 Silvia Alberti-Violetti1*
Silvia Alberti-Violetti1* Marco Ardigò2
Marco Ardigò2 Cesare Massone3
Cesare Massone3 Alessandro Pileri4,5
Alessandro Pileri4,5 Raffaella Sala6
Raffaella Sala6 Miriam Teoli2
Miriam Teoli2 Vieri Grandi7
Vieri Grandi7 Pietro Quaglino8
Pietro Quaglino8 Nicola Pimpinelli7
Nicola Pimpinelli7 Emilio Berti1
Emilio Berti1- 1Dermatology Unit, Fondazione IRCCS Ca’ Granda Ospedale Maggiore Policlinico, Department of Pathophysiology and Transplantation, University of Milan, Milan, Italy
- 2San Gallicano Dermatological Institute IRCCS, Rome, Italy
- 3Dermatology Unit & Scientific Directorate, Galliera Hospital, Genova, Italy
- 4Dermatology, IRCCS Azienda Ospedaliera-Universitaria di Bologna, Policlinico di Sant’Orsola, Bologna, Italy
- 5Department of Medical and Surgical Sciences, Alma Mater Studiorum University of Bologna, Bologna, Italy
- 6Dermatology Unit, ASST Spedali Civili and University of Brescia, Brescia, Italy
- 7Department of Health Sciences, Dermatology Unit, University of Florence, Florence, Italy
- 8Department of Medical Sciences, Dermatology Clinic, University of Turin, Turin, Italy
Background: Topical chlormethine (CL) is recommended as a first-line treatment for early-stage mycosis fungoides (MF) and in 2017, the European Medicines Agency approved the CL gel formulation to treat adult patients. More recently, to increase patient compliance and adherence, clinicians have developed flexible protocols that allow the concomitant use of CL gel with topical corticosteroids in daily practice regimens. Therefore, sharing real-life data on CL gel use and side effects management may help improve the use of this agent.
Objectives: To expand knowledge about the actual use of CL gel in patients with MF, the present study assessed the improvement of MF skin lesions after CL gel treatment and provided information on the management of cutaneous adverse events (AEs) in a real-life setting.
Methods: This was an Italian retrospective study conducted among six dermatology referral centers. Patients ≥18 years affected by MF and in treatment with CL gel (160 µ/g), alone or in combination according to routine clinical practice, between December 2019 and December 2021 were considered. The study’s primary aim was to evaluate the effectiveness of CL gel in terms of overall response rate (ORR) after 3 months of treatment.
Results: A total of 79 patients (61% male) with different stages of MF (84% early stage) were included. CL gel was prescribed mainly in association with topical corticosteroids (66% of patients). ORR after 3 months of treatment was 42%, with no differences between early- and advanced-stage MF. Response rates improved over time up to 97% after 18 months of treatment. Overall, 66 AEs were reported in 67% of patients; most were hyperpigmentation (45%) and irritant contact dermatitis (37%). Six AEs led to treatment discontinuation, and five out of six (83%) patients who reported these events resumed treatment after interruption. No AEs were classified as severe.
Conclusions: Our observations support the use of CL gel in patients with early- and advanced-stage MF, making it a valuable treatment option.
1 Introduction
Among cutaneous T-cell lymphoma, the most common form is represented by mycosis fungoides (MF), involving about 60% of cases (1, 2). Skin malignant T-cell infiltration represents the main characteristic of MF, which initial presentation generally involves skin patches and/or plaques which can progress to tumors or erythroderma (3, 4). Diagnosis is frequently delayed and made after several biopsies, and the staging is based on the 2007 TNMB revision (5–7).
Guidelines for the treatment of MF are based on the stage of the disease and primarily aim to reduce symptoms, prevent disease progression, and improve the quality of life (QoL) (8). Currently, topical chlormethine (CL), an alkylating agent used successfully in the treatment of cutaneous T-cell lymphoma since the 1950s, represents the first-line treatment for early-stage patients, according to recommendations by the National Comprehensive Cancer Network and international guidelines (1, 9–11). CL acts by a cytotoxic mechanism on DNA, predominantly altering the neoplastic cell growth and increasing the immunogenic potential of the host (12, 13).
Initially, CL was formulated in an aqueous solution, whose use was limited by the high rate of skin hypersensitivity. The formulation of CL as a vaseline-based ointment partially improved the tolerability, but the rapid drug degradation limited the effectiveness of this formulation (14). In 2013, a multicenter phase II, randomized, blinded study (201 study) compared the efficacy and safety of 0.02% CL ointment with 0.02% CL gel in patients with persistent or recurrent stage I or IIA MF for whom corticosteroids were forbidden, demonstrating the non-inferiority of the gel (15). In this study, the authors recorded longer and faster responses in patients treated with gel compared with the ointment treatment (15). As in previous literature evidence, no detectable systemic absorption of the drug was reported (15, 16). The gel formulation was approved by the European Medicines Agency in 2017 for treating adult patients with MF, and is now commercially available in several European countries (17). In Italy, CL gel is indicated for the treatment of MF in all stages.
More recently, to increase patient compliance and adherence, and prevent treatment discontinuation, clinicians have developed more flexible protocols that allow also the concomitant use of CL gel with topical corticosteroids in daily practice regimens (18–20). Therefore, sharing real-life data on actual use of CL gel and side effect management in clinical practice may help improve the use of this agent.
In the present study, we assess the improvement of skin lesions after CL gel treatment, alone or in combination, as well as information on managing cutaneous adverse events (AEs) according to daily clinical practice. We aim to expand knowledge about the use of CL gel for MF, specifically to determine whether the clinical benefit of topical CL gel persists during long-term therapy, and to evaluate local AEs.
2 Patients and methods
2.1 Study design and patients
This was an Italian retrospective study conducted among six dermatology referral centers (Milan, Rome, Genoa, Bologna, Brescia, and Florence) belonging to the Italian Lymphoma Foundation (“Fondazione Italiana Linfomi, FIL”) cutaneous lymphomas task force. Adult patients with MF and treated with CL gel (160 µg/g), alone or in combination according to routine clinical practice, between December 2019 and December 2021 were considered. Patients for whom retrospective data or information on the type and duration of therapy and clinical outcomes were not available were excluded. The study was conducted according to the Good Clinical Practice International Conference on Harmonization (GCP ICH) E6 following the ethical principles of the Declaration of Helsinki and current legislation on non-profit observational studies. The study protocol was notified to the Ethics Committee of Milano Area 2 (protocol number 7202; 10/02/2022). All the participants signed an informed consent form.
2.2 Study measures
For each patient, the following data were retrieved and collected in a dedicated and anonymized database: gender, age, ethnicity, concomitant therapies, diagnosis (clinical variants), stage, modified severity-weighted assessment tool (15) at the start of therapy and after 3, 6, 12 and 18 months (where applicable) of therapy. AEs and possible disease progression were also reported.
The study’s primary aim was to assess the effectiveness of CL gel in terms of overall response rate (ORR), intended as the percentage of patients who achieved a complete (CR) or partial (PR) response to the treatment after 3 months of treatment. The definition of CR and PR was based on the EORTC-ISCL-USCLC (European Organization for the Research and Treatment of Cancer, International Society for Cutaneous Lymphomas, United States Cutaneous Lymphoma Consortium) criteria (21).
The secondary objective was to compare ORR at 3 months according to the disease stage (early stage: IA, IIA, IB vs advanced stage: IIB). We also seek to report the ORR after 6, 12, and 18 months of treatment according to the stage of disease (early-stage vs advanced-stage), based on proposed treatment duration according to clinical practice, and managed according to the response to therapy. AEs were collected including the type of skin reaction (allergic contact dermatitis assessed through patch test or irritant contact dermatitis) and the percentage of patients who continued the drug application after suspension due to AEs. Correlation analyses were also performed to assess the relationship between skin reactions and ORR.
2.3 Statistical analysis
Continuous variables were shown as mean and standard deviation (st.d) or median and interquartile range (IQR) and categorical variables as number and percentage. The Chi-square test was used to compare categorical variables. ORR time was estimated using the Kaplan-Meier method. Odds ratios (OR) were reported with 95% CIs.
Patients with available data at baseline and relevant time points were included. This results in a diverse population dimension (n) for each parameter at each time point, characteristic of a real-world study.
3 Results
A total of 79 patients (n=48, 61% male) with different stages of MF (n=66, 84% early stage) were included in the study. The median age was 63 years (IQR: 52.3–70). Most patients had classical MF (n=60, 76%).
CL gel administration consisted of daily or alternate application, depending on the skin reaction. CL gel was administered with TCS in 66% of patients (n=52). The most used were high-potency topical steroids. Most patients followed an alternate application of CL (4–5 days a week; n=49; 64%). The percentage of patients who used additional TCS was significantly higher in the alternate CL application group (n=40; 82%) than in the daily application group (n=12; 43%; p<0.001). The clinical characteristics and treatment regimens of the involved patients are summarized in Table 1.
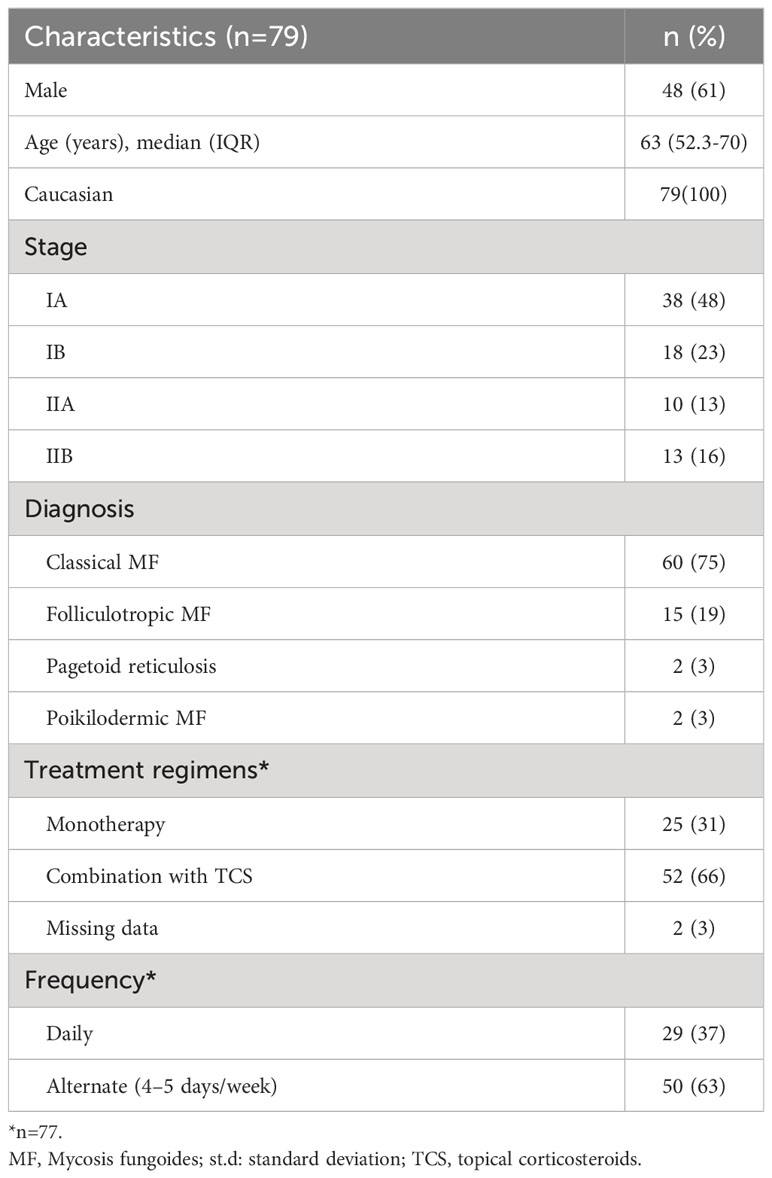
Table 1 Summary of clinical characteristics and treatment regimens.
A total of 35 (44%) patients had concomitant therapies that started before the prescription of CL gel therapy. Among these patients, 12 were advanced stage (92% of all advanced-stage patients) and 27 early stage (41% of all early-stage patients). Concomitant therapies were mainly bexarotene (n=13, 16%), acitretin (n=9, 11%, all patients were in the early stage), and local radiotherapy (RT; n=8, 10%). Supplementary Table 1 summarizes the concomitant therapies according to the disease stage.
3.1 Effectiveness of CL gel treatment
ORR was 42% (n=32) after 3 months of treatment. CR was reported in 12 patients (16%), PR in 20 patients (26%), 43 patients (57%) had stable disease (SD), and one patient had a progression of disease (PD).
3.2 Secondary outcomes
Response rates increased over time, starting from 42% (n=32/76) after 3 months of treatment up to 97% (n=31/32) after 18 months of treatment (Table 2). A total of 21/32 (74%) patients responding at 3 months stopped the application before 12 months of treatment because of achieving CR.
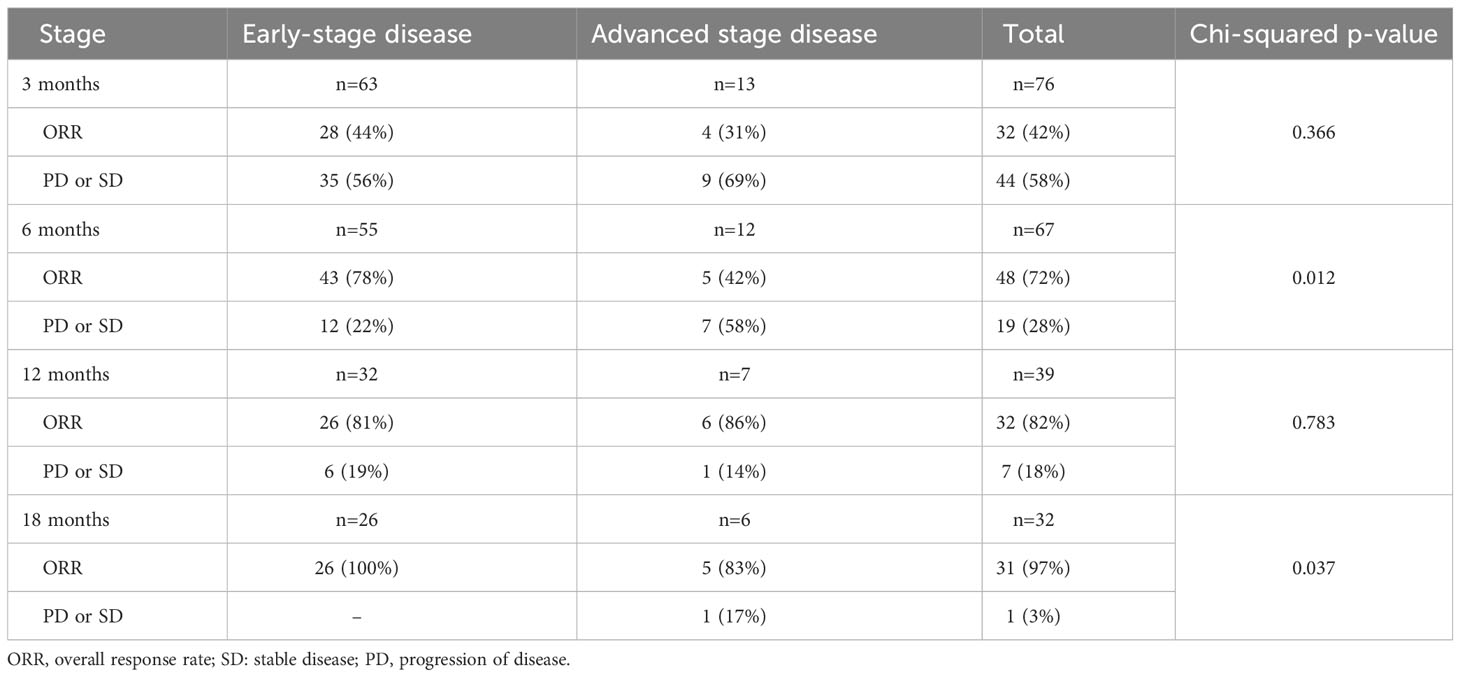
Table 2 Overall response rate (complete or partial response) by stage and visit.
After 3 months of treatment, no significant differences were observed in the proportion of patients achieving CR or PR between early-stage (n=28, 44%) and advanced-stage (n=4, 31%; Chi-squared p=0.366) disease (Table 2). Otherwise, after 6 and 18 months of treatment, the percentage of patients with CR or PR was significantly higher in patients with early-stage disease than in those with advanced-stage disease (6 months: n=43, 78% vs n=5, 42%, Chi-squared p=0.012; 18 months: n=26, 100% vs n=5, 83%, Chi-squared p=0.037) (Table 2).
The mean time to CR/PR was 7.0 ± 0.6 months. The median time to response was significantly shorter in patients with the early-stage disease than those with the advanced-stage disease (6.0 vs 12.0 months; p=0.042; Figure 1).
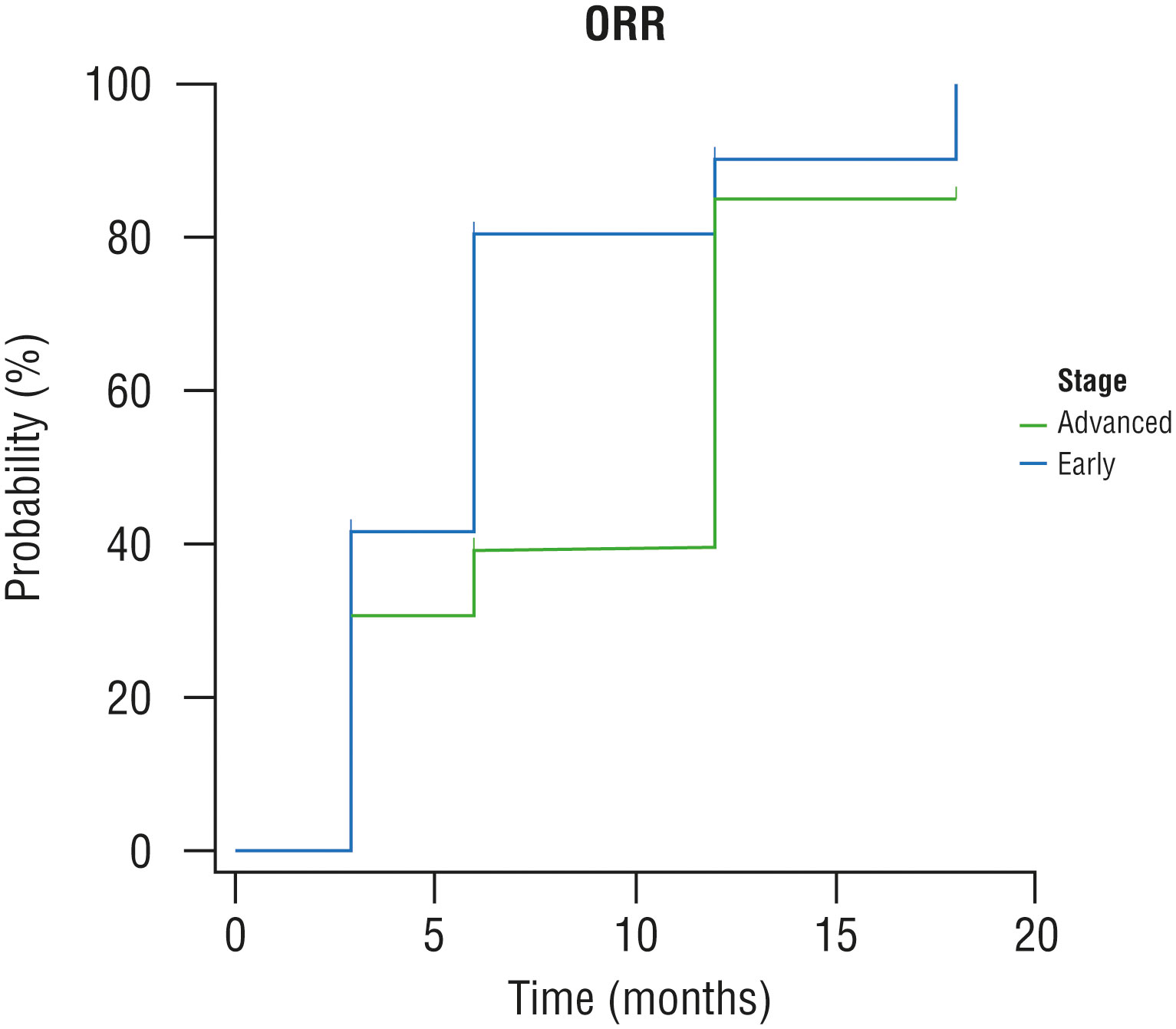
Figure 1 Kaplan-Meier curves, time for overall response rate by stage. ORR: overall response rate.
The mean percentage of skin lesions treated with CL gel among patients with early-stage disease was significantly higher (87%, st.d: 18%) than in advanced-stage patients (67%, st.d: 31%; p=0.002). In the same group of patients, a trend toward the absence of PD was reported (n=55, 85% of patients had no PD), compared with patients with advanced-stage disease (n=8, 62% of patients had no PD; Chi-squared p=0.056). At the same time, a trend toward a lower percentage of treated lesions was reported in patients with PD compared with patients who did not have a progression of disease (85%, st.d: 20% vs 77%, st.d: 20%; p=0.214).
3.3 Safety
The median treatment duration was 26 weeks (1–120 weeks). Overall, 66 AEs were reported in 53 patients (67%); most AEs were hyperpigmentation (n=36, 45%), followed by irritant contact dermatitis (ICD; n=29, 37%) (Table 3). TCS were prescribed to 28 out of 29 (97%) patients who experienced ICD. The frequency of ICD was significantly higher in patients with alternate applications compared with daily application (46% vs 21%, OR: 0.3, CI: 0.1–0.9, p=0.028) (Table 3). The frequency of hyperpigmentation was lower in patients with alternate applications, but the statistical significance was not reached (58% vs 38%, p=0.141) (Table 3).
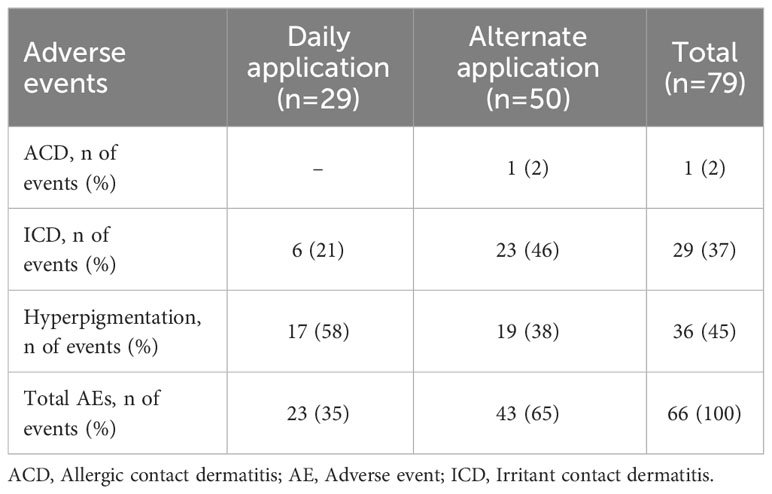
Table 3 Adverse events by the number of applications.
Six (19%) AEs led to treatment discontinuation, and five out of six (83%) patients who reported these events resumed treatment after a period of interruption. No AEs were classified as severe.
3.3.1 Correlation analyses
Considering the best response, a significantly higher ORR was reported in patients with hyperpigmentation (94%) than in patients without hyperpigmentation (77%; p=0.034; Supplementary Table 2). No correlation was observed between the occurrence of ICD and the ORR (Supplementary Table 3).
4 Discussion
CL gel is the first skin-directed therapy purposely developed for the treatment of MF and is currently recommended as first-line therapy for treating adult patients with MF by international guidelines (1, 9, 10).
According to guidelines, skin directed therapies can be associated with systemic therapies in MF patients with advanced-stage disease, as a complement to optimize the response to these therapies and reduce side effects (22, 23). In real-life management of MF, patients with early- and advanced-stage disease are prescribed more flexible CL gel regimens than those reported in the pivotal study, providing also combined treatment with low-frequency TCS application or radiotherapy or other treatments (15, 18, 19, 24). However, with the exception of the PROVE study, real-life data on CL gel use and side effect management in clinical practice are limited mainly to small populations or case series (12, 25–30).
Our study included 79 patients, representing one of the largest patient cohorts in reference to available real-life studies. In our cohort, most patients were in the early stage (84%), and CL gel was mainly prescribed in combination with TCS (66% of patients), according to the guidelines (9–11). In 92% of cases, advanced-stage patients followed a concomitant therapy. In these patients, CL gel was mainly used on the difficult-to-treat areas, which were more resistant to systemic therapies.
Our findings showed that CL gel was effective for treating lesions in 42% of patients after 3 months of therapy, with no differences between early- and advanced-stage MF (Chi-squared p=0.366). These data align with previous evidence from real-world literature, which reports an ORR between 40–50% (25–30).
After 6 and 18 months of treatment, the percentage of patients with CR or PR was significantly higher in patients with early-stage disease than in those with advanced-stage disease (p=0.012 and p=0.037, respectively). Moreover, the mean time to clinical response was shorter in patients with early-stage disease than in those with advanced-stage disease (p=0.042). The mean percentage of treated lesions was higher in early-stage patients compared with advanced stage (p=0.002). This result could be related to the trend toward the absence of PD observed in this patient group, considering also that the percentage of treated lesions was lower in patients with PD. This observation aligns with previous real-life evidence suggesting that patients with early-stage disease may have more-durable responses or higher response rates to CL gel than patients with advanced-stage disease (28).
We observed that response rates increased over time (from 42% at 3 months to 97% at 18 months), highlighting the importance of constant treatment with CL gel, as previously observed (28, 30).
Throughout the current study, 39% of patients developed some degree of dermatitis. Among them, almost all patients (97%) who experienced ICD were also prescribed TCS. Previous prospective and real-life studies supported this combined approach and reported that the use of TCS allowed the long-term administration of CL gel until clinical response, without altering its activity (26, 31, 32). In particular, in the prospective, randomized, open-label MIDAS study, the use of topical triamcinolone ointment showed to be a useful adjuvant when treating patients with CL gel, reducing inflammation without altering the effectiveness of the therapy.28 Only six patients using CL gel discontinued the treatment and, in five cases, patients resumed treatment with reduced applications. Although dermatitis is commonly reported during CL gel treatment, a reduction in the frequency of treatment administration may reduce treatment discontinuation, and the occurrence of dermatitis does not affect the likelihood of response, as observed in our cohort (33). These data support the versatile use of CL gel with dose and application rate adaptability.
In our cohort, 35 patients experienced skin hyperpigmentation, which spontaneously resolved after the treatment. Moreover, the ORR was significantly higher in patients with hyperpigmentation (94%) than those without hyperpigmentation (77%; p=0.034). Consistent with previous observations, our results support the association between hyperpigmentation and post-inflammatory dermatitis in regressing lesions, with an effect on melanocytes, as evidenced by an increase in the basal number of melanocyte (27).
This analysis has some limitations typical of observational studies; for example, the reduced number of patients at follow-up, particularly at 12 and 18 months and the inaccurate monitoring of the onset of side effects. However, the assessment of the duration of response after treatment discontinuation due to CR was not among the aims of the study, which were the ORR and safety of CL gel treatment. In addition, therapeutic regimens were not-standardized, as frequently observed in real-life studies, with most of advanced-stage patients performing concomitant therapies (92%), even if the use of systemic treatments was prior to the introduction of CL gel. For completeness of information, it should be reported that at the time of the study, maintenance therapies after CR were not part of clinical practice.
Despite these limitations, our study includes one of the largest series of MF patients treated in a real-world practice setting, providing useful data to optimize the daily use of CL gel treatment.
5 Conclusion
This study represents one of the largest series of MF patients treated in a real-world practice setting. Results showed that after 3 months of treatment, CL gel was effective in MF patients with both early- and advanced-stage disease, with a good tolerability profile. Response rates increased over time, highlighting the importance of continued treatment with CL gel. According to our data, CL gel can be effectively and safely used in combination with other therapies for MF. In conclusion, our observations support the use of CL gel in patients with early- and advanced-stage MF, making it a valuable treatment option.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by Ethics Committee of Milano Area 2 (register number 7202, 10/02/2022). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
SA-V: Conceptualization, Data curation, Formal analysis, Writing – original draft, Writing – review & editing. MA: Data curation, Formal analysis, Writing – review & editing. CM: Data curation, Formal analysis, Writing – review & editing. AP: Data curation, Formal analysis, Writing – review & editing. RS: Data curation, Formal Analysis, Writing – review & editing. MT: Data curation, Formal Analysis, Writing – review & editing. VG: Data curation, Formal Analysis, Writing – review & editing. PQ: Data curation, Formal Analysis, Writing – review & editing. NP: Data curation, Formal Analysis, Writing – review & editing. EB: Data curation, Formal Analysis, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
Editorial, graphical, and statistical assistance was provided by Simonetta Papa, PhD, Valentina Mirisola, PhD, Massimiliano Pianta, Valentina Attanasio and Aashni Shah (Polistudium SRL, Milan, Italy). This assistance was supported by Recordati Rare Diseases.
Conflict of interest
SA-V: advisory board from Takeda, Kyowa Kirin, Helsinn-Recordati; CM: advisory board from Takeda, Kiowa Kirin; PQ: advisory board and speaker fee from Takeda, Kyowa Kirin, Celgene, Helsinn-Recordati, Therakos.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2023.1298296/full#supplementary-material
References
1. Willemze R, Hodak E, Zinzani PL, Specht L, Ladetto M, Guidelines Committee ESMO. Primary cutaneous lymphomas: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol (2018) 29:iv30–40. doi: 10.1093/annonc/mdy133
2. Willemze R, Cerroni L, Kempf W, Berti E, Facchetti F, Swerdlow SH, et al. The 2018 update of the WHO-EORTC classification for primary cutaneous lymphomas. Blood. (2019) 133:1703–14. doi: 10.1182/blood-2018-11-881268
3. Hwang ST, Janik JE, Jaffe ES, Wilson WH. Mycosis fungoides and Sézary syndrome. Lancet. (2008) 371:945–57. doi: 10.1016/S0140-6736(08)60420-1
4. Krejsgaard T, Odum N, Geisler C, Wasik MA, Woetmann A. Regulatory T cells and immunodeficiency in mycosis fungoides and Sézary syndrome. Leukemia. (2012) 26:424–32. doi: 10.1038/leu.2011.237
5. Kaufman AE, Patel K, Goyal K, O'Leary D, Rubin N, Pearson D, et al. Mycosis fungoides: developments in incidence, treatment and survival. J Eur Acad Dermatol Venereol. (2020) 34:2288–94. doi: 10.1111/jdv.16325
6. Denis D, Beneton N, Laribi K, Maillard H. Management of mycosis fungoides-type cutaneous T-cell lymphoma (MF-CTCL): focus on chlormethine gel. CMAR. (2019) 11:2241–51. doi: 10.2147/CMAR.S138661
7. Olsen E, Vonderheid E, Pimpinelli N, Willemze R, Kim Y, Knobler R, et al. Revisions to the staging and classification of mycosis fungoides and Sezary syndrome: a proposal of the International Society for Cutaneous Lymphomas (ISCL) and the cutaneous lymphoma task force of the European Organization of Research and Treatment of Cancer (EORTC). Blood. (2007) 110:1713–22. doi: 10.1182/blood-2007-03-055749
8. Wehkamp U, Ardigò M, Papadavid E, Querfeld C, Nikbakht N. Chlormethine gel for patients with mycosis fungoides cutaneous T cell lymphoma: A review of efficacy and safety in clinical trial and real-world settings. Adv Ther (2022) 39:3979–4002. doi: 10.1007/s12325-022-02219-w
9. Latzka J, Assaf C, Bagot M, Cozzio A, Dummer R, Guenova E, et al. EORTC consensus recommendations for the treatment of mycosis fungoides/Sézary syndrome - Update 2023. Eur J Cancer. (2023) 195:113343. doi: 10.1016/j.ejca.2023.113343
10. National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines (NCCN Guidelines®). Primary cutaneous lymphomas. Version 2.2020 . Available at: https://www.nccn.org/professionals/physician_gls/pdf/primary_cutaneous.pdf (Accessed 20 12 2022).
11. Gilson D, Whittaker SJ, Child FJ, Scarisbrick JJ, Illidge TM, Parry EJ, et al. British Association of Dermatologists and U.K. Cutaneous Lymphoma Group guidelines for the management of primary cutaneous lymphomas 2018. Br J Dermatol (2019) 180:496–526. doi: 10.1111/bjd.17240
12. Laghi A, Franceschini C, Mandel VD, Teoli M, Musicco F, Sansone M, et al. Topical chlormethine gel in the treatment of mycosis fungoides: A single-center real-life experience and systematic review of the literature. Dermatol Ther (2022) 35:e15683. doi: 10.1111/dth.15683
13. Chang YT, Ignatova D, Hoetzenecker W, Pascolo S, Fassnacht C, Guenova E. Increased chlormethine-induced DNA double-stranded breaks in Malignant T cells from mycosis fungoides skin lesions. JID Innov (2021) 2:100069. doi: 10.1016/j.xjidi.2021.100069
14. Kim YH, Martinez G, Varghese A, Hoppe RT. Topical nitrogen mustard in the management of mycosis fungoides: update of the Stanford experience. Arch Dermatol (2003) 139:165–73. doi: 10.1001/archderm.139.2.165
15. Lessin SR, Duvic M, Guitart J, Pandya AG, Strober BE, Olsen EA, et al. Topical chemotherapy in cutaneous T-cell lymphoma: positive results of a randomized, controlled, multi-center trial testing the efficacy and safety of a novel 0.02% mechlorethamine gel in mycosis fungoides. JAMA Dermatol (2013) 149:25–32. doi: 10.1001/2013.jamadermatol.541
16. Querfeld C, Geskin LJ, Kim EJ, Scarisbrick JJ, Quaglino P, Papadavid E, et al. Lack of systemic absorption of topical mechlorethamine gel in patients with mycosis fungoides cutaneous T-cell lymphoma. J Invest Dermatol (2021) 141:1601–1604.e2. doi: 10.1016/j.jid.2020.12.009
17. Summary of Product Characteristics – Ledaga. London, UK: Actelion Registration Ltd (2017). Available at: https://ec.europa.eu/health/documents/community-register/2017/20170303136935/anx_136935_en.pdf.
18. Geskin LJ, Bagot M, Hodak E, Kim EJ. Chlormethine gel for the treatment of skin lesions in all stages of mycosis fungoides cutaneous t-cell lymphoma: a narrative review and international experience. Dermatol Ther (Heidelb). (2021) 11:1085–106. doi: 10.1007/s13555-021-00539-3
19. Wehkamp U, Jost M, Gosmann J, Grote U, Bernard M, Stadler R. Management of chlormethine gel treatment in mycosis fungoides patients in two German skin lymphoma centers. J Dtsch Dermatol Ges. (2021) 19:1057–9. doi: 10.1111/ddg.14462
20. Mathieu S, Ram-Wolff C, Baylot-Barry M, D’Incan M, Bagot M. L'expérience française de l'usage du gel de chlorméthine pour le traitement du mycosis fongoïde: une série rétrospective de 107 cas du GFELC [The French experience of the use of chlormethine gel for the treatment of mycosis fungoides: a retrospective series of 107 cases of GFELC]. Ann Dermatol Vénéréologie (2016) 143:S155. doi: 10.1016/j.annder.2016.09.166
21. Olsen EA, Whittaker S, Willemze R, Pinter-Brown L, Foss F, Geskin L, et al. Primary cutaneous lymphoma: recommendations for clinical trial design and staging update from the ISCL, USCLC, and EORTC. Blood. (2022) 140:419–37. doi: 10.1182/blood.2021012057
22. Elsayad K, Stadler R, Steinbrink K, Eich HT. Combined total skin radiotherapy and immune checkpoint inhibitors: A promising potential treatment for mycosis fungoides and Sezary syndrome. J Dtsch Dermatol Ges. (2020) 18:193–7. doi: 10.1111/ddg.14044
23. Jennings T, Duffy R, Gochoco A, Knoblauch K, Shi W, Alpdogan SO, et al. Valchlor maintenance therapy for patients with mycosis fungoides who received low dose total skin electron beam treatment. Chin Clin Oncol (2019) 8:13. doi: 10.21037/cco.2018.10.01
24. Elsayad K, Susek KH, Eich HT. Total skin electron beam therapy as part of multimodal treatment strategies for primary cutaneous T-cell lymphoma. Oncol Res Treat (2017) 40:244–52. doi: 10.1159/000475634
25. Kim EJ, Geskin L, Guitart J, Querfeld C, Girardi M, Musiek A, et al. Real-world experience with mechlorethamine gel in patients with mycosis fungoides-cutaneous lymphoma: preliminary findings from a prospective observational study. J Am Acad Dermatol (2020) 83:928–30. doi: 10.1016/j.jaad.2019.12.070
26. Kim EJ, Guitart J, Querfeld C, Girardi M, Musiek A, Akilov OE, et al. The PROVe study: US real-world experience with chlormethine/mechlorethamine gel in combination with other therapies for patients with mycosis fungoides cutaneous T-cell lymphoma. Am J Clin Dermatol (2021) 22:407–14. doi: 10.1007/s40257-021-00591-x
27. Prag Naveh H, Amitay-Laish I, Zidan O, Leshem YA, Sherman S, Noyman Y, et al. Real-life experience with chlormethine gel for early-stage mycosis fungoides with emphasis on types and management of cutaneous side-effects. J Dermatol Treat (2022) 33:2364–70. doi: 10.1080/09546634.2021.1967266
28. Koumourtzis M, Lampadaki K, Dalamaga M, Papadavid E. Chlormethine gel is efficient and safe in mycosis fungoides skin lesions. Acta Derm Venereol. (2022) 102:adv00730. doi: 10.2340/actadv.v102.1095
29. Garcia-Saleem TJ, Stonesifer CJ, Khaleel AE, Geskin LJ. Management of mycosis fungoides with topical chlormethine/mechlorethamine gel: a Columbia University Cutaneous Lymphoma Center experience. Acta Derm Venereol. (2021) 101:adv00544. doi: 10.2340/00015555-3911
30. Papadavid E, Koumourtzis M, Nikolaou V, Lampadaki K, Marinos L, Patsatsi A, et al. Chlormethine gel is effective for the treatment of skin lesions in patients with early- and late-stage mycosis fungoides in clinical practice. J Eur Acad Dermatol Venereol. (2022) 36:1751–7. doi: 10.1111/jdv.18183
31. Querfeld C, Nelson WW, Gor D, Pashos CL, Doan QV, Turini M, et al. Maintenance and concomitant therapy use with chlormethine gel among patients with stage IA/IB mycosis fungoides-type cutaneous T-cell lymphoma (MF-CTCL): A real-world evidence study. Dermatol Ther (Heidelb). (2022) 12:2781–95. doi: 10.1007/s13555-022-00831-w
32. Alexander-Savino CV, Chung CG, Gilmore ES, Carroll SM, Poligone B. Randomized mechlorethamine/chlormethine induced dermatitis assessment study (MIDAS) establishes benefit of topical triamcinolone 0.1% ointment cotreatment in mycosis fungoides. Dermatol Ther (Heidelb) (2022) 12:643–54. doi: 10.1007/s13555-022-00681-6
Keywords: chlormethine gel, CL gel, mycosis fungoides, MF, cutaneous T-cell lymphoma
Citation: Alberti-Violetti S, Ardigò M, Massone C, Pileri A, Sala R, Teoli M, Grandi V, Quaglino P, Pimpinelli N and Berti E (2024) Effectiveness and tolerability of chlormethine gel for the management of mycosis fungoides: a multicenter real-life evaluation. Front. Oncol. 13:1298296. doi: 10.3389/fonc.2023.1298296
Received: 21 September 2023; Accepted: 29 November 2023;
Published: 04 January 2024.
Edited by:
Mohammed Kashani-Sabet, California Pacific Medical Center, United StatesReviewed by:
Khaled Elsayad, University of Münster, GermanyRose Moritz, Charité University Medicine Berlin, Germany
Jennifer DeSimone, University of Virginia, United States
Copyright © 2024 Alberti-Violetti, Ardigò, Massone, Pileri, Sala, Teoli, Grandi, Quaglino, Pimpinelli and Berti. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Silvia Alberti-Violetti, c2lsdmlhLmFsYmVydGlAdW5pbWkuaXQ=