 Bereket Duko
Bereket Duko Alemayehu Toma
Alemayehu Toma Solomon Asnake
Solomon Asnake Yacob Abraham1
Yacob Abraham1- 1Faculty of Health Sciences, College of Medicine and Health Sciences, Hawassa University, Hawassa, Ethiopia
- 2Faculty of Medical Sciences, College of Medicine and Health Sciences, Hawassa University, Hawassa, Ethiopia
Background: Depressive and anxious symptoms are more regularly seen in HIV-infected people than in the general population. This investigation planned to evaluate the magnitude and factors related to depressive and anxiety symptoms among HIV patients in South Ethiopia, 2018.
Methods: This was an institution-based cross-sectional study directed among 363 HIV-infected individuals who had a customary visit at Hawassa University Comprehensive Specialized Hospital and Yirgalem Hospital, Ethiopia, who were incorporated into the study through systematic sampling techniques. The hospital anxiety and depression scale (HADS) was utilized to take a look at anxious and depressive symptoms.
Results: The mean age of the respondents was 37.66 years (SD ±10.03). The prevalence of depression and anxiety were 32.0% and 34.4%, respectively. Patients who were living alone [AOR = 1.94, (95% CI: 1.06, 3.56)], had poor social support [AOR = 5.57, (95% CI: 1.20, 10.84)] or had HIV-related perceived stigma [AOR = 2.35, (95% CI: 1.44, 3.84)] were more likely to have depression as compared to their counterparts. Those with a previous history of mental illness [AOR = 3.36, (95% CI: 1.31, 8.61)] and poor social support [AOR = 6.67, (95% CI: 1.47, 10.33)] were more likely to have anxiety symptoms.
Conclusion: The prevalence of anxiety and depression in the current study was high. Concerned health departments of the country should create guidelines to screen and treat depression and anxiety among HIV patients. Further research on hazard factors of depression and anxiety ought to be examined to strengthen and expand these findings.
Background
Human immunodeficiency virus (HIV) remains a noteworthy social issue worldwide in general and, in low- and middle-income nations specifically, where a considerable number of individuals living with HIV/AIDS (PLWHA) can be found. The WHO in 2017 reported that an estimated 36.7 million individuals were living with HIV infection and AIDS, with 2.1 million new cases and 1.1 million deaths as a result of HIV-associated causes (1).
Since 1990, HIV infection-associated death has reduced due to the introduction of active antiretroviral therapy (ART). Thus, people who are living with HIV/AIDS have begun to live longer. Nevertheless, people with HIV/AIDS are prone to mental illness, especially depression and anxiety, because of sexual-related problems, social and perceived stigma, the undesirable effects of antiretroviral treatment and neurophysiological changes (2, 3). Investigations indicated that as compared to HIV-negative individuals or the general population, depression occurs at rates two to four times higher in HIV-positive individuals (4–9). It has been observed to be related with higher HIV viral loads and lower CD4 number, even in the wake of controlling for the impacts of adherence, which predict illness advancement and mortality (6, 10–12).
Among psychiatric problems when compared with the general population, anxiety and depression are commonly found in HIV-affected people (6–10). Depression is a conceivably hazardous condition that can impact not just personal satisfaction, connections, work and adherence to therapeutic consideration, as well as possibly survival. The effect of mental health problems on HIV patients is frequently underestimated and is more critical in resource-constrained settings, which is due to an absence of training for health care providers, lack of awareness among HIV patients and lack of guidelines to manage psychiatric disorders in HIV clinics (13, 14).
People living with HIV/AIDS are increasingly inclined to display anxious and depressive symptoms which, thus, affects the stigma associated with the illness, decreases personal satisfaction, increases mortality, lessens medication adherence and impedes their capacity to resist disease (13–16). Having low income, being widowed, being female, having no job, substance abuse including alcohol, non-adherence to medication, low educational status and being in stage III and stage IV were factors that contribute to depression and anxiety among HIV patients (17–19). These show that anxiety and depression greatly affect these patient populations’ treatment outcomes.
Therefore, this study aimed to assess the magnitude and correlates of depressive and anxious symptom among HIV patients in South Ethiopia.
Methods
Study design and setting: This research was undertaken as an institution-based cross-sectional study at Hawassa University Comprehensive Specialized Hospital (HUCSH) and Yirgalem General Hospital (YGH), South Ethiopia, from January 22, 2018 to March 22, 2018. HUCSH is the only comprehensive specialized university hospital in the region, and it is situated at Hawassa city, 273km from Addis Ababa, the capital of Ethiopia. This hospital started delivering service in 2004 and provides both outpatient and inpatient services for more than 18 million people in its catchment area. The hospital has over 400 beds for inpatient service. YGH is in the town of Yirgalem, which is 42km from Hawassa City and was established in 1966, delivers both inpatient and outpatient services to about 4.2 million people.
Sample size determination and sampling procedure: A single-population proportion formula was used to obtain the required sample size using a 95% confidence interval and a 5% margin of error using the prevalence of depression and anxiety: (larger proportion) proportion = 38.94% (17). Study participants were allocated to their respective study setting through a proportional allocation method. The study population was incorporated through a systematic sampling technique, K = 4. A total of 363 individuals with HIV who had follow-up for treatment were recruited for the study. The study participants who had hearing problems, patients who had known severe psychiatric illness or those who needed intensive care therapy were not interviewed.
Data collection: Experienced and trained psychiatry nurses gathered the data using interviewer-administered questioner. The data collection instrument incorporated socio-economic as well as demographic characteristics and clinically-related factors depicting questions. HIV-associated stigma was assessed through the 11-item HIV stigma scale. This scale comprised of four-point Likert questions concerning apparent isolation, shame, blame or guilt and disclosure of HIV status. The item scores of this scale questions summed to build a sole stigma variable. Study participants were classified as having or not having seen stigma utilizing the mean of the stigma scale (≥18.38 or ≥5.86) (20, 21). The Oslo 3-item social support scale was utilized to collect social support related issues. It has a total score scale running from 3 to 14 with three general classifications: “poor support” 3–8, “moderate support” 9–11 and “strong support” 12–14 (22). Anxious and depressive symptoms were assessed using the Hospital Anxiety and Depression Scale (HADS). This is a 14-item questionnaire used to screen for manifestations of depression and anxiety symptoms. It was approved for local use in Ethiopia, and its internal consistency was 0.78 for anxiety, 0.76 for depression subscales and 0.87 for both scales. The scales utilize a cut-off point for anxiety and depression >8 (23).
Data Processing and Analyses: The collected data was checked for comprehensiveness, consistency and, at that point data was coded, cleaned and entered into EPI info version 7. SPSS version 22 was utilized to examine the data. The association of every independent variable with the dependent variable was assessed by bivariate analysis. In order to distinguish potential confounders, a multi-variable logistic regression model was utilized. A p-value of under 0.05 was considered statistically significant, and adjusted odds ratio with 95% CI was determined to decide the association. Finally, the information was displayed by utilizing numbers, frequencies, tables, graphs and figures.
Results
Socio-Demographic Characteristics of the Study Participants
A total of 363 study participants were selected for the investigation with a participation rate of 98.1%. The mean (±SD) age of the respondents was 37.66 years (±10.03). Among the investigation participants, 239 (65.8%) were females, 165 (45.5%) had primary school as their maximum level of education, 188 (51.8%) were married, 128 (35.3%) were merchants and 128 (35.3%) received less than 2500 Ethiopian birr per month (Table 1).
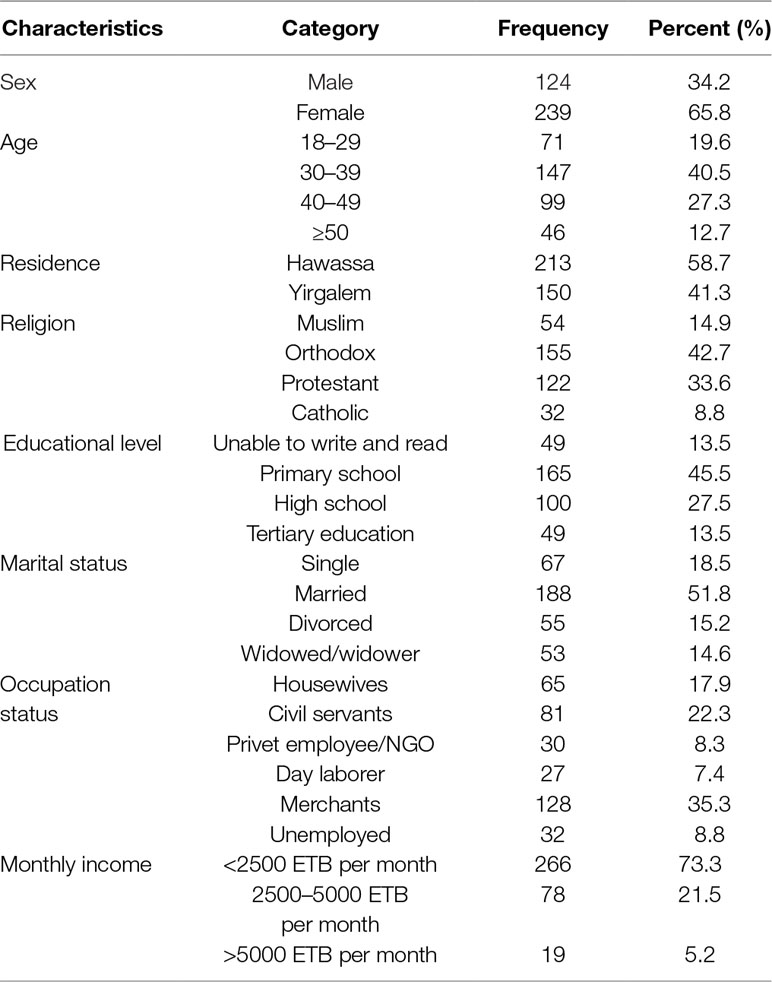
Table 1 Socio-demographic characteristics of people living with HIV/AIDS at Hawassa University Comprehensive Specialized Hospital and Yirgalem Hospital, South Ethiopia, 2018.
Clinical and Psychosocial Characteristics of the Study Participants
A total of 309 (85.1%) of the study participants were on ART, 154 (42.4%) had poor social support, 308 (84.8%) had CD4 cell count ranges between 200 and 1000, 220 (60.6%) had a child or children and 45 (12.4%) were currently using substances (alcohol and tobacco products) (Table 2).
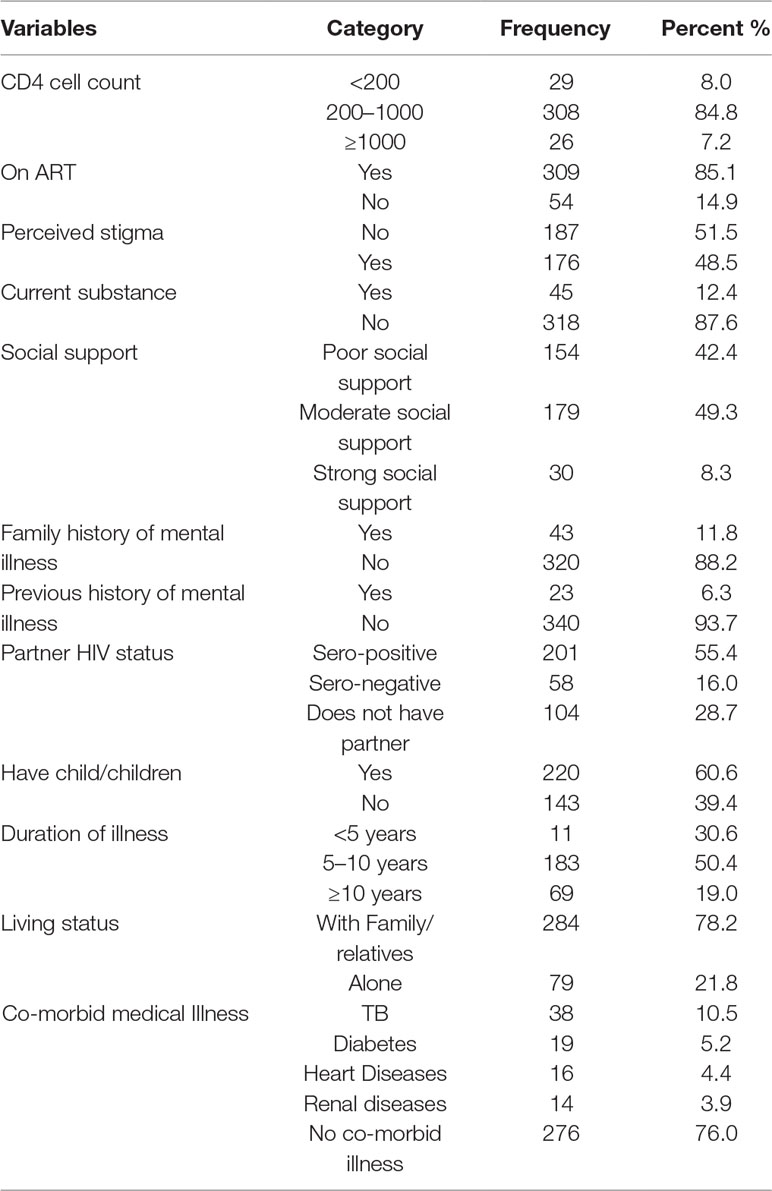
Table 2 Clinical and psychosocial characteristics of people living with HIV/AIDS at Hawassa University Comprehensive Specialized Hospital and Yirgalem Hospital, South Ethiopia, 2018.
Prevalence of Depressive and Anxiety Symptoms and Their Correlates
The magnitude of co-occurring depression and anxiety in this study was 33.5%, while the prevalence of depression and anxiety was 32.0% and 34.4%, respectively. Multivariable binary logistic regression analysis revealed that HIV patients who had no children, were living alone, had perceived HIV related stigma and those who had poor social support were associated with depressive symptoms (Table 3). On the other hand, patients who had a previous history of psychiatric illness and poor social support were associated with anxiety symptoms (Table 4).
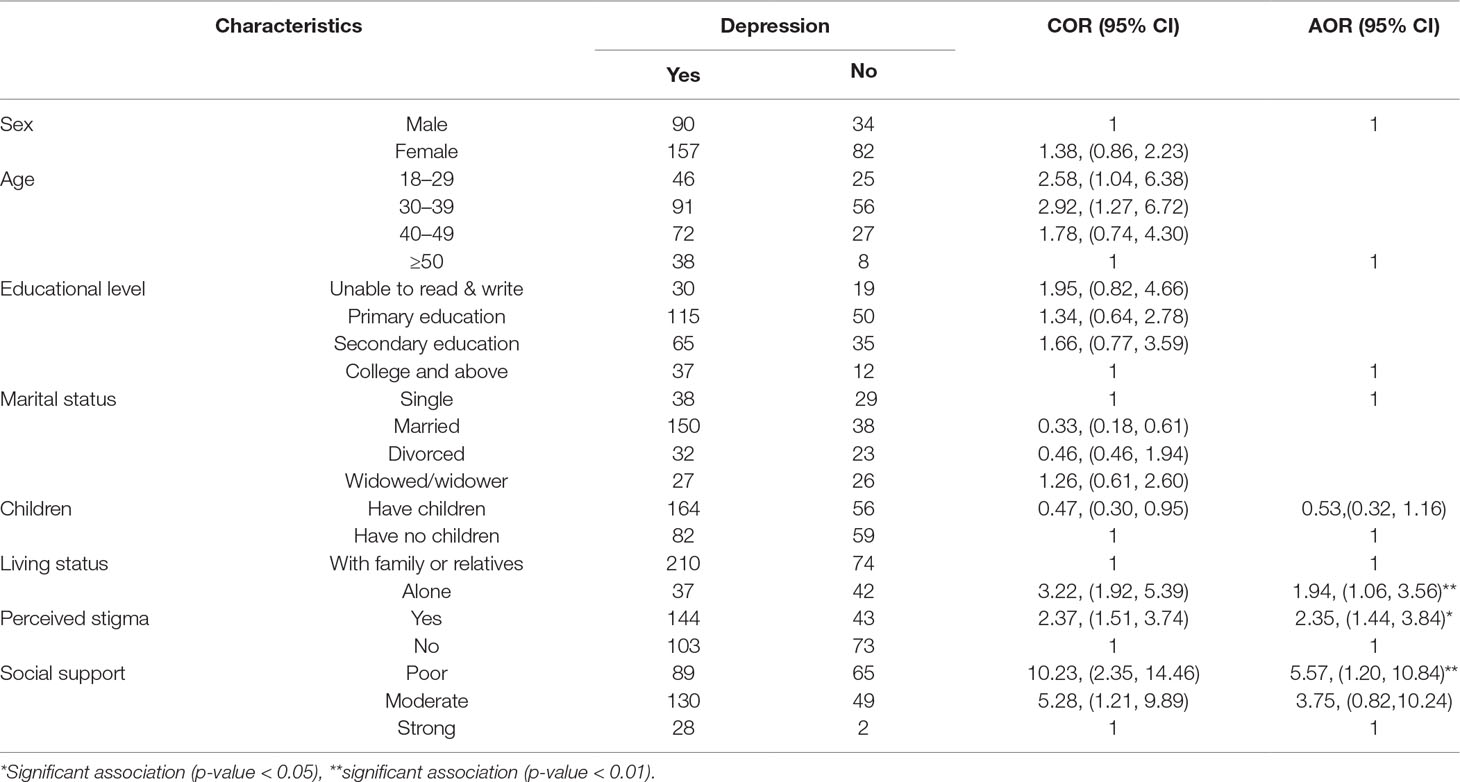
Table 3 Factors associated with depression among people living with HIV/AIDS at Hawassa University Comprehensive Specialized Hospital and Yirgalem Hospital, South Ethiopia, 2018.
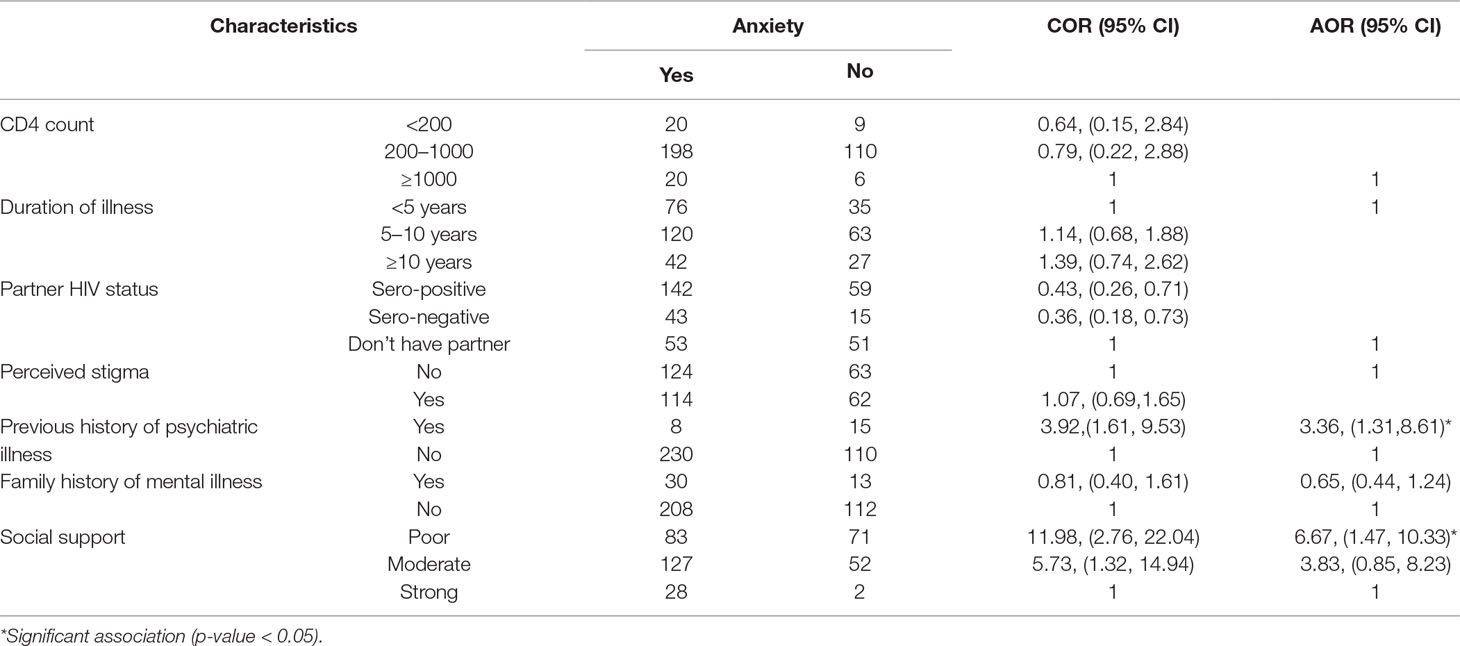
Table 4 Factors associated with anxiety among people living with HIV/AIDS at Hawassa University Comprehensive Specialized Hospital and Yirgalem Hospital, South Ethiopia, 2018.
Discussion
The prevalence of depression in the current study was in line with finding from South Africa (24). However, the current study finding was higher than other studies in Ghana, Nigeria, South Africa and Brazil (18, 25–29). On the other hand, it is lower than other studies in Ethiopia (17, 26, 30), in Delhi (India) (19), North Central Nigeria (31), in Cameroon 63% (32), USA, Denmark (33, 34, China, India and Cameron (35–37). The prevalence of anxiety symptoms in the current study was 34.4%, which is similar with studies conducted in Ethiopia (25), USA, South Africa, Canada and Western Europe (17, 37–39). However, the finding was lower than studies conducted in Albania and China (19, 27, 32) but higher than studies conducted in Ethiopia, Ghana, Thailand, Brazil and Asia (26, 38, 40–42). This study used the hospital anxiety and depression scale (HADS) for assessing anxiety and depressive symptoms among HIV patients while others used the Hamilton depression scale (HDS), Beck’s depression scale (BDS), Beck’s anxiety scale (BAS), the State trait anxiety scale (STAS) or Patient health questionnaire item 9 (PHQ9). Socio-demographic and economic variation could play a vital role for the difference in the magnitude of depression and anxiety between studies from Ethiopia and other studies from other parts of the world.
Study participants who had HIV-related self-felt stigma had more depression when contrasted to their counterparts. This is in line with other findings in Botswana (43) and in Ethiopia (17, 26, 30, 34). HIV is associated with a large amount of stigma and, along these lines, HIV patients might think it is less demanding to be separated from everyone else in order to maintain a strategic distance from stigma or segregation, or they might not have the vitality to be socially connected (30–34). Stigma by itself might build dimensions of exhaustion and diminishing consideration or feelings of uselessness.
People living HIV/AIDS who were living alone were 1.94 times more prone to have depressive symptoms when contrasted to those HIV patients who were living with their family or relatives. Being forlorn is a solid hazard factor for depressive symptoms, well beyond proportions of target social interaction (44, 45).
Patients who had poor social support had a statically significant association with depressive and anxiety symptoms when contrasted to patients with good social support. This is comparable with other studies in India (19) and in Nigeria (18, 19, 22, 26, 31, 32). This may be because of the way that social separation diminishes social support, which can negatively affect mental and physical prosperity. Likewise, these patients preferred to abstain from looking for assistance from others and from opening up about their wellbeing because of social stigma towards themselves, which builds their seclusion and loneliness (19, 26).
Lastly, HIV patients with a past history of mental issues were 3.36 times more prone to experiencing anxiety symptoms. It is not clear whether the existence of HIV affects the seriousness of past psychiatric symptoms of patients or not. This may be because HIV by itself may cause progressively extreme symptoms. Moreover, HIV-affected patients with previous psychiatric problems presumably demonstrate a relapse of previous illness.
Conclusion
The magnitudes of depression and anxiety among HIV patients were high (32% and 34.4%, respectively). Perceived HIV-related stigma, living alone and poor social support had a significant association with depressive symptoms. Having a previous history of psychiatric illness and poor social support had a significant association with anxiety symptoms. Concerned health departments of the country should create principles and standards to screen and treat these conditions in this patient population. Further research on the hazards of anxiety and depression ought to be directed to reinforce and widen these findings
Study Limitations
We did not use standard tools or scales for substance abuse-related factors. Some important variables like medication adherence and opportunistic infections were not included.
Ethical Approval and Consent to Participate:
Ethical clearance for this study was acquired from the Research and Ethics Review Committee of College of Medicine and Health Sciences, Hawassa University, Ethiopia. A letter of permission was acquired from the Research and Community Service Directorate of the College of Medicine and Health Sciences, Hawassa University and submitted to Hawassa University Comprehensive Specialized Hospital and Yirgalem General Hospital, Ethiopia. Study participants were informed about their rights to interrupt the interview at any time and written informed consent was obtained from each study participant. Confidentiality was maintained at all levels of the study. HIV-positive subjects who were found to have moderate to severe depressive and anxiety symptoms were referred to psychiatry clinics for further investigations.
Data Availability Statement
All relevant data are within the paper.
Ethics Statement
Ethical clearance for this study was obtained from the Research and Ethics Review Committee of the College of Medicine and Health Sciences, Hawassa University. Permission letter was obtained from Research and community service directorate of the College of Medicine and Health Sciences, Hawassa University and, submitted to Hawassa University Comprehensive Specialized Hospital and Yirgalem General Hospital. Study participants were informed about their rights to interrupt the interview at any time and written informed consent was obtained from each study participants. Confidentiality was maintained at all levels of the study. HIV positive subjects who were found to have moderate to severe depressive and anxiety symptoms were referred to psychiatry clinics for further investigations.
Author Contributions
BD conceived the study and was involved in the study design, reviewed the article, analysis, report writing and drafted the manuscript. AT, YA and SA were involved in the study design and proposal development. All authors read and approved the final manuscript.
Funding
This study was funded by Hawassa University, Ethiopia. The funding only covers the data collection and write up. No funding received for open access publications and other publication processing fee.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The reviewer AT declared a shared affiliation, with no collaboration, with the authors to the handling editor.
Acknowledgements
The authors recognize Hawassa University, Ethiopia for financing the investigation. The authors appreciate the data measurement personnel, their supervisors and the respective study institution for their assistance and the study participants for their participation in giving all vital data.
References
1. World Health Organization. Facts on HIV/AIDS (2017). http://www.who.int/features/factfiles/hiv/en/
2. Phillips KD, Sowell RL, Rojas M, Tavakoli A, Fulk LJ, Hand GA. Physiological and psychological correlates of fatigue in HIV disease. Biol Res Nurs (2004) 6:59–74. doi: 10.1177/1099800404264846
3. Schuster R, Bornovalova M, Hunt E. The influence of depression on the progression of HIV: direct and indirect effects. Behav Modif (2012) 36:123–45. doi: 10.1177/0145445511425231
4. Ciesla JA, Roberts J. Meta-analysis of the relationship between HIV infection and risk for depressive disorders. Am J Psychiatry (2001) 158:725–30. doi: 10.1176/appi.ajp.158.5.725
5. Chen F, Li F, Chen L, Li Y, Li Y, Guo Z, et al. Analysis of depression and anxiety in HIV/AIDS patients. J Dermatol Venereol (2014) 36:110–2.
6. Carrico AW, Bangsberg DR, Weiser SD, Chartier M, Dilworth SE, Riley ED. Psychiatric correlates of HAART utilization and viral load among HIV-positive impoverished persons. AIDS (2011) 25:1113–8. doi: 10.1097/QAD.0b013e3283463f09
7. Sumari-de Boer IM, Sprangers MA, Prins JM, Nieuwkerk PT. HIV stigma and depressive symptoms are related to adherence and virological response to antiretroviral treatment among immigrant and indigenous HIV infected patients. AIDS Behav (2012) 16:1681–9. doi: 10.1007/s10461-011-0112-y
8. Sabin CA, Ryom L, De Wit S, Mocroft A, Phillips AN, Worm SW, et al. Associations between immune depression and cardiovascular events in HIV infection. AIDS (2013) 27:2735–48. doi: 10.1097/01.aids.0000432457.91228.f3
9. Katon W, Schulberg H. Epidemiology of depression in primary care. Gen Hosp Psychiatry (1992) 14:237–47. doi: 10.1016/0163-8343(92)90094-Q
10. Bouhnik AD, Préau M, Vincent E, Carrieri MP, Gallais H, Lepeu G, et al. Depression and clinical progression in HIV-infected drug users treated with highly active antiretroviral therapy. Antivir Ther (2005) 10:53–61.
11. Ammassari A, Antinori A, Aloisi MS, Trotta MP, Murri R, Bartoli L, et al. Depressive symptoms, neurocognitive impairment, and adherence to highly active antiretroviral therapy among HIV-infected persons. Psychosomatics (2004) 45:394–402. doi: 10.1176/appi.psy.45.5.394
12. Kleeberger CA, Buechner J, Palella F, Detels R, Riddler S, Godfrey R, et al. Changes in adherence to highly active antiretroviral therapy medications in the multicenter AIDS cohort study. AIDS (2004) 18:683–8. doi: 10.1097/00002030-200403050-00013
13. Charlson FJ, Baxter AJ, Cheng HG, Shidhaye R, Whiteford HA. The burden of mental, neurological, and substance use disorders in China and India: a systematic analysis of community representative epidemiological studies. Lancet (2016) 388:376–89. doi: 10.1016/S0140-6736(16)30590-6
14. Ian E, Gwen CL, Soo CT, Melissa C, Chun-Kai H, Eosu K, et al. The burden of HIV-associated neurocognitive disorder (HAND) in the Asia-Pacific region and recommendations for screening. Asian J Psychiatr (2015) 22:182–9. doi: 10.1016/j.ajp.2015.10.009
15. Aguocha M, Uwakwe R, Duru CB, Diwe KC, Augcha JK, Enwere OO, et al. Prevalence and Socio-demographic Determinants of Depression among Patients Attending HIV/AIDS Clinic in a Teaching Hospital in Imo State, Nigeria”. Am J Med Sci Med (2016) 3:106–12. doi: 10.12691/ajmsm-3-6-4
16. National Mental Health Strategy and Federal Ministry of Health. There is no health without mental health. Ethiopia: National Mental Health Strategy and Federal Ministry of Health (2015). https://www.mhinnovation.net/sites/default/files/downloads/innovation/reports/ETHIOPIA-NATIONAL-MENTAL-HEALTH-STRATEGY-2012-1.pdf
17. Eshetu DA, Woldeyohannes SM, Alemayehu M, Techane GN, Tegegne MT, Dagne K. Prevalence of depression and associated factors among HIV/AIDS Patients attending ART Clinic at Debrebirhan referral hospital, North Showa, Amhara Region, Ethiopia. Am J Commun Psychol (2014) 2(6):101–8.
18. Campos LN, Guimarães MDC, Remien RH. Anxiety and depression symptoms as risk factors for nonadherence to antiretroviral therapy in Brazil. AIDS Behav (2011) 14(2):289–99. doi: 10.1007/s10461-008-9435-8
19. Bhate MS, Munjal S. Prevalence of depression in people living with HIV/AIDS undergoing ART and factors associated with it. J Clin Diagn Res (2014) 8(10):WC01–4. doi: 10.7860/JCDR/2014/7725.4927
20. Van Rie A, Sengupta S, Pungrassami P, Balthip Q, Choonuan S, Kasetjaroen Y, et al. Measuring stigma associated with tuberculosis and HIV/AIDS in southern Thailand: exploratory and confirmatory factor analyses of two new scales. Trop Med Int Health (2008) 13(1):21–30. doi: 10.1111/j.1365-3156.2007.01971.x
21. Franke MF, Muñoz M, Finnegan K, Zeladita J, Sebastian JL, Bayona JN, et al. Validation and abbreviation of an HIV stigma scale in an adult spanish-speaking population in urban Peru. Aids & Behav (2010) 14:189–99. doi: 10.1007/s10461-008-9474-1
22. Dalgard OS, Dowrick C, Lehtinen V, Vazquez-Barquero JL, Casey P, Wilkinson G, et al. Negative life events, social support and gender difference in depression, social psychiatry and psychiatric epidemiology. Soc Psychiatry Psychiatr Epidemiol (2006) 41(6):444–51. doi: 10.1007/s00127-006-0051-5
23. Reda AA. Reliability and Validity of the Ethiopian Version of the Hospital Anxiety and Depression (HADS) in HIV Infected Patients. PLoS One (2011) 6(1):e16049. doi: 10.1371/journal.pone.0016049
24. Pappin M, Wouters E, Booysen FL. Anxiety and depression amongst patients enrolled in a public sector antiretroviral treatment programme in South Africa: a crosssectional study. BMC Public Health (2012) 12:244. doi: 10.1186/1471-2458-12-244
25. Tesfaw G, Ayano G, Awoke T, Assefa D, Birhanu Z, Miheretie G, et al. Prevalence and correlates of depression and anxiety among patients with HIV on-follow up at Alert Hospital, Addis Ababa, Ethiopia. BMC Psychiatry (2016) 16(1):368. doi: 10.1186/s12888-016-1037-9
26. Berhe H, Bayray A. Prevalence of depression and associated factors among people livingwith HIV/AIDSI in Tigray, Ethiopia. IJPSR (2013) 4(2):765–75. doi: 10.13040/IJPSR.0975-8232.4(2).765-75
27. Asante KO. Social support and the psychological wellbeing of people living with HIV/AIDS in Ghana. Afr J Psychiatry (2012) 15:340–5. doi: 10.4314/ajpsy.v15i5.42
28. Nüesch R, Gayet-Ageron A, Chetchotisakd P, Prasithsirikul W, Kiertiburanakul S, Munsakul W, et al. The impact of combination Antiretroviral Therapy and its interruption on anxiety, stress, depression and quality of life in Thai patients. Open AIDS J (2009) 3:35–45. doi: 10.2174/1874613600903010038
29. Duko B, Geja E, Zewude M, Mekonen S. Prevalence and associated factors of depression among patients with HIV/AIDS in Hawassa, Ethiopia, cross-sectional study. Ann Gen Psychiatry (2018) 17:45. doi: 10.1186/s12991-018-0215-1
30. Mohammed M, Mengistie B, Dessie Y, Godana W. Prevalence of Depression and Associated Factors among HIV Patients Seeking Treatments in ART Clinics at Harar Town, Eastern Ethiopia. J AIDS Clin Res (2015) 6:474. doi: 10.4172/2155-6113.1000474
31. Shittu RO, Issa BA, Olanrewaju GT, Mahmoud AO, Odeigah LO, Salami AK, et al. Prevalence and correlates of depressive disorders among people living with HIV/AIDS, in North Central Nigeria. J AIDS Clin Res (2013) 4:251. doi: 10.4172/2155-6113.1000251
32. L’akoa RM, Noubiap JJ, Fang Y, Ntone FE, Kuaban C. Prevalence and correlates of depressive symptoms in HIV-positive patients: a cross-sectional study among newly diagnosed patients in Yaoundé, Cameroon. BMC Psychiatry (2013) 13:228. doi: 10.1186/1471-244X-13-228
33. Belete A, Andaregie G, Tareke M, Birhan T, Azale T. Prevalence of anxiety and associated factors among people living with HIV/AIDS at Debretabor general hospital Anti Retro Viral clinic Debretabor, Amhara, Ethiopia. Am J Psychiatry Neurosci (2014) 2(6):109–14. doi: 10.11648/j.ajpn.20140206.15
34. Rao D, Feldman BJ, Fredericksen RJ, Crane PK, Simoni JM, Kitahata MM, et al. A structural equation model of HIV-related stigma, depressive symptoms, and medication adherence. AIDS Behav (2012) 6(3):711–6. doi: 10.1007/s10461-011-9915-0
35. Amiya RM, Poudel KC, Poudel-Tandukar K, Pandey BD, Jimba M. Perceived family support, depression, and suicidal ideation among people living with HIV/AIDS: a cross-sectional study in the Kathmandu Valley, Nepal. PLoS One (2014) 9(3):e90959. doi: 10.1371/journal.pone.0090959
36. Martatino IY, Habibie R, Sahrah A, Wardhana AA. The innovative of aniety disorder healing: Nutri Moringa pudding for pudding for HIV/AIDS infected patients. Int J Asian Soc Sci (2014) 4(11):1100–9. https://econpapers.repec.org/RePEc:asi:ijoass:2014:p:1100-1109
37. Aina Y, Susman JL. Understanding comorbidity with depression and anxiety disorders. J Am Osteopath Assoc (2006) 106(5 Suppl 2):S9–S14.
38. Liu L, Pang R, Sun W, Wu M, Qu P, Lu C, et al. Functional social support, psychological capital,and depressive and anxiety symptoms among people living with HIV/AIDS employed full-time. BMC Psychiatry (2013) 13:324. doi: 10.1186/1471-244X-13-324
39. Obadeji A, Ogunlesi AO, Adebowale TO. Prevalence and predictors of depression in people living with HIV/AIDS attending an outpatient clinic in n Nigeria. Iran Psychiatry Behav Sci (2014) 8(1):26–31. doi: 10.1186/1471-244X-13-324
40. Reif S, Proeschold-Bell RJ, Yao J, Legrand S, Uehara A, Asiimwe E, et al. Three types of self-efficacy associated with medication adherence in patients with co-occurring HIV and substance use disorders, but only when mood disorders are present. J Multidiscip Healthc (2013) 6:229–37. doi: 10.2147/JMDH.S44204
41. Sun W, Wu M, Qu P, Lu C, Wang L. Psychological well-being of people living with HIV/AIDS under the new epidemic characteristics in China and the risk factors: a population-based study. Int J Infect Dis (2014) 28:147–52. doi: 10.1016/j.ijid.2014.07.010
42. Gohain Z, Halliday MAL. Internalized HIV-stigma, mental health, coping and perceived social support among people living with HIV/AIDS in Aizawl District—a pilot study. Psychology (2014) 5:1794–812. doi: 10.4236/psych.2014.515186
43. Gupta R, Dandu M, Packel L, Rutherford G, Leiter K, Phaladze N, et al. Depression and HIV in Botswana: a population-based study on gender-specific socio economic and behavioral correlates. PLoS One (2010) 5:e14252. doi: 10.1371/journal.pone.0014252
44. Cacioppo JT, Hughes ME, Waite LJ, Hawkley LC, Thisted RA. Loneliness as a specific risk factor for depressive symptoms: cross-sectional and longitudinal analyses. Psychol Aging (2006) 21(1):140–51. doi: 10.1037/0882-7974.21.1.140
Keywords: depressive symptom, anxiety symptom, perceived stigma, social support, HIV, Ethiopia
Citation: Duko B, Toma A, Asnake S and Abraham Y (2019) Depression, Anxiety and Their Correlates Among Patients With HIV in South Ethiopia: An Institution-Based Cross-Sectional Study. Front. Psychiatry 10:290. doi: 10.3389/fpsyt.2019.00290
Received: 12 March 2019; Accepted: 15 April 2019;
Published: 07 May 2019.
Edited by:
Yuan-Pang Wang, University of São Paulo, BrazilReviewed by:
Asres Bedaso Tilahune, Hawassa University,EthiopiaMinale Tareke, Bahir Dar University, Ethiopia
Copyright © 2019 Duko, Toma, Asnake and Abraham. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Bereket Duko,YmVya29sZS5kYWRAZ21haWwuY29tLA== orcid.org/0000-0002-4419-0016