 Chunyu Yang
Chunyu Yang You Zhou
You Zhou Mengfan Xia
Mengfan Xia- 1College of Law and Political Science, Nanjing University of Information Science and Technology, Nanjing, China
- 2School of Social and Behavioral Sciences, Nanjing University, Nanjing, China
- 3The Graduate School of Humanities and Social Science, University of Melbourne, Melbourne, VIC, Australia
Objectives: The existing studies found that resilience is a salient trait that can significantly affect people's psychological well-being with substance use disorders (SUDs). However, few studies examined how the mechanisms are connected between resilience and mental health among patients with Diagnostic and Statistical Manual of Mental Disorders—fifth edition SUD. This study investigated the mediation effects of positive affect, perceived social support, and self-esteem on the effect of resilience on perceived stress and life satisfaction in SUD patients.
Design: A total of 415 patients diagnosed with Diagnostic and Statistical Manual of Mental Disorders—fifth edition SUD from the south of China joined the research.
Outcome Measures: The study applied Connor–Davidson Resilience Scale, Positive and Negative Affect Scale, Multidimensional Scale of Perceived Social Support, Rosenberg Self-Esteem Scale, and Satisfaction with Life Scale to measure patients' resilience, positive affect, self-esteem, perceived social support, perceived stress, and life satisfaction.
Results: Structural equation model analysis revealed that positive affect and self-esteem partially mediate the relationship between resilience and perceived stress. In contrast, positive affect and perceived social support partially mediate the relationship between resilience and life satisfaction.
Conclusion: The findings provide insights for evidence-based substance abuse intervention that positive affect, self-esteem, and perceived social support can conditional the effects of resilience on promoting the mental health of SUD patients.
Background
Substance use disorders (SUDs) have been widely considered a global threat, posing enormous risks to individual well-being and cohesion of societies (1). As one of the overarching social problems, numerous studies have examined the correlations between SUD and psychological processes. Many studies show that perceived stress and life satisfaction are two prominent factors that play significant roles in influencing addiction severity and integral well-being (2).
Perceived stress is defined as individuals' cognitive appraisals over their stress level (3). Numerous addiction theories have depicted the theoretical linkage between perceived stress and substance abuse (4–6). For example, tension reduction theory (6) and self-medication hypothesis (5) postulate that chronic perceived stress is one of the primary motivations of taking illicit substances, which may temporarily alleviate psychological distress. Empirical findings also reveal that exposure to stress and post-traumatic stress disorder can increase illicit drug consumption level, frequency, and severity (7–11). Further, clinical observations suggest that substance users with higher perceived stress tend to report higher relapse rates (12, 13). Therefore, exploring the strategies to reduce perceived stress among people with SUD is of great importance for minimizing SUD's detrimental impacts and enlarging both the physical and mental well-being of people with SUD.
Life satisfaction is conceptualized as an individual's cognitive appraisal regarding their life's overall satisfaction (14). Life satisfaction has been used as a complementary method for assessing psychological well-being (15). Wide ranges of studies suggest that low life satisfaction is one of the salient predictors of some psychological disorders, including SUDs (2), anxiety (16), depression (17), and internet addiction disorders (18). Individuals with high life satisfaction report a lower level of substance abuse and mental health disorders (16). Life satisfaction has also been implemented as a diagnostic tool for SUD rehabilitation (19). Thus, exploring the potential mechanisms that boost life satisfaction among patients with SUD is crucial for combating the physical and psychological distress, promoting SUD rehabilitation processes.
Resilience
Resilience has been regarded as one of the most critical determinants closely correlated to perceived stress and life satisfaction (20, 21). The definitions of resilience are generally based around two concepts, adversities and positive adaptions, conceptualizing individuals' capacity to bounce back when exposed to ranges of misfortunes (22, 23). The recent studies tend to define resilience, beyond the scope of a trait, as a dynamic psychological process that is susceptible to demographic factors [e.g., population, time, and place; (24)] and tends to promote other psychological traits [e.g., affect balance, self-esteem, and perceived social support; (23, 25)].
The relationships among resilience, perceived stress, and life satisfaction have been well-documented. A substantial body of studies conducted in the populations of non-users have shown that individuals with a higher level of resilience are reported to have lesser perceived stress in life events (20, 26, 27). Studies also suggest that people with higher resilience tend to experience a higher level of life satisfaction (28). However, although theoretical and empirical studies have suggested the associations among resilience, perceived stress, and life satisfaction, few focused on exploring the underlying mechanisms among them, especially among patients with SUD.
Positive Affect, Self-Esteem, and Perceived Social Support as Mediators
Based on the existing theoretical and empirical studies, three items were the potential mediators in the impacts of resilience on perceived stress and life satisfaction. The first potential mediator is positive affect, whose definition was distinguished from positive emotion in history, but both have been used interchangeably nowadays (29, 30). Positive affect is conceptualized as the “pleasant ends” that can produce adaptive outcomes for flourishing individuals' mental and physical health (29). Fredrickson (31) suggests that positive affect is encompassed by the broaden-and-build theory (31–33), which denotes that positive affect can broaden mindsets by building enduring bio-psycho-social resources (e.g., social connections and coping methods), then achieving long-term adaptive outcomes such as happiness (34), psychological growth (35), creativity (36), immune function (37), reduction of an inflammatory response (38), and physical pain release (39). Studies have demonstrated that positive affect has an interactive relationship with resilience (40, 41) and life satisfaction (42, 43). Meanwhile, studies also identify that positive affect can significantly and effectively buffer the adverse impacts of perceived stress by widening thought–action repertoires, which facilitate generativity and behavioral flexibility (44). Based on theoretical and empirical studies, we hypothesized that positive affect would be the first mediator in the present study.
Extant studies indicate that self-esteem may be the second mediator. The widely accepted definition of self-esteem refers to the individual's general evaluation toward themselves (45, 46). However, there is a dispute regarding whether self-esteem is a component of resilience, the present study aligned with the mainstream perspectives which treat self-esteem as a separate concept (47–50). People with high self-esteem are motivated to maintain positive evaluations of themselves, further denoted by terror management theory (51). The theory depicts that self-esteem works as a buffer for anxiety-related events and various threats, promoting and maintaining a positive self-evaluation [e.g., (45, 51)].
Numerous empirical studies have shown that resilience can significantly facilitate self-esteem (25, 48, 52). Meanwhile, self-esteem is reported as a strong predictor of life satisfaction (45, 53, 54). Although rare attention has been paid to the association between self-esteem and perceived stress (55, 56), the terror management theory (51) posits that self-esteem is beneficial for preventing individuals from the impacts of the anxiety-related event, a salient predictor of perceived stress (57). Thus, the present study hypothesized that self-esteem is the second mediator in the impacts of resilience on perceived stress and life satisfaction in SUD patients.
Perceived social support is identified as the third mediator of the links. Although there is a statement that a supportive relationship is a key refinement of resilience, Pangello et al. (58) suggest that further research with regard to the overlaps between resilience and other concepts is needed, as the definitions and operationalizations of resilience are inconsistent. Therefore, the current research regarded perceived social support as an independent concept. Perceived social support reflects the individual's judgment over the general availability of support from relational and social boundaries (59).
The relationship between resilience and perceived social support has been documented by a wide range of studies (60–62). A majority of research focuses on examining the effects of perceived social support on resilience, suggesting that individuals with high perceived social support are reported with a higher level of resilience (60, 61, 63). A small group of studies explored how resilient people broaden their social networks and acquire supports from the established network. For example, Sexton et al. (64) suggested that resilient people are more likely to express their thoughts and find sympathetic friends, which are the salient factors for reducing psychological burdens (62). Furthermore, perceived social support has been identified with the roles of maintaining physical and mental well-being (65–69). Notably, groups of studies have found that people with high perceived social support are reported with a higher level of life satisfaction (70, 71), whereas some studies suggest that perceived social support has a negative association with perceived stress (72, 73). Based on the present observations, we hypothesized that perceived social support is the third mediator of the study.
Context of Substance Use Disorders
Many social studies emphasize that psychological processes are susceptible to contextual and situational factors (74, 75). SUD is one of the significant contextual factors that can contribute to a wide range of variances in an individual's biological homeostasis (76, 77), psychological states (78, 79), relational and social boundaries (80), occupational performance (81), and cultural beliefs (82).
The present study focused on examining how underlying associations are shaped between psychological traits and mental health within the context of SUD. People with SUD may suffer more physical, psychological, relational, and social difficulties and challenges than non-users. For example, due to discrimination and social exclusion, studies showed that people with SUD report a lower level of perceived social support than non-users (83). Also, the relationship between support-giver and patients has been altered by bio-power, formed through designated interventions (59). Therefore, how the psychological traits are associated with mental health within the context of SUD is uncertain.
Present Study
To reveal the uncertainties, the present study dedicated to examining whether positive affect, self-esteem, and perceived social support mediate the effects of resilience on perceived stress and life satisfaction, respectively. Based on the previous studies, we hypothesized that resilience exerts effects on perceived stress and life satisfaction via positive affect, self-esteem, and social support among people with SUD (Figure 1).
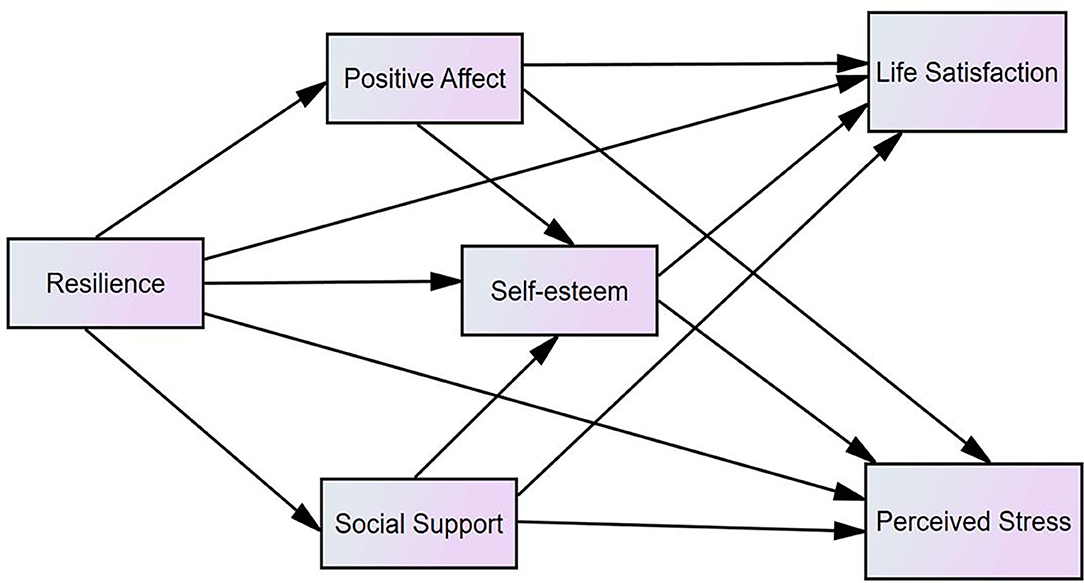
Figure 1. The hypothesized model (N = 415).
Methods
Participants and Design
The participants were comprised of 415 (322 males and 93 females, excluding one missing data) patients with SUD. All participants were recruited from two rehabilitation centers in the south of China. Nine demographic characteristics were measured in the study: age, sex, education, marital status, annual income, employment, months of detoxification, and substance types. The inclusion criteria of the study were as follows: age of 18 years or more, right-handed, normal color perception, regular and stable cognition, diagnosed with SUD within the last 12 months, and the voluntary willingness to participate. The exclusion criteria included: cognitive disabilities, psychiatric impairments, and a history of acute heart, kidney, and liver diseases, and the unwillingness to participate. As there were few missing values, we adopted listwise deletion for the cases with more than two missing values and mean imputation for the cases that had one missing value. The details of the demographic characteristics of 415 participants are shown in Table 1.
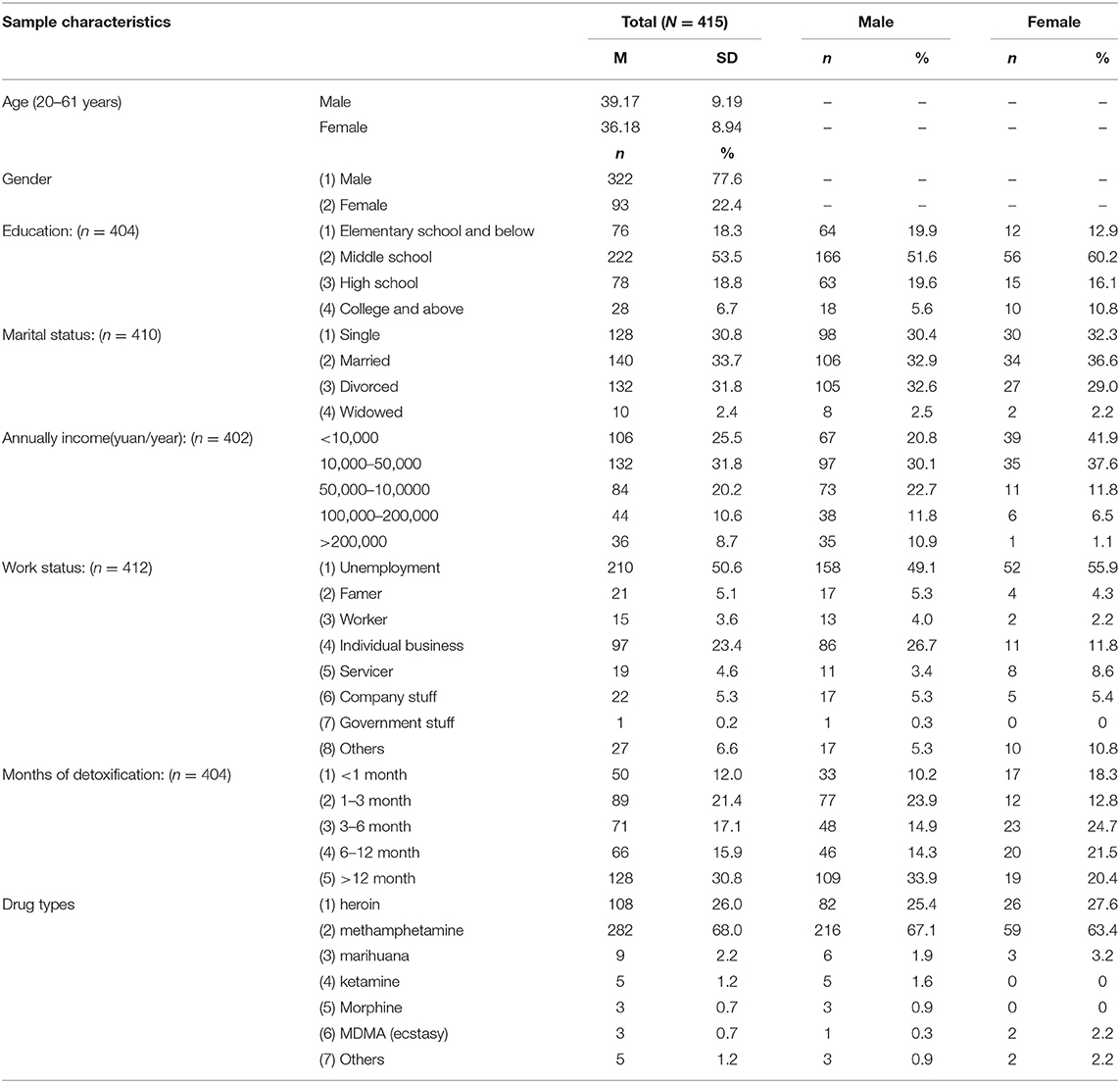
Table 1. Sample characteristics.
Procedure
The study was approved by the Ethics Committee of Nanjing Medical University, which thoroughly considered the interests of human rights, ethics, and procedure safeties. All participants showed informed consent before involving in the study. Participants were sequentially allocated into separate meeting rooms where self-report scales took 30 min on average to ensure confidentiality. At least a research assistant was available for assisting when the participants were filing the scales.
Measures
The present study applied the Connor–Davidson Resilience Scale [CD-RISC; (84)] for assessing the patients' resilience. The CD-RISC is a five-point Likert scale (from 0 = not true at all to 4 = true nearly all the time), which is designed to measure an individual's resilience level. The CD-RISC has 25 items with a total score ranging from 0 to 100. The scale assesses participants' optimism, strength, and toughness. The score reflects the level of resilience the individual experienced. Many studies have shown the satisfactory reliability and validity of the Chinese version of CD-RISC (85, 86). The Cronbach's α of CD-RISC was 0.906 in this study.
Positive and Negative Affect Scale (PANAS) was developed by Watson et al. (87) to evaluate individuals' positive and negative affect. The PANAS is a five-point Likert scale (from 1 = very slight or not at all to 5 = very strong) consisting of 20 items. Half of the items are subjected to the positive affect subscale (items 1, 3, 5, 9, 10, 12, 14, 16, 17, and 19). In this study, only the positive affect subscale was applied. The Chinese version of PANAS has been reported good reliability and validity (88). Cronbach's α of PANAS in the present study was 0.846.
Multidimensional Scale of Perceived Social Support [MSPSS; (89)] was used to measure participants' perceived social supports. The MSPSS incorporates three subscales, perceived family support subscale (items 3, 4, 8, and 11), perceived friend support subscale (items 6, 7, 9, and 12), and perceived specialist support subscale (items 1, 2, 5, and 10). The MSPSS is a seven-point Likert scale (from 1 = very strongly disagree to 7 = very strongly agree). The sum of items reflects the degree of an individual's overall perceived social support. The Chinese version of the MSPSS has been widely applied and showed satisfactory reliability and validity (90, 91). The Cronbach's α of the MSPSS in this study was 0.910.
Rosenberg Self-Esteem Scale [RSES; (92)] was used to assess the participants' self-esteem. The RSES is a four-point Likert scale (from 1 = strongly disagree to 4 = strongly agree), containing 10 items. The RSES was scored by summing total items after reverse-scoring negatively stated things (items 3, 6, 8, 9, and 10). Studies showed that the Chinese version of RSES has good reliability and validity (85, 93). Cronbach's α of RSES in this study was 0.656. According to (94), it is reasonable when Cronbach's coefficient is above 0.6. Although Cronbach's α of RSES is not as high as other variables, it is acceptable for the following research.
Perceived Stress Scale [PSS; (3)] was applied to measure participants' perceived stress. The PSS is a five-point Likert scale (from 0 = Never to 4 = Very Often), containing 14 items in which half of the items are positively stated (items 4, 5, 6, 7, 9, 10, and 13). The score of PPS is calculated by totaling all items after reverse-scoring the positive statement. The score reflects the level of individuals' perceived stress. The Chinese version of PSS's reliability and validity has demonstrated satisfactory consistency (95). Cronbach's α of PSS in this study was 0.729.
Satisfaction with Life Scale (SWLS) was used to evaluate an individual's life satisfaction. The SWLS includes five brief statements that can be rated by seven choices (from 1 = strongly disagree to 7 = strongly agree). The total score is measured by summing up each item. Satisfactory reliability and validity of SWLS in the Chinese population have been reported by many studies (96, 97). Cronbach's α of SWLS in this study was 0.838.
Diagnostic and Statistical Manual of Mental Disorders—fifth edition-based diagnostic questionnaires were administrated to assess participants' addiction severity. Eleven diagnostic criteria were embedded in 11 items in four categories in the questionnaire: impaired control over substance use (items 1 to 4), social consequences (items 5 to 7), risky use of the substance (items 8 to 9), and pharmacological indicators (items 10, 11). The 11 criteria include: symptoms of withdrawal, craving, tolerance, hazardous use, chronically use substantial amounts, substantial time on use, repeated attempt to abstinence, interpersonal issues related to substance use, social network collapses, absence from social and occupational events, and substance-related social and psychological issues. The addiction severity was calculated by counting the number of matched criteria. The Cronbach's α coefficient of the diagnostic question was 0.731.
Data Analysis
In this study, sample characteristics, the descriptive statistics, and the intercorrelation analysis were measured via IBM SPSS Statistics version 22. Following Anderson and Gerbing (98), a two-step approach was used to analyze the three mediators' mediating effects. Firstly, the measurement models that contain all variables were examined by whether the indicators could well-represent each latent variable. Secondly, we use the maximum likelihood estimation to test the structural model in the AMOS 24.0 program. Furthermore, we created several parcels using the random assignment method to control the inflated measurement errors generated by multiple items of latent variables (99).
Moreover, we use AMOS 24.0 with maximum likelihood estimation to do the path analyses. According to Hu and Bentler (100) and Siedlecki et al. (101), eight indices were used to assess the goodness-of-fit of the path models: chi-square (χ2) statistics, a root-mean-square error of approximation, standardized root mean square residual, goodness-of-fit index, Tucker–Lewis index, comparative fit index, Akaike information criterion (AIC), and expected cross-validation index (ECVI). Specifically, if chi-square (χ2) statistics <3, root-mean-square error of ~ <0.08, and the upper bound of its 90% confidence interval <0.1, standardized root mean square residual <0.08, goodness-of-fit index >0.90, Tucker–Lewis index > 0.90, and comparative fit index >0.90, the model will be considered as an acceptable fit model. Furthermore, the goodness-of-fit indices of AIC and ECVI were used to compare two or more models. A smaller value of AIC and ECVI indicated a better fit of the hypothesized model (102) and a higher potential replication (103).
Results
Preliminary Analyses
The results of descriptive statistics (including mean, SD, Cronbach's α coefficients) and the intercorrelation analysis for all variables after considering sex and age as covariates are presented in Table 2. The results indicated that income was significantly and positively correlated with resilience, positive affect, social support, self-esteem, and life satisfaction, whereas income was negatively correlated with addiction severity. Additionally, the results suggested that addiction severity was significantly associated with resilience and positive affect. Further, all intercorrelations between resilience, positive affect, perceived social support, self-esteem, life satisfaction, and perceived stress were statistically significant.
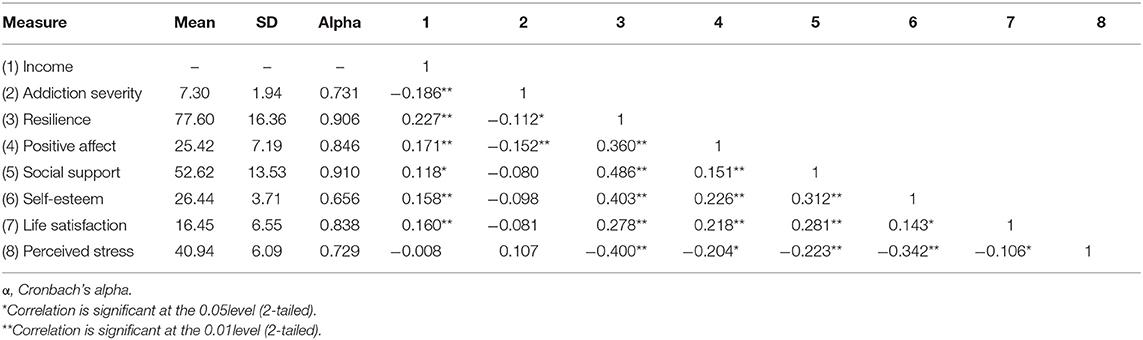
Table 2. Means, standard deviations (SD), Alpha, reliabilities, and intercorrelations among study variables after controlling gender and age.
According to Podsakoff et al. (104), we need to examine whether there was contamination using common method variance because self-report questionnaires measured all variables. We used the principle components factor analysis to examine a total of 76 items. The results showed 17 factors that revealed neither a single nor a general factor in this study, and the first factor would explain 19.69% of the variance. Therefore, the common method variance in this study was not a problem. Moreover, the factor analysis showed that 19 items in SWLS and PSS scales produced four factors, which indicated that the significant correlation between life satisfaction and perceived stress was not driven by method bias. The first factor explained 21.59% of the variance.
Mediation Analyses
Without the mediator variables, the direct paths from resilience to life satisfaction (r = 0.278, p < 0.01) and to perceived stress (r = −0.400, p < 0.01) were significant. Firstly, based on the hypothesized model (Figure 1), we built Model 1 with three mediator variables (positive affect, social support, and self-esteem) with two direct paths from resilience to life satisfaction and perceived stress. The revised model suggested a satisfactory fit to the data, and all standardized path coefficients were significant, except for the three paths: positive affect to self-esteem (β = 0.005, p = 0.868), perceived social support to perceived stress (β = −0.013, p = 0.307), and self-esteem to life satisfaction (β = 0.027, p = 0.846; Table 3). Then, we built Model 2 by eliminating the three insignificant paths of Model 1. The test results of Model 2 were satisfactory, and all the paths were significant.
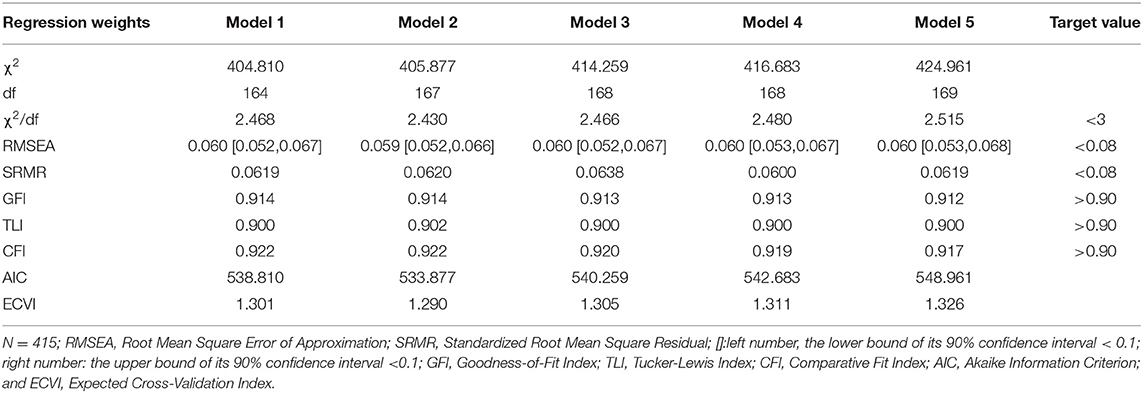
Table 3. Fit indices among competing models after controlling gender and age.
Then, the study tested whether mediators (positive affect, social support, and self-esteem) mediate the relationship between resilience and life satisfaction. Based on Model 2, Model 3 was built by eliminating the direct path from resilience to life satisfaction in Model 2. In Model 3, the revised model test results were satisfactory, and all the paths were significant. To compare Model 2 and Model 3, we used a chi-square difference test, which showed the model's fit decreased [Δχ2 (1, N = 415) = 8.382, P < 0.001]. Model 2, as yet, reported the best results regarding the goodness of fit.
Also, to test whether the mediators (positive affect, social support, and self-esteem) would mediate the relationship between resilience and perceived stress, we built Model 4 by eliminating Model 2's direct path from resilience to perceived stress. In Model 4, the revised model test results were satisfactory, and all the paths were significant. Model 5 was built by eliminating direct paths from resilience to life satisfaction and perceived stress in Model 2. The test results were also satisfactory with all the significant paths. We used a chi-square difference test to compare Model 4 with Model 5, and the results showed that the fit of the model decreased [Δχ2 (1, N = 415) = 8.278, P < 0.001]. Then, we compared the other goodness indices among five competing models, which are shown in Table 3. As a result, Model 2 was chosen as the most suitable model, and the final mediation model is shown in Figure 2.
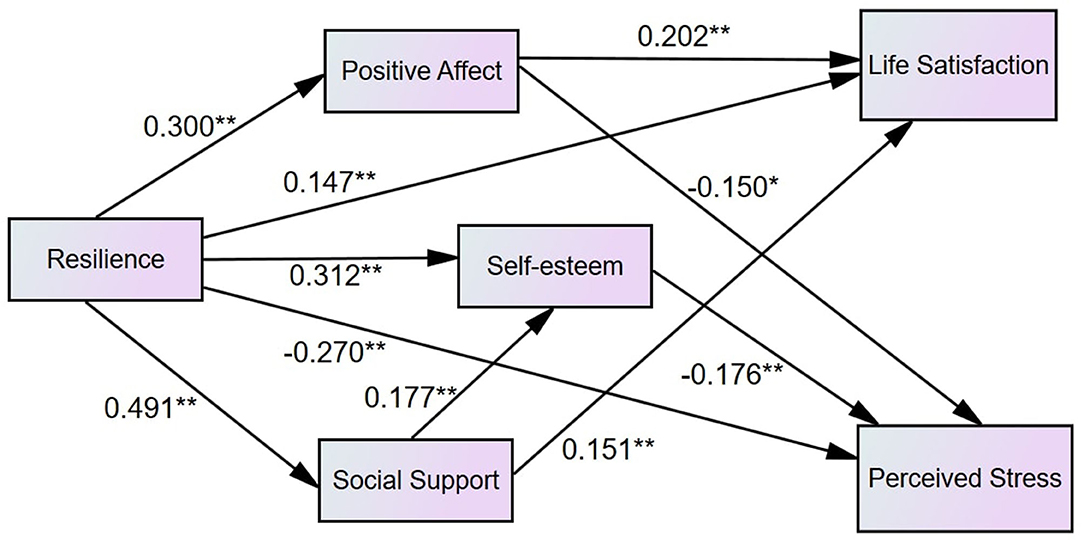
Figure 2. The finalized model after controlling gender and age (N = 415). The path coefficients are standardized. For the pictorial purpose, covariates are omitted from the figure.
Indirect Effects
The indirect effects of the model were assessed by the bootstrapping procedure method in AMOS 24.0. Referring to the recommendations of (105), due to the original data set (N = 415), 10,000 random samples were generated after controlling the effects of sex and age. Table 4 shows the indirect effects and their corresponding 95% confidence intervals, which indicated that all the indirect effects were significant. The results supported the fact that the association between resilience and life satisfaction is partially mediated by positive affect and perceived social support through two two-path mechanisms (resilience → positive affect → life satisfaction, resilience → perceived social support → life satisfaction), and the relationship between resilience and perceived stress is partially mediated by positive affect and self-esteem through two two-path mechanisms (resilience → positive affect → perceived stress, resilience → self-esteem → perceived stress) and one three-path mechanism (resilience → perceived social support → self-esteem → perceived stress).
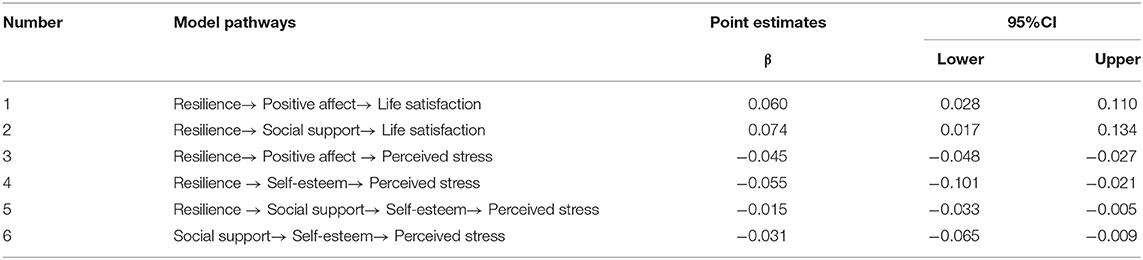
Table 4. The indirect effects of the final mediational model after controlling gender and age.
Discussion
Numerous attempts have been made to explore how to reduce perceived stress and improve life satisfaction in non-user groups (20, 26, 28), but few focus on the individuals with SUD. To our knowledge, this is the first study designed to reveal the underlying mechanisms among resilience, perceived stress, and life satisfaction in people with SUD. We designed the study on SUD people examining whether and how resilience is associated with life satisfaction and perceived stress. The findings revealed that resilience reduces perceived stress via positive affect and self-esteem and enhances life satisfaction via positive affect and perceived stress among SUD patients.
The findings of the direct effects from resilience to perceived stress and life satisfaction demonstrated that most of the non-user groups' findings regarding the relationships among resilience, perceived stress, and life satisfaction could be replicated on people with SUD. In particular, the findings suggested that the participants who scored higher in resilience were reported to have lower perceived stress and higher life satisfaction, which are in line with the corresponding studies conducted among non-user groups (26, 28, 42). These observations may provide robust evidence for specialists and policymakers of substance abuse treatment and rehabilitation that resilience plays an effective role in mitigating perceived stress and promoting life satisfaction in substance users.
Findings also suggested that positive affect and self-esteem are two mediators of the relationship between resilience and perceived stress, supporting the study's hypothesis. These findings align with previous empirical research that resilience is negatively correlated with perceived stress (20). The theoretical underpinnings for the findings are that coping strategy promoted by resilience facilitates mental flourishing (29), the core component of positive affect, and positive self-evaluation (45), the prominent factor of self-esteem. Then, positive affect and high self-esteem promote enduring psychological resources, which may effectively buffer against the perceived stress (31). Although perceived social support's mediation effect on the relationship between resilience and perceived stress was not significant, the findings showed that perceived social support was involved in a three-path mediation (resilience → perceived social support → self-esteem → perceived stress). These findings may provide a valuable perspective on substance abuse treatment and rehabilitation. The involvement of promoting positive affect and self-esteem in rehabilitation programs among SUD patients can conditional the effects of resilience on decreasing patients' perceived stress.
The findings also indicated that the relationship between resilience and life satisfaction is mediated by positive affect and perceived social support in people with SUD, providing evidence to our hypothesis. Those findings are consistent with previous empirical research that focused on the correlations between resilience and life satisfaction (21). The theoretical interpretation of the findings is that coping strategies facilitated by resilience can stimulate the processes of psychological resource integration (106), the salient component of positive affect, and shape healthier social connections, the outstanding predictor of perceived social support (107), which further raise cognitive self-appraisals over life qualities. The findings correspond with the fact that individuals with positive affect and strong social boundaries are more easily satisfied through life events (43, 108). However, the mediation effect of self-esteem was not significant in the relationship between resilience and life satisfaction, which is opposite to the studies conducted in non-user groups (28, 109). Overall, the findings may offer an implication for SUD treatment and rehabilitation that projects focus on boosting SUD patient's life satisfaction is recommended to involve the practice of building patient's resilience, positive affect, and perceived social support.
Conclusions
In conclusion, the present study has filled the gap in how resilience reduces perceived stress and promotes life satisfaction in SUD individuals. The study identifies that positive affect and self-esteem partially mediate the relationship between resilience and perceived stress. In contrast, the perceived social support and positive affect partially mediate the relationship between SUD patients' resilience and life satisfaction. The study may offer empirical perspectives on projecting and advancing substance abuse treatment and rehabilitation programs to reduce perceived stress and enhance life satisfaction.
Limitations
The present study has several limitations. First, the study lacked a control group (e.g., people without SUD). Second, the present study was cross-sectional research, which is disadvantageous in drawing a causal conclusion. Therefore, involving experimental and longitudinal research methods are highly recommended in future studies. Third, given that self-report questionnaires collected all data, although measurements had shown reliability and validity, contamination cannot be entirely ignored due to social desirability (e.g., desirability for decent scores). The semi-structured interviews are recommended to be introduced in the future to reduce respondents' subjectivity. Finally, the participants' age ranged from 20 to 61 years, so it is uncertain whether the findings can be replicated in the younger and older groups. Future studies that consider these factors may generate more accurate outcomes.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by the Ethics Committee of Nanjing Medical University. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
CY, YZ, and MX jointly drafted and conducted the manuscript. CY and MX contributed equally to this work. CY contributed to the processes of modeling and data analysis. YZ contributed to literature review, discussion, revision, and proofreading. MX contributed to data collection, participated in the writing, and finalized the manuscript. All authors read and approved the final manuscript.
Funding
This paper was supported by Research Fund for Philosophy and Social Science of Universities in Jiangsu Province (2017SJB1800) and the Program B for Outstanding PhD Candidate of Nanjing University (202001B008).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. United Nations Office on Drugs and Crime World Health Organization. International standards on drug use prevention - Second updated edition. Vienna: United Nations Office on Drugs and Crime (2018).
2. Zullig K, Valois R, Huebner E, Oeltmann J, Drane J. Relationship between perceived life satisfaction and adolescents' substance abuse. J Adolesc Health. (2001) 29:279–88. doi: 10.1016/S1054-139X(01)00269-5
3. Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. J Health Soc Behav. (1983) 24:385–96. doi: 10.2307/2136404
4. Lindenberg CS, Reiskin HK, Gendrop SC. The social stress model of substance abuse among childbearing-age women: a review of the literature. J Drug Educ. (1994) 24:253–68. doi: 10.2190/HH29-4Q1V-WK1D-DT4H
5. Mariani J, Khantzian E, Levin F. The self-medication hypothesis and psychostimulant treatment of cocaine dependence: an update. Am J Addict. (2013) 23:189–93. doi: 10.1111/j.1521-0391.2013.12086.x
6. Sher K, Levenson R. Risk for alcoholism and individual differences in the stress-response-dampening effect of alcohol. J Abnorm Psychol. (1982) 91:350–67. doi: 10.1037/0021-843X.91.5.350
7. Andersen SL, Teicher MH. Desperately driven and no brakes: developmental stress exposure and subsequent risk for substance abuse. Neurosci Biobehav Rev. (2009) 33:516–24. doi: 10.1016/j.neubiorev.2008.09.009
8. Brown PJ, Wolfe J. Substance abuse and post-traumatic stress disorder comorbidity. Drug Alcohol Depend. (1994) 35:51–9. doi: 10.1016/0376-8716(94)90110-4
9. Najavits LM, Weiss RD, Shaw SR. The link between substance abuse and posttraumatic stress disorder in women: a research review. Am J Addic. (1997) 6:273–83. doi: 10.3109/10550499709005058
10. O'hare T, Sherrer MV. Co-occurring stress and substance abuse in college first offenders. J Hum Behav Soc Environ. (2000) 3:29–44. doi: 10.1300/J137v03n01_02
11. Suarez LM, Belcher HM, Briggs EC, Titus JC. Supporting the need for an integrated system of care for youth with co-occurring traumatic stress and substance abuse problems. Am J Community Psychol. (2012) 49:430–40. doi: 10.1007/s10464-011-9464-8
12. Tavolacci MP, Ladner J, Grigioni S, Richard L, Villet H, Déchelotte P. Prevalence and association of perceived stress, substance use and behavioral addictions: a cross-sectional study among university students in France, 2009–2011. BMC public health. (2003) 13:724. doi: 10.1186/1471-2458-13-724
13. Sinha R. Chronic stress, drug use, and vulnerability to addiction. Ann N Y Acad Sci. (2008) 1141:105–30. doi: 10.1196/annals.1441.030
14. Diener E, Emmons R, Larsen R, Griffin S. The satisfaction with life scale. J Pers Assess. (1985) 49:71–5. doi: 10.1207/s15327752jpa4901_13
15. Pavot W, Diener E. Review of the satisfaction with life scale. Psychol Assess. (1993) 5:164–72. doi: 10.1037/1040-3590.5.2.164
16. Mahmoud JSR, Staten RT, Hall LA, Lennie TA. The relationship among young adult college students' depression, anxiety, stress, demographics, life satisfaction, and coping styles. Issues Ment Health Nurs. (2012) 33:149–56. doi: 10.3109/01612840.2011.632708
17. Milevsky A, Schlechter M, Netter S, Keehn D. Maternal and paternal parenting styles in adolescents: associations with self-esteem, depression and life-satisfaction. J Child Fam Stud. (2006) 16:39–47. doi: 10.1007/s10826-006-9066-5
18. Bozoglan B, Demirer V, Sahin I. Loneliness, self-esteem, and life satisfaction as predictors of Internet addiction: a cross-sectional study among Turkish university students. Scand J Psychol. (2013) 54:313–9. doi: 10.1111/sjop.12049
19. Rudolf H, Watts J. Quality of life in substance abuse and dependency. Int Rev Psychiatry. (2002) 14:190–7. doi: 10.1080/09540260220144975
20. Friborg O, Hjemdal O, Rosenvinge J, Martinussen M, Aslaksen P, Flaten M. Resilience as a moderator of pain and stress. J Psychosom Res. (2006) 61:213–9. doi: 10.1016/j.jpsychores.2005.12.007
21. Liu Y, Wang Z, Li Z. Affective mediators of the influence of neuroticism and resilience on life satisfaction. Pers Individ Dif. (2012) 52:833–8. doi: 10.1016/j.paid.2012.01.017
23. Fletcher D, Sarkar M. Psychological resilience. Eur Psychol. (2013) 18:12–23. doi: 10.1027/1016-9040/a000124
24. Brennan MA. Conceptualizing resiliency: an interactional perspective for community and youth development. Child Care Practice. (2008) 14:55–64. doi: 10.1080/13575270701733732
25. Hayter M, Dorstyn D. Resilience, self-esteem and self-compassion in adults with spina bifida. Spinal Cord. (2013) 52:167–71. doi: 10.1038/sc.2013.152
26. Richards K, Levesque-Bristol C, Templin T, Graber K. The impact of resilience on role stressors and burnout in elementary and secondary teachers. Soc Psychol Educ. (2016) 19:511–36. doi: 10.1007/s11218-016-9346-x
27. Wilks S, Croom B. Perceived stress and resilience in Alzheimer's disease caregivers: testing moderation and mediation models of social support. Aging Ment Health. (2008) 12:357–65. doi: 10.1080/13607860801933323
28. Abolghasemi A, Varaniyab S. Resilience and perceived stress: predictors of life satisfaction in the students of success and failure. Proc Soc Behav Sci. (2010) 5:748–52. doi: 10.1016/j.sbspro.2010.07.178
29. Fredrickson B, Losada M. Positive affect and the complex dynamics of human flourishing. Am Psychol. (2005) 60:678–86. doi: 10.1037/0003-066X.60.7.678
30. Lambert N, Gwinn A, Baumeister R, Strachman A, Washburn I, Gable S, et al. A boost of positive affect. J Soc Pers Relat. (2012) 30:24–43. doi: 10.1177/0265407512449400
31. Fredrickson B. What good are positive emotions? Rev Gen Psychol. (1998) 2:300–19. doi: 10.1037/1089-2680.2.3.300
32. Fredrickson B. The role of positive emotions in positive psychology: The broaden-and-build theory of positive emotions. Am Psychol. (2001) 56:218–26. doi: 10.1037/0003-066X.56.3.218
33. Fredrickson B. The broaden–and–build theory of positive emotions. Philos Trans R Soc Lond Ser B Biol Sci. (2004) 359:1367–77. doi: 10.1098/rstb.2004.1512
34. Fredrickson B, Joiner T. Positive emotions trigger upward spirals toward emotional well-being. Psychol Sci. (2002) 13:172–75. doi: 10.1111/1467-9280.00431
35. Fredrickson B, Tugade M, Waugh C, Larkin G. What good are positive emotions in crisis? A prospective study of resilience and emotions following the terrorist attacks on the United States on September 11th, 2001. J Pers Soc Psychol. (2003) 84:365–76. doi: 10.1037/0022-3514.84.2.365
36. Amabile T, Barsade S, Mueller J, Staw B. Affect and creativity at work. Adm Sci Q. (2005) 50:367–403. doi: 10.2189/asqu.2005.50.3.367
37. Davidson R, Kabat-Zinn J. Alterations in brain and immune function produced by mindfulness meditation: three caveats: response. Psychosom Med. (2004) 66:149–52. doi: 10.1097/00006842-200401000-00023
38. Steptoe A, Wardle J, Marmot M. Positive affect and health-related neuroendocrine, cardiovascular, and inflammatory processes. Proc Natl Acad Sci USA. (2005) 102:6508–12. doi: 10.1073/pnas.0409174102
39. Gil K, Carson J, Porter L, Scipio C, Bediako S, Orringer E. Daily mood and stress predict pain, health care use, and work activity in African American adults with sickle-cell disease. Health Psychol. (2004) 23:267–74. doi: 10.1037/0278-6133.23.3.267
40. Tugade M, Fredrickson B. Regulation of positive emotions: emotion regulation strategies that promote resilience. J Happiness Stud. (2006) 8:311–33. doi: 10.1007/s10902-006-9015-4
41. Zautra AJ, Johnson LM, Davis MC. Positive affect as a source of resilience for women in chronic pain. J Consult Clin Psychol. (2005) 73:212. doi: 10.1037/0022-006X.73.2.212
42. Cohn MA, Fredrickson BL, Brown SL, Mikels JA, Conway AM. Happiness unpacked: positive emotions increase life satisfaction by building resilience. Emotion. (2009) 9:361–8. doi: 10.1037/a0015952
43. Huebner E, Dew T. The interrelationships of positive affect, negative affect, and life satisfaction in an adolescent sample. Soc Indic Res. (1996) 38:129–37. doi: 10.1007/BF00300455
44. Fredrickson B, Branigan C. Positive emotions broaden the scope of attention and thought-action repertoires. Cogn Emot. (2005) 19:313–32. doi: 10.1080/02699930441000238
45. Diener E, Diener M. Cross-cultural correlates of life satisfaction and self-esteem. J Pers Soc Psychol. (1995) 68:653–63. doi: 10.1037/0022-3514.68.4.653
46. Pyszczynski T, Greenberg J, Solomon S, Arndt J, Schimel J. Why do people need self-esteem? A theoretical and empirical review. Psychol Bull. (2004) 130:435–68. doi: 10.1037/0033-2909.130.3.435
47. Arslan G. Psychological maltreatment, emotional and behavioral problems in adolescents: the mediating role of resilience and self-esteem. Child Abuse Negl. (2016) 52:200–9. doi: 10.1016/j.chiabu.2015.09.010
48. Benetti C, Kambouropoulos N. Affect-regulated indirect effects of trait anxiety and trait resilience on self-esteem. Pers Individ Dif. (2006) 41:341–52. doi: 10.1016/j.paid.2006.01.015
49. Dumont M, Provost MA. Resilience in adolescents: Protective role of social support, coping strategies, self-esteem, and social activities on experience of stress and depression. J Youth Adolesc. (1999) 28:343–63. doi: 10.1023/A:1021637011732
50. Wong MC, Sun J, Lee A, Stewart D, Cheng FF, Kan W, et al. The impact of a newly designed resilience-enhancing programme on parent-and teacher-perceived resilience environment among Health Promoting Schools in Hong Kong. J Epidemiol Commun Health. (2009) 63:2709–14. doi: 10.1136/jech.2008.074260
51. Greenberg J, Pyszczynski T, Solomon S. The causes and consequences of a need for self-esteem: a terror management theory. In R. F. Baumeister ed. Public Self and Private Self. New York, NY: Springer (1986) 189–212. doi: 10.1007/978-1-4613-9564-5_10
52. Collins AL, Smyer MA. The resilience of self-esteem in late adulthood. J Aging Health. (2005) 17:471–89. doi: 10.1177/0898264305277965
53. Moksnes UK, Espnes GA. Self-esteem and life satisfaction in adolescents—gender and age as potential moderators. Qual Life Res. (2013) 22:2921–8. doi: 10.1007/s11136-013-0427-4
54. Rey L, Extremera N, Pena M. Perceived emotional intelligence, self-esteem and life satisfaction in adolescents. Psychosoc Interv. (2011) 20:227–34. doi: 10.5093/in2011v20n2a10
55. Dolatian M, Mirabzadeh A, Forouzan AS, Sajjadi H, Majd HA, Moafi F, et al. Correlation between self-esteem and perceived stress in pregnancy and ways to coping with stress. Pajoohandeh J. (2013) 18:148–55.
56. Hubbs A, Doyle EI, Bowden RG, Doyle RD. Relationships among self-esteem, stress, and physical activity in college students. Psychol Rep. (2012) 110:469–74. doi: 10.2466/02.07.09.PR0.110.2.469-474
57. Cohen S, Williamson G. Perceived stress in a probability sample of the United States. In: Spacapan S, Oskamp S, editors. The Social Psychology of Health Claremont Symposium on Applied Social Psychology. Newbury, CA (1988). p. 31–67.
58. Pangallo A, Zibarras LD, Lewis R, Flaxman P. Resilience through the lens of interactionism: a systematic review. Psychol Assess. (2015) 27:1–20. doi: 10.1037/pas0000024
59. Haber M, Cohen J, Lucas T, Baltes B. The relationship between self-reported received and perceived social support: a meta-analytic review. Am J Community Psychol. (2007) 39:133–44. doi: 10.1007/s10464-007-9100-9
60. Howard S, Hughes BM. Benefit of social support for resilience-building is contingent on social context: examining cardiovascular adaptation to recurrent stress in women. Anxiety Stress Coping. (2012) 25:411–23. doi: 10.1080/10615806.2011.640933
61. Mo PKH, Lau JTF, Yu X, Gu J. The role of social support on resilience, posttraumatic growth, hopelessness, and depression among children of HIV-infected parents in mainland China. AIDS Care. (2014) 26:1526–33. doi: 10.1080/09540121.2014.923810
62. Ong HL, Vaingankar JA, Abdin E, Sambasivam R, Fauziana R, Tan ME, et al. Resilience and burden in caregivers of older adults: moderating and mediating effects of perceived social support. BMC Psychiatry. (2018) 18:27. doi: 10.1186/s12888-018-1616-z
63. Wilks SE, Spivey CA. Resilience in undergraduate social work students: Social support and adjustment to academic stress. Soc Work Educ. (2010) 29:276–88. doi: 10.1080/02615470902912243
64. Sexton MB, Byrd MR, von Kluge S. Measuring resilience in women experiencing infertility using the CD-RISC: examining infertility-related stress, general distress, and coping styles. J Psychiatr Res. (2010) 44:236–41. doi: 10.1016/j.jpsychires.2009.06.007
65. Han J, Kim KW, Kim TH, Jeong H, Park JY, Youn J, et al. The impact of social support on caregiver burden in dementia. Alzheimer's Dement. (2012) 8:249. doi: 10.1016/j.jalz.2012.05.661
66. Klineberg E, Clark C, Bhui KS, Haines MM, Viner RM, Head J, et al. Social support, ethnicity and mental health in adolescents. Soc Psychiatry Psychiatr Epidemiol. (2006) 41:755–60. doi: 10.1007/s00127-006-0093-8
67. Richter SS, Brown SA, Mott MA. The impact of social support and self-esteem on adolescent substance abuse treatment outcome. J Subst Abuse. (1991) 3:371–85. doi: 10.1016/S0899-3289(10)80019-7
68. Rodakowski J, Skidmore ER, Rogers JC, Schulz R. Role of social support in predicting caregiver burden. Arch Phys Med Rehabil. (2012) 93:2229–36. doi: 10.1016/j.apmr.2012.07.004
69. Hefner J, Eisenberg D. Social support and mental health among college students. Am J Orthopsychiatry. (2009) 79:491–99. doi: 10.1037/a0016918
70. Kong F, You X. Loneliness and self-esteem as mediators between social support and life satisfaction in late adolescence. Soc Indic Res. (2013) 110:271–9. doi: 10.1007/s11205-011-9930-6
71. Paterson AD, Hakim-Larson J. Arab youth in Canada: Acculturation, enculturation, social support, and life satisfaction. J Multicult Couns Devel. (2012) 40, 206–15. doi: 10.1002/j.2161-1912.2012.00018.x
72. Reeve KL, Shumaker CJ, Yearwood EL, Crowell NA, Riley JB. Perceived stress and social support in undergraduate nursing students' educational experiences. Nurse Educ Today. (2013) 33:419–24. doi: 10.1016/j.nedt.2012.11.009
73. Su X, Lau JT, Mak WW, Chen L, Choi KC, Song J, et al. Perceived discrimination, social support, and perceived stress among people living with HIV/AIDS in China. AIDS Care. (2013) 25:239–48. doi: 10.1080/09540121.2012.701713
74. Tajfel H. Human Groups and Social Categories: Studies in Social Psychology. New York, NY: Cambridge University Press (1981).
76. Caldwell J, Mule SJ, (eds). Amphetamines and Related Stimulants: Chemical, Biological, Clinical, and Sociological Aspects. Boca Raton, FL: CRC Press (2019).
77. Everitt B, Robbins T. Neural systems of reinforcement for drug addiction: from actions to habits to compulsion. Nat Neurosci. (2005) 8:1481–9. doi: 10.1038/nn1579
78. Gawin F. Cocaine addiction: psychology and neurophysiology. Science. (1991) 251:1580–6. doi: 10.1126/science.2011738
79. Libby AM, Orton HD, Stover SK, Riggs PD. What came first, major depression or substance use disorder? Clinical characteristics and substance use comparing teens in a treatment cohort. Addict Behav. (2005) 30:1649–62. doi: 10.1016/j.addbeh.2005.07.012
80. Chou KL, Liang K, Sareen J. The association between social isolation and DSM-IV mood, anxiety, and substance use disorders: wave 2 of the national epidemiologic survey on alcohol and related conditions. J Clin Psychiatry. (2011) 72:1468–76. doi: 10.4088/JCP.10m06019gry
81. Baldwin ML, Marcus SC, De Simone J. Job loss discrimination and former substance use disorders. Drug Alcohol Depend. (2010) 110:1–7. doi: 10.1016/j.drugalcdep.2010.01.018
82. Herman-Stahl M, Spencer DL, Duncan JE. The implications of cultural orientation for substance use among American Indians. Am Ind Alask Native Ment Health Res. (2003) 11:46–66. doi: 10.5820/aian.1101.2003.46
83. Barry C, McGinty E, Pescosolido B, Goldman H. Stigma, discrimination, treatment effectiveness, and policy: public views about drug addiction and mental illness. Psychiatr Serv. (2014) 65:1269–72. doi: 10.1176/appi.ps.201400140
84. Connor K, Davidson J. Development of a new resilience scale: the connor-davidson resilience scale (CD-RISC). Depress Anxiety. (2003) 18:76–82. doi: 10.1002/da.10113
85. Yang C, Zhou Y, Cao Q, Xia M, An J. The relationship between self-control and self-efficacy among patients with substance use disorders: resilience and self-esteem as mediators. Front Psychiatry. (2019) 10:388. doi: 10.3389/fpsyt.2019.00388
86. Yu X, Zhang J. Factor analysis and psychometric evaluation of the connor-davidson resilience scale (CD-RISC) with Chinese people. Soc Behav Person An Int J. (2007) 35:19–30. doi: 10.2224/sbp.2007.35.1.19
87. Watson D, Clark L, Tellegen A. Development and validation of brief measures of positive and negative affect: the PANAS scales. J Pers Soc Psychol. (1988) 54:1063–70. doi: 10.1037/0022-3514.54.6.1063
88. Liang Y, Zhu D. Subjective well-being of Chinese landless peasants in relatively developed regions: measurement using PANAS and SWLS. Soc Indic Res. (2014) 123:817–35. doi: 10.1007/s11205-014-0762-z
89. Zimet G, Dahlem N, Zimet S, Farley G. The multidimensional scale of perceived social support. J Pers Assess. (1988) 52:30–41. doi: 10.1207/s15327752jpa5201_2
90. Chou K. Assessing Chinese adolescents' social support: the multidimensional scale of perceived social support. Pers Individ Dif. (2000) 28:299–307. doi: 10.1016/S0191-8869(99)00098-7
91. Kong F, Gong X, Sajjad S, Yang K, Zhao J. How is emotional intelligence linked to life satisfaction? The mediating role of social support, positive affect and negative affect. J appiness Stud. 17:2481–2501. doi: 10.1007/s10902-018-00069-4
92. Rosenberg M. Society and the Adolescent Self-Image. Princeton, NJ: Princeton University Press (1965).
93. Chen S, Cheung F, Bond M, Leung J. Going beyond self-esteem to predict life satisfaction: the Chinese case. Asian J Soc Psychol. (2006) 9:24–35. doi: 10.1111/j.1467-839X.2006.00182.x
95. Leung D, Lam T, Chan S. (2010). Three versions of perceived stress scale: validation in a sample of chinese cardiac patients who smoke. BMC Public Health. 10:513. doi: 10.1186/1471-2458-10-513
96. Bai X, Wu C, Zheng R, Ren X. The psychometric evaluation of the satisfaction with life scale using a nationally representative sample of China. J appiness Stud. (2010) 12:183–97. doi: 10.1007/s10902-010-9186-x
97. Yang C, Xia M, Han M, Liang Y. Social support and resilience as mediators between stress and life satisfaction among people with substance use disorder in China. Front Psychiatry. (2018) 9:436. doi: 10.3389/fpsyt.2018.00436
98. Anderson JC, Gerbing DW. Structural equation modeling in practice: a review and recommended two-step approach. Psychol Bull. (1988) 103:411–23. doi: 10.1037/0033-2909.103.3.411
99. Little TD, Cunningham WA, Shahar G, Widaman KF. To parcel or not to parcel: exploring the question, weighing the merits. Struct Equ Modeling. (2002) 9:151–73. doi: 10.1207/S15328007SEM0902_1
100. Hu L, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria vs. new alternatives. Struct Equat Modeling. (1999) 6:1–55. doi: 10.1080/10705519909540118
101. Siedlecki KL, Salthouse TA, Oishi S, Jeswani S. The relationship between social support and subjective well-being across age. Soc Indic Res. (2014) 117:561. doi: 10.1007/s11205-013-0361-4
104. Podsakoff P, MacKenzie S, Lee J, Podsakoff N. Common method biases in behavioral research: a critical review of the literature and recommended remedies. J Appl Psychol. (2003) 88:879–903. doi: 10.1037/0021-9010.88.5.879
105. MacKinnon D, Lockwood C, Williams J. Confidence limits for the indirect effect: distribution of the product and resampling methods. Multivariate Behav Res. (2004) 39: 99–128. doi: 10.1207/s15327906mbr3901_4
106. Richardson GE. The metatheory of resilience and resiliency. J Clin Psychol. (2002) 58:307–21. doi: 10.1002/jclp.10020
107. Cacioppo J, Adler A, Lester P, McGurk D, Thomas J, Chen H, et al. Building social resilience in soldiers: a double dissociative randomized controlled study. J Pers Soc Psychol. (2015) 109:90–105. doi: 10.1037/pspi0000022
108. Aquino JA, Russell DW, Cutrona CE, Altmaier EM. Employment status, social support, and life satisfaction among the elderly. J Counsel Psychol. (1996) 43:480. doi: 10.1037/0022-0167.43.4.480
Keywords: substance use disorders, resilience, mental health, positive affect, self-esteem, perceived social support
Citation: Yang C, Zhou Y and Xia M (2020) How Resilience Promotes Mental Health of Patients With DSM-5 Substance Use Disorder? The Mediation Roles of Positive Affect, Self-Esteem, and Perceived Social Support. Front. Psychiatry 11:588968. doi: 10.3389/fpsyt.2020.588968
Received: 30 July 2020; Accepted: 26 October 2020;
Published: 03 December 2020.
Edited by:
Human Friedrich Unterrainer, University of Vienna, AustriaReviewed by:
Jing Sun, Griffith University, AustraliaJürgen Fuchshuber, Center for Integrative Addiction Research (CIAR), Austria
Copyright © 2020 Yang, Zhou and Xia. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: You Zhou, eW91ejdAc3R1ZGVudC51bmltZWxiLmVkdS5hdQ==
†These authors have contributed equally to this work