 Aurelio Cruz-Valdez1†‡
Aurelio Cruz-Valdez1†‡ Lina Sofia Palacio-Mejía2†‡Amado D. Quezada-Sánchez3‡
Lina Sofia Palacio-Mejía2†‡Amado D. Quezada-Sánchez3‡ Juan Eugenio Hernández-Ávila3‡Tatiana Galicia-Carmona4‡
Juan Eugenio Hernández-Ávila3‡Tatiana Galicia-Carmona4‡ Lucely del Carmen Cetina-Pérez4‡
Lucely del Carmen Cetina-Pérez4‡ Eder A. Arango-Bravo4‡David Isla-Ortiz5‡Carlos E. Aranda-Flores6‡Santos-Regino Uscanga-Sánchez7
Eder A. Arango-Bravo4‡David Isla-Ortiz5‡Carlos E. Aranda-Flores6‡Santos-Regino Uscanga-Sánchez7 Vicente Madrid-Marina8‡
Vicente Madrid-Marina8‡ Kirvis Torres-Poveda2,8*‡
Kirvis Torres-Poveda2,8*‡- 1Center for Population Health Research, Instituto Nacional de Salud Pública (INSP), Cuernavaca, Mexico
- 2Consejo Nacional de Ciencia y Tecnología (CONACYT)—Instituto Nacional de Salud Pública (INSP), Cuernavaca, Mexico
- 3Center for Evaluation and Surveys Research, Instituto Nacional de Salud Pública (INSP), Cuernavaca, Mexico
- 4Department of Clinical Research and Medical Oncology, Instituto Nacional de Cancerología (INCAN), Mexico City, Mexico
- 5Department of Oncology Gynecology, Instituto Nacional de Cancerología (INCAN), Mexico City, Mexico
- 6Oncology Department, Hospital General de México “Eduardo Liceaga”, Mexico City, Mexico
- 7Gynecologist Oncologist of MAGNI Gineco-Obstetras S.C, Mexico City, Mexico
- 8Chronic Infections and Cancer Division, Center for Research on Infectious Diseases, Instituto Nacional de Salud Pública (INSP), Cuernavaca, Mexico
Introduction: The COVID-19 pandemic disrupted the preventive services for cervical cancer (CC) control programs in Mexico, which will result in increased mortality. This study aims to assess the impact of the pandemic on the interruption of three preventive actions in the CC prevention program in Mexico.
Methods: This study is a retrospective time series analysis based on administrative records for the uninsured population served by the Mexican Ministry of Health. Patient data were retrieved from the outpatient service information system and the hospital discharge database for the period 2017–2021. Data were aggregated by month, distinguishing a pre-pandemic and a pandemic period, considering April 2020 as the start date of the pandemic. A Poisson time series analysis was used to model seasonal and secular trends. Five process indicators were selected to assess the disruption of the CC program, these were analyzed as monthly data (N=39 pre-pandemic, N=21 during the pandemic). HPV vaccination indicators (number of doses and coverage) and diagnostic characteristics of CC cases were analyzed descriptively. The time elapsed between diagnosis and treatment initiation in CC cases was modeled using restricted cubic splines from robust regression.
Results: Annual HPV vaccination coverage declined dramatically after 2019 and was almost null in 2021. The number of positive Papanicolaou smears decreased by 67.8% (90%CI: -72.3, -61.7) in April–December 2020, compared to their expected values without the pandemic. The immediate pandemic shock (April 2020) in the number of first-time and recurrent colposcopies was -80.5% (95%CI:−83.5, −77.0) and -77.9% (95%CI: −81.0, −74.4), respectively. An increasing trend was observed in the proportion of advanced stage and metastatic CC cases. The fraction of CC cases that did not receive medical treatment or surgery increased, as well as CC cases that received late treatment after diagnosis.
Conclusions: Our analyses show significant impact of the COVID-19 pandemic with declines at all levels of CC prevention and increasing inequalities. The restarting of the preventive programs against CC in Mexico offers an opportunity to put in place actions to reduce the disparities in the burden of disease between socioeconomic levels.
Introduction
Cervical cancer (CC) is caused majorly by a persistent infection of high-risk human papilloma virus (HR-HPV). This neoplasm is considered preventable by HPV vaccination, for those cases caused by the genotypes included in the available vaccines and by routine screening for precancerous lesions. However, CC remains a significant cause of cancer-related mortality and a major public health problem, particularly in low- and middle-income countries (LMICs) (1). In 2020, GLOBOCAN estimated the occurrence of 604,127 new cases (particularly in middle-aged women) and 341,831 deaths from CC worldwide, with 80% occurring in LMICs (2). In 2020 9,439 new cases (4.8%) and 4335 deaths were estimated in Mexico, with a 5-year prevalence of 38/100,000, which is equivalent to 25026 prevalent cases (3).
In 2020, the World Health Assembly adopted a strategy for the elimination of CC, with the intention of achieving for all countries an incidence rate of less than 4 cases per 100,000 women by 2030 (4). For this, three strategies have been proposed: prevention (target of 90% of girls aged 15 years or younger fully vaccinated against HPV), early detection (target of 70% of women aged 35–45 years screened by molecular methods to detect HR-HPV DNA), and guaranteed treatment (target of 90% of women) diagnosed with CC.
According to the Mexican standard NOM 014-SSA2-1994 for the prevention, detection, diagnosis, treatment, control, and epidemiological surveillance of CC, a comprehensive control program for CC in Mexico must include all three types of prevention (5). Primary prevention includes specific protective actions through the free delivery of the anti-HPV prophylactic vaccine, in a two-doses vaccination schedule since 2016, as part of a universal program targeting girls in fifth grade of primary school, aged 9-11 years.
Secondary prevention includes early detection of premalignant cervical lesions in women aged 25–34 years either by a Papanicolaou (Pap) smear test or direct visualization with acetic acid when a Pap smear is not available, and biomolecular testing for HPV detection in women aged 35–64 years. These tests should be performed free of charge to all applicant women in public sector health facilities (5).Tertiary prevention includes the follow-up of women with premalignant lesions and CC, and timely treatment (6).
Latin America and the Caribbean (LAC) has been one of the areas most affected by the ongoing COVID-19 pandemic, with Mexico as an epicenter. Mexico has the fifth highest number of COVID-19 deaths in the world, after the United States, Brazil, India, and Russia (7). COVID-19 has affected, either directly or indirectly, all health systems in the world (8–10). Maternal and child health services, among other health services and programs, have reported poorer results and disruptions because of the pandemic (11, 12); sexual and reproductive health services (13, 14) and cancer screening programs have also been impacted (15).
Cancer screening programs worldwide, including CC preventive programs, have been particularly affected by the COVID-19 pandemic, as evidenced by lower HPV vaccination coverage rates (16, 17), fewer histological and cytological samples taken, fewer immunohistochemistry and molecular tests performed (18), fewer supplies available to perform molecular HPV laboratory services (19), a lower proportion of women screened for CC before and during the COVID-19 pandemic (20), excess CC diagnosis (21), and longer delays in treating cancer patients (22–24).
During the pandemic phase, Mexican national health authorities implemented hospital conversion strategies, prioritizing the allocation of human and biomedical resources for COVID-19 patients requiring hospitalization (25). Hospital conversion affected all “nonessential” health services, including public cancer screening programs. Further disruptions to these services came from reduced availability of public transportation, patient fear of going to hospitals, and staffing shortages, as some health workers were reassigned to support COVID-19 response services (26).
Since estimating the effect of COVID-19 on the resilience of health services depends on several assumptions, it is necessary to evaluate the effect of COVID-19 on primary, secondary and tertiary prevention strategies to compensate for opportunities lost due to the pandemic. Therefore, this study aims to assess the impact of the COVID-19 pandemic on the disruption of activities at all three levels of the CC prevention program in Mexico.
Materials and methods
Study design
This is a retrospective time series analysis based on administrative records to evaluate the disruption caused by the COVID-19 pandemic in the CC care program for uninsured population, served by the Mexican Ministry of Health (MoH). Administrative records of health services provided in outpatient and inpatient care in facilities managed by the MoH and clinical records of the National Cancer Institute (INCAN) were analyzed.
Data source
Data were retrieved from the outpatient services information system (SIS) (27) and the hospital discharges database (SAEH) for the period 2017-2021. Both systems collect information on the part of the population lacking social security (approximately 50% of Mexico’s total population) that received medical care in health facilities administered by the MoH. Anonymized data on patients who attended INCAN in the period 2017–2021 were also included. Approval was obtained for access to clinical record information (INCAN/CI/O411/O411/2022/082). INCAN is one of the main oncology referral centers in Mexico, managed by the MoH and serving the uninsured population. Data were aggregated by month; pre-pandemic and pandemic periods were identified, with April 2020 as the start date of the pandemic. Thus, the pre-pandemic period was defined as January 2017 to March 2020 (39 months), and the pandemic period as April 2020 to December 2021 (21 months).
Measured indicators
Data retrieved from the SIS included HPV vaccination data (primary prevention): vaccination, coverage, first and second doses of HPV vaccine in female students in grade 5 and/or 11 years of schooling, and third dose of HPV vaccine in females aged 14 years and older; data on screening and treatment of precancerous lesions (secondary prevention): total cytology read, positive cytology, first-time colposcopy, and recurrent colposcopy; diagnosis and treatment of invasive cancer (tertiary prevention): CC-related hospital discharges according to ICD-10 leading cause classification. Indicators of the level of tertiary prevention retrieved from the INCAN database included: histopathological diagnosis, clinical stage, type of treatment and time from diagnosis to initiation of treatment.
Five process indicators were selected to evaluate the disruption on the CC care program: total Pap smears read, positive Pap smears, first-time colposcopy, and subsequent colposcopy as indicators of the secondary prevention level, and CC-related hospital discharges according to ICD-10 classification of main cause as indicators of the tertiary prevention level. In Mexico, HPV vaccination is massively administered during the National Health Weeks; thus, these indicators of vaccine administration could not be included in our statistical models; instead, the results of a descriptive analysis are given in the corresponding section. Data on tertiary prevention retrieved from the INCAN database were aggregated by pre-pandemic and pandemic periods and by month to calculate average time between diagnosis and treatment initiation.
Statistical analysis
A descriptive analysis of all variables was performed; frequencies, percentages, and central tendency and dispersion statistics were calculated, and data were plotted to capture trends. We fitted Poisson regression models using each of the five process indicators as dependent variable. These models were fitted with Newey-West standard errors, which are consistent in terms of heteroscedasticity and autocorrelation (28). Our linear predictor, the logarithm of the mean in a Poisson regression model, included a linear time term and indicator variables for each month of the year (one excluded as a reference category) to model seasonal fluctuations around the trend. The trend model coefficient was expressed as the mean ratio between consecutive months after exponentiation, including a 95% confidence interval. Our models were trained from January 2017 through March 2020, extending the trend to include a seasonality component from April 2020 through December 2021, to estimate expected monthly values for each process indicator under the model and during the pandemic period; these were used to contrast observed values.
The sum of expected values for each of the five process indicators was calculated for four periods: April 2020, April-December 2020, January-December 2021, and April 2020 to December 2021. Standard errors for periods longer than a month were obtained through the delta method, to generate 95% confidence intervals (29). The differences between observed and expected values were then calculated, and confidence limits were mapped from those obtained for expected values to the differences. The differences were also calculated as percentages with respect to the expected values. In this framework, the analyzed process indicators in the pandemic period were considered as realized observations, rather than random variables; therefore, the inference problem focused on estimating baseline values that reproduced a pre-pandemic environment and approximated a counterfactual to the pandemic. A similar approach has been previously applied to estimate excess deaths from different causes in Mexico (30).
The time (number of days) elapsed from diagnosis to treatment initiation from INCAN patient records was modelled as a function of the calendar time (year and month) of patient records using robust regression. Predictors included monthly indicator variables (except for a reference category) to capture possible seasonal fluctuations, and a 4-knot restricted cubic splines function with respect to monthly time (31, 32).
Results
Impact on HPV vaccination (primary prevention)
HPV vaccination is administered during National Health Weeks in October or November each year. The observed patterns from 2017 to 2021 are shown in Figure 1, with a significantly reduced vaccine delivery in 2019 compared to previous years. HPV vaccination dropped to near zero after April 2020. This pattern was also evident for the second dose, with no reduction in 2019. The third dose in risk population, in contrast, is delivered throughout the year (Figure 1), although significantly fewer vaccines were applied after April 2020. With respect to HPV vaccination coverage rates in the target population, showed a significant decline for the first dose of 59% in 2018 to 30.1% in 2019, 17.8% in 2020 and 1.2% in 2021.
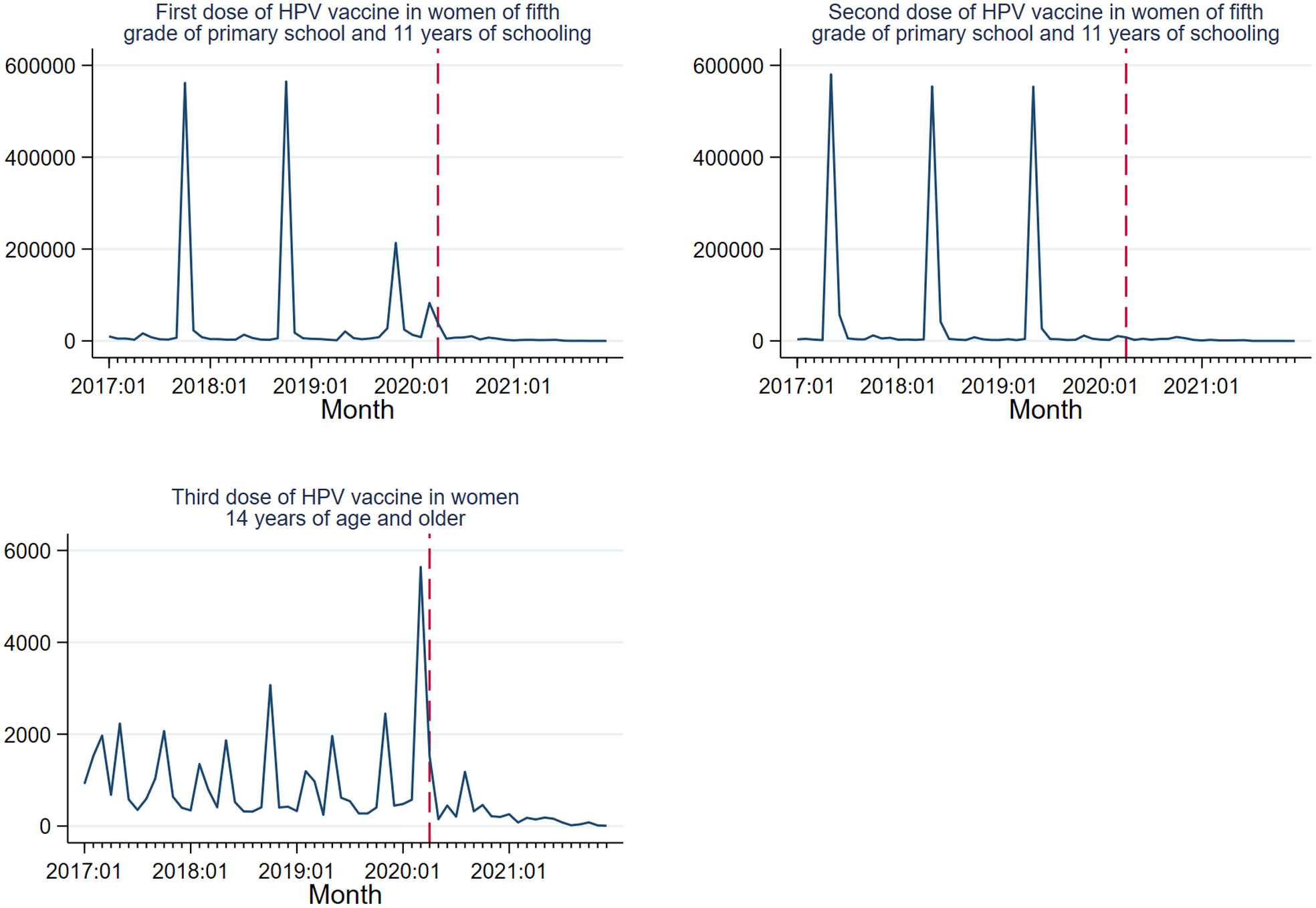
Figure 1 HPV vaccination trends 2017–2021. Mexico. Source: Outpatient provided services information system. 2017-2021. DGIS.
Impact on screening and treatment of precancerous lesions (secondary prevention)
Monthly descriptive statistics for selected program indicators are shown in Table 1. In general, the number and variability of services provided were lower during the pandemic than in the pre-pandemic months, except for CC hospital discharges, which showed similar descriptive statistics in both periods.
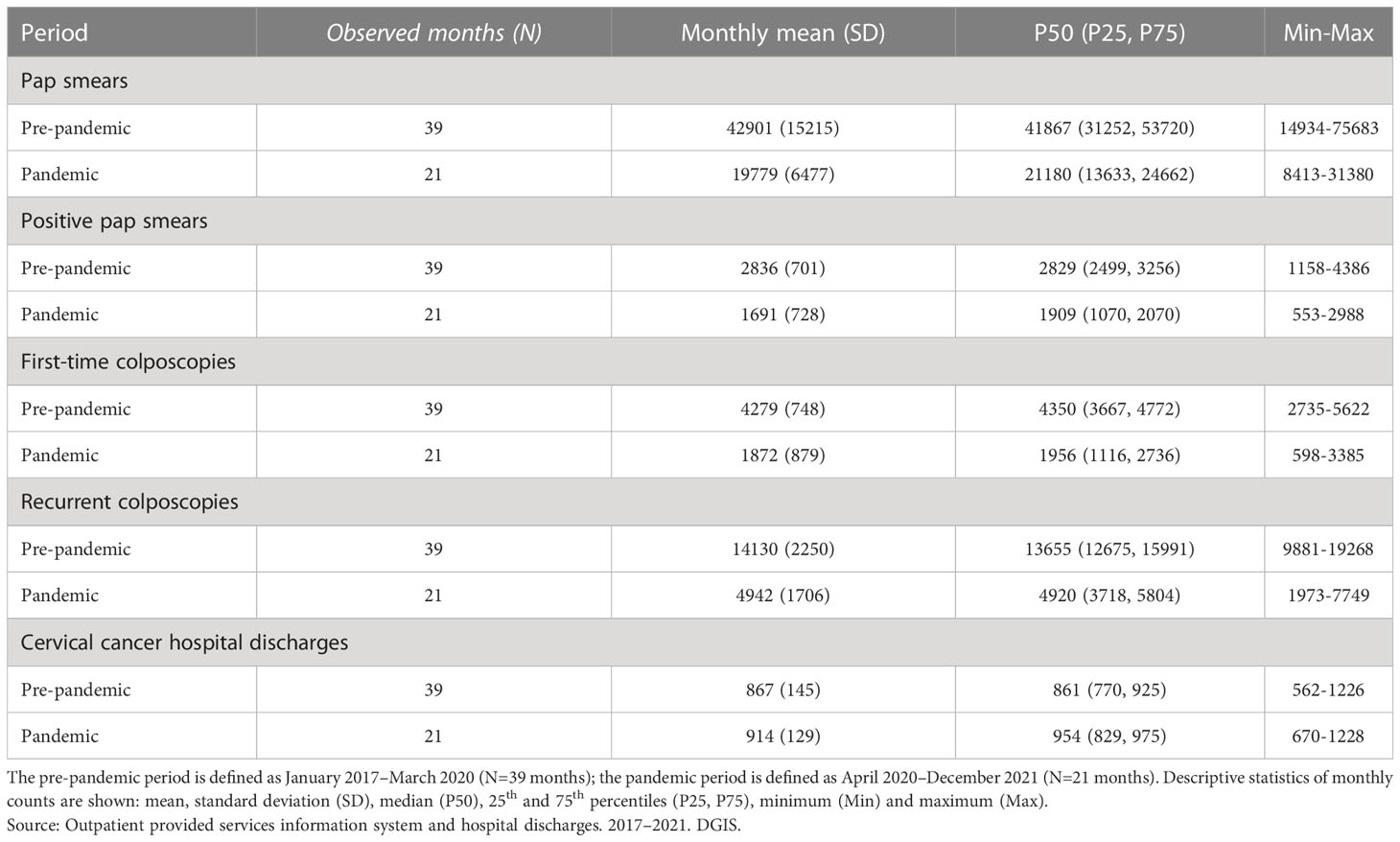
Table 1 Descriptive statistics of monthly data of selected indicators of the CC program.
Observed counts of process indicators related to CC program services along with their differences with respect to their expected values under a pre-pandemic trend are shown in Table 2 for four pandemic periods: a) an immediate shock in April 2020, b) April to December 2020, c) January to December 2021, and d) April 2020 to December 2021. At the beginning of the pandemic period in Mexico (April 2020), the number of Pap smears showed an abrupt reduction of 38.0% (Table 2), followed by a slow upward trend (Figure 2). Results from the Poisson time-series model that adjusted for seasonal fluctuations showed a negative slope during the pre-pandemic period with a monthly reduction of 2.1% (mean ratio [MR] = 0.979, 95% CI: 0.976–0.982) in the number of Pap smears, this corresponds to an annual reduction of 22.5%. Overall, the number of Pap tests decreased by 44.1% in 2020 (April–December) with respect to the number expected as predicted by our model. The number of Pap smears recovered in 2021, exceeding by 12.6% our model predictions. In the period April 2020–December 2021, an overall reduction of 16.1% was observed (Table 2).
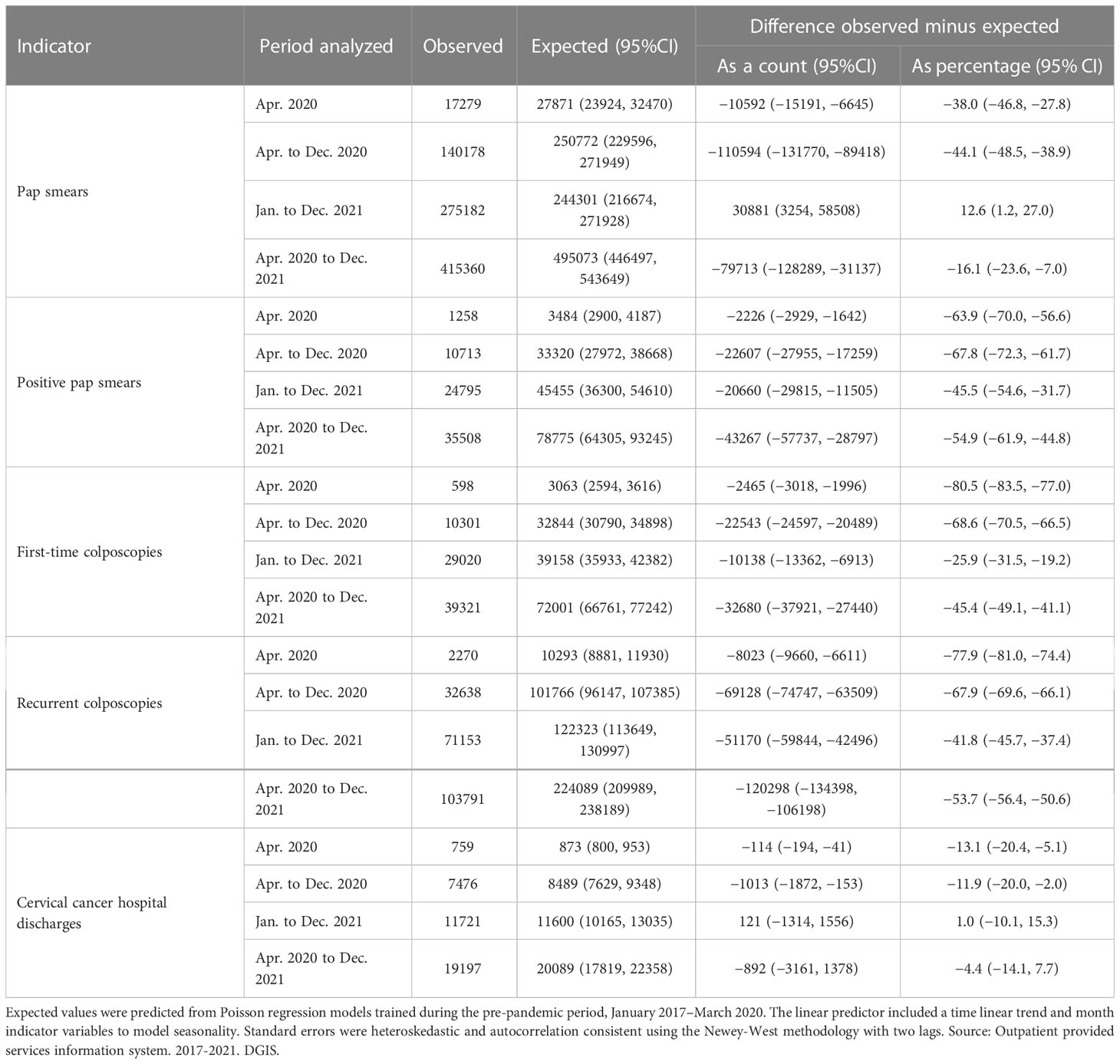
Table 2 Estimation of changes in secondary prevention services and CC hospital discharges in the pandemic period with respect to pre-pandemic projected trends.
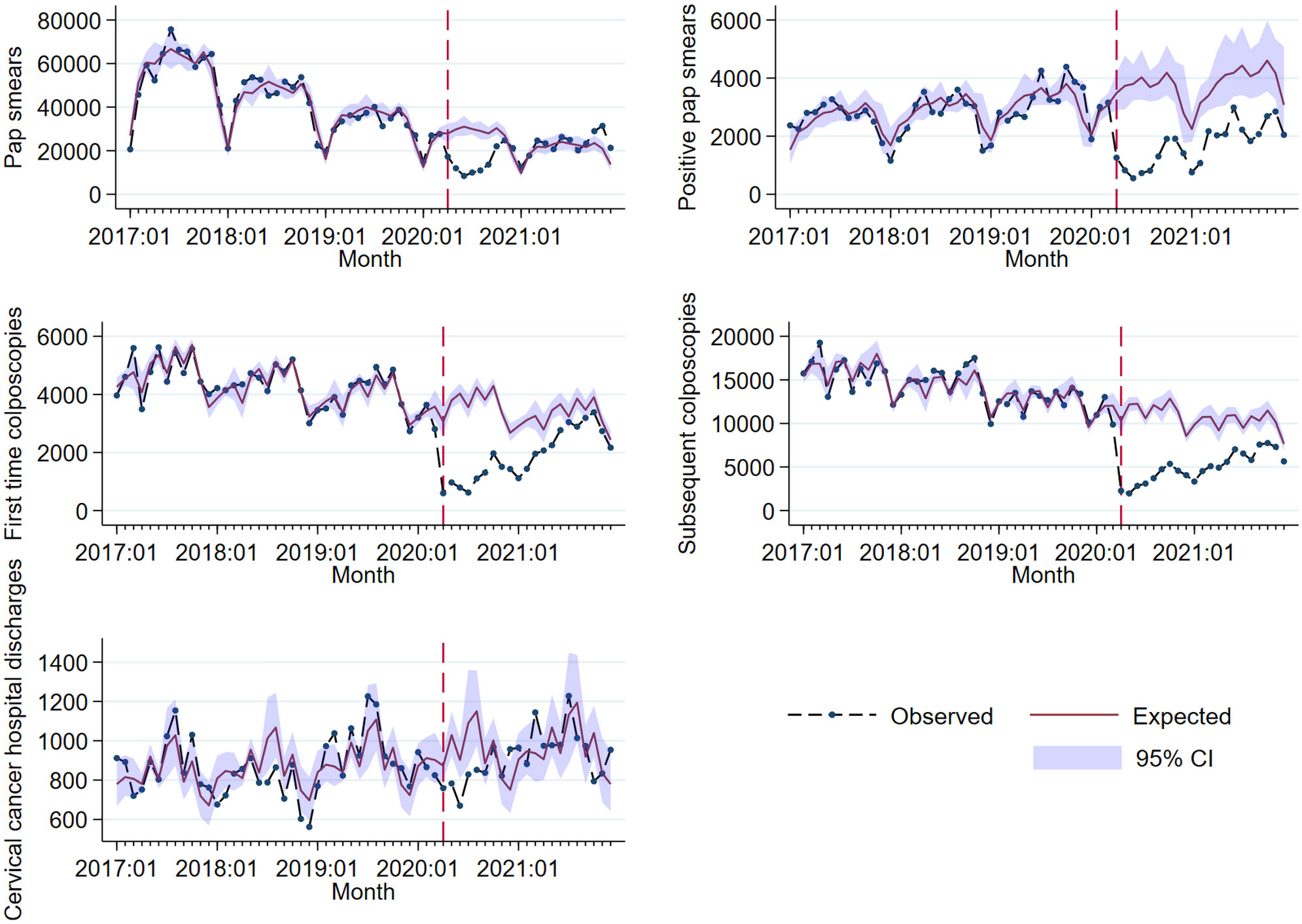
Figure 2 Observed and fitted trends for five process indicators to evaluate disruption of the CC program. Source: Outpatient provided services information system and Hospital discharges. 2017-2021. DGIS. The dashed line marks the start of the pandemic period (April 2020–December 2021). Expected trends were obtained from Poisson models trained during the pre-pandemic period (January 2017–March 2020). The linear predictor included a time linear trend and month indicator variables to model seasonality. Standard errors were heteroskedastic and autocorrelation consistent using the Newey-West methodology with two lags. CI, Confidence Interval.
With respect to pre-pandemic data, positive results of Pap smears showed an upward trend, although a reduction of 63.9% was observed at the beginning of the pandemic (April 2020). A reduction of 67.8% was found in positive Pap smears in the period April–December 2020, compared with the value predicted by our model. The overall reduction in 2021 was 45.4%, and it was 54.9% in the period April 2020–December 2021 (Table 2).
The number of first-time and recurrent colposcopies showed a downward trend in the pre-pandemic period after adjusting for seasonality; on average, there was a monthly decrease of 0.7% (MR = 0.992, 95% CI: 0.990–0.994) in the number of first-time colposcopies, and a decrease of 0.9% (MR = 0.990, 95% CI: 0.989–0.993) in the number of recurrent colposcopies, corresponding to an average annual reduction of 9.1% and 10.6%, respectively. The number of first-time and recurrent colposcopies also showed a sudden reduction of 80.5% and 77.9%, respectively, in April 2020, followed by an upward trend (Table 2; Figure 2).
Despite this recovery trend, the number of first-time and recurrent colposcopies was below the expected values throughout the pandemic period, as shown in Table 2. A reduction of 68.6% was observed in the number of first-time colposcopies in 2020, and of 25.9% in 2021, while the number of recurrent colposcopies was lower than the expected value by 67.9% in 2020 and by 41.8% in 2021. During the entire pandemic period, the number of first-time and recurrent colposcopies was lower than expected according to our model by 45.4% and 53.7%, respectively (Figure 2).
Impact on diagnosis and treatment of invasive cancer (tertiary prevention)
The number of CC-related hospital discharges also showed a reduction at the beginning of the pandemic period, albeit to a lesser extent (13.1%), followed by a recovery trend in 2020 and 2021 (Table 1; Figure 2). An overall reduction of 11.9% was observed in 2020 with respect to expected hospital discharges in our model. In 2021, no significant differences were observed in the number of hospital discharges with respect to our model in the absence of a pandemic shock.
The distribution of categories of tertiary prevention indicators from patient data of the INCAN database are described in Table 3. An analysis of the number of histopathological diagnoses during the pandemic showed a slight decrease in squamous (from 83.6% to 82.3%) and adenosquamous (from 2.2% to 1.7%) diagnoses compared to the pre-pandemic period, and a small increase in adenocarcinomas (from 10.7% to 11.4%) and neuroendocrine involvement (from 1.6% to 1.9%). While a higher proportion of women were diagnosed in an early stage (21.6%) pre-pandemic; this proportion dropped to 11.4% during the pandemic. A slight increase in the proportion of locally advanced stages was also observed, from 61.8% to 63.6%, while the fraction of metastatic patients increased from 16.6% to 24.5%. The occurrence of untreated cases increased by 3.2 percentage points in the pandemic compared to the pre-pandemic period, and the percentage of women who had access to surgical treatment decreased from 21.1% to 11.7%. With respect to the time elapsed from diagnosis to treatment initiation, the percentage of women who were cared for immediately after diagnosis increased in the pandemic from 5.2% (pre-pandemic) to 8.4%, as did those who were treated within 1-2 weeks. Overall, the fraction of women seen within 2 weeks increased from 6.6% to 9.9%; however, the proportion who received treatment after 8 weeks increased from 36.6% to 46.6% (Table 3).
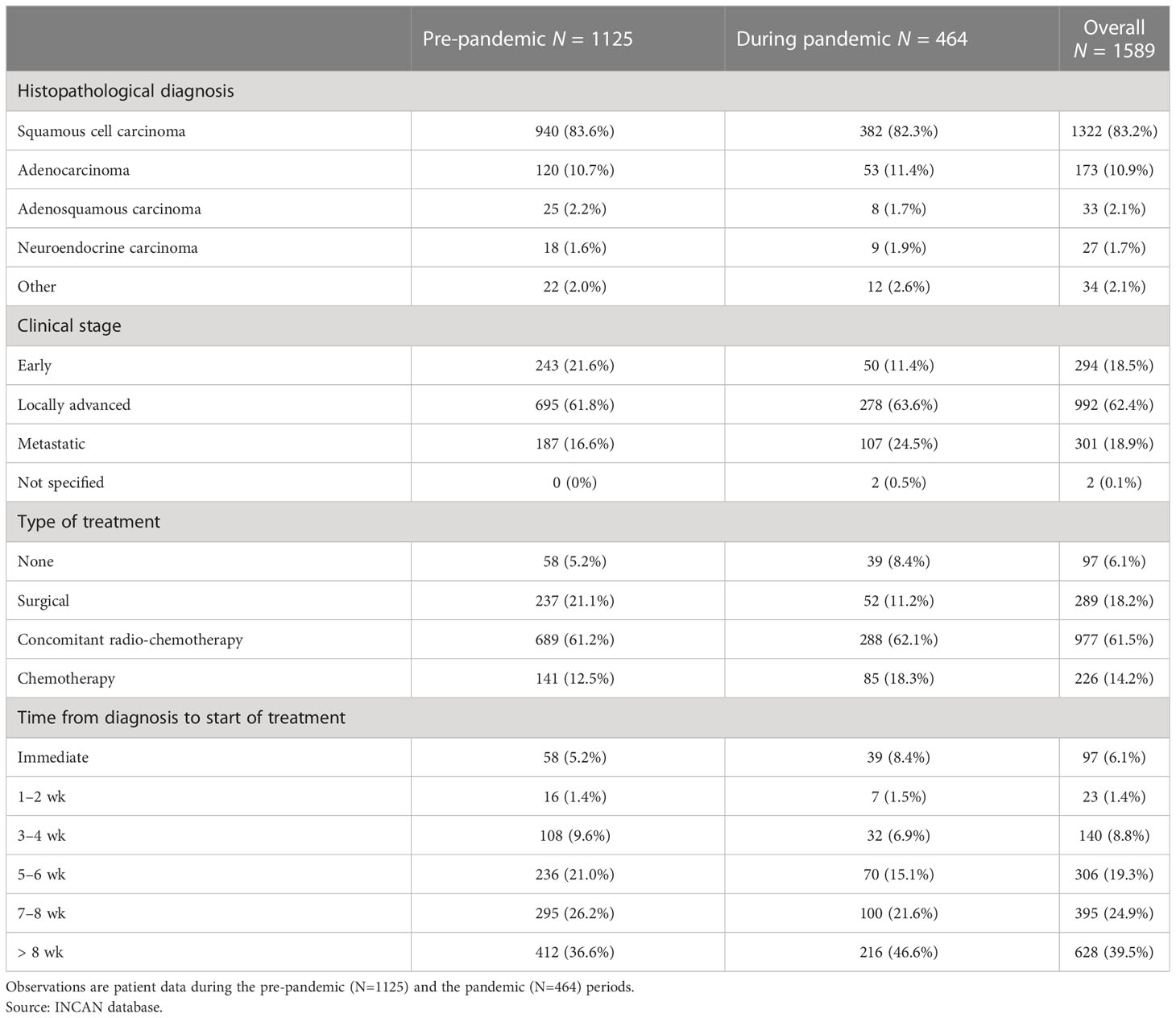
Table 3 Indicators of the tertiary prevention level from INCAN database.
A robust regression analysis of the average time elapsed between diagnosis and treatment initiation (in days) as a function of the date of patient records is shown in Figure 3. The restricted cubic spline clearly shows an increasing trend in the time between diagnosis and initiation of treatment after April 2020, even though fewer patients were received. The point size of each data point is proportional to the number of patients.
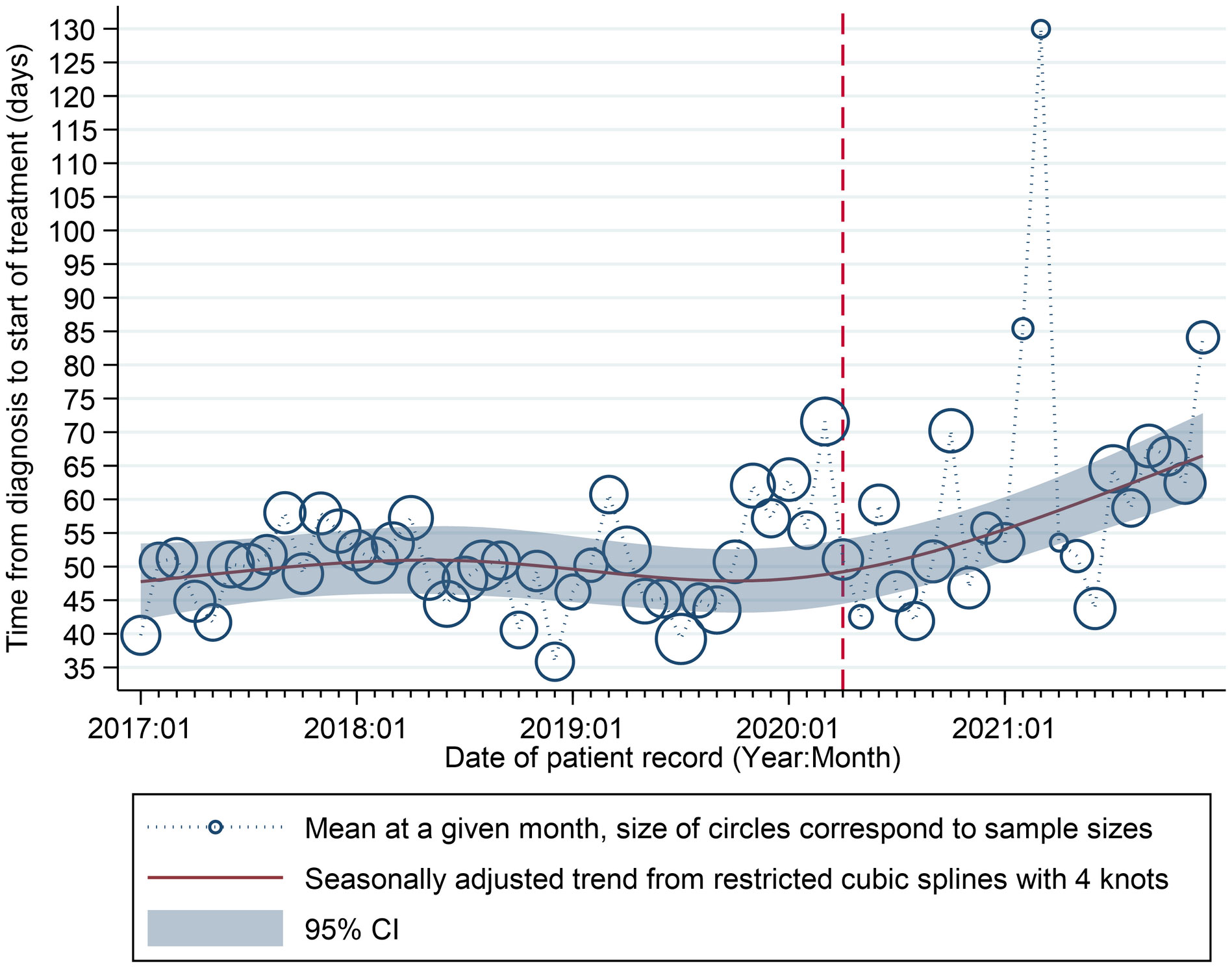
Figure 3 Time elapsed from diagnosis to treatment initiation (days) and date of patient records. Source: INCAN Database Relationship between time from diagnosis and start of treatment. The data points show the average time in days between diagnosis and start of treatment for each month in the INCAN database from January 2017 to December 2021 and the solid line are the fitted values from robust regression model. The dashed line marks the start of our defined pandemic period.
Discussion
The COVID-19 pandemic has disrupted CC screening programs around the world. This study assesses the impacts of the COVID-19 pandemic on CC prevention program in Mexico. It is important to highlight that given the limited availability of data sources and their quality, we organized effects into three levels considering the following indicators: first, the number of HPV vaccine doses and coverage in the target population (primary prevention); second, the number of positive Pap smears and, and the number of initial and subsequent colposcopy examinations (secondary prevention); third, the number of discharges associated with CC, histopathological diagnosis, clinical stage, type of treatment and time from diagnosis to initiation of treatment (tertiary prevention).
Overall, our analyses revealed significant declines in all levels of CC prevention. In primary prevention, the sharp decline in HPV vaccine doses delivered to the target populations between 2020 and 2021 coincides with the COVID-19 pandemic and the shortage of HPV vaccines on the global market due to an increased demand for such vaccines to achieve the elimination of CC as global target (33) In Mexico, this led to a temporary suspension of vaccination efforts and delayed interventions for the 2020, 2021, and 2022 target populations.
According to the WHO/UNICEF report, we found that vaccination was almost nil in 2021 (34). The COVID-19 pandemic has limited access to vaccines (not just against HPV) in many low- and middle-income countries (35). It is unclear whether the vaccine production capacity will meet global demand. Countries that have discontinued routine HPV vaccination can start plans for future catch-up campaigns for young people who missed HPV vaccination during the pandemic. However, the Strategic Advisory Group of Experts on Immunization (SAGE) Committee proposed strategies to address vaccine shortages during this period, including pausing vaccination of older women (> 15 years), establishing multi-age cohorts until sufficient supplies are available to meet global demand and protocols for delaying the second dose of vaccine by 2-3 years (33).
Two previous studies documented the impact of the COVID-19 pandemic on HPV vaccination services. Estimates of the impact of HPV vaccine coverage during the pandemic in the United States reported that coverage declined in March and April 2020, reaching a low of 23% in previous years (17). Another study reported a significant reduction in the average dose of HPV vaccine administered in Brazil from April to September 2019 (16). Many low- and middle-income countries had to delay of introduction of HPV vaccination (35).
In Mexico, as in other LAC countries, efforts to immunize target populations should be pursued in the months and years ahead in order to restore HPV vaccination rates and minimize medium-term consequences (36). In the long term, HPV vaccines accessibility will improve with the development of new, cheaper and faster-to- manufacture vaccines, which are expected to become available in the next few years (35). One government measure is to administrate only one dose of HPV vaccine. It is well known that one dose of HPV vaccine suffices to achieve good HPV serum antibody levels in girls under 12 years of age and is recommended (37). Therefore, this measure suffices to protect the target population of this group of HPV vaccines.
Regarding secondary prevention, the only indicators available for analysis were the number of analyzed/positive Pap smears and the number of initial and subsequent colposcopy examinations. It is important to note that although cervical screening in Mexico includes both cytology and molecular HPV testing, only information on cytology results is available.
Successful secondary prevention of CC is a multistep process that includes screening of the target population, triage of positive results, colposcopy-biopsy to confirm cervical precancer, and treatment of the precancer. Although limited, comparing the number of Pap smears and colposcopies performed during the pandemic with previous periods allows us to estimate the impact of disruptions of CC prevention program.
The number of positive Pap smears dropped at the start of the pandemic a tends to recover in 2021. This recovery coincides with the application of specific technical guidelines and protocols to reduce the risk of contracting COVID 19 issued by national health authorities (38). In Mexico, only one previous study has performed a similar analysis using data from various health services from the Mexican Institute Social Security (IMSS) Health Information System including the number of women screened for CC between January 2019 and December 2020, this indicator fell by 68% (39).
In an international context, the significant decline in cervical cancer screening rates was due to lockdowns and travel restrictions to contain the COVID-19 pandemic (20). In a study conducted in England, a 6.4% deficit was observed in the number of screening samples with respect to expected values before the pandemic (21).
The overall reduction in the number of Pap smear tests during the pandemic in 2020 with respect to historical data found herein (41.1%) is similar to that reported in Belgium (43.3%) (18) but lower than in Scotland (56%) (40), Italy (64.5%) (41), California (78%) (42), the United States (84%) (43), Canada (85%) (44), and Slovenia (92%) (45).
While our results show that the number of colposcopy procedures performed in Mexico was already declining in the pre-pandemic era, the number of first and recurrent colposcopy procedures decreased further by 45.4% and 53.7% in 2020–2021. A Canadian study reported an average monthly reduction of 39.7% in colposcopy volumes from March to August 2020 compared with the same period in 2019 and a 75.1% reduction at the onset of the pandemic (44). However, other studies that did not provide numerical data reported that colposcopy in women with minor or low-grade cytological abnormalities or persistent HPV infection was delayed worldwide because of the pandemic (40).
According to information from Mexico’s Unified Epidemiological Surveillance System, the impact of the COVID-19 pandemic on CC care programs was reflected in the lower number of reported cases of intraepithelial lesion in 2020 (46). We observed a slight recovery in 2021, but the number of cases was still below those reported in 2019. On the other hand, there are no official reports showing the impact of COVID-19 on indicators included in the regulatory documents related to screening coverage, diagnosis, evaluation and treatment of intraepithelial lesions, and efficiency in access to health services.
At the level of tertiary prevention, according to INCAN data, the most frequently diagnosed type of CC in Mexico before the pandemic was squamous cell carcinoma. Unfortunately, the pandemic there was an increase in the number of cases diagnosed at locally advanced and—even worse—metastatic stages. This result is consistent with a comparative analysis of three independent cervical models by the Cancer Intervention and Surveillance Network of the National Cancer Institute, which found that COVID-19-associated disease would cause a small net increase in the number of CC cases by 2027 (47).
Among the most relevant indicators for evaluating tertiary prevention efforts are the proportion of diagnosed CC cases that received treatment and the estimated time to initiate therapy (48). Our analysis shows that between 2020 and 2021, the proportion of untreated CC confirmed cases increased, while the proportion of early-stage CC cases treated with surgery decreased, becoming the scenario predicted by expert groups in hospitals with significant burden of COVID-19 cases (49).
The meantime between the diagnosis of CC and initiation of treatment has increased since the start of the pandemic. Most patients started treatment after eight weeks, and the relative numbers of this group have continued to increase during the pandemic. Evaluation of this indicator is important in Mexico, as the population most affected by COVID-19-related mortality lives in overpopulated and poor areas (50) and is also the most affected by CC (51).
This delay in treatment because of the pandemic has been badly documented, and few studies have described the impact of treatment delay on survival in patients with early-stage CC (22–24). A US study reported that the average wait time from CC diagnosis to hysterectomy was 4 weeks, and longer waiting times of 2 to 12 weeks were associated with an increased risk of all-cause mortality (23). Since the designated treatment procedures for radical hysterectomy in early-stage CC require hospitalization, these procedures will have to be postponed in areas with higher hospital demand (49).
In our study, it was not possible to analyze survival because the follow-up times of patients during the pandemic are still very short. According to a study on survival of delaying the initiation of concurrent chemoradiotherapy in women with locally advanced CC, in the absence of factors related to tumor aggressiveness, a short waiting time for treatment initiation (<10 weeks) may not be associated with an increased risk of mortality in women with this type of cancer (24). This study is relevant in the context of the current COVID-19 pandemic because fluctuating waves of infection force highly specialized hospitals to significantly reduce access to oncology care services, which would mean a delay in the treatment of these patients.
This study identified several areas for improvement at each sub-process or level of CC prevention program in Mexico, which have been affected by disruptions of preventive health and cancer care services because of the COVID-19 pandemic, in order to achieve the WHO goal of eliminating CC by 2030. Considering the cost of human life and suffering, implementing proper management of CC prevention programs should be a top priority for decision-makers and policy makers of CC prevention systems in all LAC countries to improve the performance indicators (52, 53), owing to the high prevalence of CC, the female cancer with the greatest preventive potential given its natural history.
The WHO global strategy to promote the elimination of CC as a public health issue proposes three coverage targets to be achieved (4): HPV immunization coverage in 15-year-old girls (70%); cervical screening coverage in women aged 35–45 years (70%), at least once in lifetime screening with valid evidence; and treatment coverage in women with precancerous lesions or CC (90%).
From 2017 to 2021, coverage of LAC complete HPV immunization schedule remains low (54). In the region, about 74% of women aged 30–49 years have been screened for cervical cancer at least once in their lifetime (55). The reported full coverage of the HPV vaccination program in Mexico was 97%, 96%, 95%, 5%, 5%, and 1% in 2017, 2018, 2019, 2020, and 2021, respectively (34). Screening coverage in 2019 exceeded 50% of the target population for that year. Although diagnostic screening coverage in colposcopy clinics exceeded 50% in 2019, there is no reliable information on the proportion of patients treated within 92 calendar days (56).
A disadvantage of multistep prevention programs is the need for multiple patient visits, including screening, colposcopy, treatment, and surveillance. At each step, there is a possibility that follow-up could be lost because of factors related to the patient, provider or health system, and an untreated precancerous lesion could progress to cancer (57). In this context, we suggest strategies to improve the prevention, diagnosis, and timely treatment program of CC in Mexico and to achieve the goal of CC elimination at the preventive level through their respective components, as well as three main actors for implementing the program, as shown in Figure 4.
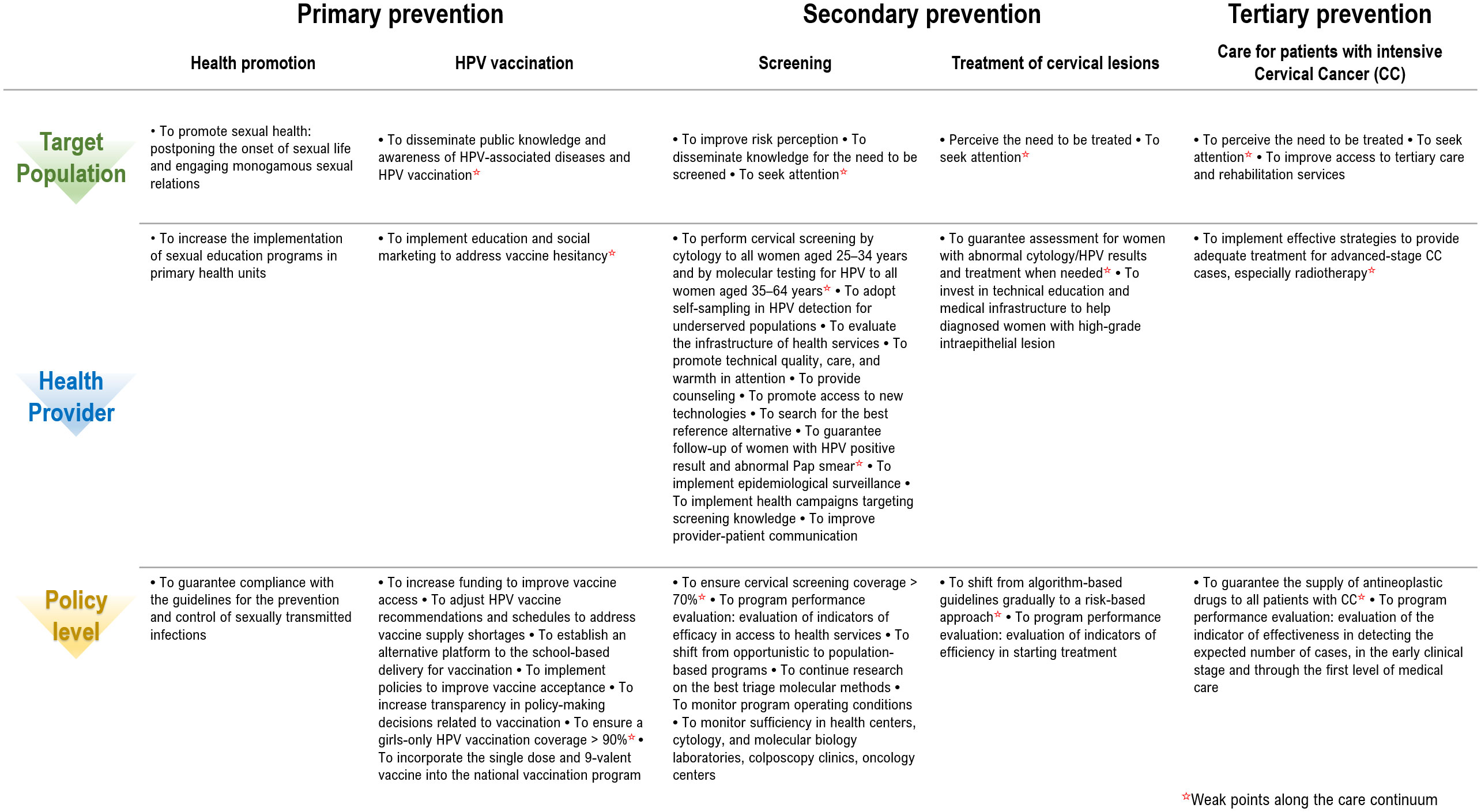
Figure 4 Process model of the cervical cancer prevention program in Mexico. The proposed strategies should be considered by health care providers and policymakers along the cascade of care to move toward the goal of eliminating cervical cancer in Mexico, as well as the critical control points in Mexico’s cervical cancer prevention program process model. *Weaknesses along the continuum of care.
Our study has strengths and limitations. The main strength and contribution of this work is that it allowed us to identify areas affected by the impact of the pandemic in order to improve CC prevention program and provide recommendations for policymakers involved in the management of this program in Mexico towards the goal of CC elimination.
The main limitation of this study is the use of data sources collected from available administrative records which may have quality issues and lack of opportunity. Unfortunately, data on HPV test positivity, on treatment to premalignant lesions, and diagnostic evaluation were not available. Additionally, our data does not include information on CC-related hospital admissions, and thus does not cover the most negative outcomes (death or continuous in-patient treatment during the observation period). A specific limitation was the use of single center data for analysis of the impact at the level of tertiary prevention, since INCAN does not necessarily reflect what happens in all specialized hospitals in the health sector. However, given that the regulations of cancer programs are similar for the health sector and considering that it is one of the main resolutive hospitals in the CC and with the largest budget, possibly the impact of the epidemic is greater in the hospitals with less infrastructure.
In conclusion, the COVID-19 pandemic had a direct impact on CC prevention efforts at all levels in Mexico. This study documents the deterioration in the performance of the CC prevention program by demonstrating the adverse impacts of the pandemic on effectiveness and access to health services because of a significant reduction in the number of HPV vaccines applied and the lower number of patients attending first-time and recurrent colposcopy exams. The impact on the program’s efficiency is also evidenced by the increase in the proportion of cases that started treatment more than 8 weeks after diagnosis and the lower proportion of CC cases detected at an early clinical stage.
Therefore, improving the performance of CC prevention program is crucial to reduce delays in vaccination, to achieve long-term reduction in the incidence of HPV infection, guarantee follow-up of positive cases, promote early detection of invasive cancers, timely initiation of treatment, and to promote disease-free survival. Among other measures, home vaginal self-sampling could offer options for CC prevention and treatment to women with restricted access to health services. These strategies should not only aim to fill the unmet needs created by the pandemic, but also eliminate negative and unnecessary aspects of care for this disease.
In this context, we propose some recommendations that include improving the quality of processes at all three levels of care; for example, improving epidemiological surveillance systems by establishing cancer registries; expand the reach of single-dose immunization; self-collection of vaginal samples for timely molecular diagnostics; early detection in older women; and in according to IARC Handbook, switching from conventional cytology to liquid-bases samples to do HPV as primary screening with cytology triage and typing of the same sample, which could have a large impact on efficacy and maybe on compliance to follow up (58).
Data availability statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found in the article/Supplementary Material.
Author contributions
Conceptualization, KT-P and AC-V. Data curation, LP-M, JH-A and AQ-S. formal analysis, KT-P, LP-M, JH-A and AQ-S. Investigation, KT-P, AC, CA-F, RU, and VM-M. Methodology, KT-P, AC, LP-M, JH-A and AQ-S. Project administration, KT-P. Resources, LP-M, JH-A, AQ-S, TG-C, EA-B, DI-O and LC-P. Software, LP-M, JH-A and AQ-S. Supervision, KT-P. Validation, KT-P and AC. Visualization, LP-M, JH-A and AQ-S. Writing—original draft, KT-P, AC-V, LP-M, JH-A, AQ-S, CA-F, S-RU-S and VM-M. Writing—review and editing, KT-P, AC-V, LP-M, JH-A, AQ-S, S-RU-S, and VM-M. All authors revised the manuscript. All authors contributed to the article and approved the submitted version.
Funding
This work was funded by the Instituto Nacional de Salud Pública, Mexico, and grants from the Consejo Nacional de Ciencia y Tecnología (CONACYT, Mexico) to KTP (FONSEC SSA/IMSS/ISSSTE-2018 grant # A3-S-49099) and to VMM (grant CATEDRAS-2014-C01-#245520).
Acknowledgments
The authors thank the General Directorate for Information in Health for making available the database of services provided 2017–2021 hospital discharge and outpatient services dataset and the Unidad de Inteligencia en Salud Pública for integrating of the information used in this manuscript.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Arbyn M, Weiderpass E, Bruni L, de Sanjoseí S, Saraiya M, Ferlay J, et al. Estimates of incidence and mortality of cervical cancer in 2018: A worldwide analysis. Lancet Glob Health (2020) 8(2):e191–203. doi: 10.1016/S2214-109X(19)30482-6
2. International Agency for Research on Cancer. Cancer Today [Internet]. Cancer incidence and mortality statistics worldwide. Cancer incidence and mortality statistics worldwide. (Lyon, France: WHO) (2020). Available at: https://gco.iarc.fr/today/data/factsheets/cancers/23-Cervix-uteri-fact-sheet.pdf.
3. International Agency for Research on Cancer. Cancer Today [Internet]. Cancer incidence and mortality statistics in Mexico (Lyon, France: WHO) (2020). Available at: https://gco.iarc.fr/today/data/factsheets/populations/484-mexico-fact-sheets.pdf
4. Global strategy to accelerate the elimination of cervical cancer as a public health problem. Geneva: World Health Organization (2020). Available at: https://www.who.int/publications/i/item/9789240014107.
5. Secretariía de Salud. Modificacioín a la Norma oficial mexicana NOM-014- SSA2–1994, para la prevencioín, deteccioín, diagnoístico, tratamiento, control y vigilancia epidemioloígica del caíncer ceírvico uterino . Available at: http://www.salud.gob.mx/unidades/cdi/nom/m014ssa294.pdf.
6. Secretariía de Salud. Programa de Accioín: caíncer ceírvico uterino. In: Programa de Accioín Especiífico Prevencioín y control del Caíncer de la mujer 2013–2018. Mexico City (2002). Available at: https://www.gob.mx/salud/acciones-y-programas/programa-de-accion-especifico-prevencion-y-control-del-cancer-de-la-mujer-2013-2018-9275.
7. Statista, "statista.com," number of novel coronavirus (COVID-19) deaths worldwide as of February 3, 2023, by country, 3 February 2023 . Available at: https://www.statista.com/statistics/1093256/novel-coronavirus-2019ncov-deaths-worldwide-by-country/ (Accessed 7 February 2023).
8. Pujolar G, Oliver-Anglès A, Vargas I, Vázquez ML. Changes in access to health services during the COVID-19 pandemic: A scoping review. Int J Environ Res Public Health (2022) 19(3):1749–79. doi: 10.3390/ijerph19031749
9. Tuczyńska M, Matthews-Kozanecka M, Baum E. Accessibility to non-COVID health services in the world during the COVID-19 pandemic: Review. Front Public Health (2021) 9:760795. doi: 10.3389/fpubh.2021.760795
10. Hategeka C, Carter SE, Chenge FM, Katanga EN, Lurton G, Mayaka SM, et al. Impact of the COVID-19 pandemic and response on the utilisation of health services in public facilities during the firstwave in Kinshasa, the democratic republic of the Congo. BMJ Global Health (2021) 6(7):e005955. doi: 10.1136/bmjgh-2021-005955
11. Aranda Z, Binde T, Tashman K, Tadikonda A, Mawindo B, Maweu D, et al. Disruptions in maternal health service use during the COVID-19 pandemic in 2020: Experiences from 37 health facilities in low- income and middle-income countries. BMJ Global Health (2022) 7(1):e007247. doi: 10.1136/bmjgh-2021-007247
12. Shapira G, Ahmed T, Drouard SHP, Amor Fernandez P, Kandpal E, Nzelu C, et al. Disruptions in maternal and child health service utilization during COVID-19: Analysis from eight sub-Saharan African countries. Health Policy Plan (2021) 36(7):1140–51. doi: 10.1093/heapol/czab064
13. Adelekan B, Goldson E, Abubakar Z, Mueller U, Alayande A, Ojogun T, et al. Effect of COVID-19 pandemic on provision of sexual and reproductive health services in primary health facilities in Nigeria: A cross-sectional study. Reprod Health (2021) 18(1):166–87. doi: 10.1186/s12978-021-01217-5
14. Banke-Thomas A, Yaya S. Looking ahead in the COVID-19 pandemic: emerging lessons learned for sexual and reproductive health services in low- and middle-income countries. Reprod Health (2021) 18(1):248–55. doi: 10.1186/s12978-021-01307-4
15. Alkatout I, Biebl M, Momenimovahed Z, Giovannucci E, Hadavandsiri F, Salehiniya H, et al. Has COVID-19 affected cancer screening programs? A systematic review. Front Oncol (2021) 11:675038. doi: 10.3389/fonc.2021.675038
16. Silva TMRD, Nogueira de Sá ACMG, Beinner MA, Abreu MNS, Matozinhos FP, Sato APS, et al. Impact of the COVID-19 pandemic on human papillomavirus vaccination in Brazil. Int J Public Health (2022) 67:1604224. doi: 10.3389/ijph.2022.1604224
17. Daniels V, Saxena K, Roberts C, Kothari S, Corman S, Yao L, et al. Impact of reduced human papillomavirus vaccination coverage rates due to COVID-19 in the united states: A model based analysis. Vaccine (2021) 39(20):2731–35. doi: 10.1016/j.vaccine.2021.04.003
18. de Pelsemaeker MC, Guiot Y, Vanderveken J, Galant C, Van Bockstal MR. The impact of the COVID-19 pandemic and the associated Belgian governmental measures on cancer screening, surgical pathology and cytopathology. Pathobiology (2021) 88(1):46–55. doi: 10.1159/000509546
19. Poljak M, Cuschieri K, Waheed DE, Baay M, Vorsters A. Impact of the COVID-19 pandemic on human papillomavirus-based testing services to support cervical cancer screening. Acta Dermatovenerol Alp Pannonica Adriat (2021) 30(1):21–6. doi: 10.1159/000509546
20. Sasidharanpillai S, Ravishankar N. The short-term impact of COVID-19 pandemic on cervical cancer screening: A systematic review and meta-analysis. Asian Pac J Cancer Prev (2022) 23(5):1497–504. doi: 10.31557/APJCP.2022.23.5.1497
21. Castanon A, Rebolj M, Pesola F, Pearmain P, Stubbs R. COVID-19 disruption to cervical cancer screening in England. J Med Screen (2022) 4:9691413221090892. doi: 10.1177/09691413221090892
22. Matsuo K, Huang Y, Matsuzaki S, Klar M, Wright JD. Effect of delay in surgical therapy for early-stage cervical cancer: An implication in the coronavirus pandemic. Eur J Cancer (2020) 139:173–76. doi: 10.1016/j.ejca.2020.08.025
23. Matsuo K, Novatt H, Matsuzaki S, Hom MS, Castaneda AV, Licon E, et al. Wait-time for hysterectomy and survival of women with early-stage cervical cancer: A clinical implication during the coronavirus pandemic. Gynecol Oncol (2020) 158(1):37–43. doi: 10.1016/j.ygyno.2020.05.019
24. Matsuo K, Huang Y, Matsuzaki S, Ragab OM, Roman LD, Wright JD. Association between definitive chemoradiotherapy wait-time and survival in locally-advanced cervical cancer: Implications during the coronavirus pandemic. Gynecol Oncol (2021) 161(2):414–21. doi: 10.1016/j.ygyno.2021.02.026
25. Gómezchico-Velasco R, Villanueva-Sáenz CS, Salazar-Lizárraga D, Yáñez-Gutiérrez L, Márquez-González H. COVID-19 and fontan: bioethical analysis derived from the need for hospital reconversion. Bol Med Hosp Infant Mex (2022) 79(1):44–50. doi: 10.24875/BMHIM.21000058
26. Sollozo-Dupont I, Galvaín-Espinoza HA, Castillo-Loípez JP, Beniítez-Loípez EO, Rocha-Nava SL, Villasenãor-Navarro Y. Impact of the covid-19 pandemic on breast cancer screening and how to act quickly and safely. Salud Publica Mex (2022) 64:333–9. doi: 10.21149/13412
27. Secretaría de Salud. Dirección general de información en salud, in: Subsitema de egresos hospitalarios. Available at: https://sinba.salud.gob.mx/CubosDinamicos (Accessed 15 June 2022).
28. Newey WK, West KD. A simple, positive semi-definite, heteroskedasticity and autocorrelation consistent covariance matrix. Econometrica (1987) 55(3):703–8.
30. Palacio-Mejía LS, Hernández-Ávila JE, Hernández-Ávila M, Dyer-Leal D, Barranco A, Quezada-Sánchez AD, et al. Leading causes of excess mortality in Mexico during the COVID-19 pandemic 2020-2021: A death certificates study in a middle-income country. Lancet Reg Health Am (2022) 13:100303. doi: 10.1016/j.lana.2022.100303
32. Harrell FE Jr. General aspects of fitting regression models. In: Regression modeling strategies with applications to linear models, logistic regression, and survival analysis. New York, NY: Springer (2010). p. 18–9.
33. Garland SM, Stanley MA, Giuliano AR, Moscicki AB, Kaufmann A, Bhatla N, et al. IPVS statement on "Temporary HPV vaccine shortage: Implications globally to achieve equity". Papillomavirus Res (2020) 9:100195. doi: 10.1016/j.pvr.2020.100195
34. WHO. WHO joint reporting form on immunization (eJRF). 2017 – 2021 . Available at: https://immunizationdata.who.int/pages/coverage/hpv.html?CODE=MEX&ANTIGEN=PRHPV1_F&YEAR.
35. Toh ZQ, Russell FM, Garland SM, Mulholland EK, Patton G, Licciardi PV. Human papillomavirus vaccination after COVID-19. JNCI Cancer Spectr (2021) 5(2):pkab011. doi: 10.1093/jncics/pkab011
36. Smith DL, Perkins RB. Low rates of HPV vaccination and cervical cancer screening: Challenges and opportunities in the context of the COVID-19 pandemic. Prev Med (2022) 159:107070. doi: 10.1016/j.ypmed.2022.107070
37. Gilca V, Salmerón-Castro J, Sauvageau C, Ogilvie G, Landry M, Naus M, et al. Early use of the HPV 2-dose vaccination schedule: Leveraging evidence to support policy for accelerated impact. Vaccine (2018) 36(32 Pt A):4800–5. doi: 10.1016/j.vaccine.2018.02.004
38. Secretarias de Salud y del Trabajo y Previsión Social. Lineamientos y documentos técnicos por COVID-19. Available at: https://www.gob.mx/profedet/documentos/lineamientos-y-documentos-tecnicos-por-covid-19.
39. Doubova SV, Leslie HH, Kruk ME, Pérez-Cuevas R, Arsenault C. Disruption in essential health services in Mexico during COVID-19: An interrupted time series analysis of health information system data. BMJ Glob Health (2021) 6(9):e006204. doi: 10.1136/bmjgh-2021-006204
40. Masson H. Cervical pap smears and pandemics: The effect of COVID-19 on screening uptake & opportunities to improve. Womens Health (Lond) (2021) 17:17455065211017070. doi: 10.1177/17455065211017070
41. Acuti Martellucci C, Morettini M, Flacco ME, Manzoli L, Palmer M, Giacomini G, et al. Delivering cervical cancer screening during the COVID-19 emergency. BMJ Sex Reprod Health (2021) 47(4):296–99. doi: 10.1136/bmjsrh-2021-201099
42. Miller MJ, Xu L, Qin J, Hahn EE, Ngo-Metzger Q, Mittman B, et al. Impact of COVID-19 on cervical cancer screening rates among women aged 21-65 years in a Large integrated health care system - southern California, January 1-September 30, 2019, and January 1-September 30, 2020. MMWR Morb Mortal Wkly Rep (2021) 70(4):109–13. doi: 10.15585/mmwr.mm7004a1
43. DeGroff A, Miller J, Sharma K, Sun J, Helsel W, Kammerer W, et al. COVID-19 impact on screening test volume through the national breast and cervical cancer early detection program, January-June 2020, in the united states. Prev Med (2021) 151:106559. doi: 10.1016/j.ypmed.2021.106559
44. Meggetto O, Jembere N, Gao J, Walker MJ, Rey M, Rabeneck L, et al. The impact of the COVID-19 pandemic on the Ontario cervical screening program, colposcopy and treatment services in Ontario, Canada: A population-based study. BJOG (2021) 128(9):1503–10. doi: 10.1111/1471-0528.16741
45. Ivanuš U, Jerman T, Gašper Oblak U, Meglič L, Florjančič M, Strojan Fležar M, et al. The impact of the COVID-19 pandemic on organised cervical cancer screening: The first results of the Slovenian cervical screening programme and registry. Lancet Reg Health Eur (2021) 5:100101. doi: 10.1016/j.lanepe.2021.100101
46. Secretaría de salud. Dirección general de Epidemiología. Boletín histórico epidemiológico (2021). Available at: https://www.gob.mx/salud/acciones-y-programas/historico-boletin-epidemiologico.
47. Burger EA, Jansen EE, Killen J, Kok IM, Smith MA, Sy S, et al. Impact of COVID-19-related care disruptions on cervical cancer screening in the united states. J Med Screen (2021) 28(2):213–6. doi: 10.1177/09691413211001097
48. Austad K, Chary A, Xocop SM, Messmer S, King N, Carlson L, et al. Barriers to cervical cancer screening and the cervical cancer care continuum in rural Guatemala: A mixed-method analysis. J Glob Oncol (2018) 4:1–10. doi: 10.1200/JGO.17.00228
49. Ramirez PT, Chiva L, Eriksson AGZ, Frumovitz M, Fagotti A, Gonzalez Martin A, et al. COVID-19 global pandemic: Options for management of gynecologic cancers. Int J Gynecol Cancer (2020) 30(5):561–3. doi: 10.1136/ijgc-2020-001419
50. Ríos V, Denova-Gutiérrez E, Barquera S. Association between living in municipalities with high crowding conditions and poverty and mortality from COVID-19 in Mexico. PLoS One (2022) 17(2):e0264137. doi: 10.1371/journal.pone.0264137
51. Knaul FM, Rodriguez NM, Arreola-Ornelas H, Olson JR. Cervical cancer: lessons learned from neglected tropical diseases. Lancet Glob Health (2019) 7(3):e299–300. doi: 10.1016/S2214-109X(18)30533-3
52. Godoy LR, Possati-Resende JC, Guimarães YM, Pedrão PG, Dos Reis R, Longatto-Filho A. Implementation of HPV tests in Latin America: What we learned; what should we have learned, and what can we do better? Cancers (Basel) (2022) 14(11):2612–24. doi: 10.3390/cancers14112612
53. Alfaro K, Maza M, Cremer M, Masch R, Soler M. Removing global barriers to cervical cancer prevention and moving towards elimination. Nat Rev Cancer (2021) 21(10):607–8. doi: 10.1038/s41568-021-00396-4
54. WHO. WHO joint reporting form on immunization (eJRF). 2017 – 2021. Available at: https://immunizationdata.who.int/pages/coverage/hpv.html?CODE=AMR&ANTIGEN=PRHPVC_F&YEAR.
55. Bruni L, Serrano B, Roura E, Alemany L, Cowan M, Herrero R, et al. Cervical cancer screening programmes and age-specific coverage estimates for 202 countries and territories worldwide: a review and synthetic analysis. Lancet Glob Health (2022) 10(8):e1115–27. doi: 10.1016/S2214-109X(22)00241-8
56. Centro Nacional de Equidad de Género y Salud Reproductiva (CNEGySR). Base de datos de. [en línea]: Sistema de información de cáncer de la mujer (SICAM procacu) . México: Secretaría de Salud (Accessed 24 June 2022).
57. Wentzensen N, Clarke MA, Perkins RB. Impact of COVID-19 on cervical cancer screening: Challenges and opportunities to improving resilience and reduce disparities. Prev Med (2021) 151:106596. doi: 10.1016/j.ypmed.2021.106596
Keywords: COVID-19, uterine cervical neoplasm, prevention and control, health impact assessment, time series analysis, Mexico
Citation: Cruz-Valdez A, Palacio-Mejía LS, Quezada-Sánchez AD, Hernández-Ávila JE, Galicia-Carmona T, Cetina-Pérez LdC, Arango-Bravo EA, Isla-Ortiz D, Aranda-Flores CE, Uscanga-Sánchez S-R, Madrid-Marina V and Torres-Poveda K (2023) Cervical cancer prevention program in Mexico disrupted due to COVID-19 pandemic: Challenges and opportunities. Front. Oncol. 13:1008560. doi: 10.3389/fonc.2023.1008560
Received: 01 August 2022; Accepted: 27 February 2023;
Published: 09 March 2023.
Edited by:
Alessandra Buja, University of Padova, ItalyReviewed by:
Martin Perez-Santos, Benemérita Universidad Autónoma de Puebla, MexicoPaolo Giorgi Rossi, IRCCS Local Health Authority of Reggio Emilia, Italy
Copyright © 2023 Cruz-Valdez, Palacio-Mejía, Quezada-Sánchez, Hernández-Ávila, Galicia-Carmona, Cetina-Pérez, Arango-Bravo, Isla-Ortiz, Aranda-Flores, Uscanga-Sánchez, Madrid-Marina and Torres-Poveda. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Kirvis Torres-Poveda, a2p0b3JyZXNAaW5zcC5teA==
†These authors have contributed equally to this work and share first authorship
‡ORCID: Aurelio Cruz-Valdez, orcid.org/000-0003-0656-7166
Lina Sofia Palacio-Mejía, orcid.org/0000-0003-3203-9420
Amado D. Quezada-Sánchez, orcid.org/0000-0003-3258-8198
Juan Eugenio Hernández-Ávila, orcid.org/0000-0001-9638-6718
Tatiana Galicia-Carmona, orcid.org/0000-0001-5556-9155
Lucely Cetina-Pérez, orcid.org/0000-0003-2018-7338
Eder Arango-Bravo, orcid.org/0000-0002-6501-8776
David Isla-Ortiz, orcid.org/0000-0001-8987-8669
Carlos E. Aranda-Flores, orcid.org/0000-0002-3204-103X
Vicente Madrid-Marina, orcid.org/0000-0002-9305-6884
Kirvis Torres-Poveda, orcid.org/0000-0001-9608-9617