 Florian Hotzy1*
Florian Hotzy1* Anastasia Theodoridou1
Anastasia Theodoridou1 Paul Hoff1
Paul Hoff1 Andres R. Schneeberger2,3,4
Andres R. Schneeberger2,3,4 Erich Seifritz1
Erich Seifritz1 Sebastian Olbrich1
Sebastian Olbrich1 Matthias Jäger1
Matthias Jäger1- 1Department for Psychiatry, Psychotherapy and Psychosomatics, University Hospital of Psychiatry Zurich, Zurich, Switzerland
- 2Psychiatrische Dienste Graubuenden, Chur, Switzerland
- 3Universitaere Psychiatrische Kliniken Basel, Universitaet Basel, Basel, Switzerland
- 4Department of Psychiatry and Behavioral Sciences, Albert Einstein College of Medicine, New York, NY, United States
Introduction: Although knowledge about negative effects of coercive measures in psychiatry exists, its prevalence is still high in clinical routine. This study aimed at define risk factors and test machine learning algorithms for their accuracy in the prediction of the risk to being subjected to coercive measures.
Methods: In a sample of involuntarily hospitalized patients (n = 393) at the University Hospital of Psychiatry Zurich, we analyzed risk factors for the experience of coercion (n = 170 patients) using chi-square tests and Mann Whitney U tests. We trained machine learning algorithms [logistic regression, Supported Vector Machine (SVM), and decision trees] with these risk factors and tested obtained models for their accuracy via five-fold cross validation. To verify the results we compared them to binary logistic regression.
Results: In a model with 8 risk-factors which were available at admission, the SVM algorithm identified 102 out of 170 patients, which had experienced coercion and 174 out of 223 patients without coercion (69% accuracy with 60% sensitivity and 78% specificity, AUC 0.74). In a model with 18 risk-factors, available after discharge, the logistic regression algorithm identified 121 out of 170 with and 176 out of 223 without coercion (75% accuracy, 71% sensitivity, and 79% specificity, AUC 0.82).
Discussion: Incorporating both clinical and demographic variables can help to estimate the risk of experiencing coercion for psychiatric patients. This study could show that trained machine learning algorithms are comparable to binary logistic regression and can reach a good or even excellent area under the curve (AUC) in the prediction of the outcome coercion/no coercion when cross validation is used. Due to the better generalizability machine learning is a promising approach for further studies, especially when more variables are analyzed. More detailed knowledge about individual risk factors may help to prevent the occurrence of situations involving coercion.
Introduction
The use of coercive measures (e.g., seclusion, physical and mechanical restraint, forced medication) in psychiatric patients is a massive invasion in their integrity and freedom. As a result, the usage of coercion is controversially discussed since the beginning of modern psychiatry and certain approaches have tried to reduce its rates (1). Although some of those approaches were successful, there are still many patients in which coercion is used. Often the usage of coercion seems necessary when the patients are a danger for themselves or for others due to an underlying psychiatric disorder (2, 3). These situations are always associated with an ethical dilemma. On one side coercion shall help to protect the patient's or other's integrity (2, 3). On the other hand it restricts the freedom of the person which is one of the basic human rights (4). Being a threat to oneself or others may have different reasons in psychiatric patients. In some situations patients are delusional and feel threatened by others which leads to the reaction to protect themselves and can result in threats to other patients or staff (5). Also in situations where the patients are threatening themselves or have suicidal ideations caused by the symptoms of their psychiatric disorder, coercive measures might become necessary to secure the patients survival.
The use of coercion distinguishes psychiatry from other medical disciplines where informed patients can decide to accept or reject a specific measure. Psychiatry at one hand aims to help the patients to develop a self-determined life without burden of psychiatric symptoms. On the other hand psychiatry is legally determined to reject the patients freedom to move (involuntary hospitalization) but also the freedom to reject a specific measure (forced medication, physical or mechanical restraint, seclusion) if harm to self or others has to be disrupted.
It is obvious that such situations are challenging for the patients but also for the therapeutic team. Those challenges were topic of previous studies where it was shown that patients who experienced coercive measures often describe feelings of helplessness (6, 7), fear (8), anger (9, 10) and humiliation (11). Due to that, some patients stated to avoid searching for psychiatric help in a crisis (12, 13). On the other hand there were some patients who retrospectively agree with the coercive measure (7, 9) and state that they would like to be forced into treatment again in the case of a future crisis (14). These contrary findings underline the controversy of this topic.
It was the goal of earlier studies to understand which patients experience coercion and to characterize their clinical, but also their socioeconomic features. Gaining better understanding of risk factors to experience coercion was thought to be helpful in the development of therapeutic strategies for patients at risk and thus, to reduce the prevalence of coercion.
During the last years specialized psychiatric intensive care units (PICU) had been the center of extensive research and it could be shown that some patient characteristics are associated with the transfer from a general psychiatric unit to a PICU and with the usage of coercion on these specialized wards (15). Furthermore psychotic disorders were shown to be frequently associated with coercion (16–24). Also personality disorders (25, 26), substance-use-related disorders (19) and mental retardation (25) were found to be associated with coercion. A history of aggression (16–18, 22, 23, 25, 27–29) was frequently found to be associated with coercion and violence/threats were described to be the second most frequent reasons after agitation/disorientation for the usage of coercion (30). Patients with a history of former voluntary and/or involuntary commitments (IC) and frequent hospitalizations (16–20, 24) and those with longer duration of hospitalizations (31) were also described to experience coercion more often. Those factors were described nearly uniformly throughout literature. Whereas other factors like male (20, 23–25, 32, 33) and female gender (22, 29) or younger (19, 20, 23, 25, 28, 29, 32, 33) and older age (22, 24) were controversially associated with coercion in different study sites. These inconsistent findings impede the definition of risk-factors which are independent of specific countries. The inconsistencies between study sites were discussed to be caused by cultural influences, organizational factors, societal factors, the clinic-culture or a combination (34, 35). Besides that, one has to bear in mind that prior studies followed different methodological approaches to analyze data which additionally limits the comparability between different study sites. Some studies used descriptive approaches (16, 32) or group comparisons with binominal, non-parametric tests or ANOVA (17–20, 22–24, 26, 29, 30). To describe risk factors regression analysis was frequently used (19–21, 23, 26, 28, 29, 31, 33) and some studies extended their findings with an estimation of the area under the curve (AUC) (23). One study used a latent class analysis (LCA) which is capable of detecting the presence of groups in individuals with relatively homogeneous clinical courses (25). Another study used Multilevel random effects modeling (27). Only a few studies tried to describe the potency of specific risk factors to affect the outcome coercion/no coercion. Furthermore, the description of the specificity and sensitivity of the statistical models is scarce. One study which followed this approach described an acceptable AUC for one model using bivariate analysis (23). Another study found that with the included parameters only a limited prediction of patients at risk was possible (31). Thus, besides the analysis of risk factors at our study site, the second aim of this study was to find statistical approaches with a good balance in their specificity and sensitivity and prediction accuracy for the outcome “coercion/no coercion” in psychiatric inpatients. Furthermore we wanted to analyze the risk factors for their weights in affecting the outcome coercion/no coercion.
In today's psychiatric research machine learning is an emerging methodology. It is connoted with a great potential for innovation and paradigm shift as the algorithms facilitate integration of multiple measurements as well as allow objective predictions of previously “unseen” observations. We used this new approach to train and compare models with parameters available at admission and after discharge. To test for the hypothesis that machine learning algorithms are effective in the prediction of the outcome coercion/no coercion in psychiatric patients we compared binary regression analysis to the machine learning algorithms according to their sensitivity, specificity, accuracy, and AUC. Furthermore, we used machine learning to weight the included predictors for their potency in affecting the outcome coercion/no coercion. For the comparison of the two approaches we analyzed clinical data of involuntarily hospitalized patients at the University Hospital of Psychiatry Zurich and built two groups depending on the outcome Coercion/No Coercion.
Methods
Setting
The study was reviewed and approved by the Cantonal Ethics Commission of Zurich, Switzerland (Ref.-No. EK: 2016-00749, decision on 01.09.2016). Commitment documents as well as the medical records of patients involuntarily hospitalized at the University Hospital of Psychiatry Zurich during a 6-month period from January first to June 30, 2016 were analyzed.
N = 16 wards of the University Hospital of Psychiatry Zurich with a total of 252 beds were included. The clinic provides mental health services for a catchment area of 485,000 inhabitants.
Study Sample
No exclusion criteria were defined. We screened a comprehensive cohort of all patients admitted voluntarily and involuntarily to the University Hospital of Psychiatry Zurich during a 6-month period from January first to June 30, 2016 (n = 1,699 patients). For the analysis we included involuntarily committed patients (n = 577) and voluntarily committed patients who were retained at a later stage during their hospitalization and then changed to the legal status of involuntary hospitalization (n = 35).
Selection of Predictor Variables
Selection of predictor variables for “training” an algorithm in machine learning is challenging. We used a recommended method and searched the literature databases for variables which were already described to be associated with the usage of coercion: Psychiatric diagnosis (16–24), aggressive behavior (16–18, 22, 23, 25, 27–30), former voluntary or involuntary commitment (IC) and frequent hospitalizations (16–20, 24), gender (20, 22–25, 29, 32, 33), and age (19, 20, 22, 23, 25, 28, 29, 32, 33) were identified as variables of interest. We searched the routine documentation in the electronic medical files of the patients for these variables. The medical files include documentation about the socio-demographic parameters, admission circumstances, prescribed medication, documentation of coercive measures, and treatment planning. As there was no standardized assessment for aggression we searched which indirect information could be used and found IC due to danger to others and involvement of police in the admission process as indirect markers for aggressive behavior. Furthermore we included the procedural aspects abscondence, appeal to the court, duration until day passes, duration of IC, duration of hospitalization into analysis. When patients are exposed to coercive medication mostly antipsychotics or benzodiazepines are used. We were interested if the patients, exposed to coercion differed from those without coercion according to their regular prescribed medication during hospitalization. Thus, we searched the medical files for the prescription of medication classes (antipsychotics, antidepressants, benzodiazepines, and others).
Analysis and Machine Learning
We conducted analysis with MATLAB (MATLAB and Statistics Toolbox Release 2012b, The MathWorks, Inc., Natick, Massachusetts, United States.) and SPSS 23.0 (IBM Corp. Released 2011. IBM SPSS Statistics for Windows, Version 23.0. Armonk, NY: IBM Corp.) for Windows.
In a first step we compared patients with/without experience of coercion. We used cross-tabulation with chi-square tests for categorical variables. Due to the non-normal distribution we used Mann–Whitney tests for numeric variables. Variables that differed between both groups in bivariate analyses were included as potential risk factors in multivariate analysis. To analyze the impact of the risk factors on the outcome coercion/no coercion binary logistic regression analysis was used with coercion/no coercion as the dependent variable. The goodness of fit of the binary logistic regression model was assessed by the receiver operating characteristic (ROC) curve method. The AUC served as the criterion to determine the level of discrimination. Discrimination was deemed acceptable at AUC values between 0.7 and 0.79, excellent at values between 0.8 and 0.89, and outstanding at values over 0.9 (23). The specificity and sensitivity, positive predictive value (PPV) and negative predictive value (NPV) were calculated from the results of the different models.
Because of multiple comparisons Bonferroni's adjustments were made to prevent Type I error inflation (α = 0.05/5 = 0.01).
In a second step we tested the hypothesis that machine learning algorithms can be used to predict the outcome. Again the outcome of coercion/no coercion was used as dependent variable. Because the outcome was already defined, supervised learning algorithms [Logistic regression, supported vector machine (SVM), and bagged trees algorithms] were used. We used cross-validation to test the trained model. The training set was divided in 5 equal sized subsets with one part being used to train a model and the other four subsets to evaluate the accuracy of the learnt model (five-fold cross validation). The error rate of each subset was an estimate of the error rate of the classifier. Cross-validation is used in machine learning to establish the generalizability of an algorithm to new or previously “unseen” subjects. The validity of the algorithms in predicting the outcome coercion from no coercion was evaluated using prediction accuracy, sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV). In this study, sensitivity and specificity represented correctly predicted occurrence of coercion (true positives) and correctly predicted lack of coercion (true negatives), respectively.
Logistic Regression
The classifier models the class probabilities as a function of the linear combination of predictors. Logistic regression utilizes a typical linear regression formulation.
Support Vector Machines (SVM)
This technique separates data by a hyperplane, trying to maximize the margin and creating the maximum distance between the hyperplane and the values which lie on each side. The higher this distance gets the better is the reduction of the expected generalization error.
SVM are robust in dealing with large numbers of features included because only those features which lie on the margin of the hyperplane are included. If data are non-linear and separation is not possible on one hyperplane, SVM can create more dimensional hyperplanes in a higher dimensional feature space. SVM methods are binary. So in the case of this study where we compared the patient group with/without coercion no dummy-variables had to be created for the response-feature.
Decision Trees
Decision trees classify instances by sorting them based on feature values. The nodes represent instances in the feature to be classified and the branches represent values that the node can become. The instance which divides the training data in the best way is selected as the root node. Than the instance which best divides this feature is chosen and so on. There are many ways to select the instance which is best at dividing data. It is possible to train ensembles of regression trees. They combine results from many weak learners into one high-quality ensemble model and are potent in the analysis of skewed data.
In generally, methods like SVMs and neural networks perform well with balanced continuous and multi-dimensional features whereas logic-based systems like decision trees or rule learners perform better with discrete/categorical variables.
SVMs are potent in dealing with large data which increase their prediction accuracy. These techniques can also work in the case of multi co-linearity and non-linear relationships. Logic based systems like decision trees are easier to interpret than SVMs.
Imbalance Problem
Class imbalance where the number of patients in one class (e.g., no coercion) exceeds the patients in the other class (e.g., coercion) is a common problem in machine learning. A typical machine learning algorithm trained with an imbalanced data set would assign new observations to the majority class (e.g., no coercion) (36). In this study we met this problem by creating an artificial group with balanced distribution of the outcome (coercion/no coercion). We assigned random numbers to the cohort of 612 patients which were involuntary hospitalized during the study period. We selected those patients without documentation of coercion during their hospitalization and sorted them by ascending numbers. We then excluded the first half of this group of patients. Thus, we conducted the analysis with 393 patients (no coercion: n = 223, coercion: n = 170). In those patients who experienced coercion, at least one coercive measure (e.g., seclusion, coercive medication, restraint alone, or in combination) was used during hospitalization.
Results
Comparison Between Groups of Patients With/Without Coercion During Involuntary Hospitalization
Being a threat to others (72%) or self and others (20%) were the most frequent reasons for the usage of coercion. Clinical aspects like a higher CGI at admission, psychotic or personality disorders, the prescription of antipsychotics and benzodiazepines, harm to others or harm to self and others before admission, and male gender were significantly associated with the usage of coercion. From the procedural side being retained, police involvement at admission, the number of former admissions, a history of IC, a longer duration until patients were allowed for day passes, duration until revocation of involuntary hospitalization and duration of hospitalization, appeal for prolongation from the clinic but also appeal for early discharge from the patient were significantly associated with the use of coercion. We found an association between a secondary diagnosis of a substance-use-related disorder and coercion which was not significant (for details see Tables 1, 2).
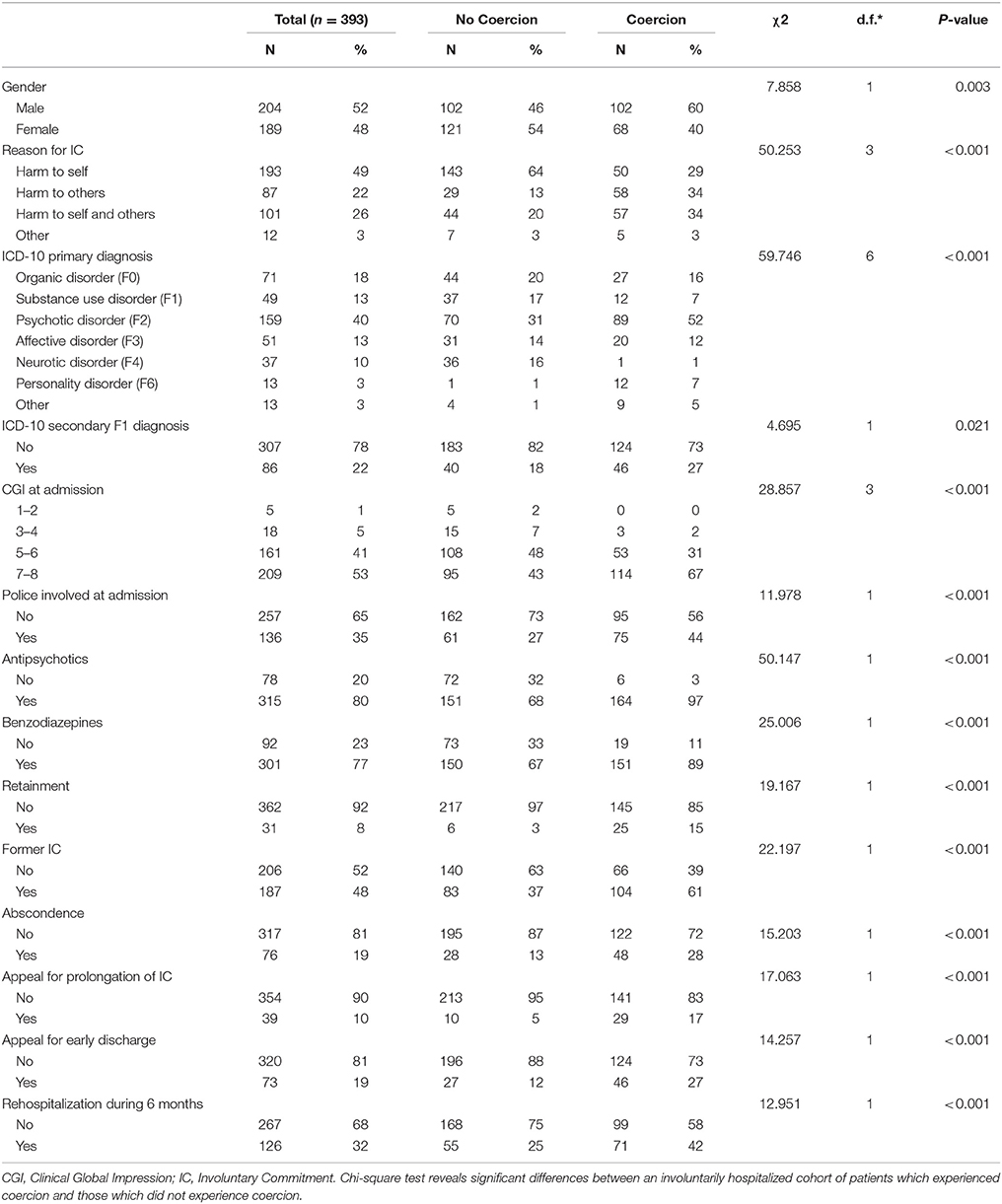
Table 1. Comparison of socio-demographic and clinical aspects in patients with/without coercion.
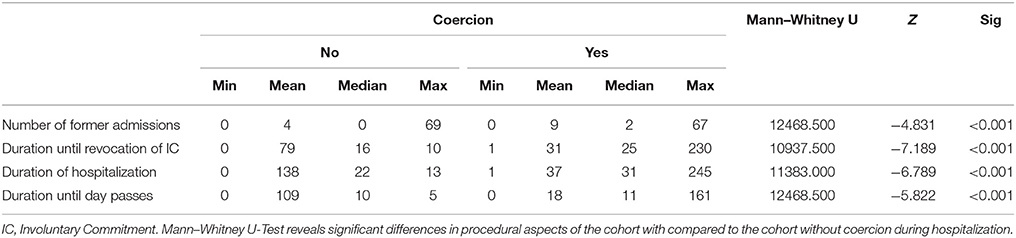
Table 2. Comparison of socio-demographic and clinical aspects in patients with/without coercion.
Age at admission (Mann–Whitney U: 17454.000, Z: −1.346, p = 0.178, n = 393) and Nationality did not differ significantly between the groups [ = 6.466, p = 0.373, n = 393]. Also we found no significant group difference for skills in German language, which is the official language in the state of Zurich, [χ2 = 0.384, p = 0.825, n = 393] and educational-level [ = 8.285, p = 0.218, n = 393].
Two Models to Predict the Outcome Coercion/No Coercion
The main question of this study was to find models with a good accuracy in the prediction of the outcome coercion/no coercion. With a supervised learning technique a predictive model can be tested for both, input and output data. We trained and tested two models for their accuracy in the prediction of the outcome coercion/no coercion. For comparison we computed the same two models in binary logistic regression.
The first model included data which were available at hospital admission. In the second model we included variables which are available after a whole course of hospitalization. We hypothesized this second model to have higher prediction accuracy. The variables included in both models are shown in Table 3.
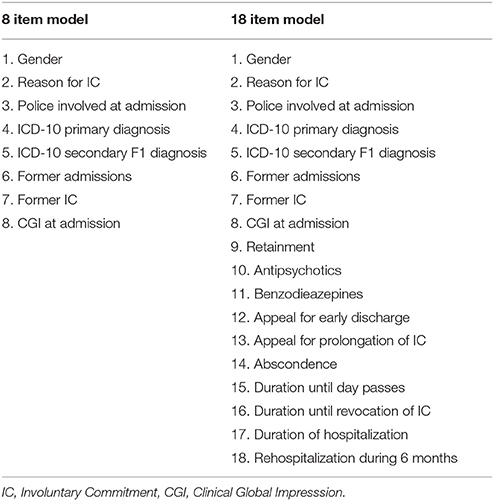
Table 3. Included predictors in both models.
Binary logistic regression in SPSS and logistic regression in ML had the same results for B, SE, and p. This is comprehensible as logistic regression utilizes a typical linear regression formulation. The calculation of the coefficients/weights is different between both approaches and led to different results. Details are shown in Table 4.
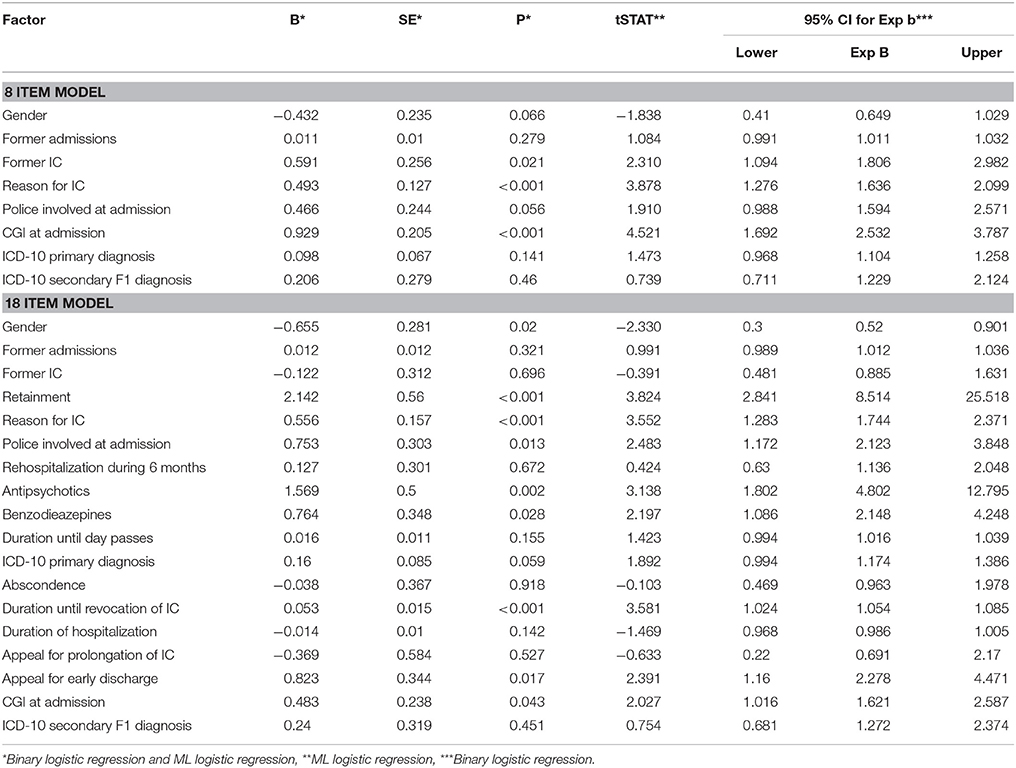
Table 4. Findings of binary logistic regression and ML logistic regression.
The machine learning algorithms (Quadratic SVM, Ensemble RUSBoosted Trees and Logistic regression) predicted the outcome parameters (coercion/no coercion) with a balanced accuracy ranging from 66.5 to 69% (the quadratic SVM algorithm identified 102 out of 170 patients which experienced coercion) in the model with 8 parameters and 71.5–76% in the model with 18 parameters. In contrast the binary logistic regression in SPSS had a balanced accuracy of 68.5% in the 8 item model and 78.5% in the 18 item model. In the 18 item model the logistic regression algorithm identified 121 out of 170 patients which experienced coercion (sensitivity). This resulted in an accuracy of 75%. The binary logistic regression of SPSS identified 124 out of 170 patients which experienced coercion and was more potent in predicting those who did not experience coercion (187 out of 223 patients). This resulted in an accuracy of 78.5%.The Quadratic SVM was able to predict 185 out of 223 patients without coercion and had less potency in predicting the outcome coercion (117 out of 170 patients). For details see Table 5.
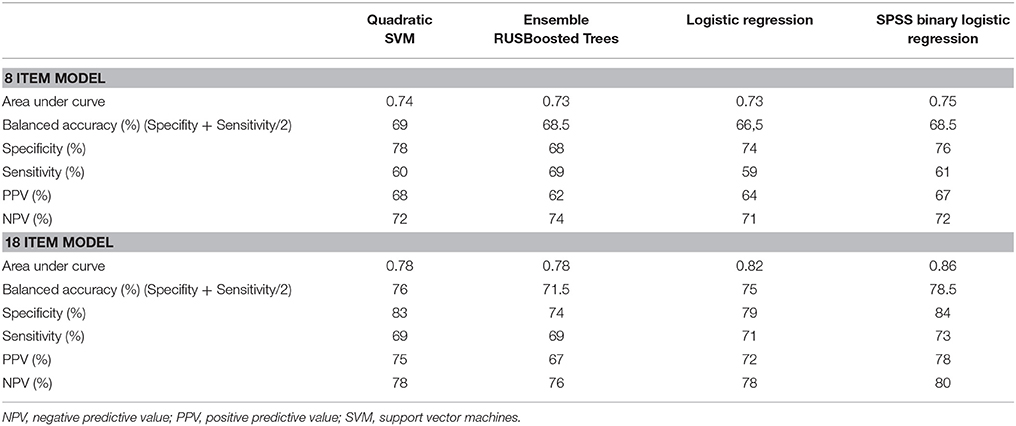
Table 5. Comparison of the 8 and 18 item models.
Due to inconsistent findings in literature we also created two models which did not include the variables gender and substance-use-related disorders as co-diagnosis (which was not significantly associated in our bivariate analyses). The results were comparable but not as robust as the 8 and 18 item model. They are shown in Table 6.
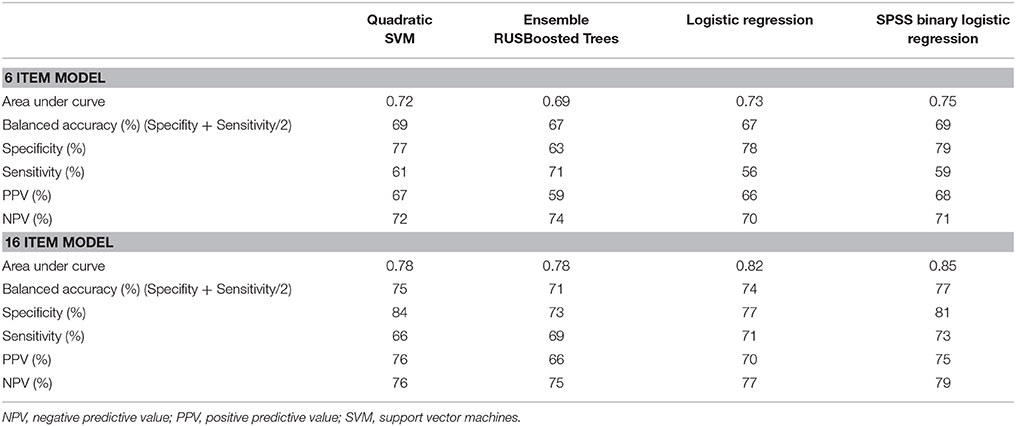
Table 6. Comparison of the 6 and 16 item models.
Weighting of Risk Factors to Experience Coercion
In a next step we analyzed the relevance of each variable in the prediction of the outcome coercion/no coercion. We compared the weights of the included variables between logistic regression in ML and binary logistic regression. We analyzed the relevance of predictor variables in distinguishing the outcome coercion/no coercion. Positive coefficients or weighting factors were assigned to an increase in coercion for the 8 and 18 item models.
In the model with 8 items the CGI at admission had the highest weight. In ML this was followed by the reason for IC, former IC and a police involvement at admission. In binary logistic regression the second weighted predictor was former IC followed by reason for IC and police involvement at admission.
In the 18 item model retainment was the highest weighted predictor. In ML this was followed by duration until revocation of IC, reason for IC at admission and prescription of antipsychotic medication. In binary logistic regression antipsychotic medication was weighted after retainment, followed by appeal for early discharge and the prescription of benzodiazepines. In both models female gender was negatively weighted. For details see Figure 1.
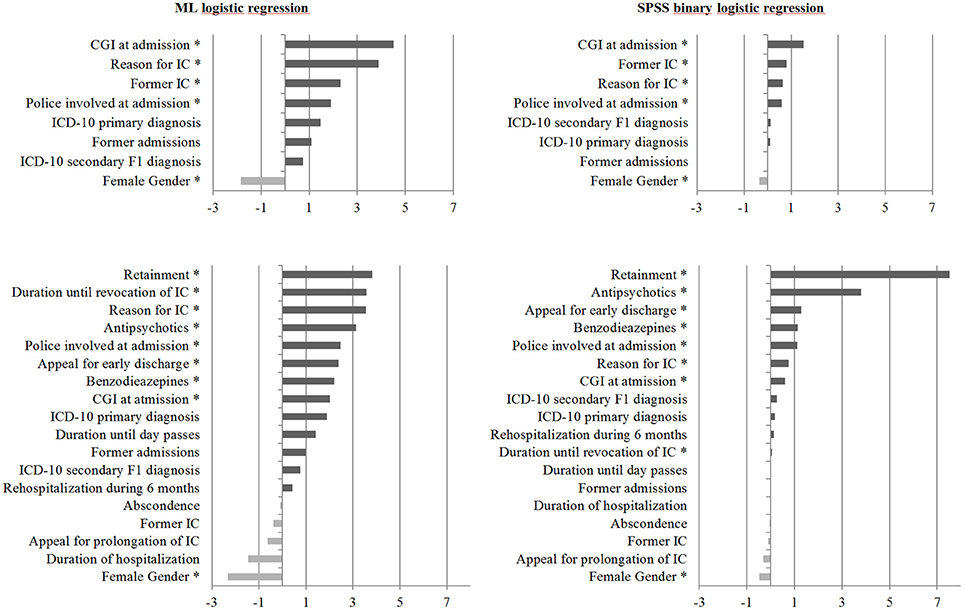
Figure 1. Bar graphs showing weighting factors assigned to each variable based on their relevance in distinguishing the outcome coercion from no coercion. Variables which increase the probability of an individual patient to experience coercion were assigned positive weighting factors whilst those that decrease the probability of a patient experiencing coercion were assigned negative weighting factors. *Significant at the 0.05 level.
Discussion
This study could show that machine learning algorithms can predict the outcome of coercion/no coercion in a patient group with a good accuracy and have some advantages compared to binary logistic regression which also appeared to have a good accuracy. All algorithms achieved greater than chance (50%) accuracy in distinguishing patients with coercion from those without coercion. We could verify the hypothesis that a model with a higher number of variables (including variables which occur during the course of hospitalization) was more potent in the prediction of the outcome coercion/no coercion. The AUC was acceptable in the model with 8 items with values from 0.73 to 0.75. In the model with 18 items the AUC reached values from 0.78 to 0.86 which implies excellent results in 2 out of 4 algorithms. In the model with 8 items quadratic SVM had the best accuracy whereas binary logistic regression had the best accuracy in the 18 item model. All the included algorithms had a good balance of specificity and sensitivity. Although the binary logistic regression appeared to have a slightly better AUC than the machine learning algorithms the machine learning algorithms appear to have an advantage. By using cross validation the training data are divided into a set of data where the model is trained and another k (in this study k = 5) sets of data where the trained model is validated. Thus, the accuracy of the trained model is verified in data sets which are independent of the trained data. This allows better generalizability for the prediction accuracy because it was tested on “new” data. This is different from conventional binary logistic regression where all data are used in one analysis and generalizability is limited.
The fact that the models can predict the occurrence of coercion/no coercion with a good accuracy of 69% in the model with 8 parameters and even more in the model with 18 parameters underlines the relevance of the included variables for clinical use and future research. Although the parameter were not able to explain all variance some of them can be defined as substantial “risk factors” for the experience of coercion during psychiatric hospitalization. In the 8 item model the CGI at admission had the highest weight, followed by reason for IC, former IC, and police involvement at admission. In the 18 item model retainment had the highest weight.
By knowing risk factors and their weights it might be possible to identify groups of patients at risk by using a risk assessment tool. Patients could be divided into different risk groups. Treatment strategies could be adjusted to the different risk groups and help to prevent the occurrence of situations in which the usage of coercion seems necessary. Harm to others as reason for IC, former IC, and police involvement at admission were high weighted in both approaches. Combined with the finding that most coercive measures were applied due to harm to others this implies that aggression is a challenge for staff. This has also been shown in other studies (26, 30, 37–39) and was one reason to develop specialized PICU's where staff is trained in aggression management (40). Retainment, the highest weighted predictor in the 18 item model, implies a high-risk situation and should be considered as a reason for the transfer to such PICUs (15). The CGI, which was highly weighted in the 8 item model is not specific but implies that patients at risk may be more likely to meet the criteria for severe mental illness (SMI). Although being less weighted, the psychiatric diagnosis should also be included in the risk assessment. Patients with a psychotic disorder or a personality disorder appeared to have an increased risk to experience coercion in our analysis and in previous literature (16–26). Also male gender should be considered in the risk assessment. Nevertheless, gender needs to be reflected with caution because other studies found female gender to be significantly associated with coercion (22, 29).
In patients at risk the regular use of the Brøset Violence Checklist could be helpful in identifying situations where the risk for aggressive behavior is increased (41) and was shown to result in a decreased rate of aggressive incidents (42). A cooperation between mental health community and hospital teams (43), personal safety plans or treatment planning (25, 43), single rooms and retreat-rooms on the ward may help avoiding interpersonal stress. As mentioned above it was also shown that the segregation of disruptive patients in a psychiatric intensive care unit (PICU) (44) and the ward atmosphere (35) were effective in the reduction of aggressive behavior. A more recovery orientated view might be helpful to build a relationship between patient and the therapeutic team. Also staff training in communication skills, fast building and maintenance of a stable therapeutic relationship could help to reduce situations in which coercion is used (37).
As mentioned above, previous studies followed different methodological protocols. To provide comparability between different study sites, statistical models should be used which follow a comparable methodological approach. These models should have a good accuracy and be easy to replicate in different countries. This study could show that ML algorithms (logistic regression, SVM, decision trees) can predict the outcome coercion /no coercion in a group of patients with a good accuracy and explain some of the variance. Furthermore machine learning can be used for weighting of the included predictors. Cross validation provides a better generalizability of the results which is attractive for the usage in different study sites. Previous studies could show that beside risk-factors in patients also procedural factors like closed ward doors (45), architecture and atmosphere of a ward (35, 46) or interpersonal factors like escalating behavior of staff (47, 48) may be a risk for violent behavior in the patients and consecutively the usage of coercion. Future studies should therefore aim to analyze the weights of clinical culture, attitude toward coercion in the therapeutic teams and organizational factors to test if these factors account for the unexplained variance in the prediction models used in this study.
Limitations
Some limitations must be mentioned regarding to this study. Although we runned tests for each predictor alone and different combinations of the predictors some of the predictor variables may influence each other. This may have lead to a bias in the prediction potency of the models.
Artificial balance was created by decreasing the number of participants with the outcome no coercion.
In the group comparison some categories (e.g., diagnostic groups, harm-criteria, CGI-groups) were very small and due to that may have contributed to a significant effect. Previous studies showed comparable findings. On this background we included these small groups in analysis. Further studies should re-evaluate our results with a bigger sample size.
The analysis was based on retrospectively collected data, and it was not possible to assess the subjective perspectives of patients and physicians in a standardized form. Due to the retrospective character of the study the psychopathological symptoms could not be assessed in a standardized way. Because of that, important information about the severity of symptoms during the situation in which coercion was used is lacking. Furthermore it was not possible to assess if alternatives were used before coercion had to be used. We were not able to include data on treatment culture and socio-cultural factors in general into our analysis. This would be an interesting topic for future research.
Conclusion
This study was able to show that ML is useful in the prediction of coercion and reach comparable results to binary logistic regression although the trained algorithms are used on new sets of validation data (five-fold cross validation) which allows a better generalizability. ML is a promising approach for further research on risk factors and the occurrence of coercion in psychiatry.
Weighting of risk factors may be helpful in the risk-assessment of the individual patients. In patients at risk special therapeutic strategies could be helpful to prevent the occurrence of aggressive behavior and consecutively coercion. Future studies should evaluate the potency of these strategies and the usefulness of risk-assessment tools.
Ethics Statement
The study was reviewed and approved by the Cantonal Ethics committee of Zurich, Switzerland (Ref.-No. EK: 2016-00749, decision on 01.09.2016). Commitment documents as well as the medical records of patients involuntarily hospitalized at the University Hospital of Psychiatry Zurich during a 6-month period from January first to June 30, 2016 were analyzed. All procedures were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This is a retrospective study. For this type of study formal consent is not required. This article does not contain any studies with animals performed by any of the authors.
Author Contributions
FH, SO, and MJ: conception and design, data collection, analysis and interpretation of data; FH: drafting the article; FH, AS, AT, PH, ES, SO, and MJ: revising the article critically for important intellectual content; FH, SO, MJ, AS, AT, PH, and ES: final approval of the version to be published.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Steinert T. After 200 years of psychiatry: are mechanical restraints in Germany still inevitable? Psychiatr Prax. (2011) 38:348–51. doi: 10.1055/s-0031-1276871
2. Zinkler M, Priebe S. Detention of the mentally ill in Europe–a review. Acta Psychiatr Scand. (2002) 106:3–8. doi: 10.1034/j.1600-0447.2002.02268.x
3. Lay B, Salize HJ, Dressing H, Ruesch N, Schoenenberger T, Buehlmann M, et al. Preventing compulsory admission to psychiatric inpatient care through psycho-education and crisis focused monitoring. BMC Psychiatry (2012) 12:136. doi: 10.1186/1471-244X-12-136
4. United Nation. General Assembly Convention on the Rights of Persons with Disabilities (2006) Available onlinbe at: http://www.un.org/esa/socdev/enable/rights/convtexte.htm
5. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®). Arlington, VA: American Psychiatric Publishing (2013).
6. Bergk J, Flammer E, Steinert T. “Coercion Experience Scale” (CES)–validation of a questionnaire on coercive measures. BMC Psychiatry (2010) 10:5. doi: 10.1186/1471-244X-10-5
7. Greenberg WM, Moore-Duncan L, Herron R. Patients' attitudes toward having been forcibly medicated. Bull Am Acad Psychiatry Law (1996) 24:513–24.
8. Naber D, Kircher T, Hessel K. Schizophrenic patients' retrospective attitudes regarding involuntary psychopharmacological treatment and restraint. Eur Psychiatry (1996) 11:7–11.
9. Haglund K, Von Knorring L, Von Essen L. Forced medication in psychiatric care: patient experiences and nurse perceptions. J Psychiatr Ment Health Nurs. (2003) 10:65–72. doi: 10.1046/j.1365-2850.2003.00555.x
10. Wynn R. Restraint and seclusion in a Norwegian university psychiatric hospital. Int J Circumpolar Health (2004) 63:445–7. doi: 10.3402/ijch.v63i4.17763
11. Whittington R, Bowers L, Nolan P, Simpson A, Neil L. Approval ratings of inpatient coercive interventions in a national sample of mental health service users and staff in England. Psychiatr Serv. (2009) 60:792–8. doi: 10.1176/ps.2009.60.6.792
12. Swartz MS, Swanson JW, Hannon MJ. Does fear of coercion keep people away from mental health treatment? Evidence from a survey of persons with schizophrenia and mental health professionals. Behav Sci Law (2003) 21:459–72. doi: 10.1002/bsl.539
13. Smith SB. Restraints: retraumatization for rape victims? J Psychosoc Nurs Ment Health Serv. (1995) 33:23–8.
14. Lucksted A, Coursey RD. Consumer perceptions of pressure and force in psychiatric treatments. Psychiatr Serv. (1995) 46:146–52.
15. Cullen AE, Bowers L, Khondoker M, Pettit S, Achilla E, Koeser L, et al. Factors associated with use of psychiatric intensive care and seclusion in adult inpatient mental health services. Epidemiol Psychiatr Sci. (2018) 27:51–61. doi: 10.1017/S2045796016000731
16. Steinert T, Martin V, Baur M, Bohnet U, Goebel R, Hermelink G, et al. Diagnosis-related frequency of compulsory measures in 10 German psychiatric hospitals and correlates with hospital characteristics. Soc Psychiatry Psychiatr Epidemiol. (2007) 42:140–5. doi: 10.1007/s00127-006-0137-0
17. Ketelsen R, Schulz M, Driessen M. [Coercive measures: a comparison between six psychiatric departments]. Gesundheitswesen (2011) 73:105–11. doi: 10.1055/s-0029-1246181
18. Flammer E, Steinert T, Eisele F, Bergk J, Uhlmann C. Who is subjected to coercive measures as a psychiatric inpatient? a multi-level analysis. Clin Pract Epidemiol Ment Health (2013) 9:110–9. doi: 10.2174/1745017901309010110
19. Korkeila JA, Tuohimaki C, Kaltiala-Heino R, Lehtinen V, Joukamaa M. Predicting use of coercive measures in Finland. Nord J Psychiatry (2002) 56:339–45. doi: 10.1080/080394802760322105
20. Knutzen M, Mjosund NH, Eidhammer G, Lorentzen S, Opjordsmoen S, Sandvik L, et al. Characteristics of psychiatric inpatients who experienced restraint and those who did not: a case-control study. Psychiatr Serv. (2011) 62:492–7. doi: 10.1176/ps.62.5.pss6205_0492
21. Kalisova L, Raboch J, Nawka A, Sampogna G, Cihal L, Kallert TW, et al. Do patient and ward-related characteristics influence the use of coercive measures? Results from the EUNOMIA international study. Soc Psychiatry Psychiatr Epidemiol. (2014) 49:1619–29. doi: 10.1007/s00127-014-0872-6
22. Sercan M, Bilici R. [Restraint variables in a regional mental health hospital in Turkey]. Turk Psikiyatri Dergisi (2009) 20:37–48.
23. Dumais A, Larue C, Drapeau A, Menard G, Giguere Allard M. Prevalence and correlates of seclusion with or without restraint in a Canadian psychiatric hospital: a 2-year retrospective audit. J Psychiatr Ment Health Nurs. (2011) 18:394–402. doi: 10.1111/j.1365-2850.2010.01679.x
24. Odawara T, Narita H, Yamada Y, Fujita J, Yamada T, Hirayasu Y. Use of restraint in a general hospital psychiatric unit in Japan. Psychiatry Clin Neurosci. (2005) 59:605–9. doi: 10.1111/j.1440-1819.2005.01422.x
25. Beck NC, Durrett C, Stinson J, Coleman J, Stuve P, Menditto A. Trajectories of seclusion and restraint use at a state psychiatric hospital. Psychiatr Serv. (2008) 59:1027–32. doi: 10.1176/appi.ps.59.9.1027
26. Knutzen M, Bjorkly S, Eidhammer G, Lorentzen S, Mjosund NH, Opjordsmoen S, et al. Characteristics of patients frequently subjected to pharmacological and mechanical restraint–a register study in three Norwegian acute psychiatric wards. Psychiatry Res. (2014) 215:127–33. doi: 10.1016/j.psychres.2013.10.024
27. Bowers L, Van Der Merwe M, Nijman H, Hamilton B, Noorthorn E, Stewart D, et al. The practice of seclusion and time-out on English acute psychiatric wards: the City-128 Study. Arch Psychiatr Nurs. (2010) 24:275–86. doi: 10.1016/j.apnu.2009.09.003
28. Migon MN, Coutinho ES, Huf G, Adams CE, Cunha GM, Allen MH. Factors associated with the use of physical restraints for agitated patients in psychiatric emergency rooms. Gen Hosp Psychiatry (2008) 30:263–8. doi: 10.1016/j.genhosppsych.2007.12.005
29. Zhu XM, Xiang YT, Zhou JS, Gou L, Himelhoch S, Ungvari GS, et al. Frequency of physical restraint and its associations with demographic and clinical characteristics in a Chinese psychiatric institution. Perspect Psychiatr Care (2014) 50:251–6. doi: 10.1111/ppc.12049
30. Keski-Valkama A, Sailas E, Eronen M, Koivisto AM, Lonnqvist J, Kaltiala-Heino R. The reasons for using restraint and seclusion in psychiatric inpatient care: a nationwide 15-year study. Nord J Psychiatry (2010) 64:136–44. doi: 10.3109/08039480903274449
31. Hendryx M, Trusevich Y, Coyle F, Short R, Roll J. The distribution and frequency of seclusion and/or restraint among psychiatric inpatients. J Behav Health Serv Res. (2010) 37:272–81. doi: 10.1007/s11414-009-9191-1
32. Happell B, Gaskin CJ. Exploring patterns of seclusion use in Australian mental health services. Arch Psychiatr Nurs. (2011) 25:e1–8. doi: 10.1016/j.apnu.2011.04.001
33. Keski-Valkama A, Sailas E, Eronen M, Koivisto AM, Lonnqvist J, Kaltiala-Heino R. Who are the restrained and secluded patients: a 15-year nationwide study. Soc Psychiatry Psychiatr Epidemiol. (2010) 45:1087–93. doi: 10.1007/s00127-009-0150-1
34. Steinert T, Lepping P, Bernhardsgruetter R, Conca A, Hatling T, Janssen W, et al. Incidence of seclusion and restraint in psychiatric hospitals: a literature review and survey of international trends. Soc Psychiatry Psychiatr Epidemiol. (2010) 45:889–97. doi: 10.1007/s00127-009-0132-3
35. Rohe T, Dresler T, Stuhlinger M, Weber M, Strittmatter T, Fallgatter A. Bauliche Modernisierungen in psychiatrischen Kliniken beeinflussen Zwangsmaßnahmen. Der Nervenarzt. (2017) 88:70–7. doi: 10.1007/s00115-015-0054-0
36. Dubey R, Zhou J, Wang Y, Thompson PM, Ye J. Alzheimer's Disease Neuroimaging I. Analysis of sampling techniques for imbalanced data: an n = 648 ADNI study. Neuroimage (2014) 87:220–41. doi: 10.1016/j.neuroimage.2013.10.005
37. Husum TL, Bjorngaard JH, Finset A, Ruud T. A cross-sectional prospective study of seclusion, restraint and involuntary medication in acute psychiatric wards: patient, staff and ward characteristics. BMC Health Serv Res. (2010) 10:89. doi: 10.1186/1472-6963-10-89
38. Bowers L. On conflict, containment and the relationship between them. Nurs Inq. (2006) 13:172–80. doi: 10.1111/j.1440-1800.2006.00319.x
39. El-Badri SM, Mellsop G. A study of the use of seclusion in an acute psychiatric service. Aust N Z J Psychiatry (2002) 36:399–403. doi: 10.1046/j.1440-1614.2002.01003.x
40. Gwinner K, Ward L. Storytelling, Safeguarding, Treatment, and Responsibility: attributes of recovery in psychiatric intensive care units. J Psychiatr Intensive Care (2015) 11:105–18. doi: 10.1017/S1742646414000181
41. Woods P, Almvik R. The Broset violence checklist (BVC). Acta Psychiatr Scand. (2002) 106:103–5. doi: 10.1034/j.1600-0447.106.s412.22.x
42. Abderhalden C, Needham I, Dassen T, Halfens R, Haug HJ, Fischer JE. Structured risk assessment and violence in acute psychiatric wards: randomised controlled trial. Br J Psychiatry (2008) 193:44–50. doi: 10.1192/bjp.bp.107.045534
43. Fiorillo A, De Rosa C, Del Vecchio V, Jurjanz L, Schnall K, Onchev G, et al. How to improve clinical practice on involuntary hospital admissions of psychiatric patients: suggestions from the EUNOMIA study. Eur Psychiatry (2011) 26:201–7. doi: 10.1016/j.eurpsy.2010.01.013
44. Vaaler AE, Iversen VC, Morken G, Flovig JC, Palmstierna T, Linaker OM. Short-term prediction of threatening and violent behaviour in an Acute Psychiatric Intensive Care Unit based on patient and environment characteristics. BMC Psychiatry (2011) 11:44. doi: 10.1186/1471-244X-11-44
45. Lang UE, Hartmann S, Schulz-Hartmann S, Gudlowski Y, Ricken R, Munk I, et al. Do locked doors in psychiatric hospitals prevent patients from absconding? Eur J Psychiatry (2010) 24:199–204. doi: 10.4321/S0213-61632010000400001
46. Salzmann-Erikson M. Limiting patients as a nursing practice in psychiatric intensive care units to ensure safety and gain control. Perspect Psychiatr Care (2015) 51:241–52. doi: 10.1111/ppc.12083
47. Whittington R, Wykes T. Aversive stimulation by staff and violence by psychiatric patients. Br J Clin Psychol. (1996) 35(Pt 1):11–20.
Keywords: coercion, seclusion, restraint, coercive medication, involuntary hospitalization, machine learning
Citation: Hotzy F, Theodoridou A, Hoff P, Schneeberger AR, Seifritz E, Olbrich S and Jäger M (2018) Machine Learning: An Approach in Identifying Risk Factors for Coercion Compared to Binary Logistic Regression. Front. Psychiatry 9:258. doi: 10.3389/fpsyt.2018.00258
Received: 08 November 2017; Accepted: 24 May 2018;
Published: 12 June 2018.
Edited by:
Meichun Mohler-Kuo, University of Applied Sciences and Arts of Western Switzerland, SwitzerlandReviewed by:
Eric Noorthoorn, GGNet Mental Health Centre, NetherlandsRaoul Borbé, Universität Ulm, Germany
Copyright © 2018 Hotzy, Theodoridou, Hoff, Schneeberger, Seifritz, Olbrich and Jäger. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Florian Hotzy, Zmxvcmlhbi5ob3R6eUBwdWsuemguY2g=