 Ju-Yeon Lee
Ju-Yeon Lee Dahye Ban2
Dahye Ban2 Jae-Min Kim
Jae-Min Kim Sung-Wan Kim
Sung-Wan Kim- 1Chonnam National University Medical School, Gwangju, South Korea
- 2Gwangju Bukgu Community Mental Health Center, Gwangju, South Korea
Objectives: Psychotic-like experiences (PLEs) and problematic internet use (PIU) are common in adolescents. However, little is known about the association between PLEs and PIU among adolescents. The present study examined the associations between PLEs and PIU and negative life events among adolescents.
Methods: In total, 1,678 adolescents attending high school were recruited for a cross-sectional survey. They completed self-reported assessments of PLEs using the Prodromal Questionnaire-16 (PQ-16) and measures of depression, anxiety, self-esteem, internet use, and negative life events using the Center for Epidemiological Studies Depression Scale (CES-D), the State-Trait Anxiety Inventory (STAI), the Rosenberg Self-Esteem Scale (RSES), the Korean Scale for Internet Addiction (K-scale), and the Lifetime Incidence of Traumatic Events for Children (LITE-C), including cybersexual harassment and school violence.
Results: A total of 1,239 subjects (73.8%) scored at least 1 on the PQ-16. The mean total and distress PQ-16 scores were significantly higher in students who used mental health services. The total and distress prodromal questionnaire-16 (PQ-16) scores were positively correlated with the CES-D, STAI-S, STAI-T, LITE-C, and K-scale scores but negatively correlated with the RSES score. Hierarchical linear regression analysis revealed that PLEs were significantly associated with a high K-scale score and the incidence of negative life events, such as LITE-C, cybersexual harassment, and bully–victims.
Conclusion: Our results demonstrate that PIU and negative life experiences were significantly associated with PLEs in adolescents. Assessment and therapeutic intervention with regard to internet use as a coping strategy for stress are needed to prevent the development of clinical psychotic symptoms.
Introduction
Psychotic-like experiences (PLEs) are subclinical hallucinations and delusions that are common among adolescents (1) and are a manifestation of at-risk mental states (ARMS) for psychosis (2, 3). The presence of PLEs does not necessarily predict future conversion to psychosis (4), but it is important to address such experiences as they cause distress and functional impairment similar to individuals who transition to psychosis (5). Several psychosocial factors, such as depression, anxiety, poor self-esteem, and negative life experiences, have been reported to be risks for PLEs (6–9). In the context of negative life experiences, PLEs are associated with childhood trauma and recent life events (10, 11). Because adolescence is a distinct life stage with specific developmental tasks, adolescents must cope with various psychological events and bodily changes (12). In particular, school bullying creates substantial stress, especially during adolescence, when peer relationships become important. Cyberbullying (including sexual harassment) has become common, especially among teenagers who use the internet extensively (13). Research has revealed several serious mental health problems caused by the cyberbullying of adolescents (14).
The literature indicates that coping with the stress associated with PLEs may be important in terms of determining psychiatric outcomes (15, 16). Maladaptive coping is associated with the strong relationship between psychopathology and poor functioning in those with psychotic disorders (17, 18). Recent studies in adolescents have indicated that individuals who report subclinical psychotic experiences also commonly use poor coping styles (19). Addictive behaviors, including internet addiction, are known to be negative coping strategies with stressful events and deteriorate the individual functioning (20–22). Problematic internet use (PIU), conceptualized as “internet addiction,” is characterized by persistent compulsive use of the internet that interferes with daily life, leading to significant clinical impairment (23).
PIU is a serious public mental health problem worldwide, especially in adolescents (24). In addition, adolescents who consult for PIU have comorbid mental health problems (25). From a clinical perspective, it is important to explore mental health problems in adolescents with PIU and vice versa. A recent study showed that nonclinical PLE is positively associated with PIU in young adults (26). In our previous study, PIU in patients with a schizophrenia spectrum disorder was significantly associated with dysfunctional coping with stressful events. However, few studies have investigated the association between PLEs and PIU among adolescents. In particular, as South Korea has high-speed internet and a high rate of excessive smartphone use among teenagers (95.9%) (27), PIU is becoming a serious social problem, particularly among adolescents.
This study investigated the associations among PLEs, negative life events, and PIU in Korean community high school students. In particular, we assessed negative life events among adolescents due to not only childhood trauma but also recent stressful events including cybersexual harassment and bullying at school. This study will further facilitate our understanding of these issues in the community setting, including intervention and prevention for adolescents with PLE symptoms.
Methods
Study Design and Participants
This study was a community-based cross-sectional survey undertaken between July and September 2016 in Gwangju, Korea. In total, 2,013 first- and second-grade students from five high schools participated in the survey. Of the 2,013 students, 1,678 (83.4%) were included in the analyses after excluding incomplete or inappropriate responses on the scales. This survey was approved by the principal of each school, and the sample comprised students who voluntarily agreed to complete the questionnaires with informed consent. All measures, including data on sociodemographic characteristics, were self-administered. The Institutional Review Board of Chonnam National University Hospital approved the study. All participants gave written informed consent prior to participation in the study.
Measures
Sociodemographic characteristics. Gender, age, religion, and academic achievement information were obtained from the students. The students were asked about their experience using mental health services offered by a psychiatric clinic, a community center, a counseling center, and a Wee Center (the name given by the Education Office of Korea); the Wee Center offers programs and counseling to city-based students with mental health problems.
Psychotic-like experiences. The Prodromal Questionnaire-16 (PQ-16) is a brief self-report screening questionnaire that assesses the presence of positive and negative symptoms on a two-point scale (true/false) (28). The total score on the PQ-16 was calculated by adding up the agreed items. For each endorsed item, distress was rated on a four-point scale (ranging from no distress to high distress). The distress scale ranged from 0 to 96. The validity of the Korean version of the PQ-16 has been well established (29).
Depression and anxiety. Depression was measured using the Center for Epidemiological Studies Depression Scale (CES-D) (30). The CES-D contains 20 items regarding depressive symptoms experienced in the past week that are rated on a Likert-type scale [“less than 1 day” to “most or all (5–7) days”]. Possible total scores range from 0 to 60, and a higher score reflects greater depression. The reliability and validity of the Korean version of the CES-D have been well established (31). Anxiety was measured using the State-Trait Anxiety Inventory for Children (STAIC) (32). The STAIC consists of two independent domains with 20 items that measure state (STAI-S) and trait (STAI-T) anxiety levels on a three-point Likert scale. Total scores range from 20 to 60 on each domain, with higher scores indicating a higher level of anxiety. The reliability and validity of the Korean version of the STAIC have been well established (33).
Self-esteem. To measure self-esteem, we used the Rosenberg’s Self-Esteem Scale (RSES), which contains 10 items on a four-point Likert scale. A higher score indicates more positive self-esteem (34).
Internet use. PIU was assessed by the short-form Korean Scale for Internet Addiction (K-scale) for adolescents, which was developed by the Korea National Information Society Agency and has been validated in a Korean population (35). The scale consists of 15 items measuring daily life disturbances, virtual interpersonal relationships, deviant behaviors, withdrawal, and tolerance; items are rated on a four-point Likert-type scale.
Negative life events. Lifetime Incidence of Traumatic Events–Child (LITE-C) is a self-checklist that assesses loss and traumatic experiences in children and adolescents (36). The score is calculated by adding the number of “yes (presence)” responses to 16 types of trauma in the LITE-C. In addition to the LITE-C, we added some negative life events, such as cyber harassment and bullying; we included victims, witnesses, and bully–victims.
Statistical Analyses
We calculated PQ-16 numbers and percentages. The mean score differences between various categorical sociodemographic factors were analyzed using the t-test and analysis of variance (ANOVA). Descriptive statistics were employed to estimate the means and standard deviations of continuous variables. Pearson’s correlation coefficient analysis was performed to evaluate the relationships between clinical variables and PQ-16 scores. We used hierarchical linear regression to examine the effects of clinical status, negative life events, and PIU, which were related to PQ-16 score in univariate analyses on PQ-16 score. In step 1, participants’ clinical information (depression, anxiety, and self-esteem), which were significantly correlated with dependents, were entered. In step 2, negative life experiences including LITE-C, which were significantly differences in PQ-16 score tested by t-test or Pearson’s correlation, were entered. Final step, K-scale indicating PIU that was significantly correlated with dependents, was entered. Output results including R2, R2-changes, F value, and standardization regression coefficient (ခβ) were provided in the regression models. Statistical Package for the Social Sciences (SPSS) for Windows software (ver. 21.0; SPSS Inc., Chicago, IL, USA) was used to perform the statistical tests. All statistical tests were two-tailed, and p-values <0.05 were considered significant.
Results
Of the 1,678 students, 1,078 were boys (64.2%) and 600 were girls. The mean age was 18.6 ± 0.5 years. The mean total and distress scores on the PQ-16 were 2.3 ± 2.6 and 38.0 ± 3.0, respectively. The distribution of PQ-16 total scores is shown in Figure 1. A total of 1,239 subjects (73.8%) scored at least 1 on the PQ-16; 11.9% scored 6 or more, indicating the clinical significance of ARMS. Table 1 shows the mean differences in PQ-16 scores by demographic factors. We found no significant difference in PQ-16 scores by gender, religion, or academic achievement. The mean total and distress PQ-16 scores were significantly higher in students who used mental health services. The Wee Center was the most frequently visited institution (n = 87), followed by the community center (n = 46), the counseling center (n = 34), and the psychiatric clinic (n = 29). In terms of negative life events, students who experienced cybersexual harassment scored significantly higher in total and distress PQ-16 scores. Both mean scores were significantly higher for students who experienced school violence as victims, witnesses, and bully–victims.
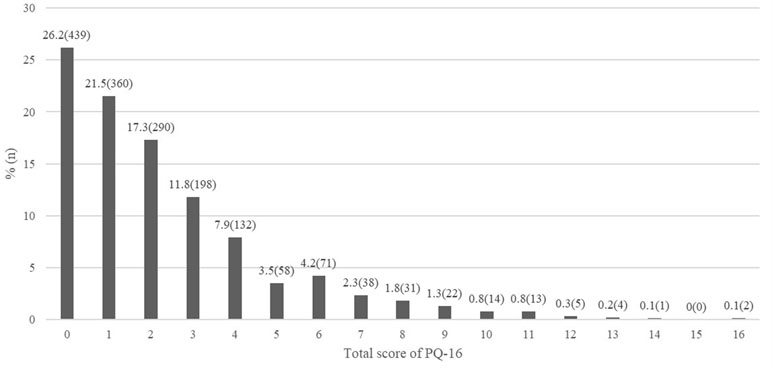
Figure 1 Percentage of number on the total score of PQ-16 (n = 1,678).
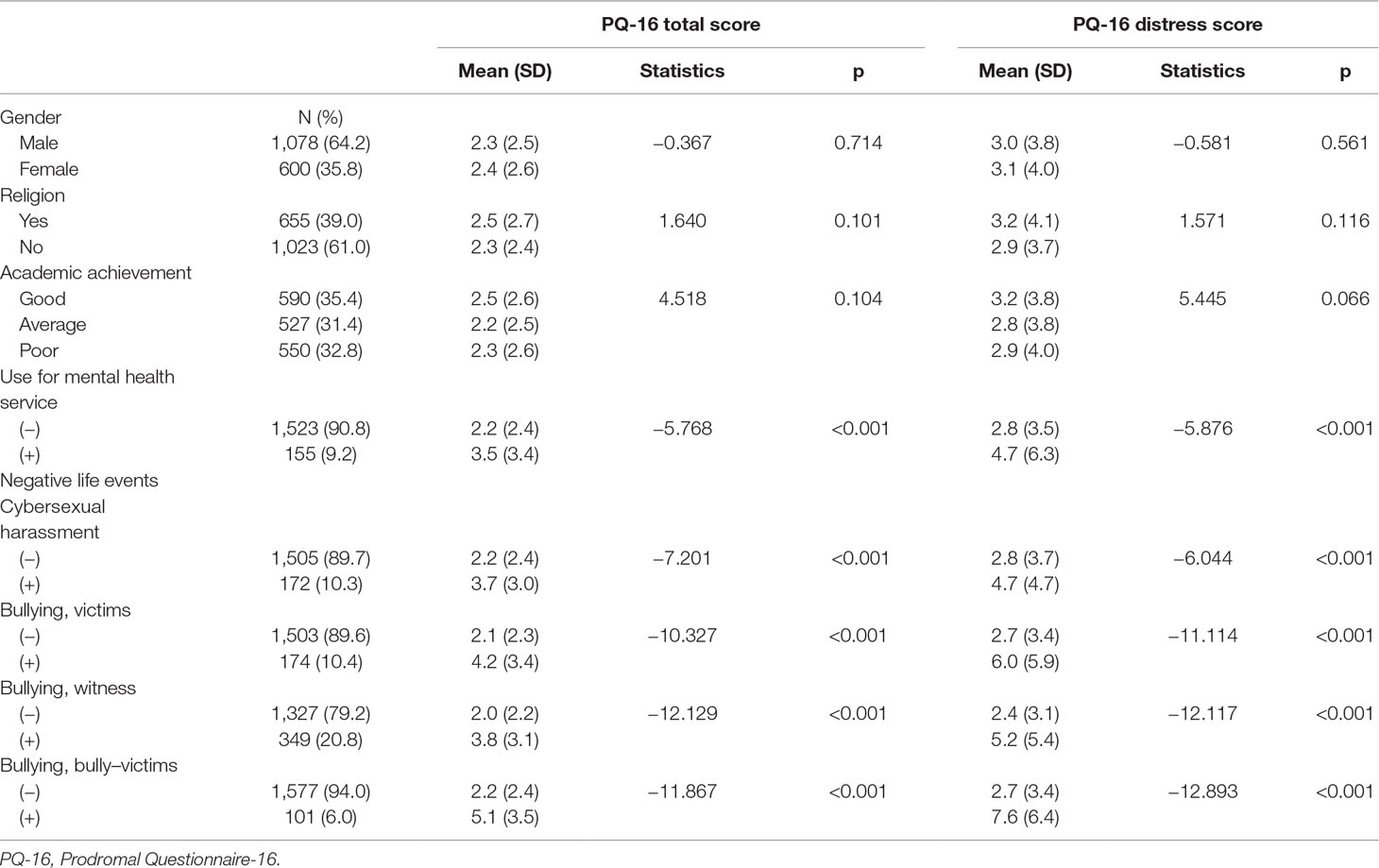
Table 1 Sociodemographic factors that influence PQ-16 score.
Correlational analyses revealed that both the total and distress PG-16 scores were positively correlated with the CES-D, STAI-S, STAI-T, LITE-C, and K-scale scores and negatively with the RSES score (Table 2). The results of the hierarchical multiple regression analyses for PQ-16 score are shown in Table 3. The hierarchical multiple regression for PQ-16 total score revealed that at step 1, clinical information (depression, anxiety, and self-esteem) contributed significantly to the regression model, F (4,15) = 147.72, p < 0.001, and accounted for 28.1% of the variation in PQ-16 total score. Adding negative life events to the regression model explained an additional 8.5% of the variation in PQ-16 total score, and this change in R2 was significant, F (5,15) = 40.58, p < 0.001. Finally, the addition of K-scale to the regression model explained an additional 1.0% of the variation in PQ-16 total score, and this change in R2 was also significant, F (1,15) = 25.07, p < 0.001. The independent variables accounted for 37.7% of variance in PQ-16 total score. The hierarchical multiple regression for PQ-16 distress score revealed that at step 1, clinical information contributed significantly to the regression model, F (4,15) = 147.68, p < 0.001, and accounted for 28.0% of the variation in PQ-16 distress score. Adding negative life events to the regression model explained an additional 7.8% of the variation in PQ-16 distress score, and this change in R2 was significant, F (5,15) = 37.10, p < 0.001. Finally, the addition of K-scale to the regression model explained an additional 0.9% of the variation in PQ-16 distress score, and this change in R2 was also significant, F (1,15) = 22.68, p < 0.001. The independent variables accounted for 36.8% of variance in PQ-16 distress score. Ultimately, high scores on the CES-D, STAI-T, K-scale, and LITE-C scale; low scores on the RSES scale; and status as a bully–victim were strongly associated with both the total and distress PQ-16 scores. Cybersexual harassment predicted the total PQ-16 score but not the distress score.

Table 2 Clinical measures and their Pearson’s correlation coefficients with PQ-16 score.
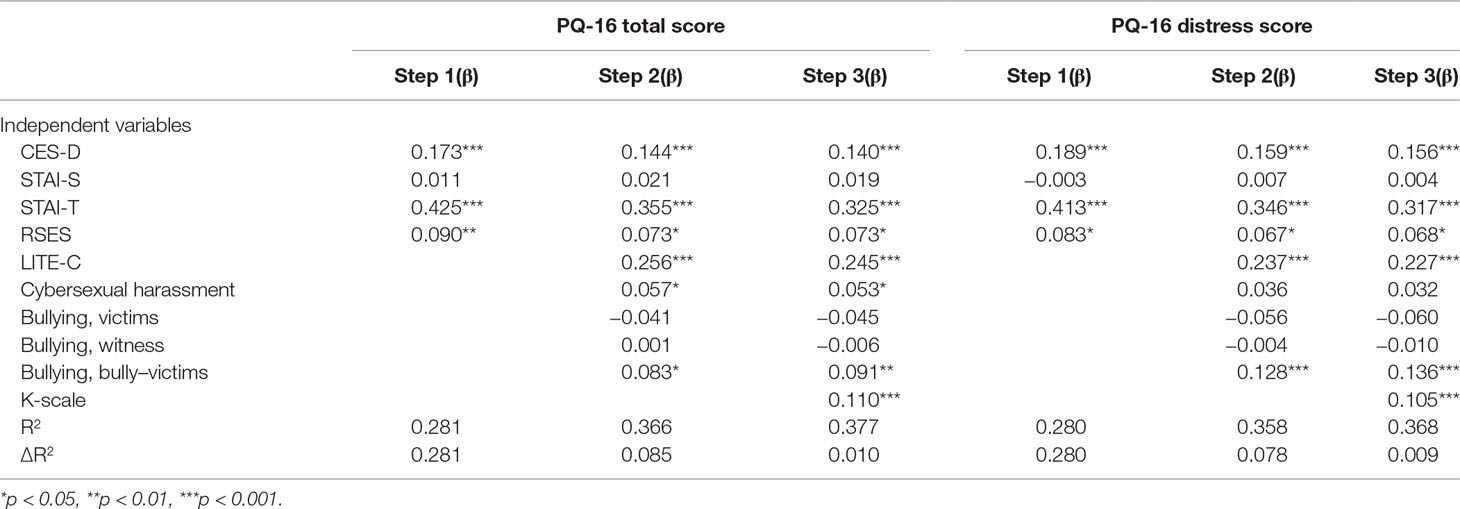
Table 3 Hierarchical linear regression analyses predicting PQ-16 score.
Discussion
The fact that a high percentage of participants scored at least 1 on a PQ-16 item (73.8%) is consistent with previous research in young community samples (37). Also, the percentage of students who scored at least 6 on positive PQ-16 items (indicative of clinical significance) was 11.9%, thus higher than the prevalence rate of 5–8% in the general population (38, 39). This result is in line with the prevalence of PLEs in adolescents (about 10%; thus generally higher than in adults) (40, 41).
In this study, students who used a mental health service had higher mean PQ-16 total and distress scores. It is possible that students with a variety of mental health problems, such as emotional and behavioral difficulties, use mental health services. PLEs are more frequent in help-seeking subjects (42, 43). In particular, PLE-associated distress may encourage help-seeking behavior (44). Our findings suggest that students with mental health problems and PLEs tend to have help-seeking behavior. Furthermore, individuals seeking help to deal with their PLEs could be viewed as being in the prodromal phase of various disorders. However, our results show that approximately half of students who used mental health services were referred to the Wee Center, which offers counseling services to students. Our recent study showed that school counselors are unfamiliar with the concept of high risk for psychosis and lack of confidence in treating those who have had PLEs (45). Early detection and timely delivery of psychiatric services for those who have PLEs is important to prevent a delay in the implementation of an early intervention. In this regard, teachers and school counselors should be provided with proper education regarding students with PLEs.
The severity levels of PLEs and distress as measured by the PQ-16 were associated with psychological difficulties, such as depression, anxiety, and low self-esteem. These results are in line with those of previous studies showing that PLEs were associated with various psychopathologies (46–49). Depression increased the risk of transition to a full-blown psychotic disorder in the ARMS study (50). One previous work suggested that the association between PLEs and poor functioning might be explained by the extent of depression (42). We found that low self-esteem was significantly associated with both total and distress PQ-16 scores. One cognitive model of psychosis suggests that a low self-concept is related to the development and maintenance of PLEs (51). A recent study indicated that those experiencing more hallucinatory-like events exhibited lower levels of self-esteem (52). In our study, trait anxiety was significantly associated with PLEs according to the regression analysis. Trait anxiety serves as a proxy for proneness in those who experience maladaptive anxiety (53); those who score high in “trait anxiety” exhibit differential processing of threatening information. This tendency is termed “attentional threat bias”; one previous study reported that trait anxiety significantly influenced the relationship between cognitive bias and PLEs (54). Our results suggest that biased cognitive processes in adolescents exhibiting high levels of trait anxiety may independently affect PLEs.
Although most PLEs experienced during adolescence are transitional in nature, 20% of subjects experience persistent PLEs, and 7% develop psychotic disorders in adulthood (55). Psychopathologies, such as depression, anxiety, and poor self-esteem, should be routinely assessed and considered for treatment given that they may contribute to later psychosis.
In this study, students who had negative life events, including losses or trauma and recent stressful events, such as cybersexual harassment and school violence, exhibited higher total and distress PQ-16 scores. A strong body of literature has addressed the role of childhood trauma as one of the risk factors for developing a psychotic illness in adolescence (46, 56). Furthermore, although many researchers investigating the relationship between trauma and psychosis have focused on the role of childhood adversity, there is growing evidence for a role of recent stressful life events in the development of psychosis (10, 57). Accordingly, in our study, cybersexual harassment and bullying were significantly associated with PLEs in adolescents. Cybersexual harassment is a type of internet abuse, which can take various forms, such as unsolicited posts and comments on social media sites. There is evidence that individuals with unwanted sexual experiences are at higher risk for developing PLEs (58). Public attention has focused on adolescent internet-mediated victimization, including unwanted exposure to online pornography and sexual messaging, which increase their vulnerability to sexual victimization (59). Our research suggests that cybersexual harassment may be a negative and threatening event that is predictive of PLEs in adolescents.
In particular, the regression analysis showed that the bully–victim status after school violence was a predictor of PLEs. Our findings support previous studies indicating that the prevalence of PLEs is greater in adolescents who have been exposed to school violence, including both victims and perpetrators of bullying (46). This finding suggests that traumatic experiences related to school violence seem to have a salient impact on PLEs, particularly during adolescence when peer relationships become critical to consolidate personal identity (60, 61).
In our study, the PLE was significantly associated with PIU measured by the K-scale in the regression analysis. PIU can be recognized as a maladaptive way of coping with life’s stressors (20, 21). Several studies have found that ARMS individuals tend to engage in more maladaptive coping than nonpsychiatric controls (62, 63). Furthermore, there is some evidence that individuals with schizophrenia experience a disruption in the biological system that responds to stress (64, 65). In a population of stabilized patients with schizophrenia, PIU was significantly associated with ineffective coping strategies to alleviate stress (66). Our findings suggest that the development of PLEs is associated with maladaptive coping strategies during the process of responding to stressful events. This is the first study to determine the relationship between PLEs and PIU among adolescents. Specialized interventions, including problem solving and coping skills training, are needed to help adolescents who have more access to the internet to exploit the internet as a positive coping strategy.
Our study had several limitations. First, this study was cross-sectional; therefore, longitudinal studies are required to confirm the directionality of the relationships in the present analysis, particularly between PIU and PLEs. Additionally, as it is probable that PLEs could make adolescents more likely to be victimized, we may have underestimated the associations between PLEs and negative life events. Second, the generalizability of the results is limited given the targeting of recruited students from one community. Third, we relied on self-reported measures and did not conduct clinical interviews, limiting the clinical validity of the data.
In conclusion, PLEs among adolescents were likely to co-occur with emotional problems, particularly depression, trait anxiety, and low self-esteem. In addition, this study highlights the associations among PLEs, negative life events, and PIU in community adolescents. Our results suggest that a number of traumatic events, including cybersexual harassment and bullying, may increase the risk of PLEs among adolescents. PIU, a maladaptive strategy used to cope with negative life events, was associated with PLEs in adolescents. These have potentially important clinical implications to manage and help adolescents with traumatic events and PIU to prevent the development of more serious clinical psychosis.
Ethics Statement
This survey was approved by the principal of each school, and the sample comprised students who voluntarily agreed to complete the questionnaires with informed consent. All measures, including data on sociodemographic characteristics, were selfadministered.
The Institutional Review Board of Chonnam National University Hospital approved the study. All participants gave written informed consent prior to participation in the study.
Author Contributions
SWK and JYL were involved in the conception and design of the study. DB conducted the data collection. SWK and JYL were involved in the analysis and drafted the manuscript. JMK, SYK, ILS, and JSY revised the manuscript critically for important intellectual content. All authors contributed to and have approved the final manuscript.
Funding
This study was supported by a grant of the Korean Mental Health Technology R&D Project, Ministry of Health & Welfare, Republic of Korea (HM15C1140).
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Rössler W, Riecher-Rössler A, Angst J, Murray R, Gamma A, Eich D, et al. Psychotic experiences in the general population: a twenty-year prospective community study. Schizophr Res (2007) 92:1–14. doi: 10.1016/j.schres.2007.01.002
2. Poulton R, Caspi A, Moffitt TE, Cannon M, Murray R, Harrington H. Children’s self-reported psychotic symptoms and adult schizophreniform disorder: a 15-year longitudinal study. Arch Gen Psychiatry (2000) 57:1053–8. doi: 10.1001/archpsyc.57.11.1053
3. Welham J, Scott J, Williams G, Najman J, Bor W, O’Callaghan M, et al. Emotional and behavioural antecedents of young adults who screen positive for non-affective psychosis: a 21-year birth cohort study. Psychol Med (2009) 39:625–34. doi: 10.1017/S0033291708003760
4. Yung AR, Yuen HP, Berger G, Francey S, Hung TC, Nelson B, et al. Declining transition rate in ultra high risk (prodromal) services: dilution or reduction of risk? Schizophr Bull (2007) 33:673–81. doi: 10.1093/schbul/sbm015
5. Fusar-Poli P, Rocchetti M, Sardella A, Avila A, Brandizzi M, Caverzasi E, et al. Disorder, not just a state of risk: meta-analysis of functioning and quality of life in subjects at high clinical risk for psychosis. Br J Psychiatry (2015) 207:198–206. doi: 10.1192/bjp.bp.114.157115
6. McGrath JJ, Saha S, Al-Hamzawi A, Andrade L, Benjet C, Bromet EJ, et al. The bidirectional associations between psychotic experiences and DSM-IV mental disorders. Am J Psychiatry (2016) 173:997–1006. doi: 10.1176/appi.ajp.2016.15101293
7. van Os J, Kenis G, Rutten BP. The environment and schizophrenia. Nature (2010) 468:203–12. doi: 10.1038/nature09563
8. Saha S, Scott J, Varghese D, McGrath J. Anxiety and depressive disorders are associated with delusional-like experiences: a replication study based on a National Survey of Mental Health and Wellbeing. BMJ Open (2012) 30:2. doi: 10.1136/bmjopen-2012-001001
9. Thewissen V, Myin-Germeys I, Bentall R, de Graaf R, Vollebergh W, van Os J. Instability in self-esteem and paranoia in a general population sample. Soc Psychiatry Psychiatr Epidemiol. (2007) 42:1–5. doi: 10.1007/s00127-006-0136-1
10. Kraan T, Velthorst E, Smit F, de Haan L, van der Gaag M. Trauma and recent life events in individuals at ultra high risk for psychosis: review and meta-analysis. Schizophr Res (2015) 161:143–9. doi: 10.1016/j.schres.2014.11.026
11. Brown GW, Birley JL. Crises and life changes and the onset of schizophrenia. J Health Soc Behav (1968) 9:203–14. doi: 10.2307/2948405
12. Turk J, Graham P, Verhulst F. Adolescence and psychiatric disorders often beginning in adolescence. In: Child and adolescent psychiatry. A developmental approach, 4th ed. New York: Oxford University Press (2007). p. 265–311. doi: 10.1093/med/9780199216697.003.0005
13. Smith PK, Mahdavi J, Carvalho M, Fisher S, Russell S, Tippett N. Cyberbullying: its nature and impact in secondary school pupils. J Child Psychol Psychiatry (2008) 49:376–85. doi: 10.1111/j.1469-7610.2007.01846.x
14. Suzuki K, Asaga R, Sourander A, Hoven CW, Mandell D. Cyberbullying and adolescent mental health. Int J Adolesc Med Health (2012) 24:27–35. doi: 10.1515/ijamh.2012.005
15. Peters E, Day S, McKenna J, Orbach G. Delusional ideation in religious and psychotic populations. Br J Clin Psychol (1999) 38:83–96. doi: 10.1348/014466599162683
16. Bak M, Myin-Germeys I, Hanssen M, Bijl R, Vollebergh W, Delespaul P, et al. When does experience of psychosis result in a need for care? A prospective general population study. Schizophr Bull (2003) 29:349–58. doi: 10.1093/oxfordjournals.schbul.a007010
17. Armando M, Sandini C, Chambaz M, Schaer M, Schneider M, Eliez S. Coping strategies mediate the effect of stressful life events on schizotypal traits and psychotic symptoms in 22q11.2 deletion syndrome. Schizophr Bull (2018) 15:S525–S535. doi: 10.1093/schbul/sby025
18. Yanos PT, Moos RH. Determinants of functioning and well-being among individuals with schizophrenia: an integrated model. Clin Psychol Rev (2007) 27:58–77. doi: 10.1016/j.cpr.2005.12.008
19. Lin A, Wigman JT, Nelson B, Vollebergh WA, van Os J, Baksheev G, et al. The relationship between coping and subclinical psychotic experiences in adolescents from the general population–a longitudinal study. Psychol Med (2011) 41:2535–46. doi: 10.1017/S0033291711000560
20. Valentino RJ, Lucki I, Van Bockstaele E. Corticotropin-releasing factor in the dorsal raphe nucleus: linking stress coping and addiction. Brain Res (2010) 16:29–37. doi: 10.1016/j.brainres.2009.09.100
21. McNicol ML, Thorsteinsson EB. Internet addiction, psychological distress, and coping responses among adolescents and adults. Cyberpsychol Behav Soc Netw (2017) 20:296–304. doi: 10.1089/cyber.2016.0669
22. Tang J, Yu Y, Du Y, Ma Y, Zhang D, Wang J. Prevalence of internet addiction and its association with stressful life events and psychological symptoms among adolescent internet users. Addict Behav (2014) 39:744–7. doi: 10.1016/j.addbeh.2013.12.010
23. Aboujaoude E. Problematic Internet use: an overview. World Psychiatry (2010) 9:85–90. doi: 10.1002/j.2051-5545.2010.tb00278.x
24. Christakis DA. Internet addiction: a 21st century epidemic? BMC Med (2010) 18:61. doi: 10.1186/1741-7015-8-61
25. Ko CH, Yen JY, Yen CF, Chen CS, Chen CC. The association between Internet addiction and psychiatric disorder: a review of the literature. Eur Psychiatry (2012) 27:1–8. doi: 10.1016/j.eurpsy.2010.04.011
26. Mittal VA, Dean DJ, Pelletier A. Internet addiction, reality substitution and longitudinal changes in psychotic-like experiences in young adults. Early Interv Psychiatry (2013) 7:261–9. doi: 10.1111/j.1751-7893.2012.00390.x
27. Korea Internet and Security Agency. 2016 Survey on Internet Usage. Seoul: Korea Internet and Security Agency (2017).
28. Ising HK, Veling W, Loewy RL, Rietveld MW, Rietdijk J, Dragt S, et al. The validity of the 16-item version of the Prodromal Questionnaire (PQ-16) to screen for ultra high risk of developing psychosis in the general help-seeking population. Schizophr Bull (2012) 38:1288–96. doi: 10.1093/schbul/sbs068
29. Kim SW, Chung YC, Kang YS, Kim JK, Jang JE, Jhon M, et al. Validation of the Korean version of the 16-item prodromal questionnaire in a non-help-seeking college population. Psychiatry Investig (2018) 15:111–7. doi: 10.30773/pi.2017.04.24
30. Orme JG, Reis J, Herz EJ. Factorial and discriminant validity of the Center for Epidemiological studies Depression (CESD) scale. J Clin Psychol (1986) 42:28–33. doi: 10.1002/1097-4679(198601)42:1<28::AID-JCLP2270420104>3.0.CO;2-T
31. Cho MJ, Kim KH. Diagnostic validity of the CES-D (Korean version) in the assessment of DSM-III-R major depression. J Korean Neuropsychiatr Assoc (1993) 32:381–99.
32. Spielberger CD. Manual for state-trait anxiety inventory for children. Palo Alto, CA: Consulting Psychologists Press (1973). doi: 10.1037/t06497-000
33. Cho SC, Choi JS. Development of Korean version of state-trait anxiety inventory for children. Seoul J Psychiatry (1989) 14:150–7.
34. Rosenberg M. Society and the adolescent self-image. Princeton, NJ: Princeton University Press (1965). doi: 10.1515/9781400876136
35. National Information Society Agency. Third standardization of Korean internet addiction proneness scale. Seoul, Korea: NIA Research Report (2011).
36. Greenwald R, Rubin A. Assessment of posttraumatic symptoms in children: development and preliminary validation of parent and child scales. Res Soc Work Pract (1999) 9:61–75. doi: 10.1177/104973159900900105
37. Brandizzi M, Schultze-Lutter F, Masillo A, Lanna A, Curto M, Lindau JF, et al. Self-reported attenuated psychotic-like experiences in help-seeking adolescents and their association with age, functioning and psychopathology. Schizophr Res (2014) 160:110–7. doi: 10.1016/j.schres.2014.10.005
38. Shevlin M, Murphy J, Dorahy MJ, Adamson G. The distribution of positive psychosis-like symptoms in the population: a latent class analysis of the National Comorbidity Survey. Schizophr Res (2007) 89:101–9. doi: 10.1016/j.schres.2006.09.014
39. van Os J, Linscott RJ, Myin-Germeys I, Delespaul P, Krabbendam L. A systematic review and meta-analysis of the psychosis continuum: evidence for a psychosis proneness-persistence-impairment model of psychotic disorder. Psychol Med (2009) 39:179–95. doi: 10.1017/S0033291708003814
40. Dolphin L, Dooley B, Fitzgerald A. Prevalence and correlates of psychotic like experiences in a nationally representative community sample of adolescents in Ireland. Schizophr Res (2015) 169:241–7. doi: 10.1016/j.schres.2015.09.005
41. Calkins ME, Moore TM, Merikangas KR, Burstein M, Satterthwaite TD, Bilker WB, et al. The psychosis spectrum in a young U.S. World Psychiatry (2014) 13:296–305. doi: 10.1002/wps.20152
42. Yung AR, Buckby JA, Cotton SM, Cosgrave EM, Killackey EJ, Stanford C, et al. Psychotic-like experiences in nonpsychotic help-seekers: associations with distress, depression, and disability. Schizophr Bull (2006) 32:352–9. doi: 10.1093/schbul/sbj018
43. Schultze-Lutter F, Michel C, Ruhrmann S, Schimmelmann BG. Prevalence and clinical significance of DSM-5-attenuated psychosis syndrome in adolescents and young adults in the general population: the Bern Epidemiological At-Risk (BEAR) study. Schizophr. Bull. (2013) 40:1499–508. doi: 10.1093/schbul/sbt171
44. Lewis S, Morrison AP, Barkus E, Bentall R, Stirling J, Hopkins R, et al. Levels of distress in samples at risk of psychosis. Schizophr Bull (2005) 31:228.
45. Lee JY, Chung YC, Kim JM, Shin IS, Yoon JS, Kim SW. School counselors’ recognition of the ultra-high risk for psychosis. Psychiatry Investig (2018) 15:320–4. doi: 10.30773/pi.2017.06.19
46. Kelleher I, Harley M, Lynch F, Arseneault L, Fitzpatrick C, Cannon M. Associations between childhood trauma, bullying and psychotic symptoms among a school-based adolescent sample. Br J Psychiatry (2008) 193:378–82. doi: 10.1192/bjp.bp.108.049536
47. Karatzias T, Gumley A, Power K, O’Grady M. Illness appraisals and self-esteem as correlates of anxiety and affective comorbid disorders in schizophrenia. Compr Psychiatry (2007) 48:371–5. doi: 10.1016/j.comppsych.2007.02.005
48. Romm KL, Rossberg JI, Hansen CF, Haug E, Andreassen OA, Melle I. Self-esteem is associated with premorbid adjustment and positive psychotic symptoms in early psychosis. BMC Psychiatry (2011) 11:136. doi: 10.1186/1471-244X-11-136
49. Jang JH, Lee YJ, Cho SJ, Cho IH, Shin NY, Kim SJ. Psychotic-like experiences and their relationship to suicidal ideation in adolescents. Psychiatry Res (2014) 215:641–5. doi: 10.1016/j.psychres.2013.12.046
50. Yung AR, Phillips LJ, Yuen HP, Francey SM, McFarlane CA, Hallgren M, et al. Psychosis prediction:12-month follow-up of a high-risk (‘‘prodromal’’) group. Schizophr Res (2003) 60:21–32. doi: 10.1016/S0920-9964(02)00167-6
51. Garety PA, Kuipers E, Fowler D, Freeman D, Bebbington PE. A cognitive model of the positive symptoms of psychosis. Psychol Med (2001) 31:189–95. doi: 10.1017/S0033291701003312
52. Gaweda Ł, Holas P, Kokoszka A. Dysfunctional meta-cognitive beliefs and anxiety, depression and self-esteem among healthy subjects with hallucinatory-like experiences. Psychiatr Pol (2012) 46:933–49.
53. Chambers JA, Power KG, Durham RC. The relationship between trait vulnerability and anxiety and depressive diagnoses at long-term follow-up of Generalized Anxiety Disorder. J Anxiety Disord (2004) 18:587–607. doi: 10.1016/j.janxdis.2003.09.001
54. Prochwicz K, Kłosowska J. The interplay between trait anxiety, cognitive biases and attentional control in healthy individuals with psychotic-like experiences. Psychiatry Res (2018) 259:44–50. doi: 10.1016/j.psychres.2017.09.085
55. Kaymaz N, Drukker M, Lieb R, Wittchen HU, Werbeloff N, Weiser M, et al. Do subthreshold psychotic experiences predict clinical outcomes in unselected non-help-seeking population-based samples? A systematic review and meta-analysis, enriched with new results. Psychol Med (2012) 42:2239–53. doi: 10.1017/S0033291711002911
56. De Loore E, Drukker M, Gunther N, Feron F, Deboutte D, Sabbe B, et al. Childhood negative experiences and subclinical psychosis in adolescence: a longitudinal general population study. Early Interv Psychiatry (2007) 1:201–7. doi: 10.1111/j.1751-7893.2007.00027.x
57. Mayo D, Corey S, Kelly LH, Yohannes S, Youngquist AL, Stuart BK. The role of trauma and stressful life events among individuals at clinical high risk for psychosis: a review. Front Psychiatry (2017) 8:55. doi: 10.3389/fpsyt.2017.00055
58. Lataster T, van Os J, Drukker M, Henquet C, Feron F, Gunther N, et al. Childhood victimisation and developmental expression of non-clinical delusional ideation and hallucinatory experiences: victimisation and non-clinical psychotic experiences. Soc Psychiatry Psychiatr Epidemiol. (2006) 41:423–8. doi: 10.1007/s00127-006-0060-4
59. Wolak J, Ybarra ML, Mitchell K, Finkelhor D. Current research knowledge about adolescent victimization via the Internet. Adolesc Med State Art Rev (2007) 18:325–41.
60. Tarrant M, North AC, Edridge MD, Kirk LE, Smith EA, Turner RE. Social identity in adolescence. J Adolesc (2001) 24:597–609. doi: 10.1006/jado.2000.0392
61. Tanti C, Stukas AA, Halloran MJ, Foddy M. Social identity change: shifts in social identity during adolescence. J Adolesc (2011) 34:555–67. doi: 10.1016/j.adolescence.2010.05.012
62. Jalbrzikowski M, Sugar CA, Zinberg J, Bachman P, Cannon TD, Bearden CE. Coping styles of individuals at clinical high risk for developing psychosis. Early Interv Psychiatry (2014) 8:68–76. doi: 10.1111/eip.12005
63. Kim KR, Song YY, Park JY, Lee EH, Lee M, Lee SY, et al. The relationship between psychosocial functioning and resilience and negative symptoms in individuals at ultra-high risk for psychosis. Aust N Z J Psychiatry (2013) 47:762–71. doi: 10.1177/0004867413488218
64. Horan WP, Blanchard JJ. Emotional responses to psychosocial stress in schizophrenia: the role of individual differences in affective traits and coping. Schizophr Res (2003) 60:271–83. doi: 10.1016/S0920-9964(02)00227-X
65. Ritsner MS, Gibel A, Ponizovsky AM, Shinkarenko E, Ratner Y, Kurs R. Coping patterns as a valid presentation of the diversity of coping responses in schizophrenia patients. Psychiatry Res (2006) 144:139–52. doi: 10.1016/j.psychres.2005.09.017
Keywords: psychotic-like experience, internet use, stress, coping, anxiety, depression
Citation: Lee J-Y, Ban D, Kim S-Y, Kim J-M, Shin I-S, Yoon J-S and Kim S-W (2019) Negative Life Events and Problematic Internet Use as Factors Associated With Psychotic-Like Experiences in Adolescents. Front. Psychiatry 10:369. doi: 10.3389/fpsyt.2019.00369
Received: 11 January 2019; Accepted: 13 May 2019;
Published: 29 May 2019.
Edited by:
Lex Wunderink, GGZ Friesland, NetherlandsReviewed by:
Michael W. Best, Queen’s University, CanadaStefanie Julia Schmidt, Universität Bern, Switzerland
Copyright © 2019 Lee, Ban, Kim, Kim, Shin, Yoon and Kim. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sung-Wan Kim, c3draW1AY2hvbm5hbS5hYy5rcg==