 Thomas W. Scheewe1,2*
Thomas W. Scheewe1,2* Frederike Jörg3,4
Frederike Jörg3,4 Tim Takken5
Tim Takken5 Jeroen Deenik6
Jeroen Deenik6 Davy Vancampfort7,8
Davy Vancampfort7,8 Frank J. G. Backx9Wiepke Cahn1
Frank J. G. Backx9Wiepke Cahn1- 1Department of Psychiatry, Rudolf Magnus Institute for Neuroscience, University Medical Center Utrecht, Utrecht, Netherlands
- 2Department of Human Movement and Education, Windesheim University of Applied Sciences, Zwolle, Netherlands
- 3Rob Giel Research Center, University Center of Psychiatry, University Medical Center Groningen, University of Groningen, Groningen, Netherlands
- 4Research Department, GGZ Friesland (Friesland Mental Health Services), Leeuwarden, Netherlands
- 5Child Development and Exercise Center, Wilhelmina Children's Hospital, University Medical Center Utrecht, Utrecht, Netherlands
- 6GGz Centraal, Amersfoort, Netherlands
- 7University Psychiatric Center KU Leuven, Leuven, Belgium
- 8Department of Rehabilitation Sciences, KU Leuven, Leuven, Belgium
- 9Department of Rehabilitation, Physical Therapy Science and Sports, Rudolf Magnus Institute for Neuroscience, University Medical Center Utrecht, Utrecht, Netherlands
Introduction: The aim of this study was to objectively assess time spent in physical activity (PA) and sedentary behavior (SB) in patients with schizophrenia compared to healthy controls matched for age, gender and socioeconomic status. Associations between both PA and cardiorespiratory fitness (CRF) and mental and physical health parameters in patients with schizophrenia were examined.
Materials and Methods: Moderate and vigorous PA (MVPA), moderate PA, vigorous PA, total and active energy expenditure (TEE and AEE), number of steps, lying down and sleeping time was assessed with SenseWear Pro-2 body monitoring system for three 24-h bouts in patients with schizophrenia (n = 63) and matched healthy controls (n = 55). Severity of symptoms (Positive and Negative Syndrome Scale and Montgomery and Åsberg Depression Rating Scale), CRF (peak oxygen uptake, VO2peak), body mass index (BMI), and metabolic syndrome were assessed.
Results: Patients with schizophrenia performed less MVPA and moderate activity had lower TEE and AEE, spent more time per day lying down and sleeping, and had poorer CRF compared to healthy controls. The amount of MVPA, but especially CRF was associated with severity of negative symptoms in patients with schizophrenia. Only CRF was associated with BMI.
Discussion: The current data offer further evidence for interventions aiming to increase physical activity and decrease sedentary behavior. Given strong associations of CRF with both negative symptoms and BMI, treatment aimed at CRF-improvement may prove to be effective.
Introduction
The premature mortality risk in patients with schizophrenia is two to three times higher compared to the general population leading to a 7–20 year reduction in life expectancy (1–3), mainly due to cardiovascular disease (4, 5). The increased cardio-metabolic risk is partly attributable to side effects of antipsychotic medication such as weight gain, dyslipidemia, and diabetes mellitus (4, 6).
Three recent meta-analyses show patients with schizophrenia engage in less physical activity (PA) (7), have high levels of sedentary behavior (SB) in their waking day (8), and have low cardiorespiratory fitness (CRF)-levels (9). The majority of the included studies used self-report to assess PA (7) which, due to recall errors and social desirability bias, has limited validity (10, 11). Illustrative, whereas no difference in PA was found using self-report measurement, accelerometry showed a large reduction of PA in patients with schizophrenia compared to healthy controls (12). As for SB, a meta-analysis demonstrated that patients with psychosis spend 11 h of their waking day being sedentary. Again, objective measurement of SB demonstrated significantly higher levels of SB compared to self-report measurements (8).
In patients with psychosis, a limited number of studies have suggested that high levels of SB and low levels of PA are associated with an increased cardio-metabolic risk [e.g., (13, 14)]. These studies did not take CRF into account, and most of these studies assessed SB and PA using self-report (10, 11). One study examined independent associations of objectively measured SB and PA with cardio-metabolic risk in inpatients with schizophrenia as well as in age/sex/body mass index-matched healthy controls (15), but failed to take CRF into account. As far as we know, only one study (16) did include CRF when investigating associations between SB and PA with cardio-metabolic risk factors in patients with psychosis. This study showed that SB is, independently of PA and CRF, associated with the individual risk factors waist and fasting blood glucose. Strikingly, CRF, even when controlled for SB and PA, remained significantly associated with clustered cardio-metabolic risk and the individual risk factor waist. The study by Bueno-Antequera et al. (16) is mildly hampered by some limitations. For instance, they did not include healthy controls, measured CRF with a submaximal test instead of a “gold standard” cardiopulmonary exercise testing (CPET), thus limiting the validity of its results (17), and had a small sample of size of outpatients, predominantly men. Therefore, they call for more research, as well as the use of (gold standard) objective measures.
The aim of this study, therefore, is to compare objectively assessed SB and PA, as well as CRF measured by CPET, in patients with schizophrenia with matched, physically inactive, but otherwise healthy controls using data from the “The Outcome of Psychosis and Fitness Therapy” study (TOPFIT).
The second aim was to determine whether SB, PA, and CRF were associated with mental and physical health parameters in both patients with schizophrenia and matched healthy controls.
Materials and Methods
Participants and Setting
This study included data of 63 patients with a schizophrenia spectrum disorder and 55 healthy controls, matched for gender, age, and socioeconomic status (expressed as the highest educational level of one of the parents). Patients were recruited at the University Medical Center Utrecht (Netherlands) (n = 26) and regional mental health care institutes (Altrecht; GGZ Duin- en Bollenstreek; GGZ Friesland) (n = 37). Healthy controls (n = 55) were recruited from the local population via advertisements. Participants were enrolled in the study between May 2007 and May 2010 and written informed consent was obtained after the procedures, and possible side effects were explained. This study was part of the TOPFIT project (“The Outcome of Psychosis and Fitness Therapy”) and registered in the ISRCTN register (http://www.controlled-trials.com/ISRCTN46241817). Patients had a diagnosis of schizophrenia (n = 45), schizoaffective (n = 15), or schizophreniform disorder (n = 3) according to the Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV). Diagnosis was confirmed by psychiatrists using the Comprehensive Assessment of Schizophrenia and History (CASH) (18). Patients were stable on antipsychotic medication, i.e., using the same dosage for at least 4 weeks prior to inclusion. They showed no evidence for significant cardiovascular, neuromuscular, endocrine or other somatic disorders that prevented safe participation in the study (19). Patients had no primary diagnosis of alcohol or substance abuse and had an IQ ≥ 70, as measured with the Wechsler Adult Intelligence Scale Short Form (WAIS-III SF) (20).
The inclusion criteria for the healthy controls were no diagnosis of psychiatric disorders according to DSM-IV lifetime, no first-degree relative with a psychotic or depressive disorder, and being physically inactive before inclusion (i.e., undertaking <1 h of moderate PA weekly; based on self-report). The study was approved by the Human Ethics Committee of the University Medical Center Utrecht and research committees of participating centers.
Assessments
All measurements were assessed by a research assistant and a sports physician. Participants were asked to wear the SenseWear Pro-2 (BodyMedia, Inc., Pittsburgh, PA), body monitoring system during three 24-h time bouts (2 weekdays and 1 weekend day) except during water-based activities. This device objectively measures PA and estimates energy expenditure (21–23). The SenseWear was worn over the right arm triceps muscle and assesses minute-to-minute data through multiple sensors, namely a two-axis accelerometer and sensors measuring heat flux, galvanic skin and near body-temperature. Data are combined with gender, age, body weight, and height, to measures physical (in)activity and estimate energy expenditure using algorithms developed by the manufacturer (SenseWear Professional software, version 5.1.0.1289).
Several variables were calculated from the SenseWear data. PA was expressed in average metabolic equivalents (MET; in kcal/kg/h), an indicator of daily energy expenditure. The unit MET was used to estimate the amount of oxygen used by the body during SB and PA. Daily average time spend in total SB (<3 MET), moderate and vigorous PA (MVPA) (≥3MET), moderate (3–6 MET), vigorous (≥6 MET) were calculated from all minutes with a MET-value. Total energy expenditure (TEE; in kcals), active energy expenditure (AEE; in kcals: ≥3 MET), number of steps, lying down and sleeping time were also estimated. Data was accepted when the average on-body measuring time was at least 1,368 min per day (95% of a 24-h bout).
CRF, defined as the ability of the circulatory and respiratory systems to supply oxygen to skeletal muscles during sustained physical activity, was assessed with a cardiopulmonary exercise test (CPET), performed using a 20 watt per minute (W/min) step wise incremental protocol to exhaustion on a cycle ergometer (Lode Excalibur, Lode BV, Groningen, the Netherlands) (24). CRF was defined as the highest oxygen uptake during any 30-s interval during the test (VO2peak ml·kg−1·min−1) (25). Waist circumference (in cm) and anthropometric measurements (height in cm and weight in kg), using the same calibrated equipment in all participants, and metabolic syndrome (MetS), assessed according to the International Diabetes Foundation criteria (26), were obtained by the sports physician prior to the CPET.
To evaluate the severity of schizophrenia symptoms, the Positive and Negative Syndrome Scale (PANSS) total, positive, negative, and general (sub)scores were assessed (27). The Montgomery Åsberg Depression Rating Scale (MADRS) assessed co-morbid depressive symptoms (28). Detailed information on the amount and type of prescribed antipsychotic and other medication were gathered. Current antipsychotic medication prescribed was described in cumulative dosage and converted into haloperidol equivalents, conformable to a table from the Dutch National Health Service (29).
Statistical Analyses
SPSS 25.0 was used to analyze the data (Armonk, NY: IBM Corp). All statistical tests were performed two-tailed and a p < 0.05 was considered significant. Data were examined for outliers. All analyses were performed with and without extreme outliers to examine their influence on results. In case of non-normal distribution logarithmic transformation was applied.
Multiple analyses of variance for non-categorical variables and χ2 analyses for categorical variables were used to examine differences between patients with schizophrenia and matched healthy controls in demographic and clinical variables. Univariate analyses were used to examine differences in SB, MVPA, moderate PA, vigorous PA, TEE, and AEE, number of steps, lying down and sleeping time, and CRF between patients and healthy controls. Gender, age, WAIS IQ-score, marital status, employment status, and Body Mass Index (BMI) were included in analyses as possible confounding factors. To investigate if differences exist between day of measurement (weekdays vs. weekend) within and between groups (patients vs. controls), repeated measures analysis of variance were performed comparing the average weekday vs. weekend day SB, MVPA, moderate PA, vigorous PA, TEE and AEE, number of steps, lying down, and sleeping time. Correction for multiple testing was applied according to the Bonferroni-correction procedure.
In patients, backward linear regression analysis (criterion: probability of F-to-remove ≥0.10) was used to assess whether the independent variables gender, age, PANSS positive, PANSS negative, PANSS general, employment status, and MADRS-score were associated with the level of SB, MVPA, and CRF (VO2peak ml·kg−1·min−1). Similarly, we examined the association between physical health parameters (gender, age, employment status, BMI, haloperidol equivalent of antipsychotic medication prescribed, and number met criteria for the MetS) and SB, MVPA, and CRF (VO2peak ml·kg−1·min−1). We repeated the latter regression analyses in healthy controls, examining the association between physical health parameters (gender, age, employment status, BMI, number of met criteria for MetS) and SB, MVPA, and CRF.
Results
Descriptive Statistics
Demographic and illness characteristics are shown in Table 1. Healthy controls had lower BMI (p = 0.01), waist circumference (p = 0.002), triglycerides (p < 0.001), and LDL-cholesterol (p = 0.02). Healthy controls were less likely to have MetS (p = 0.04), met on average less MetS criteria (p = 0.003), and smoked less cigarettes per day (p ≤ 0.001). Healthy controls were more likely married (p ≤ 0.001), had a higher IQ (p ≤ 0.001), and higher HDL-cholesterol levels (p < 0.001). No significant differences in demographic and illness characteristics, except higher diastolic blood pressure (p = 0.02) and lower HDL-cholesterol (p = 0.007), were found between male and female patients. There were no differences in type [χ = 5.68; p = 0.77] and dose [F(1, 58) = 1.24; p = 0.27] of antipsychotic medication used between genders in patients.
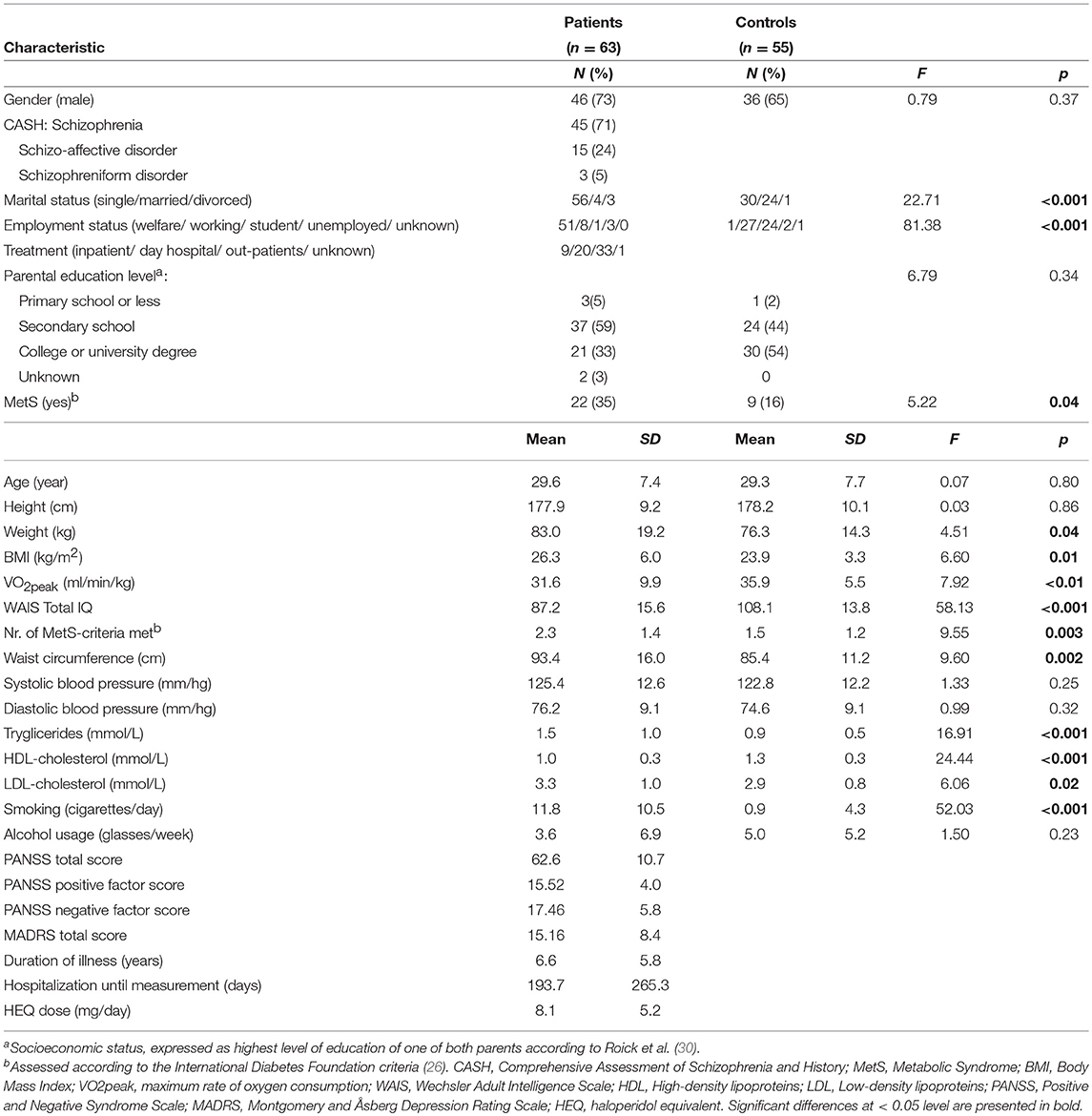
Table 1. Demographic and clinical characteristics for patients with schizophrenia and matched healthy controls.
Differences in SB, PA, and CRF
All variables, except SB, moderate PA, vigorous PA, and active energy expenditure data, complied with normality and homogeneity of variance demands. After logarithmic transformation of these variables, all data were analyzed parametrically. Average on-body percentage was below 95 percent in one patient with schizophrenia and three healthy controls. In total, 62 patients and 52 healthy controls, with an average on-body time of 98.3 (SD: 1.4) and 98.0 (SD: 1.2) percent, respectively, were thus included in further analyses. Results are presented in Table 2. Compared to physically inactive but otherwise healthy matched controls, patients showed significantly higher SB (p = 0.005), less MVPA (p = 0.005), and less moderate PA (p ≤ 0.001), but equal vigorous PA (p = 0.15). Patients with schizophrenia had significantly lower total (p = 0.001) and active (p = 0.002) energy expenditure compared to controls. Though the average daily number of steps taken was lower in patients with schizophrenia (mean: 8040; SD: 3072) than in controls (mean: 8884; SD: 2837), this difference did not reach significance (p = 0.16). Patients spent significantly more time lying down (p ≤ 0.001) and sleeping (p < 0.001) (expressed as minutes per day) than controls. Patients had significantly poorer CRF than healthy controls (p < 0.01). Controlling for gender, age, BMI, and marital status did not change results. Controlling for WAIS IQ led to non-significance for TEE only. However, controlling for employment status led to non-significant differences in SB, PA, and TEE and AEE, but not in lying down and sleeping time. Bonferroni-correction for multiple testing did not influence the conclusions.
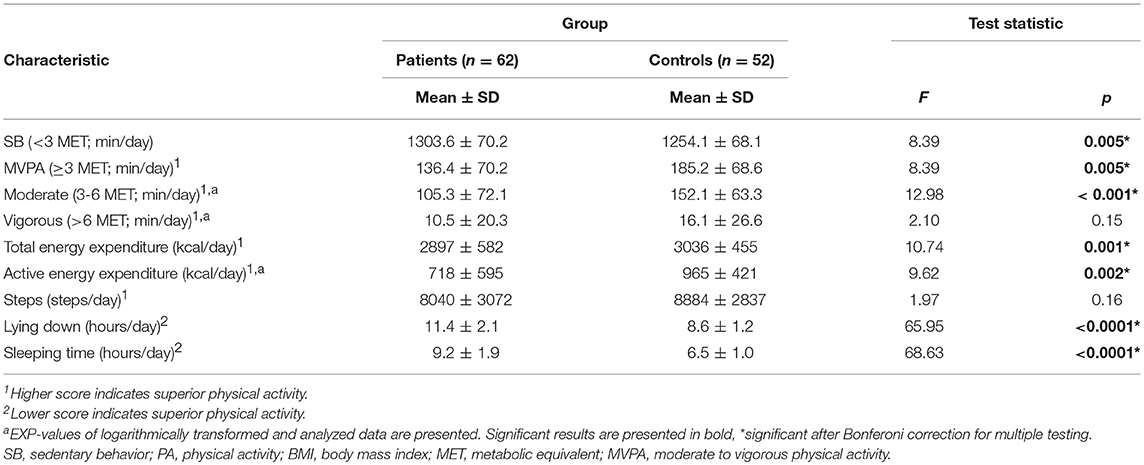
Table 2. SB and PA in patients with schizophrenia and matched healthy controls, controlled for gender, age, and BMI influences.
Differences in SB and PA on Weekdays vs. Weekend Days
Except for vigorous PA, patients and controls demonstrated significantly more SB, significantly less time on MVPA and moderate PA, had lower TEE and AEE, took fewer steps, and spent more time lying down and sleeping during the weekend compared to weekdays (Monday through Friday) (see Table 3). After Bonferroni-correction for multiple testing participants still took significantly fewer steps and spent more time lying down and sleeping. No significant differences between the two 24-h weekday assessments were found in either patients or controls for any of the SB or PA variables (all p > 0.20). Whereas, no differences in PA or energy expenditure were found between Saturdays or Sundays in healthy controls, patients had less MVPA (p = 0.04) and lower TEE (p = 0.005), and AEE (p = 0.009) on Saturdays compared to Sundays.
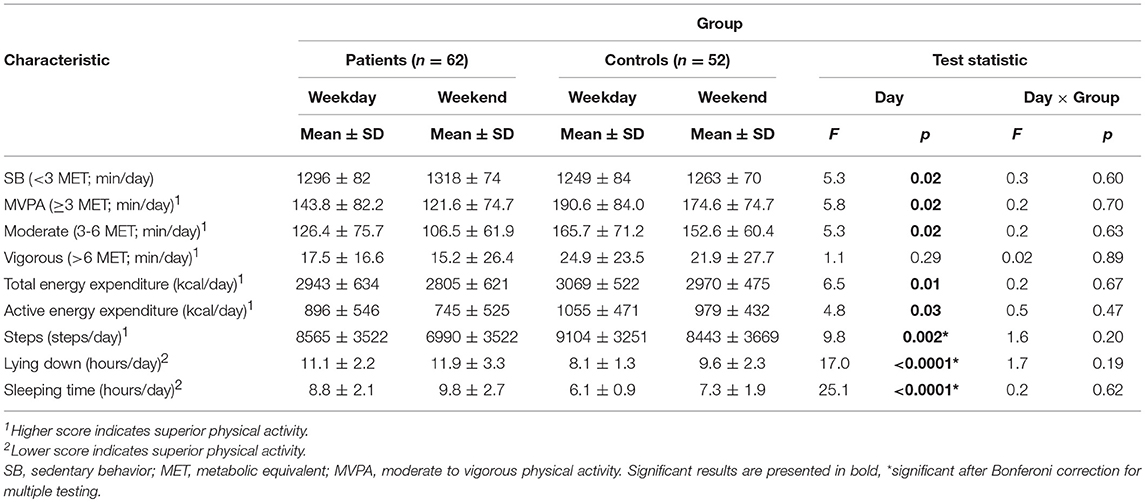
Table 3. Differences between day of measurement (weekdays vs. weekend) within (day) and between groups (day × group; patients vs. controls).
Associations of SB, MVPA, and CRF With Mental and Physical Health
In patients, for mental health, a significant final model for SB emerged [F(1, 59) = 4.46; p = 0.039; R2 = 0.069] in which PANSS negative score (beta = 0.263; p = 0.039) was significantly associated with SB. In the final model, gender, age, employment status, WAIS IQ, PANSS positive, PANSS general, and MADRS-score were not significantly associated with SB. This means that increasing severity of negative symptoms was associated with more SB. An identical but inversed model emerged for MVPA which means that increasing severity of negative symptoms was associated with fewer MVPA. For mental health, a significant model for CRF emerged also [F(4, 56) = 17.195; p < 0.00000001; R2 = 0.551] in which gender (female vs. male; beta = −0.398; p < 0.0001), age (beta = −0.417; p < 0.0001), and PANSS negative score (beta = −0.502; p < 0.00001) MADRS score (beta = 0.198; p = 0.040) were significantly associated with CRF level indicating female gender, higher age, and more severe depressive and particularly negative symptoms were associated with poorer CRF.
In patients, for physical health, no significant final model for either SB nor MVPA emerged since none of the variables (gender, age, employment status, BMI, haloperidol equivalent of antipsychotic medication prescribed, and number met criteria for the MetS) were significantly associated with SB or MVPA, respectively. For physical health, a significant model for CRF did emerge [F(4, 54) = 17.566; p < 0.00000001; R2 = 0.570] in which gender (female vs. male; beta = −0.255; p = 0.011), age (beta = −0.214; p = 0.032), employment status (beta = −2.04; p = 0.032), and BMI (beta = −0.489; p < 0.00001) were significantly associated with CRF level. This means female gender, higher age, being unemployed or on welfare, and higher BMI were associated with poorer CRF. When negative symptoms and BMI were combined in one regression model with CRF, both factors were equally related.
In healthy controls, a significant model emerged for MVPA [F(7, 10) = 7.095; p = 0.002; R2 = 0.225] in which gender (female vs. male, beta = 0.307; p = 0.02) and BMI (beta = −0.31, p = 0.02) were significantly associated with MVPA. The same holds for SB [F(7, 19) = 7.095; p = 0.002; R2 = 0.225; with gender −0.307, p = 0.02 and BMI 0.32, p = 0.02 being significantly associated] and CRF [F(3, 48) = 18.101; p < 0.00000001; R2 = 0.531, with again gender −0.638, p < 0.0000001, employment status (beta = −0.210; p = 0.056), and BMI −0.54, p < 0.0001 being significantly associated with CRF]. Noteworthy, females tended to have more MVPA and less SB, but poorer CRF. The latter corresponds with the model in patients, in which also female gender and higher BMI were associated with poorer CRF.
Discussion
This study examined objectively measured PA and inactivity, SB and CRF in patients with schizophrenia compared to inactive healthy controls. Patients with schizophrenia performed significantly less MVPA, moderate PA, more SB, had lower total and active energy expenditure, spent more time per day lying down and sleeping, and had poorer CRF compared to healthy controls. The amount of MVPA, but more prominently CRF level, was associated with the severity of negative symptoms in patients with schizophrenia. Only CRF, and not SB or MVPA, was associated with BMI.
This study adds to current knowledge by being one of the few to include CRF in studying the relationship between PA, SB and cardiovascular disease, and, more importantly, by being the only one to use the gold standard CPET in measuring CRF. CRF indeed appeared independently related to cardio-metabolic risk, more so than SB or PA. This has two implications; it stresses the importance of taking CRF into account when assessing patients' physical health status, and it implies that the implementation of interventions aiming to increase CRF is of utmost importance in tackling the alarming cardio-metabolic health of patients with schizophrenia (31). Two previous intervention studies showed this was feasible in patients with schizophrenia (32, 33). In the current study, we found an association between CRF and severity of negative symptoms, which is in line with previous research (34). The direction of this association is as of yet not exactly known; it may seem conspicuous to think negative symptoms lead to inactivity which in turn affects CRF levels. There is however emerging evidence that a bidirectional association may be possible as well. Two studies found evidence of a direct relationship of CRF (35) on cognition and PANSS symptomatology (36), respectively. In other areas, such as depression and bipolar disorder, the effect of physical activity on mood has been widely established, even though the mechanisms through which physical activity and brain functioning (mood, cognition and symptoms) affect each other are not completely understood yet. Nonetheless, this gives hope to the idea that interventions aiming to increase CRF may also reduce negative symptoms (37). This could, on its turn, have important functional benefits as well since negative symptoms evidently impact an individual's functional capacity in daily activities (38).
Our results are furthermore consistent with previous studies which reported lower levels of PA in patients with schizophrenia compared to healthy comparison subjects (30, 39–44). In line with earlier findings, we found patients with schizophrenia spend less time on moderate PA, but not on vigorous PA (43). In accordance with the only study that used doubly labeled water, the established criterion standard method for free-living energy expenditure assessment, we found reduced total and active energy expenditure in patients with schizophrenia (45).
Some limitations should be considered when interpreting present findings. First, SenseWear reliably assesses PA and energy expenditure in normal and overweight healthy adults (21–23, 46), yet has not been validated in patients with schizophrenia. SenseWear overestimated energy expenditure in obese subjects (46) and the current study included 15 obese patients and 2 obese healthy controls (BMI>30). Papazoglou et al. (46) used an older software version than the present study which was later shown to have an inferior accuracy (23). Second, as this is a cross-sectional study, only relationships between SB, PA, and CRF, and mental and physical health parameters could be examined, not causality. Third, we did not succeed in enrolling healthy controls fully matching the schizophrenia patient group, other than on age, socio-economic status and inactivity. In terms of cardiometabolic health, the patients were much worse off, which on the one hand stresses the seriousness of their health condition, but on the other hand impedes true comparison of the two groups. In addition, patients with schizophrenia and healthy subjects volunteered to engage in the study, which may have led to some selection bias because subjects motivated for PA and health improvement might have had greater interest in this study. Accordingly, this may have led to an overestimation of activity levels compared to the entire schizophrenia population. Also, the absence of a matched psychiatric control group is a limitation of our study. It would have been interesting to see whether activity patterns and CRF levels of patients with schizophrenia differ from patients with other psychiatric diagnoses. This might also shed light on the role of negative symptoms, which may be present in patients with other psychiatric disorders but are often more pronounced in patients with schizophrenia. Fourth, one could argue that the CPET is too strenuous for patients with schizophrenia. In our study, however, all controls and all but four patients with schizophrenia met maximal effort demand (RER peak ≥1.1), albeit that patients with schizophrenia did reach significantly lower average RER peak values than controls. This could however in part be due to poorer CRF and the fact that they are not accustomed to perform high-intensity exercise. Last, others often define SB as <1.5 MET whereas we defined it as <3 MET. This may have led to a higher estimate of SB.
In conclusion, our study shows patients with schizophrenia perform less PA, expend less total and active energy, spend more time lying down and sleeping, and have poorer CRF compared to physically inactive matched, healthy controls. Given the remarkably strong associations of CRF with both negative symptoms and BMI, improvement of CRF should be a primary treatment aim, which may affect both mental and physical health in patients with schizophrenia.
Data Availability
The datasets generated for this study are available on request to the corresponding author.
Author Contributions
TS, FB, TT, and WC conceived, designed, and amended the study and wrote the protocol. TS was responsible for the acquisition of the data. TS, FJ, and TT performed the statistical analyses. TS, FJ, and TT wrote the first draft of the manuscript. All authors provided critical review of the manuscript and approved the final version.
Funding
This project was funded primarily by the UMCU, Netherlands. In addition, this work was funded by the Dutch Diabetes Research Foundation (Project Grant 2007.00.040). A research assistant was partly funded by Lilly Pharmaceuticals, Houten, the Netherlands (Project Grant Ho01–TOPFIT). Janssen Pharmaceuticals, Tilburg, Netherlands made a general financial contribution for this project. The Dutch Psychomotor Therapy Foundation, Utrecht, the Netherlands gave a financial contribution for this project. The study sponsors had no further role in study design, in the collection, analysis and interpretation of data; in the writing of the report; and in the decision to submit the paper for publication.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We gratefully acknowledge all participants in the TOPFIT study for their willingness to cooperate.
References
1. Hayes JF, Marston L, Walters K, King MB, Osborn DPJ. Mortality gap for people with bipolar disorder and schizophrenia: UK-based cohort study 2000–2014. Br J Psychiatry. (2017) 211:175–81. doi: 10.1192/bjp.bp.117.202606
2. Tanskanen A, Tiihonen J, Taipale H. Mortality in schizophrenia: 30-year nationwide follow-up study. Acta Psychiatr Scand. (2018) 138:492–9. doi: 10.1111/acps.12913
3. Walker ER, McGee RE, Druss BG. Mortality in mental disorders and global disease burden implications a systematic review and meta-analysis. JAMA Psychiatry. (2015) 72:334–41. doi: 10.1001/jamapsychiatry.2014.2502
4. Correll CU, Detraux J, De Lepeleire J, De Hert M. Effects of antipsychotics, antidepressants and mood stabilizers on risk for physical diseases in people with schizophrenia, depression and bipolar disorder. World Psychiatry. (2015) 14:119–36. doi: 10.1002/wps.20204
5. Laursen TM, Wahlbeck K, Hallgren J, Westman J, Osby U, Alinaghizadeh H, et al. Life expectancy and death by diseases of the circulatory system in patients with bipolar disorder or schizophrenia in the Nordic countries. PLoS ONE. (2013) 8:e67133. doi: 10.1371/journal.pone.0067133
6. Correll CU, Solmi M, Veronese N, Bortolato B, Rosson S, Santonastaso P, et al. Prevalence, incidence and mortality from cardiovascular disease in patients with pooled and specific severe mental illness: a large-scale meta-analysis of 3,211,768 patients and 113,383,368 controls. World Psychiatry. (2017) 16:163–80. doi: 10.1002/wps.20420
7. Stubbs B, Firth J, Berry A, Schuch FB, Rosenbaum S, Gaughran F, et al. How much physical activity do people with schizophrenia engage in? A systematic review, comparative meta-analysis and meta-regression. Schizophr Res. (2016) 176:431–40. doi: 10.1016/j.schres.2016.05.017
8. Stubbs B, Williams JE, Gaughran F, Craig T. How sedentary are people with psychosis? A systematic review and meta-analysis. Schizophr Res. (2016) 171:103–9. doi: 10.1016/j.schres.2016.01.034
9. Vancampfort D, Rosenbaum S, Schuch F, Ward PB, Richards J, Mugisha J, et al. Cardiorespiratory fitness in severe mental illness: a systematic review and meta-analysis. Sports Med. (2017) 47:343–52. doi: 10.1007/s40279-016-0574-1
10. Prince SA, Adamo KB, Hamel ME, Hardt J, Connor Gorber S, Tremblay M. A comparison of direct versus self-report measures for assessing physical activity in adults: a systematic review. Int J Behav Nutr Phys Act.(2008) 5:56. doi: 10.1186/1479-5868-5-56
11. Sallis JF, Saelens BE. Assessment of physical activity by self-report: status, limitations, and future directions. Res Q Exerc Sport. (2000) 71:1–14. doi: 10.1080/02701367.2000.11082780
12. Firth J, Stubbs B, Vancampfort D, Schuch FB, Rosenbaum S, Ward PB, et al. The validity and value of self-reported physical activity and accelerometry in people with schizophrenia: a population-scale study of the UK biobank. Schizophr Bull. (2017). 44:1293–300. doi: 10.1093/schbul/sbx149
13. Nyboe L, Vestergaard CH, Moeller MK, Lund H, Videbech P. Metabolic syndrome and aerobic fitness in patients with first-episode schizophrenia, including a 1-year follow-up. Schizophr Res. (2015) 168:381–7. doi: 10.1016/j.schres.2015.07.053
14. Stubbs B, Gardner-Sood P, Smith S, Ismail K, Greenwood K, Farmer R, et al. Sedentary behaviour is associated with elevated C-reactive protein levels in people with psychosis. Schizophr Res. (2015) 168:461–4. doi: 10.1016/j.schres.2015.07.003
15. Stubbs B, Chen LJ, Chung MS, Ku PW. Physical activity ameliorates the association between sedentary behavior and cardiometabolic risk among inpatients with schizophrenia: a comparison versus controls using accelerometry. Compr Psychiatry. (2017) 74:144–50. doi: 10.1016/j.comppsych.2017.01.010
16. Bueno-Antequera J, Oviedo-Caro MA, Munguia-Izquierdo D. Sedentary behaviour, physical activity, cardiorespiratory fitness and cardiometabolic risk in psychosis: the psychiactive project. Schizophr Res. (2018) 195:142–8. doi: 10.1016/j.schres.2017.10.012
17. Heyward VH, Gibson A. Advanced Fitness Assessment and Exercise Prescription, 7th ed. Champaign, Illinois: Human Kinetics (2014).
18. Andreasen NC, Flaum M, Arndt S. The Comprehensive Assessment of Symptoms and History (CASH). An instrument for assessing diagnosis and psychopathology. Arch Gen Psychiatry. (1992) 49:615–23. doi: 10.1001/archpsyc.1992.01820080023004
19. Bille K, Figueiras D, Schamasch P, Kappenberger L, Brenner JI, Meijboom FJ, et al. Sudden cardiac death in athletes: the lausanne recommendations. Eur J Cardiovasc Prev Rehabil. (2006) 13:859–75. doi: 10.1097/01.hjr.0000238397.50341.4a
20. Christensen BK, Girard TA, Bagby RM. Wechsler adult intelligence scale-third edition short form for index and IQ scores in a psychiatric population. Psychol Assess. (2007) 19:236–40. doi: 10.1037/1040-3590.19.2.236
21. Fruin ML, Rankin JW. Validity of a multi-sensor armband in estimating rest and exercise energy expenditure. Med Sci Sports Exerc. (2004) 36:1063–9. doi: 10.1249/01.MSS.0000128144.91337.38
22. Jakicic JM, Marcus M, Gallagher KI, Randall C, Thomas E, Goss FL, et al. Evaluation of the SenseWear Pro Armband to assess energy expenditure during exercise. Med Sci Sports Exerc. (2004) 36:897–904. doi: 10.1249/01.MSS.0000126805.32659.43
23. Welk GJ, McClain JJ, Eisenmann JC, Wickel EE. Field validation of the MTI actigraph and bodymedia armband monitor using the IDEEA monitor. Obesity. (2007) 15:918–28. doi: 10.1038/oby.2007.624
24. Godfrey S. Exercise Testing in Children: Applications in Health and Disease. Philadelphia: Saunders (1974).
25. Astorino TA. Alterations in VOmax and the VO plateau with manipulation of sampling interval. Clin Physiol Funct Imaging. (2009) 29:60–7. doi: 10.1111/j.1475-097X.2008.00835.x
26. Alberti KGMM, Eckel RH, Grundy SM, Zimmet PZ, Cleeman JI, Donato KA, et al. Harmonizing the metabolic syndrome: a joint interim statement of the international diabetes federation task force on epidemiology and prevention; National heart, lung, and blood institute; American heart association; World heart federation; International atherosclerosis society; And international association for the study of obesity. Circulation. (2009) 120:1640–5. doi: 10.1161/CIRCULATIONAHA.109.192644
27. Kay SR, Fiszbein A, Opler LA. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr Bull. (1987) 13:261–76. doi: 10.1093/schbul/13.2.261
28. Montgomery SA, Asberg M. A new depression scale designed to be sensitive to change. Br J Psychiatry. (1979) 134:382–9. doi: 10.1192/bjp.134.4.382
29. Commissie Farmaceutische Hulp. Farmacotherapeutisch Kompas. Amstelveen: Commissie Farmacotherapeutische Hulp van het College van Zorgverzekeringen (2002).
30. Roick C, Fritz-Wieacker A, Matschinger H, Heider D, Schindler J, Riedel-Heller S, et al. Health habits of patients with schizophrenia. Soc Psychiatry Psychiatr Epidemiol. (2007) 42:268–76. doi: 10.1007/s00127-007-0164-5
31. Sassen B, Cornelissen VA, Kiers H, Wittink H, Kok G, Vanhees L. Physical fitness matters more than physical activity in controlling cardiovascular disease risk factors. Eur J Cardiovasc Prev Rehabil. (2009) 16:677–83. doi: 10.1097/HJR.0b013e3283312e94
32. Heggelund J, Nilsberg GE, Hoff J, Morken G, Helgerud J. Effects of high aerobic intensity training in patients with schizophrenia: a controlled trial. Nord J Psychiatry. (2011) 65:269–75. doi: 10.3109/08039488.2011.560278
33. Scheewe TW, Backx FJG, Takken T, Jörg F, van Strater ACP, Kroes AG, et al. Exercise therapy improves mental and physical health in schizophrenia: a randomised controlled trial. Acta Psychiatr Scand. (2012) 127:464–73. doi: 10.1111/acps.12029
34. Vancampfort D, Knapen J, Probst M, Scheewe T, Remans S, De Hert M. A systematic review of correlates of physical activity in patients with schizophrenia. Acta Psychiatr Scand. (2012) 125:352–62. doi: 10.1111/j.1600-0447.2011.01814.x
35. Holmen TL, Egeland J, Andersen E, Bigseth TT, Engh JA. The association between cardio-respiratory fitness and cognition in schizophrenia. Schizophr Res. (2018) 193:418–22. doi: 10.1016/j.schres.2017.07.015
36. Curcic D, Stojmenovic T, Djukic-Dejanovic S, Dikic N, Vesic-Vukasinovic M, Radivojevic N, et al. Positive impact of prescribed physical activity on symptoms of schizophrenia: randomized clinical trial. Psychiatr Danub. (2017) 29:459–65. doi: 10.24869/psyd.2017.459
37. Rimes RR, de Souza Moura AM, Lamego MK, de Sa Filho AS, Manochio J, Paes F, et al. Effects of exercise on physical and mental health, and cognitive and brain functions in schizophrenia: clinical and experimental evidence. CNS Neurol Disord Drug Targets. (2015) 14:1244–54. doi: 10.2174/1871527315666151111130659
38. Aubin G, Stip E, Gelinas I, Rainville C, Chapparo C. Daily activities, cognition and community functioning in persons with schizophrenia. Schizophr Res. (2009) 107:313–8. doi: 10.1016/j.schres.2008.08.002
39. Brown S, Birtwistle J, Roe L, Thompson C. The unhealthy lifestyle of people with schizophrenia. Psychol Med. (1999) 29:697–701. doi: 10.1017/S0033291798008186
40. Heald A, Pendlebury J, Anderson S, Narayan V, Guy M, Gibson M, et al. Lifestyle factors and the metabolic syndrome in Schizophrenia: a cross-sectional study. Ann Gen Psychiatry. (2017) 16:12. doi: 10.1186/s12991-017-0134-6
41. Kruisdijk F, Deenik J, Tenback D, Tak E, Beekman A, van Harten P, et al. Accelerometer-measured sedentary behaviour and physical activity of inpatients with severe mental illness. Psychiatry Res. (2017) 254:67–74. doi: 10.1016/j.psychres.2017.04.035
42. Lindamer LA, McKibbin C, Norman GJ, Jordan L, Harrison K, Abeyesinhe S, et al. Assessment of physical activity in middle-aged and older adults with schizophrenia. Schizophr Res. (2008) 104:294–301. doi: 10.1016/j.schres.2008.04.040
43. Ratliff JC, Palmese LB, Reutenauer EL, Liskov E, Grilo CM, Tek C. The effect of dietary and physical activity pattern on metabolic profile in individuals with schizophrenia: a cross-sectional study. Compr Psychiatry. (2012) 53:1028–33. doi: 10.1016/j.comppsych.2012.02.003
44. Ringen PA, Faerden A, Antonsen B, Falk RS, Mamen A, Rognli EB, et al. Cardiometabolic risk factors, physical activity and psychiatric status in patients in long-term psychiatric inpatient departments. Nord J Psychiatry. (2018) 72:1–7. doi: 10.1080/08039488.2018.1449012
45. Sharpe JK, Stedman TJ, Byrne NM, Wishart C, Hills AP. Energy expenditure and physical activity in clozapine use: implications for weight management. Aust N Z J Psychiatry. (2006) 40:810–4. doi: 10.1080/j.1440-1614.2006.01888.x
Keywords: physical activity, sedentary behavior, cardiorespiratory fitness, schizophrenia, matched healthy controls
Citation: Scheewe TW, Jörg F, Takken T, Deenik J, Vancampfort D, Backx FJG and Cahn W (2019) Low Physical Activity and Cardiorespiratory Fitness in People With Schizophrenia: A Comparison With Matched Healthy Controls and Associations With Mental and Physical Health. Front. Psychiatry 10:87. doi: 10.3389/fpsyt.2019.00087
Received: 08 October 2018; Accepted: 07 February 2019;
Published: 28 February 2019.
Edited by:
Brendon Stubbs, King's College London, United KingdomReviewed by:
Łukasz Gawȩda, University Medical Center Hamburg-Eppendorf, GermanyGaelle Eve Doucet, Icahn School of Medicine at Mount Sinai, United States
Copyright © 2019 Scheewe, Jörg, Takken, Deenik, Vancampfort, Backx and Cahn. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Thomas W. Scheewe, dHcuc2NoZWV3ZUB3aW5kZXNoZWltLm5s