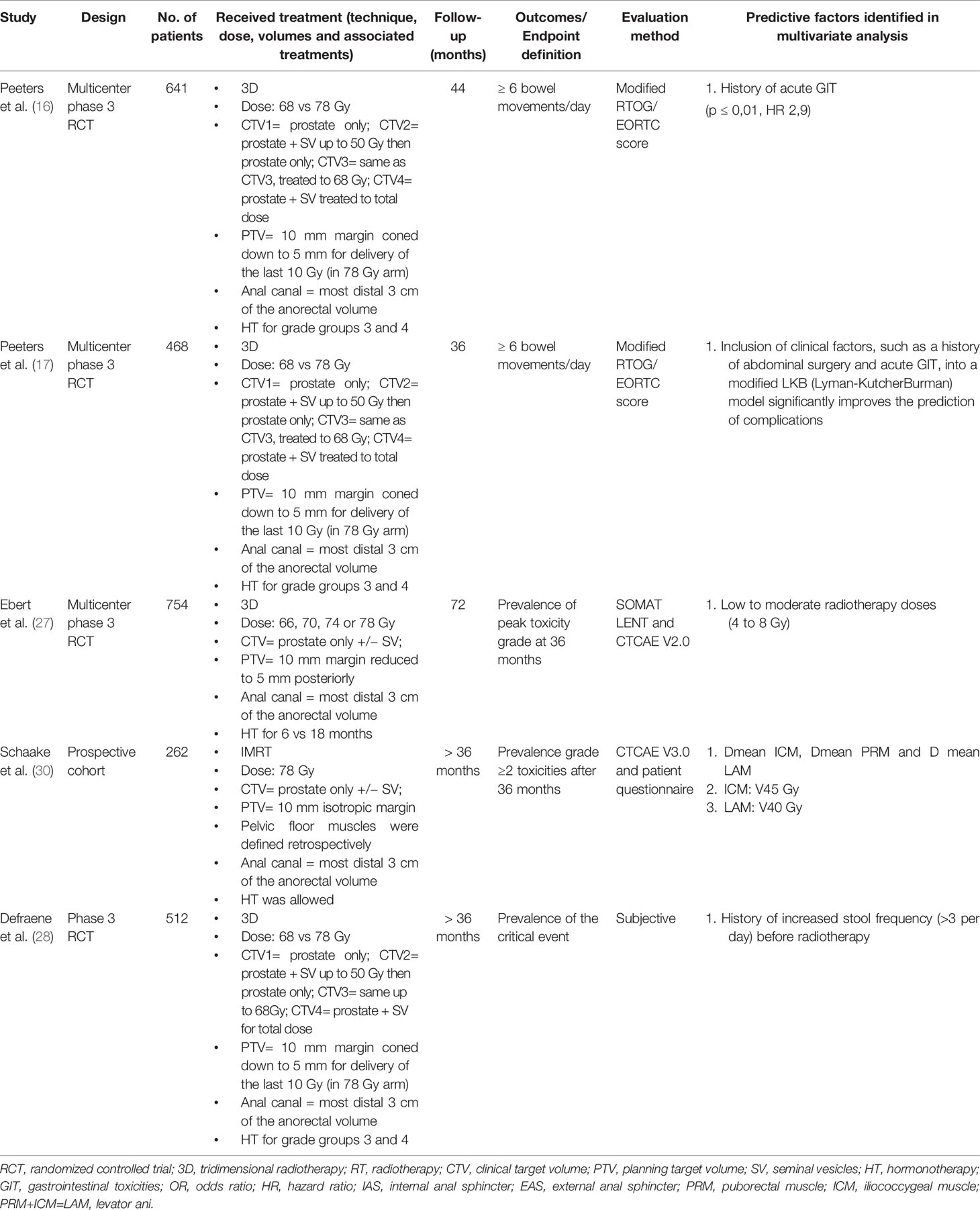
Table 2 Identification of predictive factors for the late occurrence of diarrheas and increased stool frequency in patients with localized prostate cancer treated with pelvic radiotherapy.
As for patient-related predictive factors, a history of previous abdominal surgery is related to an increased risk in stool frequency and in diarrhea after prostate RT (17). Other studies (16, 17, 28) have also shown that the presence of acute GI side effects during RT or a history of GI symptoms prior to irradiation are both risk factors for increased stool frequency and diarrhea later on.
Impact of Anal Canal Irradiation on Renesmus, Stool Urgency, and Incontinence in the Context of Pelvic Radiotherapy
The risk of chronic stool urgency and tenesmus (grade ≥2) after prostate RT varies between 3% and 12%. Stool incontinence is reported to be around 5% in most series; however, it greatly affects patients’ quality of life (19), hence, the need to find dosimetric and patient-related factors than can predict which patients are more at risk of developing stool incontinence. Table 3 summarizes some of these factors related to the AC.
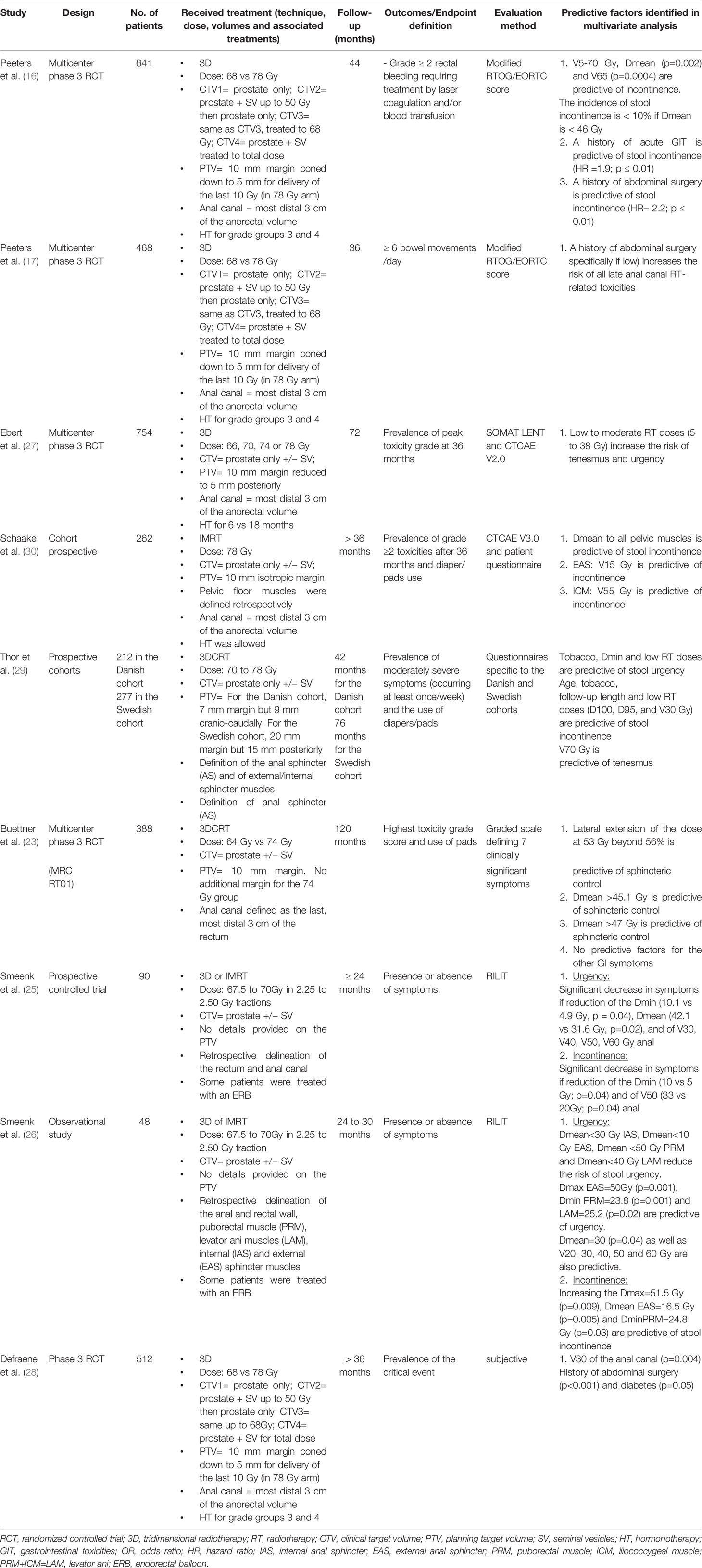
Table 3 Identification of predictive factors for tenesmus, stool urgency or incontinence in patients with localized prostate cancer treated with pelvic radiotherapy.
Low to moderate doses of RT to the AC were associated with increased risk of tenesmus, stool urgency, and incontinence to the same extent as higher doses. Indeed, Peeters et al. (16) showed that all dosimetric parameters to the anal wall were significantly predictive of stool incontinence. Smeenk et al. (25) found a significant decrease in AC rest pressure in patients presenting with stool urgency and incontinence. Moreover, AC Dmin, Dmean, V30, V40, V50, and V60 of the AC were all correlated with the incidence of stool urgency and incontinence in this study (25). The V30 Gy and a dose of 5 to 38 Gy to the AC were also identified as predictive factors in an NTCP model by Defraene et al. (28). In a multicenter RCT of 388 patients, with a median follow-up of 24 months, Buettner et al. (23) established a significant positive correlation between sphincter-related symptoms and the dose received specifically by the AC wall. The authors recommended mean doses of 30 Gy or less to the anal sphincter and of 27 Gy at most to the AC surface to limit the risks of tenesmus, stool urgency and incontinence.
The frequency, intensity, and chronicity of LGIT have been significantly correlated with manometric studies of anal pressures (8–12). Some of these studies showed a change in the morphology of the internal and external sphincters, whereas others did not, underlying a possible, but not proven, contribution of the AC in the occurrence of lower LGIT related to prostate RT. This relation between the tissue response of anal structures to RT and anorectal dysfunction is further supported by a cohort study of 309 patients with prostate cancer treated by RT (10). With a median follow-up of 3.8 years, the patients with high RT-induced anorectal dysfunction had changes to the anorectal mucosa, increased rectal sensory response to distension, and reduced maximum anal resting pressure as assessed by anal manometri (10). Altogether, these findings suggest a correlation between RT-induced LGIT and RT-induced morphologic changes to the AC. They also suggest a specific role for the AC in the development of these LGIT.
Irradiation of the pudendal nerve, which is closely related to the AC, was also implicated in the development of stool incontinence. In a retrospective study, 17 patients with localized prostate cancer were treated by RT whereas a control group of 57 patients were not (35). The authors described a loss of response of the pudendal nerve to stimulation in 10 patients treated with RT (62.5%) vs 3 patients (6.5%) in the control group (p< 0,001). Moreover, there was altered pudendal nerve response in four patients treated with RT to the prostate (25.1%) vs seven (15.2%) in the control group (p< 0,001). It would be interesting to see if spatial extension of the dose to the AC played a role in the occurrence of these LGIT, as was shown for the rectum (34). Finally, radiation doses to the pelvic floor muscles and anal sphincters have been shown to have an impact on the occurrence of stool urgency and incontinence (26).
As for patient-related predictive factors, once again, a history of abdominal surgery was a risk factor for the development of tenesmus, stool urgency, and incontinence (16, 17, 21, 22, 24, 28) whereas the use of anti-hypertensive medications seemed protective (21, 22). Interestingly, the “lower” the level of the abdominal surgery was, the more the risk of such LGIT. One hypothesis to explain this is the fact that abdominal surgery causes a state of inflammation prior to RT, with an increased production of cytokines (20, 36, 37). Furthermore, surgery alters the neurovascular system in the area of concern, leading to higher sensitivity to radiation (17). Finally, it appears that diabetic patients are more at risk as well (28), probably through the same inflammatory processes.
Impact of AC Irradiation on Gastrointestinal and Abdominal Pain in the Context of Pelvic Irradiation
There is scarce data available on this type of symptom and their frequency after prostate RT. It seems however that less than 5% of patients present with grade ≥ 2 late gastrointestinal or abdominal pain (16, 24, 38) (Table 4). Peeters et al. (16) showed that the presence of acute GIT during RT or a history of GI symptoms prior to irradiation significantly increases the incidence of gastrointestinal and abdominal pain later. According to a study by Thor et al., tobacco smoking and hormonotherapy are contributing factors, whereas the V15 of the AC could be predictive of late GI or abdominal pain (29). However, no anal or rectal dosimetric parameters were shown to be directly related to these symptoms.
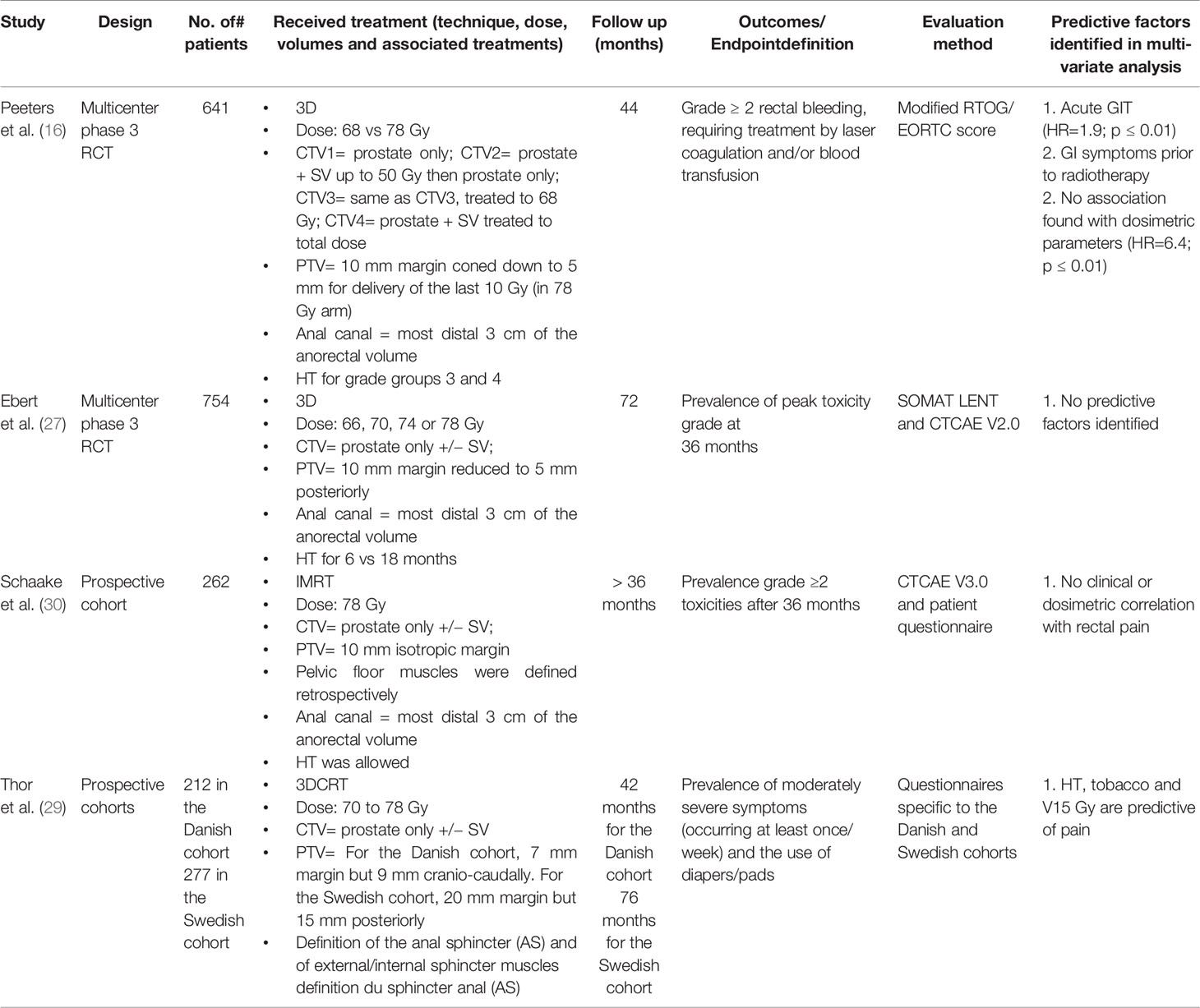
Table 4 Identification of predictive factors for late abdominal or rectal pain in patients with localized prostate cancer treated with pelvic radiotherapy.
Recommendations on How to Optimize the Anal Canal Radio-Induced Tolerance
Table 5 summarizes all the recommendations derived from this literature review regarding irradiation of the anal canal during prostate RT.
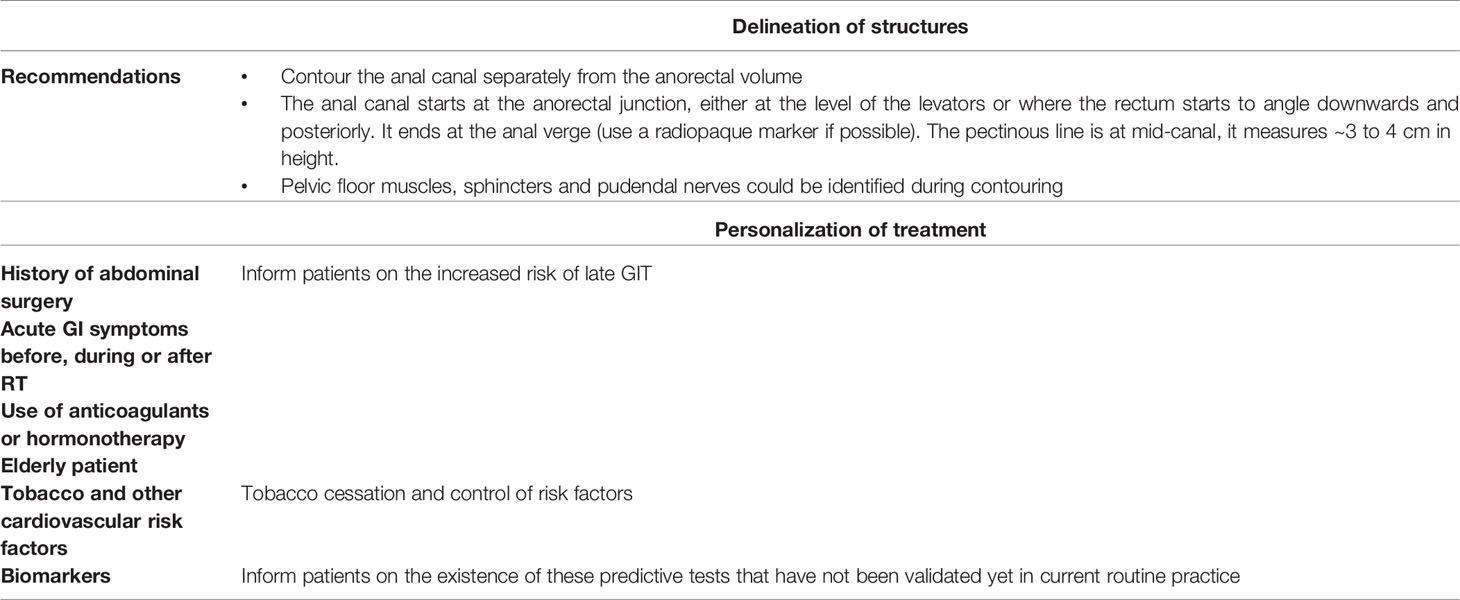
Table 5 Optimization of late gastrointestinal tolerance after radiotherapy for localized prostate cancer.
Taking Into Account the Patients’ Medical History and Their Individual Factors in Predicting Late GIT
It is primordial to consider the patients’ clinical factors, in addition to the dosimetric analysis, in order to limit RT related LGIT (28). An adaptation of the dose levels could then be done based on these clinical risk factors. Patients should be informed of a potential increased risk of GIT if they have any of the described risk factors, namely any prior abdominal surgery, cardiovascular or smoking history or history of GI symptoms prior to RT. We also believe that the concept of rectal capacitance, which is well described in the context of RT for rectal cancer (39), should be further studied in prostate RT in order to better predict the risk of LGIT. This specific point could be extrapolated to the AC in future studies. An exciting area of innovation is the emergence of biomarkers (genomic, SNPs, micro-RNA, radiation-induced lymphocyte apoptosis, etc.) that can predict radiation induced toxicities. These could allow clinicians to adapt the management of patients that have individual susceptibility to ionizing radiation (40). Indeed, there are reports already of the existence of genetic factors that could predispose to anorectal bleeding (41–44).
Contouring the Anal Canal Separately From the Rectum During Treatment Planning
Our literature review showed that there is a significant heterogeneity in the dosimetric studies looking at LGIT. Moreover, the pathophysiology of the AC is unique and independent of that of the rest of the GI system (ano-rectal and/or small bowel). Thus, it is important to contour the AC separately from the rectum or anorectal volume during treatment planning. We propose that an anal probe be inserted in the AC specifically and metal fiducial markers placed at the anal verge at the time of treatment simulation in order to facilitate delineation of the AC. Contouring of the AC should follow published guidelines (4).
Considering the Dose-Effect Relationship
Intensity-modulated, image-guided radiotherapy (IMRT/IGRT) was shown to significantly decrease the incidence of GIT and is now the standard of care for prostate RT (45). Thus, it is important to mention that most of the dosimetric data derived from our literature review are from 3DCRT studies. Furthermore, there are no reports in the literature of AC-specific dosimetric data in case of moderate hypofractionated RT for the prostate (46). Taking these caveats into account, our literature review shows that low, medium, and high doses of radiation were all correlated to AC-specific LGIT. This makes it extremely complex to establish dosimetric constraints for the AC that would help in limiting GIT. These findings, however, highlight a possible dose-effect relationship for the AC. To definitively prove such a dose-effect relationship, it will be important in future trials to specifically delineate the AC as an OAR and include an evaluation of the GIT specifically related to the AC.
Identifying and Contouring Anatomical Structures Adjacent to the Anal Canal During Treatment Planning
Different muscles and nerves could be individually contoured with the help of MRI imaging, and assuming that they receive similar doses to the AC, the same dose constraints could be applied in order to reduce the risk of LGIT.
Evaluation of Toxicities Using Standardized Scales and Quality of Life Questionnaires
One of the main limitations to the evaluation of LGIT, as highlighted in this review, is the heterogeneity that exists among the different symptom evaluation scales used in studies. The use of specific, well-validated symptoms scales is key in the design of future prospective studies evaluating the tolerance of the AC to RT. By the same token, it will be important to include quality of life scales and Patients Reported Outcomes questionnaires in these studies.
Use of Spacers and Endorectal Balloons
Studies on the daily use of endorectal balloons showed that they efficiently reduce doses to the AC and the risks of LGIT. Thus, the use of spacer technologies could be a viable technical approach in reducing AC-related GIT (47).
Limitations of the Study
One of the main limitations of this narrative review is the fact that it is based on a small number of publications (nine). This is mainly because our research question is very specific and that there is limited literature on the specific subject of AC-related LGIT and limited publications that delineated the AC individually in their study design. Another limitation of the study is the fact that the majority of the reviewed papers used 3DCRT, which is no longer the standard of care for the treatment of prostate cancer. Moreover, we did not identify any reports of moderate hypofractionated prostate RT looking specifically at the contribution of AC dosimetry to the development of LGIT. There is also the variability related to the different toxicity scales used throughout studies as well as the definition and contouring of the anal canal subvolumes. Other limitations are inherent to any narrative review, including bias related to the selection of papers, which we tried to mitigate by having specific inclusion and exclusion criteria. However, we recognize that certain publications meeting our inclusion criteria may have been missed. Finally, we want to highlight the fact that a causal relation between dose to the AC and the occurrence of LGIT cannot be inferred from this literature review. The evidence summarized here suggests an important role for the AC, however, this role cannot be fully dissociated from the contribution of the rectum, anorectum, or other adjacent structures and of patient-related predictive factors.
Conclusion
Despite limited literature on the subject, our review highlighted the potential role that irradiation of the AC plays in the development of LGIT after prostate/pelvic RT. It also highlights how important it is to take patients’ specific clinical risk factors into account. Identification of the AC independently of the anorectal volume, and an optimization of the dosimetry related to the AC and adjacent structures, will be essential in improving side effects related to prostate RT. Finally, tolerance to prostate RT should be evaluated using validated scales and quality of life questionnaires in the context of prospective studies.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Author Contributions
Conceptualization: PS, MD, RC, and MB. Data curation: PS, MB, and RC. Formal analysis: PS, MD, and RC. Investigation: PS, MD, RC, and MB. Methodology: PS and RC. Project administration: PS and MB. Supervision: PS and RC. Validation: SS, IL, DA, TN, TV, and VV. Visualization: all co-authors. Writing—original draft: PS, MD, and MB. Writing—review and editing: all co-authors. All authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Gami B, Harrington K, Blake P, Dearnaley D, Tait D, Davies J, et al. How Patients Manage Gastrointestinal Symptoms After Pelvic Radiotherapy. Aliment Pharmacol Ther (2003) 18(10):987–94. doi: 10.1046/j.1365-2036.2003.01760.x
2. Krol R, Smeenk RJ, van Lin EN, Hopman WP. Impact of Late Anorectal Dysfunction on Quality of Life After Pelvic Radiotherapy. Int J Colorectal Dis (2013) 28(4):519–26. doi: 10.1007/s00384-012-1593-5
3. Moreau-Claeys MV, Peiffert D. Normal Tissue Tolerance to External Beam Radiation Therapy: Anal Canal. Cancer Radiother (2010) 14(4-5):359–62. doi: 10.1016/j.canrad.2010.01.009
4. Noel G, Antoni D, Barillot I, Chauvet B. [Delineation of Organs at Risk and Dose Constraints]. Cancer Radiother (2016) 20(Suppl):S36–60. doi: 10.1016/j.canrad.2016.07.032
5. Yeoh EE, Holloway RH, Fraser RJ, Botten RJ, Di Matteo AC, Moore JW, et al. Anorectal Dysfunction Increases With Time Following Radiation Therapy for Carcinoma of the Prostate. Am J Gastroenterol (2004) 99(2):361–9. doi: 10.1111/j.1572-0241.2004.04037.x
6. Matta R, Chapple CR, Fisch M, Heidenreich A, Herschorn S, Kodama RT, et al. Pelvic Complications After Prostate Cancer Radiation Therapy and Their Management: An International Collaborative Narrative Review. Eur Urol (2019) 75(3):464–76. doi: 10.1016/j.eururo.2018.12.003
7. Resnick MJ, Koyama T, Fan KH, Albertsen PC, Goodman M, Hamilton AS, et al. Long-Term Functional Outcomes After Treatment for Localized Prostate Cancer. N Engl J Med (2013) 368(5):436–45. doi: 10.1056/NEJMoa1209978
8. Lund JA, Kaasa S, Wibe A, Widmark A, Fransson P. Late Radiation Effects to the Rectum and Anus After Treatment for Prostate Cancer; Validity of the LENT/SOMA Score. Acta Oncol (2013) 52(4):727–35. doi: 10.3109/0284186X.2013.747695
9. Yeoh EK, Holloway RH, Fraser RJ, Botten RJ, Di Matteo AC, Butters J. Pathophysiology and Natural History of Anorectal Sequelae Following Radiation Therapy for Carcinoma of the Prostate. Int J Radiat Oncol Biol Phys (2012) 84(5):e593–9. doi: 10.1016/j.ijrobp.2012.06.032
10. Petersen SE, Bregendahl S, Langschwager M, Laurberg S, Brock C, Drewes AM, et al. Pathophysiology of Late Anorectal Dysfunction Following External Beam Radiotherapy for Prostate Cancer. Acta Oncol (2014) 53(10):1398–404. doi: 10.3109/0284186X.2014.926029
11. Yeoh EK, Bartholomeusz DL, Holloway RH, Fraser RJ, Botten R, Di Matteo A, et al. Disturbed Colonic Motility Contributes to Anorectal Symptoms and Dysfunction After Radiotherapy for Carcinoma of the Prostate. Int J Radiat Oncol Biol Phys (2010) 78(3):773–80. doi: 10.1016/j.ijrobp.2009.08.050
12. Choi Y, Park W, Rhee PL. Can Anorectal Manometry Findings Predict Subsequent Late Gastrointestinal Radiation Toxicity in Prostate Cancer Patients? Cancer Res Treat (2016) 48(1):297–303. doi: 10.4143/crt.2014.333
13. Gulliford SL, Foo K, Morgan RC, Aird EG, Bidmead AM, Critchley H, Evans PM, et al. Dose-Volume Constraints to Reduce Rectal Side Effects From Prostate Radiotherapy: Evidence From MRC RT01 Trial ISRCTN 47772397. Int J Radiat Oncol Biol Phys (2010) 76(3):747–54. doi: 10.1016/j.ijrobp.2009.02.025
14. National Cancer Institute (US). Cancer Therapy Evaluation Program. In: Common Terminology Criteria for Adverse Events: (CTCAE). Cancer Therapy Evaluation Program (2003). Available at: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/ctc.htm.
15. Pan YB, Maeda Y, Wilson A, Glynne-Jones R, Vaizey CJ. Late Gastrointestinal Toxicity After Radiotherapy for Anal Cancer: A Systematic Literature Review. Acta Oncol (2018) 57(11):1427–37. doi: 10.1080/0284186X.2018.1503713
16. Peeters ST, Lebesque JV, Heemsbergen WD, van Putten WL, Slot A, Dielwart MF, et al. Localized Volume Effects for Late Rectal and Anal Toxicity After Radiotherapy for Prostate Cancer. Int J Radiat Oncol Biol Phys (2006) 64(4):1151–61. doi: 10.1016/j.ijrobp.2005.10.002
17. Peeters ST, Hoogeman MS, Heemsbergen WD, Hart AA, Koper PC, Lebesque JV. Rectal Bleeding, Fecal Incontinence, and High Stool Frequency After Conformal Radiotherapy for Prostate Cancer: Normal Tissue Complication Probability Modeling. Int J Radiat Oncol Biol Phys (2006) 66(1):11–9. doi: 10.1016/j.ijrobp.2006.03.034
18. Cox JD, Stetz J, Pajak TF. Toxicity Criteria of the Radiation Therapy Oncology Group (RTOG) and the European Organization for Research and Treatment of Cancer (EORTC). Int J Radiat Oncol Biol Phys (1995) 31(5):1341–6. doi: 10.1016/0360-3016(95)00060-C
19. Fellin G, Fiorino C, Rancati T, Vavassori V, Baccolini M, Bianchi C, et al. Clinical and Dosimetric Predictors of Late Rectal Toxicity After Conformal Radiation for Localized Prostate Cancer: Results of a Large Multicenter Observational Study. Radiother Oncol (2009) 93(2):197–202. doi: 10.1016/j.radonc.2009.09.004
20. Valdagni R, Vavassori V, Rancati T, Fellin G, Baccolini M, Bianchi C, et al. Increasing the Risk of Late Rectal Bleeding After High-Dose Radiotherapy for Prostate Cancer: The Case of Previous Abdominal Surgery. Results From a Prospective Trial. Radiother Oncol (2012) 103(2):252–5. doi: 10.1016/j.radonc.2012.03.012
21. Fellin G, Rancati T, Fiorino C, Vavassori V, Antognoni P, Baccolini M, et al. Long Term Rectal Function After High-Dose Prostatecancer Radiotherapy: Results From a Prospective Cohort Study. Radiother Oncol (2014) 110(2):272–7. doi: 10.1016/j.radonc.2013.09.028
22. Fiorino C, Rancati T, Fellin G, Vavassori V, Cagna E, Casanova Borca V, et al. Late Fecal Incontinence After High-Dose Radiotherapy for Prostate Cancer: Better Prediction Using Longitudinal Definitions. Int J Radiat Oncol Biol Phys (2012) 83(1):38–45. doi: 10.1016/j.ijrobp.2011.06.1953
23. Buettner F, Gulliford SL, Webb S, Sydes MR, Dearnaley DP, Partridge M. The Dose-Response of the Anal Sphincter Region–an Analysis of Data From the MRC RT01 Trial. Radiother Oncol (2012) 103(3):347–52. doi: 10.1016/j.radonc.2012.03.002
24. Fiorino C, Fellin G, Rancati T, Vavassori V, Bianchi C, Borca VC, et al. Clinical and Dosimetric Predictors of Late Rectal Syndrome After 3D-CRT for Localized Prostate Cancer: Preliminary Results of a Multicenter Prospective Study. Int J Radiat Oncol Biol Phys (2008) 70(4):1130–7. doi: 10.1016/j.ijrobp.2007.07.2354
25. Smeenk RJ, Hopman WP, Hoffmann AL, van Lin EN, Kaanders JH. Differences in Radiation Dosimetry and Anorectal Function Testing Imply That Anorectal Symptoms may Arise From Different Anatomic Substrates. Int J Radiat Oncol Biol Phys (2012) 82(1):145–52. doi: 10.1016/j.ijrobp.2010.08.023
26. Smeenk RJ, Hoffmann AL, Hopman WP, van Lin EN, Kaanders JH. Dose-Effect Relationships for Individual Pelvic Floor Muscles and Anorectal Complaints After Prostate Radiotherapy. Int J Radiat Oncol Biol Phys (2012) 83(2):636–44. doi: 10.1016/j.ijrobp.2011.08.007
27. Ebert MA, Foo K, Haworth A, Gulliford SL, Kennedy A, Joseph DJ, et al. Gastrointestinal Dose-Histogram Effects in the Context of Dose-Volume-Constrained Prostate Radiation Therapy: Analysis of Data From the RADAR Prostate Radiation Therapy Trial. Int J Radiat Oncol Biol Phys (2015) 91(3):595–603. doi: 10.1016/j.ijrobp.2014.11.015
28. Defraene G, Van den Bergh L, Al-Mamgani A, Haustermans K, Heemsbergen W, Van den Heuvel F, et al. The Benefits of Including Clinical Factors in Rectal Normal Tissue Complication Probability Modeling After Radiotherapy for Prostate Cancer. Int J Radiat Oncol Biol Phys (2012) 82(3):1233–42. doi: 10.1016/j.ijrobp.2011.03.056
29. Thor M, Olsson CE, Oh JH, Petersen SE, Alsadius D, Bentzen L, et al. Relationships Between Dose to the Gastro-Intestinal Tract and Patient-Reported Symptom Domains After Radiotherapy for Localized Prostate Cancer. Acta Oncol (2015) 54(9):1326–34. doi: 10.3109/0284186X.2015.1063779
30. Schaake W, van der Schaaf A, van Dijk LV, Bongaerts AH, van den Bergh AC, Langendijk JA. Normal Tissue Complication Probability (NTCP) Models for Late Rectal Bleeding, Stool Frequency and Fecal Incontinence After Radiotherapy in Prostate Cancer Patients. Radiother Oncol (2016) 119(3):381–7. doi: 10.1016/j.radonc.2016.04.005
31. Fiorino C, Valdagni R, Rancati T, Sanguineti G. Dose-Volume Effects for Normal Tissues in External Radiotherapy: Pelvis. Radiother Oncol (2009) 93(2):153–67. doi: 10.1016/j.radonc.2009.08.004
32. Landoni V, Fiorino C, Cozzarini C, Sanguineti G, Valdagni R, Rancati T. Predicting Toxicity in Radiotherapy for Prostate Cancer. Phys Med (2016) 32(3):521–32. doi: 10.1016/j.ejmp.2016.03.003
33. Drean G, Acosta O, Ospina JD, Fargeas A, Lafond C, Corrégé G, et al. Identification of a Rectal Subregion Highly Predictive of Rectal Bleeding in Prostate Cancer IMRT. Radiother Oncol (2016) 119(3):388–97. doi: 10.1016/j.radonc.2016.04.023
34. Buettner F, Gulliford SL, Webb S, Sydes MR, Dearnaley DP, Partridge M. Assessing Correlations Between the Spatial Distribution of the Dose to the Rectal Wall and Late Rectal Toxicity After Prostate Radiotherapy: An Analysis of Data From the MRC RT01 Trial (ISRCTN 47772397). Phys Med Biol (2009) 54(21):6535–48. doi: 10.1088/0031-9155/54/21/006
35. Loganathan A, Schloithe AC, Hutton J, Yeoh EK, Fraser R, Dinning PG, et al. Pudendal Nerve Injury in Men With Fecal Incontinence After Radiotherapy for Prostate Cancer. Acta Oncol (2015) 54(6):882–8. doi: 10.3109/0284186X.2015.1010693
36. Yeoh E, Tam W, Schoeman M, Moore J, Thomas M, Botten R, et al. Argon Plasma Coagulation Therapy Versus Topical Formalin for Intractable Rectal Bleeding and Anorectal Dysfunction After Radiation Therapy for Prostate Carcinoma. Int J Radiat Oncol Biol Phys (2013) 87(5):954–9. doi: 10.1016/j.ijrobp.2013.08.034
37. van Lin EN, Kristinsson J, Philippens ME, de Jong DJ, van der Vight LP, Kaanders JH, et al. Reduced Late Rectal Mucosal Changes After Prostate Three-Dimensional Conformal Radiotherapy With Endorectal Balloon as Observed in Repeated Endoscopy. Int J Radiat Oncol Biol Phys (2007) 67(3):799–811. doi: 10.1016/j.ijrobp.2006.09.034
38. Cicchetti A, Rancati T, Ebert M, Fiorino C, Palorini F, Kennedy A, et al. Modelling Late Stool Frequency and Rectal Pain After Radical Radiotherapy in Prostate Cancer Patients: Results From a Large Pooled Population. Phys Med (2016) 32(12):1690–7. doi: 10.1016/j.ejmp.2016.09.018
39. Ihnat P, Slívová I, Tulinsky L, Ihnát Rudinská L, Máca J, Penka I. Anorectal Dysfunction After Laparoscopic Low Anterior Rectal Resection for Rectal Cancer With and Without Radiotherapy (Manometry Study). J Surg Oncol (2018) 117(4):710–6. doi: 10.1002/jso.24885
40. Brengues M, Lapierre A, Bourgier C, Pèlegrin A, Özsahin M, Azria D. T Lymphocytes to Predict Radiation-Induced Late Effects in Normal Tissues. Expert Rev Mol Diagn (2017) 17(2):119–27. doi: 10.1080/14737159.2017.1271715
41. Someya M, Yamamoto H, Nojima M, Hori M, Tateoka K, Nakata K, et al. Relation Between Ku80 and MicroRNA-99a Expression and Late Rectal Bleeding After Radiotherapy for Prostate Cancer. Radiother Oncol (2015) 115(2):235–9. doi: 10.1016/j.radonc.2015.04.008
42. Valdagni R, Rancati T, Ghilotti M, Cozzarini C, Vavassori V, Fellin G, et al. To Bleed or Not to Bleed. A Prediction Based on Individual Gene Profiling Combined With Dose-Volume Histogram Shapes in Prostate Cancer Patients Undergoing Three-Dimensional Conformal Radiation Therapy. Int J Radiat Oncol Biol Phys (2009) 74(5):1431–40. doi: 10.1016/j.ijrobp.2008.10.021
43. Kerns SL, Fachal L, Dorling L, Barnett GC, Baran A, Peterson DR, et al. Radiogenomics Consortium Genome-Wide Association Study Meta-Analysis of Late Toxicity After Prostate Cancer Radiotherapy. J Natl Cancer Inst (2020) 112:179–90. doi: 10.1093/jnci/djz075
44. Burri RJ, Stock RG, Cesaretti JA, Atencio DP, Peters S, Peters CA, et al. Association of Single Nucleotide Polymorphisms in SOD2, XRCC1 and XRCC3 With Susceptibility for the Development of Adverse Effects Resulting From Radiotherapy for Prostate Cancer. Radiat Res (2008) 170(1):49–59. doi: 10.1667/RR1219.1
45. Delobel JB, Gnep K, Ospina JD, Beckendorf V, Chira C, Zhu J, et al. Nomogram to Predict Rectal Toxicity Following Prostate Cancer Radiotherapy. PLoS One (2017) 12(6):e0179845. doi: 10.1371/journal.pone.0179845
46. Langrand-Escure J, de Crevoisier R, Llagostera C, Créhange G, Delaroche G, Lafond C, et al. Dose Constraints for Moderate Hypofractionated Radiotherapy for Prostate Cancer: The French Genito-Urinary Group (GETUG) Recommendations. Cancer Radiother (2018) 22(2):193–8. doi: 10.1016/j.canrad.2017.11.004
Keywords: prostate cancer, radiotherapy, gastrointestinal toxicities, anal canal, rectum
Citation: Sargos P, Faye MD, Bacci M, Supiot S, Latorzeff I, Azria D, Niazi TM, Vuong T, Vendrely V and de Crevoisier R (2021) Late Gastrointestinal Tolerance After Prostate Radiotherapy: Is the Anal Canal the Culprit? A Narrative Critical Review. Front. Oncol. 11:666962. doi: 10.3389/fonc.2021.666962
Received: 11 February 2021; Accepted: 13 May 2021;
Published: 16 June 2021.
Edited by:
Amar U Kishan, University of California, Los Angeles, United StatesReviewed by:
Eric Lehrer, Icahn School of Medicine at Mount Sinai, United StatesLuca Faustino Valle, University of California, Los Angeles, United States
Copyright © 2021 Sargos, Faye, Bacci, Supiot, Latorzeff, Azria, Niazi, Vuong, Vendrely and de Crevoisier. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Paul Sargos, cC5zYXJnb3NAYm9yZGVhdXgudW5pY2FuY2VyLmZy