 John A. Engh1*
John A. Engh1* Jens Egeland1,2
Jens Egeland1,2 Ole A. Andreassen3,4
Ole A. Andreassen3,4 Gry Bang-Kittilsen1
Gry Bang-Kittilsen1 Therese T. Bigseth1
Therese T. Bigseth1 Tom L. Holmen1
Tom L. Holmen1 Egil W. Martinsen4Jon Mordal1Eivind Andersen5
Egil W. Martinsen4Jon Mordal1Eivind Andersen5- 1Division of Mental Health and Addiction, Vestfold Hospital Trust, Tønsberg, Norway
- 2Department of Psychology, University of Oslo, Oslo, Norway
- 3NORMENT, KG Jebsen Centre for Psychosis Research, Oslo, Norway
- 4Division of Mental Health and Addiction, Institute of Clinical Medicine, University of Oslo, Oslo, Norway
- 5Faculty of Humanities, Sports and Educational Science, University of South-Eastern Norway, Horten, Norway
People with schizophrenia often have an unhealthy sedentary lifestyle with low level of physical activity and poor cardiorespiratory fitness—an important predictor of cardiovascular disease. We investigated the relations between cardiorespiratory fitness and both sedentary time and different aspects of physical activity, such as daily steps, light intensity physical activity, and moderate-to-vigorous physical activity. Using accelerometer as an objective measure of sedentary time and physical activity we estimated their relations to cardiorespiratory fitness in 62 patients with schizophrenia with roughly equal gender distribution, mean age of 36 and 15 years illness duration. We found a significant association between daily steps and cardiorespiratory fitness when accounting for gender, age, sedentary time, light intensity physical activity, and respiratory exchange ratio (maximal effort). Moderate-to-vigorous physical activity was not significantly associated with cardiorespiratory fitness. In conclusion, the amount of steps throughout the day contributes to cardiorespiratory fitness in people with schizophrenia, independently of light intensity physical activity and sedentary time. We did not find a significant relationship between moderate-to-vigorous physical activity and cardiorespiratory fitness. This may have implications for the choice of strategies when helping patients with schizophrenia improve their cardiorespiratory fitness.
Introduction
People with schizophrenia are prone to overweight, diabetes and chronic metabolic disease (1) and often have a deleterious lifestyle, including low levels of moderate-to-vigorous physical activity (MVPA) and high levels of sedentary time (2). The average life expectancy is 15–20 years shorter than the general population, and cardiovascular disease (CVD) is the largest contributing factor to the increase in mortality (3). Low cardiorespiratory fitness (CRF) is a strong independent risk factor for all-cause mortality (4, 5) associated with low life expectancy and increased risk for CVD in the general population (4–6) and in schizophrenia (7, 8). Thus, knowledge on how to effectively improve CRF in schizophrenia is urgently needed. The beneficial effects of MVPA and the smaller effects of light intensity physical activity (PA) on CRF in the general population are well documented (9, 10). Less is known about the relations in people with schizophrenia. Another aspect of interest is the extent sedentary time influences CRF in the patient group. Sedentary time refers to the time spent for any duration or in any context in sedentary behaviors, defined as any waking behavior characterized by an energy expenditure equal to or less than 1.5 the resting metabolic rate while in a sitting, reclining or lying posture (11–13). Recent studies suggest that sedentary time is an important determinant of CRF levels, which is independent of physical activity (14, 15) A third aspect of interest is the total PA level. The number of daily steps have been associated with positive health effects in the general population (16) and in individuals with high cardiovascular risk (17). Studies on healthy overweight persons have indicated that reduced total daily PA causes reduction in CRF as well as worsening of other cardiometabolic health outcomes (18, 19). Increasing the total PA by walking (i.e., daily steps), as well as breaking the sedentary habit could be a path to improved CRF distinct from light intensity PA and MVPA (20, 21). It is not known whether the potential health effects facilitated by daily steps in people with schizophrenia are cumulative, increasing with the amount of total PA. The aim of the current study was to examine whether objectively assessed light intensity PA, MVPA, total daily steps, and sedentary time, exert independent influences on CRF in people with schizophrenia.
Materials and Methods
Participants
Sixty-two patients were recruited from the main study Effects of physical activity in psychosis (EPHAPS) from August 2014 through September 2016 in catchment area-based and publicly funded outpatient psychiatric clinics in Vestfold County, Norway. A subgroup of the patients was referred from primary health care to the outpatient clinics for specific participation in the project. Patients diagnosed with schizophrenia spectrum disorder established using SCID I (22) who were aged 18–67 and understood and spoke a Scandinavian language were eligible for the study. Interviews were conducted by a clinical psychologist or a specialist in psychiatry. For further details on study design see Engh et al. (23) and on patient recruitment, study eligibility and data collection see Engh et al. (23) and Andersen et al. (24). All except one patient received antipsychotic treatment. Demographic and clinical characteristics are presented in Table 1.
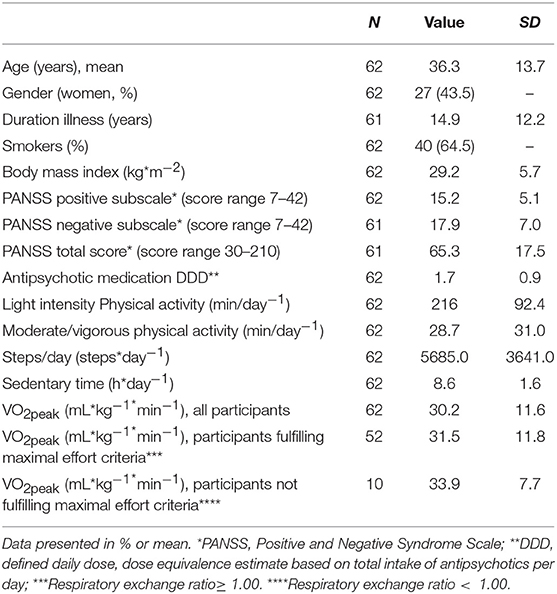
Table 1. Demographic and clinical characteristics, physical activity and sedentary time of the participants.
Assessments
For further details on measurement of physical activity, sedentary time, and oxygen uptake see (24). PA and sedentary time was assessed using the ActiGraph GT3X+ (ActiGraph, LLC, Pensacola, FL, USA) worn over the left hip while awake for four consecutive days. Analyses were restricted to participants who wore the accelerometer for a minimum of 10 h per day for 2 days or more. To identify different intensities of PA, count thresholds corresponding to the energy cost of the given intensity were applied to the data set. Sedentary time was defined as all activity < 100 counts per minute (CPM), a threshold that corresponds with sitting, reclining, or lying down (25). Light intensity PA was defined as 100–2019 CPM, moderate as 2020–5998 CPM, and vigorous as CPM ≥ 5999 (26). The amount of minutes per day at different intensities was based on summing the time where the activity count met the criteria for the specific intensity. Cardiorespiratory fitness (CRF) was operationalized as VO2peak measuring the highest oxygen uptake in a maximum exercise test on a treadmill (Woodway, Würzburg, Germany). Some individuals may fail to reach true VO2max, and for the sake of conservative reporting, we therefore use the term VO2peak (mL*kg−1*min−1). We used a modified Balke protocol (27), where speed was held constant at 5 km·h−1 and the inclination angle was increased by one degree every minute until exhaustion within 6–12 min. Gas exchange was continuously sampled in a mixing chamber every 30 s by breathing into a two-way breathing valve (2700 series, Hans Rudolph Inc., Kansas City, USA). The breathing valve was connected to a Jaeger Oxycon Pro used to analyze the oxygen and carbon content. Maximal effort was assessed by the respiratory exchange ratio (RER). Participants reached the criteria when RER ≥ 1.00. Participants' psychotropic drugs prescription was presented as defined daily dose (DDD) based on approved dose recommendations. DDD provides a rough estimate of participants' drugs consumption utilizing the assumed average maintenance dose per day for each specific drug used independent of dosage form for its main indication on adults (i.e., schizophrenia for antipsychotics). For example, the DDDs for chlorpromazine and risperidone are 300 mg and 5 mg respectively. DDD were calculated in accordance with guidelines from the World Health Organization Collaborating Center for Drug Statistics Methodology (http://www.whocc.no/atcdd). Information on smoking, illness duration and medication was obtained through interview and the use of hospital records. Weight was measured without shoes in light clothing by a SECA electronic scale to the nearest 0.5 kg. Height was measured without shoes with a transportable stadiometer and set to the nearest 0.5 cm.
Statistics
Variables that were not normally distributed (steps/day; MVPA) were log-transformed in the statistical analyses. Multiple regression analyses (all covariates entered concomitantly in the model) were employed to examine the relationships between independent variables and VO2peak. VO2peak was used to represent the outcome, cardiorespiratory fitness. Selection of variables in the regression model was based on Pearson correlation tests between VO2peak, measures of physical activity and sedentary time and other variables with assumed clinical importance. Correlation coefficients are shown in Table 2. Due to high correlation between the independent variables MVPA and steps/day (r = 0.73) two separate regression analyses were employed using each of these two independent variables and all other selected variables. The independent variable steps/day, and not MVPA, was included in the final regression model. When testing for multicollinearity correlations between independent variables were sufficiently low (r < 0.70) and the variation inflation factor fell within the criteria (VIF < 10). All statistical analyses were performed using IBM SPSS (Statistical Pack- age for the Social Sciences for Windows, version 24, IBM, Inc., Chicago, IL, USA).
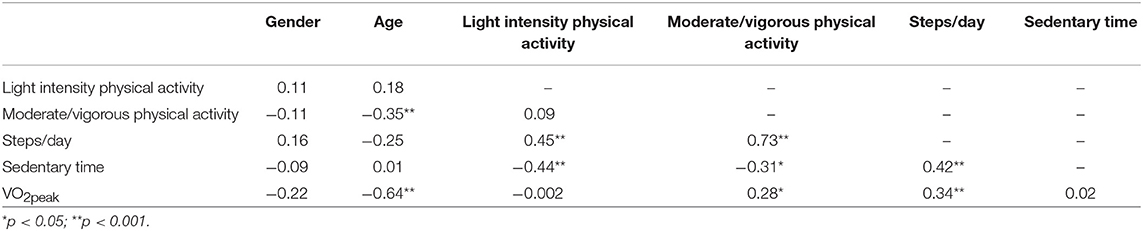
Table 2. Correlation coefficients between physical activity measures, sedentary time, and VO2peak.
Results
As shown in Table 3, VO2peak was significantly associated with gender, age and steps/day when all other covariates were controlled. Regression coefficients and standard errors can be found in the table. In a separate regression analysis encompassing MVPA in addition to the independent variables gender, age, light intensity PA and sedentary time, MVPA did not contribute to VO2peak. Eighty-four percent of the participants obtained the criteria for RER. The main results were unaltered in a multiple regression analysis with participants attaining RER ≥ 1.00.
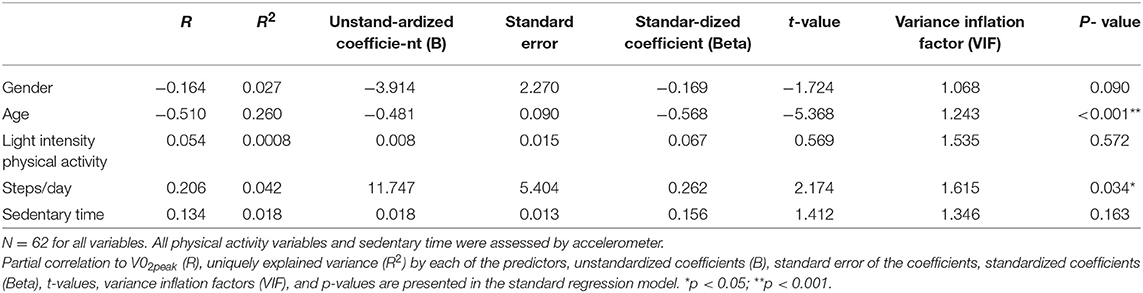
Table 3. Regression analysis presenting explained variance in VO2peak.
Discussion
The main finding in the current study was that total daily steps was significantly associated with VO2peak, independently of light intensity physical activity, the amount of time spent sedentary and maximal effort during testing of oxygen consumption. Moderate-to-vigorous physical activity was not significantly associated with VO2peak. Our findings suggest that the amount of daily walking activity is of importance for patients with schizophrenia by contributing to the established health indicator VO2peak. As a measure of the total physical activity daily steps differs from the measures of physical activity at defined levels of activity. VO2peak may reflect the individual's participation in physical activity of different intensity. The influence of physical activity at specific intensity levels on VO2peak has been focus of previous research. A meta-regression of moderators of physical activity showed that low VO2peak was associated with low levels of moderate-to-vigorous physical activity (2). In a recent study of patients with psychosis using a 6 min-walking test as a proxy for CRF, both MVPA and total PA showed significant moderate positive correlations with CRF (28). The findings in the current study indicate that repeated or prolonged sequences of walking could have favorable health effects in schizophrenia. However, the current study investigating the relations between VO2peak and physical activity at different intensity levels, sedentary behavior and daily steps in patients with schizophrenia needs to be replicated.
A comparison of studies using objective assessments of PA and sedentary behavior with studies based on self-reports suggests that people with schizophrenia underestimate the amount of sedentary time and overestimate the duration of their PA (2). The objective assessment of PA is a strength of the current study. A limitation is the cross sectional design without the opportunity to draw inferences concerning causal effects. The encouragement of repeated indoor, as well as outdoor physical activity, could be organized according to personal preference and implemented as part of treatment in community-based mental health care. In conclusion, the amount of steps throughout the day contributes to VO2peak in people with schizophrenia, independently of light intensity physical activity and sedentary time. Moderate-to-vigorous physical activity was not significantly associated with VO2peak. This may have implications for the choice of strategies when helping patients with schizophrenia improve their cardiorespiratory fitness.
Ethics Statement
This study was carried out in accordance with the recommendations of Regional Ethics Committee of Southern and Eastern Norway (REK Sør-Øst) under file number 2014/372/REK Sør-Øst C with written informed consent from all subjects. All subjects gave written informed consent in accordance with the Declaration of Helsinki. The protocol was approved by the Regional Ethics Committee of Southern and Eastern Norway (REK Sør-Øst).
Author Contributions
JAE and EA conceived the study. JAE, JE, EA, and JM acquired funding and approval of the ethics committee. These four researchers, in addition to EWM and OAA, contributed to study design. TLH, TTB, GB-K and JM carried out parts of the clinical testing. The manuscript has been drafted by JAE, EA, JE, OAA, GB-K, TTB, TLH, EWM, and JM. All authors read, worked on and approved the final manuscript.
Funding
The main study (EPHAPS) has received funding from Vestfold Hospital Trust, South-Eastern Norway Regional Health Authority, Norwegian Extra Foundation for Health and Rehabilitation through EXTRA funds, Norwegian Research network in Severe Mental Illness (NORSMI), NORMENT/KG Jebsen Center for Psychosis Research, Torgeir Lindvik's Trust, and Civitan International.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The investigators would like to thank the patients participating in the study, and the members of the EPHAPS study group who participated in the data collection and data management. We also give special thanks to Helge Bjune, Ole-Jakob Bredrup, Ellen Gurine Færvik, Jan-Freddy Hovland, Camilla Lahn-Johannessen, and Bjørn-Einar Oscarsen for conducting the measurements.
References
1. Ringen PA, Engh JA, Birkenaes AB, Dieset I, Andreassen OA. Increased mortality in schizophrenia due to cardiovascular disease - a non-systematic review of epidemiology, possible causes, and interventions. Front Psychiatry (2014) 5:137. doi: 10.3389/fpsyt.2014.00137
2. Vancampfort D, Firth J, Schuch FB, Rosenbaum S, Mugisha J, Hallgren M, et al. Sedentary behavior and physical activity levels in people with schizophrenia, bipolar disorder and major depressive disorder: a global systematic review and meta-analysis. World Psychiatry (2017) 16:308–15. doi: 10.1002/wps.20458
3. Correll CU, Solmi M, Veronese N, Bortolato B, Rosson S, Santonastaso P, et al. Prevalence, incidence and mortality from cardiovascular disease in patients with pooled and specific severe mental illness: a large-scale meta-analysis of 3,211,768 patients and 113,383,368 controls. World Psychiatry (2017) 16:163–80. doi: 10.1002/wps.20420
4. Blair SN, Kampert JB, Kohl HW III, Barlow CE, Macera CA, Paffenbarger RS, et al. Influences of cardiorespiratory fitness and other precursors on cardiovascular disease and all-cause mortality in men and women. JAMA (1996) 276:205–10. doi: 10.1001/jama.1996.03540030039029
5. Lee DC, Sui X, Artero EG, Lee IM, Church TS, McAuley PA, et al. Long-term effects of changes in cardiorespiratory fitness and body mass index on all-cause and cardiovascular disease mortality in men: the Aerobics Center Longitudinal Study. Circulation (2011) 124:2483–90. doi: 10.1161/CIRCULATIONAHA.111.038422
6. Kodama S, Saito K, Tanaka S, Maki M, Yachi Y, Asumi M, et al. Cardiorespiratory fitness as a quantitative predictor of all-cause mortality and cardiovascular events in healthy men and women: a meta-analysis. JAMA (2009) 301:2024–35. doi: 10.1001/jama.2009.681
7. Hayes JF, Marston L, Walters K, King MB, Osborn DPJ. Mortality gap for people with bipolar disorder and schizophrenia, UK-based cohort study 2000–2014. Br J Psychiatry. (2017) 211:175–81. doi: 10.1192/bjp.bp.117.202606
8. Samaras K, Correll CU, Curtis J. Premature mortality and schizophrenia-the need to heal right from the start. JAMA Psychiatry (2016) 73:535–6. doi: 10.1001/jamapsychiatry.2015.3432
9. Oja P. Dose response between total volume of physical activity and health and fitness. Med Sci Sports Exerc. (2001) 33 (6 Suppl):S428–37; discussion S452–3.
10. McGuire KA, Ross R. Incidental physical activity is positively associated with cardiorespiratory fitness. Med Sci Sports Exerc. (2011) 43:2189–94. doi: 10.1249/MSS.0b013e31821e4ff2
11. Yates T, Wilmot EG, Davies MJ, Gorely T, Edwardson C, Biddle S, et al. Sedentary behavior: what's in a definition? Am J Prev Med. (2011) 40:e33–4; author reply e34. doi: 10.1016/j.amepre.2011.02.017
12. Pate RR, O'Neill JR, Lobelo F. The evolving definition of “sedentary.” Exerc Sport Sci Rev. (2008) 36:173–8. doi: 10.1097/JES.0b013e3181877d1a
13. Tremblay MS, Aubert S, Barnes JD, Saunders TJ, Carson V, Latimer-Cheung AE, et al. Sedentary Behavior Research Network (SBRN) - terminology consensus project process and outcome. Int J Behav Nutr Phys Act. (2017) 14:75. doi: 10.1186/s12966-017-0525-8
14. Kulinski JP, Khera A, Ayers CR, Das SR, de Lemos JA, Blair SN, et al. Association between cardiorespiratory fitness and accelerometer-derived physical activity and sedentary time in the general population. Mayo Clin Proc. (2014) 89:1063–71. doi: 10.1016/j.mayocp.2014.04.019
15. Bouchard C, Blair SN, Katzmarzyk PT. Less sitting, more physical activity, or higher fitness? Mayo Clin Proc. (2015) 90:1533–40. doi: 10.1016/j.mayocp.2015.08.005
16. Dwyer T, Pezic A, Sun C, Cochrane J, Venn A, Srikanth V, et al. Objectively measured daily steps and subsequent long term all-cause mortality, the tasped prospective cohort study. PLoS ONE (2015) 10:e0141274. doi: 10.1371/journal.pone.0141274
17. Yates T, Haffner SM, Schulte PJ, Thomas L, Huffman KM, Bales CW, et al. Association between change in daily ambulatory activity and cardiovascular events in people with impaired glucose tolerance (NAVIGATOR trial): a cohort analysis. Lancet (2014) 383:1059–66. doi: 10.1016/S0140-6736(13)62061-9
18. Olsen RH, Krogh-Madsen R, Thomsen C, Booth FW, Pedersen BK. Metabolic responses to reduced daily steps in healthy nonexercising men. JAMA (2008) 299:1261–3. doi: 10.1001/jama.299.11.1259
19. Krogh-Madsen R, Thyfault JP, Broholm C, Mortensen OH, Olsen RH, Mounier R, et al. A 2-wk reduction of ambulatory activity attenuates peripheral insulin sensitivity. J Appl Physiol. (1985) (2010) 108:1034–40. doi: 10.1152/japplphysiol.00977.2009
20. Bjørgaas M, Vik JT, Saeterhaug A, Langlo L, Sakshaug T, Mohus RM, et al. Relationship between pedometer-registered activity, aerobic capacity and self-reported activity and fitness in patients with type 2 diabetes. Diabetes Obes Metab. (2005) 7:737–44. doi: 10.1111/j.1463-1326.2004.00464.x
21. Cao ZB, Miyatake N, Higuchi M, Ishikawa-Takata K, Miyachi M, Tabata I. Prediction of VO2max with daily step counts for Japanese adult women. Eur J Appl Physiol. (2009) 105:289–96. doi: 10.1007/s00421-008-0902-8
22. Spitzer RL, Williams JB, Gibbon M, First MB. The structured clinical interview for DSM-III-R (SCID) I: History, rationale, and description. Arch Gen Psychiatry (1992) 49:624–9.
23. Engh JA, Andersen E, Holmen TL, Martinsen EW, Mordal J, Morken G, et al. Effects of high-intensity aerobic exercise on psychotic symptoms and neurocognition in outpatients with schizophrenia: study protocol for a randomized controlled trial. Trials (2015) 16:557. doi: 10.1186/s13063-015-1094-2
24. Andersen E, Holmen TL, Egeland J, Martinsen EW, Bigseth TT, Bang-Kittilsen G, et al. Physical activity pattern and cardiorespiratory fitness in individuals with schizophrenia compared with a population-based sample. Schizophr Res. (2018) 201:98–104. doi: 10.1016/j.schres.2018.05.038
25. Matthews CE, Chen KY, Freedson PS, Buchowski MS, Beech BM, Pate RR, et al. Amount of time spent in sedentary behaviors in the United States, 2003–2004. Am J Epidemiol. (2008) 167:875–81. doi: 10.1093/aje/kwm390
26. Troiano RP. A timely meeting: objective measurement of physical activity. Med Sci Sports Exerc. (2005) 37(11 Suppl.):S487–9. doi: 10.1249/01.mss.0000185473.32846.c3
27. Balke B, Ware RW. An experimental study of physical fitness of air force personnel. U S armed forces Med J. (1959) 10:675–88.
Keywords: schizophrenia, lifestyle, cardiovascular disease, daily steps, physical activity, cardiorespiratory fitness, accelerometer, sedentary time
Citation: Engh JA, Egeland J, Andreassen OA, Bang-Kittilsen G, Bigseth TT, Holmen TL, Martinsen EW, Mordal J and Andersen E (2019) Objectively Assessed Daily Steps—Not Light Intensity Physical Activity, Moderate-to-Vigorous Physical Activity and Sedentary Time—Is Associated With Cardiorespiratory Fitness in Patients With Schizophrenia. Front. Psychiatry 10:82. doi: 10.3389/fpsyt.2019.00082
Received: 08 July 2018; Accepted: 06 February 2019;
Published: 26 February 2019.
Edited by:
Philip B. Ward, University of New South Wales, AustraliaReviewed by:
Bartlomiej Stanczykiewicz, Wroclaw Medical University, PolandJavier Bueno-Antequera, Universidad Pablo de Olavide, Spain
Copyright © 2019 Engh, Egeland, Andreassen, Bang-Kittilsen, Bigseth, Holmen, Martinsen, Mordal and Andersen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: John A. Engh, am9obi5lbmdoQG1lZGlzaW4udWlvLm5v