 Adrianna Senczyszyn
Adrianna Senczyszyn Renata Wallner
Renata Wallner Dorota Maria Szczesniak
Dorota Maria Szczesniak Mateusz Łuc
Mateusz Łuc Joanna Rymaszewska
Joanna Rymaszewska- Department of Psychiatry, Wroclaw Medical University, Wroclaw, Poland
Objectives: Subjective Cognitive Decline (SCD) and Mild Cognitive Impairment (MCI) are common in elderly population, and constitute a high-risk group for progression to dementia. Innovative, complex, and engaging non-pharmacological methods of cognitive stimulation, implementable at this stage, are needed. The aim of the study was to determine the effect of Computerized Cognitive Training (CCT) combined with Whole Body Stimulation (WBC) on cognitive functions of older adults with SCD and MCI.
Methods: A 9-week single-blind pre/post case control trial was conducted. The study enrolled 84 adults aged 60 or older, allocated to one of two intervention groups: EG; CCT with psychoeducation, EG2; CCT with psychoeducation and 10 WBC sessions, or the control group (CG), which comprised patients receiving usual care. The primary outcome measures were cognitive functions evaluated with MoCA scale and several other neuropsychological tools. Depressive symptoms assessed with the GDS scale constituted the secondary outcome measures.
Results: The results show evidence for increased performance in the assessment of general cognitive functioning in both EGs (p ≤ 0.05). Significant improvement was also visible in several cognitive domains, such as verbal fluency (EG1 & EG2), learning ability and immediate memory (EG1 & EG2), delayed memory (EG2), attentional control (EG1), and information processing (EG2) (p ≤ 0.05). However, only in the group with combined interventions (CCT + WBC) the participants presented significantly less depressive symptoms (p ≤ 0.05).
Conclusions: The results of the study suggest that CCT, especially in combination with WBC, might be a practical and effective method of improving cognitive performance. Moreover, this combination leads to a reduction of depressive symptoms.
Introduction
The world's population is aging rapidly. According to World Population Prospects: the 2019 Revision, by 2050, one in four persons living in Europe and Northern America could be aged 65 or above, and the number of persons aged 80 is expected to triple (1). Social and health systems in both developing and developed countries are not prepared for such demographic change. The increase in life expectancy results in higher incidence and prevalence of age-related cognitive decline, which involves neurodegenerative changes, such as loss of neurons and a decrease in the production of neurotransmitters. These changes are manifested by general slowness of psychomotor skills (2) along with reduced memory, attention, executive functions, and reasoning capacities (3). So far, there are no curative pharmaceutical methods of treatment for cognitive impairment and dementia (4). Alarmingly, due to the sense of diminished mental capabilities, older adults often exhibit withdrawal from many areas of activity (e.g., professional, social, educational) and a decrease in their independence and self-esteem (2, 5) as well as the stigma phenomenon (6). For these reasons, they need to be provided with opportunities to avoid social isolation and loss of interest (7).
Therapeutic methods of cognitive and social stimulation are being sought in order to achieve these goals. In our study, we investigated whether Computerized Cognitive Training (CCT) combined with Whole Body Cryotherapy (WBC) could constitute effective methods of cognitive stimulation.
Computerized Cognitive Trainings
Computerized Cognitive Trainings (CCTs) constitute a relatively new non-pharmacological approach to cognitive stimulation. Studies on their effectiveness suggest that participation in cognitively and socially engaging activities can slow down the deteriorative processes (8–10). CCTs are conducted as group or individual training sessions with the use of electronic devices (e.g., computer, laptop, tablet, etc.,), and consist of various assignments intended to stimulate selected cognitive functions, such as attention, verbal and non-verbal memory, working memory, processing speed, or visuospatial skills. Moreover, CCTs include novel learning experiences–participants who are not familiar with digital devices need to acquire new skills, which in turn may lead to the creation of new neural pathways (11, 12). CCTs are characterized by a high level of control over the session, the use of standardized tasks and involvement of participants in planned, customizable, and structured activities (13).
There are two basic assumptions underlying CCTs. Firstly, training a particular cognitive function regularly can help maintain or increase the level of its efficiency. Secondly, the effects of the training can be generalized and lead to an improvement in the general functioning of patients (transfer of the trained skills) (14). CCTs are often accompanied by psychoeducational activities, e.g., (15, 16) during which the characteristics of cognitive domains as well as specific learning techniques that are beneficial for them are being discussed.
Whole-Body Cryotherapy
Another promising method of non-pharmacological treatment of cognitive decline is called Whole-Body Cryotherapy or Cryostimulation (WBC). WBC involves a repetitive, short-term (up to 3 min) exposure to extremely low temperatures, and is nowadays widely used to relieve symptoms of various ailments in the course of which inflammation, muscle spasms, chronic pain, and swelling are observed (17–20). Systematic review revealed that WBC may exert beneficial effects on the lipid profile in terms of lowering the levels of total cholesterol, LDL, and triglycerides (21). Preliminary studies suggest that it may also be an effective method of improving cognitive functioning, especially memory processes (22). According to current knowledge, vascular malfunction, mitochondrial damage, oxidative stress and inflammatory response contribute to the development of cognitive deterioration, and WBC might be a response to these processes (20, 23–26). Recent studies suggest anti-inflammatory, anti-analgesic, metabolic, hormonal, and anti-oxidant effects of this therapy based on the underlying physiological responses (21, 27, 28). Since WBC addresses some of the aforementioned processes contributing to cognitive deterioration, we postulate that it might be considered as a relatively safe and low-cost method of its prevention. However, the exact mechanisms underlying the influence of cryogenic temperature intervention on cognitive functions requires further investigation (21, 29).
Materials and Methods
Study Design
The study was designed as a pre/post case control trial. There were two intervention groups and one control group: EG1–Experimental Group with Computerized Cognitive Training and EG2– Experimental Group with Computerized Cognitive Training and Whole-Body Cryotherapy, and CG– Control Group–which were comprised of community dwelling older people. The groups were matched for age, gender, and level of cognitive functioning. Cognitive assessment in EGs was conducted twice: in the first week before the first session of CCT (T1) and in the week after the last CCT (T2). CG was also assessed twice, with a 9-week break period. Participants who were present at least 80% of the intervention sessions were deemed adherent. The research protocol for this trial was reviewed and approved by the Bioethical Committee (number KB61/218) at Wroclaw Medical University. The consort flow diagram modified for non-randomized trial design is presented in Figure 1.
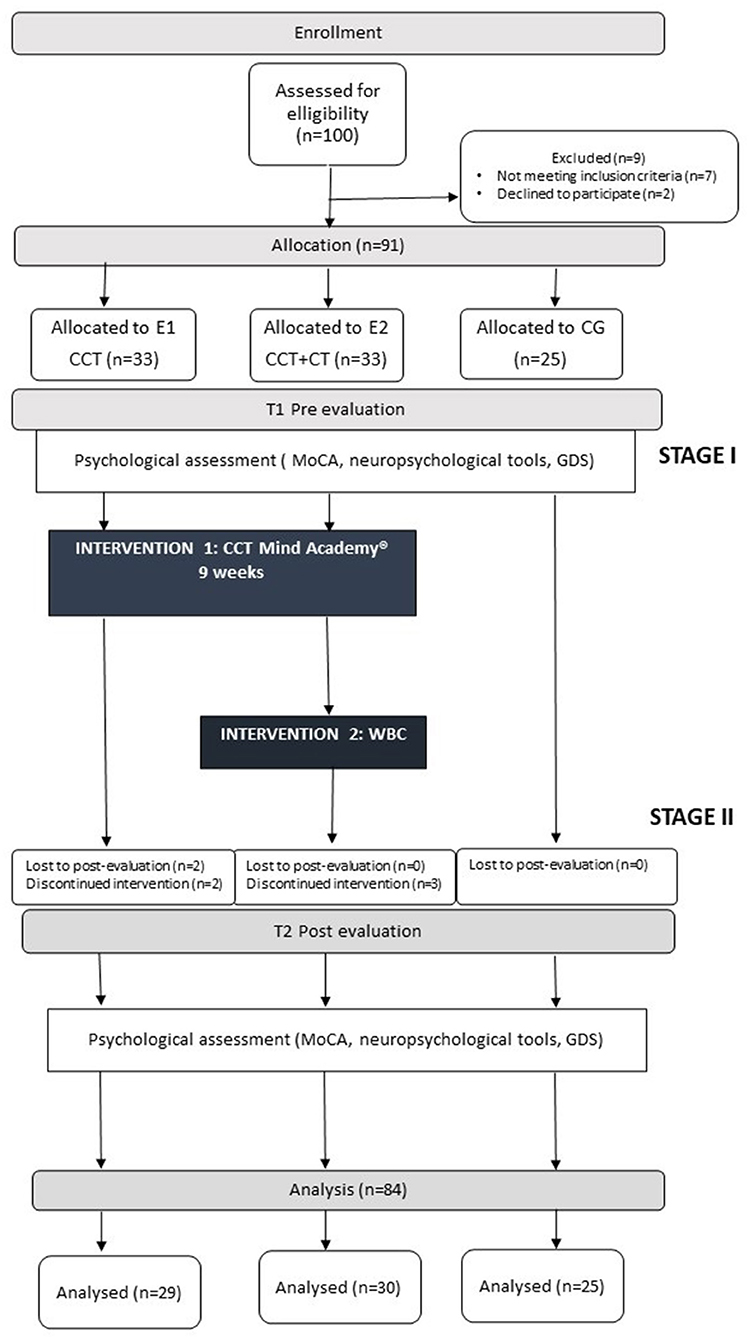
Figure 1. The consort flow diagram modified for non-randomized trial design.
Subjects
One hundred community-dwelling elderly people from the Lower Silesian Public Library in Wroclaw were enrolled in the study. All of them had subjective cognitive impairments, which were either confirmed in objective neuropsychological assessment (participants with MCI) or not (participants with SCD). Theinclusion criteria for CCT were: age ≥ 60 years, basic computer knowledge, cognitive norm/mild cognitive impairment (MCI). Cognitive functioning was assessed with the Montreal Cognitive Assessment, MoCA, and the cut-off points were: >26 for norm, 26–20 for MCI, ≤ 19 for dementia (30, 31). The exclusion criteria included more advanced cognitive decline (19 ≤ MoCA), inability to understand questions and written information, psychosis, standard contradictions to use WBC (e.g., acute respiratory diseases, acute cardiovascular disease like coronary disease, circulatory insufficiency, unstable hypertension, cold intolerance, claustrophobia, cryoglobulinemia, cancer, deep vein diseases, hypothyroidism, neuropathies, purulent skin differences, Reynaud disease), and previous exposition to WBC treatment.
Seven people did not meet the inclusion criteria (≤19 MoCA), two refused to participate. Those among the 91 people who were unable to attend regular CCT were assigned to the control group (n = 25). As a result, 66 participants were cognitively able and willing to commit to CCT/CCT + WBC. The participants from this group in whom there were no standard contraindications to the use of WBC were assigned to CCT + WBC. As a result, the EGs were equinumerous (EG1 n = 33, EG2 n = 33). Over the course of the intervention, seven participants dropped out (four due to some minor health problem, three went on vacation), leaving final sample size of 84. They received detailed oral and written information regarding the design of the study, the possibility to resign at any of its stages and information on the anonymity of the study. Before the study began, the participants provided their written consent to its terms. Additionally, those who underwent WBC were informed about the procedure in the presence of a clinician. EGs and CG were homogeneous in terms of sociodemographic variables, MoCA, and Geriatric Depression Scale (GDS) (32, 33).
Intervention
CCT was conducted in a group format comprising 8–12 participants per group. Participants from EGs attended the Lower Silesian Public Library once a week for 1.5-h sessions, for 9 weeks. Each session comprised of 3 components:
(1) psychoeducation: promotion of knowledge about healthy brain aging, brain training possibilities, learning and compensation strategies, etc.,;
(2) Computerized Cognitive Training: individual computer tasks targeting specific cognitive functions;
(3) interactive group tasks: including tasks introduced to increase the stimulation of cognitive functions and social interactions between the participants.
What is more, each session was followed by a homework assignment corresponding to the main subject of a particular group task. The CCT program referred to the concept of cognitive stimulation (14, 34), which is an approach based on engaging participants not only in a range of cognitive tasks, but also exercises conducted in groups, introduced to promote social activation. The cognitive tasks used in the project were selected from the Mind Academy® cognitive training (Formsoft®, Wroclaw, Poland), an educational program created to improve mental capacity in the elderly. The cognitive exercises offered by Mind Academy® target a whole spectrum of cognitive domains, such as attention, immediate and delayed memory, mental flexibility, processing speed, categorization, reaction time, and visuospatial skills. During each training session, the participants followed an individualized training course (the difficulty level of the tasks was adapting to the progress made by each person). Each session was conducted and supervised by a certified trainer who conducted CCTs in accordance with the instructions of a standardized 9-week training schedule. The second type of procognitive stimulation was WBC. The cryotherapy chamber (CR 2002, Wroclaw type), cooled by liquid nitrogen, had two rooms: the vestibule/antechamber (with the temperature of −60°C, and the proper chamber with temperature from −110°C on the first day to −130°C on the following days).
Cryotherapy sessions lasted 2 min in the main chamber with 30 s extra for adaptation in the vestibule before and after the proper session (35). The chamber was used by 5–6 people at the same time. The participants wore minimal, woolen or cotton clothing. To reduce the risk of injuries caused by the cold and to protect their limbs and heads, the participants put on gloves, high-knee socks, dry shoes, beanies, and mouth masks. Before every WBC session, each participant was examined by a physician who also measured their blood pressure.
Instruments
The primary outcome measures were general cognitive functions and selected domains of cognitive functioning listed below. Depressive symptoms constituted the secondary outcome. Each cognitive domain (attention and working memory, psychomotor speed, visuospatial/constructional functions, executive functions, language skills, verbal and visual memory) was evaluated by an independent psychometric tool. To reduce the risk of test performance improvement after CCT, as a result of learning the effect of repeated assessments, parallel versions of MoCA and RBANS, were used.
Psychometric tools used to assess participants' cognitive performance:
Primary Outcomes
General Cognitive Performance
• The Montreal Cognitive Assessment Scale (MoCA) (score range: 0–30). Cut-off points (>26 for norm, 26–20 for MCI, ≤ 19 for dementia) were taken from the first Polish language version (31).
Attention and Working Memory
• Digit Span from MoCA (score range: 0–2) assessing attentional control, sustained attention and immediate memory.
• Serial Sevens from MoCA (score range: 0–2) measuring working memory.
Psychomotor Speed
• The Trail Making Test A (TMT: part A) (36, 37) (time in s′) measuring psychomotor speed.
Executive Functions
• The Stroop Color and Word Test (SCWT) (38) (time in s′) for the assessment of the ability to inhibit cognitive interference.
• Phonemic Fluency Test (36) letter “k” (T1), “m” (T2), (number of words in s′) measuring phonemic verbal productivity and executive control.
Language Skills
• Semantic Fluency “fruits and vegetables” (T1), “pieces of clothing” (T2) from the Repeatable Battery for the Assessment of Neuropsychological Status (RBANS) (39) (score range: 0–40) for the assessment of semantic verbal productivity.
• Picture Naming from RBANS (score range: 0–10) assessing mental lexicon searching and naming skills.
Verbal Memory
• List Learning from RBANS (score range: 0–40) measuring the learning ability and immediate episodic memory.
• List Recall from RBANS (score range: 0–10) for the assessment of delayed episodic memory.
• Logical Memory I from RBANS (score range: 0–24) measuring the learning ability and immediate logical episodic memory.
• Logical Memory II from RBANS (score range: 0–12) for the assessment of episodic logical delayed memory.
Visual Memory
• Figure Recall from RBANS (score range: 0–20) measuring delayed visual memory.
Visuospatial/Constructional Function
• Figure Copy from RBANS (score range: 0–20) assessing planning and organization.
• Line Orientation from RBANS (score range: 0–20) measuring visual-spatial orientation.
Secondary Outcome
Depressive Symptoms
• The Geriatric Depression Scale, 30-item version, (score range: 0–30) for the assessment of depressive symptoms. The cut-off points were as follows: norm: 0–9, mild depressives: 10–19, severe depressives: 20–30.
Statistical Analysis
The D'Agostino-Pearson test and visual assessment were used to analyse the normality of the data. Demographic characteristics at baseline were compared using the Fisher exact test for independent samples (gender, place of residence, education, work, marital status) and the Kruskal-Wallis tests (age). Primary and secondary outcome measures obtained in baseline and follow-up were compared using the Fisher exact test for independent samples (qualitative variable) and Kruskal Wallis (quantitative variables). Multiple factor analysis of differences between groups and changes in time in test results was obtained using linear mixed models in the case of quantitative characteristics surveys, or cumulative link model in the case of ordinal characteristics. The level of statistical significance was set at 0.05. Calculations were made using the R for Windows package (version 3.6.1).
Results
Demographic Characteristics
Eighty-four people with MCI or SCD completed the study–59 in experimental groups (n = 29 in EG1, n = 30 in EG2) and 25 in the control group. The mean age of EG1 participants was 77.1 (±5.7), EG2 = 71.1 (±6.9), and CG = 69.4 (±6.3). Married patients constituted 60% of EG1, 51.72% of EG2, and 40% of CG. Most patients were female– 89.7% in EG1, 76.6% in EG2, and 72% in CG. At least half of all participants had higher education: EG1 = 55.1%, EG2 = 56.7%, CG = 64%. The majority of people enrolled in the study lived in big cities (100% in EG1, 93.3% in EG2, and 96% in CG) and were retired (96.5% in EG1, 100% in EG2, and 100% in CG). EGs and CG were similar in terms of global cognitive status [MoCA mean scores: EG1 = 25 (±2.3 SD), EG2 = 25.1 (±2.7 SD), CG = 25.4 (±2.7 SD)] and depressive symptoms [GDS mean scores: EG1 = 8.8 (±5.7 SD), EG2 = 7.7 (±5.1 SD), CG = 8.4 (±5.7 SD)] measured before the interventions. Detailed demographic characteristics are presented in Table 1.
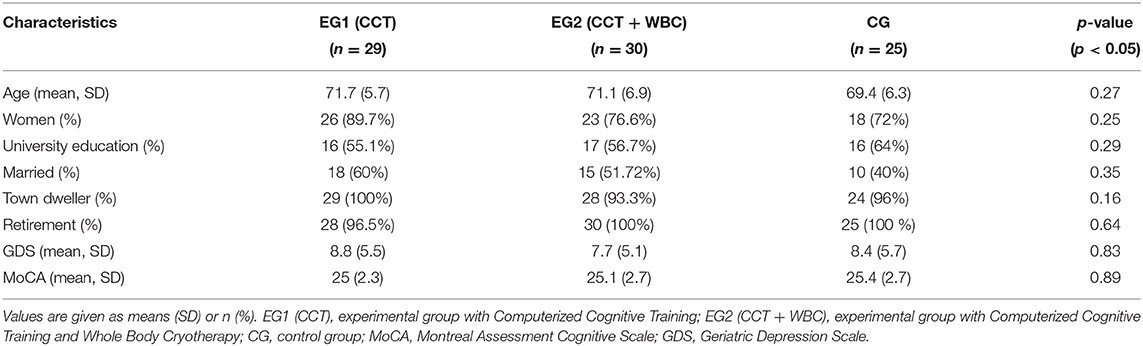
Table 1. Baseline characteristics of the participants.
Cognitive Outcomes
Primary Outcomes
Global Cognitive Functioning
The multiple factor analysis showed significant time by group interaction in favor of EGs: EG1 (CTT) and EG2 (CCT + WBC) in comparison to CG for general cognitive functioning (MoCA: EG1 p = 0.002, t = 3.137, EG2 = p = 0.000, t = 4.023). However, no significant difference between EG1 and EG2 was observed (p = 0.373, t = −0.895). Moreover, taking into account the clinical interpretation of the scores obtained by subsequent participants, it is observed that over time, in both experimental groups, some patients (EG1 = 4 people, EG2 = 12 people) changed the category from MCI (MoCA: 20–26) to cognitive norm (MoCA > 26), wherein there was no such change in categorical adherence in CG. The results of selective cognitive function subtests were more ambiguous.
Attention and Working Memory
Primarily, in the time by group attention and working memory assessment, the participants in EG1 improved their performance in the Digit Span subtest from MoCA (p = 0.041, OR = 8.041), but the participants in EG2 did not (p = 0.232, OR = 3.227). However, the overtime comparison between the experimental groups in Digit Span was insignificant (p = 0.350, OR = 0.401). In the latter subtest–Serial Sevens from MoCA–the time by group difference was insignificant in both EGs (EG1 p = 0.773, OR = 1.253, EG2 p = 0.993, OR = 0.994).
Psychomotor Speed
In the assessment of psychomotor speed conducted with the use of the Trail Making Test: part A only the difference between EG2 and CG measured over time was statistically significant (EG2 p = 0.035, t = −2.148), while in EG1 the difference was close to significance (EG1 p = 0.083, t = −1.753). The difference between EGs was insignificant (p = 0.778, t = −0.270).
Executive Functions
With regard to executive functions, the improvement in the group by time assessment was statistically significant (EG1 p = 0.000, t = 3.640, p = 0.003, t = 3.042) only in Phonemic Fluency from MoCA. Nevertheless, the group by time over time comparison between EGs was insignificant (p = 0.517, t = 0.651).
Language Skills
Similarly, only in one of the tools used for the language skills group by time assessment the difference was statistically significant (Semantic Fluency from RBANS EG1 p = 0.010, t = 3.640, EG2 p = 0.010, t = 2.619). However, the same effect did not persist in the EGs over time comparison (p = 0.953, t = 0.059).
Verbal Memory
In the case of verbal memory, two out of four subtests supported the hypothesized group-time interaction in at least one EG: Logical Memory I from RBANS (EG1 p = 0.007, t = 2.770, EG2 p = 0.004, t = 2.992) and List Recall from RBANS (EG1 p = 0.751, p = 0.319, EG2 p = 0.025, t = 2.280). In the List Recall subtest the over time difference between EG1 and EG2 was statistically significant in favor of EG2 (p = 0.008, t = 2.705), in Logical Memory I–insignificant (p = 0.836, t = 0.208).
Visual Memory
In the visual memory domain, measured with Figure Recall from RBANS, the hypothesized group-time interaction was not observed (EG1 p = 0.619, t = 0.499, EG2 p = 0.643, t = 0.466).
Visuospatial/Constructional Function
In the last cognitive domain: visuospatial/constructional function, assessed with Line Orientation and Figure Copy from RBANS, the expected over-time improvement was observed only in one subtest in EG2: Figure Copy (EG1 p = 0.147, t = 1.466, EG2 p = 0.000, t = 3.639).
Secondary Outcome
Depressive Symptoms
The results show evidence of a decrease in depressive symptoms in the time-group comparison; however, the difference was statistically significant only in EG2 (EG1 p = 0.387, t = 0.871, EG2 p = 0.033, t = 2.165). Furthermore, taking into account the clinical interpretation of the scores obtained by subsequent participants, some participants in EGs changed their category from depression to norm (EG1 = 2 people, EG2 = 4 people), while one opposite case was observed in CG. However, the obtained results did not show a significant difference between EG1 and EG2 measured over time (p = 0.184, t = 1.339). Change in depression symptoms assessed with the use of the GDS scale was not associated with an improvement in cognitive performance in any of the cognitive domains enhanced after the intervention (MoCA p = 0.395, TMT A p = 0.954, Digit Span p = 0.952, 0 p = 0.667, Phonemic Fluency p = 0.333, List Recall p = 0.437, Logic Memory I p = 0.205). Detailed scores are described in Tables 2, 3.
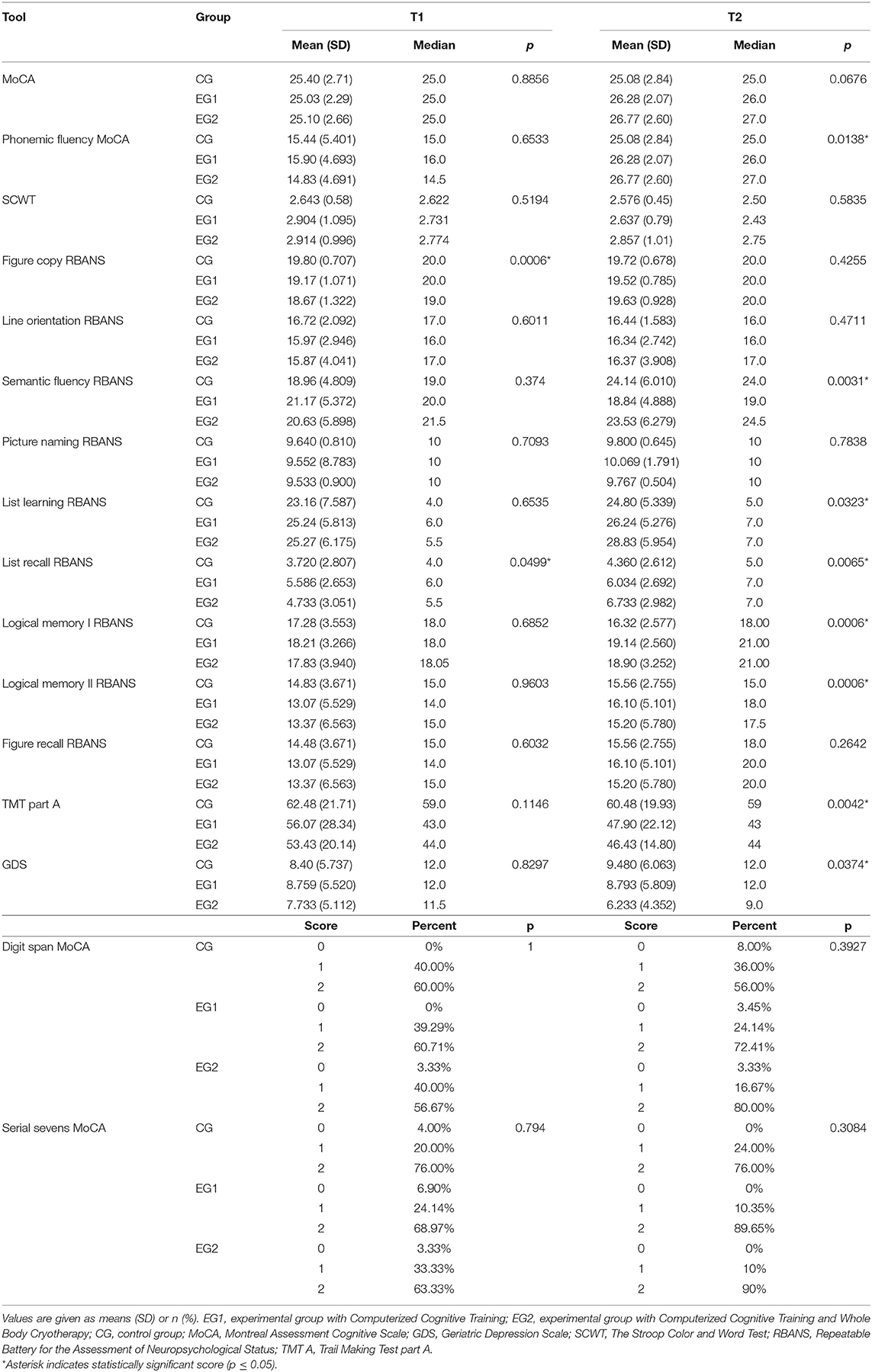
Table 2. Primary and secondary outcome measures obtained in baseline and follow-up.
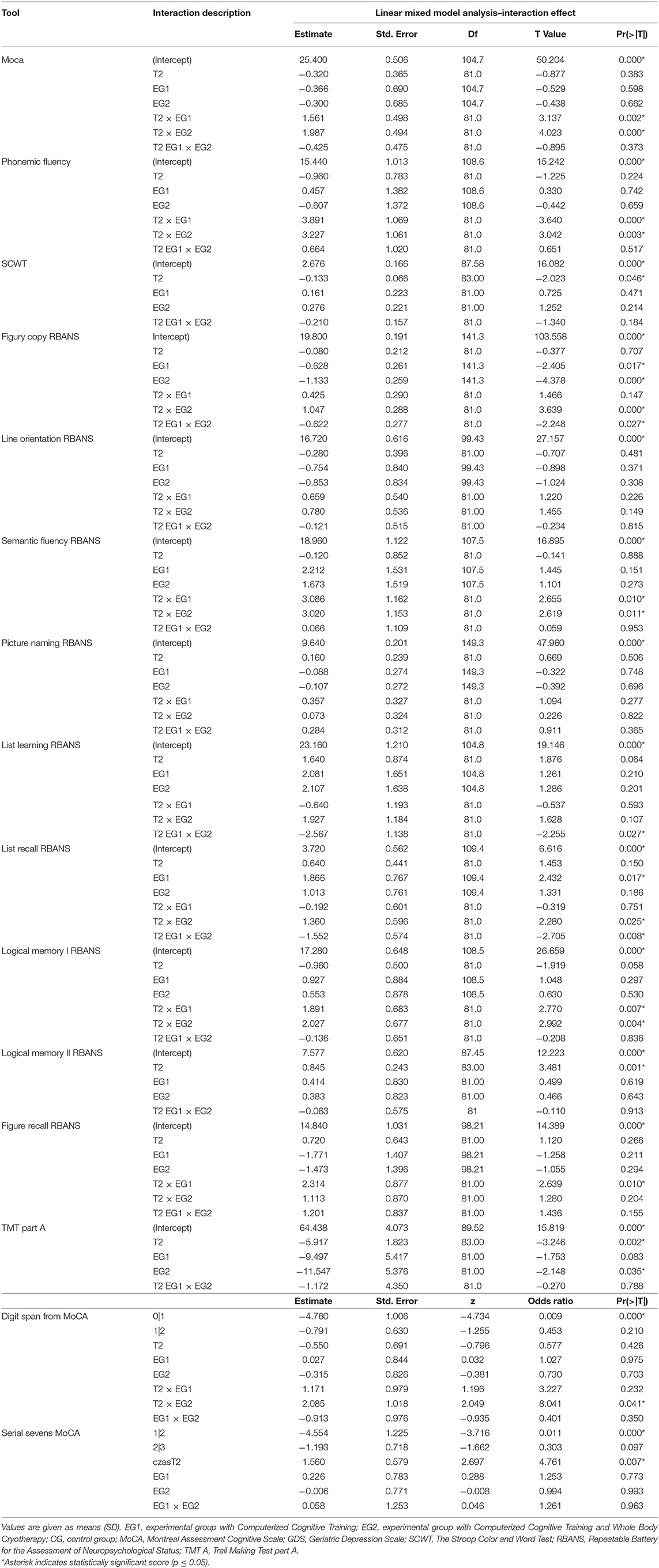
Table 3. Linear mixed model analysis results (T1, T2).
Discussion
In the past decade, we have been observing increasing interest in developing non-pharmacological procognitive interventions aimed at maintaining cognitive performance and delaying the onset of dementia. In the present study, we evaluated a combination of two different stimulating interventions: CCT and WBC administered to individuals with MCI and cognitive norm. The results indicated that CCT, especially combined with WBC, may lead to the improvement of already deteriorated cognitive functions. Moreover, combining CCT with WBC seems to result in a reduction of depressive symptoms.
In the case of global cognitive functioning measured by MoCA, we observed significantly higher scores in T2 in both EGs in relation to CG. In the assessment of specific cognitive domains, we also observed some positive changes. In EG1, the group in which only CCT was conducted, the improvement was particularly visible with regard to: attentional control (the ability to concentrate), sustained attention (the ability to maintain concentration) (Digit Span from MoCA), psychomotor speed (TMT: part A), verbal productivity (Sematic Fluency from RBANS and Phonemic Fluency from MoCA) and immediate memory (Logical Memory I from RBANS). The present findings are thus compliant with the nature of the Mind Academy® CCT, which focuses on such cognitive functions as attention (selective, sustained, divided, and executive), various memory and planning tasks and psychomotor speed. What is more, the group format of the training and the fact that the participants were given home tasks, which were presented publicly afterwards, resulted in increased social interaction, which might have led to the observed improvement in verbal fluency. The results are also consistent with some other studies on the effectiveness of CCT, which reported improvement in global functioning (40, 41), processing speed (42), immediate memory (41, 43, 44), and phonological fluency (45).
Moreover, the results of our study suggest that combining CCT with WBC leads to a slight enhancement of the procognitive effect of CCT as in two subtests (Figure Copy and List Recall from RBANS) the difference in the performance in T2 was statistically significant, in favor of EG2 (CCT + WBC). What is more, the impact of CCT alone on depressive symptoms was very limited, and the combination of CCT and WBC allowed us to address this issue, since a reduction in depressive symptoms was observed in the combined intervention, but not in CCT alone. This indicates that WBC affects the mood regardless of social interactions. Our results are in line with the results of other studies aimed at addressing alterations of mood after cryotherapy sessions (19, 46, 47). Seeing that the change in depression symptoms assessed by the GDS scale was not associated with an improvement in cognitive performance in any of the cognitive domains enhanced after the intervention, we may conclude that the improvement was probably caused by the intervention itself, not by the reduction of depressive symptoms.
Notably, the results of this study could suggest that WBC may improve cognition in humans. However, the exact mechanisms underlying the impact of cryogenic temperature on cognitive functioning requires further investigation (29). As current research suggests (48, 49), BDNF (brain-derived neurotrophic factor) could be a potential mediator of this effect. BDNF is a growth factor of the central nervous system, crucial for neuronal development and maintaining proper brain functions, such as cognition (50). By activating the pathways responsible for the regulation of neuron survival, BDNF acts in a neuroprotective way and helps prevent or inhibit the pathophysiological processes leading to cognitive deterioration (48, 49). Therefore, we recommend further research on the effectiveness of WBC, in which BDNF will be measured before and after the WBC/WBC + CCT intervention.
There were several limitations to the current study, apart from the relatively small sample and the lack of randomized allocation to the experimental groups and the control group. Firstly, it was not designed to examine the stability of CCT and WBC benefits over time. Secondly, it was a single-blinded trial; while it seems impossible to blind the trainee and participants, given the nature of the interventions, it nevertheless introduces the risk of expectation bias. Thirdly, it was difficult to distinguish specific contributions of the psychoeducation part and group tasks to cognitive improvement in participants. The Mind Academy® was intentionally designed as a multifaceted, enjoyable cognitive training that acquaints participants with knowledge of health-aging rules, and specific mnemotechnics. Therefore, we cannot conclude whether CCT used individually and without the psychoeducational part is as effective as CCT used in a group setting in combination with psychoeducation. Fourthly, we should note that all participants of the project were seniors purposely seeking stimulating activities. Keeping in mind that volunteers for research projects tend to be highly educated with higher socio-economic status (51), less anxious (52), and even healthier (53, 54) than general population, we should be aware of the risk of volunteer bias in the study sample. Fiftly, we choose 14 different subtest (two for each cognitive domain) for cognitive function assessment and the abundance of them may have increased a risk of making a type I error (“false positivity”). On the other hand, given concerns about statistical power (related to relatively low sample size in our study), we opted not to use correction for multiple tests in order to avoid type II error (“false negativity”). At the same time, the most prominent asset of the study was the fact that it assessed the effectiveness of two innovative approaches to cognitive function enhancement. Both approaches possess documented distinct mechanisms of impacting human brain. CCT is believed to induce the formation of new neuronal connections (neuroplasticity) and maintain the already existing pathways, while, WBC targets the neurodegenerative process by means of regulating the production of inflammatory mediators, such as cytokines IL-6 and IL-10 (55), nitric oxide (NO) (22). These mediators are released as a consequence of amyloid-beta deposition and the inflammatory response caused by the deposits. To our knowledge, no intervention study combining these two procognitive approaches and investigating whether WBC may enhance CCT's effectivity has been conducted before.
Moreover, unlike most related studies that focus on people already having major cognitive problems, we included only high-risk individuals. Accordingly, we could evaluate the effectiveness of CCT/CCT + WBC in seniors who experience slight cognitive decline and seek beneficial methods of slowing down the deteriorative process. What is more, the methods proposed by us are safe, widely available and low-cost, enabling their common use and implementation as a non-pharmacological intervention aimed at maintaining good cognitive performance.
In this study, we examined the effectiveness of Computerized Cognitive Training (CCT) combined with Whole Body Cryotherapy (WCB) in improving cognitive functions in older adults. We compared the results of patients from three groups: two experimental groups–EG1, in which CCT was used alone, EG2, in which interventions (CCT + WBC) were combined, and a control group, which included patients receiving usual care. After examining the results, the statistical analysis conducted by us showed that after the intervention the performance in the assessment of general cognitive functioning increased in both EGs. A significant improvement was also visible in several cognitive domains such as: verbal productivity, learning ability, and immediate memory, delayed memory, attentional control and information processing at T2 compared to T1 (p ≤ 0.05). Nevertheless, only in the group with combined interventions (CCT + WBC) the participants presented significantly less depressive symptoms (p ≤ 0.05), and we claim that in order to address cognitive decline and mood decline, CCT, and WBC ought to be combined.
Future studies should shed more light on the sustainability of benefits obtained as a result of procognitive interventions (longitudinal assessment). Additionally, they should investigate whether the transfer of skills acquired during the training occurs e.g., depending on whether the participants who have undergone CCT/CCT + WBC are more cognitively efficient in their every-day life. Further, well-designed randomized clinical trials on WBC and WBC + CCT would help provide more definitive evidence regarding the efficacy of these methods. Additionally, more investigation (e.g., in animal models) is needed in order to determine the mechanisms underlying WBC, namely the pathway linking exposure to extreme cold to the regulation of the inflammatory response.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
Ethics Statement
The studies involving human participants were reviewed and approved by Bioethical Committee (number KB61/218) at Wroclaw Medical University. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
AS and RW conceived and planned the study. AS, DS, and RW carried out the study. AS took the lead in writing the manuscript. All authors contributed to the interpretation of the results, provided critical feedback, and helped to shape the research, analysis, and manuscript.
Funding
The study was funded by the statutory funds of the Wroclaw Medical University in cooperation with the company Creator Sp. z o.o. in Wrocław. The funding institution had no role in the study design, collection, analysis, or interpretation of the data, writing the manuscript, or the decision to submit the paper for publication.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Abbreviations
WBC, whole-body cryotherapy; CCT, computerized cognitive training; EG, experimental group; CG, control group; SCD, subjective cognitive decline; MoCA, Montreal Assessment Scale; TMT, Trail Making Test; RBANS, Repeatable Battery for the Assessment of Neuropsychological Status; SCWT, The Stroop Color and Word Test; GDS, Geriatric Depression Scale; BDNF, brain-derived neurotrophic factor; NO, nitric oxide.
References
1. United Nations Department of Economic and Social Affairs Population Division. World Population Prospects 2019: Highlights. ST/ESA/SER.A/423 (2019).
2. Mahncke HW, Connor BB, Appelman J, Ahsanuddin ON, Hardy JL, Wood RA, et al. Memory enhancement in healthy older adults using a brain plasticity-based training program: a randomized, controlled study. Proc Natl Acad Sci. (2006) 103:12523–8. doi: 10.1073/pnas.0605194103
3. Mrakic-Sposta S, Di Santo SG, Franchini F, Arlati S, Zangiacomi A, Greci L, et al. Effects of combined physical and cognitive virtual reality-based training on cognitive impairment and oxidative stress in MCI patients: a pilot study. Front Aging Neurosci. (2018) 10:282. doi: 10.3389/fnagi.2018.00282
4. Rouse HJ, Small BJ, Faust ME. Assessment of cognitive training & social interaction in people with mild to moderate dementia: a pilot study. Clin Gerontol. (2019) 42:421–34. doi: 10.1080/07317115.2019.1590489
5. Jing W, Willis R, Feng Z. Factors influencing quality of life of elderly people with dementia and care implications: a systematic review. Arch Gerontol Geriatr. (2016) 66:23–41. doi: 10.1016/j.archger.2016.04.009
6. Urbańska K, Szcześniak D, Rymaszewska J. The stigma of dementia. Postep Psychiatr i Neurol. (2015) 24:225–30. doi: 10.1016/j.pin.2015.10.001
7. Tagliabue CF, Guzzetti S, Gualco G, Boccolieri G, Boccolieri A, Smith S, et al. A group study on the effects of a short multi-domain cognitive training in healthy elderly Italian people. BMC Geriatr. (2018) 18:321. doi: 10.1186/s12877-018-1014-x
8. Schultheisz TSDV, Aquino RR de, Alves ABF, Radl ALM, Serafim A de P. Effect of cognitive stimulation workshops on the self-esteem and cognition of the elderly: a pilot project. Dement e Neuropsychol. (2018) 12:421–6. doi: 10.1590/1980-57642018dn12-040013
9. Shao Y, Mang J, Li P, Wang J, Deng T, Xu Z. Computer-based cognitive programs for improvement of memory, processing speed and executive function during age-related cognitive decline: a meta-analysis. PLoS ONE. (2015) 10:e0130831. doi: 10.1371/journal.pone.0130831
10. Turunen M, Hokkanen L, Bäckman L, Stigsdotter-Neely A, Hänninen T, Paajanen T, et al. Computer-based cognitive training for older adults: determinants of adherence. PLoS ONE. (2019) 14:e0219541. doi: 10.1371/journal.pone.0219541
11. Duda BM, Sweet LH. Functional brain changes associated with cognitive training in healthy older adults: a preliminary ALE meta-analysis. Brain Imaging Behav. (2020) 14:1247–62. doi: 10.31234/osf.io/5kj3z
12. Li BY, He NY, Qiao Y, Xu HM, Lu YZ, Cui PJ, et al. Computerized cognitive training for Chinese mild cognitive impairment patients: a neuropsychological and fMRI study. NeuroImage Clin. (2019) 22:101691. doi: 10.1016/j.nicl.2019.101691
13. Senczyszyn A, Wallner R. Cognitive training and cognitive rehabilitation as non-pharmacological therapeutic strategies inParkinson's disease: areview of research. Aktual Neurol. (2019) 18:85–93. doi: 10.15557/AN.2018.0012
14. Clare L, Woods B, Moniz Cook ED, Orrell M, Spector A. Cognitive rehabilitation cognitive training for early-stage Alzheimer's disease vascular dementia. In: Clare L, , editor. Cochrane Database of Systematic Reviews. Chichester: John Wiley & Sons, Ltd. (2003) p. CD003260.
15. Naismith SL, Mowszowski L, Diamond K, Lewis SJG. Improving memory in Parkinson's disease: a healthy brain ageing cognitive training program. Mov Disord. (2013) 28:1097–103. doi: 10.1002/mds.25457
16. Petrelli A, Kaesberg S, Barbe MT, Timmermann L, Fink GR, Kessler J, et al. Effects of cognitive training in Parkinson's disease: a randomized controlled trial. Parkinsonism Relat Disord. (2014) 20:1196–202. doi: 10.1016/j.parkreldis.2014.08.023
17. Jastrzabek R, Straburzyńska-Lupa A, Rutkowski R, Romanowski W. Effects of different local cryotherapies on systemic levels of TNF-α, IL-6, and clinical parameters in active rheumatoid arthritis. Rheumatol Int. (2013) 33:2053–60. doi: 10.1007/s00296-013-2692-5
18. Pawik M, Kowalska J, Rymaszewska J. The effectiveness of whole-body cryotherapy and physical exercises on the psychological well-being of patients with multiple sclerosis: a comparative analysis. Adv Clin Exp Med. (2019) 28: 1477–83. doi: 10.17219/acem/104529
19. Rymaszewska J, Tulczynski A, Zagrobelny Z, Kiejna A, Hadrys T. Influence of whole body cryotherapy on depressive symptoms–preliminary report. Acta Neuropsychiatr. (2003) 15:122–8. doi: 10.1034/j.1601-5215.2003.00023.x
20. Stanek A, Cholewka A, Wielkoszyński T, Romuk E, Sieroń A. Whole-body cryotherapy decreases the levels of inflammatory, oxidative stress, and atherosclerosis plaque markers in male patients with active-phase ankylosing spondylitis in the absence of classical cardiovascular risk factors. Mediators Inflamm. (2018) 2018:8592532 doi: 10.1155/2018/8592532
21. Rymaszewska J, Stańczykiewicz B, Lion K, Misiak B. The impact of whole-body cryotherapy on lipid profile: a systematic review and meta-analysis. Complement Ther Med. (2020) 55:102568. doi: 10.1016/j.ctim.2020.102568
22. Rymaszewska J, Lion KM, Pawlik-Sobecka L, Pawłowski T, Szcześniak D, Trypka E, et al. Efficacy of the whole-body cryotherapy as add-on therapy to pharmacological treatment of depression-a randomized controlled trial. Front Psychiatry. (2020) 11:522. doi: 10.3389/fpsyt.2020.00522
23. Aliev G, Smith MA, Obrenovich ME, De La Torre JC, Perry G. Role of vascular hypoperfusion-induced oxidative stress and mitochondria failure in the pathogenesis of Alzheimer's disease. Neurotox Res. (2003) 5:491–504. doi: 10.1007/BF03033159
24. Grammas P. Neurovascular dysfunction, inflammation and endothelial activation: Implications for the pathogenesis of Alzheimer's disease. J Neuroinflammation. (2011) 8:1–12. doi: 10.1186/1742-2094-8-26
25. Silva MVF, Loures CDMG, Alves LCV, De Souza LC, Borges KBG, Carvalho MDG. Alzheimer's disease: risk factors and potentially protective measures. J Biomed Sci. (2019) 26:1–11. doi: 10.1186/s12929-019-0524-y
26. Fan L, Mao C, Hu X, Zhang S, Yang Z, Hu Z, et al. New insights into the pathogenesis of Alzheimer's disease. Front Neurol. (2020) 10:1–12. doi: 10.3389/fneur.2019.01312
27. Stanek A, Cholewka A, Gadula J, Drzazga Z, Sieron A, Sieron-Stoltny K. Can whole-body cryotherapy with subsequent kinesiotherapy procedures in closed type cryogenic chamber improve BASDAI, BASFI, and some spine mobility parameters and decrease pain intensity in patients with ankylosing spondylitis? Biomed Res Int. (2015) 2015:404259. doi: 10.1155/2015/404259
28. Lombardi G, Ziemann E, Banfi G. Whole-body cryotherapy in athletes: from therapy to stimulation. An Updated Review of the Literature. Front Physiol. (2017) 8:258. doi: 10.3389/fphys.2017.00258
29. Misiak B, Kiejna A. Translating whole-body cryotherapy into geriatric psychiatry - a proposed strategy for the prevention of Alzheimer's disease. Med Hypotheses. (2012) 79:56–8. doi: 10.1016/j.mehy.2012.03.033
30. Nasreddine ZS, Phillips NA, Bédirian V, Charbonneau S, Whitehead V, Collin I, et al. The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc. (2005) 53:695–9. doi: 10.1111/j.1532-5415.2005.53221.x
31. Magierska J, Magierski R, Fendler W, Kłoszewska I, Sobów TM. Zastosowanie polskiej adaptacji montrealskiego testu do oceny funkcji poznawczych (MoCA) w przesiewowej ocenie funkcji poznawczych. Neurol Neurochir Pol. (2012) 46:130–9. doi: 10.5114/ninp.2012.28255
32. Yesavage JA, Brink TL, Rose TL, Lum O, Huang V, Adey M, et al. Development and validation of a geriatric depression screening scale: a preliminary report. J Psychiatr Res. (1982) 17:37–49. doi: 10.1016/0022-3956(82)90033-4
33. Albiński R, Kleszczewska-Albińska A, Bedyńska S. [Geriatric Depression Scale (GDS). Validity and reliability of different versions of the scale–review]. Psychiatr Pol. (2011) 45:555–62.
34. Kim K, Han JW, So Y, Seo J, Kim YJ, Park JH, et al. Cognitive stimulation as a therapeutic modality for dementia: a meta-Analysis. Psychiatry Investig. (2017) 14:626–39. doi: 10.4306/pi.2017.14.5.626
35. Rymaszewska J, Skrzek A, Giemza Cz, Piotrowska A, Kikowski Ł, Kabała T, et al. The Code of Good Practice in Systemic Cryotherapy. Available online at: https://kriokomory.pl/kodeks/ (accessed May 31, 2021).
36. Tombaugh TN. Trail Making Test A and B: Normative data stratified by age and education. Arch Clin Neuropsychol. (2004) 19:203–14. doi: 10.1016/S0887-6177(03)00039-8
37. Rajtar-Zembaty A, Przewoznik D, Bober-Płonka B, Starowicz-Filip A, Rajtar-Zembaty J, Nowak R, et al. Zastosowanie Testu Łaczenia Punktów do oceny elastyczności poznawczej u chorych z zaburzeniami mowy po udarze mózgu. Aktual Neurol. (2015) 15:11–7. doi: 10.15557/AN.2015.0002
38. Morrow SA. Normative data for the stroop color word test for a North American population. Can J Neurol Sci. (2013) 40:842–7. doi: 10.1017/S0317167100015997
39. Silverberg ND, Wertheimer JC, Fichtenberg NL. An effort index for the Repeatable Battery for the Assessment of Neuropsychological Status (RBANS). Clin Neuropsychol. (2007) 21:841–54. doi: 10.1080/13854040600850958
40. González-Palau F, Franco M, Bamidis P, Losada R, Parra E, Papageorgiou SG, et al. The effects of a computer-based cognitive and physical training program in a healthy and mildly cognitive impaired aging sample. Aging Ment Heal. (2014) 18:838–46. doi: 10.1080/13607863.2014.899972
41. Bahar-Fuchs A, Webb S, Bartsch L, Clare L, Rebok G, Cherbuin N, et al. Tailored and adaptive computerized cognitive training in older adults at risk for dementia: a randomized controlled trial. J Alzheimers Dis. (2017) 60:889–911. doi: 10.3233/JAD-170404
42. Lin F, Heffner KL, Ren P, Tivarus ME, Brasch J, Chen DG, et al. Cognitive and neural effects of vision-based speed-of-processing training in older adults with amnestic mild cognitive impairment: a pilot study. J Am Geriatr Soc. (2016) 64:1293–8. doi: 10.1111/jgs.14132
43. Basak C, Boot WR, Voss MW, Kramer AF. Can training in a real-time strategy video game attenuate cognitive decline in older adults? Psychol Aging. (2008) 23:765–77. doi: 10.1037/a0013494
44. Rosen AC, Sugiura L, Kramer JH, Whitfield-Gabrieli S, Gabrieli JD. Cognitive training changes hippocampal function in mild cognitive impairment: a pilot study. J Alzheimers Dis. (2011) 26:349–57. doi: 10.3233/JAD-2011-0009
45. Barban F, Annicchiarico R, Pantelopoulos S, Federici A, Perri R, Fadda L, et al. Protecting cognition from aging and Alzheimer's disease: a computerized cognitive training combined with reminiscence therapy. Int J Geriatr Psychiatry. (2016) 31:340–8. doi: 10.1002/gps.4328
46. Rymaszewska J, Ramsey D. Whole body cryotherapy as a novel adjuvant therapy for depression and anxiety. Arch Psychiatry Psychother. (2008) 56:63–8. doi: 10.1007/s00005-008-0006-5
47. Rymaszewska J, Urbanska K, Szcześniak D, Pawłowski T, Pieniawska-Smiech K, Kokot I, et al. Whole-body cryotherapy - promising add-on treatment of depressive disorder. Psychiatr Pol. (2018) 53: 1053–67. doi: 10.12740/PP/OnlineFirst/91298
48. Giuffrida ML, Copani A, Rizzarelli E. A promising connection between BDNF and Alzheimer's disease. Aging. (2018) 10:1791–2. doi: 10.18632/aging.101518
49. Ng TKS, Ho CSH, Tam WWS, Kua EH, Ho RCM. Decreased serum brain-derived neurotrophic factor (BDNF) levels in patients with Alzheimer's disease (AD): a systematic review and meta-analysis. Int J Mol Sci. (2019) 20:1–26. doi: 10.3390/ijms20020257
50. Hayashi H, Takagi N. Endogenous neuroprotective molecules and their mechanisms in the central nervous system. Biol Pharm Bull. (2015) 38:1104–8. doi: 10.1248/bpb.b15-00361
51. Peters-Davis ND, Burant CJ, Braunschweig HM. Factors associated with volunteer behavior among community dwelling older persons. Act Adapt Aging. (2001) 26:29–44. doi: 10.1300/J016v26n02_03
52. Almeida L, Kashdan TB, Nunes T, Coelho R, Albino-Teixeira A, Soares-Da-Silva P. Who volunteers for phase I clinical trials? Influences of anxiety, social anxiety and depressive symptoms on self-selection and the reporting of adverse events. Eur J Clin Pharmacol. (2008) 64:575–82. doi: 10.1007/s00228-008-0468-8
53. Jordan S, Watkins A, Storey M, Allen SJ, Brooks CJ, Garaiova I, et al. Volunteer bias in recruitment, retention, and blood sample donation in a randomised controlled trial involving mothers and their children at six months and two years: a longitudinal analysis. PLoS ONE. (2013) 8:e67912 doi: 10.1371/journal.pone.0067912
54. De Barreto PS, Ferrandez AM, Saliba-Serre B. Are older adults who volunteer to participate in an exercise study fitter and healthier than non-volunteers? The participation bias of the study population. J Phys Act Heal. (2013) 10:359–67. doi: 10.1123/jpah.10.3.359
Keywords: mild cognitive impairment, cognitive functions, whole body cryotherapy, computerized cognitive training, dementia, aging, non-pharmacological methods
Citation: Senczyszyn A, Wallner R, Szczesniak DM, Łuc M and Rymaszewska J (2021) The Effectiveness of Computerized Cognitive Training Combined With Whole Body Cryotherapy in Improving Cognitive Functions in Older Adults. A Case Control Study. Front. Psychiatry 12:649066. doi: 10.3389/fpsyt.2021.649066
Received: 03 January 2021; Accepted: 01 June 2021;
Published: 25 June 2021.
Edited by:
Marc Fakhoury, Lebanese American University, LebanonReviewed by:
Cristiano Capurso, University of Foggia, ItalyBenoit Michel Dugue, University of Poitiers, France
Copyright © 2021 Senczyszyn, Wallner, Szczesniak, Łuc and Rymaszewska. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Adrianna Senczyszyn, YWRyaWFubmEuc2VuY3p5c3p5bkBzdHVkZW50LnVtZWQud3JvYy5wbA==