 Hao Zeng
Hao Zeng Yalun Li
Yalun Li Ye Wang2
Ye Wang2 Meijuan Huang
Meijuan Huang Yan Zhang
Yan Zhang Panwen Tian
Panwen Tian Weimin Li
Weimin Li- 1Department of Respiratory and Critical Care Medicine, West China Hospital, West China School of Medicine, Sichuan University, Chengdu, China
- 2Department of Respiratory and Critical Care Medicine, Lung Cancer Treatment Center, West China Hospital, Sichuan University, Chengdu, China
- 3Department of Thoracic Oncology, Cancer Center, West China Hospital, Sichuan University, Chengdu, China
- 4Department of Respiratory and Critical Care Medicine, West China Hospital, Sichuan University, Chengdu, China
Several double ALK fusions coexisting in one patient have been reported. However, few studies have reported the clinical efficacy of ALK inhibitors in rare double ALK fusions. Here, we described a rare PDK1-ALK, STRN-ALK double-fusion variant in a patient with metastatic lung adenocarcinoma. The patient responded well to alectinib (600 mg) twice daily. This case shows a promising treatment option for patients with rare ALK double-fusion variants.
Introduction
Anaplastic lymphoma kinase-positive (ALK-positive) disease occurs in approximately 5% of all patients with non-small cell lung cancer (NSCLC) (1). It has been reported that in a series of 80 ALK fusion-positive patients, 16.2% harbored more than 1 ALK fusion (2). More than 20 fusion partners for ALK in NSCLC have been reported with the increased utilization of next-generation sequencing (NGS). Several ALK double-fusion variants, such as DYSF-ALK/ITGAV-ALK and EML4-ALK/BIRC6-ALK, showed a good response to different ALK inhibitors, such as crizotinib and alectinib, respectively (3, 4). The clinical response to ALK inhibitors varies for different ALK variants. Alectinib, a highly selective ALK inhibitor, showed superior efficacy and lower toxicity in untreated ALK-positive NSCLC than crizotinib. Meanwhile alectinib has also demonstrated an overall survival (OS) benefit in the ALEX study (5, 6). However, few data have reported the sensitivity of alectinib in NSCLC harboring ALK double-fusion variants (4). Here, we first present a patient with rare double-fusion variants, PDK1-ALK and STRN-ALK, who responded well to standard doses of alectinib treatment.
Case Presentation
A 29-year-old Chinese female non-smoker presented to our hospital with a 2-month history of chest pain. She was an accountant without a family history of cancers. She did not have a history of exposure to any professional or environmental carcinogen. Superficial lymph nodes were not palpable, and no other physical examinations showed abnormalities. On June 15, 2020, a contrast-enhanced computed tomography (CT) scan showed a 2.7 cm×2.5 cm mass in the hilum of the middle lobe of the right lung (Figure 1A) with mediastinal lymph node metastases and multiple metastases in the ribs and thoracic vertebras. Transthoracic needle biopsy established the pathologic diagnosis of lung solid-predominant adenocarcinoma (T2N2M1c, stage IVB). ALK-Ventana (D5F3), keratin 7, napsin A and thyroid transcription factor-1 were positive by immunohistochemistry staining, and then PDK1-ALK (P7:A20, allelic frequency: 12.85%), STRN-ALK (S3:A20, allelic frequency: 27.11%) double-fusion (Figures 2A, B) and a variable splicing mutation in exon 9 of TP53 (allelic frequency: 4.84%) were identified in the same tumor tissue by DNA-based NGS (mean depth of the reads was 1200X), while the other driver gene mutations, including EGFR, KRAS and ROS1, were not detected. Given the promising efficacy and tolerability of alectinib, the patient was administered alectinib (600 mg twice daily) as the first-line treatment. A follow-up CT scan found that the lesions shrank to 1.4 cm × 1.1 cm after 1 month, 1.2 cm × 1.0 cm after 4 months, and 1.1 cm × 0.7 cm after 7 months of alectinib treatment (Figures 1B–D). The response of the reduction of the mass size changes with the continue of the treatment. The patient is still in follow-up, and no severe adverse reactions have been observed.
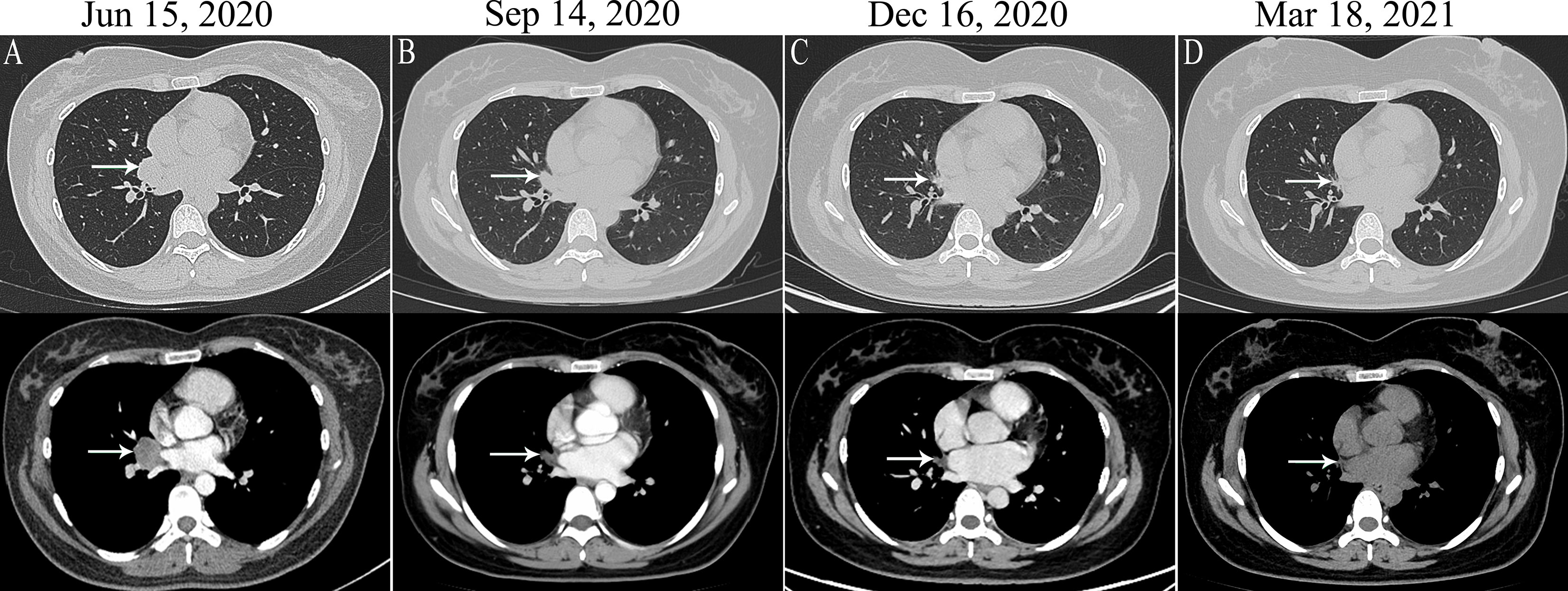
Figure 1 The lung target lesion on CT (white arrow). (A) Computed tomography (CT) scan showed a 2.7 cm×2.5 cm mass in the hilum of the right lung before treatment. (B) the imaging of lung target lesion after 1 month of alectinib treatment (1.4 cm × 1.1 cm lesions). (C) the imaging of lung target lesion after 4 months of alectinib treatment (1.2 cm × 1.0 cm lesions); (D) the imaging of lung target lesion after 7 months of alectinib treatment (1.1 cm × 0.7 cm lesions).
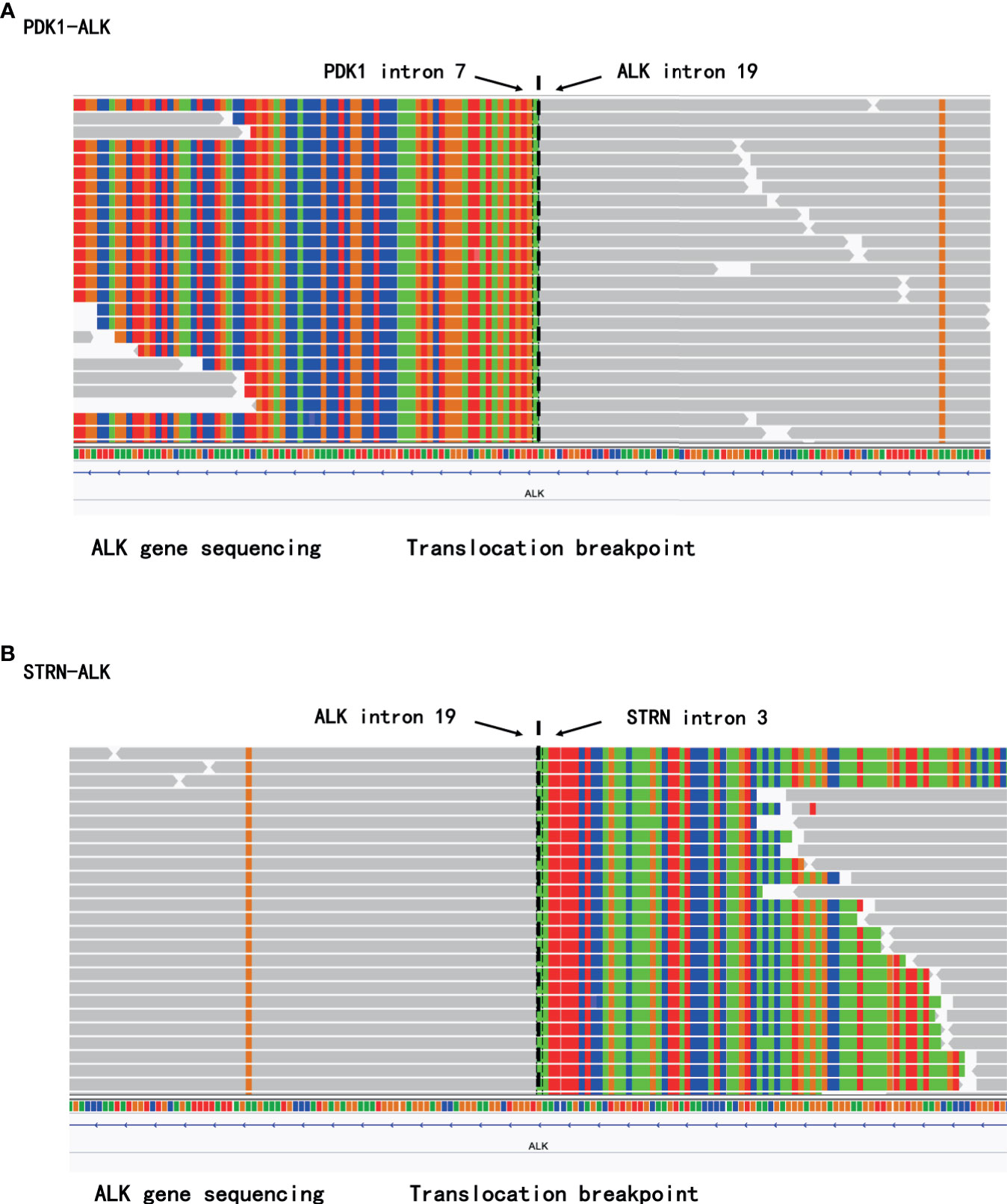
Figure 2 The rare PDK1-ALK and STRN-ALK fusion was identified in the same tumor tissue by next-generation sequencing (NGS). (A) sequencing reads of PDK1 and ALK by the Integrative Genomics Viewer. (B) sequencing reads of STRN and ALK by the Integrative Genomics Viewer.
Discussion
Many partners for ALK fusions in NSCLC have been reported, including the Huntington interacting protein 1 gene (HIP1), baculoviral IAP repeat containing 6 gene (BIRC6), and B cell CLL/lymphoma 11A gene (BCL11A), which benefit from crizotinib therapy (7–9). Alectinib, ceritinib and brigatinib are currently recommended as first-line choices in Europe and lorlatinib also in the USA (5, 10, 11). Our case first describes the promising efficacy of alectinib treatment of two rare fusions, PDK1-ALK and STRN-ALK, in a patient with lung adenocarcinoma.
The pyruvate dehydrogenase kinase 1 (PDK1) gene is located on chromosome 2q31.1 and has 24 exons, and is a direct hypoxia-inducible factor 1 (HIF1) target gene. Hypoxia, a universal feature of solid tumors, induces PDK1 gene expression caused via HIF1 (12). The expression levels of PDK-1 mRNA and protein were markedly elevated in NSCLC, and knockdown of PDK-1 can induce cancer cell apoptosis through the Hippo-YAP/IRS2 signaling pathway (13). To date, no other PDK1 fusion gene has been reported. Our patient harbored a PDK1-ALK fusion with intron 7 of PDK1 ligated to intron 19 of ALK, and experienced clinical improvement with alectinib treatment.
Similarly located on chromosome 2, the STRN gene encodes a protein with a coiled-coil domain that leads to constitutive activation of ALK kinase via dimerization (14). STRN-ALK has been reported in three cases of lung adenocarcinoma that were administered ALK inhibitors, and two showed a response to crizotinib and ceritinib. However, a 51-year-old Japanese male who was diagnosed with recurrent lung adenocarcinoma harboring STRN-ALK was resistant to alectinib 600 mg once a day as first-line therapy (Table 1) (14–16). Nakanishi Y et al. (16) attributed the nonresponse of alectinib to vimentin expression and ATP binding cassette subfamily B member 1 (ABCB1) mRNA overexpression. Additionally, pharmacokinetic data indicated that doses of alectinib were related to clinical activity in a dose-escalation study (300-900 mg twice a day) (17), and Gadgeel et al. (17) chose 600 mg alectinib twice a day as the recommended dose. Similarly, even in an Asian patient population, Zhou et al. (18) confirmed the clinical benefit of alectinib (600 mg twice daily) as a first-line treatment for ALK-positive NSCLC. The use of a low dose of alectinib might be a potential cause of treatment failure in patients who came from Japan.

Table 1 STRN-ALK fusion in patients with lung cancer in previous studies.
A few limitations are associated with the study. Due to the rarity of the ALK double-fusion variants, only one patient was reported in our case. The results need more cases or large cohort studies to verify in the future.
Patient Perspective
The patient thought that we diagnosed the disease promptly and treated appropriately, and she would continually follow doctors’ advice.
Conclusions
We are first to report two novel rare fusions, PDK1-ALK and STRN-ALK, that coexist in one patient with lung adenocarcinoma and are sensitive to alectinib. These double ALK fusions responded well to treatment with a standard dose of alectinib. Additionally, NGS assays can provide reliable diagnostic information on novel fusion partner genes for patients with NSCLC.
Data Availability Statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found below: http://www.biosino.org/node/project/detail/OEP002216, We have uploaded detailed raw data of sequences to https://www.biosino.org/node/. All data can be viewed in NODE (http://www.biosino.org/node) by pasting the accession (OEP002216) into the text search box or through the URL: http://www.biosino.org/node/project/detail/OEP002216.
Ethics Statement
The patient involved in this case report provided written informed consent authorizing the use and disclosure of her protected health information. Written informed consent was obtained from the patient in accordance with the Declaration of Helsinki for publication of the clinical data and any accompanying images. Institutional approval was not required to publish the case details. The patients/participants provided their written informed consent to participate in this study. Written informed consent was obtained from the patient for publication of the case report and the accompanying images.
Author Contributions
Conceptualization: HZ, Y-LL, YW, M-JH and YZ. Data collection: HZ, Y-LL, YW, M-JH and YZ. Writing-original draft preparation: HZ and Y-LL. Administrative Support: P-WT and W-ML. All authors contributed to the article and approved the submitted version.
Funding
This work was supported by the National Science Foundation of China (grant number 82072598, 81871890, and 91859203); the National Key Development Plan for Precision Medicine Research of China (grant number 2017YFC0910004); the Science and Technology Program of Sichuan, China (grant number 2020YFS0572) and the Major Science and Technology Innovation Project of Chengdu City, China (grant number 2020-YF08-00080-GX).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
NGS, next-generation sequencing; NSCLC, Non-small cell lung cancer; CT, computed tomography; HIP1, huntington interacting protein 1 gene; BIRC6, baculoviral IAP repeat containing 6 gene; BCL11A, B cell CLL/lymphoma 11A gene; PDK1, pyruvate dehydrogenase kinase 1; HIF1, hypoxia-inducible factor 1; ABCB1, ATP binding cassette subfamily B member 1; LAC, lung adenocarcinoma; PFS, progression free survival; OS, overall survival; CK7, keratin 7; TTF-1, thyroid transcription factor-1; EGFR, epidermal growth factor receptor; KRAS, Kirsten rat sarcoma viral oncogene homolog.
References
1. Dearden S, Stevens J, Wu YL, Blowers D. Mutation Incidence and Coincidence in Non Small-Cell Lung Cancer: Meta-Analyses by Ethnicity and Histology (Mutmap). Ann Oncol (2013) 24(9):2371–6. doi: 10.1093/annonc/mdt205
2. Li J, Zhang B, Zhang Y, Xu F, Zhang Z, Shao L, et al. Concomitant Mutation Status of ALK-Rearranged Non-Small Cell Lung Cancers and Its Prognostic Impact on Patients Treated With Crizotinib. Transl Lung Cancer Res (2021) 10(3):1525–35. doi: 10.21037/tlcr-21-160
3. Yin J, Zhang Y, Zhang Y, Peng F, Lu Y. Reporting on Two Novel FusionsCoexisting in One Patient With Adenocarcinoma of Lung, Sensitive to Crizotinib. J Thorac Oncol (2018) 13(3):e43–5. doi: 10.1016/j.jtho.2017.10.025
4. Zhong JM, Zhang GF, Lin L, Li DY, Liu ZH. A Novel EML4-ALK BIRC6-ALK Double Fusion Variant in Lung Adenocarcinoma Confers Sensitivity to Alectinib. Lung Cancer (2020) 145:211–2. doi: 10.1016/j.lungcan.2020.04.030
5. Peters S, Camidge DR, Shaw AT, Gadgeel S, Ahn JS, Kim DW, et al. Alectinib Versus Crizotinib in Untreated ALK-Positive Non-Small-Cell Lung Cancer. N Engl J Med (2017) 377(9):829–38. doi: 10.1056/NEJMoa1704795
6. Mok T, Camidge DR, Gadgeel SM, Rosell R, Dziadziuszko R, Kim DW, et al. Updated Overall Survival and Final Progression-Free Survival Data for Patients With Treatment-Naive Advanced ALK-Positive Non-Small-Cell Lung Cancer in the ALEX Study. Ann Oncol (2020) 31(8):1056–64. doi: 10.1016/j.annonc.2020.04.478
7. Tian Q, Deng W-J, Li Z-W. Identification of a Novel Crizotinib-Sensitive BCL11A-ALK Gene Fusion in a Nonsmall Cell Lung Cancer Patient. Eur Respir J (2017) 49(4):1602149. doi: 10.1183/13993003.02149-2016
8. Shan L, Jiang P, Xu F, Zhang W, Guo L, Wu J, et al. BIRC6-ALK, a Novel Fusion Gene in ALK Break-Apart FISH-Negative Lung Adenocarcinoma, Responds to Crizotinib. J Thorac Oncol (2015) 10(6):e37–9. doi: 10.1097/JTO.0000000000000467
9. Hong M, Kim RN, Song JY, Choi SJ, Oh E, Lira ME, et al. HIP1-ALK, a Novel Fusion Protein Identified in Lung Adenocarcinoma. J Thorac Oncol (2014) 9(3):419–22. doi: 10.1097/JTO.0000000000000061
10. Camidge DR, Kim HR, Ahn MJ, Yang JCH, Han JY, Hochmair MJ, et al. Brigatinib Versus Crizotinib in Advanced ALK Inhibitor-Naive ALK-Positive Non-Small Cell Lung Cancer: Second Interim Analysis of the Phase III ALTA-1L Trial. J Clin Oncol (2020) 38(31):3592–603. doi: 10.1200/JCO.20.00505
11. Solomon BJ, Besse B, Bauer TM, Felip E, Soo RA, Camidge DR, et al. Lorlatinib in Patients With ALK-Positive Non-Small-Cell Lung Cancer: Results From a Global Phase 2 Study. Lancet Oncol (2018) 19(12):1654–67. doi: 10.1016/s1470-2045(18)30649-1
12. Kim JW, Tchernyshyov I, Semenza GL, Dang CV. HIF-1-Mediated Expression of Pyruvate Dehydrogenase Kinase: A Metabolic Switch Required for Cellular Adaptation to Hypoxia. Cell Metab (2006) 3(3):177–85. doi: 10.1016/j.cmet.2006.02.002
13. Wang G, Liu X, Xie J, Meng J, Ni X. PDK-1 Mediated Hippo-YAP-IRS2 Signaling Pathway and Involved in the Apoptosis of Non-Small Cell Lung Cancer Cells. Biosci Rep (2019) 39(5):BSR20182099. doi: 10.1042/BSR20182099
14. Ren H, Hou X, Eiken PW, Zhang J, Pierson KE, Nair AA, et al. Identification and Development of a Lung Adenocarcinoma PDX Model With STRN-ALK Fusion. Clin Lung Cancer (2019) 20(2):e142–7. doi: 10.1016/j.cllc.2018.11.002
15. Yang Y, Qin SK, Zhu J, Wang R, Li YM, Xie ZY, et al. A Rare STRN-ALK Fusion in Lung Adenocarcinoma Identified Using Next-Generation Sequencing-Based Circulating Tumor DNA Profiling Exhibits Excellent Response to Crizotinib. Mayo Clin Proc Innov Qual Outcomes (2017) 1(1):111–6. doi: 10.1016/j.mayocpiqo.2017.04.003
16. Nakanishi Y, Masuda S, Iida Y, Takahashi N, Hashimoto S. Case Report of Non-Small Cell Lung Cancer With STRN-ALK Translocation: A Nonresponder to Alectinib. J Thorac Oncol (2017) 12(12):e202–4. doi: 10.1016/j.jtho.2017.08.009
17. Gadgeel SM, Gandhi L, Riely GJ, Chiappori AA, West HL, Azada MC, et al. Safety and Activity of Alectinib Against Systemic Disease and Brain Metastases in Patients With Crizotinib-Resistant ALK-Rearranged Non-Small-Cell Lung Cancer (AF-002JG): Results From the Dose-Finding Portion of a Phase 1/2 Study. Lancet Oncol (2014) 15(10):1119–28. doi: 10.1016/s1470-2045(14)70362-6
18. Zhou C, Kim SW, Reungwetwattana T, Zhou J, Zhang Y, He J, et al. Alectinib Versus Crizotinib in Untreated Asian Patients With Anaplastic Lymphoma Kinase-Positive Non-Small-Cell Lung Cancer (ALESIA): A Randomised Phase 3 Study. Lancet Respir Med (2019) 7(5):437–46. doi: 10.1016/s2213-2600(19)30053-0
Keywords: alectinib, ALK fusion, lung adenocarcinoma, targeted therapy, double-fusion variant
Citation: Zeng H, Li Y, Wang Y, Huang M, Zhang Y, Tian P and Li W (2021) Case Report: Identification of Two Rare Fusions, PDK1-ALK and STRN-ALK, That Coexist in a Lung Adenocarcinoma Patient and the Response to Alectinib. Front. Oncol. 11:722843. doi: 10.3389/fonc.2021.722843
Received: 09 June 2021; Accepted: 28 July 2021;
Published: 13 August 2021.
Edited by:
Haishu Lin, Shenzhen Technology University, ChinaReviewed by:
Petros Christopoulos, Heidelberg University Hospital, GermanyHanan Anbar, Dubai Pharmacy College, United Arab Emirates
Copyright © 2021 Zeng, Li, Wang, Huang, Zhang, Tian and Li. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Panwen Tian, bXJhc2NlbmRAMTYzLmNvbQ==
†These authors have contributed equally to this work