 Helio Gomes Rocha Neto1*
Helio Gomes Rocha Neto1* Carlos Eduardo Estellita-Lins2José Luiz Martins Lessa3Maria Tavares Cavalcanti3
Carlos Eduardo Estellita-Lins2José Luiz Martins Lessa3Maria Tavares Cavalcanti3- 1Centro Universitario Lusíada, São Paulo, Brazil
- 2Fundação Oswaldo Cruz (Fiocruz), Rio de Janeiro, Brazil
- 3Instituto de Psiquiatria, Universidade Federal do Rio de Janeiro, Rio de Janeiro, Brazil
Background: Mental State Examination (MSE) is compared with physical examination as a reliable method of objective data investigation. There is a growing concern with psychiatric clinics, nosology, and the reliability of diagnostic interview methods as a source of valid diagnostic strategy. Efforts to achieve an international diagnosis protocol have been unsuccessful or polemical. This paper focuses on psychopathology, MSE, and mental function development within Brazilian psychiatry over the last few decades.
Methods: Searches, interviews, and narrative reviews were done to look for systematic ways in which to conduct MSE, mental functions, symptom clusters, orientations about data observation and records. Brazilian psychopathology textbooks were examined, if they provided access to consolidated knowledge on psychopathology examination.
Results: Sixteen textbooks were selected from a 49 year span. Descriptive psychopathology with phenomenological orientation was the primary trend in the MSE. Concepts derived from different traditions, most lacking common terminology, suggested some divergence among authors. Recommendations for patient observation and how to collect objective data was clear, but MSE standardization efforts were missing. A detailed description of mental function abnormalities was the main MSE record strategy, without consensus about ways to summarize and record this data. In an examination summary, mental strata was divided into “mental functions,” and MSE subsets were frequent. All authors considered the following mental functions: consciousness, perception, thought, memory, attention, orientation, and volition.
Discussion: Psychiatric competence demands MSE proficiency. Official documents are not clear about performance and recording standards. MSE data was usually recorded through descriptive psychopathology. A shift from detailed descriptive findings, to an array of observed pathological elements, described through a mental function checklist was observed over time. Clinical practice and research guidelines should consider the development of reliable MSE practices; however, it has been neglected by modern psychiatry/neuroscience through the excessive emphasis on interview protocols. Better MSE practices, and the improvement of bedside skill in psychiatry are necessary and depend on the recovery of psychopathological debates and semiological reasoning, which will allow the return of phenomenology-oriented “observational” techniques.
Introduction
In modern clinical medicine, a diagnosis is obtained through the crossover of symptoms, obtained by anamnesis or by a clinical interview, and signs of symptoms, obtained through a physical examination and laboratory or image tests (1). The former is supposed to spark multiple hypotheses which the clinician then further investigates by looking at patient's signs and symptoms. Semiology has been described in many textbooks as Porto (2) or Bates (3), and was over time formalized as the paramount method of clinical examination in internal medicine.
Such standard foundational programs were made possible through Claude Bernard's experimental medicine (4), confirmed by Alvan Feinstein one century later, whereby stating that recent clinical epidemiology belongs to the same epistemological strata (5–7). The same method was implemented in most medical specialties, including psychiatry (8, 9). With regard to general medical practice, physical examination (PE), lab, and image procedures provide the standard method to gather objective information, which is then used to refine the previously elaborated hypothesis through the anamnesis/interview method. The very idea of a PE and semiology was strengthened by the transformations of modern medicine, and was consolidated with the Flexnerian reformation of medical schools (10, 11).
Psychiatry has tried to take part in this agenda and match such standards (12). Clinical interviews as a standard procedure for anamnesis in psychiatry, has been rigorously investigated. An extensive bibliography, concerning how to improve an examiners agreement about symptoms, and a rising consensus about the need for a minimal structure for better clinician reliability, is now evident (13–19). Mental health practice often uses Mental State Examination (MSE) as an equivalent to PE from routine clinical examination and as a reliable method for objective data gathering (13, 20–22), since PE and MSE are logically correlated. However, clinical interview/anamnesis is previous to, and also guides PE procedures and laboratory searches, but it is the core of the mental/psychic examination process and used predominately in most cases. However, the interview is a narrative, history taking method, and not an objective sign gatherer tool.
The interview should be a narrative, recollection method, not an objective investigative tool. PE is consistently mentioned throughout almost all propaedeutical textbooks in medicine, with minimal, if not aesthetical, variations. MSE however has not achieved any international protocol or structured general tool, not even a minimal array of standard techniques and clinical report methods. Although MSEs widespread use as a PE correlative might not be suitable and may also be equivocated (9, 23, 24), it still universally used to gather data, objective information and evidence in mental health practice.
MSE was simultaneously developed in different regions of the world, influenced by philosophically-oriented ideas on psychopathology (25, 26). Many psychopathology textbooks have also been written in different languages, according to different traditions, which have resulted in vast variations in technique and nomenclature (27, 28). Nevertheless, mental semiology has been overlooked in most historiographical efforts, despite the importance of nosological history (29).
In the last 30 years, new trends in the history of psychiatry in Brazil developed, but none has considered mental examination. Estellita-Lins attempted to emphasize the phenomenology of living space (espace vécu) in Jaspers Psychopathology Textbook and its vital role concerning signs, “evidence” and examination (30). Cheniaux (31) reviewed some of the Brazilian, and even foreign textbooks about “descriptive psychopathology,” searching for conceptual regularity or terminological “uniformity” among authors, but MSE was not addressed. Viotti Daker worked on the main Brazilian textbook by Nobre de Melo, examining its psychopathological models (32). Again, the MSE was not mentioned, but Melo's emphasis on fully assessing the person, before evaluating the particular functions subdivision, is noteworthy.
There is an increasing concern related to clinics and nosology in psychiatry. This concern might be traced back to Nancy Andreassen's claim concerning the loss of psychopathological knowledge by younger psychiatrists, and to Parnas' Danish group that contested the validity of the schizophrenia nosologic construct in DSM/ICD, further extended to the unreliability of diagnostic interview methods with structured diagnostic questionnaires (33, 34). We should also mention Jacob's questioning of MSE training in India (28), Aragona's interrogation about the collaboration of neuroscience in psychiatric diagnosis, among many others (35). As Rodrigues and Banzato have stated, if a sound agreement concerning the “validity” of a concept in psychiatry had already been achieved, there would not be such confusion around it (36).
We foresee epistemological issues concerning psychiatry and mental health care, that have not yet been resolved, as the importance of examination skills and training in the evidence-based era. These themes are not simply classificatory issues but are fundamental psychopathological efforts demanding a discussion concerning the diagnosis process in mental health and psychiatry.
This study deals with modern psychiatry from a historical perspective but addresses some clinical problems such as MSE, examination reporting, patient records and psychopathology teaching/transmission. A narrow comprehension of what evidence means may have been overlooked such as bedside skills and in particular phenomenological examining tradition (37–39). Maybe ongoing “taxonomic issues” and “classification wars” in psychiatry (40–42) are fair and useful, but we should also pinpoint some relevant matters that concern the examination, clinical reasoning and the diagnostic process itself (43).
Aiming to elucidate the origins, development, and methods of how MSE has been consolidated in Brazil, a review was carried out on the national literature.
Methods
MSE still lacks proper categorization in MESH and DeCS, and the best results of descriptors or key word searches were related to standard clinical interviews, therefore unsuitable for systematic MSE research purposes. Textbooks are known to be the introductory means to access expert knowledge in the medical field as defined by Ludwig Fleck (44). It was then decided to consider textbooks on psychopathology as a primary reference, following a timeline based on its reference and contents. A backward reference search was carried out at the start of 2017, using the Universidade Federal do Rio de Janeiro Library System, to look for psychopathology textbooks written or edited by Brazilian authors (UFRJ, Rede Minerva).1 The same search strategy was extended to main bookstore digital systems, and sites specialized in old or out of print editions, and finally to Google and Google Scholar. The main search string used was “psicopatologia” or “psiquiatria.”
Results
An initial list of 35 textbooks was selected. Among them were textbooks translated into Portuguese, not edited or written by Brazilian authors, and which were therefore excluded. Other books without any relevant chapters on MSE were also excluded. Twelve textbooks were finally chosen for the present study. The original list of books found and selected are presented in Tables 1, 2. Whenever possible, the first and last edition of each book was consulted, and discussions about systematic ways to conduct MSE, the ordering of MSE topics (distinct functions), orientations about data gathering and registration, definitions about “mental functions” and its levels, symptom clusters, groupings and set organization, were studied. Referenced articles and books citations were also checked. In older textbooks, terms and notions that are semantically related to MSE have changed over time. Therefore, any mention of a mental examination that clearly described careful mental observation techniques or descriptions was considered as similar or equivalent to MSE.
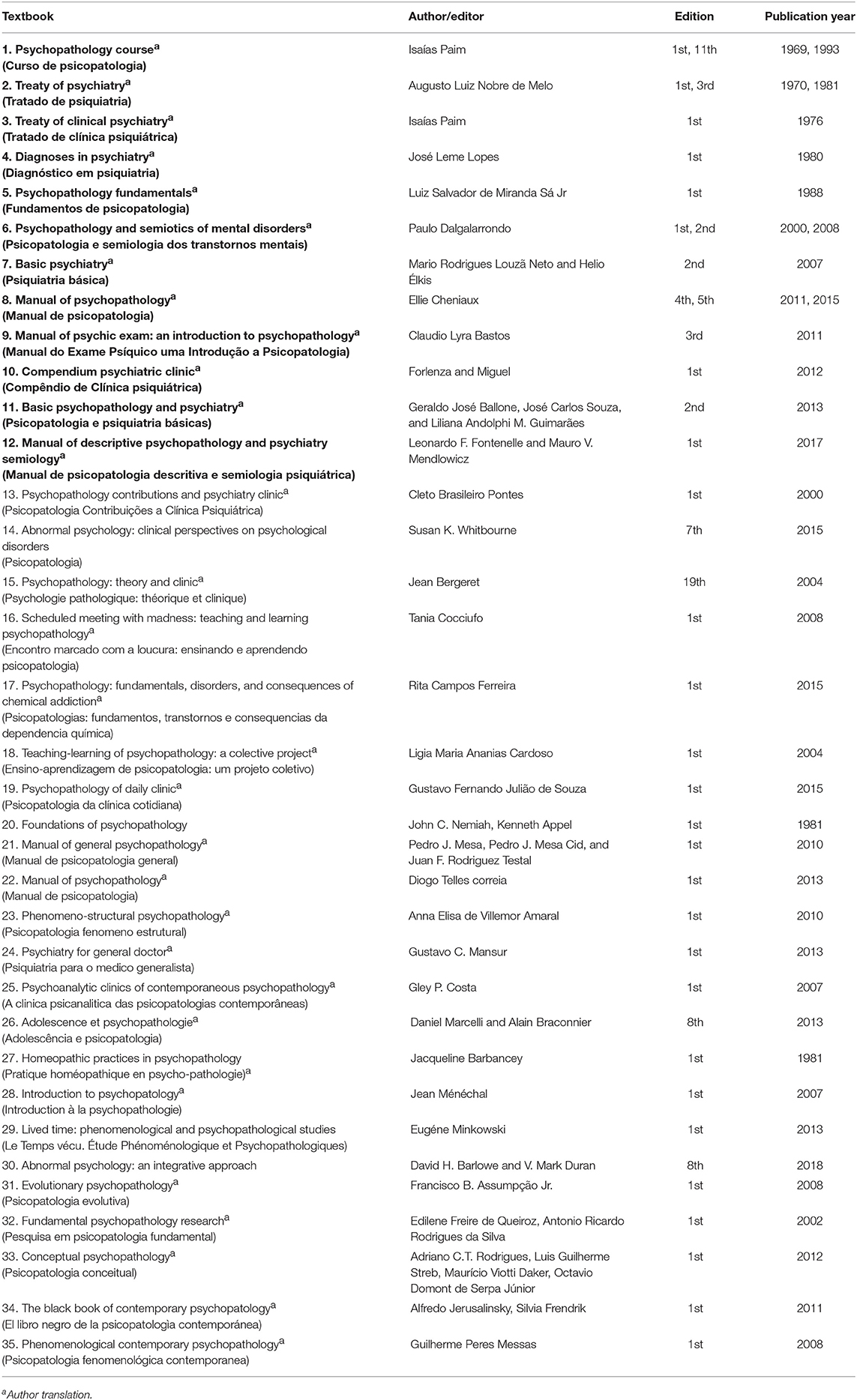
Table 1. Textbook set with editions, publication years, and the 12 titles (in bold) chosen for investigation of MSE.
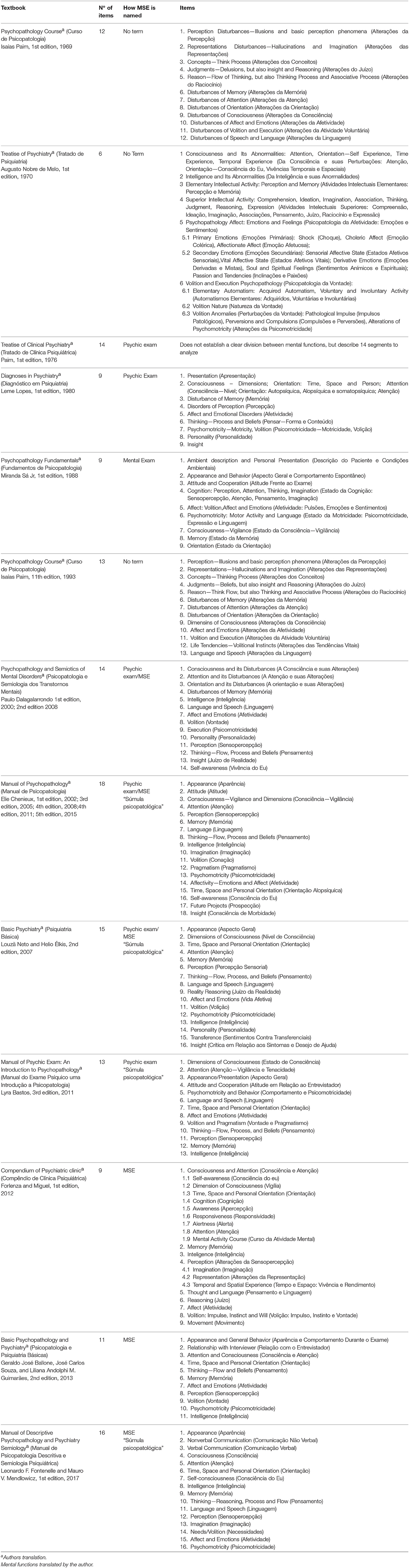
Table 2. MSE in the investigated textbooks, number of items, how it is named, and their items or assessed functions.
A comprehensive review was carried out on Brazilian authors, researchers and literature, focusing on different MSE traditions, describing its various approaches and MSE segmentation around psychic functions. The list of discrete elements assembled into MSE was studied in detail. A structured method to register significant psychopathological abnormalities/anomalies through examinations did show up in the search results. It was identified as “súmula psicopatológica” (psychopathological summary) in some textbooks.
The works examined spanned over the last 49 years. The books were written mostly by psychiatrists with clinical expertise, working as University Professors or lecturers. Most publications were designed to teach psychopathology to medical doctors being trained as a resident/internist in psychiatry. No MSE standard was identified, even though every author confirmed its relevance and consistency.
Most authors provided orientations on how to proceed with a careful patient observation during an interview, aimed at obtaining objective data. The most referred method, to organize and register MSE, consistently cited by some authors, was descriptive psychopathology with a phenomenological orientation. Textbooks agreed and actively encouraged a very detailed description of observed mental functions as the best way to record MSE. Additionally, there was no agreement on how to summarize its components (20–22, 45–54).
Throughout the time span studied, MSE was not the standard term used to refer to psychic examination and was first adopted in 2000 in the Brazilian psychopathology and semiology textbook by Paulo Dalgalarrondo (46), after which it was consistently used. It remains unclear if the term was chosen because of evidence-based efforts on examination, or if it represents a particular tradition. Regardless, Luiz Salvador de Miranda Sá Jr mentioned “mental examination,” an expression semantically related (50), and Elias Paim called it “psychic examination” around 1976, as did Leme Lopes in about 1980 (51, 55). The only author that did not use MSE after 2000 was Claudio Lyra Bastos, who still mentioned “Psychic Examination” (47).
All authors used subdivisions to analyze and describe MSE, but each provided a specific set. Even though there was a clear consensus that consciousness could only be artificially fragmented for didactic purposes, no agreement, convergence or discussion about the nature or number of necessary items could be identified. The theoretical basis underlying the operating subdivisions is therefore lacking. It remains unclear how these mental strata turned into a divided set of “mental functions.” Table 2 shows the items that form MSE, according to each author.
A concise examination summary through “súmula psicopatológica” was mentioned by only four authors (21, 22, 45, 47, 48). It was not possible to track the origins of this notion, since the authors did not mentioned or contextualize it. Some hypothesis is developed through discussion.
It is noteworthy that among the initial textbook list, some belonged to a field aimed at researching psychotherapy and psychoanalysis—therefore promoting a broader signification of psychopathology. Although these books were not included, and considering that psychoanalytic psychopathology is different from descriptive psychopathology, it probably suggests that psychoanalysis has had some influence in Brazilian psychiatric practices, perhaps in a slightly different way than what occurred in the United States (33, 56, 57). The term “interview” has widespread use when referring to the diagnostic and therapeutic encounter with patients, including psychoanalytical sessions, which may add further confusion when searching for Psychiatric methods of MSE using indexed expressions, and which justifies the frequency of these textbooks in the initial search sample. A better evaluation of such influence would be desirable, but it is out of the scope of this paper.
Discussion
Mental Health as a Brazilian tradition started in the nineteenth-century, after the creation of the hospice, by a Portuguese emperor (58–61). It was not before the beginning of 1900, however, that academic psychiatry began to thrive, particularly after studies published by Juliano Moreira, Ulisses Pernambucano, followed by studies on forensic psychiatry published by Nina Rodrigues and Franco da Rocha psychiatry (62–64).
The first psychopathology textbook edited by a Brazilian author was published by Isaías Paim at the very end of the 1960s (52), as far as we were able to trace. Paim's textbook stresses that psychopathology is not a psychiatric “tool,” but an entirely different “science,” that could be applied by psychiatrists to comprehend and investigate mental illness (52). Influenced by German and French authors, Paim thoroughly recommended detailed observations and descriptions of subjective reports (52) and behaviors as the best way to register and carry out psychic examination (55). This coupling of observation and description was continually reinforced by most authors analyzed (20–22, 45–55, 65).
The vast majority of textbooks considered MSE with clear subdivisions, except Paim's (55) Psychiatry Treatise. The number of partitions ranged from 6 (49) up to 18 items (45). The first time they are referred to as “Mental Functions” in our textbook sample was in Dalagalarrondo's “Psicopatologia e Semiologia” (46). Despite considerable variations in mental function descriptions and items adopted, all authors have explicitly considered the following mental functions: consciousness, perception, thought (not frequently comprising its 3-fold structure—Flow, Process, and content/Beliefs), memory, attention, orientation, and volition. Paim did not list mental functions in his treatise but had openly used it in his 1969 psychopathology textbook. These conceptual developments in Brazilian psychopathology call for further studies. We considered them as hints at the importance of mental function fragmentation and structure in psychopathology.
It was not possible to identify how subdivisions were adopted or created according to Brazilian textbooks. The lack of theoretical background may be responsible for the significant variation observed. Dividing or stratifying MSE seems to be the best method to analyze and to conveniently engage in description efforts, to evaluate psychic life. A discussion concerning ways to split MSE for adequate observation and educational purposes is out of the scope of the present review, but highly desirable. Since there are no globally standardized guidelines on psychopathology training (66), bedside examination skills must be regarded seriously, as an asset worth further exploring.
This chronologically considered textbook series, suggests that the first Brazilian authors that wrote about psychopathology—Nobre de Melo, (49) and Isaías Paim, (52)—did not aim to or were not used to describe MSE as mental function subdivisions, but were eager to build long and meticulous reports of observed behavior, through a personal interaction with patients. Contemporary Brazilian authors however usually mention clear descriptions of mental function subdivisions, setting standards on how to study MSE and how to describe it. It was not possible to identify a “standard” MSE organization, although a written description of all that is observed is consistent in both older and recent textbooks (20–22, 45–48, 50, 51, 53–55, 65). We could not identify any efforts aimed toward comparative clinical psychopathology.
The origins of the clinical resume called “súmula psicopatológica” could not be identified. It may have a forensic and juridical background, as its etymology suggests. Besides lawsuit writing rights, there were many other compulsory examination practices that the Brazilian and then the eugenics Constitution (1937) recommended. Psychiatrists were accountable for defining a person's state of mental health in many common judiciary cases such as criminal subjects, couples before marriage, institutionalized children, among others. For instance, forensic demands synthesis during a long diagnostic process and extensive judicial records.
Some leading psychiatrists, such as Franco da Rocha were very fond of this reporting procedure after clinical examination. A historiographic article, reviewing old patient files, depicts an explicit use of “súmula” by psychiatrists (67–69) when writing down their patient's observations around 1929. It is then possible to affirm that the use of “súmula” as the name given to the set of observed signs and symptoms in psychiatric interview was already widespread in Brazilian psychiatry by the early twenties.
Within the textbook set investigated, the first register of the word “súmula”—as a concise list of mental function subdivisions, containing psychopathological disturbances, observed through MSE—appears in Dalgalarrondo's textbook (46). The term “súmula psicopatológica” was also mentioned in Cheniaux psychopathology treatise (70). Cheniaux's communication, however, admitted that this precise notion had been in colloquial use since the early 90s, and declared that he was first introduced to it by prof Dr. Miguel Chalub, who also introduced him to categorized lists of mental functions with descriptive purposes2.
Chalub, in turn, declared that he learned this exact expression from Professor José Leme Lopes, the chairman of UFRJ Psychiatric Institute in the seventies.2 However, Leme Lopes' “Diagnoses in Psychiatry,” published in 1980 does not contain any mention of it (51). Neither Chalub nor Cheniaux needed to trace its roots but acknowledged its common use in bedside practices. Both authors hypothesized that it was borrowed from international psychopathological tradition, and that it become mainstream through everyday use in many institutional facilities in Brazil. The same inference about the expression “mental function” might therefore be adopted.
Efforts to standardize medical examinations have been at the core of scientific experimental medicine. These attempts have branched alongside psychopathology developments. The systematization of diagnostic psychiatric interview has been considered a significant step toward the improvement of clinician reliability. However, doubts about the best way to use it clinically, still remains (15, 71, 72). Countries, like Denmark, have already regulated the use of at least one standard interview in clinical practice, for any diagnosis in psychiatry (73) and others such as Australia use diagnostic tools in a mental health triage (74, 75). These are anamnesis/interview standardized methods however, not MSE.
ICD and DSM contain examining tools (Schedules for Clinical Assessment in Neuropsychiatry—SCAN, Structured Clinical Interview for DSM-5 Disorders—SCID-5, Mini International Neuropsychiatric Interview—MINI) (76–78). OPCRIT is supposedly useful to organize MSE, although it seems vastly different from what is usually accepted in descriptive psychopathology, since it provides neither mental function subdivisions nor any coordinated step care to enhance MSE observation and description (79). Nevertheless, the entire MSE procedure demands more than a structured interview, since it is not analogous to anamnesis, but correlated to the PE procedure. We suppose that MSE is not entirely congruent or wholly embedded in semi-structured interview protocols. Attempting to turn personal experiences into objective data is probably a source of unreliability between examiners, as previously described (19, 80–84). As far as we know, there is no standard method or procedure for MSE.
Parnas argues that DSM-V and ICD-10 were constructed to avoid subjectivity, but its developers have not accomplished such intent (23). He emphasizes that it is easy to find objective, observable signs inside many diagnostic criteria, such as “blunt affect” in schizophrenia or “fast speech” in mania. Such categories should have been avoided in a categorial diagnostic system based on a standard interview, that was developed to eliminate examiner opinion as a source of unreliability. In a standard interview, all diagnostic emphasis relies on a “yes” and “no” type series of questions, directed at the patient, who decides if a symptom is or is not present. If MSE categories were to be used in a categorial diagnostic system, it should provide a template MSE method to be followed by the examiner during practice. A list of valid abnormal psychopathological categories for classificatory issues should also be provided.
In Brazil, at least one recent official report, demands a careful description of MSE subdivisions into patient record files (85). The official document on psychiatric training in Brazil states that all candidates must be proficient on MSE skills (apply and record). Despite that, a standard MSE is not explicitly provided, and it is not clear how it should be done or registered (86). The Brazilian Association of Psychiatry (ABP), the professional body responsible for education, training, setting and raising standards in Brazilian Psychiatry, did not mention or provide any statements concerning MSE, until now (4th of May 2018).3
Since 2014, doctors that have experience in psychiatry or that have attended a psychiatry internship and desire to obtain a certificate in psychiatry must be submitted to a practical clinical examination test, in which they are observed while interviewing and examining a patient.3 It is not evident in the documentation how the MSE, or even the clinical interview, would be assessed and what they are expected to perform during a practical examination test (87). The only clue provided is from Dalgalarrondo's textbook inclusion of bibliographic references, which suggests that a detailed descriptive MSE and “súmula psicopatológica” is expected from candidates.
Conclusion
Our research suggests that descriptive psychopathology seems to be the usual MSE method used to observe and record data, not much different from the European schools or other parts of the world (80). Seven mental functions were consistently identified in the selected textbooks (consciousness, perception, thought, memory, attention, orientation, and volition), however no standard MSE and mental functions set was found. It was possible to identify a shift from the semiological discussion in Brazil during the last 50 years, from a detailed descriptive routine observed during the patient interaction to an array of observed pathological elements described through a mental function checklist. The “súmula psicopatológica” appears to be one pattern of examination, which could be improved or updated. Ethnopsychiatry or transcultural psychiatry research is needed regarding MSE, to achieve a regional attunement with patients and to comprehend the MSE practice in general.
MSE altogether, with anamnesis or a clinical interview, provides the basis for psychiatric clinics and research. Good clinical exercise and research guidelines in psychiatry must include the development of reliable MSE practice; however, it seems to have been neglected by modern psychiatry and neuroscience. Stressing interview protocols might flatten examination skills and impoverish MSE abilities. Development of better MSE practices and the improvement of bedside skills in psychiatry rely on reviving the psychopathological debate and semiologic reasoning of a vibrant tradition, and allowing for the return to a phenomenology-oriented “observational” technique.
Since we are now dealing with knowledge that has almost become lost, the recovery of the history of psychiatry and of national/regional practices plays a paramount role in bringing previous experiences to the foreground, that could assist in the pursuit of this everlasting objective. In other words, the history of psychiatry plays a critical and hermeneutical role, and particular national attempts and enterprises in psychopathology should be re-evaluated. Practice standardization is now an international goal, but should not lead to one-way, top-down unification from high-tech oriented research centers, as global mental health policies have already advised. A call for diverse, multiple and manifold cultural experiences in MSE is necessary for the future development and improvement in Psychiatric practice and research.
Limitations
This is a comprehensive review about Psychopathology Textbooks in Brazil and, although rigorous work has been done, it is possible that some critical publication is lacking due to methodological bias. Furthermore, because we dealt with vintage books, which have not yet been cataloged by electronic repositories, it is possible that old Brazilian Textbooks with some contradictory information were not found. Mainstream psychiatry has neglected psychiatric semiology, Mental State Examination, Mental Functions and its role in psychopathology standards and clinical practice, so it is possible that other authors have already answered the questions presented here, which was not picked up by our search strategy. This is a very complicated issue that needs to be addressed by a multi-professional team of linguists, anthropologist, science and medicine historians, and psychiatry practitioners. Further work may clarify and better elucidate these questions and issues.
Author Contributions
HR elaborated the search strategy, compiled the main data, and written the text. CE-L reviewed the compiled data, added most of historical data, and reviewed the main text. JL contributed for the elaboration of search strategy, delineated the main objective, and reviewed the final version of the text. MC contributed as main reviewer of data gathering, text writing, and conclusion.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Footnotes
References
1. Kasper DL, Braunwald E, Hauser S, Longo D, Jameson JL, Fauci AS. Harrison's Principles of Internal Medicine. 16th ed. New York, NY: McGraw-Hill Professional (2006).
3. Bickley LS, Bates B, Hoekelman RA. Bates' Guide to Physical Examination and History Taking. Philadelphia, PA: Lippincott Williams and Wilkins (1999). p. 789.
4. Bernard C. Introduction à L'étude de la Médecine Expérimentale Parm. Baillière: Claude Bernard (1865).
5. Feinstein AR. Boolean algebra and clinical taxonomy. N Engl J Med. (1963) 269:929–38. doi: 10.1056/NEJM196310312691801
6. Feinstein AR. Scientific methodology in clinical medicine. Ann Intern Med. (1964) 61:1162. doi: 10.7326/0003-4819-61-6-1162
7. Feinstein AR. An additional basic science for clinical medicine: IV. The development of clinimetrics. Ann Intern Med. (1983) 99:843. doi: 10.7326/0003-4819-99-6-843
8. Weisz G. The emergence of medical specialization in the nineteenth century. Bull Hist Med. (2003) 77:536–75. doi: 10.1353/bhm.2003.0150
9. Ramos Gorostiza P, Adan Manes J. Misunderstanding psychopathology as medical semiology: an epistemological enquiry. Psychopathology. (2011) 44:205–15. doi: 10.1159/000322692
10. Flexner A. Medical Education in the United States and Canada Bulletin Number Four. The Flexner Report. Carnegie Bulletin (1910). p. 364.
11. Rodrigues AMM, de Freitas CHA, Guerreiro M das G da S, Jorge MSB. Preceptorship in the perspective of comprehensive care: conversations with nurses. Rev Gaúcha Enferm. (2014) 35:106–12. doi: 10.1590/1983-1447.2014.02.43946
12. Foucault M, Gros F, Ewald F, Fontana A. Le Gouvernement de Soi et Des Autres: Cours au Collège de France, 1973-1974. Paris: Gallimard (2003).
14. Taggart C, O'Grady J, Stevenson M, Hand E, Mc Clelland R, Kelly C. Accuracy of diagnosis at routine psychiatric assessment in patients presenting to an accident and emergency department. Gen Hosp Psychiatry. (2006) 28:330–5. doi: 10.1016/j.genhosppsych.2006.05.002
15. Sartorius N, Janca A. Psychiatric assessment instruments developed by the World Health Organization. Soc Psychiatry Psychiatr Epidemiol. (1996) 31:55–69. doi: 10.1007/BF00801901
16. Helzer JE. The use of a structured diagnostic interview for routine psychiatric evaluations. J Nerv Ment Dis. (1981) 169:45–9. doi: 10.1097/00005053-198101000-00006
17. Chen Y, Li H, Li Y, Xie D, Wang Z, Yang F, et al. Resemblance of symptoms for major depression assessed at interview versus from hospital record review. PLoS ONE. (2012) 7:e28734. doi: 10.1371/journal.pone.0028734
18. Martin DC. The mental status examination. In: Walker HK, Hall WD, Hurst JW, editors. Clinical Methods: The History, Physical, and Laboratory Examinations. Boston, MA: Butterworths (1990). p. 1087.
19. Aboraya A, First MB. Point/counterpoint: the reliability of psychiatric diagnosis. Psychiatry. (2007) 4:22–5.
20. Souza JC, Guimarães LAM, Ballone GJ. Psicopatologia e Psiquiatria Básicas. 2nd ed. São Paulo: Vetor (2013). p. 314.
21. Cheniaux EJ. Manual de Psicopatologia. 4th edição. Rio de Janeiro: Guanabara Koogan (2011). p. 218.
22. Elkis H, Dalgalarrondo P. Exame psíquico. In: Louzã Neto MR, Elkis H, editors. Psiquiatria Básica. Porto Alegre: Artmed (2007). p. 712.
23. Parnas J, Sass LA, Zahavi D. Rediscovering psychopathology: the epistemology and phenomenology of the psychiatric object. Schizophr Bull. (2013) 39:270–7. doi: 10.1093/schbul/sbs153
24. Kendler KS, Parnas J. Philosophical Issues in Psychiatry III : The Nature and Sources of Historical Change. New York, NY: Oxford University press (2015).
26. Kendler KS, Parnas J. Philosophical Issues in Psychiatry: Explanation, Phenomenology, and Nosology. Baltimore, MD: Johns Hopkins University Press (2008). p. 424.
27. Tilley DH, Hoffman JA. Mental status examination: myth or method. Compr Psychiatry. (1981) 22:562–4. doi: 10.1016/0010-440X(81)90004-3
28. Jacob KS. Mental state examination: the elicitation of symptoms. Psychopathology. (2003) 36:1–5. doi: 10.1159/000069653
29. Blashfield RK. The Classification of Psychopathology : Neo-Kraepelinian and Quantitative Approaches. New York, NY: Plenum Press (1984). p. 354.
30. Estellita-lins C. Visibilidade e conhecimento: investigando a semiologia psiquiátrica. In: Rodrigues ACT, Streb LG, Viotti Daker M, Domont De Serpa Junior O, editors. Psicopatologia Conceitual. 1st ed. São Paulo: Roca (2012). p. 73–102.
31. Cheniaux E. Psicopatologia descritiva: existe uma linguagem comum? Rev Bras Psiquiatr. (2005) 27:157–62. doi: 10.1590/S1516-44462005000200017
32. Viotti Daker M. Revisitando nobre de melo: conceitos em psiquiatria. In: Rodrigues ACT, Streb LG, Viotti Daker M, Serpa Junior OD, editors. Psicopatologia Conceitual. 1st ed. São Paulo: Roca (2012) 31–50.
33. Andreasen NC. DSM and the death of phenomenology in america: an example of unintended consequences. Schizophr Bull. (2007) 33:108–12. doi: 10.1093/schbul/sbl054
34. Parnas J. A disappearing heritage: the clinical core of schizophrenia. Schizophr Bull. (2011) 37:1121–30. doi: 10.1093/schbul/sbr081
35. Aragona M. The impact of translational neuroscience on revisiting psychiatric diagnosis: state of the art and conceptual analysis. Balkan Med J. (2017) 34:487–92. doi: 10.4274/balkanmedj.2017.1190
36. Rodrigues ACT, Banzato CEM. Validade: um exame de seu significado na nosologia psiquiátrica. In: Rodrigues ACT, Streb LG, Daker MV, Serpa Junior OD, editors. Psicopatologia Conceitual. São Paulo: Roca (2012). p. 115–30.
38. Peixoto AJ. Birth, death, and resurrection of the physical examination: clinical and academic perspectives on bedside diagnosis. Yale J Biol Med. (2001) 74:221–8.
39. American Psychiatric Association. The American Psychiatric Association Practice Guidelines for the Psychiatric Evaluation of Adults. Practice Guidelines. Arlington, TX: American Psychiatric Association (2015).
40. American Psychiatric Association. In: Diagnostic and Statistical Manual of Mental Disorders. 4th Edition. Text Revision (DSM-IV-TR). Arlington, TX: American Psychiatric Association (2000). p. 943.
41. Pan American Health Organization. ClassificaÇão Estatística Internacional de DoenÇas e Problemas Relacionados à Saúde : Décima Revisão. 7th ed. São Paulo: Edusp (1999).
42. American Psychiatric Association. DSM-5 Task Force. In: Diagnostic and Statistical Manual of Mental Disorders : DSM-5. 5th ed. Arlington, VA; Washington, DC: American Psychiatric Association (2013). p. 947.
43. Banzato CEM. Assigning things to their proper class: taxonomic issues and trends in psychiatry. Rev Latinoam Psicopatol Fundam. (2002) 5:11–9. doi: 10.1590/1415-47142002001002
44. Ludwik F. Genesis and Development of a Scientific Fact. Chicago, IL: The University of Chicago Press (1979).
46. Dalgalarrondo P. Psicopatologia e Semiologia dos Transtornos Mentais. Porto Alegre: Artes Medicas (2000).
48. Fontenelle LF, Mendlowicz MV. Manual de Psicopatologia Descritiva e Semiologia Psiquiátrica. 1st ed. Rio de Janeiro: Revinter (2017). p. 123.
50. de Miranda-Sá LS Jr. Fundamentos de Psicopatologia. 1st ed. Rio de Janeiro: Atheneu Editora (1988). p. 352.
51. Leme Lopes J. Diagnóstico em Psiquiatria. 1st ed. Rio de Janeiro: Cultura Médica (1980). p. 235.
53. Paim I. Curso de Psicopatologia. 11th ed. São Paulo: Editora Pedagógica e Universitária (1993). p. 285.
54. Del Sant R, Marchetti RL, Tavares H, Wang Y-P, Cordás TA. Avaliação psicopatológica ao longo da vida. In: Forlenza OV, Miguel EC, editors. Compêndio de Clínica Psiquiátrica. 1a. Barueri: Manole (2012). p. 708.
56. Aboraya A, Nasrallah H, Muvvala S, El-Missiry A, Mansour H, Hill C, et al. The standard for clinicians' interview in psychiatry (SCIP): a clinician-administered tool with categorical, dimensional, and numeric output-conceptual development, design, and description of the SCIP. Innov Clin Neurosci. (2016) 13:31–77.
57. Wilson M. DSM-III and the transformation of American psychiatry: a history. Am J Psychiatry. (1993) 150:399–410. doi: 10.1176/ajp.150.3.399
58. Moreira J. Notícia sobre a evolução da assistência a alienados no Brasil (1905). Rev Latinoam Psicopatol Fundam. (2011) 14:728–68. doi: 10.1590/S1415-47142011000400012
59. Galdini AM, Oda R, Dalgalarrondo P. O início da assistência aos alienados no Brasil ou importância e necessidade de estudar a história da psiquiatria. Rev Latinoam Psicopat Fund. (2004) 7:128–41. doi: 10.1590/1415-47142004001012
60. Venacio ATA. As Fases de Juliano Moreira: luzes e Sombras Sobre seu Acervo Pessoal e Suas Publicações. Rio de Janeiro: Estudos Históricos (2005). Available online at: http://bibliotecadigital.fgv.br/ojs/index.php/reh/article/viewFile/2241/1380
61. Coelho Edler F, Edler FC. A medicina brasileira no século XIX: um balanço historiográfico. Asclepio. (1998) 50:169–86.
62. Oda A, Dalgalarrondo P. Juliano Moreira : um psiquiatra negro frente ao racismo científico. Rev Bras Psiquiatr. (2000) 22:178–9. doi: 10.1590/S1516-44462000000400007
63. Ana Teresa A. Venancio. Doença mental, raça e sexualidade nas teorias psiquiátricas de Juliano Moreira. Physis Rev Saúde Coletiva. (1991) 14:283–305.
65. Dalgalarrondo P. Psicopatologia e Semiologia dos Transtornos Mentais. 2a edição. Porto Alegre: Artmed (2008). p. 440.
66. Stanghellini G, Fiorillo A. Five reasons for teaching psychopathology. World Psychiatry. (2015) 14:107–8. doi: 10.1002/wps.20200
67. Mota A, da Marinho MGSM. História da Psiquiatria: Ciência, Práticas e Tecnologias de Uma Especialidade Médica. São Paulo: USP; Faculdade de Medicina: UFABC; Universidade federal do ABC: CD.G Casa de Soluções e Editora (2012).
68. Monarcha C. Escola “Pacheco e Silva” anexada ao Hospital de Juqueri (1929-1940). Bol Acad Paul Psicol. (2010) 30:7–20. Available online at: http://pepsic.bvsalud.org/scielo.php?script=sci_arttext&pid=S1415-711X2010000100002
69. Ribeiro PS. Um Médico, Uma Ideia e um Hospital: Dr. Franco da Rocha e a Concepção do Juqueri. História da Psiquiatria: Ciência, Práticas e Tecnologias Uma Especialidade Médica. São Paulo: USP (2012). p. 145–58.
70. Cheniaux E. Manual de Psicopatologia. 1st ed. Rio de Janeiro: Grupo Gen - Guanabara Koogan (2000). p. 235.
71. Kawa S, Giordano J. A brief historicity of the Diagnostic and Statistical Manual of Mental Disorders: Issues and implications for the future of psychiatric canon and practice. Philos Ethics Human Med. (2012) 7:2. doi: 10.1186/1747-5341-7-2
72. Rosenberger P, Lewine R. Conceptual issues in the choice of a structured psychiatric interview. Compr Psychiatry. (1982) 23:116–23. doi: 10.1016/0010-440X(82)90056-6
74. Broadbent M, Moxham L, Dwyer T. The development and use of mental health triage scales in Australia. Int J Ment Health Nurs. (2007) 16:413–21. doi: 10.1111/j.1447-0349.2007.00496.x
75. Broadbent M, Creaton A, Moxham L, Dwyer T. Review of triage reform: the case for national consensus on a single triage scale for clients with a mental illness in Australian emergency departments. J Clin Nurs. (2010) 19:712–5. doi: 10.1111/j.1365-2702.2009.02988.x
76. Wing JK. SCAN: Schedules fonr Clinical Assessment in Neuropsychiatry. Arch Gen Psychiatry. (1990) 47:589–93. doi: 10.1001/archpsyc.1990.01810180089012
77. Sheehan DV, Lecrubier Y, Sheehan KH, Amorim P, Janavs J, Weiller E, et al. The Mini-International Neuropsychiatric Interview (M.I.N.I.): the development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J Clin Psychiatry. (1998) 59(Suppl. 2):22–33; quiz: 34–57.
78. First MB, Williams JBW. SCID-5-CV: Structured Clinical Interview for DSM-5 Disorders: Clinician Version. Arlington, TX: American Psychiatric Association Publishing (2016).
79. Brittain PJ, Lobo SEM, Rucker J, Amarasinghe M, Anilkumar APP, Baggaley M, et al. Harnessing clinical psychiatric data with an electronic assessment tool (opcrit+): the utility of symptom dimensions. PLoS ONE. (2013) 8:e58790. doi: 10.1371/journal.pone.0058790
80. Häfner H. Descriptive psychopathology, phenomenology, and the legacy of Karl Jaspers. Dialogues Clin Neurosci. (2015) 17:19–29.
81. Aboraya A, Rankin E, France C, El-Missiry A, John C. The reliability of psychiatric diagnosis revisited: the clinician's guide to improve the reliability of psychiatric diagnosis. Psychiatry. (2006) 3:41–50.
82. Bongiovi-Garcia ME, Merville J, Almeida MG, Burke A, Ellis S, Stanley BH, et al. Comparison of clinical and research assessments of diagnosis, suicide attempt history and suicidal ideation in major depression. J Affect Disord. (2009) 115:183–8. doi: 10.1016/j.jad.2008.07.026
83. Gabriel A. Problem-solving strategies in psychiatry: differences between experts and novices in diagnostic accuracy and reasoning. Adv Med Educ Pract. (2013) 4:11. doi: 10.2147/AMEP.S38372
84. Kreitman N, Sainsbury P, Morrissey J, Towers J, Scrivener J. The reliability of psychiatric assessment: an analysis. Br J Psychiatry. (1961) 107:887–908. doi: 10.1192/bjp.107.450.887
85. Conselho Federal de Medicina. Resolução N° 2.153, de 30 de Setembro de 2016. Brasilia (2017). p. 87–8.
Keywords: mental state examination, psychopathology, descriptive psychopathology, history of medicine, psychiatry, diagnosis, diagnosis technics and procedures
Citation: Rocha Neto HG, Estellita-Lins CE, Lessa JLM and Cavalcanti MT (2019) Mental State Examination and Its Procedures—Narrative Review of Brazilian Descriptive Psychopathology. Front. Psychiatry 10:77. doi: 10.3389/fpsyt.2019.00077
Received: 20 July 2018; Accepted: 04 February 2019;
Published: 05 March 2019.
Edited by:
Diogo Telles-Correia, Universidade de Lisboa, PortugalReviewed by:
Mauricio Viotti Daker, Federal University of Minas Gerais, BrazilRicardo de Oliveira-Souza, Instituto D'Or de Pesquisa e Ensino (IDOR), Brazil
Copyright © 2019 Rocha Neto, Estellita-Lins, Lessa and Cavalcanti. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Helio Gomes Rocha Neto, aGdyb2NoYW5ldG9AZ21haWwuY29t