Abstract
Background:
Partial breast irradiation with Intra-operative radiotherapy (IORT) has become a popular management option as opposed to whole breast radiation using external beam radiotherapy for breast cancer patients. While previous studies have highlighted the use of IORT in breast cancer patients, there is a scarcity of literature on the use of IORT in those who also have ipsilateral pacemakers. Thus, the aim of our case report is to highlight the applicability of IORT in breast cancer patients who also have a pacemaker.
Case Reports:
Two female patients with an implanted dual-chamber pacemaker presented with a diagnosis of left-sided invasive ductal carcinoma on mammogram. Mammography of the left breast revealed a 10 mm and 7 mm spiculated mass, respectively, further confirmed with an ultrasound-guided core biopsy that was conclusive of clinical Stage I T1 N0 grade 2, ER +, PR + Her2 – invasive ductal carcinoma. They met our eligibility criteria for IORT, which is being performed as a registry trial. These patients underwent a wide excision lumpectomy along with IORT.
Conclusion:
Our findings underscore the successful use of targeted IORT for breast-conserving surgery in a patient with invasive ductal carcinoma and pacemaker, hence eliminating the necessity for relocating pacemaker surgeries in these patients. Furthermore, no device failure or malfunction for the pacemaker was recorded before, during, or after the surgery, demonstrating the safety of using IORT in patients with preinstalled pacemaker despite a lack of evidence on safe radiation dosage or manufacturer guidelines. Nonetheless, the effects of IORT on pacemaker < 10 cm were not studied in our patients and further clinical studies are recommended to reinforce the applicability and safe distance of IORT in breast cancer patients with pacemaker.
Introduction
Breast cancer is the most common newly diagnosed malignancy among women across the United States (1). Of all the cancers diagnosed in women, breast cancer accounts for about 1/3rd of the cases (2). The incidence of breast cancer increases roughly by 0.5% per year, and approximately 290,560 patients will be diagnosed with breast cancer in 2022 (1, 2). Nonetheless, many treatment options for breast cancer management have arisen over the years. While the majority of patients who opt for breast conservation receive whole-breast irradiation (WBI), there has been a change in preference toward partial breast irradiation (PBI) delivered over 5 days. Additionally, intra-operative radiotherapy (IORT) allows for a single dose to be administered at the time of lumpectomy. Furthermore, because of the intrinsic benefit of tissue preservation and breast conservation, IORT has become a popular choice for patients (3–6). Prior study by the TARGIT group has demonstrated that the short-range kilovoltage energy sources minimize the radiation dosage to normal tissues by eliminating the electromagnetic radiation and scattered radiation typical of external beam radiotherapy (EBRT) while also being safe and effective (7). A parallel randomized trial on 2298 patients by the same group found that TARGIT-IORT was non-inferior to EBRT, with a local recurrence rate of 2.11% for TARGIT-IORT vs. 0.95% for EBRT (8). Furthermore, using the same patients, the same group reported long-term outcomes evaluating the impact of tumor size, grade, receptor status, and lymph node status on local recurrence-free survival, as well as the impact of local recurrence on distant relapse and mortality (9). They found no difference in 5-year local recurrence-free survival between TARGIT-IORT and EBRT in any tumor subgroup. Additionally, they reported that TARGIT-IORT significantly reduced non-breast cancer mortality, even when patients received supplemental EBRT, with a Hazard Ratio (HR) of 0.38 (95% CI 0.17–0.88, p = 0.0091) (9).
A caveat to the use of IORT is presumed to be patients with preinstalled cardiac pacemakers. This may relate to the fact that the ionizing radiation interferes with the modern cardiac pacemaker that has complementary metal oxide semiconductor circuitry (CMOS). The number of cardiac pacemakers implanted worldwide has increased dramatically, from approximately half a million in 2002 to nearly a million in 2016 (10–12). In the United States, approximately 200,000 pacemakers are implanted in bradycardic patients each year (13). In an older population, the increasing overlap between these two groups is anticipated to contribute to an increase in the number of instances involving people with pacemaker and breast cancer (12). There is a paucity of literature looking at the use of IORT in patients with pacemakers, and the manufacturers are less likely to conduct cardiac pacemaker testing with various IORT devices due to a large number of devices available on the market for both (14). Thus, our case reports aim to highlight the applicability of IORT in breast cancer patients who also have a pacemaker on the same side.
Case Reports
Patient 1
An 82-year-old female presented with a lump in her left breast for 1-month post-dual-chamber pacemaker implantation for sinus bradycardia. Mammography of the left breast revealed a 10 mm spiculated mass noted in the middle depth of the left breast at approximately the 2:00 axis (Figure 1). Subsequently, an ultrasound guided core biopsy revealed clinical Stage I T1 (10 mm) N0 grade 2, ER +, PR + Her2 – invasive ductal carcinoma. She had a PMHx of chronic kidney disease, diabetes mellitus, hypercholesterolemia, hypertension, hypothyroidism, venous insufficiency, and a dual-lead pacemaker (DDD mode, model Biotronik type Edora DR-T ProMRI) implanted for sinus bradycardia. The pacemaker was programed to a lower rate of 60 bpm and a maximum of 130 bpm. The pacemaker was placed anatomically in a subcutaneous pocket in the upper pole of the left breast, 10 cm away from the primary tumor.
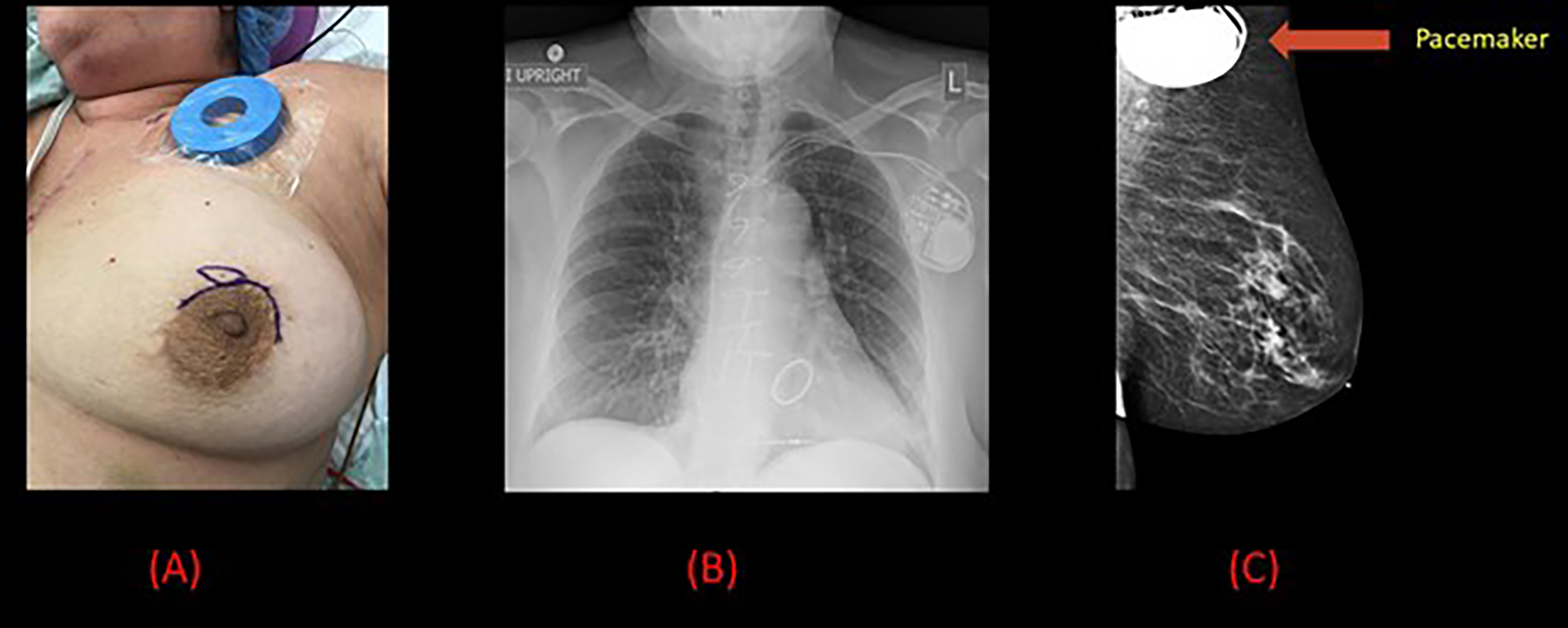
Figure 1

Pre-operative and radiological images for patient 1. (A) Pre-operative image of the left breast with the location of the pacemaker marked by a circle in the superior portion close to the neck and the inferior circle indicates the presence of radiological seed. (B) Chest x-ray demonstrating left sided pacemaker with dual leads projecting over the right atrium and right ventricle. (C) Mammogram demonstrating a 10 mm spiculated mass in the left breast along with the pacemaker.
During the multidisciplinary meeting, the patient’s condition was discussed. Due to the proximity of the tumor to the pacemaker, and keeping the patient’s comorbidities in mind, it was collectively decided that a localized left breast lumpectomy along with targeted IORT will be offered.
The IORT would be delivered by the intrabeam system using targeted intraoperative radiotherapy (TARGIT) technique which is administering IORT through a spherical applicator placed in the tumor bed for a time duration determined by the applicator’s diameter (15). As a result, IORT avoids the requirement for the pacemaker to be relocated, which would have been necessary prior to external beam radiotherapy. Prior to the surgery, she underwent placement of an iodine-125 seed by Radiology under mammographic guidance to localize the tumor and sentinel lymph node biopsy was not performed since it would not affect her management.
Wide local excision was performed and TARGIT-IORT was delivered during surgery using the Intrabeam 600 (Zeiss, Oberkochen, Germany) (Figure 2). Ultrasound was then used to measure the distance from the applicator to the skin with the closest bridge being inferior at 10.6 mm. IORT was delivered with a 40-mm diameter spherical applicator, delivering 20 Gy to the surface of the surgical margin in direct contact with the applicator for a duration of 25 minutes. In vivo dosimetry was performed by placing an optically stimulated luminescence dosimeter (OSLD) under the radiation shield on the skin surface in close proximity to the pacemaker site during treatment. The measured absorbed dose resulting from the Zeiss INTRABEAM IORT system radiation on the skin surface in close proximity to the pacemaker site was measured to be 0.23 Gy, using the same methodology described previously by our group (16).
Figure 2
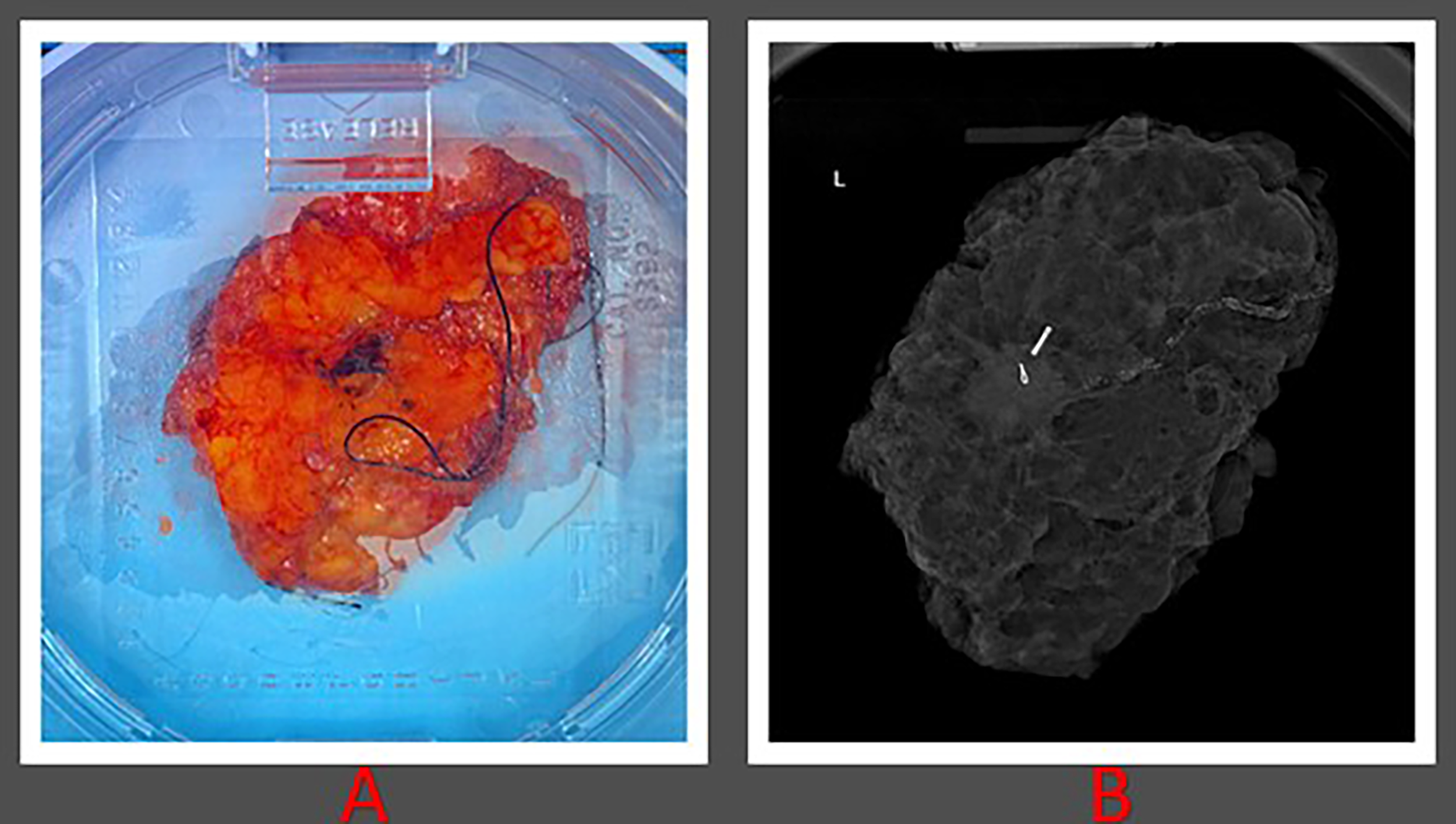
Histopathological images of patient 1. (A) Gross lumpectomy specimen measuring 10 cm in dimension extending from superior to inferior margin and measuring 6.2 cm extending from lateral to medial margin. (B) Lumpectomy specimen with presence of radiological seed.
The surgery and TARGIT procedure were both successful. The patient tolerated the procedure very well, and there was no malfunction of the pacemaker device throughout the surgery or IORT. The patient made an uneventful recovery and was sent home the same day. Histology confirmed the presence of an 18 mm grade 2 invasive ductal carcinoma with admixed lobular features that had been fully removed with clear margins. The tumor tested positive for ER/PR but negative for Her-2. As part of her adjuvant endocrine therapy, a treatment plan with aromatase inhibitor was decided.
Patient 2
A 64-year-old female with a history of surgically managed right invasive lobular carcinoma with lumpectomy, sentinel lymph node biopsy, and whole breast radiation 6 years back presented with an incidental finding of a 7 mm spiculated mass in the anterior to middle depth at 12:00 axis of the left breast on a routine follow-up mammogram (Figure 3). An ultrasound guided core biopsy revealed clinical stage I T1 (7 mm) N0 grade 2, ER +, PR + Her2 – invasive ductal carcinoma and a focal ductal carcinoma in situ (DCIS), nuclear grade 2, cribriform type. The patient also had a history of atrial fibrillation, hepatitis C, asthma, chronic obstructive pulmonary disease (COPD), mitral stenosis, pulmonary hypertension, mitral valve replacement, cerebrovascular accident, and dual-lead pacemaker (DDD mode, model Medtronic type AZURE XT DR MRI) implanted for Mobitz type II heart block. The pacemaker was programed to a lower rate of 60 bpm and a maximum of 130 bpm. Anatomically, the pacemaker was placed in a subcutaneous pocket in the upper pole of the left breast, 10 cm away from the primary tumor.
Figure 3
Pre-operative and radiological images for patient 2. (A) Pre-operative image of the left breast with a magnet placed on the pacemaker and surgical marking indicating the tumor site. (B) Chest x-ray demonstrating left sided pacemaker with leads projecting over the right atrium and right ventricle. (C) Mammogram demonstrating a 7 mm spiculated mass in the left breast along with the pacemaker.
Patient underwent wide local excision followed by TARGIT-IORT during surgery delivered with the help of an Intrabeam 600. The distance from the applicator to the skin was then measured using ultrasound, with the closest bridge being inferior at 20 mm. IORT was delivered with using a 35-mm diameter spherical applicator, which delivered 20 Gy to the surface of the surgical margin in direct contact with the applicator for a duration of 16 minutes. During treatment, an OSLD was placed on the skin surface beneath the radiation shield, close to the pacemaker site, for in vivo dosimetry. The measured absorbed dose from the Intrabeam IORT system radiation on the skin surface near the pacemaker site was estimated to be 0.185 Gy.
Both the surgery and the TARGIT procedures were successful. The procedures were well tolerated by the patient, and there was no malfunction of the pacemaker device during surgery or IORT. The patient made an uneventful recovery and was discharged the same day. Histology confirmed the presence of a 12 mm grade 2 invasive micropapillary carcinoma excised with clear margins. The tumor tested positive for ER/PR but negative for Her-2.
Discussion
The effect of radiation therapy on implanted electronic devices such as pacemaker is difficult to estimate (17, 18). The dose contribution from scatter during radiotherapy with high-energy megavoltage beams, are the primary concern for pacemakers if they are not directly in the radiation treatment field. Radiation often affects the device’s random access memory (RAM), which can have a detrimental influence on device function and, in higher amounts, may permanently damage electrical components (19). However, this is rarely seen unless the device is in close proximity to radiation. Radiation-induced electromagnetic interference may shut the magnetic reed switch, resulting in an unanticipated reversion to an OFF mode, necessitating restoration to therapy mode (19). Because of these concerns, EBRT utilization is not recommended in the proximity of the pacemaker, with many surgeons choosing to remove the complete system and reimplant on the opposite side to clear the area for surgery and eventual radiation therapy, despite the risk of lead extraction (20–23). Contrastingly, few prefer to reimplant the pacemaker from the prepectoral pocket into the neck pocket via small cervicotomy, which allows the device to be far away from the radiation site (24). Many of these concerns are bridged by the use of IORT. Since most pacemaker are placed on the left side, the findings of our study underscore the utility of IORT, particularly in the management of the left sided breast cancer.
Another limitation for the use of EBRT is increased non-breast cancer related mortality rate when compared to TARGIT-IORT (8). WBI has proven to have an increased incidence of second cancers and heart diseases (25–27). The incidence of lung cancer mortality without breast cancer recurrence ≥ 10 years after radiotherapy had a rate ratio of 2.10 (95% confidence interval (CI), 1.48 to 2.98; P = <0.001) on the basis of 134 cancer patients (25). Furthermore, EBRT has been proven to cause various heart diseases including ischemic heart disease, coronary stenosis, myocardial infarction, valvular disease, pericarditis and other cardiac abnormalities (25–27). However, these complications are negated using IORT which significantly decreases the non-breast cancer related mortality rate (45 vs. 74 events for TARGIT-IORT and EBRT, respectively, hazard ratio 0.59; 95% CI, 0.40 to 0.86; P=0.005), including the cardiovascular causes (8). As a result, IORT may be a prudent choice of treatment, particularly in patients with pre-existing cardiac conditions such as pacemaker.
IORT allows a single high dose of radiation to be delivered directly to the surgical margins shortly after tumor excision, and the very low energy (50 kVp) minimizes scatter and radiation exposure to the surrounding tissues, which in turn reduces the risk of electromagnetic interference (4, 28, 29). IORT can lead to higher patient compliance owing to shorter treatment duration and fewer visits, which may overall lead to better patient experience (30). Additionally, patients with locally recurrent breast cancer who have previously undergone breast conserving surgery with EBRT can undergo a second breast-conserving surgery with IORT as an alternative to mastectomy (31). Furthermore, a previous randomized control trial conducted by the TARGIT group demonstrated that TARGIT-IORT is both safe and efficacious (7). Contrastingly, there is no current consensus on the use of IORT in patients with breast cancer and concomitant pacemaker, and surgeons remain cautious because pacemaker failures due to radiation can theoretically occur at any dose (32). As a result, many of them opt to use surgery and adjuvant therapy to treat these patients (33). Furthermore, elderly patients, such as patient 1, who was 82 years old, could benefit from surgery and endocrine therapy while avoiding radiotherapy (34). The decision to give this patient radiotherapy was based on the Cancer and Leukemia Group B (CALGB) 9343 trial which found that adding radiation therapy to endocrine therapy improved locoregional recurrence in women age ≥ 70 years (35). Kunkler et al. (36) also randomized 1,326 patients with non-metastatic hormone receptor-positive breast cancer who were at least 65 years old, had breast-conserving surgery, and were receiving adjuvant hormone therapy. The authors reported that the rate of local recurrence after 10 years was significantly higher in patients who did not receive radiation therapy compared to patients who did (9.8% vs. 0.9%), supporting our decision to treat this patient with radiotherapy.
Although previous studies have evaluated the utility of IORT in patients with breast cancer, fewer have elucidated its use when associated with a presence of ipsilateral pacemaker (7, 14, 33). Chen et al. (29) assessed the dose for a patient with a pacemaker being treated in the left breast with IORT in phantom cases. They found that as the radial distance between the applicator and the pacemaker increases, the radiation exposure to the pacemaker decreases. In their study, despite the radiation dose being increased to 10-20 Gy, no pacemaker device malfunctions, or failures were observed. Additionally, Keshtgar et al. (33) reported a case of left-sided invasive ductal carcinoma of the breast with a pacemaker in an elderly woman. They reported a tumor-to-pacemaker distance of 9 cm that was successfully treated with IORT. Over the course of 26 minutes, they delivered a radiation dose of 20 Gy to the surgical margin and 6 Gy to an area 1 cm away from the surgical margin. Similarly, in both of our patients who were successfully treated with IORT, the tumor-to-pacemaker distance was 10 cm. In addition, a 20 Gy radiation dose was delivered to the surgical margin in both patients, and an absorbed dose of 0.23 Gy and 0.185 Gy to the skin at the pacemaker site were measured, respectively. Thus, our findings add to the limited existing literature on use of IORT in breast cancer patients with ipsilateral pacemaker. Furthermore, our findings show that successful radiotherapy can be delivered without the need for the pacemaker to be reimplanted on the contralateral side or in a neck pocket. To support the widespread applicability of IORT as a treatment modality in breast cancer patients with pacemaker, further clinical studies are needed.
The use of such single high-dose radiation delivered directly to the surgical margins in patients with pacemaker is a step in the right direction. However, from a practical standpoint, it is unclear how much radiation exposure to the pacemaker a clinician should consider acceptable. The American Association of Physicists in Medicine (AAPM) Task Group 203 (TG-203) recently recommended that radiation exposure to the pacemaker up to 2 Gy is considered low risk, while exposures greater than 5 Gy are considered high risk (37). Moreover, the threshold for radiation exposure for pacemaker devices varies from each manufacturer. Medtronic, Inc. (Minneapolis, MN, USA), St. Jude Medical (St. Paul, MN, USA), Biotronik SE & Co (Berlin, Germany), and Boston Scientific (Boston, MA, USA) are the primary manufacturers of pacemaker in the United States. The maximum dose threshold for Medtronic varies from 1 Gy to 5 Gy depending on the model of pacemaker (33, 38), 20-30 Gy for St. Jude Medical (39, 40), and not specified for both Biotronik SE & Co (41) and Boston Scientific (42). Due to the large volume of products available in the market, we explicitly recommend future studies determining the optimal and maximum threshold dose safe for each device as well as safe distance from pacemaker to establish new guidelines.
Conclusion
Our findings underscore the successful use of targeted IORT for breast-conserving surgery in a patient with invasive ductal carcinoma and pacemaker, hence eliminating the necessity for reimplant pacemaker surgeries in these patients. Furthermore, no device failure or malfunction for the pacemaker was recorded before, during, or after the surgery, demonstrating the safety of using IORT in patients with preinstalled pacemaker despite a lack of evidence on safe radiation dosage or manufacturer guidelines. Nonetheless, the effects of IORT on pacemaker < 10 cm were not studied in our patients and further clinical studies are recommended to reinforce the applicability and safe distance of IORT in breast cancer patients with pacemaker.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Statements
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Ethics statement
Ethical review and approval were not required for the study on human participants in accordance with the local legislation and institutional requirements. The patients/participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
FB: substantial contributions to acquisition of data and involved in drafting and revision of the manuscript. KJ and MM: substantial contributions in revising the manuscript. NB, WT, JF, and KM: equal contributions to acquisition of data and in the revision of the manuscript. SF: substantial contributions to data acquisition, involved in drafting and revising the manuscript. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1
American Cancer Society. Cancer Facts & Figures 2021. Atlanta: American Cancer Society (2021). Available at: https://www.cancer.org/research/cancer-facts-statistics/all-cancer-facts-figures/cancer-facts-figures-2021.html.
2
SiegelRLMillerKDFuchsHEJemalA. Cancer Statistics, 2022. CA Cancer J Clin (2022) 72(1):7–33. doi: 10.3322/caac.21708
3
SkandarajahARLynchACMackayJRNganSHeriotAG. The Role of Intraoperative Radiotherapy in Solid Tumors. Ann Surg Oncol (2009) 16(3):735–44. doi: 10.1245/s10434-008-0287-2
4
VaidyaJSTobiasJSBaumMKeshtgarMJosephDWenzFet al. Intraoperative Radiotherapy for Breast Cancer. Lancet Oncol (2004) 5(3):165–73. doi: 10.1016/S1470-2045(04)01412-3
5
AlvaradoMDConollyJParkCSakataTMohanAJHarrisonBLet al. Patient Preferences Regarding Intraoperative Versus External Beam Radiotherapy Following Breast-Conserving Surgery. Breast Cancer Res Treat (2014) 143(1):135–40. doi: 10.1007/s10549-013-2782-9
6
TangACohanCMBeattieGCuretonELSvahnJDLyonLLet al. Patients Older 65 Years With Early Breast Cancer Prefer Intraoperative Radiation as a Locoregional Treatment Choice. Ann Surg Oncol (2021) 28(9):5158–63. doi: 10.1245/s10434-021-09618-3
7
VaidyaJSJosephDJTobiasJSBulsaraMWenzFSaundersCet al. Targeted Intraoperative Radiotherapy Versus Whole Breast Radiotherapy for Breast Cancer (TARGIT-A Trial): An International, Prospective, Randomised, non-Inferiority Phase 3 Trial. Lancet (2010) 376(9735):91–102. doi: 10.1016/S0140-6736(10)60837-9
8
VaidyaJSBulsaraMBaumMWenzFMassarutSPigorschSet al. Long Term Survival and Local Control Outcomes From Single Dose Targeted Intraoperative Radiotherapy During Lumpectomy (TARGIT-IORT) for Early Breast Cancer: TARGIT-A Randomised Clinical Trial. BMJ (2020) 370:m2836. doi: 10.1136/bmj.m2836
9
VaidyaJSBulsaraMBaumMWenzFMassarutSPigorschSet al. New Clinical and Biological Insights From the International TARGIT-A Randomised Trial of Targeted Intraoperative Radiotherapy During Lumpectomy for Breast Cancer. Br J Cancer (2021) 125(3):380–9. doi: 10.1038/s41416-021-01440-8
10
ZarembaTJakobsenARSøgaardMThøgersenAMRiahiS. Radiotherapy in Patients With Pacemakers and Implantable Cardioverter Defibrillators: A Literature Review. Europace (2016) 18(4):479–91. doi: 10.1093/europace/euv135
11
WoodMAEllenbogenKA. Cardiology Patient Pages. Cardiac Pacemakers Patient's Perspective Circulation (2002) 105(18):2136–8.
12
WadasadawalaTPandeyAAgarwalJPJalaliRLaskarSGChowdharySet al. Radiation Therapy With Implanted Cardiac Pacemaker Devices: A Clinical and Dosimetric Analysis of Patients and Proposed Precautions. Clin Oncol (R Coll Radiol) (2011) 23(2):79–85. doi: 10.1016/j.clon.2010.08.031
13
Van der ZeeSDoshiS. Permanent Leadless Cardiac Pacing: American College of Cardiology (2016). Available at: https://www.acc.org/latest-in-cardiology/articles/2016/03/23/08/09/permanent-leadless-cardiac-pacing#:~:text=Each%20year%2C%20approximately%20200%2C000%20pacemakers,clear%20benefit%20from%20pacing%20therapy.
14
RamdasYBennCAGrubnikAMayatYHolmesDR. Targeted Intraoperative Radiotherapy Is a Safe Approach for Patients With Pacemakers: A Case Study and Literature Review. Case Rep Oncol (2020) 13(2):916–22. doi: 10.1159/000508946
15
VaidyaJSBaumMTobiasJSMorganSD'SouzaD. The Novel Technique of Delivering Targeted Intraoperative Radiotherapy (Targit) for Early Breast Cancer. Eur J Surg Oncol (2002) 28(4):447–54. doi: 10.1053/ejso.2002.1275
16
BrodinNPMehtaKJBasavatiaAGoddardLCFoxJLFeldmanSMet al. A Skin Dose Prediction Model Based on In Vivo Dosimetry and Ultrasound Skin Bridge Measurements During Intraoperative Breast Radiation Therapy. Brachytherapy (2019) 18(5):720–6. doi: 10.1016/j.brachy.2019.05.012
17
RodriguezFFilimonovAHenningACoughlinCGreenbergM. Radiation-Induced Effects in Multiprogrammable Pacemakers and Implantable Defibrillators. Pacing Clin Electrophysiol (1991) 14(12):2143–53. doi: 10.1111/j.1540-8159.1991.tb06485.x
18
SoulimanSKChristieJ. Pacemaker Failure Induced by Radiotherapy. Pacing Clin Electrophysiol (1994) 17(3 Pt 1):270–3. doi: 10.1111/j.1540-8159.1994.tb01387.x
19
Guidant Corporation Cardiac Rhythm Management Technical Services. The Impact of Radiation on Guidant Implantable Pacemakers (IPMs) and Implantable Cardioverter Defibrillators (ICDs). St. Paul, MN: Guidant Corporation. (2003). pp. 1–6.
20
CroshawRKimYLappinenEJulianTTrombettaM. Avoiding Mastectomy: Accelerated Partial Breast Irradiation for Breast Cancer Patients With Pacemakers or Defibrillators. Ann Surg Oncol (2011) 18(12):3500–5. doi: 10.1245/s10434-011-1784-2
21
DorenkampMStrombergerCvon HeymannCHaverkampWWustPRoserM. Radiation Therapy in Patients With Cardiac Pacemakers or Implantable Cardioverter Defibrillators. Interdisciplinary Safety Recommendations. Strahlenther Onkol (2013) 189(1):5–17. doi: 10.1007/s00066-012-0243-8
22
LambertPDa CostaAMarcyPYKrepsSAngellierGMarciéSet al. Pacemaker, Implanted Cardiac Defibrillator and Irradiation: Management Proposal in 2010 Depending on the Type of Cardiac Stimulator and Prognosis and Location of Cancer. Cancer Radiother (2011) 15(3):238–49. doi: 10.1016/j.canrad.2010.12.003
23
WilkoffBLLoveCJByrdCLBongiorniMGCarrilloRGCrossleyGHet al. Transvenous Lead Extraction: Heart Rhythm Society Expert Consensus on Facilities, Training, Indications, and Patient Management: This Document was Endorsed by the American Heart Association (AHA). Heart Rhythm (2009) 6(7):1085–104. doi: 10.1016/j.hrthm.2009.05.020
24
MazzettiHATentoriMC. Breast Cancer and Pacemakers. Europace (2014) 16(2):303–5. doi: 10.1093/europace/eut218
25
TaylorCCorreaCDuaneFKAznarMCAndersonSJBerghJet al. Estimating the Risks of Breast Cancer Radiotherapy: Evidence From Modern Radiation Doses to the Lungs and Heart and From Previous Randomized Trials. J Clin Oncol (2017) 35(15):1641–9. doi: 10.1200/JCO.2016.72.0722
26
WennstigAKGarmoHWadstenLLagerqvistBFredrikssonIHolmbergLet al. Risk of Coronary Stenosis After Adjuvant Radiotherapy for Breast Cancer. Strahlenther Onkol (2022) 198:630–8 doi: 10.1007/s00066-022-01927-0
27
McGalePDarbySCHallPAdolfssonJBengtssonNOBennetAMet al. Incidence of Heart Disease in 35,000 Women Treated With Radiotherapy for Breast Cancer in Denmark and Sweden. Radiother Oncol (2011) 100(2):167–75. doi: 10.1016/j.radonc.2011.06.016
28
RollinsKELoboDN. Intraoperative Goal-Directed Fluid Therapy in Elective Major Abdominal Surgery: A Meta-Analysis of Randomized Controlled Trials. Ann Surg (2016) 263(3):465–76. doi: 10.1097/SLA.0000000000001366
29
ChenYGoenkaASharmaAWangLCaoYJamshidiA. SU-F-T-654: Pacemaker Dose Estimate Using Optically Stimulated Luminescent Dosimeter for Left Breast Intraoperative Radiation Therapy. Med Phys (2016) 43(6Part23):3614. doi: 10.1118/1.4956839
30
CoombsNJCoombsJMVaidyaUJSingerJBulsaraMTobiasJSet al. Environmental and Social Benefits of the Targeted Intraoperative Radiotherapy for Breast Cancer: Data From UK TARGIT-A Trial Centres and Two UK NHS Hospitals Offering TARGIT IORT. BMJ Open (2016) 6(5):e010703. doi: 10.1136/bmjopen-2015-010703
31
BoehmKMChenJTrichterSAbdallahHZhuoRNowakEJet al. Characterization of Recurrences Following Second Breast-Conserving Surgery With Intraoperative Radiotherapy. Ann Surg Oncol (2020) 27(5):1638–44. doi: 10.1245/s10434-019-07908-5
32
MoutonJHaugRBridierADodinotBEschwegeF. Influence of High-Energy Photon Beam Irradiation on Pacemaker Operation. Phys Med Biol (2002) 47(16):2879–93. doi: 10.1088/0031-9155/47/16/304
33
KeshtgarMREatonDJReynoldsCPigottKDavidsonTGauter-FleckensteinBet al. Pacemaker and Radiotherapy in Breast Cancer: Is Targeted Intraoperative Radiotherapy the Answer in This Setting? Radiat Oncol (2012) 7:128. doi: 10.1186/1748-717X-7-128
34
KirwanCCColesCEBlissJGroup PPW. It's PRIMETIME. Postoperative Avoidance of Radiotherapy: Biomarker Selection of Women at Very Low Risk of Local Recurrence. Clin Oncol (R Coll Radiol) (2016) 28(9):594–6.
35
HughesKSSchnaperLABellonJRCirrincioneCTBerryDAMcCormickBet al. Lumpectomy Plus Tamoxifen With or Without Irradiation in Women Age 70 Years or Older With Early Breast Cancer: Long-Term Follow-Up of CALGB 9343. J Clin Oncol (2013) 31(19):2382–7. doi: 10.1200/JCO.2012.45.2615
36
KunklerIHWilliamsLJJackWJCameronDADixonJMinvestigators PI. Breast-Conserving Surgery With or Without Irradiation in Women Aged 65 Years or Older With Early Breast Cancer (PRIME II): A Randomised Controlled Trial. Lancet Oncol (2015) 16(3):266–73. doi: 10.1016/S1470-2045(14)71221-5
37
MiftenMMihailidisDKrySFReftCEsquivelCFarrJet al. Management of Radiotherapy Patients With Implanted Cardiac Pacemakers and Defibrillators: A Report of the AAPM TG-203. Med Phys (2019) 46(12):e757–e88. doi: 10.1002/mp.13838
38
Medtronic Incorporated. Therapeutic Radiation. Mounds View, MN: CRDM Technical Services (2008). p. 2.
39
HudsonFCoulshedDD'SouzaEBakerC. Effect of Radiation Therapy on the Latest Generation of Pacemakers and Implantable Cardioverter Defibrillators: A Systematic Review. J Med Imaging Radiat Oncol (2010) 54(1):53–61. doi: 10.1111/j.1754-9485.2010.02138.x
40
SylmarCA. St. Jude Medical. Radiation. 1-3, 9/02 and Electromagnetic Interference: Cardiac Rhythm Management Division. Sylmar, CA, USA: St. Jude Medical. pp. 1–6.
41
Biotronik SE and Co. KG. Electromagnetic Compatibility of BIOTRONIK Cardiac Pacemakers, ICDs and CRT Devices (2017). Available at: https://biotronik.cdn.mediamid.com/cdn_bio_doc/bio23016/8207/bio23016.pdf.
42
Boston Scientific Corporation (2012). Available at: https://www.bostonscientific.com/content/dam/bostonscientific/quality/education-resources/english-a4/EN_ACL_Therapeutic_Radiation_20120925.pdf.
Summary
Keywords
breast cancer, intraoperative radiotherapy, pacemaker, case report, TARGIT, breast, invasive duct breast cancer (IDC)
Citation
Bhimani F, Johnson K, Brodin NP, Tomé WA, Fox J, Mehta K, McEvoy M and Feldman S (2022) Case Report: Can Targeted Intraoperative Radiotherapy in Patients With Breast Cancer and Pacemakers be the New Standard of Care?. Front. Oncol. 12:927174. doi: 10.3389/fonc.2022.927174
Received
23 April 2022
Accepted
20 June 2022
Published
12 July 2022
Volume
12 - 2022
Edited by
Mangesh A. Thorat, Guy’s and St Thomas’ NHS Foundation Trust, United Kingdom
Reviewed by
Nathan Coombs, Great Western Hospital, United Kingdom; Jordan Slagowski, The University of Chicago, United States; Jayant S. Vaidya, University College London, United Kingdom
Updates
Copyright
© 2022 Bhimani, Johnson, Brodin, Tomé, Fox, Mehta, McEvoy and Feldman.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sheldon Feldman, sfeldman@montefiore.org
This article was submitted to Breast Cancer, a section of the journal Frontiers in Oncology
Disclaimer
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.