Introduction
Since the United States Food and Drug Administration (FDA) approved the use of extracorporeal photopheresis (ECP) in the palliative treatment of cutaneous T-cell lymphoma (CTCL) in 1988 (1), many other indications have been successfully explored. However, most of these approaches still demand further randomized clinical trials, including graft-vs.-host disease (GvHD), rejection of solid organ transplantation, and a wide range of autoimmune diseases.
ECP is a leukapheresis-based therapy where the patient’s whole blood is collected and separated into its different components; the collected leukocytes are treated extracorporeally with a photosensitizing agent and then exposed to ultraviolet-A (UV-A) irradiation before reinfusion.
Interestingly, despite the vast marketing experience of the ECP therapy gathered over more than 30 years and the manufacturing improvement of photopheresis devices, no significant changes have occurred around the photosensitizing drugs, which remain restricted to 8-methoxypsoralen (8-MOP, methoxsalen).
Few preclinical and early phase clinical trials have explored different photosensitizers during the last decade. Other ECP photosensitizing agents with equivalent (or better) safety, efficacy, and cost profiles could be available in the marketing landscape of low-income regions that cannot afford the current financial and economic costs of these promising therapies.
This Opinion paper aims to raise some regulatory considerations regarding the conventional photosensitizing agent (8-MOP), emphasizing the potential usefulness of other drugs and non-pharmacological systems for photosensitization during ECP.
ECP regulatory landscape
The FDA considers a photopheresis system a “combination product” comprising two regulated components: a drug (photosensitizer) and a device (leukapheresis machine) (2). Furthermore, the European Medicines Agency (EMA) refines the regulation of medicinal products used with a medical device by defining “integral,” “co-packaged,” and “referenced” combinations. Those referenced products “combine two (or more) product information of the medicinal product refers to a specific medical device to be used, and the specified medical device is obtained separately by the user of the medicinal product” (3).
For instance, 8-MOP branded as UVADEX® Sterile Solution (Mallinckrodt Pharmaceuticals, Ireland- United States) has been granted FDA authorization in combination with one specific photopheresis device only (UVAR®, and its more recent superseding device, THERAKOS® CELLEX®, both Therakos Inc., Mallinckrodt Pharmaceuticals) (4) that correspond to closed, “online” ECP methods. In Europe, ECP products manufactured using open “offline” methods are subject to Advanced Therapeutic Medical Product (ATMP) regulations (5).
Nevertheless, it is widely accepted that a combination product’s primary mode of action (PMOA) is “the single mode of action expected to make the most significant contribution to the overall intended therapeutic effects of the combination” (2). In ECP, the PMOA relies on photosensitizers, comprised of drugs and irradiation systems, rather than the leukapheresis device. A few online and integrated systems for cellular collection, photoactivation, and infusion are available (e.g., THERAKOS® CELLEX® device and AMICUS® Blue ECP system, Fresenius Kabi, Germany); however, evidence also shows that ECP has effectiveness using different marketed photosensitizers and photoactivation devices (e.g., MacoGenic G2 irradiation device, Macopharma, France). Those offline platforms treat leukocytes harvested by other apheresis machines not necessarily intended for ECP protocols (e.g., SPECTRA OPTIA® Apheresis System, Terumo BCT, Japan) and are not approved as combination products, as mentioned earlier.
Discussion
Irradiation devices for ECP
Photoactivation devices play pivotal roles in ECP PMOA. The UV-A irradiation dose (intensity and duration) and the plate film thickness can polarize to either the immunizing or tolerogenic effects exerted by ECP (6, 7). These dual capabilities are crucial for clinical conditions that can be treated with photopheresis: while enhanced immune responses are desirable in cancer scenarios (e.g., CTCL as the primary approved indication), ECP tolerizing effects are required in cases such as solid organ transplantation, GvHD, and autoimmune diseases.
Photosensitizer drugs for ECP: Capabilities beyond 8-MOP
Unfortunately, there is no consensus as to what in-process and pharmaceutical controls should be performed for ECP products; therefore, there is a critical need for harmonized quality-control assays, as stated and summarized as (5):
-
- Cellular composition of ECP products;
-
- Induction of apoptosis in lymphocytes;
-
- Monocyte polarization;
-
- Psoralen photoadducts;
-
- T cell suppression; and,
-
- Capacity for antigen cross-presentation.
Although many questions about PMOA of photosensitizers and ECP as a whole procedure remain inconclusive, the main advances in pharmacological development, manufacturing, quality controls, and preclinical and clinical uses, correspond to 8-MOP.
Like other psoralens, 8-MOP, upon UV-A photoactivation (wavelength: 315˗400 nm), conjugates and forms covalent bonds with DNA that lead to monofunctional (addition to a single strand) and bifunctional (crosslinking of psoralen to both DNA strands) photoadducts. Lastly, it results in inhibition of DNA synthesis and cell division (4, 8). The apoptotic fate of extracorporeally exposed cells consists of the ECP PMOA generating antigen-specific immune and clinical responses, which are not described here (8).
Traditionally, the combined administration of psoralens (orally or topically) with UV-A (PUVA) has been widely used to manage psoriasis and CTCL patients. Eventually, non-8-MOP psoralens and other photosensitizer drugs, such as those used in photodynamic therapy (PDT), can be applied in ECP (9). Table 1 summarizes distinctive characteristics, preclinical, and clinical evidence of current and potential photosensitizers for ECP.
Table 1
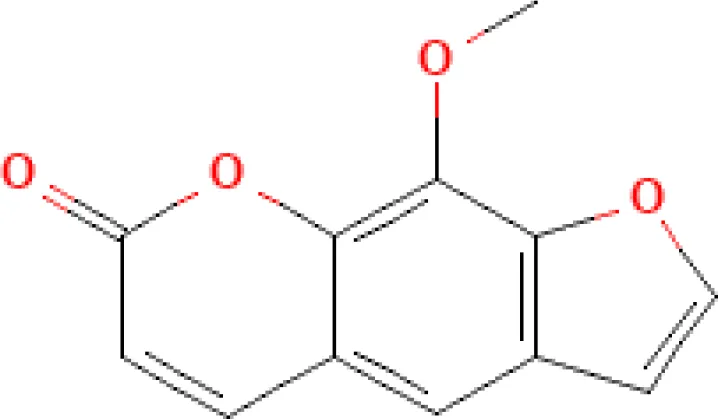
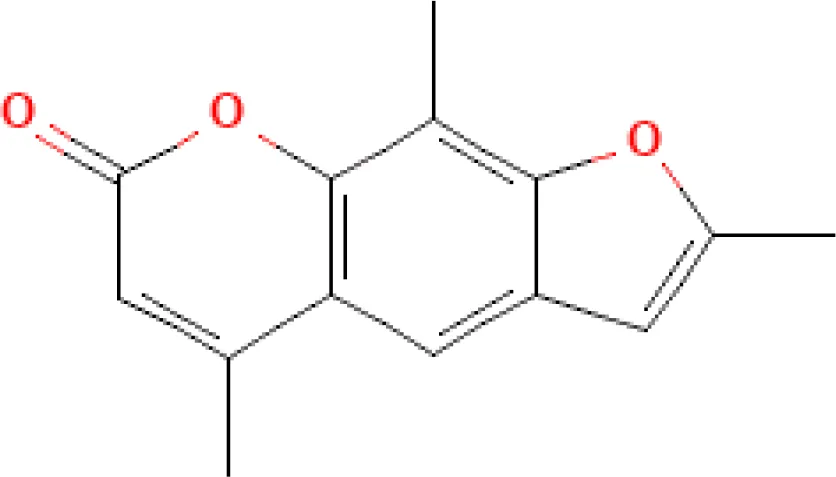
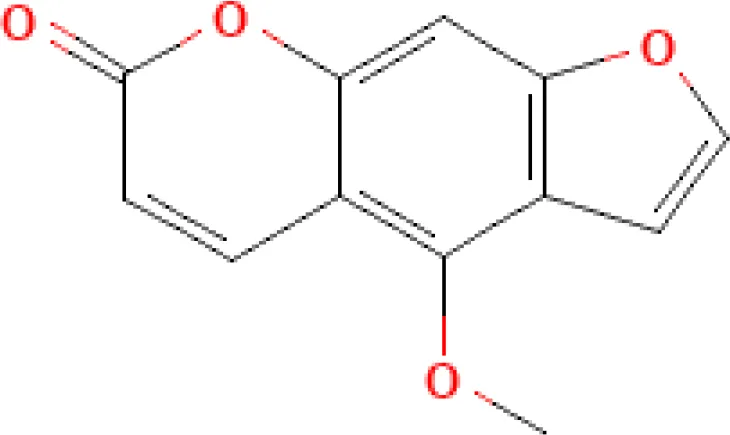
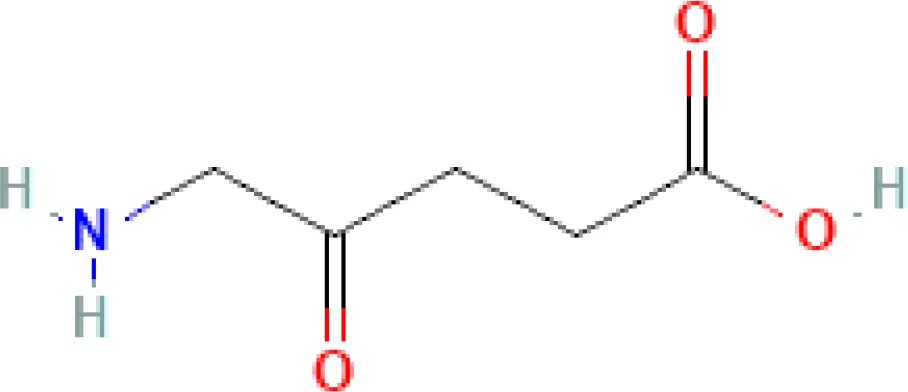
| Photosensitizer | ATC code | Chemical structure | Current indications | Required light (wavelength, nm) | ECP regulatory status | Preclinical (P) and clinical (C) evidence on ECP |
|---|---|---|---|---|---|---|
| Psoralens for systemic use | ||||||
| 8-methoxypsoralen (8-MOP, methoxsalen) | D05BA02 |
|
- Psoriasis - Vitiligo - CTCL (ECP) |
UV-A (315˗400) |
- Marketing authorization (CTCL) | - Vast post-authorization experience (C) - Ongoing clinical trials for new indications (e.g., NCT05168384, NCT05413005) (C) |
| Trioxsalen (trimethylpsoralen, trisoralen) | D05BA01 |
|
- Vitiligo (discontinued) | UV-A (315˗400) |
- Unknown or not reported | - Unknown or not reported |
| 5-methoxypsoralen (5-MOP, bergapten) | D05BA03 |
|
- Psoriasis - Vitiligo - CTCL |
UV-A (315˗400) |
- Unknown or not reported | - (10) (C) * |
| Sensitizer used in PDT § | ||||||
| 5-aminolevulinic acid (5-ALA) | L01XD04 |
|
- Actinic keratosis - Glioma (intraoperative optical imaging agent) |
Visible light (400˗635) |
- Preclinical studies - Early phase clinical trials |
- (11) (P) ** - (12) (P) - (13) (P) - (14) (P) - (9) (C) - NCT04164849 (C) |
| Electromagnetic spectrum of light applied for ECP |

|
|||||
Current and potential photosensitizer drugs for ECP.
*Case report on concomitant use of 5-MOP (PUVA) and 8-MOP (ECP); **In vitro administration of hexaminolevulinate, an ester of 5-ALA
§ Other drugs in this group include: porfimer sodium, methyl aminolevulinate, temoporfin, efaproxiral, padeliporfin (unknown or not reported use for ECP)
ATC, Anatomical Therapeutic Chemical; CTCL, Cutaneous T-Cell Lymphoma; ECP, Extracorporeal Photopheresi; PDT, Photodynamic therapy; PUVA, Psoralen and UV-A; UV-A, Ultraviolet-A Light (Source: PubMed, PubChem, and ClinicalTrials.gov databases).
In 1996, Wolf et al. described the successful treatment of a patient with photoaccentuated erythroderma and idiopathic CD4 T lymphocytopenia using 5-methoxypsoralen (5-MOP)-PUVA, and ECP with 8-MOP concomitantly (10). However, there are no publications of ECP procedures delivered with 5-MOP or trioxsalen (trimethylpsoralen) to date.
In contrast, PDT photosensitizers, such as 5-aminolevulinic acid (5-ALA), have emerged in preclinical (11–14) and early phase clinical trials (9) as an alternative to the authorized 8-MOP for ECP. PDT typically involves systemic or topical administration of a lesion-localizing photosensitizer (e.g., 5-ALA) and its subsequent activation by visible light (400˗780 nm, represented by blue and red arrowheads in the electromagnetic spectrum of Table 1), primarily resulting in a singlet oxygen-induced photodamage in the exposed cells (12, 14). Nevertheless, further preclinical research is needed to clarify ECP mechanisms of action, resulting in appropriate harmonized quality controls for these photosensitizers.
The alternative use of 5-ALA is supported by ex vivo investigations that show that this photosensitizer affects T-cells from chronic GvHD patients more selectively and efficiently than those treated with 8-MOP-ECP, through the formation of protoporphyrin IX. Consequently, reducing the number of ECP treatments can be achieved using 5-ALA (9). This finding occurs even with a UV-A light source resembling emission spectral wavelengths to those of the built-in certified UV-A commercial photopheresis systems (340˗410 nm) (12, 14).
The clinical applications of novel photosensitizing drugs are limited based on the number of published clinical trials, procedures, and patients enrolled. For instance, the cited work of Christensen et al. reported 82 ECP treatments with 5-ALA in five chronic GvHD patients who responded poorly to 8-MOP-photopheresis after a minimum of three months of treatment. Although safety and tolerability were found to be adequate (9), no additional clinical evidence is yet available. Only another phase I/II clinical trial using 5-ALA-ECP has been registered on ClinicalTrials.gov (NCT04164849) for patients with active Crohn’s disease, as shown in Table 1. Still, more clinical studies are required to demonstrate differences in safety, efficacy, and cost profiles compared to the approved 8-MOP.
Apoptosis induced by light: Are ECP-photosensitizers still needed?
Insulting agents that trigger “immediate” pre-programmed cell death (pre-PCD) apoptosis include PDT, UV-A1 (340˗400 nm), and agents that generate singlet-oxygen damage to mitochondrial membranes (e.g., with 5-ALA). “Intermediate” apoptosis occurs to a significant extent within 4 h, but requires more than 30 min, and high doses of either UV-B (290˗320 nm) or UV-C (200˗290 nm) radiation, and any agent that activates a membrane receptor containing a death domain, such as Fas/CD95/APO-1. “Delayed” apoptosis occurs well after 4 h (or days), and examples of agents that induce primarily delayed PCD apoptosis are UV-B, UV-C, X-rays, and any agent that causes significant DNA damage (15).
However, different wavelength photons have been used to treat various diseases without the need for photosensitizing drugs, resulting in necrosis but also inducing cell apoptosis (desired PMOA of ECP), with consequent changes in the production of soluble mediators (cytokine profiles), modulation of the expression of cell-surface associated molecules, and damage in pathogenetically relevant cells (cytotoxicities) (15, 16). It has been demonstrated that in vitro UV-A1 and UV-B irradiation alone induced T cell apoptosis, which reduces inflammatory infiltrates in T cell-mediated skin diseases (16). Still, the chances to use other types of radiations to induce apoptosis extracorporeally require further photoimmunologic studies.
Conclusions
Additional developments in manufacturing and evaluating innovative ECP-photosensitizing drugs are rising needs that should accompany the development of photopheresis medical devices. Moreover, alternative non-pharmacological systems for in vitro photosensitization and apoptosis induction are strategies that should be further explored. Compliance with regulatory requirements derived from the emerging knowledge might extend the new indications for ECP, benefiting more patients and healthcare systems.
Acknowledgments
The author gratefully acknowledges Eng. Diana Patricia Hermida Vitar, MSc, for critical reading of the manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Statements
Author contributions
YMCA is the sole author and agrees to be accountable for the content of the work.
Conflict of interest
The author is an Investigator and Principal Investigator of two clinical trials examples of new indications of ECP using 8-MOP (NCT05168384 and NCT05413005, respectively; Table 1).
References
1
Edelson R Berger C Gasparro F Jegasothy B Heald P Wintroub B et al . Treatment of cutaneous T-cell lymphoma by extracorporeal photochemotherapy. preliminary results. N Engl J Med (1987) 316(6):297–303. doi: 10.1056/NEJM198702053160603
2
US Food and Drug Administration . Principles of premarket pathways for combination products (2022). Available at: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/principles-premarket-pathways-combination-products (Accessed July 15, 2022).
3
European Medicines Agency . Guideline on quality documentation for medicinal products when used with a medical device (2021). Available at: https://www.ema.europa.eu/en/quality-documentation-medicinal-products-when-used-medical-device (Accessed July 15, 2022).
4
Drugs@FDA: FDA-Approved Drugs . UVADEX (2022). Available at: https://www.accessdata.fda.gov/scripts/cder/daf/index.cfm (Accessed July 15, 2022).
5
Ahrens N Geissler EK Witt V Berneburg M Wolff D Hirt SW et al . European Reflections on new indications for extracorporeal photopheresis in solid organ transplantation. Transplantation (2018) 102(8):1279–83. doi: 10.1097/TP.0000000000002244
6
Durazzo TS Tigelaar RE Filler R Hayday A Girardi M Edelson RL . Induction of monocyte-to-dendritic cell maturation by extracorporeal photochemotherapy: initiation via direct platelet signaling. Transfusion apheresis science: Off J World Apheresis Association: Off J Eur Soc Haemapheresis (2014) 50(3):370–8. doi: 10.1016/j.transci.2013.11.008
7
Edelson R Wu Y Schneiderman J . American Council on ECP (ACE): Why now? J Clin apheresis (2018) 33(4):464–8. doi: 10.1002/jca.21627
8
Vieyra-Garcia PA Wolf P . Extracorporeal photopheresis: A case of immunotherapy ahead of its time. Transfusion Med hemotherapy: offizielles Organ der Deutschen Gesellschaft fur Transfusionsmedizin und Immunhamatologie (2020) 47(3):226–35. doi: 10.1159/000508479
9
Christensen E Foss OA Quist-Paulsen P Staur I Pettersen F Holien T et al . Application of photodynamic therapy with 5-aminolevulinic acid to extracorporeal photopheresis in the treatment of patients with chronic graft-versus-Host disease: A first-in-Human study. Pharmaceutics (2021) 13(10):1558. doi: 10.3390/pharmaceutics13101558
10
Wolf P Müllegger R Cerroni L Aigner R Fueger G Höfler G et al . Photoaccentuated erythroderma associated with CD4+ T lymphocytopenia: successful treatment with 5-methoxypsoralen and UVA, interferon alfa-2b, and extracorporeal photopheresis. J Am Acad Dermatol (1996) 35(2 Pt 2):291–4. doi: 10.1016/s0190-9622(96)90651-9
11
Cunderlíková B Vasovič V Randeberg LL Christensen E Warloe T Nesland JM et al . Modification of extracorporeal photopheresis technology with porphyrin precursors. comparison between 8-methoxypsoralen and hexaminolevulinate in killing human T-cell lymphoma cell lines in vitro. Biochim Biophys Acta (2014) 1840(9):2702–8. doi: 10.1016/j.bbagen.2014.05.020
12
Holien T Gederaas OA Darvekar SR Christensen E Peng Q et al . Comparison between 8-methoxypsoralen and 5-aminolevulinic acid in killing T cells of photopheresis patients ex vivo. Lasers Surg Med (2018) 50(5):469–75. doi: 10.1002/lsm.22806
13
Sando Y Matsuoka KI Sumii Y Kondo T Ikegawa S Sugiura H et al . 5-aminolevulinic acid-mediated photodynamic therapy can target aggressive adult T cell leukemia/lymphoma resistant to conventional chemotherapy. Sci Rep (2020) 10(1):17237. doi: 10.1038/s41598-020-74174-x
14
Darvekar S Juzenas P Oksvold M Kleinauskas A Holien T Christensen E et al . Selective killing of activated T cells by 5-aminolevulinic acid mediated photodynamic effect: Potential improvement of extracorporeal photopheresis. Cancers (2020) 12(2):377. doi: 10.3390/cancers12020377
15
Godar DE . Light and death: photons and apoptosis. J Invest Dermatol Symposium Proc (1999) 4(1):17–23. doi: 10.1038/sj.jidsp.5640175
16
Krutmann J Morita A . Mechanisms of ultraviolet (UV) b and UVA phototherapy. J Invest Dermatol Symposium Proc (1999) 4(1):70–2. doi: 10.1038/sj.jidsp.5640185
Summary
Keywords
5-aminolevulinic acid, 5-methoxypsoralen, 8-methoxypsoralen, apoptosis, extracorporeal photopheresis, photoimmunology, photosensitizer, phototherapy
Citation
Castillo-Aleman YM (2022) Beyond 8-methoxypsoralen as the photosensitizer for extracorporeal photopheresis. Front. Oncol. 12:996973. doi: 10.3389/fonc.2022.996973
Received
20 July 2022
Accepted
27 September 2022
Published
18 October 2022
Volume
12 - 2022
Edited by
J. Luis Espinoza, Kanazawa University, Japan
Reviewed by
Jill Adamski, Mayo Clinic Arizona, United States
Updates
Copyright
© 2022 Castillo-Aleman.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yandy Marx Castillo-Aleman, yandy.castillo@adscc.ae
This article was submitted to Hematologic Malignancies, a section of the journal Frontiers in Oncology
Disclaimer
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.