 Pavel Knytl1,2
Pavel Knytl1,2 Veronika Voráčková1,2
Veronika Voráčková1,2 Aneta Dorazilová1,3
Aneta Dorazilová1,3 Mabel Rodriguez1,4
Mabel Rodriguez1,4 Aneta Cvrčková1,5
Aneta Cvrčková1,5 Edita Kofroňová6
Edita Kofroňová6 Martin Kuchař1,6
Martin Kuchař1,6 Zuzana Kratochvílová1
Zuzana Kratochvílová1 Petra Šustová1
Petra Šustová1 Silvie Čerešňáková1,7
Silvie Čerešňáková1,7 Pavel Mohr1,2*
Pavel Mohr1,2*- 1National Institute of Mental Health, Klecany, Czechia
- 2Third Faculty of Medicine, Charles University, Prague, Czechia
- 3Faculty of Arts, Masaryk University, Brno, Czechia
- 4Faculty of Arts, Charles University, Prague, Czechia
- 5Faculty of Social Studies, Masaryk University, Brno, Czechia
- 6University of Chemistry and Technology, Prague, Czechia
- 7First Faculty of Medicine, Charles University, Prague, Czechia
Background: Neuroactive steroids (NAS) affect neurotransmitter systems and cognition; thus, they play role in etiopathogenesis of psychiatric disorders.
Aims: The primary aim was to examine cognition and effects of NAS on cognitive functioning in first-episode psychosis patients and in their healthy siblings. The secondary aims were to verify whether cognitive deficit is an endophenotype of psychosis and whether higher NAS levels represent a high-risk factor for psychosis.
Methods: Studied participants were 1) patients with first episode of psychosis, 2) healthy siblings of the patients, and 3) matching healthy controls. Study procedures included administration of a battery of neuropsychological tests assessing six cognitive domains and examination of NAS plasma levels [cortisol (CORT), 11-deoxycorticosterone (DOC), testosterone (TEST), dehydroepiandrostendione (DHEA), dihydrotestosterone (DHT), and progesterone (PROG)].
Results: A total of 67 subjects were analyzed (16 patients, 22 siblings, and 29 controls). Significant group differences were found in most of the cognitive domains; the patients had the lowest scores. The Kruskal–Wallis test revealed significant group differences in CORT levels (p < 0.01), TEST (p < 0.01), and DHT (p < 0.001); no difference was found in PROG, DHEA, and DOC. All cognitive domains, except for attention, were affected by the NAS levels. CORT levels of patients correlated with speed of processing (r = 0.55) and working memory (r = 0.52), while PROG levels correlated with abstraction (r = −0.63). In siblings, there was a negative correlation between TEST levels and verbal memory (r = −0.51) and PROG with attention (r = −0.47).
Conclusions: Our results verified that individual domains of cognitive deficit (abstraction and verbal memory) can be considered as an endophenotype of psychosis. Higher levels of cortisol and testosterone in siblings are consistent with high-risk states for psychosis. Multiple interactions between NAS and cognitive functioning, particularly memory functions, were observed. Study limitations (small sample size and administration of antipsychotic medication) did not allow us to establish unequivocally NAS as an endophenotype.
Introduction
Complex etiopathological mechanisms of schizophrenia are still poorly understood and their key features are yet to be identified. The widely cited dopaminergic theory (1) seems to be just an ending point of several pathophysiological processes in which other neurotransmitter systems (e.g., glutamatergic, GABAergic, and serotoninergic) are involved, as well (2–4).
In addition to other factors, neurotransmission is significantly affected by steroid substances synthetized in the central nervous system (CNS), labeled as “neurosteroids” (5, 6). A more general term, “neuroactive steroids” (NAS) is used for all substances that interact with the CNS in two different modes. First, genomically, through binding with intracellular steroid receptors, NAS can change gene expression. Second, interacting with membrane neurotransmitter receptors, NAS can modulate psychopathology of psychiatric disorders (7, 8). NAS may exhibit therapeutic potential, and their antidepressant, anxiolytic, and antipsychotic effects have been reported (9–11). Targeting NAS metabolism is considered as a novel therapeutic approach (12–14). Alterations of NAS are currently being studied intensively to investigate their role in the pathophysiology of schizophrenia, with an accumulating amount of evidence suggesting their involvement (12, 15, 16). However, the findings are not consistent, mostly due to the treatment, age, or gender effects (17–19).
Studies showed that early intervention can improve outcome of schizophrenia patients (20, 21). Therefore, prodromal phases of psychotic disorders are the focus of current research efforts (22). Healthy siblings of schizophrenia patients are a well-defined population at higher risk of developing illness (23). One promising approach on how to investigate etiopathogenesis of psychiatric disorders is through endophenotypes (24). Endophenotypes are state independent, observed in actively manifested illness or in remission and are present in healthy relatives of patients, but not in the general population.
Various candidate endophenotypes of schizophrenic disorder have been proposed, e.g., structural changes of the white and grey brain matter, biochemical blood markers, neurophysiological measures, or impairment of cognitive and social functioning (25). Cognitive deficit was also consistently observed in a population at risk of psychosis (26). A recent meta-analysis found a correlation between cognitive impairment and metabolic syndrome, suggesting an effect of metabolic alteration on cognition (27).
Several studies linked NAS to cognitive functioning of schizophrenia spectrum patients (28). NAS were also examined as candidate adjunctive agents for treatment of cognitive impairment in schizophrenia (29, 30). However, there are so far no data on the relationship of NAS and cognition among high-risk individuals.
The primary aim of our study was to examine the differences in cognitive performance of first-episode patients with psychosis, their siblings, and healthy controls. The secondary goal was to examine the effect of NAS on cognition, in order to verify whether cognitive deficit is an endophenotype of psychosis and whether higher levels of NAS represent a high-risk factor for psychotic disorder.
Materials and Methods
Study Sample
The study was conducted at the National Institute of Mental Health, Czechia. The study sample consisted of three groups of subjects: (1) first-episode psychosis patients; (2) their unaffected siblings; and (3) matching healthy controls. Patients met the International Statistical Classification of Diseases and Related Health Problems, 10th revision (ICD-10), criteria for schizophrenia (F20.x), acute psychosis (F23.x), or schizoaffective disorder (F25.x), first episode (31). Siblings and the control group were assessed with the Mini International Neuropsychiatric Interview (MINI) to rule out any current or past psychiatric disorders. Exclusion criteria in all groups were organic brain disorder, neurological or endocrine disease, substance dependence, intellectual disability, motor or perceptual handicap, and incapacity to provide informed consent. The study protocol was approved by the local ethical committee, and all subjects signed an informed consent form.
Study Procedures
Basic demographic and clinical data, sex, age, education, medical history, family history, and duration of untreated psychosis were recorded. Severity of psychotic symptoms in the patient group was assessed with the Positive and Negative Syndrome Scale (PANSS) and the Clinical Global Impression (CGI). Patients were assessed during the non-acute phase of their illness (CGI ≤ 4). The MINI was used to examine psychiatric comorbidity among patients and to verify the absence of psychiatric disorder in siblings and healthy controls.
Cognitive tests were administered by trained psychologists, using both pencil-paper and computer methods. Composition of the neuropsychological battery was based on the expert consensus and our previous research (32, 33). The battery evaluated cognitive functions in the following six domains: psychomotor speed/speed of processing [tested with Verbal Fluency Test; Stroop Test: word, color; Trail Making Test (TMT) A; Wechsler Adult Intelligence Scale (WAIS-III): digit–symbol coding]; attention (Continuous Performance Task); working memory/flexibility [WAIS-III: digit span; WAIS-III: letter–number sequencing; Wechsler Memory Scale (WMS-III): spatial span; TMT-B; Stroop Test: color word]; verbal memory (Auditory Verbal Learning Test, WMS-III: logical memory); visual memory (Rey–Osterrieth Complex Figure Test), and abstraction (WAIS-III: similarities; WAIS-III: comprehension; Picture arrangement; Wisconsin Card Sorting Test; Tower of London). For a detailed description and calculation of the composition and consistency of cognitive domains, see Rodriguez et al. (33). Participants were tested in two consecutive sessions with a break in between, and maximum time of psychological assessment was 120 min.
All subjects had their blood samples taken after 12 h of fasting; females were in the follicular phase of their menstrual cycle. NAS that previously showed an impact on the cognition of schizophrenia patients were assessed (28, 34–38). Plasma levels of cortisol (CORT), 11-deoxycorticosterone (DOC), testosterone (TEST), dehydroepiandrostendione (DHEA), dihydrotestosterone (DHT), and progesterone (PROG) were analyzed with liquid chromatography and mass spectroscopy in laboratories of the University of Chemistry and Technology in Prague.
Statistical Analysis
Fisher’s exact test was used to detect possible differences in distribution of sex and education between the groups. Non-parametric Kruskal–Wallis test and epsilon squared as effect size were used to assess the age differences to compare cognitive performance between the groups and for the group comparison of the NAS levels. The Dunn test was used for the post hoc multiple comparison; p-values were adjusted with the Benjamini–Hochberg method. Non-parametric version of analysis of covariance (ANCOVA) was used to examine possible differences in the NAS levels between the groups in relation to cognitive performance. For statistical analyses, R software version 3.3.2 was used.
Results
Study Sample
The total number of enrolled subjects was 74 (22 patients, 23 siblings, and 29 controls). Six patients and one sibling were excluded from the analyses due to the following reasons: manifested psychotic symptoms during cognitive testing, non-native Czech speaker, history of multiple episodes, and incorrect diagnosis. Analyzed study sample included 67 subjects: 16 first-episode patients, 22 siblings, and 29 healthy controls. There was no significant group difference in sex ratio (Fisher’s exact test: p = 0.535; Cramer’s V = 0.14), education (Fisher’s exact test: p = 0.09; Cramer’s V = 0.32), or age [Kruskal–Wallis test: H(2) = 2.95, p = 0.23; ε2 = 0.05]. For details, see Table 1.
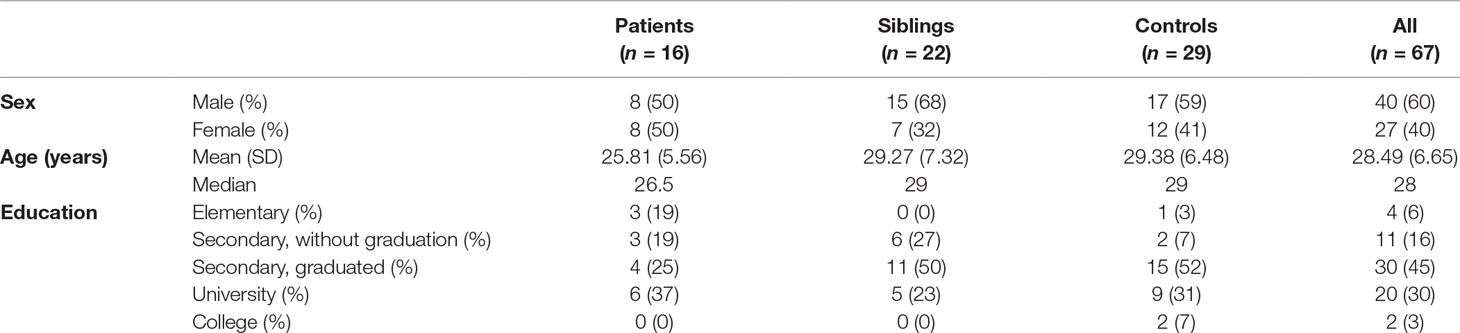
Table 1 Study sample, demographic characteristics.
Data on the patients’ psychiatric history (duration of illness, duration of untreated psychosis, length of antipsychotic treatment, and drug dosage in chlorpromazine equivalents) are shown in Table 2. Except for one patient, all of them were treated with antipsychotic medication. Fourteen were given oral monotherapy (for 7 subjects olanzapine 10–30 mg p.d.; 4 risperidone 3–4.5 mg p.d.; 1 aripiprazole 15 mg p.d.; 1 clozapine 175 mg p.d.; and 1 patient quetiapine 500 mg p.d). Four patients were prescribed a combination of two oral drugs (olanzapine 25 mg + haloperidol 6 mg; olanzapine 30 mg + aripiprazole 30 mg; and aripiprazole 15 mg + clozapine 150 mg), and four subjects were administered long-acting injectable antipsychotics (for 2 patients paliperidone 150 mg monthly; 1 olanzapine 300 mg biweekly; and 1 flupenthixol 40 mg monthly).
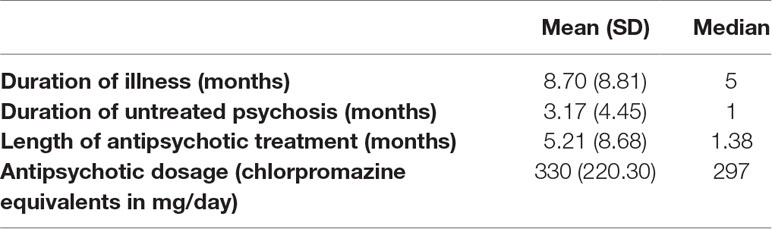
Table 2 Psychiatric history of the patients.
Cognition
Mean and median values of Z-scores for each of the cognitive domains are summarized in Table 3. Significant group differences were found in most of the cognitive domains, with the exception of attention. Kruskal–Wallis test: visual memory [H(2) = 12.67, p < 0.01, ε2 = 0.19]; verbal memory [H(2) = 15.38, p < 0.001, ε2 = 0.24]; abstraction [H(2) = 10.09, p < 0.01, ε2 = 0.15]; psychomotor speed [H(2) = 6.66, p < 0.05, ε2 = 0.1]; working memory [H(2) = 8.75, p < 0.05, ε2 = 0.13]; attention [H(2) = 1.39, p > 0.05, ε2 = 0.02].
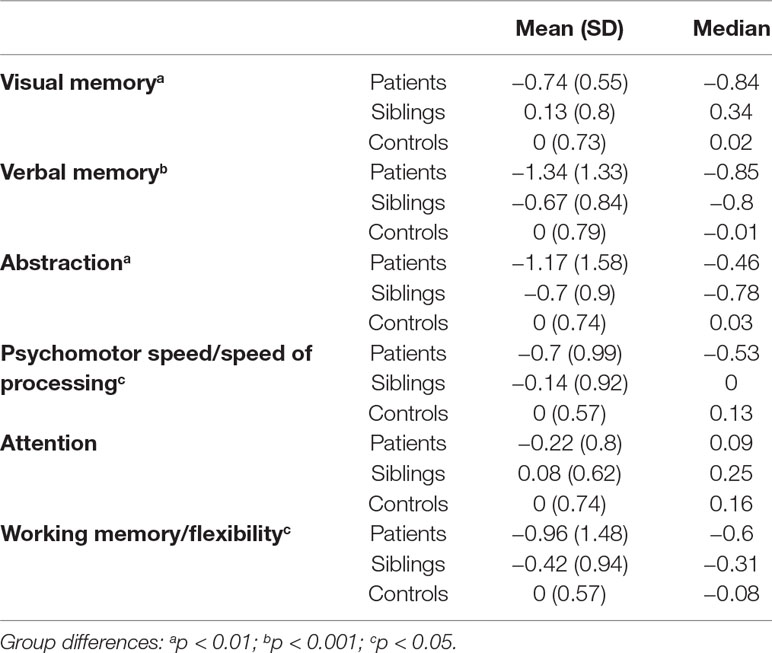
Table 3 Descriptive characteristics of cognitive domains (z-scores).
Results of the post hoc Dunn test with the Benjamini–Hochberg correction (median values listed in Table 3) revealed that visual memory performance of controls was statistically superior to that of patients (p < 0.05), performance of siblings was significantly better than that of patients (p < 0.05), and no difference between siblings and controls was observed. In verbal memory, controls performed significantly better than patients (p < 0.001) and siblings (p < 0.01), but no difference was detected between patients and siblings. In abstraction, controls performed significantly better than patients (p < 0.05) and siblings (p < 0.05), but no difference was found between patients and siblings. In psychomotor speed/speed of processing, control subjects outperformed significantly patients (p < 0.05), while no significant difference was observed between controls and siblings or between patients and siblings. In working memory/flexibility, control subjects performed significantly better than patients (p < 0.05), but no significant differences were detected between controls and siblings and between patients and siblings.
Neuroactive Steroids
Mean and median values of plasma levels of the analyzed NAS (CORT, DOC, TEST, DHEA, DHT, and PROG) are summarized in Table 4. Kruskal–Wallis test revealed significant differences between the groups in CORT levels [H(2) = 11.77, p < 0.01, ε2 = 0.18], TEST [H(2) = 11.57, p < 0.01, ε2 = 0.18] and DHT [H(2) = 16.69, p < 0.001, ε2 = 0.25]. No differences were found in levels of PROG [H(2) = 0.30, p > 0.05, ε2 = 0.005], DHEA [H(2) = 3.66, p > 0.05, ε2 = 0.06], and DOC [H(2) = 5.19, p > 0.05, ε2 = 0.08].
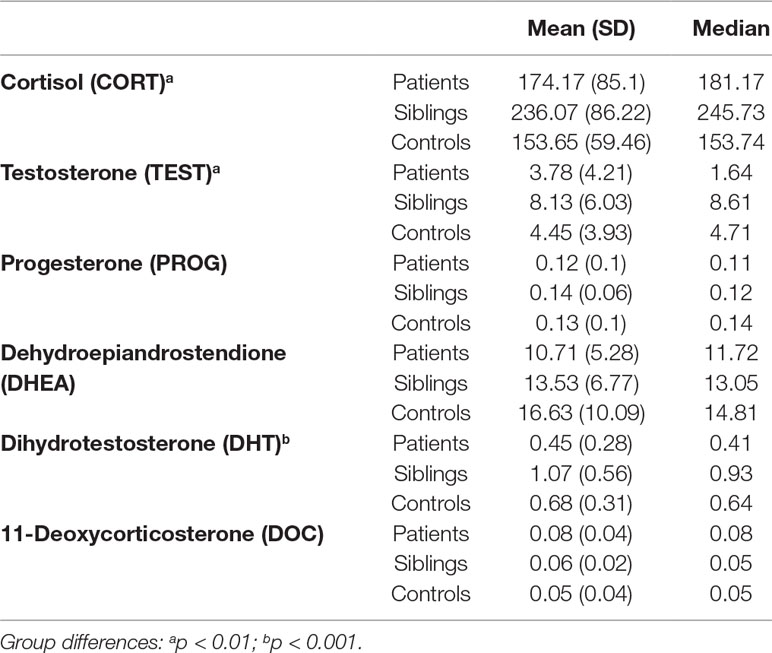
Table 4 Plasma levels of the selected neuroactive steroids (ng/ml).
Post hoc multiple comparisons (Dunn test) and adjustments with the Benjamini–Hochberg correction (median values listed in Table 4) found that CORT levels were significantly higher in siblings than in controls (p < 0.01), while no differences in CORT were detected between patients and siblings and between patients and controls. TEST levels were significantly higher in siblings than in both controls (p < 0.01) and patients (p < 0.01), but no difference was observed between patients and controls. Levels of DHT were significantly higher in siblings than in controls (p < 0.05) and in patients (p < 0.001), but DHT levels were significantly higher in controls than in patients (p < 0.05).
Effect of Neuroactive Steroids on Cognition
The relationship of NAS with cognition across the study groups was tested with non-parametric ANCOVA. For CORT, equality was rejected for verbal memory (test of equality: p = 0.0185), visual memory (p = 0.0374), and working memory (p = 0.0179) but not for speed of processing (p = 0.0744), abstraction (p = 0.1991), and attention (p = 0.2856). Parallelism was rejected for verbal memory (test of parallelism: p = 0.0097) and working memory (p = 0.012) but not for visual memory (p = 0.1092).
In TEST analysis, equality was rejected for verbal memory (p = 0.0303), visual memory (p = 0.0109), and abstraction (p = 0.0118) but not for speed of processing (p = 0.1636), working memory (p = 0.0563), and attention (p = 0.4698). Parallelism was rejected for verbal memory (p = 0.0177), visual memory (p = 0.0108), and abstraction (p = 0.0095) but not for speed of processing (p = 0.1096) and attention (p = 0.4976).
In PROG, equality was rejected for visual memory (p = 0.027) and abstraction (p = 0.0108) but not verbal memory (p = 0.1665), speed of processing (p = 0.25), working memory (p = 0.3633), and attention (p = 0.8943). Parallelism was rejected for abstraction (p = 0.0076) but not visual memory (p = 0.0736).
In DHEA, equality was rejected for verbal memory (p = 0.0456) and visual memory (p = 0.016) but not for speed of processing (p = 0.593), abstraction (p = 0.0814), attention (p = 0.5217), and working memory (0.6568). Parallelism was rejected for verbal memory (p = 0.0445) and visual memory (p = 0.024).
In DHT, equality was rejected for verbal memory (p = 0.0055), visual memory (p = 0.0149), speed of processing (p = 0.0146), abstraction (p = 0.0063), and working memory (p = 0.022) but not for attention (0.5326). Parallelism was rejected for verbal memory (p = 0.0054), visual memory (p = 0.0143), speed of processing (p = 0.0115), abstraction (p = 0.0066), and working memory (p = 0.0112).
In DOC, equality was rejected for verbal memory (p = 0.0095) and visual memory (p = 0.024) but not for speed of processing (p = 0.1703), abstraction (p = 0.1164), attention (p = 0.524), and working memory (0.793). Parallelism was rejected for verbal memory (p = 0.0081) and visual memory (p = 0.044).
Significant positive correlations of NAS with cognition in patients were found between the cortisol levels and speed of processing (r = 0.55), and working memory (r = 0.52), and negative correlations were found between progesterone and abstraction (r = −0.63) (Table 5). In siblings, there was a negative correlation between testosterone and verbal memory (r = −0.51) and between progesterone and attention (r = −0.47) (Table 6). No significant correlation was observed in healthy controls.

Table 5 Correlations between neurosteroid levels and domains of cognition—patients.
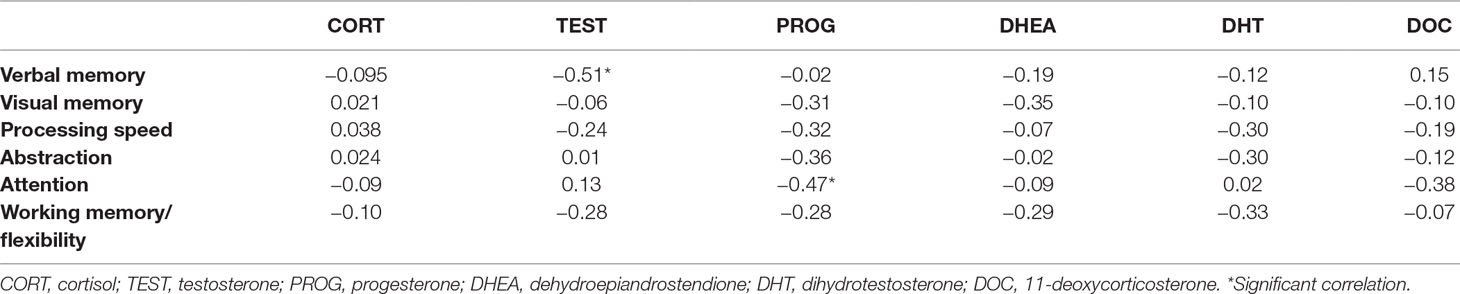
Table 6 Correlations between neurosteroid levels and domains of cognition—siblings.
Discussion
Our results confirmed the presence of global cognitive deficit in first-episode schizophrenia patients (FES). This finding, impaired cognition across all studied domains, as compared with healthy controls, is in full agreement with published research (39, 40). Additionally, functional correlates of cognitive deficit in FES have been reported recently (41). Cognitive dysfunction, albeit less pronounced than in patients, has been previously described among healthy first-degree relatives as well (42). Cognitive functioning is therefore considered as one of the most consistent endophenotypes of psychotic disorders (43).
Notably, our results strongly suggest that the endophenotype is not the global cognitive functioning but more likely individual, specific domains of cognition. We found verbal memory and abstraction significantly impaired in both patients and siblings compared with controls. Moreover, the performance in verbal memory and abstraction did not differ between patients and siblings; thus, both domains can be viewed as candidate intermediate endophenotypes (26, 44). The results further corroborate findings of other authors who identified executive control functions (i.e., abstraction and flexibility) and verbal memory as the most impaired cognitive domains that did not differ between unaffected siblings and patients with psychotic or bipolar disorder (42, 45, 46).
Analysis of NAS revealed significantly higher plasma levels of cortisol, testosterone, and dihydrotestosterone in siblings as compared with healthy controls. Siblings also had higher levels of testosterone and dihydrotestosterone than had patients. Somewhat surprisingly, no difference in NAS between patients and controls was observed, except for the higher levels of DHT in controls. Since all FES were already treated with antipsychotics, an effect of medication on steroid levels cannot be completely ruled out. Previous studies demonstrated the impact of second-generation antipsychotics on NAS levels in rodent models (17, 47). Decreased testosterone in our FES group can hence be related to administration of antipsychotic drugs (48). While the small number of patients in our study and the heterogeneity of drugs used do not allow more detailed analysis of the impact of specific antipsychotics on the NAS levels, it should be acknowledged that the length of drug treatment was in fact very short (median 1.38 months).
Observed higher levels of testosterone and its active metabolite dihydrotestosterone among healthy siblings seem to be in contrast to previously reported data (49). Nonetheless, in some models, high testosterone has been associated with a hyperdopaminergic state, a presumptive high-risk state for development of psychosis (50, 51). A recent meta-analysis also confirmed higher testosterone levels in FES (15). Increased levels of cortisol in siblings are consistent with published literature, since higher cortisol levels have been repeatedly found among high-risk populations (52, 53) and are associated with higher transition rate into psychosis (54).
Cognition is a very intricate and complex neural process, based on synaptic plasticity, connectivity, and density. Various agents, including neurosteroids, can affect its neurodevelopment (55). It has been discussed that particularly DHEA and its sulfate conjugate play an important role in the development, neuroprotection, and restoration of neuronal characteristics through aging, although the studies with supplementation demonstrated only a small effect (56).
Despite the small sample size, we were able to identify several interactions between the cognitive performance and neurosteroids. The only cognitive domain not affected by steroid levels was attention. The most notable impact of NAS was on all domains of memory functions: Verbal memory was significantly influenced by CORT, TEST, DHEA, DHT, and DOC; visual memory by CORT, TEST, PROG, DHEA, DHT, and DOC; and working memory by CORT and DHT. Abstraction interacted with TEST, PROG, and DHT, and speed of processing interacted only with DHT. Similarly, other authors consistently reported positive effects of testosterone on memory function (including enhancement of hippocampal plasticity), and the effects of progesterone differ according to acute or chronic administration (55, 57).
While no significant correlation was observed in healthy individuals, cortisol levels in patients were associated with better performance in processing speed and working memory, which is in contrast with previous findings that associated higher CORT levels with poorer cognitive performance (34, 35, 58). Progesterone levels in patients were negatively associated with abstraction. In siblings, testosterone correlated negatively with verbal memory and progesterone with attention. The role of progesterone is rarely investigated; a single study identified a correlation between PROG and cognitive functioning in male schizophrenia patients (38).
Previous findings in healthy subjects underlined the higher impact of NAS on cognition in men than in women (59). For example, the role of testosterone in cognitive impairment has been discussed in male patients with schizophrenia only (37). Clearly, the effects of NAS levels on cognitive functioning should be interpreted according to gender. Due to the limited sample size, we were not able to analyze the gender difference in study groups.
In summary, we were able to endorse cognitive deficit as an endophenotype of psychotic disorder. While the results are still preliminary, the major finding is the observation that most likely not a global dysfunction but individual domains of cognition (i.e., abstraction and verbal memory) might be the foundation of cognitive endophenotype. Impairment in specific cognitive domains is shared by both first-episode patients and their healthy siblings and distinguishes them from the general population.
There are several study limitations (primarily small sample size, cross-sectional design without follow-up, and patients who were not drug naive) that prevent us from any generalization of neurosteroid data and do not allow for their plasma levels to be established unequivocally as an endophenotype of schizophrenia. We were not able to verify or reject steroid metabolome as a diagnostic tool, as suggested previously (60). Nevertheless, higher levels of cortisol and testosterone in siblings are consistent with high-risk states for psychosis, and cortisol levels are associated with higher transition rates to fully develop psychosis. Finally, our study results revealed in both patients and siblings multiple interactions between NAS and cognitive functioning, especially memory functions. If replicated in a larger study sample, this observation could have potential implications for timely therapeutic interventions in high-risk individuals, prodromal phases, and early phases of psychotic disorders.
Ethics Statement
The study protocol was approved by the Ethical Committee of the National Institute of Mental Health, Czechia. All study subjects signed an informed consent form.
Author Contributions
PK collected clinical and biochemical data, recruited subjects, and drafted the manuscript. VV collected and analyzed neuropsychological data and recruited subjects. AD and PS collected neuropsychological data. MR designed neuropsychological testing and interpreted cognitive data. AC performed statistical analyses. EK and MK analyzed biochemical samples. ZK designed neuropsychological testing. SC collected clinical data. PM drafted the study design, interpreted the results, and drafted the manuscript.
Funding
The study was supported by grant from the Czech Ministry of Health, no. AZV 15-28998A; by grant from the Czech Science Foundation, no. 16-13093S; and by the project NPU4NUDZ LO1611 of the Czech Ministry of Education, Youth and Sports.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Howes OD, Kapur S. The dopamine hypothesis of schizophrenia: version III—the final common pathway. Schizophr Bull (2009) 35(3):549–62. doi: 10.1093/schbul/sbp006
2. Coyle JT. Glutamate and schizophrenia: beyond the dopamine hypothesis. Cell Mol Neurobiol (2006) 26(4–6):365–84. doi: 10.1007/s10571-006-9062-8
3. Taylor SF, Tso IF. GABA abnormalities in schizophrenia: a methodological review of in vivo studies. Schizophr Res (2015) 167(1–3):84–90. doi: 10.1016/j.schres.2014.10.011
4. Eggers AE. A serotonin hypothesis of schizophrenia. Med Hypotheses (2013) 80(6):791–4. doi: 10.1016/j.mehy.2013.03.013
5. Baulieu EE. Steroid hormones in the brain: several mechanisms. In: Fuxe K, Gustafson JA, Wetterberg L, editors. Steroid hormone regulation of the brain. New York: Pergamon Press (1981). p. 3–14. doi: 10.1016/B9780-08-026864-4.50007-4
6. Banga PV, Patil CY, Deshmukh GA, Chandaliya KC, Baig MS, Doifode SM. Biosynthesis, mechanism of action and clinical importance of neuroactive steroids: pearls from literature. Int J Nutr Pharmacol Neurol Dis (2013) 3(2):77–86. doi: 10.4103/2231-0738.112826
7. Tuem KB, Atey TM. Neuroactive steroids: receptor interactions and responses. Front Neurol (2017) 8:442. doi: 10.3389/fneur.2017.00442
8. Dubrovsky BO. Steroids, neuroactive steroids and neurosteroids in psychopathology. Prog Neuropsychopharmacol Biol Psychiatry (2005) 29(2):169–92. doi: 10.1016/j.pnpbp.2004.11.001
9. Uzunova V, Sampson L, Uzunov DP. Relevance of endogenous 3alpha-reduced neurosteroids to depression and antidepressant action. Psychopharmacology (2006) 186:351–61. doi: 10.1007/s00213-005-0201-6
10. Longone P, di Michele F, D’Agati E, Romeo E, Pasini A, Rupprecht R. Neurosteroids as neuromodulators in the treatment of anxiety disorders. Front Endocrinol (2011) 2:55. doi: 10.3389/fendo.2011.00055
11. Ugale RR, Hirani K, Morelli M, Chopde CT. Role of neuroactive steroid allopregnanolone in antipsychotic-like action of olanzapine in rodents. Neuropsychopharmacology (2004) 29:1597–609. doi: 10.1038/sj.npp.1300460
12. Cai HL, Cao T, Zhou X, Yao JK. Neurosteroids in schizophrenia: pathogenic and therapeutic implications. Front Psychiatry (2018) 9:73. doi: 10.3389/fpsyt.2018.00073
13. Ritsner MS. The clinical and therapeutic potentials of dehydroepiandrosterone and pregnenolone in schizophrenia. Neuroscience (2011) 191:91–100. doi: 10.1016/j.neuroscience.2011.04.017
14. Cai H, Zhou X, Dougherty GG, Reddy RD, Haas GL, Montrose DM, et al. Pregnenolone-progesterone-allopregnanolone pathway as a potential therapeutic target in first-episode antipsychotic-naïve patients with schizophrenia. Psychoneuroendocrinology (2018) 90:43–51. doi: 10.1016/j.psyneuen.2018.02.004
15. Misiak B, Frydecka D, Loska O, Moustafa AA, Samochowiec J, Kasznia J, et al. Testosterone, DHEA and DHEA-S in patients with schizophrenia: a systematic review and meta-analysis. Psychoneuroendocrinology (2018) 89:92–102. doi: 10.1016/j.psyneuen.2018.01.007
16. Ritsner MS. Pregnenolone, dehydroepiandrosterone, and schizophrenia: alterations and clinical trials. CNS Neurosci Ther (2010) 16(1):32–44. doi: 10.1111/j.1755-5949.2009.00118.x
17. Marx CE, VanDoren MJ, Duncan GE, Lieberman JA, Morrow AL. Olanzapine and clozapine increase the GABAergic neuroactive steroid allopregnanolone in rodents. Neuropsychopharmacology (2003) 28(1):1–13. doi: 10.1038/sj.npp.1300015
18. Nechmad A, Maayan R, Ramadan E, Morad O, Poyurovsky M, Weizman A. Clozapine decreases rat brain dehydroepiandrosterone and dehydroepiandrosterone sulfate levels. Eur Neuropsychopharmacol (2003) 13:29–31. doi: 10.1016/S0924-977X(02)00077-9
19. Hill M, Lukáč D, Lapčík O, Sulcová J, Hampl R, Pouzar V, et al. Age relationships and sex differences in serum levels of pregnenolone and 17-hydroxypregnenolone in normal subjects. Clin Chem Lab Med (2005) 37(4):439–47. doi: 10.1515/CCLM.1999.072
20. Cechnicki A, Hanuszkiewicz I, Polczyk R, Bielańska A. Prognostic value of duration of untreated psychosis in long-term outcome of schizophrenia. Med Sci Monit (2011) 17(5):CR277–283. doi: 10.12659/MSM.881768
21. Addington J, Van Mastrigt S, Addington D. Duration of untreated psychosis: impact on 2-year outcome. Psychol Med (2004) 34(2):277–84. doi: 10.1017/S0033291703001156
22. McGorry PD. Early intervention in psychosis: obvious, effective, overdue. J Nerv Ment Dis (2015) 203(5):310–8. doi: 10.1097/NMD.0000000000000284
23. Waddington JL, Corvin AP, Donohoe G, O’Tuathaigh CMP, Mitchell KJ, Gill M. Functional genomics and schizophrenia: endophenotypes and mutant models. Psychiatr Clin North Am (2007) 30(3):365–99. doi: 10.1016/j.psc.2007.04.011
24. Gottesman II, Gould TD. The endophenotype concept in psychiatry: etymology and strategic intentions. Am J Psychiatry (2003) 160(4):636–45. doi: 10.1176/appi.ajp.160.4.636
25. Allen AJ, Griss ME, Folley BS, Hawkins KA, Pearlson GD. Endophenotypes in schizophrenia: a selective review. Schizophr Res (2009) 109(1–3):24–37. doi: 10.1016/j.schres.2009.01.016
26. Hou CL, Xiang YT, Wang ZL, Everall I, Tang Y, Yang C, et al. Cognitive functioning in individuals at ultra-high risk for psychosis, first-degree relatives of patients with psychosis and patients with first-episode schizophrenia. Schizophr Res (2016) 174(1–3):71–6. doi: 10.1016/j.schres.2016.04.034
27. Bora E, Akdede BB, Alptekin K. The relationship between cognitive impairment in schizophrenia and metabolic syndrome: a systematic review and meta-analysis. Psychol Med (2017) 47(6):1030–40. doi: 10.1017/S0033291716003366
28. Ritsner MS, Strous RD. Neurocognitive deficits in schizophrenia are associated with alterations in blood levels of neurosteroids: a multiple regression analysis of findings from a double-blind, randomized, placebo-controlled crossover trial with DHEA. J Psychiatr Res (2010) 44(2):75–80. doi: 10.1016/j.jpsychires.2009.07.002
29. Kreinin A, Bawakny N, Ritsner MS. Adjunctive pregnenolone ameliorates the cognitive deficits in recent-onset schizophrenia: an 8-week, randomized, double-blind, placebo-controlled trial. Clin Schizophr Relat Psychoses (2017) 10(4):201–10. doi: 10.3371/CSRP.KRBA.013114
30. Strous RD, Stryjer R, Maayan R, Gal G, Viglin D, Katz E, et al. Analysis of clinical symptomatology, extrapyramidal symptoms and neurocognitive dysfunction following dehydroepiandrosterone (DHEA) administration in olanzapine treated schizophrenia patients: a randomized, double-blind placebo controlled trial. Psychoneuroendocrinology (2007) 32(2):96–105. doi: 10.1016/j.psyneuen.2006.11.002
31. World Health Organization. The ICD-10 classification of mental and behavioural disorders: clinical descriptions and diagnostic guidelines. Geneva: World Health Organization (1992).
32. Nuechterlein KH, Green MF, Kern RS, Baade LE, Barch DM, Cohen JD, et al. The MATRICS Consensus Cognitive Battery, part 1: test selection, reliability, and validity. Am J Psychiatry (2008) 165(2):203–13. doi: 10.1176/appi.ajp.2007.07010042
33. Rodriguez M, Fajnerová I, Sedláková K, Dorazilová A, Voráčková V, Paštrňák M, et al. Cluster analysis and correlations between cognitive domains: cognitive performance in a Czech sample of first episodes schizophrenia spectrum disorders—preliminary results. Psychiatrie (2017) 21(1):4–11.
34. Walder DJ, Walker EF, Lewine RJ. Cognitive functioning, cortisol release, and symptom severity in patients with schizophrenia. Biol Psychiatry (2000) 48:1121–32. doi: 10.1016/S0006-3223(00)01052-0
35. Havelka D, Prikrylova-Kucerova H, Prikryl R, Ceskova E. Cognitive impairment and cortisol levels in first-episode schizophrenia patients. Stress (2016) 19(4):383–9. doi: 10.1080/10253890.2016.1193146
36. Allott KA, Yuen HP, Bartholomeusz CF, Rapado-Castro M, Phassouliotis C, Butselaar F, et al. Stress hormones and verbal memory in young people over the first 12 weeks of treatment for psychosis. Psychiatry Res (2018) 260:60–6. doi: 10.1016/j.psychres.2017.11.044
37. Moore L, Kyaw M, Vercammen A, Lenroot R, Kulkarni J, Curtis J, et al. Serum testosterone levels are related to cognitive function in men with schizophrenia. Psychoneuroendocrinology (2013) 38(9):1717–28. doi: 10.1016/j.psyneuen.2013.02.007
38. Bratek A, Koźmin-Burzyńska A, Krysta K, Cierpka-Wiszniewska K, Krupka-Matuszczyk I. Effects of hormones on cognition in schizophrenic male patients—preliminary results. Psychiatr Danub (2015) 27(1):261–5.
39. Schaefer J, Giangrande E, Weinberger DR, Dickinson D. The global cognitive impairment in schizophrenia: consistent over decades and around the world. Schizophr Res (2013) 150(1):42–50. doi: 10.1016/j.schres.2013.07.009
40. Aas M, Dazzan P, Mondelli V, Melle I, Murray RM, Pariante CM. A systematic review of cognitive function in first-episode psychosis, including a discussion on childhood trauma, stress, and inflammation. Front Psychiatry (2014) 4:182. doi: 10.3389/fpsyt.2013.00182
41. Rodriguez M, Zaytseva Y, Cvrčková A, Dvořaček B, Dorazilová A, Jonáš J, et al. Cognitive profiles and functional connectivity in first-episode schizophrenia spectrum disorders: linking behavioural and neuronal data. Front Psychol (2019) 10:689. doi: 10.3389/fpsyg.2019.00689
42. Snitz BE, Macdonald AW, Carter CS. Cognitive deficits in unaffected first-degree relatives of schizophrenia patients: a meta-analytic review of putative endophenotypes. Schizophr Bull (2006) 32(1):179–94. doi: 10.1093/schbul/sbi048
43. Seidman LJ, Giuliano AJ, Meyer EC, Addington J, Cadenhead KS, Cannon TD, et al. Neuropsychology of the prodrome to psychosis in the NAPLS Consortium: relationship to family history and conversion to psychosis. Arch Gen Psychiatry (2010) 67(6):578–88. doi: 10.1001/archgenpsychiatry.2010.66
44. Chu AOK, Chang WC, Chan SKW, Lee EHM, Hui CLM, Chen EYH. Comparison of cognitive functions between first-episode schizophrenia patients, their unaffected siblings and individuals at clinical high-risk for psychosis. Psychol Med (2018) 18:1–8. doi: 10.1017/S0033291718002726
45. Cannon TD, Bearden CE, Hollister JM, Rosso IM, Sanchez LE, Hadley T. Childhood cognitive functioning in schizophrenia patients and their unaffected siblings: a prospective cohort study. Schizophr Bull (2000) 26(2):379–93. doi: 10.1093/oxfordjournals.schbul.a033460
46. Kulkarni S, Jain S, Janardhan Reddy YC, Kumar KJ, Kandavel T. Impairment of verbal learning and memory and executive function in unaffected siblings of probands with bipolar disorder. Bipolar Disord (2010) 12(6):647–56. doi: 10.1111/j.1399-5618.2010.00857.x
47. Barbaccia ML, Affricano D, Purdy RH, Maciocco E, Spiga F, Biggio G. Clozapine, but not haloperidol, increases brain concentrations of neuroactive steroids in the rat. Neuropsychopharmacology (2001) 25(4):489–97. doi: 10.1016/S0893-133X(01)00254-8
48. Roke Y, van Harten PN, Buitelaar JK, Tenback DE, de Rijke YB, Boot AM. Antipsychotic-induced hyperprolactinemia and testosterone levels in boys. Horm Res Paediatr (2012) 77(4):235–40. doi: 10.1159/000337910
49. van Rijn S, Aleman A, de Sonneville L, Sprong M, Ziermans T, Schothorst P, et al. Neuroendocrine markers of high risk for psychosis: salivary testosterone in adolescent boys with prodromal symptoms. Psychol Med (2011) 41(9):1815–22. doi: 10.1017/S0033291710002576
50. Sinclair D, Purves-Tyson TD, Allen KM, Weickert CS. Impacts of stress and sex hormones on dopamine neurotransmission in the adolescent brain. Psychopharmacology (Berl) (2014) 231(8):1581–99 doi: 10.1007/s00213-013-3415-z
51. Howes OD, Montgomery AJ, Asselin MC, Murray RM, Valli I, Tabraham P, et al. Elevated striatal dopamine function linked to prodromal signs of schizophrenia. Arch Gen Psychiatry (2009) 66(1):13–20. doi: 10.1001/archgenpsychiatry.2008.514
52. Carol EE, Mittal VA. Resting cortisol level, self-concept, and putative familial environment in adolescents at ultra high-risk for psychotic disorders. Psychoneuroendocrinology (2015) 57:26–36. doi: 10.1016/j.psyneuen.2015.03.018
53. Yıldırım O, Dogan O, Semiz M, Kilicli F. Serum cortisol and dehydroepiandrosterone-sulfate levels in schizophrenic patients and their first-degree relatives. Psychiatry Clin Neurosci (2011) 65:584–91. doi: 10.1111/j.1440-1819.2011.02252.x
54. Walker EF, Trotman HD, Pearce BD, Addington J, Cadenhead KS, Cornblatt BA, et al. Cortisol levels and risk for psychosis: initial findings from the North American prodrome longitudinal study. Biol Psychiatry (2013) 74(6):410–7. doi: 10.1016/j.biopsych.2013.02.016
55. Colciago A, Casati L, Negri-Cesi P, Celotti F. Learning and memory: steroids and epigenetics. J Steroid Biochem Mol Biol (2015) 150:64–85. doi: 10.1016/j.jsbmb.2015.02.008
56. Samaras N, Samaras D, Frangos E, Forster A, Philippe J. A review of age-related dehydroepiandrosterone decline and its association with well-known geriatric syndromes: is treatment beneficial? Rejuvenation Res (2013) 16(4):285–94. doi: 10.1089/rej.2013.1425
57. Halari R, Kumari V, Mehrotra R, Wheeler M, Hines M, Sharma T. The relationship of sex hormones and cortisol with cognitive functioning in Schizophrenia. J Psychopharmacol (2004) 18(3):366–74. doi: 10.1177/026988110401800307
58. MacLusky NJ, Hajszan T, Prange-Kiel J, Leranth C. Androgen modulation of hippocampal synaptic plasticity. Neuroscience (2006) 138(3):957–65. doi: 10.1016/j.neuroscience.2005.12.054
59. Chen CY, Wu CC, Huang YC, Hung CF, Wang LJ. Gender differences in the relationships among neurosteroid serum levels, cognitive function, and quality of life. Neuropsychiatr Dis Treat (2018) 14:2389–99. doi: 10.2147/NDT.S176047
Keywords: neuroactive steroids, cognition, endophenotype, siblings, psychosis
Citation: Knytl P, Voráčková V, Dorazilová A, Rodriguez M, Cvrčková A, Kofroňová E, Kuchař M, Kratochvílová Z, Šustová P, Čerešňáková S and Mohr P (2019) Neuroactive Steroids and Cognitive Functions in First-Episode Psychosis Patients and Their Healthy Siblings. Front. Psychiatry 10:390. doi: 10.3389/fpsyt.2019.00390
Received: 07 February 2019; Accepted: 17 May 2019;
Published: 18 June 2019.
Edited by:
Virginio Salvi, ASST Fatebenefratelli Sacco, ItalyReviewed by:
Gianluca Rosso, Ospedale San Luigi Gonzaga, ItalyMaria Salvina Signorelli, Università degli Studi di Catania, Italy
Copyright © 2019 Knytl, Voráčková, Dorazilová, Rodriguez, Cvrčková, Kofroňová, Kuchař, Kratochvílová, Šustová, Čerešňáková and Mohr. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Pavel Mohr, cGF2ZWwubW9ockBudWR6LmN6