 Gaia Sampogna1*
Gaia Sampogna1* Roberto Brugnoli2,3
Roberto Brugnoli2,3 Giuseppe Didato4
Giuseppe Didato4 Maurizio Elia5
Maurizio Elia5 Edoardo Ferlazzo6
Edoardo Ferlazzo6 Gianluca Serafini7
Gianluca Serafini7 Giampaolo Vatti8
Giampaolo Vatti8 Umberto Volpe9
Umberto Volpe9 Flavio Villani10
Flavio Villani10 Gabriele Sani2,3
Gabriele Sani2,3- 1Department of Psychiatry, University of Campania “L. Vanvitelli”, Naples, Italy
- 2Department of Psychiatry, Fondazione Policlinico Universitario Agostino Gemelli IRCCS, Rome, Italy
- 3Department of Neuroscience, Section of Psychiatry, Università Cattolica del Sacro Cuore, Rome, Italy
- 4Epilepsy Unit, Fondazione IRCCS Istituto Neurologico Carlo Besta, Milan, Italy
- 5Oasi Research Institute-IRCCS, Troina, Italy
- 6Department of Medical and Surgical Sciences, Magna Graecia University, Catanzaro, Italy
- 7Department of Neuroscience, Rehabilitation, Ophthalmology, Genetics, Maternal and Child Health (DINOGMI), Section of Psychiatry, University of Genoa, Genoa, Italy
- 8Unità Operativa Complessa Neurology and Clinical Neurophysiology, University Hospital of Siena, Siena, Italy
- 9Division of Clinical Neurophysiology and Epilepsy Center, Istituto di Ricovero e Cura a Carattere Scientifico Policlinico San Martino, Genoa, Italy
- 10Unit of Clinical Psychiatry, Department of Clinical Neurosciences/DIMSC, Polytechnic University of Marche, Ancona, Italy
Introduction: Medical conditions related to the nervous system affects 3.4 billion individuals worldwide and are collectively ranked as the leading cause of disability-adjusted life years (DALYs). Epilepsy is listed among the ten conditions with the highest age standardized DALYs, while depression is expected to become the first cause of disability for mental disorders by 2030. Persons with epilepsy have a higher risk of developing depression, and vice versa. Epilepsy and depression both can influence individual’s personal functioning, social activities and can increase the risk of sudden epileptic attacks. Depression is probably the most frequent psychiatric comorbidity reported in patients with epilepsy. Several studies have highlighted a bidirectional association between depression and epilepsy.
Methods: The present mini-review is based on expert meetings held in the period May-September 2024. A panel of expert clinicians, working in the field of epilepsy and of clinical psychiatry have been invited to participate, due to their experience and expertise in the topic. Panel members, under the guidance of two senior experts, have identified the relevant topics to be analyzed, discussed and commented.
Results: Included studies dealt with the historical perspective on epilepsy and depression; the complexity of diagnostic and clinical comorbidity between epilepsy and depression; the assessment tools for screening for depression in patients with epilepsy.
Discussion: The clinical condition of patients suffering from comorbid depression and epilepsy represents a challenge for neurologists and psychiatrists. Therefore, the management of comorbid epilepsy and depression requires a detailed clinical characterization of each individual case in order to develop an integrated and personalized management plan.
Introduction
Diseases affecting the nervous system represent the leading cause of disability-adjusted life years (DALYs), with 3.4 billion individuals suffering from these diseases. In the period 1990–2021, a 18.2% increase in the global DALY associated to such conditions have been recorded. Considering the top-ten conditions associated with the highest age-standardised DALYs, epilepsy ranked as first disease. Looking at mental disorders, major depression disorder (MDD) represents the third cause of burden of disease worldwide and it is expected to become the first cause of disability for mental disorders by 2030 (Beghi, 2020). Therefore, both neurological and psychiatric disorders are the leading causes of disability and death worldwide, explaining 14% of the global disease burden.
According to recent WHO estimates, more than 50 million people are affected worldwide from epilepsy, regardless of age, race, geographical region and socioeconomic status (GBD 2021 Nervous System Disorders Collaborators, 2024).
The personal, social and economic burden associated with epilepsy is significantly high, especially in terms of healthcare needs, premature death and work absenteeism and lost productivity. Moreover, patients suffering from epilepsy report high levels of stigma and discrimination, which hamper and delay the access to adequate treatments. People with epilepsy report a three times higher risk compared to general population of premature death. This mortality gap is particularly high in people suffering from epilepsy and living in low- and middle-income countries. A recent WHO report highlights that “up to 70% of people living with epilepsy could live seizure-free if properly diagnosed and treated” (Levira et al., 2017; Manole et al., 2023).
MDD represents the most common severe mental disorder, with more than 300 million of people affected worldwide. The 12-month and lifetime prevalence is of 13.4% and 26.1%, respectively, with the female population reporting a higher incidence compared to male population (14.7% vs. 7.2%, respectively) (Fischer et al., 2023; Salk et al., 2017). The incidence rates are even higher when considering special female population, such as pregnant women. In this target population, up to 10% of them who are pregnant and/or have just given birth experience depression (Sidhu et al., 2019; Fatori et al., 2020; Di Vincenzo et al., 2022; La Verde et al., 2024). Although effective treatments for MDD are available, more than 75% of people in low- and middle-income countries receive no treatment (Evans-Lacko et al., 2018; Tsigebrhan et al., 2023; Sakurai and Kanemoto, 2022). Barriers to effective care include a lack of investment in mental healthcare, lack of trained healthcare providers and social stigma associated with mental disorders (Volpe et al., 2014; Jain et al., 2023; Holt-Lunstad, 2024).
The scenario is even more complex when considering patients suffering from comorbid mental and nervous diseases, in particular suffering from epilepsy and depression. It has been repeatedly highlighted that people with epilepsy have a higher risk of developing depression, and viceversa (Kanner, 2014). Epilepsy and depression both can influence individual’s personal functioning, social activities and they can increase the risk of sudden epileptic attacks (Lee et al., 2018; Cronin et al., 2023).
In patients with epilepsy, the prevalence of depression ranges between 10.7% to 44%, with higher rates in patients with refractory epilepsy (up to 54%) (Qin et al., 2022). Depression represents the most common comorbid condition affecting people with epilepsy (Berk et al., 2023; Abe et al., 2020). The comorbid depressive disorder in people with epilepsy negatively impact on patients’ personal functioning and quality of life. Several studies have highlighted a bidirectional association between depression and epilepsy.
Based on these premises, the present mini-review has been conducted in order to clarify the complexity of comorbidity between epilepsy and depression as well as the main critical issues for the optimal clinical management of patients suffering from these conditions.
Materials and methods
The present mini-review is based on expert meetings held in the period May-September 2024. A panel of expert clinicians, working in the field of epilepsy and of clinical psychiatry have been invited to participate, due to their experience and expertise in the topic.
Panel members, under the guidance of two senior experts, have identified the following topics to be analyzed, discussed and commented: a) historical perspective on epilepsy and depression; b) complexity of comorbidity between epilepsy and depression; c) complexity of clinical presentation of depression in patients with epilepsy; d) screening for depression in patients with epilepsy; e) management plan for persons with comorbid depression and epilepsy; f) unmet clinical needs in the management plan of patients with comorbid depression and epilepsy.
This paper provides an overview of the complex clinical presentation of depressive symptoms/depressive disorder in people suffering from epilepsy and aims to point out the most urgent clinical unmet needs that should be addressed in the next future.
The main areas of interest identified during the meetings are reported in the Results’ section. Updated research studies, as well systematic reviews and meta-analyses related to the clinical characterization and management of depression in people with epilepsy were selected. No date limits were applied. Only articles in English language were selected. The final reference list was generated based on novelty, importance, originality, quality, and relevance to the scope of this review.
Results
Historical perspectives on epilepsy and depression: the long journey of complex diseases toward a modern conceptualization
Epilepsy is considered one of the oldest clinical conditions recognized by medical community, with written records dating back to 4000 BCE (Magiorkinis et al., 2010). The term “epilepsy” derives from the Greek verb epilambanein (επιλαμβάνειν), meaning to be seized or take hold. Studies carried out by Hippocrates (in 400 BC) suggested a natural cause of epilepsy, rather than considering it a divine or sacred epiphenomenon. For the first time, Hippocrates suggested the relationship between epilepsy and depression, stating that “melancholics ordinarily become epileptics, and epileptics, melancholics: what determines the preference is the direction the malady takes; if it bears upon the body, epilepsy, if upon the intelligence, melancholy” (Lewis, 1934).
During the Middle Age, epilepsy and depression were considered as magical or mystical conditions, with people suffering from epilepsy considered as possessed. Such misconception still persists in several low- and middle-income countries, nurturing the stigma surrounding people with epilepsy and delaying the access to adequate care (Kaculini et al., 2021; Saha et al., 2017; Reed, 2024).
In the essay “Anatomy of Melancholy”, written by R. Burton in 1692, he identified several social and psychological factors as causes of depression, including poverty, fear, and loneliness. Subsequently, depressive disorders have been considered as a weakness in temperament, mainly on an heritable basis and–therefore–not amenable to change.
At the same time, the neurologist John Hughlings Jackson–considered as the founder of the modern epileptology–developed the first comprehensive explanation of seizure origin. He proposed the following definition: “Epilepsy is the name given for occasional, sudden, excessive, rapid and local discharges of grey matter”. Subsequently, William Richard Gowers, Jean Martin Charcot, Charles-Moïse Briquet and Bénédict Augustin Morel proposed to differentiate epileptic convulsions from nonepileptic (hysterical) convulsions (Faber, 1997).
In 1917, S. Freud published his conceptualization of depression and he described the concept of melancholia as “being a response to loss, either real (for example, a death) or symbolic (such as failure to achieve the desired goal)” (Freud, 1954).
In 1930s the studies by Hans Berger clarified the aetiopathogenesis of epilepsy, with the discovery of phenobarbital and the development of electroencephalogram (EEG). The localisation of epileptic discharges in the brain and their association with lesions was more important than anything else in determining the character of the seizures. Nevertheless, the clinical impression continued to exist that patients with epilepsy suffer from mental problems. In 1949, the discovery of the temporal lobe focus (and, therefore, of temporal lobe epilepsy), as well as the description of the limbic system, led to the idea of mental disorders being linked to epileptic disturbances in specific brain areas. People with epilepsy were considered mentally normal, but it was assumed that brain dysfunctions would lead to seizures as well as psychological manifestations (Bear, 1979).
Currently, it is believed that not only biological factors (e.g., aetiology, focus localisation), but also medication (e.g., number and types of medication such as phenobarbital, topiramate, brivaracetam, clobazam, levetiracetam, perampanel, vigabatrin and zonisamide) can negatively impact mood (Datta, 2023). Moreover, psychological and social factors (e.g., fear of seizures, perceived stigma) are important aspects in the development of mental disorders in patients suffering from epilepsy (Mendez et al., 1986).
According to the biopsychosocial model of mental disorders, it should be argued that the complex reorganization of brain circuits leading to the two conditions occurs in predisposed individuals and such a predisposition is due to a combination of genetic background and environmental factors (Maj et al., 2020; Maj, 2023; Fusar-Poli et al., 2023). This model could be useful for explaining why some patients develop only epilepsy or only depression or both depending on the individual combinations of predisposing factors and environmental contributors/stressors (Østergaard et al., 2023; Fiorillo and Giordano, 2022; Madigan et al., 2023).
Focus on comorbidity between epilepsy and depression
Several factors should be considered for explaining the close inter-relation between epilepsy and depression. Epilepsy is a severe condition associated with high levels of stigma and discrimination. Furthermore, people suffering from epilepsy can experience limitation in their daily life (e.g., driving licence limitation/loss) as well as they have to cope with the unpredictable nature of epileptic seizures. All these factors can contribute to the poor level of self-esteem, social withdrawal, and demoralization.
People with epilepsy frequently suffer also from depression. This comorbid condition is often underdiagnosed and undertreated, due to several hampering factors including patients’ reluctance to complain about psychiatric symptoms as well as poor attention dedicated from neurologists to detect, recognize and manage mental disorders in comorbidity with epilepsy (Temple et al., 2023).
Depressive symptoms and poor levels of quality of life are reported in almost 30% of patients with epilepsy, with a higher incidence (up to 60%) in those patients suffering from drug-resistant epilepsy (Peltola et al., 2024; Robertson et al., 1987; Lambert and Robertson, 1999). Depression in epilepsy may lead to worse seizure outcome, significant functional and psychosocial disability, a higher rate of self-injurious behavior, and an increased risk of suicidal ideation and attempt (Nickels, 2021).
Although depression represents a common comorbid disorder in people with epilepsy, another reason for not treating it adequately is due to the misconception that it is a direct consequence of the disease itself or it is a medication-side effect.
Several socio-demographic and clinical factors have been identified for explaining the high risk of developing depression in people with epilepsy, including low-education level, unemployment, non-adherence with anti-seizure medications (ASMs), polypharmacological treatment, anxiety, stigma, discrimination and social isolation (Liu et al., 2024).
Furthermore, the presence of comorbid depression increases the risk of a refractory/difficult to treat form of epilepsy (Krishnan, 2020).
It has been found that up to 3 years prior to diagnosis of epilepsy, patients reported high levels of depressive and anxiety symptoms as well as of suicidal ideation (Bølling-Ladegaard et al., 2023). These findings highlight the complex pathophysiological mechanisms shared between depression and epilepsy (Galynker et al., 2024; Hesdorffer et al., 2012; Pompili et al., 2022).
As regards the neurobiological alterations in people with depression, it has been found that people report a significant bilateral reduction in hippocampal volumes, as well as a decreased cortical thickness in the frontal lobe, and decreased glial/neuronal cell density in the cingulate gyrus, rostral and caudal orbitofrontal cortex, and dorsal prefrontal cortex (Mula and Sander, 2019; Mula, 2019). The interesting finding is that also in patients suffering from chronic temporal lobe epilepsy, similar alterations can be highlighted. This should confirm–from a neurobiological viewpoint–the shared ethiopathogenesis of these clinical conditions (Mula and Sander, 2019). Moreover, studies based on animal models have clarified the role of serotonin dysfunction in patients with depression and with epilepsy. In mouse model characterized by a deletion of the 5-HTC2 receptor subunit, a lower seizure threshold for audiogenic seizures have been found, while in animal models for epilepsy and depression a reduced postsynaptic and increased presynaptic density of 5-HT1 receptors have been found (Brennan et al., 1997). Therefore, it should be argued that the alteration in serotonin neurotransmission can be responsible for the occurrence of both conditions (Maia et al., 2017; Guiard and Di Giovanni, 2015). This would also suggest that depression can represent a premorbid symptom in some epileptic syndromes.
Another neurobiological mechanism of depression, namely, the hyperactivation of the hypothalamic-pituitary-adrenal axis, is implicated also in epilepsy. The above-mentioned neurobiological pathways have been proposed for explaining the high comorbidity rates of epilepsy and depression, but no specific hypothesis can be considered conclusive (Mula and Sander, 2019).
The complexity of presentation of depression in patients with epilepsy
The complexity of interrelationship between depression and epilepsy represents a challenge for clinicians in ordinary outpatient and inpatient setting. In a recent study by Shi et al. (2023), the prevalence of depression was 27.30% in patients with epilepsy. Gilliam et al. found that in neurological outpatient unit, screening for depressive symptoms/depressive disorder are performed only in 20% of cases (Gilliam et al., 2006; Gilliam, 2005). In particular, the clinical presentation of depressive symptoms in patients with epilepsy can be subtle and difficult to detect, since in most cases the presentation is atypical.
In fact, the clinical presentation of depression in epilepsy is multifaceted with many interacting neurobiological and psychosocial determinants. In particular, the presentation of depression can be influenced by clinical features of epilepsy, in terms of seizure frequency, type, foci, or lateralization of foci, neurochemical or iatrogenic mechanisms.
Specific type of epilepsy, such as the focal form and the bilateral tonic-clonic seizures have been identified as risk factors for developing a depressive disorder. Another clinical risk factor for depression in people with epilepsy is represented by the age: for each 1 year increment, the risk of developing depression increase by 3.8%. Nevertheless, up to 70% of patients with epilepsy did not receive any treatment for comorbidity (Shi et al., 2023). A significant gender-based difference in depression rates in patients with epilepsy have been found, with female patients 4.27 times more likely to suffer from depression than males. Risk factors for depression among female patients with epilepsy included type of occupational condition, years living with epilepsy, frequency/type of seizures, number of ASM used, and EEG findings. For male patients, the most relevant risk factors include age, ethnic group, and working condition (Guo et al., 2023). Furthermore, in female patients, suffering from epilepsy for less than 10 years, being treated with psychotropic drugs and reporting generalized seizure are additional risk factors for developing depression (Vacca et al., 2022).
Clinical presentation
In patients suffering primarily from epilepsy, the most common clinical presentation of depression includes fatigue, irritability, poor tolerance to frustration, anxiety, mood lability, and anhedonia. A study carried out in Italy found that the alteration of sleeping patterns, tiredness, and loss of energy were the most common symptoms of depression in people with epilepsy (Vacca et al., 2022).
Therefore, the “atypical” presentation of depressive disorders in people with epilepsy has been considered the most common type of depression (Figure 1).
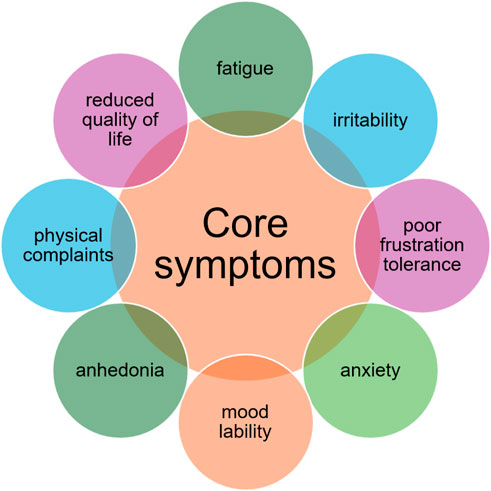
Figure 1. Clinical presentation of depression in patients with epilepsy.
In many specialized centres, the vast majority of cases where an underlying depressive disorder is detected, it is characterized by sadness, anxiety, thoughts of hopelessness/suicide, abulia, and insomnia. In other cases, depression is described as “atypical” due to the lack of training for healthcare professionals in detecting and treating such clinical conditions.
In the seminal works by Kraepelin and Bleuler, the heterogeneous presentation of depressive symptoms in patients with epilepsy was described. In particular, they highlighted that in those patients, depression was mainly characterized by irritability, fear, anxiety, anergia, pain, and insomnia (Kraepelin, 1907; Bleuler, 1949; Mula et al., 2008).
In 1986, Mendez et al. (1986), in a sample of outpatient patients with epilepsy and of matched controls, investigated the prevalence of depression using DSM-III-R criteria. They found that in the majority of patients with epilepsy they were affected from depression, reported prior suicide attempts and were four times more likely to have been hospitalized for depression compared to non-epileptic patients. Patients with epilepsy and depression presented the characteristics of the “endogenous” features of depression, characterized by psychotic traits and dysthymia. Therefore, a specific subtype of epilepsy–due to an alteration in the limbic system–was described. Blumer named such clinical condition as “interictal dysphoric disorder”, Such condition has chronic course, with recurrent symptom-free periods and can be treated with low doses of antidepressant medication. Kanner described another specific subtype of clinical depression reported by patients with epilepsy, called “dysthymic-like disorder of epilepsy”. In these patients, the clinical condition is characterized by anhedonia, hopelessness, fatigue, anxiety, irritability, lack of concentration, frustration, mood lability and alteration in appetite and sleep patterns.
Kanner described also a “subsyndromic” subtype of depression in patients with epilepsy (Kanner, 2006), characterized by patients failing to fulfil the DSM-IV criteria for major depressive disorder, but reporting symptoms of depression of mild-to-moderate severity, anxiety, irritability, physical symptoms and increased energy, with a significantly reduced levels of quality of life.
Classification based on the onset of depression compared to the seizure
Based on the onset of depression compared to the seizure, different types of depression have been identified including: 1) Preictal; 2) Ictal Focal; 3) Postictal; 4) Interictal. Among these subtypes, interictal depression is the most common (Mula et al., 2008; Kanner et al., 2024; Kanner and Palac, 2000).
People with epilepsy can develop depressive symptoms around the epileptic seizure, which are defined as peri-ictal symptoms or as a side effect of the antiseizure treatment (i.e., drugs or surgery). For the appropriate management and treatment of depression in patients with epilepsy, it is essential to identify the different factors contributing to the disorder. In fact, each of these domains can be treated using different and integrated approaches [including psychotherapy, counselling, antidepressant medications, antiseizure medication (Mula, 2019)]. Depression in epilepsy can occur in a number of different clinical contexts and not just as a comorbid disorder. Depression is reported more frequently in patients with temporal lobe epilepsy and left-sided foci, although prevalence data are controversial (Lothe et al., 2008).
Screening for depression in patients with epilepsy
Diagnosing depressive disorders in people with epilepsy can be challenging due to the complex inter-relationship between these two clinical conditions.
Therefore, it is essential in ordinary clinical practice to consider the following risk factors: seizure severity and frequency, recent changes in ASMs, number and symptoms of depressive episodes, and family history of psychiatric illness (particularly depression), which are associated to the heightened risk of developing a depressive episode.
Epilepsy with comorbid depression may present with sub-syndromic depressive episodes and clinicians should be able to perform a differential diagnosis for other psychiatric conditions, including anxiety disorders, psychotic disorders, bipolar disorders as well as should be able to detect any side-effect due to drug interactions or as a consequence of epilepsy surgery.
Therefore, it is essential to use in ordinary clinical practice validated screening tools, in order to promote an adequate and prompt detection of depressive, anxiety, and suicidal behaviours in people with epilepsy (Fiorillo et al., 2018). Screening tools only provide data that must then be carefully considered by trained personnel. Patients positive at the screening must undergo a complete mental state examination by a psychiatrists, in order to formulate an appropriate diagnosis.
Several assessment tools have been developed in order to promptly detect the presence of depressive symptoms, including the 6-item Neurological Disorders Depression Inventory for Epilepsy (NDDI-E); the Emotional Thermometer (ET); and the 21-item Liverpool Adverse Events Profile (LAEP) (Table 1). The routinary adoption of this tool has been recommended by a consensus of the Mood Disorder Initiative-Epilepsy Foundation. In particular, a score of 15 or above at NDDI-E is suggestive of a major depressive episode, but a recent meta-analysis by Kim et al. (2018) found that the optimal cutoff for detecting major depression is >13. The NDDI-E and ET have a high negative predictive value with a low positive predictive value. The low scores indicate a negative assessment and are highly reliable. A score higher than the cut-off scores may potentially indicate a positive assessment of depression but it requires an in-depth clinical assessment for confirmation. The most frequently used and developed tool targeting depression in people with epilepsy is the six-item Neurological Disorders Depression Inventory for Epilepsy (NDDI-E).
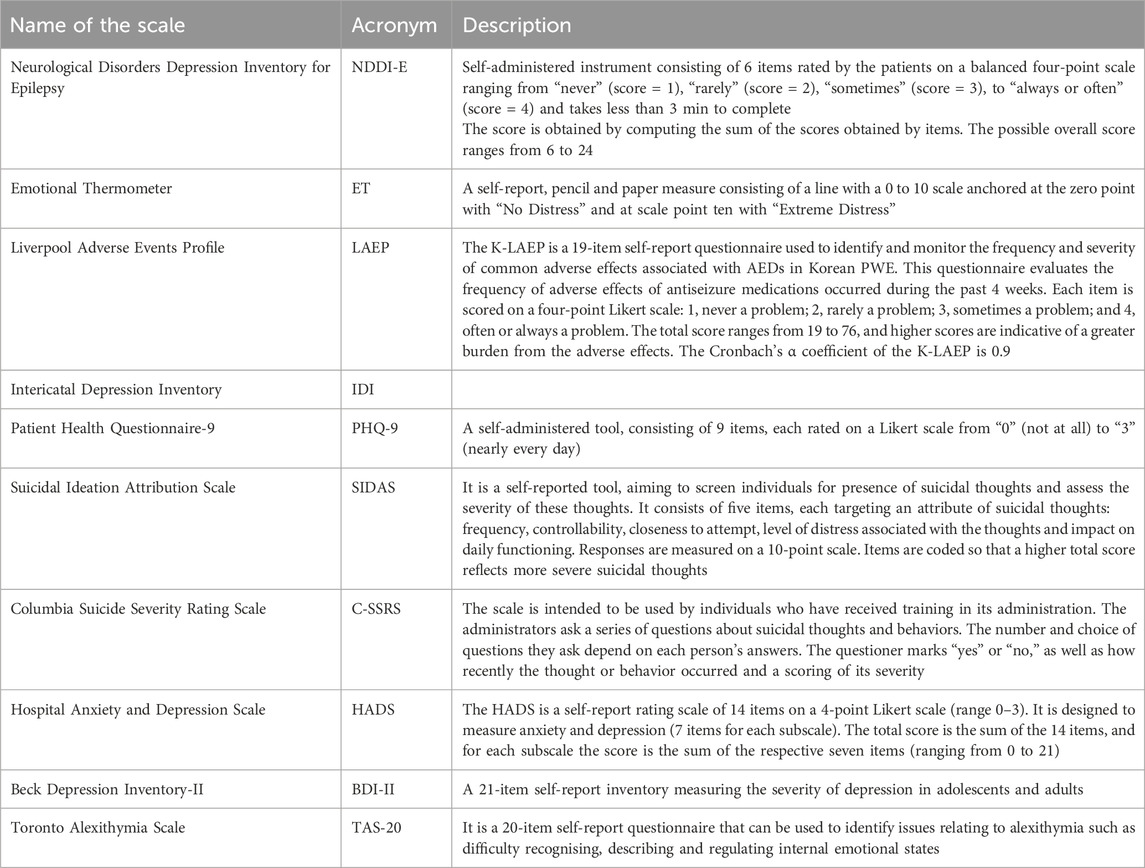
Table 1. Main assessment tools for detecting the presence of depressive symptoms and/or suicidal ideations in patients with depression and epilepsy.
Moreover, clinicians should consider administering to the patients the following screening tools such as the Patient Health Questionnaire-9 (PHQ-9), the Hospital Anxiety and Depression Scale (HADS), the Beck Depression Inventory-II (BDI-II) and the Toronto Alexithymia Scale (TAS-20).
Clinicians should carefully evaluate suicidal ideation and suicidal risk, also considering that the risk of suicide in patients with epilepsy is high, regardless of the presence of depression. Therefore, screening for suicidality should be an integral part of the evaluation of every patients with epilepsy during all follow-up period. Several assessment tools are available such as the Suicidal Ideation Attribution Scale (SIDAS) or the Columbia Suicide Severity Rating Scale (C-SSRS), which require an ad hoc training in order to be administered should be considered. However, it is essential to carefully evaluate the personal and family history in order to detect potential risk factors for suicide/suicidal ideation (Table 1).
Management plan for persons with comorbid depression and epilepsy
The management plan of patients with comorbid depression and epilepsy is complex and requires a strong collaboration among different specialties. In some cases, patients can present a personal history positive for other mental disorders, further highlighting the need for a strong collaboration between neurologists and psychiatrists.
In particular, the management plan of patients with epilepsy and depression should include pharmacological and non-pharmacological interventions (Schumacher et al., 2024; Luciano et al., 2012), based on the clinical characteristics of each individual patient (Leichsenring et al., 2023; Arroll et al., 2023; Hasler, 2023; Sampogna et al., 2024). As regards the selection of ASM, it will depend on the characteristics of the disease and the patient’s profile. A recent consensus document by Villanueva et al. (2023) has suggested to prefer the use of lamotrigine, valproate, carbamazepine, oxcarbazepine or eslicarbazepine acetate. The drug selection should be based on seizure type, age, gender, presence of comorbidities, other medications and childbearing potential (Yang et al., 2024; Brodi et al., 2016; Maguire et al., 2021).
As regards the treatment of depression in patients with epilepsy, clinicians should carefully assess the severity of the depressive symptoms, formulate the diagnosis and assess the presence of suicidal ideation and of suicidal risk (Figure 2).
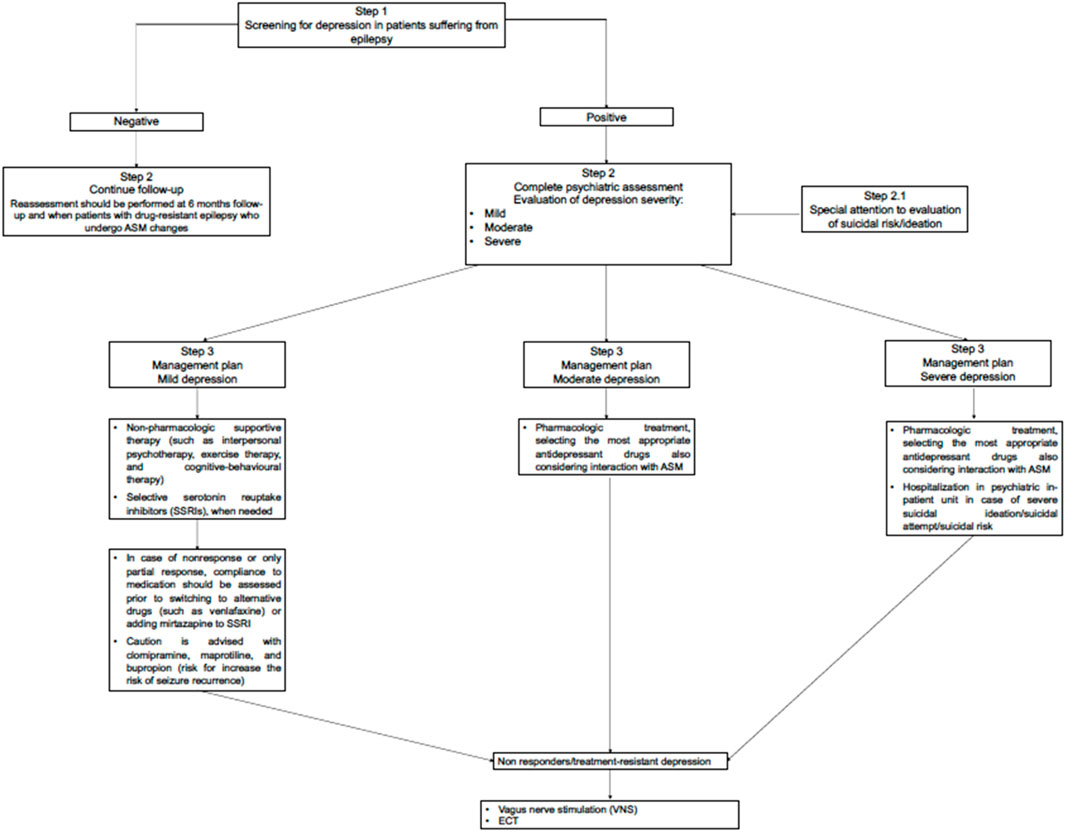
Figure 2. Flowchart for the management of depressive symptoms/comorbid depression in people with epilepsy.
Therefore, for all patients suffering from epilepsy and comorbid depression, it should be advisable to start treatment for depression as soon as possible. A dedicated attention should be paid to patients at high suicidal risk, even considering hospitalization in psychiatric units when the suicide risk is rated as very high. Reassessment for depression and suicidality should be performed at baseline and at 6 months follow-up in patients with drug-resistant epilepsy who undergo ASM changes. In particular, clinicians should consider that up to 6% of patients scored negative at baseline for suicidal ideation, when re-assessed after 6 months report significant levels of suicidal ideation. Furthermore, this risk is increased in people already positive at baseline for the presence of psychiatric comorbidity (Mula et al., 2024).
The treatment for mild depressive episode should include non-pharmacologic supportive therapy (e.g., interpersonal psychotherapy and cognitive-behavioral therapy) as a first-line treatment (Mula et al., 2022) associated with selective serotonin reuptake inhibitors (SSRIs) when needed. The pharmacological regimen including antidepressants should be maintained for at least 12 months, depending on the presence of previous depressive episodes, the type of response to antidepressant treatment. The discontinuation should be considered taking into account the time from when the patient remits at least 50% of acute depressive symptoms, since, SSRIs have a 4–6-week latency period, which can extend the total treatment time. Furthermore, it is necessary to consider whether the patient is suffering from a first episode or if it is a relapse/recurrence). Therefore, pharmacological discontinuation should be considered according to a stepwise model (Mula et al., 2022).
In case of nonresponse or only partial response, compliance to medication should be assessed prior to switching to other type of antidepressants (such as SNRI, e.g., venlafaxine) (Mula et al., 2022) or adding mirtazapine to SSRI. Caution is advised with clomipramine, maprotiline, and bupropion, as these drugs may increase the risk of seizure recurrence.
Clinicians should carefully consider and manage the possible pharmacodynamic and pharmacokinetic interactions among antidepressant drugs and ASM (as reported in Tables 2, 3). In particular, clinicians in selecting the most appropriate antidepressant drug should considered that when using SSRI, fluoxetine and paroxetine act as cytochrome 2D6 inhibitor and therefore can potentiate the toxicity related to ASM. It should be considered that among ASM also carbamazepine acts cytochrome 2D6 inhibitor.
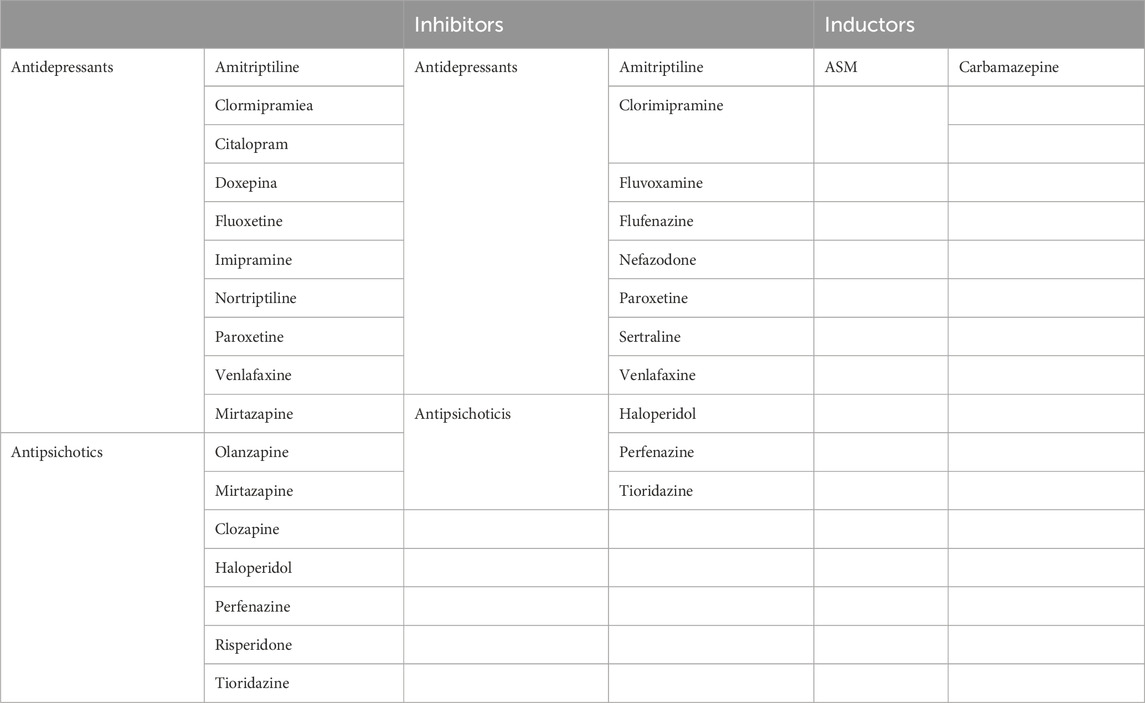
Table 2. Drugs interacting at cythocrome P450 2D6.
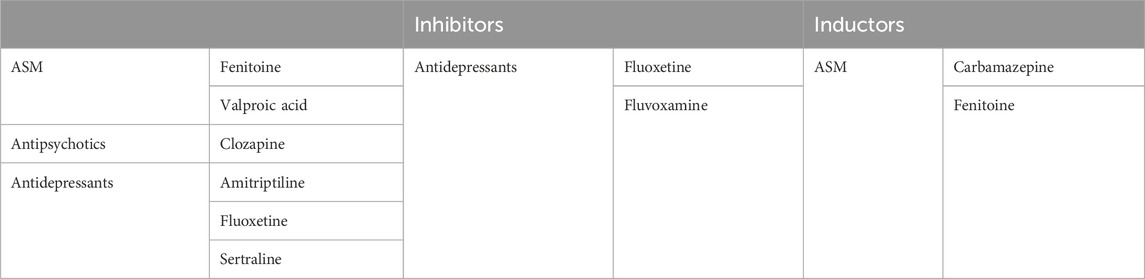
Table 3. Drugs interacting at cythocrome P450 2C9.
Caution should be applied when ASMs, are changed in female patients in preparation for pregnancy. For example, changing carbamazepine or another ASM, that has teratogenic potency to levetiracetam includes the risk of developing subsequent depression (Gammoh et al., 2024).
Clinicians must be vigilant and promptly detect mood swings or the presence of suicidal ideation, no delay treatment with ASMs or with antidepressant drugs is recommended.
The treatment of epilepsy represents a challenge due to the complexity and diversity of the mechanisms associated. Although diagnostic techniques and pharmacological treatment have been improved, there are still more patients that do not obtain a clinical remission. In particular, up to one-third of patients with epilepsy unsuccessfully respond to drug treatment, suffering from drug-resistant epilepsy (Medel-Matus et al., 2022). Patients with drug-resistant epilepsy can obtain a seizure remission period lasting for years, but more than 70% of them experience a relapse in the 12-month post-remission period. In such subgroup of patients, it is extremely relevant to detect the presence of psychiatric comorbidities, since those comorbid conditions can reduce their impact on the development of this condition and improve their response to pharmacological treatment. Moreover, in patients with drug-resistant epilepsy it is particular relevant to detect depressive symptoms, since these are significant predictors of poor quality of life and of suicidal ideation.
Vagus nerve stimulation (VNS) may be an effective palliative therapy in drug-resistant epileptic patients and it is also approved as a therapy for treatment-resistant depression. VNS may ameliorate depressive symptoms and its effect is uncorrelated to seizure response (Assenza et al., 2020). VNS may be considered for treatment-resistant depression, keeping in mind that the optimal parameters for VNS in depression may differ from those used for epilepsy (Nickels, 2021).
The use of electroconvulsive therapy (ECT) in patients with epilepsy is still controversial (Asadi-Pooya, 2017). ECT has been employed as a treatment for refractory epilepsy and status epilepticus in a few anecdotal reports, sometimes successfully. A recent scoping review highlighted that the current existing evidence have some limitations. Clinicians should carefully assess the individual case and evaluate the risk/benefit ratio for using ECT (Ong et al., 2024). If patients present suicidal thoughts or intent, they should be referred to a psychiatrist for an in-depth assessment. In most severe case, it should be considered a psychiatric hospitalization in order to protect patient’s life (Nickels, 2021). When patients with epilepsy and comorbid depression develop psychotic features, a referral to mental health centre is necessary, in order to develop a personalized treatment plan including both antidepressant and antipsychotic medication.
Another complex condition to be managed is represented by Psychogenic Non-Epileptic Seizures (PNES), defined as paroxysmal changes in behavior, consciousness and autonomic function that resembles epileptic seizures, without any electroencephalographic (EEG) alterations of epileptic seizures (Avalos et al., 2020; Berking, 2024). These clinical conditions have been recently redefined as “functional seizures”. This definition has been abandoned since it has always been perceived as stigmatizing by patients, carers and professionals themselves (Vilyte and Pretorius, 2019; Stone et al., 2024; Creed, 2023). Patients suffering from functional seizures can take an average of 7 years between the manifestation of clinical symptoms and definite diagnosis. In some cases, patients with functional seizures present a comorbid depressive disorder, which further complicate its clinical management (Jafari et al., 2020).
There is a limited knowledge regarding the best management strategies for functional seizures and comorbid depression. Several non-pharmacological and pharmacological interventions have been proposed, based on the stage of the disorder. In particular, in the initial phase of treatment (diagnosis delivery phase), effective collaboration and communication between psychiatrists and neurologists is very important, since patients should have received many diagnoses over time. An Italian multidisciplinary Consensus-Based Standard (CBS) systematic review (Gasparini et al., 2019) suggest a multidisciplinary approach to patients with functional seizures. The board recommended to carefully assess individuals with functional seizures for mood disorders, personality disorders, and psychological trauma. Cognitive behavioral therapy should be considered the first-line psychological treatment, with pharmacological interventions used to manage co-occurring conditions such as anxiety and depression.
Discussion
The complexity of comorbidity of epilepsy and depression represents a challenge for neurologists and psychiatrists, in terms of correct detection and management of these clinical conditions. Both epilepsy and depression represent severe chronic disorders, associated with a significant level of personal and social impairment, with often an underestimated prevalence of these conditions, due to stigma and misconceptions attached to these diseases. Therefore, the management of comorbid epilepsy and depression requires a detailed clinical characterization of each individual case in order to develop an integrated and personalized management plan.
Several unmet clinical needs in the management plan of patients with comorbid depression and epilepsy have been highlighted according to psychiatrists and neurologists’ viewpoint.
In particular, according to psychiatrist’s viewpoint patients with comorbid epilepsy and depression represent a challenge for daily clinical care due to the complexity in detection, diagnosis, treatment and long-term management plan (Graham-Rowe et al., 2023; Fiorillo et al., 2013). The main unmet needs reported by psychiatrists include the need to establish and strengthen a network of collaboration with neurologists in order to collaborate actively in the whole process.
In particular, the establishment of a collaborative network should accelerate the pathway to diagnosis and reduce the help-seeking delay, which should be associated with a significant improvement in patients’ quality of life. Moreover, psychiatrists highlight the fact that patients with epilepsy tend to overlook any mood or psychiatric symptoms in general, attributing all these phenomena to the underlying epileptic condition. A significant factor contributing to this should be represented by the lack of mental health literacy in the general population and by the presence of stigmatizing attitudes and behaviours towards mental health issues (Henderson, 2023; Hart et al., 2023). There is the need to promote a cultural change in the general population, as well as in the healthcare section, in order to promptly detect any mental health problem as soon as possible.
Another clinical unmet need is represented by the few data available on treatment of depression in epilepsy. Consensus documents have been released with some recommendation, but the level of evidence is still not satisfying, compared to those available for the management and treatment of patients suffering from depression or from epilepsy, as single disease (Mula, 2019; Kerr et al., 2011; Barry et al., 2008).
Taking a multidisciplinary approach to treating a mood disorder in a patient who has epilepsy might improve epilepsy and depressive disorder’s outcomes. Moreover, it is necessary to promote a shared decision-making process between clinicians and patients in order to improve patients’ outcomes (Clarke et al., 2015; Bär Deucher et al., 2016; Puschner et al., 2010).
According to neurologist’s viewpoint, the timing of the symptoms and occurrence of recent seizure activity can be used to classify depressive symptoms as preictal, ictal, postictal, or interictal. The most important clinical unmet need for neurologists is represented by the promptness of diagnosis of depressive symptoms and/or depressive episodes. Often, neurologists prioritize collecting the epileptological history leading to limited time available for a thorough investigation of potential co-occurring depressive symptoms.” Although there are assessment tools available–such as the Neurologic Disorder Depression Inventory-Epilepsy (NDDIE), which is validated tool for assessing the presence of depression and suicidality in people with epilepsy, the sensitive of the tool is somewhat limited. In particular, the NDDIE is a 6-question rating scale that is self-compiled by the patient, but it can be also scored by the clinician or be administered and scored during the appointment. However, it should be advisable to refer the patient to a specific consultation with a psychiatrist, in order to formulate a full-blown diagnosis. Although the best practice after a positive screening is to collaborate with a psychiatrist for further assessment and treatment, in some cases, this should not be possible due to a fragmentation of healthcare system.
Moreover, another relevant issue is represented by the misconception and the low level of health literacy found in the general population on epilepsy and depression. The level of stigmatization attached to epilepsy and depression is particularly high in specific culture, such as Sub-Saharan Africa, due to superstitious cultural and traditional beliefs for explaining the causes of epilepsy (Singh et al., 2018). These misconceptions can delay the access to care for epilepsy and–in turn–can have a detrimental impact on the detection of depressive symptoms in people with epilepsy.
Collaborative care has been proposed as the best way to deal with comorbidity and where it is possible to establish such a system people with comorbid conditions usually receive care which they need. Unfortunately, in many places collaborative care has not established yet and even in places in which it has been put in practice, it is made difficult because of the separation between institutions providing care for people with mental disorders and for those suffering from other disorders (Sartorious, 2013; Fiorillo and Sartorius, 2021; Momen et al., 2024). Moreover, the “fragmentation” of care and of specialties, which affects almost all professions–including medicine, represents a further obstacle for the appropriate management of patients suffering from comorbid, complex conditions such as depression and epilepsy. Therefore, an integrated model of care should be advocated by healthcare professionals in order to provide the best care to patients with epilepsy and comorbid depression, in order to develop a management plan tailored to their needs, psychiatric history, disease characteristics (Fiorillo and Giordano, 2022; Sartorious, 2013; Zachar, 2023).
The reality of clinical work in outpatient and inpatient psychiatric and neurological units is very different, with a limited access to psychiatric care, and many patients with epilepsy and comorbid depression are treated by neurologist.
However, it should be necessary to promote a correct information at the level of the general population, particularly for patients and their caregivers, about the prevalence of depressive symptoms in people with epilepsy as well as to improve educational activities for healthcare professionals, in order to disseminate screening procedure for depressive disorders and to further strengthen an integrated care management between psychiatrists and neurologists. Complex and challenging clinical conditions, such as epilepsy with comorbid depressive disorder, necessitate a biopsychosocial perspective and a collaborative, multidisciplinary strategy to ensure optimal patient management and care (Özge et al., 2023).
Moreover, depressive symptoms in people with epilepsy are often present by the time of the first recognized epileptic seizure, further highlighting the need for psychiatric screening as soon as possible, especially at the initial stages of the care process of patients with epilepsy. An in-depth psychiatric assessment should be considered also because patients may present other psychiatric comorbidities, such as anxiety disorders, attention deficit and psychotic disorders and less frequently, personality disorders.
The need for a closer collaboration between psychiatrists and neurologists Is confirmed also by the management plan to be issued for each patient. In particular, the selection of a specific antiseizure medication should consider not only its safety and tolerability, but also the risk of increasing suicidal risk or improving quality of life. Therefore, it is essential to specifically assess these dimensions before starting the management plan, and only a collaboration between psychiatrists and neurologists can work toward such global aim.
Author contributions
GS: Writing – original draft, Writing – review and editing. RB: Conceptualization, Writing – review and editing. GD: Conceptualization, Writing – review and editing. ME: Supervision, Writing – review and editing. EF: Conceptualization, Writing – review and editing. GS: Supervision, Writing – review and editing. GV: Supervision, Writing – review and editing. UV: Supervision, Writing – review and editing. FV: Supervision, Writing – review and editing. GS: Conceptualization, Supervision, Validation, Writing – original draft, Writing – review and editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This publication was supported by an unrestricted grant from Angelini Pharma S.p.A. The funder was not involved in the study design, collection, analysis, interpretation of data, the writing of this article, or the decision to submit it for publication.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Abe, C., Denney, D., Doyle, A., Cullum, M., Adams, J., Perven, G., et al. (2020). Comparison of psychiatric comorbidities and impact on quality of life in patients with epilepsy or psychogenic nonepileptic spells. Epilepsy Behav. 102, 106649. doi:10.1016/j.yebeh.2019.106649
Arroll, B., Roskvist, R., Moir, F., Harwood, M., Eggleton, K., Dowrick, C., et al. (2023). Antidepressants in primary care: limited value at the first visit. World Psychiatry 22 (2), 340. doi:10.1002/wps.21057
Asadi-Pooya, A. A. (2017). Electroconvulsive therapy and epilepsy. Epilepsia 58 (1), 176–177. doi:10.1111/epi.13642
Assenza, G., Tombini, M., Lanzone, J., Ricci, L., Di Lazzaro, V., Casciato, S., et al. (2020). Antidepressant effect of vagal nerve stimulation in epilepsy patients: a systematic review. Neurol. Sci. 41 (11), 3075–3084. doi:10.1007/s10072-020-04479-2
Avalos, J. C., Silva, B. A., Tevés Echazu, M. F., Rosso, B., Besocke, A. G., and Del Carmen Garcia, M. (2020). Quality of life in patients with epilepsy or psychogenic nonepileptic seizures and the contribution of psychiatric comorbidities. Epilepsy Behav. 112, 107447. doi:10.1016/j.yebeh.2020.107447
Bär Deucher, A., Hengartner, M. P., Kawohl, W., Konrad, J., Puschner, B., Clarke, E., et al. (2016). Participation in medical decision-making across Europe: an international longitudinal multicenter study. Eur. Psychiatry 35, 39–46. doi:10.1016/j.eurpsy.2016.02.001
Barry, J. J., Ettinger, A. B., Friel, P., Gilliam, F. G., Harden, C. L., Hermann, B., et al. (2008). Consensus statement: the evaluation and treatment of people with epilepsy and affective disorders. Epilepsy Behav. 13 (Suppl. 1), S1–S29. doi:10.1016/j.yebeh.2008.04.005
Bear, D. M. (1979). Temporal lobe epilepsy–- a syndrome of sensory-limbic hyperconnection. Cortex 15 (3), 357–384. doi:10.1016/s0010-9452(79)80064-7
Beghi, E. (2020). The epidemiology of epilepsy. Neuroepidemiology 54 (2), 185–191. doi:10.1159/000503831
Berk, M., Köhler-Forsberg, O., Turner, M., Penninx, B. W. J. H., Wrobel, A., Firth, J., et al. (2023). Comorbidity between major depressive disorder and physical diseases: a comprehensive review of epidemiology, mechanisms and management. World Psychiatry 22 (3), 366–387. doi:10.1002/wps.21110
Berking, M. (2024). Emotion regulation and mental health: current evidence and beyond. World Psychiatry 23 (3), 438–439. doi:10.1002/wps.21244
Bølling-Ladegaard, E., Dreier, J. W., Kessing, L. V., Budtz-Jørgensen, E., Lolk, K., and Christensen, J. (2023). Directionality of the association between epilepsy and depression: a nationwide register-based cohort study. Neurology 100 (9), e932–e942. doi:10.1212/WNL.0000000000201542
Brennan, T. J., Seeley, W. W., Kilgard, M., Schreiner, C. E., and Tecott, L. H. (1997). Sound-induced seizures in serotonin 5-HT2c receptor mutant mice. Nat. Genet. 16, 387–390. doi:10.1038/ng0897-387
Brodie, M. J., Besag, F., Ettinger, A. B., Mula, M., Gobbi, G., Comai, S., et al. (2016). Epilepsy, antiepileptic drugs, and aggression: an evidence-based review. Pharmacol. Rev. 68 (3), 563–602. doi:10.1124/pr.115.012021
Clarke, E., Puschner, B., Jordan, H., Williams, P., Konrad, J., Kawohl, W., et al. (2015). Empowerment and satisfaction in a multinational study of routine clinical practice. Acta Psychiatr. Scand. 131 (5), 369–378. doi:10.1111/acps.12365
Creed, F. (2023). Progress in understanding functional somatic symptoms and syndromes in light of the ICD-11 and DSM-5. World Psychiatry 22 (3), 474–475. doi:10.1002/wps.21118
Cronin, W., Kwan, P., and Foster, E. (2023). Anxiety and depressive symptoms in adults with new-onset seizures: a scoping review. Epilepsia Open 8 (3), 758–772. doi:10.1002/epi4.12766
Datta, A. N. (2023). The impact of anti-seizure medications on psychiatric disorders among children with epilepsy: both a challenge and an opportunity? J. Can. Acad. Child. Adolesc. Psychiatry 32 (3), 177–184.
Di Vincenzo, M., Sampogna, G., Della Rocca, B., Brandi, C., Mancuso, E., Landolfi, L., et al. (2022). What influences psychological functioning in patients with mood disorders? The role of clinical, sociodemographic, and temperamental characteristics in a naturalistic study. Ann. Gen. Psychiatry 21 (1), 51. doi:10.1186/s12991-022-00428-9
Evans-Lacko, S., Aguilar-Gaxiola, S., Al-Hamzawi, A., Alonso, J., Benjet, C., Bruffaerts, R., et al. (2018). Socio-economic variations in the mental health treatment gap for people with anxiety, mood, and substance use disorders: results from the WHO World Mental Health (WMH) surveys. Psychol. Med. 48 (9), 1560–1571. doi:10.1017/S0033291717003336
Faber, D. P. (1997). Jean-Martin Charcot and the epilepsy/hysteria relationship. J. Hist. Neurosci. 6 (3), 275–290. doi:10.1080/09647049709525714
Fatori, D., Zuccolo, P. F., and Polanczyk, G. V. (2020). A global challenge: maternal depression and offspring mental disorders. Eur. Child. Adolesc. Psychiatry 29 (5), 569–571. doi:10.1007/s00787-020-01556-x
Fiorillo, A., Carpiniello, B., De Giorgi, S., La Pia, S., Maina, G., Sampogna, G., et al. (2018). Assessment and management of cognitive and psychosocial dysfunctions in patients with major depressive disorder: a clinical review. Front. Psychiatry 9, 493. doi:10.3389/fpsyt.2018.00493
Fiorillo, A., and Giordano, A. (2022). The biopsychosocial model of schizophrenia and cancer: unraveling the etiopathogenesis of complex diseases. Eur. Psychiatry 65 (1), e86. doi:10.1192/j.eurpsy.2022.2349
Fiorillo, A., Malik, A., Luciano, M., Del Vecchio, V., Sampogna, G., Del Gaudio, L., et al. (2013). Challenges for trainees in psychiatry and early career psychiatrists. Int. Rev. Psychiatry 25 (4), 431–437. doi:10.3109/09540261.2013.812960
Fiorillo, A., and Sartorius, N. (2021). Mortality gap and physical comorbidity of people with severe mental disorders: the public health scandal. Ann. Gen. Psychiatry 20 (1), 52. doi:10.1186/s12991-021-00374-y
Fischer, F., Zocholl, D., Rauch, G., Levis, B., Benedetti, A., Thombs, B., et al. (2023). Prevalence estimates of major depressive disorder in 27 European countries from the European Health Interview Survey: accounting for imperfect diagnostic accuracy of the PHQ-8. BMJ Ment. Health 26 (1), e300675. doi:10.1136/bmjment-2023-300675
Freud, A. (1954). The widening scope of indications for psychoanalysis: discussion. J. Am. Psychoanal. Assoc. 2, 607–620. doi:10.1177/000306515400200404
Fusar-Poli, P., Estradé, A., Stanghellini, G., Esposito, C. M., Rosfort, R., Mancini, M., et al. (2023). The lived experience of depression: a bottom-up review co-written by experts by experience and academics. World Psychiatry 22 (3), 352–365. doi:10.1002/wps.21111
Galynker, I., Bloch-Elkouby, S., and Cohen, L. J. (2024). Suicide crisis syndrome: a specific diagnosis to aid suicide prevention. World Psychiatry 23 (3), 362–363. doi:10.1002/wps.21229
Gammoh, O., Al-Smadi, A., Mansour, M., Ennab, W., Al Hababbeh, S., Al-Taani, G., et al. (2024). The relationship between psychiatric symptoms and the use of levetiracetam in people with epilepsy. Int. J. Psychiatry Med. 59 (3), 360–372. doi:10.1177/00912174231206056
Gasparini, S., Beghi, E., Ferlazzo, E., Beghi, M., Belcastro, V., Biermann, K. P., et al. (2019). Management of psychogenic non-epileptic seizures: a multidisciplinary approach. Eur. J. Neurol. 26 (2), 205–e15. doi:10.1111/ene.13818
GBD 2021 Nervous System Disorders Collaborators (2024). Global, regional, and national burden of disorders affecting the nervous system, 1990-2021: a systematic analysis for the Global Burden of Disease Study 2021. Lancet Neurol. 23 (4), 344–381. doi:10.1016/S1474-4422(24)00038-3
Gilliam, F. G. (2005). Diagnosis and treatment of mood disorders in persons with epilepsy. Curr. Opin. Neurol. 18 (2), 129–133. doi:10.1097/01.wco.0000162853.29650.ec
Gilliam, F. G., Barry, J. J., Hermann, B. P., Meador, K. J., Vahle, V., and Kanner, A. M. (2006). Rapid detection of major depression in epilepsy: a multicentre study. Lancet Neurol. 5 (5), 399–405. doi:10.1016/S1474-4422(06)70415-X
Graham-Rowe, E., Katzer, C. B., Riaz, S., Attwood, A., Bates, L., Sainz-Fuertes, R., et al. (2023). Unmet needs of people with epilepsy: a qualitative study exploring their journey from presentation to long-term management across five European countries. Front. Neurol. 14, 1130817. doi:10.3389/fneur.2023.1130817
Guiard, B. P., and Di Giovanni, G. (2015). Central serotonin-2A (5-HT2A) receptor dysfunction in depression and epilepsy: the missing link? Front. Pharmacol. 6, 46. doi:10.3389/fphar.2015.00046
Guo, W., Li, Y. X., Zhang, Y., Lv, X. R., Wang, S. X., Zhang, S. Y., et al. (2023). Risk analysis of depression among adult patients with epilepsy of different sex: a retrospective single-center study from China. Front. Psychiatry 14, 1283983. doi:10.3389/fpsyt.2023.1283983
Hart, L. M., Jorm, A. F., Johnson, C. L., Tully, L. A., Austen, E., Gregg, K., et al. (2023). Mental health literacy for supporting children: the need for a new field of research and intervention. World Psychiatry 22 (2), 338–339. doi:10.1002/wps.21099
Hasler, B. P. (2023). Chronotype and mental health: timing seems to matter, but how, why, and for whom? World Psychiatry 22 (2), 329–330. doi:10.1002/wps.21092
Henderson, C. (2023). Challenges in improving mental health literacy at population level. World Psychiatry 22 (3), 392–393. doi:10.1002/wps.21115
Hesdorffer, D. C., Ishihara, L., Mynepalli, L., Webb, D. J., Weil, J., and Hauser, W. A. (2012). Epilepsy, suicidality, and psychiatric disorders: a bidirectional association. Ann. Neurol. 72 (2), 184–191. doi:10.1002/ana.23601
Holt-Lunstad, J. (2024). Social connection as a critical factor for mental and physical health: evidence, trends, challenges, and future implications. World Psychiatry 23 (3), 312–332. doi:10.1002/wps.21224
Jafari, A., Rezaei Tavirani, M., Parvareshi Hamrah, M., Ahmadi, K. S., and Bashi Zadeh Fakhar, H. (2020). Psychogenic non-epileptic seizures; a narrative review. Arch. Acad. Emerg. Med. 8 (1), e10.
Jain, S., Panda, S., and Garg, M. (2023). Sociodemographic determinants of epilepsy and treatment-seeking behavior among patients with epilepsy–- A hospital-based study from western India. Epilepsy Behav. 145, 109340. doi:10.1016/j.yebeh.2023.109340
Kaculini, C. M., Tate-Looney, A. J., and Seifi, A. (2021). The history of epilepsy: from ancient mystery to modern misconception. Cureus 13 (3), e13953. doi:10.7759/cureus.13953
Kanner, A. M. (2006). Depression and epilepsy: a new perspective on two closely related disorders. Epilepsy Curr. 6 (5), 141–146. doi:10.1111/j.1535-7511.2006.00125.x
Kanner, A. M. (2014). Is depression associated with an increased risk of treatment-resistant epilepsy? Research strategies to investigate this question. Epilepsy Behav. 38, 3–7. doi:10.1016/j.yebeh.2014.06.027
Kanner, A. M., and Palac, S. (2000). Depression in epilepsy: a common but often unrecognized comorbid malady. Epilepsy Behav. 1, 37–51. doi:10.1006/ebeh.2000.0030
Kanner, A. M., Shankar, R., Margraf, N. G., Schmitz, B., Ben-Menachem, E., and Sander, J. W. (2024). Mood disorders in adults with epilepsy: a review of unrecognized facts and common misconceptions. Ann. Gen. Psychiatry 23 (1), 11. doi:10.1186/s12991-024-00493-2
Kerr, M. P., Mensah, S., Besag, F., de Toffol, B., Ettinger, A., Kanemoto, K., et al. (2011). International consensus clinical practice statements for the treatment of neuropsychiatric conditions associated with epilepsy. Epilepsia 52, 2133–2138. doi:10.1111/j.1528-1167.2011.03276.x
Kraepelin. (1907). Die klinische Stellung der Melancholie (cit. n. 41), 331. See also Kraepelin’s introduction to Georges L. Dreyfus, Die Melancholie: Ein Zustandsbild des manisch-depressiven Irreseins (Jena, 1907), v–vi. For a contemporary critique of Kraepelin’s expansion of manic-depressive forms at the expense of melancholy. see Alfred Hoche.
Krishnan, V. (2020). Depression and anxiety in the epilepsies: from bench to bedside. Curr. Neurol. Neurosci. Rep. 20 (9), 41. doi:10.1007/s11910-020-01065-z
Lambert, M. V., and Robertson, M. M. (1999). Depression in epilepsy: etiology, phenomenology, and treatment. Epilepsia 40 (Suppl. 10), S21–S47. doi:10.1111/j.1528-1157.1999.tb00884.x
La Verde, M., Luciano, M., Fordellone, M., Sampogna, G., Lettieri, D., Palma, M., et al. (2024). Postpartum depression and inflammatory biomarkers of neutrophil-lymphocyte ratio, platelet-lymphocyte ratio, and monocyte-lymphocyte ratio: a prospective observational study. Gynecol. Obstet. Invest 89 (2), 140–149. doi:10.1159/000536559
Lee, S. A., Jeon, J. Y., No, S. K., Park, H., Kim, O. J., Kwon, J. H., et al. (2018). Factors contributing to anxiety and depressive symptoms in adults with new-onset epilepsy. Epilepsy Behav. 88, 325–331. doi:10.1016/j.yebeh.2018.10.005
Leichsenring, F., Steinert, C., Rost, F., Abbass, A., Heim, N., and Ioannidis, J. P. A. (2023). A critical assessment of NICE guidelines for treatment of depression. World Psychiatry 22 (1), 43–45. doi:10.1002/wps.21039
Levira, F., Thurman, D. J., Sander, J. W., Hauser, W. A., Hesdorffer, D. C., Masanja, H., et al. (2017). Premature mortality of epilepsy in low- and middle-income countries: a systematic review from the Mortality Task Force of the International League against Epilepsy. Epilepsia 58 (1), 6–16. doi:10.1111/epi.13603
Liu, G. Y., Fu, F. J., Chou, Y. X., Ye, M. S., Ouyang, Y. L., Yan, M. D., et al. (2024). Frontiers and hotspots in comorbid epilepsy and depression: a bibliometric analysis from 2003 to 2023. Front. Neurol. 15, 1413582. doi:10.3389/fneur.2024.1413582
Lothe, A., Didelot, A., Hammers, A., Costes, N., Saoud, M., Gilliam, F., et al. (2008). Comorbidity between temporal lobe epilepsy and depression: a [18F]MPPF PET study. Brain 131 (Pt 10), 2765–2782. doi:10.1093/brain/awn194
Luciano, M., Del Vecchio, V., Giacco, D., De Rosa, C., Malangone, C., and Fiorillo, A. (2012). A 'family affair'? The impact of family psychoeducational interventions on depression. Expert Rev. Neurother. 12 (1), 83–92. doi:10.1586/ern.11.131
Madigan, S., Deneault, A. A., Racine, N., Park, J., Thiemann, R., Zhu, J., et al. (2023). Adverse childhood experiences: a meta-analysis of prevalence and moderators among half a million adults in 206 studies. World Psychiatry 22 (3), 463–471. doi:10.1002/wps.21122
Magiorkinis, E., Sidiropoulou, K., and Diamantis, A. (2010). Hallmarks in the history of epilepsy: epilepsy in antiquity. Epilepsy Behav. 17, 103–108. doi:10.1016/j.yebeh.2009.10.023
Maguire, M. J., Marson, A. G., and Nevitt, S. J. (2021). Antidepressants for people with epilepsy and depression. Cochrane Database Syst. Rev. 4 (4), CD010682. doi:10.1002/14651858.CD010682.pub3
Maia, G. H., Brazete, C. S., Soares, J. I., Luz, L. L., and Lukoyanov, N. V. (2017). Serotonin depletion increases seizure susceptibility and worsens neuropathological outcomes in kainate model of epilepsy. Brain Res. Bull. 134, 109–120. doi:10.1016/j.brainresbull.2017.07.009
Maj, M. (2023). Understanding depression beyond the mind-body dichotomy. World Psychiatry 22 (3), 349–350. doi:10.1002/wps.21142
Maj, M., Stein, D. J., Parker, G., Zimmerman, M., Fava, G. A., De Hert, M., et al. (2020). The clinical characterization of the adult patient with depression aimed at personalization of management. World Psychiatry 19 (3), 269–293. doi:10.1002/wps.20771
Manole, A. M., Sirbu, C. A., Mititelu, M. R., Vasiliu, O., Lorusso, L., Sirbu, O. M., et al. (2023). State of the art and challenges in epilepsy-a narrative review. J. Personalized Med. 13 (4), 623. doi:10.3390/jpm13040623
Medel-Matus, J. S., Orozco-Suárez, S., and Escalante, R. G. (2022). Factors not considered in the study of drug-resistant epilepsy: psychiatric comorbidities, age, and gender. Epilepsia Open 7 (Suppl. 1), S81–S93. doi:10.1002/epi4.12576
Mendez, M. F., Cummings, J. L., and Benson, D. F. (1986). Depression in epilepsy. Significance and phenomenology. Arch. Neurol. 43 (8), 766–770. doi:10.1001/archneur.1986.00520080014012
Momen, N. C., Østergaard, S. D., Heide-Jorgensen, U., Sørensen, H. T., McGrath, J. J., and Plana-Ripoll, O. (2024). Associations between physical diseases and subsequent mental disorders: a longitudinal study in a population-based cohort. World Psychiatry 23 (3), 421–431. doi:10.1002/wps.21242
Mula, M. (2019). Epilepsy and depression: an update. Arch. Med. Health Sci. 7, 104–111. doi:10.4103/amhs.amhs_54_19
Mula, M., Borghs, S., Ferro, B., Zaccara, G., Dainese, F., Ferlazzo, E., et al. (2024). Effect of drug treatment changes and seizure outcomes on depression and suicidality in adults with drug-resistant focal epilepsy. Epilepsia 65 (2), 473–482. doi:10.1111/epi.17856
Mula, M., Brodie, M. J., de Toffol, B., Guekht, A., Hecimovic, H., Kanemoto, K., et al. (2022). ILAE clinical practice recommendations for the medical treatment of depression in adults with epilepsy. Epilepsia 63 (2), 316–334. doi:10.1111/epi.17140
Mula, M., Jauch, R., Cavanna, A., Collimedaglia, L., Barbagli, D., Gaus, V., et al. (2008). Clinical and psychopathological definition of the interictal dysphoric disorder of epilepsy. Epilepsia 49 (4), 650–656. doi:10.1111/j.1528-1167.2007.01434.x
Mula, M., and Sander, J. W. (2019). Current and emerging drug therapies for the treatment of depression in adults with epilepsy. Expert Opin. Pharmacother. 20 (1), 41–45. doi:10.1080/14656566.2018.1543402
Nickels, K. (2021). Adolescence and epilepsy: the perfect storm for suicidal behavior. Epilepsy Curr. 21 (2), 85–86. doi:10.1177/1535759720987549
Ong, M. J. Y., Lee, V. L. L., Teo, S. L., Tan, H. J., Trinka, E., and Khoo, C. S. (2024). Electroconvulsive therapy in refractory and super-refractory status epilepticus in adults: a scoping review. Neurocrit Care 41, 681–690. doi:10.1007/s12028-024-02003-4
Østergaard, S. D., Seidler, Z., and Rice, S. (2023). The ICD-11 opens the door for overdue improved identification of depression in men. World Psychiatry 22 (3), 480–481. doi:10.1002/wps.21124
Özge, A., Domaç, F. M., Tekin, N., Sünbül, E. A., Öksüz, N., Atalar, A. Ç., et al. (2023). One patient, three providers: a multidisciplinary approach to managing common neuropsychiatric cases. J. Clin. Med. 12 (17), 5754. doi:10.3390/jcm12175754
Peltola, J., Surges, R., Voges, B., and von Oertzen, T. J. (2024). Expert opinion on diagnosis and management of epilepsy-associated comorbidities. Epilepsia Open 9 (1), 15–32. doi:10.1002/epi4.12851
Pompili, M., Innamorati, M., Erbuto, D., Luciano, M., Sampogna, G., Abbate-Daga, G., et al. (2022). High depression symptomatology and mental pain characterize suicidal psychiatric patients. Eur. Psychiatry 65 (1), e54. doi:10.1192/j.eurpsy.2022.2312
Puschner, B., Steffen, S., Slade, M., Kaliniecka, H., Maj, M., Fiorillo, A., et al. (2010). Clinical decision making and outcome in routine care for people with severe mental illness (CEDAR): study protocol. BMC Psychiatry 10, 90. doi:10.1186/1471-244X-10-90
Qin, S. K., Yang, Z. X., Guan, Z. W., Zhang, J. H., Ping, X., Lu, Y., et al. (2022). Exploring the association between epilepsy and depression: a systematic review and meta-analysis. pLoS One 17 (12), e0278907. doi:10.1371/journal.pone.0278907
Reed, G. M. (2024). What's in a name? Mental disorders, mental health conditions and psychosocial disability. World Psychiatry 23 (2), 209–210. doi:10.1002/wps.21190
Robertson, M. M., Trimble, M. R., and Townsend, H. R. (1987). Phenomenology of depression in epilepsy. Epilepsia 28 (4), 364–372. doi:10.1111/j.1528-1157.1987.tb03659.x
Saha, R., Mohapatra, S., Kar, S. K., Tekkalaki, B., and Anand, K. S. (2017). Causative factors and phenomenology of depression in EPILEPSY—a review. Int. J. Epilepsy 4 (1).
Sakurai, H., and Kanemoto, K. (2022). Quality of life for patients with psychogenic nonepilepsy seizures in comparison with age- and gender-matched patients with epilepsy–- Cross-sectional study. Epilepsy Behav. 128, 108539. doi:10.1016/j.yebeh.2021.108539
Salk, R. H., Hyde, J. S., and Abramson, L. Y. (2017). Gender differences in depression in representative national samples: meta-analyses of diagnoses and symptoms. Psychol. Bull. 143 (8), 783–822. doi:10.1037/bul0000102
Sampogna, G., Toni, C., Catapano, P., Rocca, B. D., Di Vincenzo, M., Luciano, M., et al. (2024). New trends in personalized treatment of depression. Curr. Opin. Psychiatry 37 (1), 3–8. doi:10.1097/YCO.0000000000000903
Sartorious, N. (2013). Comorbidity of mental and physical diseases: a main challenge for medicine of the 21st century. Shanghai Arch. Psychiatry 25 (2), 68–69. doi:10.3969/j.issn.1002-0829.2013.02.002
Schumacher, L., Klein, J. P., Hautzinger, M., Härter, M., Schramm, E., and Kriston, L. (2024). Predicting the outcome of psychotherapy for chronic depression by person-specific symptom networks. World Psychiatry 23 (3), 411–420. doi:10.1002/wps.21241
Shi, W., Sun, H., Peng, W., Chen, Z., Wang, Q., Lin, W., et al. (2023). Prevalence and risk factors of anxiety and depression in adult patients with epilepsy: a multicenter survey-based study. Ther. Adv. Neurol. Disord. 16, 17562864231187194. doi:10.1177/17562864231187194
Sidhu, G. S., Sidhu, T. K., Kaur, P., Lal, D., and Sangha, N. K. (2019). Evaluation of peripartum depression in females. Int. J. Appl. Basic Med. Res. 9 (4), 201–205. doi:10.4103/ijabmr.IJABMR_23_19
Singh, S., Mishra, V. N., Rai, A., Singh, R., and Chaurasia, R. N. (2018). Myths and superstition about epilepsy: a study from North India. J. Neurosci. Rural. Pract. 9 (3), 359–362. doi:10.4103/jnrp.jnrp_63_18
Stone, J., Hoeritzauer, I., McWhirter, L., and Carson, A. (2024). Functional neurological disorder: defying dualism. World Psychiatry 23 (1), 53–54. doi:10.1002/wps.21151
Temple, J., Fisher, P., Davies, C., Millar, C., and Gemma Cherry, M. (2023). Psychosocial factors associated with anxiety and depression in adolescents with epilepsy: a systematic review. Epilepsy Behav. 149, 109522. doi:10.1016/j.yebeh.2023.109522
Tsigebrhan, R., Derese, A., Kariuki, S. M., Fekadu, A., Medhin, G., Newton, C. R., et al. (2023). Co-morbid mental health conditions in people with epilepsy and association with quality of life in low- and middle-income countries: a systematic review and meta-analysis. Health Qual. Life Outcomes 21 (1), 5. doi:10.1186/s12955-022-02086-7
Vacca, M., Fernandes, M., Spanetta, M., Placidi, F., Izzi, F., Lombardo, C., et al. (2022). Depressive symptoms in patients with epilepsy and clinically associated features in a single tertiary center. Neurol. Sci. 43 (3), 1965–1974. doi:10.1007/s10072-021-05589-1
Villanueva, V., Artal, J., Cabeza-Alvarez, C. I., Campos, D., Castillo, A., Flórez, G., et al. (2023). Proposed recommendations for the management of depression in adults with epilepsy: an expert consensus. Neurol. Ther. 12 (2), 479–503. doi:10.1007/s40120-023-00437-0
Vilyte, G., and Pretorius, C. (2019). Personality traits, illness behaviors, and psychiatric comorbidity in individuals with psychogenic nonepileptic seizures (PNES), epilepsy, and other nonepileptic seizures (oNES): differentiating between the conditions. Epilepsy Behav. 98 (Pt A), 210–219. doi:10.1016/j.yebeh.2019.05.043
Volpe, U., Fiorillo, A., Luciano, M., Del Vecchio, V., Palumbo, C., Calò, S., et al. (2014). Pathways to mental health care in Italy: results from a multicenter study. Int. J. Soc. Psychiatry 60 (5), 508–513. doi:10.1177/0020764013501648
Yang, W., Jia, Y. H., Jiang, H. Y., and Li, A. J. (2024). Antidepressant use and the risk of seizure: a meta-analysis of observational studies. Eur. J. Clin. Pharmacol. 80 (2), 175–183. doi:10.1007/s00228-023-03597-y
Keywords: depression, epilepsy, comorbidity, burden, differential diagnosis
Citation: Sampogna G, Brugnoli R, Didato G, Elia M, Ferlazzo E, Serafini G, Vatti G, Volpe U, Villani F and Sani G (2025) Clinical characterization and management of persons with comorbid epilepsy and depression: an expert opinion paper. Front. Pharmacol. 16:1592650. doi: 10.3389/fphar.2025.1592650
Received: 14 March 2025; Accepted: 06 June 2025;
Published: 01 July 2025.
Edited by:
Zongchao Han, University of North Carolina at Chapel Hill, United StatesReviewed by:
Silvia Kochen, National Scientific and Technical Research Council (CONICET), ArgentinaCopyright © 2025 Sampogna, Brugnoli, Didato, Elia, Ferlazzo, Serafini, Vatti, Volpe, Villani and Sani. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Gaia Sampogna, Z2FpYS5zYW1wb2duYUBnbWFpbC5jb20=