 Kai Zhang
Kai Zhang Lang Qian1,2†
Lang Qian1,2† Jieying Chen
Jieying Chen- 1Department of Medical Ultrasound, Fudan University Shanghai Cancer Center, Shanghai, China
- 2Department of Oncology, Shanghai Medical College of Fudan University, Shanghai, China
- 3Department of Radiology, Shanghai Tenth People’s Hospital, Tongji University School of Medicine, Shanghai, China
Purpose: No non-invasive method can accurately determine the presence of central cervical lymph node (CCLN) metastasis in papillary thyroid cancer (PTC) until now. This study aimed to investigate factors significantly associated with CCLN metastasis and then develop a model to preoperatively predict CCLN metastasis in fine-needle aspiration (FNA) reporting suspicious papillary thyroid cancer (PTC) or PTC without lateral neck metastasis.
Patients and Methods: Consecutive inpatients who were diagnosed as suspicious PTC or PTC in FNA and underwent partial or total thyroidectomy and CCLN dissection between May 1st, 2016 and June 30th, 2018 were included. The total eligible patients were randomly divided into a training set and an internal validation set with the ratio of 7:3. Univariate analysis and multivariate analysis were conducted in the training set to investigate factors associated with CCLN metastasis. The predicting model was built with factors significantly correlated with CCLN metastasis and validated in the validation set.
Results: A total of 770 patients were eligible in this study. Among them, 268 patients had histologically confirmed CCLN metastasis, while the remaining patients did not. Factors including age, BRAF mutation, multifocality, size, and capsule involvement were found to be significantly correlated with the CCLN metastasis in univariate and multivariate analysis. A model used to predict the presence CCLN metastasis based on these factors and US CCLN status yielded AUC, sensitivity, specificity and accuracy of 0.933 (95%CI: 0.905-0.960, p < 0.001), 0.816, 0.966 and 0.914 in the training set and 0.967 (95%CI: 0.943-0.991, p < 0.001), 0.897, 0.959 and 0.936 in the internal validation set.
Conclusion: Age, BRAF mutation, multifocality, size, and capsule involvement were independent predictors of CCLN metastasis in FNA reporting suspicious PTC or PTC without lateral neck metastasis. A simple model was successfully built and showed excellent discrimination to distinguish patients with or without CCLN metastasis.
Introduction
Thyroid cancer ranks the seventh in the list of newly diagnosed cancers and occurs 3.2 times more often in women than in men in China according to the latest report (1). The mortality increased slightly from 2003 to 2012, whereas the incidence increased by approximately five times during the same period (1), indicating more medical resource is needed to invest in treating this disease. Papillary thyroid cancer (PTC) is the most common thyroid cancer, which accounts for nearly 90% of all thyroid malignant tumors (2). Cervical lymph node metastases present at the time of diagnosis in 12%-81% of patients with PTCs (3). The spread of lymph node metastasis tends to progress from the central neck adjacent to thyroid to the lateral cervical compartments (4). Although controversy exists, most studies supported the prognostic significance of regional lymph node metastases in differentiated thyroid cancer (5–8). For patients with clinically apparent or biopsy-proven cervical lymph node metastasis (N1b), therapeutic neck dissection is routinely performed synchronously with thyroidectomy. For patients without metastasis to lateral neck, the role of routine prophylactic central neck dissection remains controversial. While some studies suggested that prophylactic dissection could improve disease-specific survival and local recurrence (9, 10), more other studies showed that prophylactic dissection had no improvement in locoregional recurrence but increased the likelihood of temporary morbidity (11–14). Before consensus has been reached, preoperative prediction of central cervical lymph node (CCLN) metastasis with adequate accuracy is valuable to avoid unnecessary central neck dissection in patients diagnosed as suspicious PTC or PTC in fine-needle aspiration (FNA).
Ultrasound (US) is the most important method to assess thyroid and cervical lymph nodes. However, the diagnostic efficiency of US in detecting CCLN metastasis is poor than that in lateral cervical lymph node (LCLN). A meta-analysis including 19 studies reported the pooled sensitivity, specificity, diagnostic odds ratio and area under curve of US in detecting CCLN metastasis to be 0.33, 0.93, 5.63, and 0.69, respectively; and LCLN metastasis to be 0.70, 0.84, 18.7 and 0.88, respectively (15). Nevertheless, US alone is not accurate enough for preoperative assessment of CCLN metastasis.
BRAF mutation is the most common genetic alteration in thyroid cancer, with incidence ranging from approximate 30% to more than 80% (16, 17). As one form of Raf kinases, BRAF is the most potent activator of the MAP kinase pathway, which plays an important role in tumorigenesis (18, 19). The diagnostic and prognostic value of BRAF mutation in thyroid cancer has been well documented (16). Recently, numerous studies investigated the association between BRAF mutation and (central) cervical lymph node metastasis in thyroid cancer. Some studies demonstrated BRAF mutation was correlated with (central) cervical lymph node metastasis (20, 21), while some others obtained the opposite conclusion (22–24). Therefore, this study aimed to investigate the association between CCLN metastasis and factors including clinical characteristics, US findings of thyroid and cervical lymph node, and BRAF mutation in PTC, and then develop a model to predict the presence of CCLN metastasis in FNA reporting suspicious PTC or PTC without lateral neck metastasis.
Patients and Methods
Patient Selection
Consecutive inpatients who had US-guided FNA reporting suspicious PTC or PTC (25) and underwent partial or total thyroidectomy and CCLN dissection between May 1st, 2016 and June 30th, 2018 were retrieved. The institutional review board had approved this retrospective study. The retrieved patients were reviewed for eligibility. The inclusion criteria included: 1) histologically confirmed PTC, 2) detection of BRAF mutation for thyroid lesions with specimens from preoperative FNA, 3) underwent preoperative US examination of thyroid and neck. The exclusion criteria included: 1) imaging suspicious or FNA confirmed LCLN metastasis, 2) CCLN metastasis data was missing, 3) BRAF mutation data was missing, 4) US images were missing. The flow chart of patient selection was showed in Figure 1.
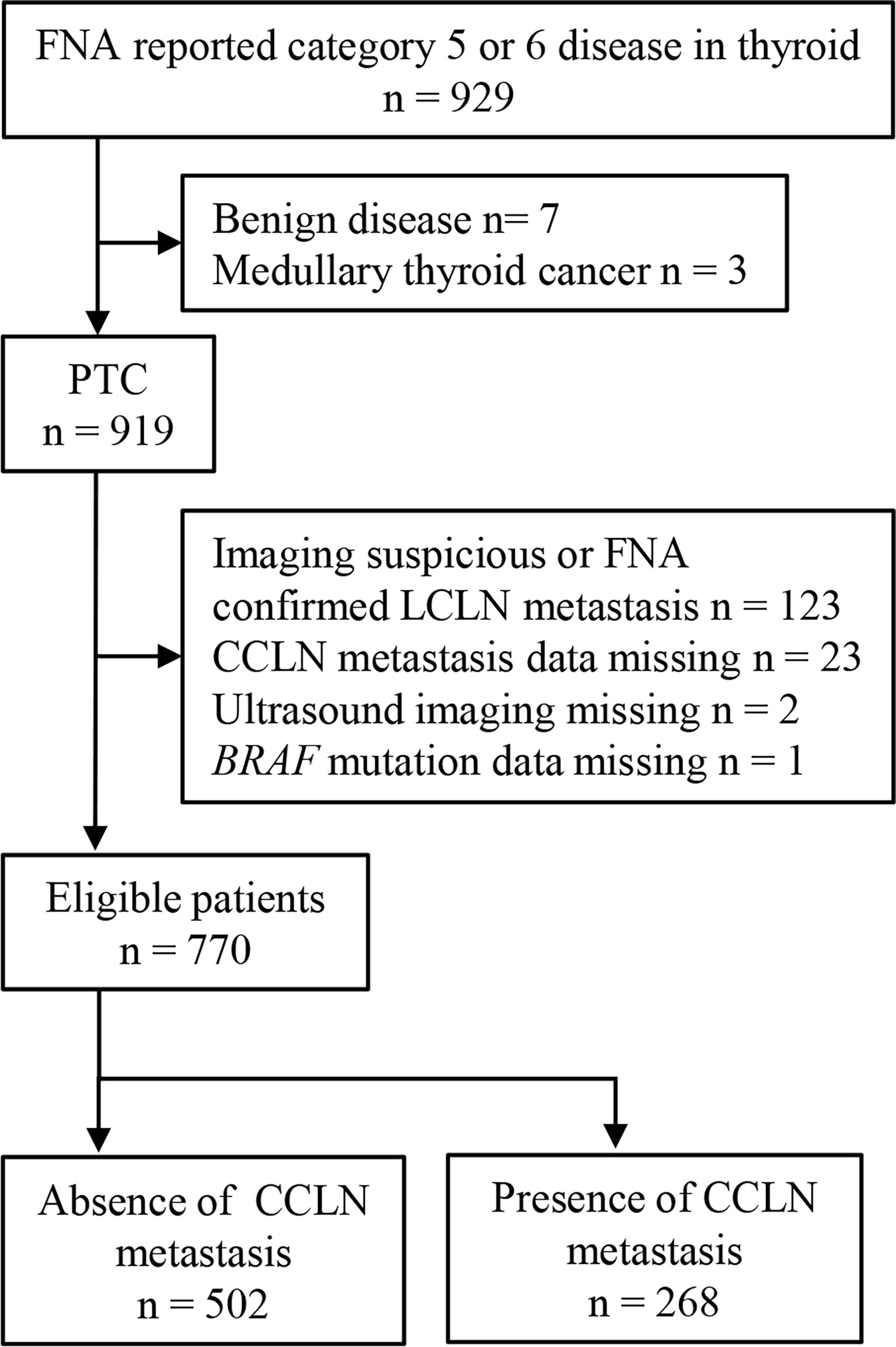
Figure 1 The flow chart of patient selection.
US Examination of Thyroid and Neck
US examination of thyroid and neck was conducted with Logic E9 (GE Healthcare, Kretz, Zipf, Austria), IU22 (Philips Medical Systems, Bothell, WA), Aixplorer (Supersonic Imaging, Aix-en-Provence, France), Aplio 500 (Toshiba medical system, Japan), and Mylab90 (Esaote, Genoa, Italy) equipped with a 5–14-MHz linear-array transducer. First, the grey-scale images of the neck were obtained for thorough evaluation of the neck anatomy, including surrounding vasculature, major salivary glands, cervical lymph nodes, and thyroid. The cervical lymph node is divided into seven levels according to their anatomic location. The CCLNs refer to the level VI and VII, whereas the LCLNs include level I, II, III, IV, and V (26). Lymph node with any of following features was considered as positive for metastasis: hypoechoic, rounded, absence of fatty hilum, cystic or partially cystic, and/or microcalcifications. For thyroid, a suspected malignant nodule was carefully evaluated for the following features: 1) size, 2) location (upper 1/3, middle 1/3, lower 1/3, isthmus), 3) component (solid, cystic-solid), 4) echogenicity (hypoechoic, iso/hyperechoic), 5) margin (circumscribed, not circumscribed), 6) shape (round/oval, irregular), 7) ratio of tall to wide (less than 1, equal/more than 1), 8) calcification (no/macrocalcification, microcalcification), 9) capsule involvement (less than 1/4 involved, equal or more than 1/4 involved), 10) depth (dorsal, ventral), 11) multifocality (solitary, multiple in unilateral lobe, multiple in bilateral lobes). Calcification in a thyroid nodule with size equal or less than 1.5 mm was defined as microcalcification, otherwise macrocalcification. Multiple nodules were defined as more than one solitary suspected malignant nodules in thyroid. In the setting of multiple nodules, the US feature of thyroid nodule was extracted from the most suspicious one, which was indicated by the malignant radiologic features or growth pattern over time.
US-Guided FNA Biopsy
The suspicious nodule in thyroid and neck was directed to US-guided FNA biopsy. Standard 21- or 23- gauge injection needles were used for FNA biopsy. Three to four passes per target nodule were made at the discretion of operator; two passes for cytologic diagnosis and one or two passes for BRAF mutation analysis. For both unilateral and bilateral multiple nodules in the thyroid, only the most suspicious was directed as target nodule. Specimens for cytologic diagnosis were evaluated by pathologist special for cytopathology and the results were reported according to The Bethesda system (25).
BRAF Mutation Analysis
BRAF V600E mutation analysis was conducted in the Pathology Department. Briefly, the DNA of specimens from FNA biopsy was extracted. Real-time PCR was performed using the BioRad-CFX96 real-time PCR system (Bio-Rad, Hercules, CA, USA). The mutant BRAF gene (encoding BRAF V600E) was amplified with specific primers. Thermal cycling conditions were initial denaturation of 1 cycle for 5 minutes at 95°C, followed by 15 cycles of 95°C for 25 s, 64°C for 20 s, and 72°C for 20 s with a final step of annealing and elongation of 31cycles at 93°C for 25 s, 60°C for 35 s and 72°C for 20 s. The BRAF V600E mutation status of each primary PTC was determined using the Human BRAF Gene V600E Mutation Fluorescence Polymerase Chain Reaction (PCR) Diagnostic Kit (Amoy Diagnostics). The FAM signals of the mutation detection system indicate the mutation status of the sample. The HEX/VIC signals indicate the internal control status. The FAM Ct value was checked for each sample: a) If the sample FAM Ct value ≥27, the sample was classified as negative or below the detection limit of the kit. b) If the sample FAM Ct value < 27, the sample was classified as mutation positive. In the end, the run files were interpreted according to the manufacturer’s instruction.
Criteria for Thyroidectomy and Central Neck Dissection
Total thyroidectomy and bilateral central neck dissection were performed in patients with bilateral thyroid cancer. For patients with unilateral cancer, the extent of thyroid surgery and ipsilateral central neck dissection were decided at the discretion of operator before the operation.
Statistical Analysis
The end-point event of this study was CCLN metastasis. For bilateral cancer, only the CCLNs ipsilateral to the FNA-targeted nodule was analyzed. The total group of patients was randomly divided into a training set and an internal validation set with the ratio of 7:3. The predicting model was developed using the training set. Univariate analysis with Chi-squared test was used to identify the variables correlated with CCLN metastasis. Factors significantly correlated with CCLN metastasis in the univariate analysis were included in the multivariate analysis, which was conducted with logistic regression analysis. Factors with p < 0.05 in the regression analysis were used to build the predicting model. The efficacy of this model was evaluated with area under the curve (AUC), sensitivity, specificity and accuracy and validated in the validation set. All tests were two-sided, and p < 0.05 indicated statistical significance. The SPSS version 19.0 (IBM Corp., Armonk, NY, USA) software was used for all statistical analysis.
Results
Patient Characteristics
A total of 770 patients, including 580 (75.3%) females and 190 (24.7%) males, with median age of 44 years (range 22 - 80 years) were eligible for this study. Among them, 251 (32.6%) patients were accompanied with Hashimoto’s thyroiditis. Five hundred and fifty-three (71.8%) patients had one solitary tumor, whereas unilateral multiple tumors were found in 71 (9.2%) patients, and bilateral multiple tumors in 146 (19.0%) patients. The median size of tumors was 8 mm (range 3 -53 mm). BRAF mutation presented in 642 (83.4%) tumors. Only 79 (10.3%) patients presented suspicious CCLN metastasis in US. Total thyroidectomy was performed in 192 (24.9%) patients, partial thyroidectomy in the remaining patients. All patients accepted central neck dissection. After surgery, 268 (34.8%) patients had histologically confirmed CCLN metastasis, while the remaining (65.2%) patients did not. The mean number of removed lymph nodes was 4.2 (range 1 to 30), and mean number of positive lymph nodes was 2.1 (range 1 to 11). Five hundred and forty-six patients (70.9% of 770) were allocated into the training set. The patient characteristics in the training set were in good agreement with that in the validation set except slightly difference in the tumor location (Table 1).
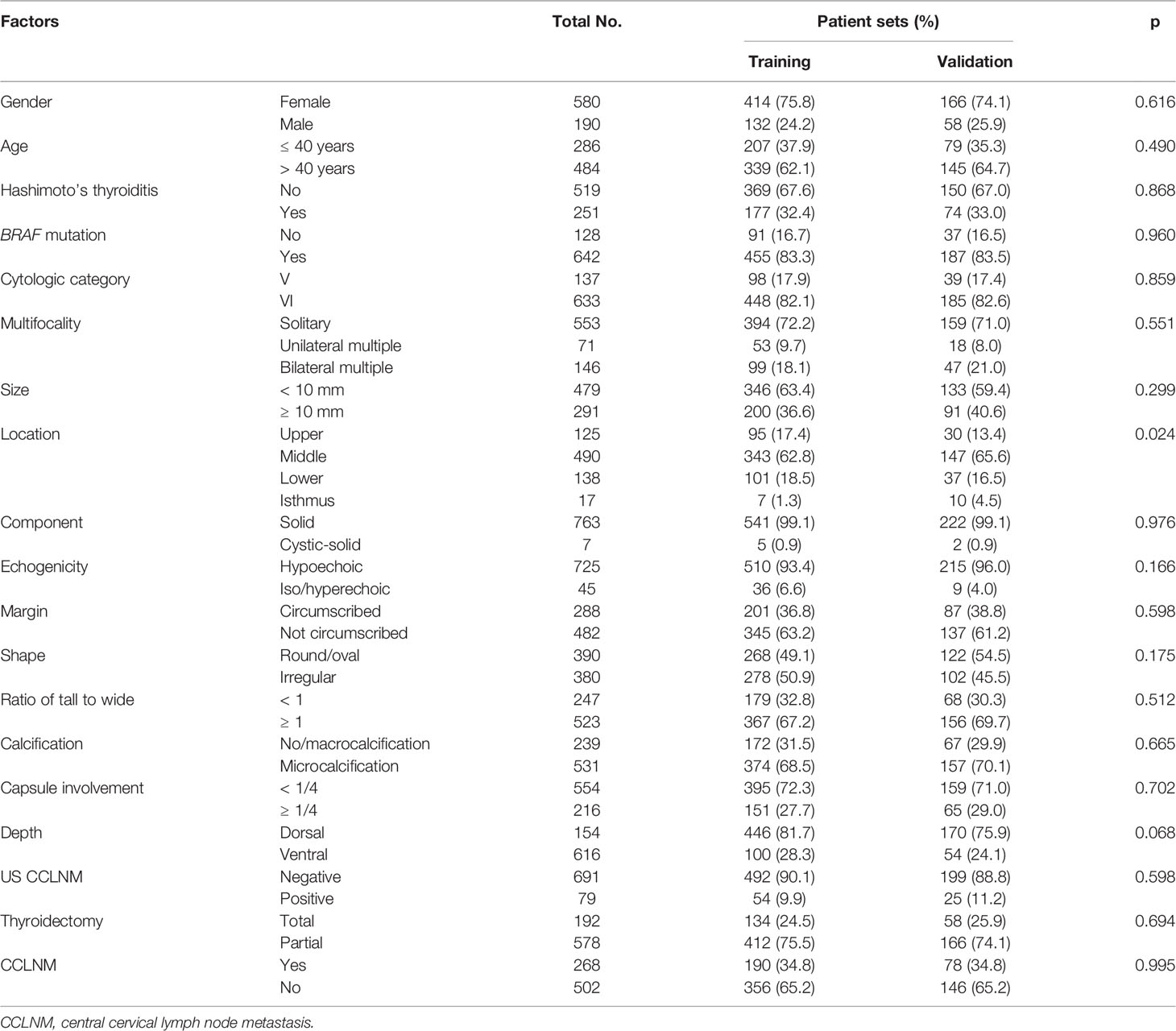
Table 1 Patient characteristics.
Univariate Analysis
The association between CCLN metastasis and 17 factors including gender, age, accompanied with Hashimoto’s thyroiditis or not, BRAF mutation status, cytologic category, multifocality, size, location, component, echogenicity, margin, shape, ratio of tall to wide, calcification, capsule involvement, depth, and US CCLN status was analyzed (Table 2). The results indicated that 10 factors including gender, age, BRAF mutation status, cytologic category, multifocality, size, ratio of tall to wide, calcification, capsule involvement, and US CCLN status were significantly associated with CCLN metastasis.
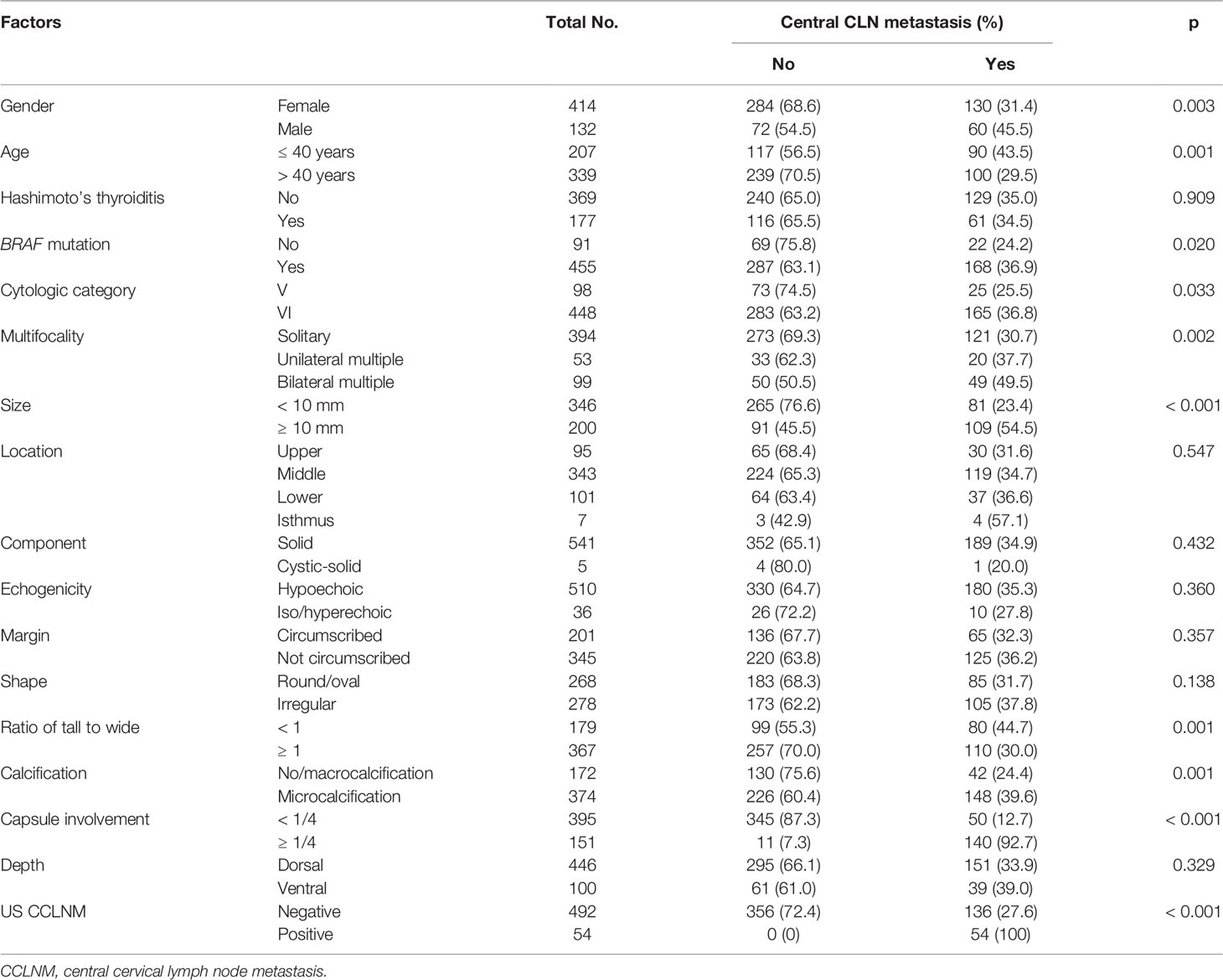
Table 2 Univariate analysis.
Multivariate Analysis
Factors significantly correlated with CCLN metastasis in the univariate analysis were included in the multivariate analysis. The results showed that age, BRAF mutation status, multifocality, size, and capsule involvement were the independent predictor of CCLN metastasis (Table 3). However, the calculated 95%CI of odds ratio (OR) for US CCLN status ranges from 0 to ∞ due to absence of patient positive for US CCLN status but without pathological confirmed CCLN metastasis (Table 2). Besides, US is the most important way to evaluate cervical lymph nodes in clinical. Therefore, US CCLN status was still included in the predicting model.
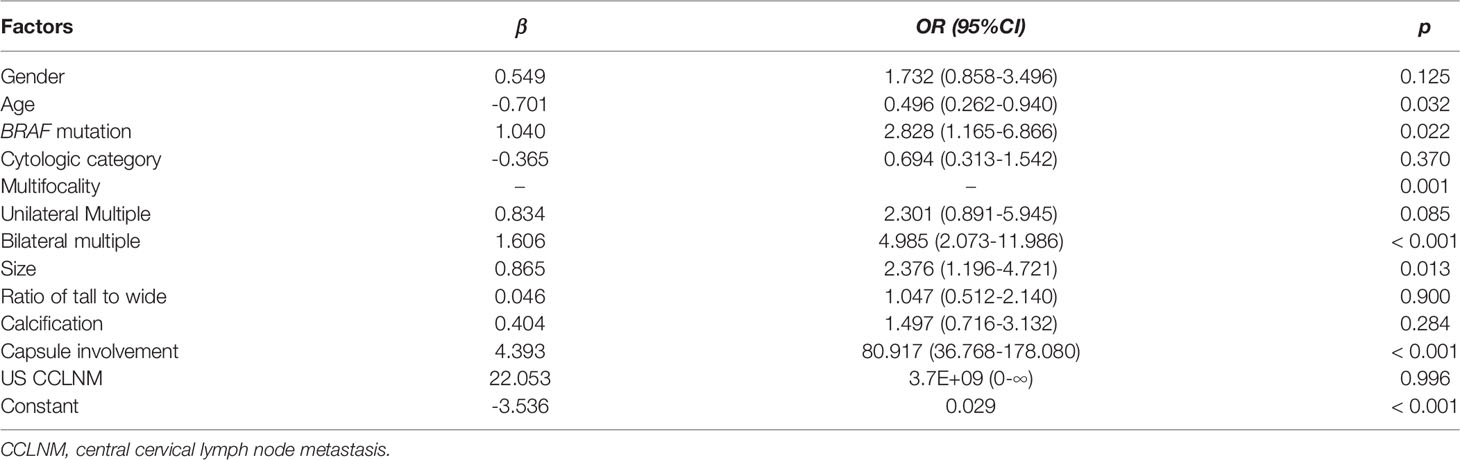
Table 3 Multivariate analysis.
Model Construction and Evaluation of Its Efficiency
The independent predictors and US CCLN status were put into the logistic regression analysis to build a predicting model (Table 4). Thus, the following model was built:
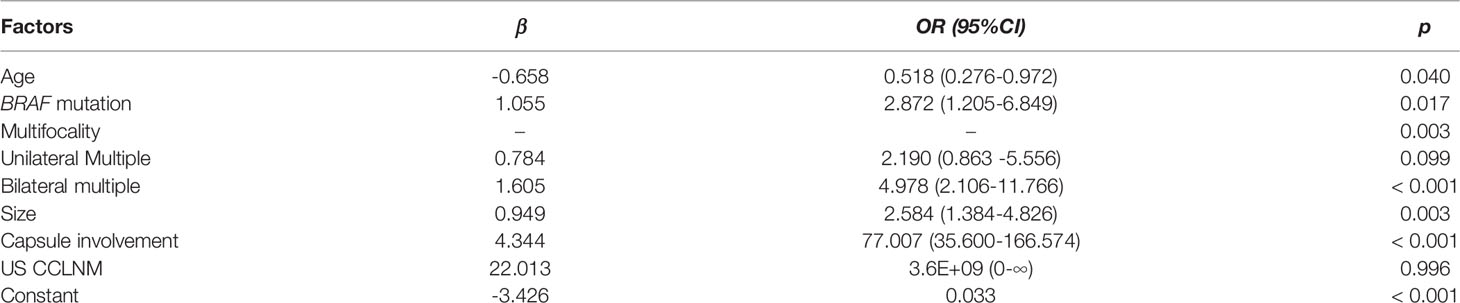
Table 4 Model based on the independent predictors.
in which, p denotes the probability of CCLN metastasis, x1 denotes age > 40 years, x2 denotes BRAF mutation, x3 denotes unilateral multiple tumors, x4 denotes bilateral multiple tumors, x5 denotes size ≥ 10 mm, x6 denotes capsule involvement, x7 denotes positive US CCLN.
The AUC of this model in predicting CCLN metastasis in the training set was 0.933 (95%CI: 0.905-0.960, p < 0.001). With the optimum cutoff of 0.465, the sensitivity, specificity and accuracy of this model were 0.816, 0.966 and 0.914, respectively. When validated in the internal validation set, the modal yielded the AUC of 0.967 (95%CI: 0.943-0.991, p < 0.001) (Figure 2). And the sensitivity, specificity and accuracy of this model in the validation set were 0.897, 0.959 and 0.936, respectively.
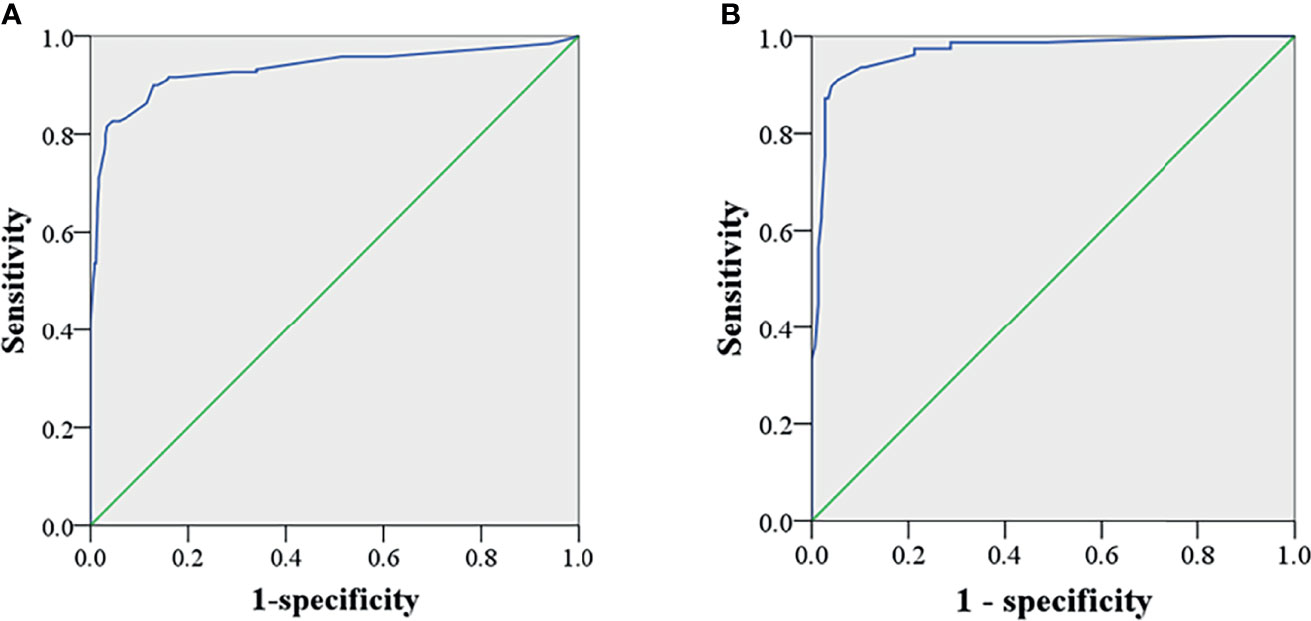
Figure 2 ROC of the test and validation set. The AUC was 0.933 (95%CI: 0.905-0.960, p < 0.001) and 0.967 (95%CI: 0.943-0.991, p < 0.001) in the training (A) and the internal validation set (B), respectively.
Discussion
The supposed benefit of prophylactic CCLN dissection in thyroid cancer without metastasis to lateral neck includes local-recurrence prevention and improved long-term survival. However, although several meta-analyses showed reduction in the risk of local-recurrence in thyroid cancer with prophylactic central neck dissection, they all stated that the surgical morbidity should not be overlooked (27–29). Furthermore, a previous prospective study showed no outcome advantage but reduction in the rate of radioiodine treatment for prophylactic central neck dissection after 5-year’s follow-up (12). The evidence quality is low, so that prophylactic central neck dissection for advanced thyroid cancer such as T3 or T4 or cN1b disease was stated as weak recommendation in the latest management guidelines of American thyroid association for differentiated thyroid cancer published in 2016 (30). Therefore, it would be more rational to perform central neck dissection in selective thyroid cancer with high risk of CCLN metastasis.
Unfortunately, to date no non-invasive imaging method can confidently classify cervical lymphadenopathy as metastasis, especially for CCLNs because they may be obstructed by the thyroid. In this study, the sensitivity of US alone for detection of CCLN metastasis was only 29.5% (79/268), though the specificity was 100% (502/502), which are comparable with previous report (15). A recent meta-analysis demonstrated that computed tomography performed poorly as US did in identifying the presence of CCLN metastasis (31). In view of the low efficiency of unimodal imaging, we tried to develop a model incorporating factors of clinicopathology, imaging and gene mutation that could be determined preoperatively to predict the CCLN metastasis. Finally, a simple predicting model was successfully built and yielded AUC of 0.933 and 0.967 in the training set and validation set, respectively, indicating the excellent discrimination and robustness of this model.
Several studies have developed various models to predict the CCLN metastasis in thyroid cancer (32–37). In comparison with these models, there are several advantages in our study. Firstly, the outward spread mode of metastasis indicates that 1) patients with LCLN metastasis are very likely accompanied with CCLN metastasis, 2) patients without LCLN metastasis may have CCLN metastasis with unknown possibility. Published data showed that patients with concurrent LCLN and CCLN metastasis accounted more than 70% of patients (155/211, ref. 37) with LCLN metastasis. Consequently, patients with suspicious or confirmed LCLN metastasis almost always undergo neck dissection covering lateral and central cervical compartment in clinical. The controversy in clinical right now is that whether there is a need to undergo central neck dissection in patients without evidence of LCLN metastasis. Patients with suspicious or confirmed LCLN metastasis therefore were excluded in our study, but not in other previous studies, making the focus of our study more relevant to the clinical problem. Secondly, our model incorporated not only clinicopathological and imaging factors commonly included in previous studies, but also BRAF gene mutation. Thirdly, BRAF mutation status was determined with specimens from the preoperative FNA biopsy. Therefore, all factors included in this model could be determined preoperatively, making it a real tool to preoperatively predict the status of CCLN metastasis. Finally, this simple model showed more excellent discrimination in both the training set and internal validation set than most previous models.
One interesting finding in this study is that CCLN metastasis was less likely to present in older patients with PTC, which was similar to previous reports (37, 38). This indicates that thyroid cancer may be more inert in old patients than in young counterparts, although the molecular mechanism is unclear. However, the impact of lymph node metastasis on survival is more apparent in older patients, which is the reason for that the change of N stage changes the prognostic stage in old patients (with T1/M0 or T2/M0 disease), but not in young patients in the AJCC manual (26). In other words, lymph node metastasis occurs in a less probability in older patients; but once it occurs, it is more detrimental.
Consistent with previous studies (17, 37–39), factors such as larger size, multifocality and capsule involvement which indicate heavier tumor burden and invasiveness without out of expectation were independent predictors and included in the model. Besides, the results of this study also supported that BRAF mutation was significantly associated with CCLN metastasis in PTC. However, although gender and calcification were significantly correlated with CCLN metastasis in the univariate analysis, they did not show statistical significance in the multivariate analysis.
One confounder should be noted in this study is that only unilateral CCLN ipsilateral to the FNA-targeted nodule was analyzed in this study. However, for patients suffered from bilateral thyroid cancer, metastasis might come from contralateral disease; for patients with unilateral cancer, metastasis might skip to contralateral CCLNs. Although no study reports how often this would happen yet, we believe it occurs rarely and would result in little impact on the results. Other limitations of this study include lack of external validation and retrospective design.
In conclusion, this study demonstrated that age, BRAF mutation, multifocality, size, and capsule involvement were independent predictors of CCLN metastasis in FNA reporting suspicious PTC or PTC without lateral neck metastasis. A simple model was successfully built based on these factors and US CCLN status and shown excellent discrimination to distinguish FNA reporting suspicious PTC or PTC with or without CCLN metastasis.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Ethics Statement
The studies involving human participants were reviewed and approved by Ethics Committee of Fudan University Shanghai Cancer Center. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author Contributions
KZ, conception, writing and supervision. LQ, writing, data collection and analysis. JC, writing and data analysis. QZ and CC, data collection and review. All authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Du L, Li R, Ge M, Wang Y, Li H, Chen W, et al. Incidence and Mortality of Thyroid Cancer in China, 2008–2012. Chin J Cancer Res (2019) 31(1):144–51. doi: 10.21147/j.issn.1000-9604.2019.01.09
2. Yang L, Zheng RS, Wang N, Zeng HM, Yuan YN, Zhang SW, et al. Analysis of Incidence and Mortality of Thyroid Cancer in China, 2013. Zhonghua zhong liu za zhi [Chinese J Oncol] (2017) 39(11):862–7. doi: 10.3760/cma.j.issn.0253-3766.2017.11.010
3. Randolph GW, Duh QY, Heller KS, LiVolsi VA, Mandel SJ, Steward DL, et al. The Prognostic Significance of Nodal Metastases From Papillary Thyroid Carcinoma Can be Stratified Based on the Size and Number of Metastatic Lymph Nodes, as Well as the Presence of Extranodal Extension. Thyroid Off J Am Thyroid Assoc (2012) 22(11):1144–52. doi: 10.1089/thy.2012.0043
4. Hughes DT, Doherty GM. Central Neck Dissection for Papillary Thyroid Cancer. Cancer Control J Moffitt Cancer Center (2011) 18(2):83–8. doi: 10.1177/107327481101800202
5. Adam MA, Pura J, Goffredo P, Dinan MA, Reed SD, Scheri RP, et al. Presence and Number of Lymph Node Metastases Are Associated With Compromised Survival for Patients Younger Than Age 45 Years With Papillary Thyroid Cancer. J Clin Oncol Off J Am Soc Clin Oncol (2015) 33(21):2370–5. doi: 10.1200/JCO.2014.59.8391
6. Nixon IJ, Wang LY, Palmer FL, Tuttle RM, Shaha AR, Shah JP, et al. The Impact of Nodal Status on Outcome in Older Patients With Papillary Thyroid Cancer. Surgery (2014) 156(1):137–46. doi: 10.1016/j.surg.2014.03.027
7. Schneider DF, Chen H, Sippel RS. Impact of Lymph Node Ratio on Survival in Papillary Thyroid Cancer. Ann Surg Oncol (2013) 20(6):1906–11. doi: 10.1245/s10434-012-2802-8
8. Bhattacharyya N. A Population-Based Analysis of Survival Factors in Differentiated and Medullary Thyroid Carcinoma. Otolaryngology–Head Neck Surg Off J Am Acad Otolaryngol-Head Neck Surg (2003) 128(1):115–23. doi: 10.1067/mhn.2003.2
9. Barczynski M, Konturek A, Stopa M, Nowak W. Prophylactic Central Neck Dissection for Papillary Thyroid Cancer. Br J Surg (2013) 100(3):410–8. doi: 10.1002/bjs.8985
10. Hartl DM, Mamelle E, Borget I, Leboulleux S, Mirghani H, Schlumberger M. Influence of Prophylactic Neck Dissection on Rate of Retreatment for Papillary Thyroid Carcinoma. World J Surg (2013) 37(8):1951–8. doi: 10.1007/s00268-013-2089-3
11. Raffaelli M, De Crea C, Sessa L, Giustacchini P, Revelli L, Bellantone C, et al. Prospective Evaluation of Total Thyroidectomy Versus Ipsilateral Versus Bilateral Central Neck Dissection in Patients With Clinically Node-Negative Papillary Thyroid Carcinoma. Surgery (2012) 152(6):957–64. doi: 10.1016/j.surg.2012.08.053
12. Viola D, Materazzi G, Valerio L, Molinaro E, Agate L, Faviana P, et al. Prophylactic Central Compartment Lymph Node Dissection in Papillary Thyroid Carcinoma: Clinical Implications Derived From the First Prospective Randomized Controlled Single Institution Study. J Clin Endocrinol Metab (2015) 100(4):1316–24. doi: 10.1210/jc.2014-3825
13. Dobrinja C, Troian M, Cipolat Mis T, Rebez G, Bernardi S, Fabris B, et al. Rationality in Prophylactic Central Neck Dissection in Clinically Node-Negative (Cn0) Papillary Thyroid Carcinoma: Is There Anything More to Say? A Decade Experience in a Single-Center. Int J Surg (2017) 41(Suppl 1):S40–S7. doi: 10.1016/j.ijsu.2017.01.113
14. Kim SK, Woo JW, Lee JH, Park I, Choe JH, Kim JH, et al. Prophylactic Central Neck Dissection Might Not Be Necessary in Papillary Thyroid Carcinoma: Analysis of 11,569 Cases From a Single Institution. J Am Coll Surg (2016) 222(5):853–64. doi: 10.1016/j.jamcollsurg.2016.02.001
15. Zhao H, Li H. Meta-Analysis of Ultrasound for Cervical Lymph Nodes in Papillary Thyroid Cancer: Diagnosis of Central and Lateral Compartment Nodal Metastases. Eur J Radiol (2019) 112:14–21. doi: 10.1016/j.ejrad.2019.01.006
16. Xing M. BRAF Mutation in Thyroid Cancer. Endocr Relat Cancer (2005) 12(2):245–62. doi: 10.1677/erc.1.0978
17. Zheng X, Peng C, Gao M, Zhi J, Hou X, Zhao J, et al. Risk Factors for Cervical Lymph Node Metastasis in Papillary Thyroid Microcarcinoma: A Study of 1,587 Patients. Cancer Biol Med (2019) 16(1):121–30. doi: 10.20892/j.issn.2095-3941.2018.0125
18. Mercer KE, Pritchard CA. Raf Proteins and Cancer: B-Raf Is Identified as a Mutational Target. Biochim Biophys Acta (2003) 1653(1):25–40. doi: 10.1016/s0304-419x(03)00016-7
19. Peyssonnaux C, Eychene A. The Raf/MEK/ERK Pathway: New Concepts of Activation. Biol Cell (2001) 93(1-2):53–62. doi: 10.1016/s0248-4900(01)01125-x
20. So YK, Son YI, Park JY, Baek CH, Jeong HS, Chung MK. Preoperative BRAF Mutation Has Different Predictive Values for Lymph Node Metastasis According to Tumor Size. Otolaryngol–Head Neck Surg Off J Am Acad Otolaryngol-Head Neck Surg (2011) 145(3):422–7. doi: 10.1177/0194599811404649
21. Kim SK, Lee JH, Woo JW, Park I, Choe JH, Kim JH, et al. BRAF V600E Mutation: Differential Impact on Central Lymph Node Metastasis by Tumor Size in Papillary Thyroid Carcinoma. Head Neck (2016) 38(Suppl 1):E1203–9. doi: 10.1002/hed.24192
22. Han PA, Kim HS, Cho S, Fazeli R, Najafian A, Khawaja H, et al. Association of BRAF V600E Mutation and MicroRNA Expression With Central Lymph Node Metastases in Papillary Thyroid Cancer: A Prospective Study From Four Endocrine Surgery Centers. Thyroid Off J Am Thyroid Assoc (2016) 26(4):532–42. doi: 10.1089/thy.2015.0378
23. Lee KC, Li C, Schneider EB, Wang Y, Somervell H, Krafft M, et al. Is BRAF Mutation Associated With Lymph Node Metastasis in Patients With Papillary Thyroid Cancer? Surgery (2012) 152(6):977–83. doi: 10.1016/j.surg.2012.08.019
24. Guo L, Ma YQ, Yao Y, Wu M, Deng ZH, Zhu FW, et al. Role of Ultrasonographic Features and Quantified BRAFV600E Mutation in Lymph Node Metastasis in Chinese Patients With Papillary Thyroid Carcinoma. Sci Rep (2019) 9(1):75. doi: 10.1038/s41598-018-36171-z
25. Cibas ES, Ali SZ. The Bethesda System for Reporting Thyroid Cytopathology. Thyroid Off J Am Thyroid Assoc (2009) 19(11):1159–65. doi: 10.1089/thy.2009.0274
26. Amin MB ed. AJCC Cancer Staging Manual 8th Edition Springer. Thyroid -Differentiated and Anaplastic Carcinoma. Eighth ed. Chicago: Springer Nature (2017). p. 876. AJCC Cancer Staging Manual 8th Edition Springer.
27. Chen L, Wu YH, Lee CH, Chen HA, Loh EW, Tam KW. Prophylactic Central Neck Dissection for Papillary Thyroid Carcinoma With Clinically Uninvolved Central Neck Lymph Nodes: A Systematic Review and Meta-Analysis. World J Surg (2018) 42(9):2846–57. doi: 10.1007/s00268-018-4547-4
28. Zhao W, You L, Hou X, Chen S, Ren X, Chen G, et al. The Effect of Prophylactic Central Neck Dissection on Locoregional Recurrence in Papillary Thyroid Cancer After Total Thyroidectomy: A Systematic Review and Meta-Analysis : pCND for the Locoregional Recurrence of Papillary Thyroid Cancer. Ann Surg Oncol (2017) 24(8):2189–98. doi: 10.1245/s10434-016-5691-4
29. Lang BH, Ng SH, Lau LL, Cowling BJ, Wong KP, Wan KY. A Systematic Review and Meta-Analysis of Prophylactic Central Neck Dissection on Short-Term Locoregional Recurrence in Papillary Thyroid Carcinoma After Total Thyroidectomy. Thyroid Off J Am Thyroid Assoc (2013) 23(9):1087–98. doi: 10.1089/thy.2012.0608
30. Haugen BR, Alexander EK, Bible KC, Doherty GM, Mandel SJ, Nikiforov YE, et al. 2015 American Thyroid Association Management Guidelines for Adult Patients With Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid Off J Am Thyroid Assoc (2016) 26(1):1–133. doi: 10.1089/thy.2015.0020
31. Xing Z, Qiu Y, Yang Q, Yu Y, Liu J, Fei Y, et al. Thyroid Cancer Neck Lymph Nodes Metastasis: Meta-Analysis of US and CT Diagnosis. Eur J Radiol (2020) 129:109103. doi: 10.1016/j.ejrad.2020.109103
32. Sun J, Jiang Q, Wang X, Liu W, Wang X. Nomogram for Preoperative Estimation of Cervical Lymph Node Metastasis Risk in Papillary Thyroid Microcarcinoma. Front Endocrinol (Lausanne) (2021) 12:613974. doi: 10.3389/fendo.2021.613974
33. Zhou SC, Liu TT, Zhou J, Huang YX, Guo Y, Yu JH, et al. An Ultrasound Radiomics Nomogram for Preoperative Prediction of Central Neck Lymph Node Metastasis in Papillary Thyroid Carcinoma. Front Oncol (2020) 10:1591. doi: 10.3389/fonc.2020.01591
34. Chen J, Li XL, Zhang YF, Wang D, Wang Q, Zhao CK, et al. Ultrasound Validation of Predictive Model for Central Cervical Lymph Node Metastasis in Papillary Thyroid Cancer on BRAF. Future Oncol (2020) 16(22):1607–18. doi: 10.2217/fon-2020-0069
35. Yang Z, Heng Y, Lin J, Lu C, Yu D, Tao L, et al. Nomogram for Predicting Central Lymph Node Metastasis in Papillary Thyroid Cancer: A Retrospective Cohort Study of Two Clinical Centers. Cancer Res Treat (2020) 52(4):1010–8. doi: 10.4143/crt.2020.254
36. Kim KE, Kim EK, Yoon JH, Han KH, Moon HJ, Kwak JY. Preoperative Prediction of Central Lymph Node Metastasis in Thyroid Papillary Microcarcinoma Using Clinicopathologic and Sonographic Features. World J Surg (2013) 37(2):385–91. doi: 10.1007/s00268-012-1826-3
37. Liu C, Xiao C, Chen J, Li X, Feng Z, Gao Q, et al. Risk Factor Analysis for Predicting Cervical Lymph Node Metastasis in Papillary Thyroid Carcinoma: A Study of 966 Patients. BMC Cancer (2019) 19(1):622. doi: 10.1186/s12885-019-5835-6
38. Feng JW, Yang XH, Wu BQ, Sun DL, Jiang Y, Qu Z. Predictive Factors for Central Lymph Node and Lateral Cervical Lymph Node Metastases in Papillary Thyroid Carcinoma. Clin Transl Oncol (2019) 21(11):1482–91. doi: 10.1007/s12094-019-02076-0
Keywords: papillary thyroid cancer, thyroid cancer, cervical lymph node, lymph node metastasis, central neck dissection
Citation: Zhang K, Qian L, Chen J, Zhu Q and Chang C (2022) Preoperative Prediction of Central Cervical Lymph Node Metastasis in Fine-Needle Aspiration Reporting Suspicious Papillary Thyroid Cancer or Papillary Thyroid Cancer Without Lateral Neck Metastasis. Front. Oncol. 12:712723. doi: 10.3389/fonc.2022.712723
Received: 21 May 2021; Accepted: 28 February 2022;
Published: 23 March 2022.
Edited by:
Mitali Dandekar, Paras Cancer Centre, IndiaReviewed by:
Jie Tan, Huazhong University of Science and Technology, ChinaAvi Hefetz Khafif, Ben-Gurion University of the Negev, Israel
Fabio Medas, University of Cagliari, Italy
Copyright © 2022 Zhang, Qian, Chen, Zhu and Chang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Kai Zhang, emhhbmdrODZAZm94bWFpbC5jb20=
†These authors have contributed equally to this work and share first authorship