 Samuel Cyr1,2†
Samuel Cyr1,2† Marie-Joelle Marcil1,3†
Marie-Joelle Marcil1,3† Marie-France Marin3,4,5Jean-Claude Tardif1,6
Marie-France Marin3,4,5Jean-Claude Tardif1,6 Stéphane Guay3,7Marie-Claude Guertin8
Stéphane Guay3,7Marie-Claude Guertin8 Camille Rosa8Christine Genest9
Camille Rosa8Christine Genest9 Jacques Forest10Patrick Lavoie1,9Mélanie Labrosse6,11Alain Vadeboncoeur1,6Shaun Selcer1,6
Jacques Forest10Patrick Lavoie1,9Mélanie Labrosse6,11Alain Vadeboncoeur1,6Shaun Selcer1,6 Simon Ducharme12,13
Simon Ducharme12,13 Judith Brouillette1,3*
Judith Brouillette1,3*- 1Research Center, Montreal Heart Institute, Montreal, QC, Canada
- 2Faculty of Pharmacy, Université de Montréal, Montreal, QC, Canada
- 3Department of Psychiatry and Addiction, Université de Montréal, Montreal, QC, Canada
- 4Department of Psychology, Université du Québec à Montréal, Montreal, QC, Canada
- 5Research Center, Institut universitaire en santé mentale de Montréal, Montreal, QC, Canada
- 6Faculty of Medicine, Université de Montréal, Montreal, QC, Canada
- 7Centre D'étude sur le Trauma, Centre de Recherche de l'Institut Universitaire en Santé Mentale de Montréal, Montreal, QC, Canada
- 8Montreal Health Innovations Coordinating Center, Montreal, QC, Canada
- 9Faculty of Nursing, Université de Montréal, Montreal, QC, Canada
- 10Department of Organization and Human Resources, ESG UQAM, Montreal, QC, Canada
- 11Division of Emergency Medicine, Department of Pediatrics, Centre hospitalier universitaire Sainte-Justine, Montreal, QC, Canada
- 12Department of Psychiatry, Douglas Mental Health University Institute, McGill University, Montreal, QC, Canada
- 13McConnell Brain Imaging Centre, Montreal Neurological Institute, McGill University, Montreal, QC, Canada
Objective: This study examined how best to identify modifiable protective and risk factors for burnout in healthcare workers in the face of the COVID-19 pandemic. Individual, occupational, organizational and social factors were investigated. The study also assessed the impact of these factors on post-traumatic stress disorder (PTSD), anxiety, and depression.
Methods: Healthcare workers in the Quebec (Canada) healthcare system were recruited between May 21 to June 5, 2020. Participants answered an electronic survey 3 months after the COVID-19 epidemic outbreak began in Canada. Using the Maslach Burnout Inventory, PTSD Checklist for DSM-5, and Hospital Anxiety and Depression Scale, we studied the prevalence of burnout, PTSD, anxiety and depression in this cohort. Multivariable logistic or linear regression models including resilience, social and organizational support, workload and access to mental health help, simulation techniques and protective personal equipment (PPE) as well as perception of PPE security were conducted for each outcome.
Results: In mid-June 2020, 467 participants completed the survey. We found that half (51.8%) of the respondents experienced burnout characterized by emotional exhaustion and/or depersonalization at least once a week. In total, 158 healthcare workers (35.6%) displayed severe symptoms of at least one of the mental health disorders (24.3% PTSD, 23.3% anxiety, 10.6% depression). Resilience (OR = 0.69, 95% CI: [0.55–0.87]; p = 0.002) and perceived organizational support (OR = 0.75, 95% CI: [0.61–0.93]; p = 0.009) were significantly associated with burnout and other outcomes. Social support satisfaction, perception of PPE security, work type and environment, mental health antecedents and reassignment were associated with PTSD and/or anxiety and/or depression, but not burnout.
Conclusion: Future studies should address primarily resilience and perceived organizational support to promote mental health and prevent burnout, PTSD, anxiety and depression.
Introduction
As of May 6, 2021, over 155 million people have been affected by the SARS-CoV2 virus and over 3 million people have died after developing COVID-19 (https://coronavirus.jhu.edu/map.html). Healthcare workers are at high risk of contracting SARS-CoV2 (1) and constitute around 10% of all confirmed cases in North America, roughly 10 to 20% in European countries and nearly 5% in China (2). In the province of Quebec, Canada, 17.2% of COVID-19 confirmed cases were medical workers (3). In addition to managing their own health and that of the population, they have to cope with rapidly changing organizational, occupational, and familial functioning. This has placed additional pressure on these professionals, in whom 30% reported burnout (4, 5) prior to the COVID-19 pandemic. Burnout is not officially considered a mental health disorder (unlike depression) but is rather defined as an occupational phenomenon “resulting from chronic workplace stress that has not been successfully managed” (6). It is characterized by “feelings of energy exhaustion; increased mental distance from work; and reduced professional efficacy.” Knowledge of the psychological impacts of the COVID-19 pandemic on health professionals, mostly physicians and nurses, is rapidly emerging (7, 8). A few studies have directly addressed burnout symptoms (9–25), including a recent meta-analysis that reported a pooled prevalence of 37.4% among healthcare workers (26).
Pre-pandemic research on burnout in healthcare workers has identified neuroticism, high workload, value incongruence, and poor job climate as risk factors (22, 27–30). In contrast, higher perceived social support and job resources protect against it (22, 27–30). Considering the impact of burnout on both the professional and personal lives of healthcare workers as well as the potential negative impact on the quality of care provided to patients (31), it is important to study the factors associated with burnout following the COVID-19 pandemic. To our knowledge, no study combined in the same analysis organizational [e.g., perceived organizational support, defined by the extent in which the organization values contributions and cares about well-being (32)], occupational (e.g., workload) and individuals [e.g., resilience, defined by positive adjustment in response to stress or trauma and measured with Connor-Davidson Resilience Scale (33)] as potential factors. Moreover, social support has been infrequently studied in the recent COVID-19 literature on burnout among healthcare workers, with only one study reporting it as a factor to be considered (34). The primary objective of our study is to identify modifiable protective and risk factors associated with burnout in a wide range of healthcare workers facing the COVID-19 pandemic. Individual, occupational, organizational, and social factors will be investigated with the objective to determine the most promising field to address for future interventions. Secondarily, we aim to study the impact of the same factors on post-traumatic stress disorder (PTSD), anxiety, and depression. Knowledge of potential protection and risk factors is crucial to roll out strategies to limit the impact of other crises similar to the COVID-19 pandemic.
Methods
Design
This cross-sectional study was approved by the ethics committees of the Montreal Heart Institute on May 14th, 2020. It comprises an electronic survey performed at 3 months (June 2020) after the start of the COVID-19 epidemic outbreak in Quebec, Canada (March 2020).
The Montreal Health Innovations Coordination Center (MHICC) specifically developed the web platform for the present study. The system used the MHICC extranet portal with secure access to web pages by a Transport Layer Security (TLS) certificate, using standard encryption technology (2,048 bit private key length and 128-bit bulk encryption key length) and an auto logoff function in the event of a sustained period of inactivity. The data collected using this platform was sent and saved to the MHICC for a period of 10 years. Each participant only had access to their own data, and in no case had access to the data of other participants. The platform was accessible in French and in English via a smartphone, a tablet or a computer.
Between May 21st and June 5th 2020, the study team recruited healthcare workers from across Quebec's healthcare system, including those in long-term care centers (in French: Centres d'hébergement de soins de longue durée [CHSLD]). To do so, we shared a newsletter explaining the objectives of the study through study collaborators' social media accounts, Quebec health professional organizations and association's networks, and conventional media. The newsletter directed the interested healthcare workers to a web page that served as an initial screening for eligibility for participation. All participants were required to have access to an e-mail address and the Internet, had to be age 18 or over and had to work as one of the listed health care work types (administrative agent, beneficiary attendant, doctor/resident doctor, laboratory technician, kitchen attendant, maintenance agent, administrator, nurse, other health professional [occupational therapists, respiratory therapists, nutritionists, psychologists, social workers, etc.]). After reading the information and consent form, the users could sign it, if desired, to become participants in the study. In addition to the survey, we asked participants if they wanted to be contacted by the research team for (1) a post-survey follow-up to collect their comments and/or questions and/or (2) feedback on their individual results if the questionnaires indicated risks of developing PTSD, anxiety or depression (while facilitating access to psychology or other mental health resources). In addition, all participants could contact the research team by phone or e-mail if they had any questions related to the research project or if they needed either psychology referral, or referral to any other mental health organizations. It should be noted that we did not use the snowball sampling technique here since the subjects who consented to participate were not invited to continue recruiting among their affiliation (35, 36).
In mid-June 2020, study coordinators sent one to three e-mails to invite participants to complete the 3-month online survey. Participants had 1 week to respond and partially completed surveys were accepted.
Measures
The main features of the tools used are presented here, but additional details about the surveyed measures are described in Supplementary Table A1 of Appendix 1. The presence of burnout was studied using the Maslach Burnout Inventory (MBI 2). The questions evaluate two dimensions of burnout syndrome, namely emotional exhaustion (“I feel burned out from my work”) and depersonalization (“I have become more callous toward people”) on a scale ranging from 0 (“never”) to 6 (“everyday”). The participant must experience at least weekly emotional exhaustion and/or depersonalization to be considered burned out (37, 38). This questionnaire has an adequate reliability, with an internal consistency of α = 0.80 (39). PTSD, anxiety, and depression symptoms were studied as continuous variables. PTSD was checked using total scores on the PTSD Checklist for DSM-5 (PCL-5), a 20-item self-report measure that assesses symptoms of PTSD with a high internal consistency (α = 0.94) (40, 41). PCL-5 corresponds mainly to the DSM-5 criteria with a variation of criterion A. Indeed, “exposure to actual death or threatened death, serious injury, or sexual violence” (42) is replaced by a “very stressful experience” without specification about COVID-19 context. Each item is rated on a scale of 0 to 4 and a score is generated (0–80). Anxiety and depression symptoms were verified using the Hospital Anxiety and Depression Scale (HADS), a questionnaire composed of 14 items in total, separated into two scales of 7 items each (anxiety and depression). Internal consistency is high for both HADS-A (α = 0.83) and for HADS-D (α = 0.82) (43–45). Items are graded on a scale of 0 to 3 and a score is produced for each of the two sub-scales (0–21). We used cut-off scores of 31 or more for PCL-5, and 11 or more for each component of HADS, as clinically significant PTSD (40, 46, 47), anxiety or depression symptoms (45).
Resilience, self-compassion, social and organizational support were measured with the Connor-Davidson Resilience Scale [α = 0.85 (33)], the Self-Compassion Scale [α = 0.91 (48)], the Social Support Questionnaire [α = 0.79 (49)] and the Perceived Organizational Support Questionnaire [α = 0.93 (50)], respectively. We also measured access to personal protective equipment (PPE) and feeling of security “When you used personal protective equipment as part of your duties, you felt [Totally safe to Totally at risk].” Socio-demographic (including sex), work type (including intensive care or emergency work, direct care of COVID patients, and reassignment), type of work environment, workload, medical characteristics (including COVID status), access to simulation technique and mental help data were also collected.
Sample Size Calculation
We calculated the sample size based on a simple logistic regression model with resilience as the single independent variable of interest. Then, we made a correction based on the correlation between the variable of interest and the model's other independent variables. The expected overall burnout rate at 3 months was 50% (21). Using a simple logistic regression model with one continuous independent variable of interest at a two-sided 0.05 significant level, a sample size of 285 participants would provide 80% power to detect an odds ratio of 0.72 for an increase of one standard deviation (SD) of the independent variable. This odds ratio is comparable to the one reported in a study on burnout and work-life balance satisfaction of physicians and the general US working population (5). In the context that our recruitment was successful, we then decided to increase our sample size objective to 500 participants. Using the same assumption as stated before (50% burnout rate), a sample size of 500 participants would provide 80% power to detect an odds ratio of 0.75 for an increase of one SD of the independent variable with a simple logistic regression at a two-sided 0.05 significant level.
Analyses
Study characteristics were summarized using counts and percentages for categorical variables and mean ± SD for continuous variables. To identify the survey response rate, we divided the number of participants who completed the survey by the total number of participants who consented to participate in the study and then multiplied by 100 to obtain a percentage. For each efficacy endpoint (burnout, PTSD, anxiety or depression), a multivariable logistic (or linear) regression model including all the pre-specified independent variables of clinical interest (resilience, social support, workload, perceived organizational support, access to mental health help, access to PPE, feeling of security using PPE and access to simulation techniques) was fit first. No variable selection was done at this stage and all independent variables were included. The pre-specified adjustment variables (psychiatric antecedents, type of employment, intensive care or emergency work, type of environment, COVID status, direct care of COVID patients, reassignment, sex) showing a p-value lower than 0.2 in univariate models were then identified and entered in the previous model including all independent variables (which were forced in the model) using the stepwise procedure. The criteria for an adjustment variable to stay in the final multivariable model was a significance level of 0.05. For each endpoint, an exploratory analysis was conducted by adding the self-compassion variable to the final multivariable model identified above. Adjusted odds ratio for logistic regressions and adjusted coefficients for linear regressions were calculated with 95% confidence intervals.
Scores for each questionnaire were calculated according to the formulas provided in the Supplementary Material. For incomplete questionnaires, it was still possible to calculate scores provided that no more than a pre-specified number of individual questions were unanswered. Otherwise, the scores were considered missing. No imputation was done for missing data. Before using multivariable regression models, the variables were closely examined for outliers, distribution issues or sparse data, and issues were fixed prior to running any statistical analysis. We also verified correlations between the pre-specified independent variables and looked at variance inflation factors to identify possible multicollinearity problems, but none were found. In addition, basics assumptions of the proposed analyses, such as linearity, were checked and all assumptions were met. All statistical tests were two sided and conducted at a 0.05 significance level. Analyses were performed with the use of SAS release 9.4 [SAS Institute Inc., Cary, NC, USA].
Results
Of the 564 participants, 467 (83%) respondents completed the 3-month survey. Two (0.4%) participants have withdrawn, one before and one after completing the 3-month survey.
Table 1 shows socio-demographic and occupational characteristics of the 467 participants, as well as COVID-19 personal and occupational demographics. The vast majority were Caucasian (93.5%) and were female sex (89.4%). More than half worked between 35 and 44 h per week, and almost all of them were still employed in the healthcare system as of June 2020. Regarding work types, nurses, physicians, and other health professionals (e.g., respiratory or occupational therapists, psychologists, social workers) accounted for three quarters of the sample; administrators, administrative agents, laboratory technicians, beneficiary attendants, and paramedics constituted the other quarter. Participants worked in diverse work environments including, in descending order, hospitals, local community service centers (in French: Centres locaux de services communautaires [CLSC]), clinics and CHSLD. About a quarter of participants worked in another environment such as rehabilitation centers or child and youth protection centers. Ninety-one percent of the respondents perceived they had access to psychological resources if needed. Concerning the PPE, 67% of the respondents always had access to it, with a majority feeling either “pretty” or “totally safe” using it. Twenty-two percent of respondents participated in COVID-related simulation-type practices, the last simulation round having occurred 1–2 months ago for 50% of these participants. Seventy percent of the respondents had been tested for SARS-CoV2 and <5% of them had received a positive status. Close to 40% of respondents were involved in direct COVID care and 33% were reassigned either to another practice area or establishment (51).
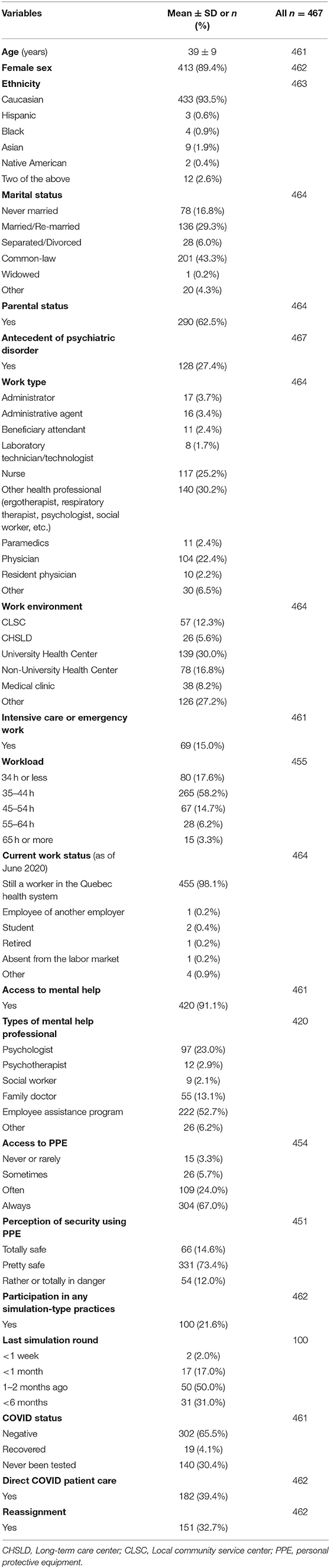
Table 1. Socio-demographic, occupational and COVID-19 specific characteristics of participants.
The scores for the psychological questionnaires included in the 3-month survey are presented in Table 2. Half of the respondents (51.8%) experienced at least weekly emotional exhaustion and/or depersonalization on the Maslach Burnout Inventory. In total, 158 different individuals (35.6%) displayed severe symptoms of at least one of the mental health disorders; 24.3% of respondents displayed severe symptoms of PTSD, 23.3% of anxiety, and 10.6% of depression. Mean scores of resilience, social support satisfaction, perceived organizational support, and self-compassion are also presented in Table 2.
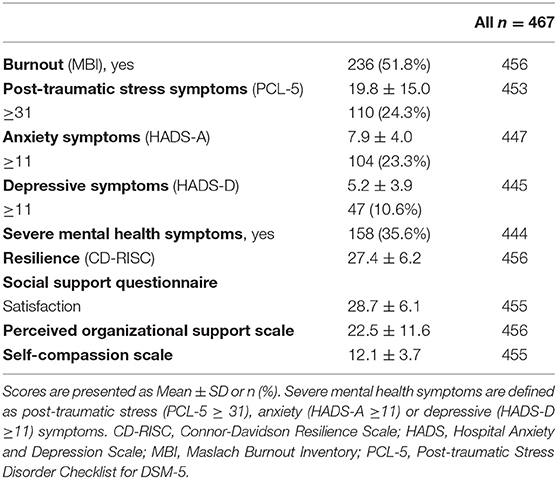
Table 2. Psychological questionnaire scores of participants.
Table 3 presents the results of the final multivariable logistic regression model for burnout status. Resilience (OR = 0.69, 95% CI: [0.55–0.87]; p = 0.002) and perceived organizational support (OR = 0.75, 95% CI: [0.61–0.93]; p = 0.009) were the only two variables significantly associated with burnout, in an inverse relationship. In other words, there is a 31% decrease in the odds of burnout for each SD (6) increase on the resilience scale; and there is a 25% decrease in the odds of burnout for each SD (12) increase on the perceived organizational support scale.
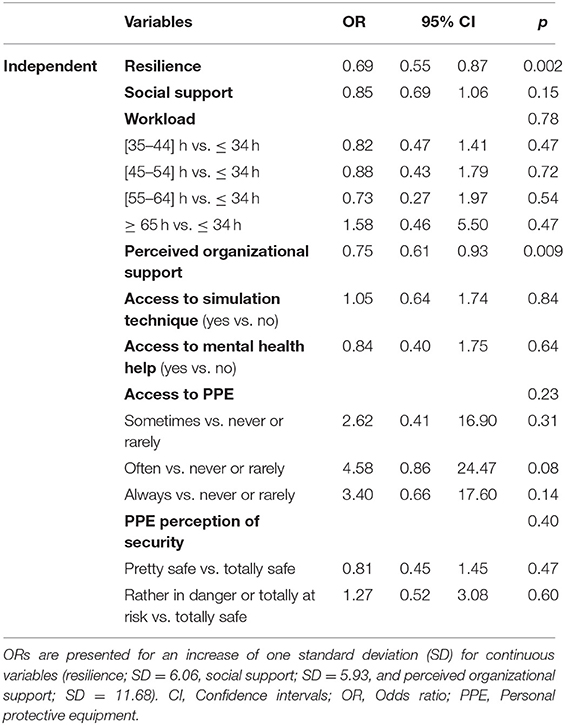
Table 3. Adjusted odds ratios, 95% confidence interval and p-values from multivariable logistic regression analysis for burnout among healthcare workers (n = 424).
Multivariable linear regression analyses were performed for PTSD, anxiety, and depression symptoms (Tables 4–6). Table 4 shows that resilience, social support satisfaction, perception of organizational support and perception of security using PPE were inversely associated with the severity of PTSD symptoms. In regard to employment types, administrative agents, administrators, other health professionals, laboratory technicians, beneficiary attendants and nurses displayed on average higher PTSD estimate scores compared to physicians. Presence of previous psychiatric conditions was positively associated with PTSD symptoms. The Table 5 shows that resilience, social support satisfaction and perceived organizational support were inversely associated with the severity of anxiety symptoms. Regarding work environments, CHSLD displayed on average significantly higher scores on the anxiety scale compared to university health centers. Non-university health center workers displayed on average significantly lower scores on the anxiety scale compared to university health centers. None of the other work environments were different in terms of anxiety compared to university health centers. Previous psychiatric conditions was significantly and positively associated with the severity of anxiety symptoms. Table 6 shows that resilience, social support, perceived organizational support, work type, reassignment, and psychiatric antecedents were significantly associated with depression symptoms' severity. Table 7 highlights significant findings across all efficacy endpoints.
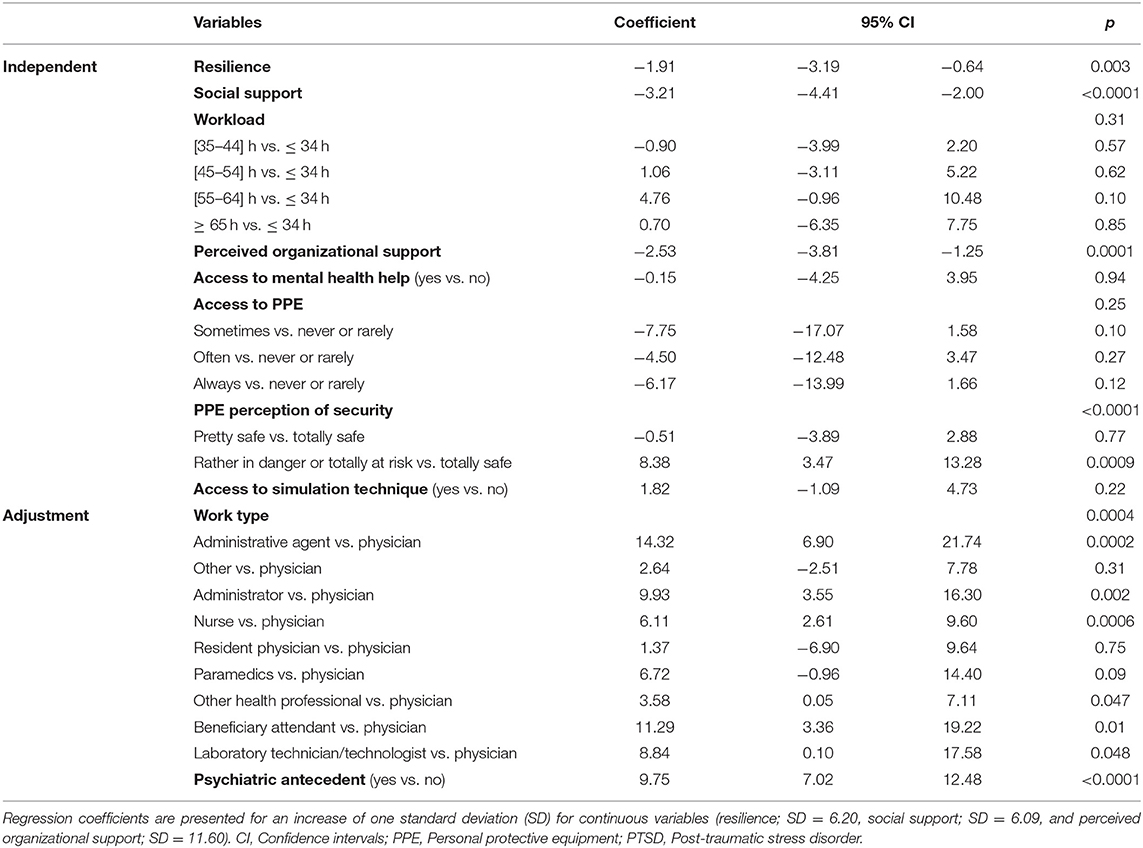
Table 4. Adjusted coefficient, 95% confidence interval and p-values from multivariable linear regression analysis for PTSD symptoms among healthcare workers (n = 426).
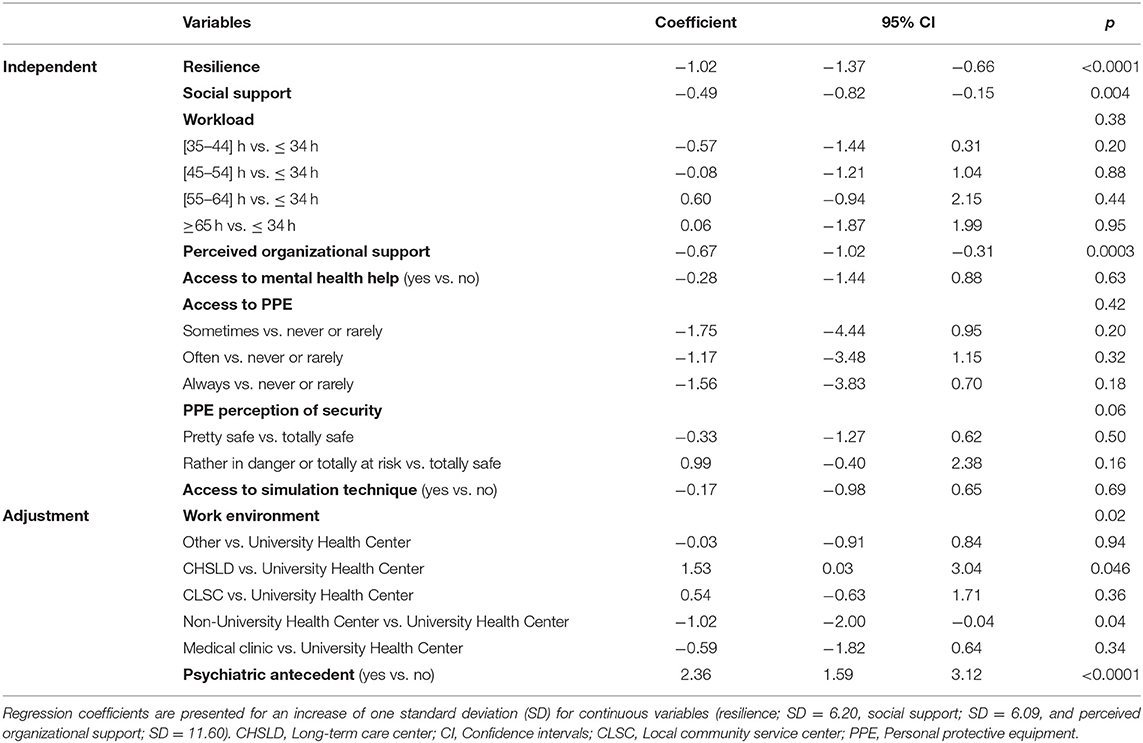
Table 5. Adjusted coefficient, 95% confidence interval and p-values from multivariable linear regression analysis for anxiety scores among healthcare workers (n = 421).
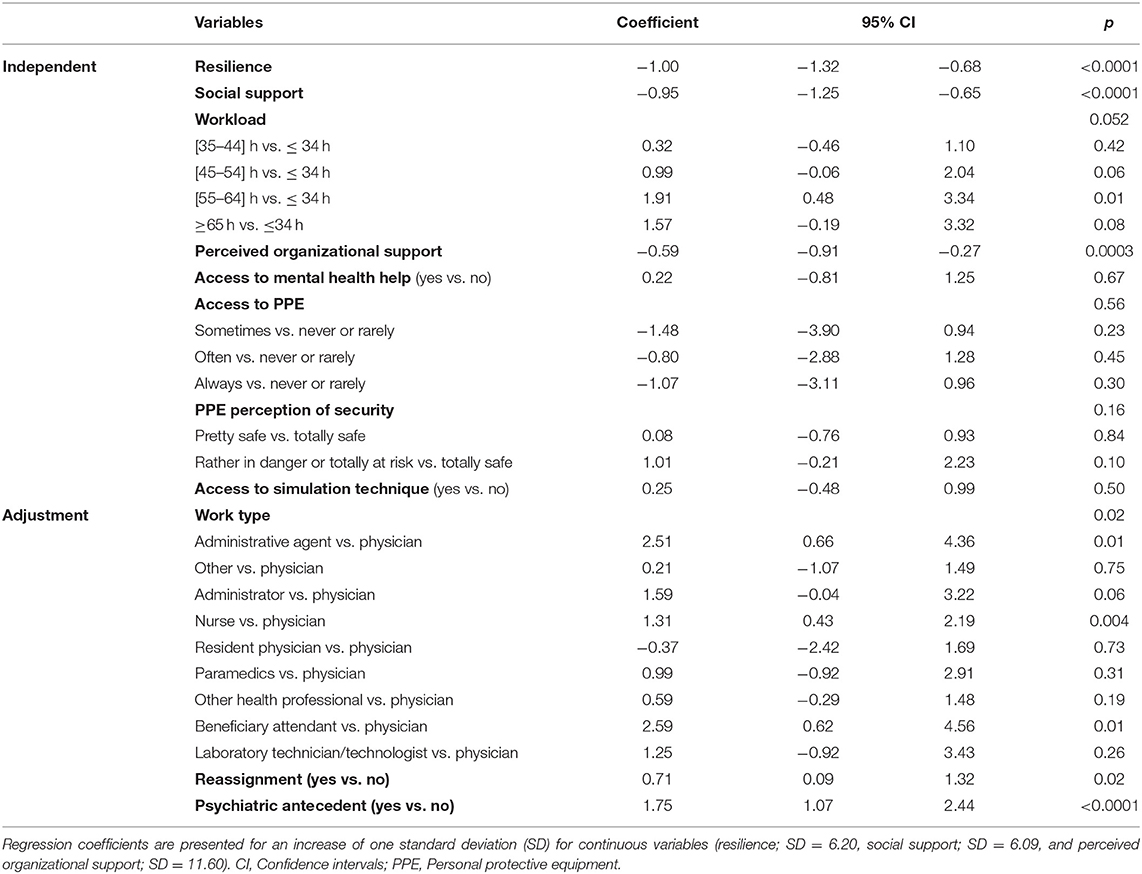
Table 6. Adjusted coefficient, 95% confidence interval and p-values from multivariable linear regression analysis for depression scores among participants (n = 419).
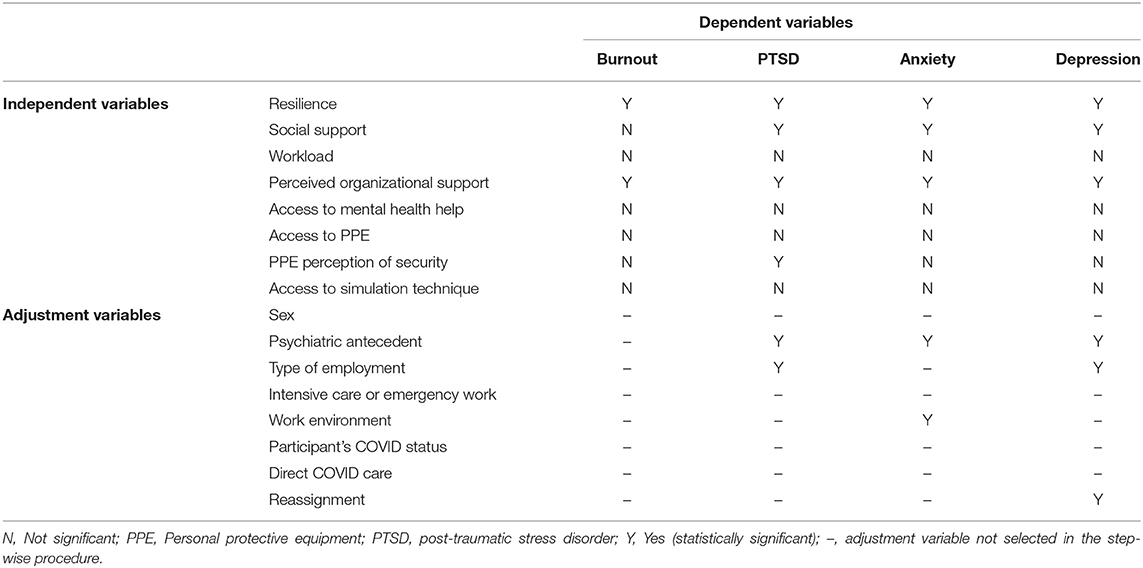
Table 7. Summary table of factors significantly associated with burnout, post-traumatic stress disorder, anxiety and depression.
For the exploratory analyses, only the PTSD and anxiety models are presented, as they are the two models that have retained the self-compassion variable (SD = 3.74) in their regression models (see Tables 8, 9). There was a significant and negative association between self-compassion and PTSD (Est: −1.56, 95% CI: [−3.03 to −0.08], p = 0.04) and anxiety symptoms (Est: −0.82, 95% CI: [−1.23 to −0.41], p < 0.0001).
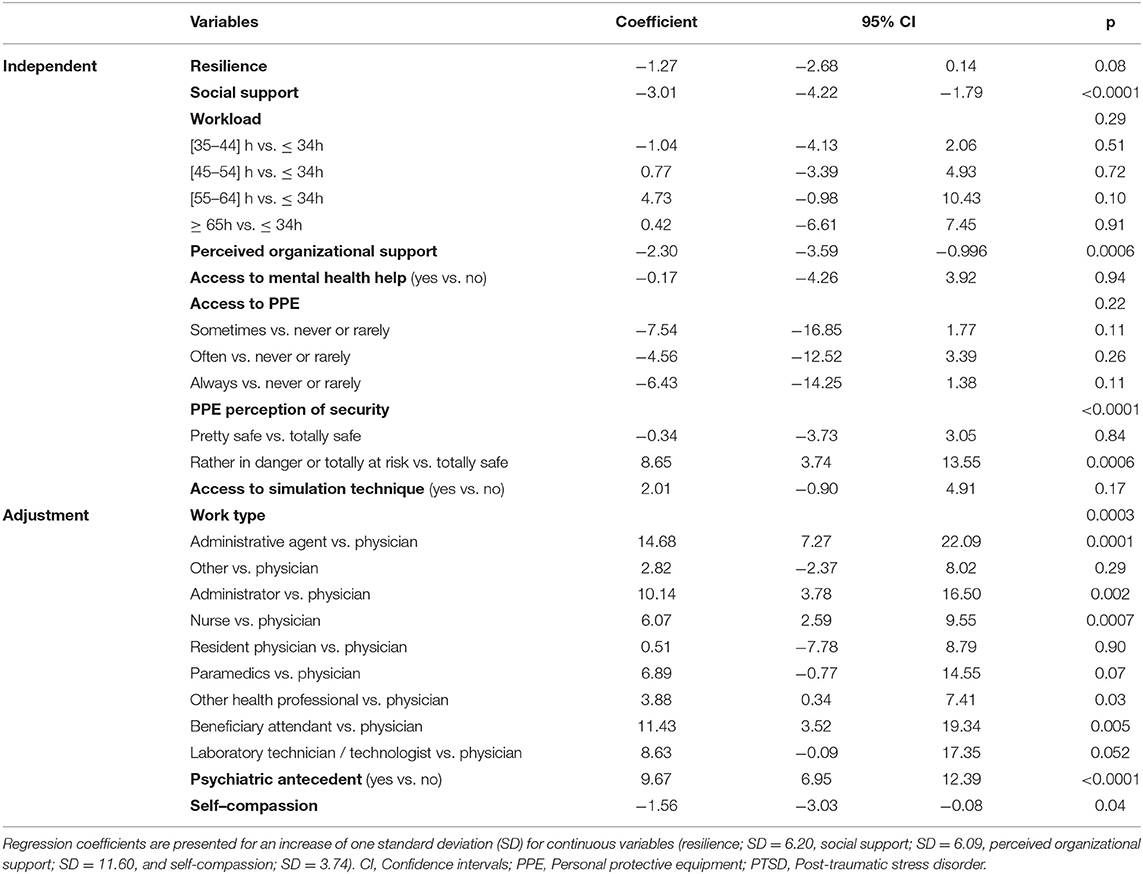
Table 8. Adjusted coefficient, 95% confidence interval and p-values from multivariable linear regression model with self-compassion variable for PTSD symptoms among healthcare workers (n = 425).
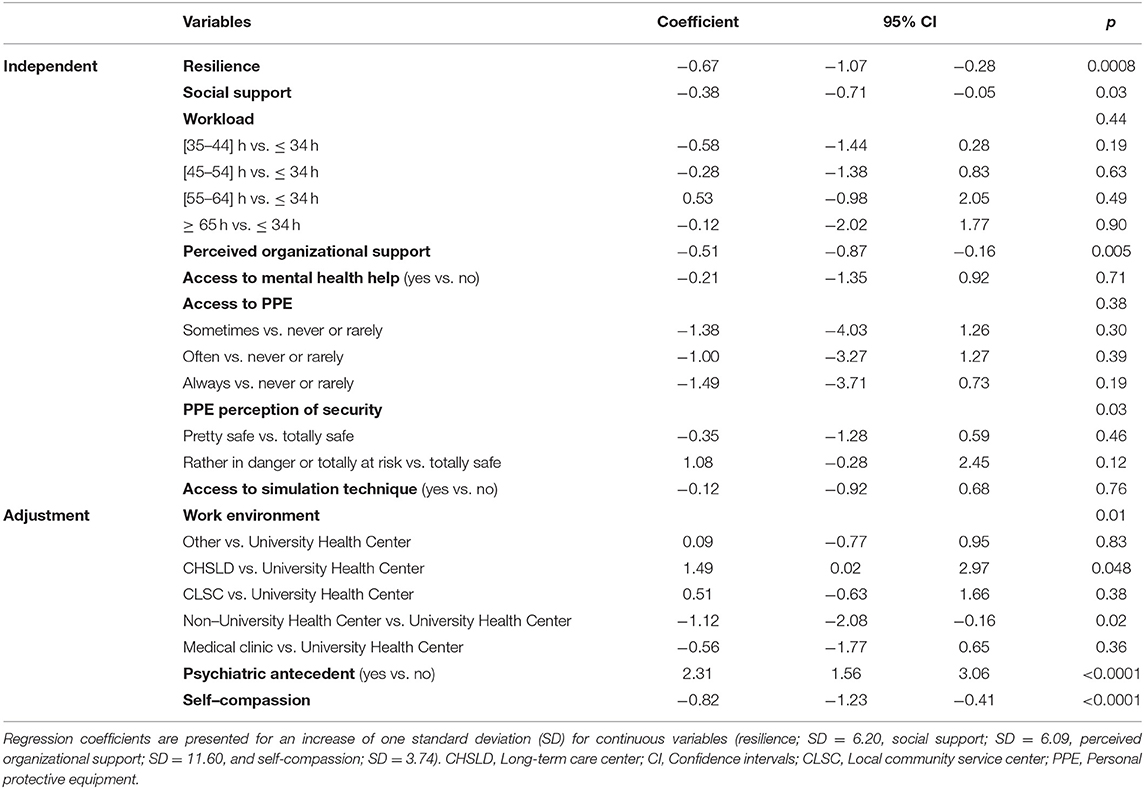
Table 9. Adjusted coefficient, 95% confidence interval and p-values from multivariable linear regression model with self-compassion variable for anxiety symptoms among healthcare workers (n = 420).
Discussion
Three months after the start of the COVID-19 pandemic, we surveyed the psychological health of 467 workers of Quebec's healthcare system. Among them, 52% met the cutoff score for burnout, much higher than pre-pandemic periods [which was estimated at ~30% (4, 5)].
Regarding psychopathologies, 24% of participants displayed clinically significant symptoms for PTSD, 23% for anxiety, and 11% for depression. These rates are consistent with those reported in the recent COVID-19 international literature on healthcare workers (7, 8), but are surprisingly similar to the rates reported before the pandemic (4). One hypothesis for this unanticipated result is the fact the thresholds to distinguish symptoms of psychopathology in self-administered questionnaires are widely heterogeneous, as are the questionnaires used (52). A final explanation is that the 3-month time point is possibly too early to detect an increase in anxio-depressive or PTSD symptoms (53). Such severe symptoms might develop months later, after initial coping mechanisms weaken.
As to factors associated with burnout and psychopathologies, in the context of COVID-related research, female sex (54), reported negative impact of work on household activities (21), urban living (55), a nursing position (56), higher exposure to COVID risks (21) and feeling pushed beyond training (21) are associated with adverse psychological outcomes. Conversely, high resilience, social support and availability of protective equipment are associated with lower levels of anxiety, burnout and insomnia (21, 56, 57). Additionally, past crises that generated important sources of strain for healthcare workers have shown the importance of verifying the impact of not only individual factors but also organizational ones on the development of burnout and psychopathologies (58–60). This proved to be the case in our study with higher resilience (individual factor) and perceived organizational support (organizational factor) being the only two variables significantly associated with better outcomes in both burnout and psychopathologies (PTSD, anxiety, depression), out of the eight independent variables verified. More particularly for burnout, they outweighed all six other independent variables as no other adjusted variables were needed to improve the model (social support, workload, access to mental help, PPE, or simulation technique, and perception of security using PPE). For PTSD, anxiety and depression symptoms, social support added to resilience and perceived organizational support in the final model as significant variables associated with symptom severity. This is consistent with results from recent COVID-19 literature; there is an inverse correlation between social support and anxio-depressive and PTSD symptoms. Surprisingly or not, social support was not significantly associated with burnout. During a notably stressful period at work, it is possible that burnout would be more strongly associated with organizational rather than social support, especially in a time of confinement.
Perception of low security while using PPE— and not lack of access per se —was associated with higher PTSD, but not with burnout or depression. Not feeling safe in the face of COVID-19 can lead to fear of becoming infected, potentially dying or infecting a patient or a loved one. As being exposed to threatened death is a cardinal criterion of PTSD, this can explain why these associations are specific to this fear-related conditions and do not hold for burnout, depression and anxiety symptoms (42). Depression was the only mental health outcome that was associated with reassignment. The loss of reference and network, having to learn a new working method, the resulting fatigue and feeling isolated can have contributed to this association.
In the final regression models, psychiatric antecedents were significantly associated with PTSD, anxiety and depression, but not burnout. For the latter, its effect was not strong enough as soon as it was combined with resilience and perceived organizational support. This reinforces the idea that burnout is not a mental disease. It also explicitizes that resilience and perceived organizational support can be protective in individual with and without psychiatric antecedents. An unexpected finding was that administrative agents and administrators had on average greater PTSD symptoms than physicians. Positions providing direct care to COVID-19 patients were not associated with PTSD symptoms. Administrators may have been confronted with multiple decisions that had an impact on the entire structure of care. Second, PCL-5 instructions refer to “response to a very stressful experience”; indeed, symptoms may appear without witnessing actual death. This falls under the aegis of vicarious trauma, which is continuous exposure to others recounting their trauma, reviewing case files or responding to the repercussions of trauma (61). Moreover, a person could have PTSD symptoms that coincide with the survey or have witnessed one of their peers suffer from COVID-19.
Our results are comparable to some similar studies in the literature published since the beginning of the pandemic (11, 57, 62–70). Indeed, among the studies with a similar design as ours, e.g., a cross-sectional study with the aim of verifying factors associated with per-pandemic psychological distress (burnout, psychopathologies) in healthcare workers, the rates of distress and the factors reported are similar to what we present here. Notably, several studies have shown high rates of burnout (64, 66, 67, 69, 70), which are comparable to the 51.8% reported here. However, the factors associated with the development of burnout sometimes differ from the ones we found, with reports of workload, type of employment and participation in training programs, all of which were not found to be significant in our study. However, in this nurse population study, moderate to high levels of burnout were reported and a negative correlation with resilience was found (r = 0.25, p < 0.05, and r = 0.31, p < 0.01 for emotional exhaustion and personal inefficacy, respectively) (67). In another study, in primary care physicians, the rate of depression (~14%) was close to the one found here, although factors identified differed as well, with high workload and a single relationship being significant risk factors for depression. However, it has to be mentioned that some other studies showed different results from ours. In particular, two studies (64, 65) showed significantly higher rates of depression and anxiety with prevalence exceeding 45% for depression and 55% for anxiety, a result all the more surprising considering that the scale used was the same as ours (HADS). It should be noted though that the population of these two studies were in a country experiencing civil war (Libya), and the addition of a major stressor such as the COVID-19 pandemic may explain these high rates of psychopathology.
Because self-compassion is a less recognized and studied variable in healthcare compared to resilience, we studied it as part of an exploratory analysis. Our results show that it has a protective effect on anxiety and PTSD, which is consistent with the general population literature (71, 72). Self-compassion refers to the understanding toward one's own feelings and reactions, along with having a well-balanced view when facing difficult situations (73). With the rapidly changing directives regarding daily work during COVID-19 pandemic, difficult emotions and feelings of inadequacy were normative experiences. Self-compassionate participants may have been protected against anxiety and PTSD, with less guilt and self-pressure.
Concerning the limits of our survey study, we cannot establish causal effects, given that we measured our outcome and factors at the same time, making the temporal relationship impossible to assess (74). Also, we may be prone to volunteer bias, as more distressed workers may have been more likely to participate in order to relate their experience; whereas others may not have enough energy to participate. We must take into account another limit in the selection of our participants, as our study was Web-based (75). In fact, this implies that only respondents who were aware of the existence of the survey were able to register, which may lead to under-representation of some specific groups of the population studied. Furthermore, we are aware that other experiences (financial, personal) could have been associated with burnout rate, but chose to focus solely on work experiences. We did so to gather modifiable factors for most hospitals' human resources and because burnout in healthcare workers is mainly driven by organizational and psychological factors with little to no contribution from demographic factors (21, 29, 54–57). Finally, the small sample size of certain groups, such as administrative agents, can limit the external validity. However, the response rate was similar between types of employment and ranged from 70 to 100%, averaging 83 ± 8%. Finally, even if the proportion of women seems high, it is representative of the overall local healthcare workers with 82% being women (76).
Our study differs from previous ones by covering a wide range of variables often treated separately. Notably, this study addresses both organizational and individual psychological health outcomes and considers a combination of factors arising from individual, social and organizational psychology. In addition, our study includes medical workers, but also non-medical health workers facing this pandemic. Our results reinforce the relevance of targeting individuals (77–79) and organizational factors to promote mental health workers facing high-stress situations. Resiliency can be worked on and improved, as it has been previously demonstrated in a meta-analysis on resilience-focused interventions (80). It is important to acknowledge that although one's resilience can be strengthened and worked on, it wouldn't translate into unacceptable environmental conditions being tolerated as a result. For its part, perceived organizational support has been widely researched in the last three decades (32). It encompasses the organization's treatment of its members, employee-organization relationship quality, human resource practices, and job conditions (32). It favors organizational commitment and task performance, general positive affect in the workplace, decreased withdrawal behaviors, turnover intentions, and perception of strain (81). One first step to target this variable in practice would be to analyze whether the source of perceived support is obtained from colleagues, supervisors or, more frequently, from the organization as a whole (82); and then use this channel to promote further interventions. The impact of individual, organizational or both types of intervention would need to be measured prospectively with well-defined targeted health outcomes and populations. Indeed, the present study clearly shows that work environment, employment type, or reassignment are associated with specific mental health symptoms. If future research or clinical initiatives aim toward screening and referring for mental disorders in healthcare workers facing a pandemic, our data suggests that depressive symptoms should specifically be screened for in reassigned workers, whereas PTSD should primarily be screened for in administrative agents, administrators, nurses, other health professionals such as respiratory therapists, beneficiary attendants and laboratory technicians. Ultimately, this research can serve both clinical and research initiatives to support the global psychological health of healthcare workers that are coping with high stress situations. Undeniably, the healthcare system is going through a major crisis with this pandemic being the most important one but probably not the last. Thus, it is likely that the identified factors may have an impact on other healthcare system crises.
Data Availability Statement
In accordance with the ethical consent provided by participants, the data underlying this article cannot be shared publicly to preserve their privacy.
Ethics Statement
The studies involving human participants were reviewed and approved by Research Ethics and New Technology Development Committee (CÉRDNT), Montreal Heart Institute, Montréal, Canada. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
JB, M-FM, J-CT and SG: conceptualization. SC, M-JM, CR, and JB: data curation. CR and M-CG: formal analysis. JB: investigation, project administration, resources, and supervision. SC, M-CG, and JB: methodology. CR and JB: validation. SC, M-JM, and JB: visualization. CR, M-CG, CG, and JB: roles/writing—original draft. All authors recruitment, funding acquisition, and writing—review and editing.
Funding
This study was carried out with financial assistance from the Gouvernement du Québec (Grant Number: 2020-2021-COVID-19-PSOv2a-51231) and the Montreal Heart Institute Foundation.
Conflict of Interest
J-CT reported grants from Amarin, grants and personal fees from Astra Zeneca, grants, personal fees, and other from Dalcor, grants from Esperion, grants from Ionis, grants from Pfizer, grants and personal fees from Sanofi, grants and personal fees from Servier, personal fees from HLS Therapeutics, outside the submitted work; In addition, J-CT had a patent Genetic markers for predicting responsiveness to therapy with hdl-raising or hdl mimicking agent pending, and a patent Methods for using low dose colchicine after myocardial infarction with royalties paid to Invention assigned to the Montreal Heart Institute.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We would like to thank M. Mezhoudi, T. Ahmed, and C. Jabre for the development of the Web platform, M-C. Strevez for her involvement as a mental health support worker, L. Blondeau for statistical expertise, M. Vadeboncoeur and L. Abdelaziz for manuscript revision.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2021.668278/full#supplementary-material
References
1. Nguyen LH, Drew DA, Graham MS, Joshi AD, Guo CG, Ma W, et al. Risk of COVID-19 among front-line health-care workers and the general community: a prospective cohort study. Lancet Public Health. (2020) 5:e475–83. doi: 10.1016/S2468-2667(20)30164-X
2. Papoutsi E, Giannakoulis VG, Ntella V, Pappa S, Katsaounou P. Global burden of COVID-19 pandemic on healthcare workers. ERJ Open Res. (2020) 6:00195-2020. doi: 10.1183/23120541.00195-2020
3. Jantzen R, Noisel N, Camilleri-Broet S, Labbe C, Malliard T, Payette Y, et al. Epidemiological characteristics of the COVID-19 spring outbreak in Quebec, Canada: a population-based study. BMC Infect Dis. (2021) 21:435. doi: 10.1186/s12879-021-06002-0
4. Canadian Medical Association. CMA National Physician Health Survey A National Snapshot: Canadian Medical Association. (2018). Available online at: https://www.cma.ca/sites/default/files/2018-11/nph-survey-e.pdf (accessed June 11, 2021).
5. Poncet MC, Toullic P, Papazian L, Kentish-Barnes N, Timsit JF, Pochard F, et al. Burnout syndrome in critical care nursing staff. Am J Respir Crit Care Med. (2007) 175:698–704. doi: 10.1164/rccm.200606-806OC
6. World Health Organization. International Classification of Diseases for Mortality and Morbidity Statistics. 11th Revision Edn. WHO (2018).
7. Sanghera J, Pattani N, Hashmi Y, Varley KF, Cheruvu MS, Bradley A, et al. The impact of SARS-CoV-2 on the mental health of healthcare workers in a hospital setting-a systematic review. J Occup Health. (2020) 62:e12175. doi: 10.1002/1348-9585.12175
8. Sheraton M, Deo N, Dutt T, Surani S, Hall-Flavin D, Kashyap R. Psychological effects of the COVID 19 pandemic on healthcare workers globally: a systematic review. Psychiatry Res. (2020) 292:113360. doi: 10.1016/j.psychres.2020.113360
9. Azoulay E, De Waele J, Ferrer R, Staudinger T, Borkowska M, Povoa P, et al. Symptoms of burnout in intensive care unit specialists facing the COVID-19 outbreak. Ann Intensive Care. (2020) 10:110. doi: 10.1186/s13613-020-00722-3
10. Barello S, Palamenghi L, Graffigna G. Burnout and somatic symptoms among frontline healthcare professionals at the peak of the Italian COVID-19 pandemic. Psychiatry Res. (2020) 290:113129. doi: 10.1016/j.psychres.2020.113129
11. Buselli R, Corsi M, Baldanzi S, Chiumiento M, Del Lupo E, Dell'Oste V, et al. Professional quality of life and mental health outcomes among health care workers exposed to Sars-Cov-2 (Covid-19). Int J Environ Res Public Health. (2020) 17:26. doi: 10.3390/ijerph17176180
12. Chor WPD, Ng WM, Cheng L, Situ W, Chong JW, Ng LYA, et al. (2020). Burnout amongst emergency healthcare workers during the COVID-19 pandemic: a multi-center study. Am J Emerg Med. doi: 10.1016/j.ajem.2020.10.040. [Epub Ahead of Print].
13. Civantos AM, Byrnes Y, Chang C, Prasad A, Chorath K, Poonia SK, et al. Mental health among otolaryngology resident and attending physicians during the COVID-19 pandemic: national study. Head Neck. (2020) 42:1597–609. doi: 10.1002/hed.26292
14. Dobson H, Malpas CB, Burrell AJ, Gurvich C, Chen L, Kulkarni J, et al. Burnout and psychological distress amongst Australian healthcare workers during the COVID-19 pandemic. Aust Psychiatry. (2021) 29:26–30. doi: 10.1177/1039856220965045
15. El Haj M, Allain P, Annweiler C, Boutoleau-Bretonniere C, Chapelet G, Gallouj K, et al. Burnout of healthcare workers in acute care geriatric facilities during the COVID-19 crisis: an online-based study. J Alzheimers Dis. (2020) 78:847–52. doi: 10.3233/JAD-201029
16. Jha SS, Shah S, Calderon MD, Soin A, Manchikanti L. The effect of COVID-19 on interventional pain management practices: a physician burnout survey. Pain Physician. (2020) 23:S271–82. doi: 10.36076/ppj.2020/23/S271
17. Kannampallil TG, Goss CW, Evanoff BA, Strickland JR, McAlister RP, Duncan J. Exposure to COVID-19 patients increases physician trainee stress and burnout. PLoS ONE. (2020) 15:e0237301. doi: 10.1371/journal.pone.0237301
18. Khasne RW, Dhakulkar BS, Mahajan HC, Kulkarni AP. Burnout among healthcare workers during COVID-19 pandemic in India: results of a questionnaire-based survey. Indian J Crit Care Med. (2020) 24:664–71. doi: 10.5005/jp-journals-10071-23518
19. Luceno-Moreno L, Talavera-Velasco B, Garcia-Albuerne Y, Martin-Garcia J. Symptoms of posttraumatic stress, anxiety, depression, levels of resilience and burnout in Spanish health personnel during the COVID-19 pandemic. Int J Environ Res Public Health. (2020) 17:30. doi: 10.3390/ijerph17155514
20. Matsuo T, Kobayashi D, Taki F, Sakamoto F, Uehara Y, Mori N, et al. Prevalence of health care worker burnout during the coronavirus disease 2019 (COVID-19) pandemic in Japan. JAMA Netw. (2020) 3:e2017271. doi: 10.1001/jamanetworkopen.2020.17271
21. Morgantini LA, Naha U, Wang H, Francavilla S, Acar O, Flores JM, et al. Factors contributing to healthcare professional burnout during the COVID-19 pandemic: a rapid turnaround global survey. PLoS ONE. (2020) 15:e0238217. doi: 10.1371/journal.pone.0238217
22. Pérez-Fuentes MDC, Molero-Jurado MDM, Gázquez-Linares JJ, Simón-Márquez MDM. Analysis of burnout predictors in nursing: risk and protective psychological factors. Eur J Psychol Appl Legal Context. (2018) 11:33–40. doi: 10.5093/ejpalc2018a13
23. Ruiz-Fernandez MD, Ramos-Pichardo JD, Ibanez-Masero O, Cabrera-Troya J, Carmona-Rega MI, Ortega-Galan AM. Compassion fatigue, burnout, compassion satisfaction and perceived stress in healthcare professionals during the COVID-19 health crisis in Spain. J Clin Nurs. (2020) 29:4321–30. doi: 10.1111/jocn.15469
24. Sarboozi Hoseinabadi T, Kakhki S, Teimori G, Nayyeri S. Burnout and its influencing factors between frontline nurses and nurses from other wards during the outbreak of coronavirus disease -COVID-19- in Iran. Investigacion Educ Enferm. (2020) 38:e3. doi: 10.17533/udea.iee.v38n2e03
25. Tan BYQ, Kanneganti A, Lim LJH, Tan M, Chua YX, Tan L, et al. Burnout and associated factors among health care workers in Singapore during the COVID-19 pandemic. J Am Med Dir Assoc. (2020) 21:1751–8.e5. doi: 10.1016/j.jamda.2020.09.035
26. Batra K, Singh TP, Sharma M, Batra R, Schvaneveldt N. Investigating the psychological impact of COVID-19 among healthcare workers: a meta-analysis. Int J Environ Res Public Health. (2020) 17:9096. doi: 10.3390/ijerph17239096
27. Dall'Ora C, Ball J, Reinius M, Griffiths P. Burnout in nursing: a theoretical review. Hum Resour Health. (2020) 18:41. doi: 10.1186/s12960-020-00469-9
28. Embriaco N, Azoulay E, Barrau K, Kentish N, Pochard F, Loundou A, et al. High level of burnout in intensivists: prevalence and associated factors. Am J Respir Crit Care Med. (2007) 175:686–92. doi: 10.1164/rccm.200608-1184OC
29. Bria M, Baban A, Dumitraşcu DL. Systematic review of burnout risk factors among European healthcare professionals. Cogn Brain Behav Interdiscipl J. (2012) XVI:423–52. Available online at: https://www.cbbjournal.ro/index.php/en/2012/73-16-3/504-systematic-review-of-burnout-risk-factors-among-european-healthcare-professionals-
30. Woodhead EL, Northrop L, Edelstein B. Stress, social support, and burnout among long-term care nursing staff. J Appl Gerontol. (2016) 35:84–105. doi: 10.1177/0733464814542465
31. De Hert S. Burnout in healthcare workers: prevalence, impact and preventative strategies. Local Reg Anesth. (2020) 13:171–83. doi: 10.2147/LRA.S240564
32. Kurtessis JN, Eisenberger R, Ford MT, Buffardi LC, Stewart KA, Adis CS. Perceived organizational support: a meta-analytic evaluation of organizational support theory. J Manag. (2015) 43:1854–84. doi: 10.1177/0149206315575554
33. Campbell-Sills L, Stein MB. Psychometric analysis and refinement of the connor-davidson resilience scale (CD-RISC): validation of a 10-item measure of resilience. J Trauma Stress. (2007) 20:1019–28. doi: 10.1002/jts.20271
34. Choudhury T, Debski M, Wiper A, Abdelrahman A, Wild S, Chalil S, et al. COVID-19 pandemic: looking after the mental health of our healthcare workers. J Occup Environ Med. (2020) 62:e373–e6. doi: 10.1097/JOM.0000000000001907
36. Naderifar M, Goli H, Ghaljaie F. (2017). Snowball sampling: a purposeful method of sampling in qualitative research. Strides Dev Med Educ. 14. doi: 10.5812/sdme.67670
37. West CP, Dyrbye LN, Sloan JA, Shanafelt TD. Single item measures of emotional exhaustion and depersonalization are useful for assessing burnout in medical professionals. J Gen Intern Med. (2009) 24:1318–21. doi: 10.1007/s11606-009-1129-z
38. Dyrbye LN, West CP, Satele D, Boone S, Tan L, Sloan J, et al. Burnout among U.S. medical students, residents, and early career physicians relative to the general U.S. population. Acad Med. (2014) 89:443–51. doi: 10.1097/ACM.0000000000000134
39. Loera B, Converso D, Viotti S. Evaluating the psychometric properties of the maslach burnout inventory-human services survey (MBI-HSS) among Italian nurses: how many factors must a researcher consider? PLoS ONE. (2014) 9:e114987. doi: 10.1371/journal.pone.0114987
40. Ashbaugh AR, Houle-Johnson S, Herbert C, El-Hage W, Brunet A. Psychometric validation of the English and French versions of the posttraumatic stress disorder checklist for DSM-5 (PCL-5). PLoS ONE. (2016) 11:e0161645. doi: 10.1371/journal.pone.0161645
41. Blevins CA, Weathers FW, Davis MT, Witte TK, Domino JL. The posttraumatic stress disorder checklist for DSM-5 (PCL-5): development and initial psychometric evaluation. J Trauma Stress. (2015) 28:489–98. doi: 10.1002/jts.22059
42. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5. Washington, DC: American Psychiatric Publishing (2013). doi: 10.1176/appi.books.9780890425596
43. Bjelland I, Dahl AA, Haug TT, Neckelmann D. The validity of the hospital anxiety and depression scale. An updated literature review. J Psychosom Res. (2002) 52:69–77. doi: 10.1016/S0022-3999(01)00296-3
44. Roberge P, Dore I, Menear M, Chartrand E, Ciampi A, Duhoux A, et al. A psychometric evaluation of the French Canadian version of the hospital anxiety and depression scale in a large primary care population. J Affect Disord. (2013) 147:171–9. doi: 10.1016/j.jad.2012.10.029
45. Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. (1983) 67:361–70. doi: 10.1111/j.1600-0447.1983.tb09716.x
46. Wortmann JH, Jordan AH, Weathers FW, Resick PA, Dondanville KA, Hall-Clark B, et al. Psychometric analysis of the PTSD checklist-5 (PCL-5) among treatment-seeking military service members. Psychol Assess. (2016) 28:1392–403. doi: 10.1037/pas0000260
47. Bovin MJ, Marx BP, Weathers FW, Gallagher MW, Rodriguez P, Schnurr PP, et al. Psychometric properties of the PTSD checklist for diagnostic and statistical manual of mental disorders-Fifth edition (PCL-5) in veterans. Psychol Assess. (2016) 28:1379–91. doi: 10.1037/pas0000254
48. Leary MR, Tate EB, Adams CE, Allen AB, Hancock J. Self-compassion and reactions to unpleasant self-relevant events: the implications of treating oneself kindly. J Pers Soc Psychol. (2007) 92:887–904. doi: 10.1037/0022-3514.92.5.887
49. Sarason IG, Sarason BR, Shearin EN, Pierce GR. A brief measure of social support: practical and theoretical implications. J Soc Pers Relat. (2016) 4:497–510. doi: 10.1177/0265407587044007
50. Worley JA, Fuqua DR, Hellman CM. The survey of perceived organisational support: which measure should we use? SA J Ind Psychol. (2009) 35:a754. doi: 10.4102/sajip.v35i1.754
51. Canada PHAo. COVID-19 pandemic guidance for the health care sector: Canada.ca. 2020. (2020). Available online at: https://www.canada.ca/en/public-health/services/diseases/2019-novel-coronavirus-infection/health-professionals/covid-19-pandemic-guidance-health-care-sector.html (accessed June 11, 2021).
52. Beidas RS, Stewart RE, Walsh L, Lucas S, Downey MM, Jackson K, et al. Free, brief, and validated: standardized instruments for low-resource mental health settings. Cogn Behav Pract. (2015) 22:5–19. doi: 10.1016/j.cbpra.2014.02.002
53. Maunder RG, Lancee WJ, Balderson KE, Bennett JP, Borgundvaag B, Evans S, et al. Long-term psychological and occupational effects of providing hospital healthcare during SARS outbreak. Emerg Infect Dis. (2006) 12:1924–32. doi: 10.3201/eid1212.060584
54. Civantos AM, Bertelli A, Goncalves A, Getzen E, Chang C, Long Q, et al. Mental health among head and neck surgeons in Brazil during the COVID-19 pandemic: a national study. Am J Otolaryngol. (2020) 41:102694. doi: 10.1016/j.amjoto.2020.102694
55. Zhang WR, Wang K, Yin L, Zhao WF, Xue Q, Peng M, et al. Mental health and psychosocial problems of medical health workers during the COVID-19 epidemic in China. Psychother Psychosom. (2020) 89:242–50. doi: 10.1159/000507639
56. Huang L, Wang Y, Liu J, Ye P, Chen X, Xu H, et al. Factors influencing anxiety of health care workers in the radiology department with high exposure risk to COVID-19. Med Sci Monit. (2020) 26:e926008. doi: 10.12659/MSM.926008
57. Xiao X, Zhu X, Fu S, Hu Y, Li X, Xiao J. Psychological impact of healthcare workers in China during COVID-19 pneumonia epidemic: a multi-center cross-sectional survey investigation. J Affect Disord. (2020) 274:405–10. doi: 10.1016/j.jad.2020.05.081
58. Carta MG, Preti A, Portoghese I, Pisanu E, Moro D, Pintus M, et al. Risk for depression, burnout and low quality of life among personnel of a university hospital in Italy is a consequence of the impact one economic crisis in the welfare system? Clin Pract Epidemiol Ment Health. (2017) 13:156–67. doi: 10.2174/1745017901713010156
59. Lee RS, Son Hing LS, Gnanakumaran V, Weiss SK, Lero DS, Hausdorf PA, et al. Inspired but tired: how medical faculty's job demands and resources lead to engagement, work-Life conflict, and burnout. Front Psychol. (2021) 12:609639. doi: 10.3389/fpsyg.2021.609639
60. Sancassiani F, Campagna M, Tuligi F, Machado S, Cantone E, Carta MG. Organizational wellbeing among workers in mental health services: a pilot study. Clin Pract Epidemiol Ment Health. (2015) 11:4–11. doi: 10.2174/1745017901511010004
61. Benfante A, Di Tella M, Romeo A, Castelli L. Traumatic stress in healthcare workers during COVID-19 pandemic: a review of the immediate impact. Front Psychol. (2020) 11:569935. doi: 10.3389/fpsyg.2020.569935
62. Agyapong VIO, Hrabok M, Vuong W, Shalaby R, Noble JM, Gusnowski A, et al. Changes in stress, anxiety, and depression levels of subscribers to a daily supportive text message program (Text4Hope) during the COVID-19 pandemic: cross-sectional survey study. JMIR Ment Health. (2020) 7:e22423. doi: 10.2196/22423
63. Das A, Sil A, Jaiswal S, Rajeev R, Thole A, Jafferany M, et al. A study to evaluate depression and perceived stress among frontline Indian doctors combating the COVID-19 pandemic. Prim Care Companion CNS Disord. (2020) 22:20m02716. doi: 10.4088/PCC.20m02716
64. Elhadi M, Msherghi A, Elgzairi M, Alhashimi A, Bouhuwaish A, Biala M, et al. The mental well-being of frontline physicians working in civil wars under coronavirus disease 2019 pandemic conditions. Front Psychiatry. (2020) 11:598720. doi: 10.3389/fpsyt.2020.598720
65. Elhadi M, Msherghi A, Elgzairi M, Alhashimi A, Bouhuwaish A, Biala M, et al. Psychological status of healthcare workers during the civil war and COVID-19 pandemic: a cross-sectional study. J Psychosom Res. (2020) 137:110221. doi: 10.1016/j.jpsychores.2020.110221
66. Elhadi M, Msherghi A, Elgzairi M, Alhashimi A, Bouhuwaish A, Biala M, et al. Burnout syndrome among hospital healthcare workers during the COVID-19 pandemic and civil war: a cross-sectional study. Front Psychiatry. (2020) 11:579563. doi: 10.3389/fpsyt.2020.579563
67. Jose S, Dhandapani M, Cyriac MC. Burnout and resilience among frontline nurses during COVID-19 pandemic: a cross-sectional study in the emergency department of a tertiary care center, North India. Indian J Crit Care Med. (2020) 24:1081–8. doi: 10.5005/jp-journals-10071-23667
68. Mrklas K, Shalaby R, Hrabok M, Gusnowski A, Vuong W, Surood S, et al. Prevalence of perceived stress, anxiety, depression, and obsessive-compulsive symptoms in health care workers and other workers in Alberta during the COVID-19 pandemic: cross-sectional survey. JMIR Ment Health. (2020) 7:e22408. doi: 10.2196/22408
69. Pniak B, Leszczak J, Adamczyk M, Rusek W, Matlosz P, Guzik A. Occupational burnout among active physiotherapists working in clinical hospitals during the COVID-19 pandemic in south-eastern Poland. Work. (2021) 68:285–95. doi: 10.3233/WOR-203375
70. Trumello C, Bramanti SM, Ballarotto G, Candelori C, Cerniglia L, Cimino S, et al. Psychological adjustment of healthcare workers in italy during the COVID-19 pandemic: differences in stress, anxiety, depression, burnout, secondary trauma, and compassion satisfaction between frontline and non-Frontline professionals. Int J Environ Res Public Health. (2020) 17:8358. doi: 10.3390/ijerph17228358
71. Conversano C, Ciacchini R, Orru G, Di Giuseppe M, Gemignani A, Poli A. Mindfulness, compassion, and self-compassion among health care professionals: what's new? A systematic review. Front Psychol. (2020) 11:1683. doi: 10.3389/fpsyg.2020.01683
72. Hashem Z, Zeinoun P. Self-Compassion explains less burnout among healthcare professionals. Mindfulness (N Y). (2020) 1–10. doi: 10.1007/s12671-020-01469-5
73. Neff K. Self-compassion: an alternative conceptualization of a healthy attitude toward oneself. Self Identity. (2003) 2:85–101. doi: 10.1080/15298860309032
74. Wang X, Cheng Z. Cross-sectional studies: strengths, weaknesses, and recommendations. Chest. (2020) 158(1S):S65–71. doi: 10.1016/j.chest.2020.03.012
75. Bethlehem J. Selection bias in web surveys. Int Stat Rev. (2010) 78:161–88. doi: 10.1111/j.1751-5823.2010.00112.x
76. Ministère de la Santé et des Services sociaux. Emplois Selon la Catégorie Professionnelle - Statistiques de Santé et de Bien être Selon le Sexe - Tout le Québec - Professionnels de la Santé. Gouv.qc.ca. (2011).
77. Hofmeyer A, Taylor R, Kennedy K. Knowledge for nurses to better care for themselves so they can better care for others during the covid-19 pandemic and beyond. Nurse Educ Today. (2020) 94:104503. doi: 10.1016/j.nedt.2020.104503
78. Raab K. Mindfulness, self-compassion, and empathy among health care professionals: a review of the literature. J Health Care Chaplain. (2014) 20:95–108. doi: 10.1080/08854726.2014.913876
79. Carmassi C, Foghi C, Dell'Oste V, Cordone A, Bertelloni CA, Bui E, et al. PTSD symptoms in healthcare workers facing the three coronavirus outbreaks: what can we expect after the COVID-19 pandemic. Psychiatry Res. (2020) 292:113312. doi: 10.1016/j.psychres.2020.113312
80. Liu JJW, Ein N, Gervasio J, Battaion M, Reed M, Vickers K. Comprehensive meta-analysis of resilience interventions. Clin Psychol Rev. (2020) 82:101919. doi: 10.1016/j.cpr.2020.101919
81. Riggle RJ, Edmondson DR, Hansen JD. A meta-analysis of the relationship between perceived organizational support and job outcomes: 20 years of research. J Bus Res. (2009) 62:1027–30. doi: 10.1016/j.jbusres.2008.05.003
Keywords: burnout, anxiety, depression, post-traumatic stress disorders, COVID-19, health personnel, psychological stress
Citation: Cyr S, Marcil M-J, Marin M-F, Tardif J-C, Guay S, Guertin M-C, Rosa C, Genest C, Forest J, Lavoie P, Labrosse M, Vadeboncoeur A, Selcer S, Ducharme S and Brouillette J (2021) Factors Associated With Burnout, Post-traumatic Stress and Anxio-Depressive Symptoms in Healthcare Workers 3 Months Into the COVID-19 Pandemic: An Observational Study. Front. Psychiatry 12:668278. doi: 10.3389/fpsyt.2021.668278
Received: 15 February 2021; Accepted: 31 May 2021;
Published: 08 July 2021.
Edited by:
Claudia Carmassi, University of Pisa, ItalyReviewed by:
Muhammed Elhadi, University of Tripoli, LibyaFederica Sancassiani, University of Cagliari, Italy
Annalisa Cordone, University of Pisa, Italy
Copyright © 2021 Cyr, Marcil, Marin, Tardif, Guay, Guertin, Rosa, Genest, Forest, Lavoie, Labrosse, Vadeboncoeur, Selcer, Ducharme and Brouillette. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Judith Brouillette, anVkaXRoLmJyb3VpbGxldHRlQGljbS1taGkub3Jn
†These authors have contributed equally to this work