 Ciqing Bao
Ciqing Bao Ling Xu1
Ling Xu1- 1Wenzhou Seventh People's Hospital, Wenzhou, China
- 2School of Mental Health, Wenzhou Medical University, Wenzhou, China
- 3Department of Obstetrics, First Affiliated Hospital of Wenzhou Medical University, Wenzhou, China
- 4Department of Neurology, First Affiliated Hospital of Wenzhou Medical University, Wenzhou, China
- 5The Affiliated Kangning Hospital of Wenzhou Medical University, Wenzhou, China
Although many risk factors for suicidal ideation have been identified, few studies have focused on suicidal ideation and pre-natal depression. The purpose was to investigate the relationship between decision-making (DM) dysfunction and sleep disturbance on suicidal ideation in pre-natal depression. Participants included 100 women in the third trimester of pregnancy, including pregnant women with pre-natal depression who had recent suicidal ideation (n = 30), pre-natal depression without SI (n = 35) and healthy controls (n = 35). The Iowa Gambling Task (IGT) was used to evaluate the DM function and the Pittsburgh Sleep Quality Index (PSQI) was used to assess the sleep index. The Edinburgh Post-natal Depression Scale (EPDS) was used to assess suicidal ideation and the seriousness of depression. Overall, the two groups with pre-natal depression showed worse sleep quality and decreased DM function compared with healthy controls. The pre-natal depression with suicidal ideation group showed a significantly higher score in subjective sleep quality and a lower score in block 5 of IGT than the pre-natal depression without suicidal ideation group. Further correlation analysis showed that suicidal ideation positively correlated with subjective sleep quality, sleep duration, and daytime function, and negatively correlated with IGT scores. Sleep disturbance and impaired DM function may be risk factors for suicidal ideation in pre-natal depression.
Introduction
Suicide in the perinatal period is an important public health problem, and suicidal ideation is, one of the most important risk factors for suicidal behavior. During pregnancy, the prevalence of suicidal ideation can reach between 5 and 14% (1–3) and there is a correlation between suicidal ideation and suicide attempts that can result in an elevated suicide risk at some point in the future (1, 4–7). There are many risk factors for suicidal ideation during pregnancy, including accidental pregnancy (8, 9), education level (10, 11), marital status (12, 13), and intimate partner violence (11, 14). Depression and anxiety may be the most important biological factors of perinatal suicide (15, 16). The incidence of perinatal depression is as high as 10–30%, and perinatal depression patients show a higher rate of suicide and self-injury than those with general depression (17). There are few studies on the decision-making (DM) function of perinatal depression patients, even though DM dysfunction may be closely related to suicidal ideation in perinatal depression patients.
DM can be defined as the cognitive process that identifies and selects the best available solution for a given problem or challenging situation based on the value and preferences of the decision maker. The Iowa Gambling Task (IGT) is one of the most commonly used DM tasks (18), and was developed to simulate real-world DM processes in vague and dangerous situations. DM is impaired in various mental illnesses, including obsessive-compulsive disorder (19), schizophrenia (20), and depression (21, 22). Teenagers and adults with DM defects are more likely to display suicidal behavior (23), and more researches have shown that DM play a very important role in suicidal behavior (24). Neurobiological studies have found that the integrity of the orbital cortex/ventral medial PFC (OFC/VMPFC) determines the ability to make decisions. When the OFC/VMPFC is impaired, people suffer from false emotional signals, leading to neglect of unfavorable factors in the future and a focus on immediate interests (25). In depression, structural changes are found in the OFC and VMPFC, and these changes are thought to be closely related to the onset and severity of depression (26, 27).
A large proportion of patients with depression have sleep disturbance and, furthermore, sleep disturbance is more common in perinatal depression than in general depression because of the physiological changes associated with pregnancy (28). There are many studies that show a correlation between pre-natal depression and sleep disturbance (29–33). Jomeen et al. (34) found that about 26% of pregnant women had mild to moderate depressive symptoms, and the sleep quality of the depressed group was worse than that of the non-depressed group. Higher Pittsburgh Sleep Quality Index (PSQI)scores in early pregnancy predict an increase in the Beck depression index scores in the second trimester, and higher PSQI scores in the second trimester predict a higher Beck depression index score in the third trimester, suggesting that sleep quality in the first trimester of pregnancy can predict the clinical symptoms of depression in the third trimester of pregnancy (35). Studies have also shown that there is a correlation between suicidal ideation and sleep during pregnancy (36–38). In one study, in mid-pregnancy, women with high sleep reactivity report elevated symptoms of insomnia, depression, and anxiety, and were more likely to participate in suicidal ideation (39). Previous studies have also suggested that sleep may optimize emotion-guided DM. For example, Pace-Schott et al. reported that after uninterrupted sleep, subjects scores better in the IGT than those that had undergone interrupted sleep (40).
Although there are no studies on DM in pregnant women with pre-natal depression, there has been some research into pregnancy and post-natal cognitive performance and mood. Many studies have shown that there may be cognitive changes in perinatal depression patients (41–46). A Portuguese study found that more dysfunctional beliefs related with maternal responsibility, more frequent negative thoughts related with personal maladjustment and with the metacognitive appraisal of the thoughts' content, and less frequent positive thoughts were significantly associated with postpartum depression symptoms (47). Stress associated with pregnancy may contribute to postpartum mental illness and its associated symptoms by compromising structural plasticity in the mPFC (48). Women may show specific areas of cognitive changes during and after pregnancy, in particular, deficits in verbal learning and memory; mood appears to be impacted as well (46).
There are currently no studies on the association suicidal ideation and DM in patients with perinatal depression. The physiological and psychological mechanisms of high suicidal ideation in perinatal depression are currently unclear. In the present study, we hypothesized that high suicidal ideation in patients with perinatal depression is closely associated with sleep disorders and impaired DM during pregnancy. The purpose of this study was to determine if sleep quality and DM ability are associated with suicidal ideation in pre-natal women with depression compared to pre-natal women without depression.
Methods
Participants
A total of 100 pregnant women in late pregnancy were recruited from the obstetrics clinic of the First Affiliated Hospital of Wenzhou Medical University. Three groups were as follows: Group SI included 30 pre-natal depression pregnant women with suicidal ideation (Edinburgh Post-natal Depression Scale (EPDS) >9 and the 10th item in the EPDS except “never”); Group NSI consisted of 35 pregnant women with antenatal depression, but no suicidal ideation (EPDS >9, item 10 in the EPDS was selected as “never”); Group CG was a control group consisting of 35 healthy pregnant women (EPDS ≤ 9, and item 10 in the EPDS was selected as “never”). Inclusion and exclusion criteria were based on clinical structured interviews and self-reports.
The inclusion criteria were: (1) adult (≥18 years old); (2) late pregnancy (28–40 weeks); and (3) willing to sign informed consent.
The exclusion criteria were: (1) history of mental illness or brain disorders; (2) chronic diseases that require regular medical care; (3) intellectual disability; (4) obvious pregnancy complications; and (5) reading and writing dysfunction.
The researchers were composed of psychiatry and mental-health graduate students and physicians, who had undergone consistent training before the experiment began. Our trained researchers collected demographic and clinical information about all pregnant women in face-to-face interviews through standardized questionnaires, including age, height, weight, ethnicity, place of residence, marital status, level of education, monthly family income, history of mental illness, and family history of mental illness. And the standardized questionnaire consists of a demographic scale with consistent guidance and content.
Assessments
The Edinburgh Post-natal Depression Scale
In western countries, the EPDS (49) is a widely used depression assessment scale. And it is believed to be effective in multiple cultures during pregnancy (50–53) and postpartum. It has 10 items testing: mood, pleasure, guilt, anxiety, fear, insomnia, ability to cope, sadness, crying, and self-injury. In accordance with the severity of the relevant symptom, each item is divided into 0–3 points and the total score ranges from 0 to 30 points. The scale has good reliability and validity in populations in mainland China (54). In this experiment, a total score of >9 was classified as depression (55).
Suicidal Ideation
To evaluate suicidal ideation, we examined item 10 of the EPDS (presented as “The thought of harming myself has occurred to me”) (56–58). Possible responses included “never” = 0, “hardly ever” = 1, “sometimes” = 2, or “quite often” = 3. Due to the particularity of China's national conditions, “never” is defined as “no suicidal ideation” and the other three are defined as “suicidal ideation.”
The Pittsburgh Sleep Quality Index
The PSQI (59) was used to assess sleep quality over the previous month. The maximum total score of the PSQI is 21 points. Nineteen individual items generate seven component scores (range 0–3, with higher scores indicating worse sleep): subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleeping medication, and daytime dysfunction. This scale has good internal consistency, test-retest reliability, and validity (60). A score of >5 is indicative of clinically significant sleep disturbance.
Iowa Gambling Task
DM was assessed using the IGT (61). Participants completed the computerized version of the IGT consisting of four decks of cards labeled A, B, C, and D. The participants made 100 card selections. After each selection, a specified amount of facsimile money was awarded. At the top of the computer screen, a bar indicates wins and losses and changes according to the amount of money won or lost after each selection. Participants were told that the aim of the game is to win as much money as possible. They were also instructed that some decks were better than others and that they have to avoid the bad decks. The total net score on the IGT is the difference between the total number of cards selected from advantageous decks (decks C′+ D′) and disadvantageous decks (decks A′+B′). Block scores were calculated for every 20 cards selected in the same manner. The total net scores range from −100 to 100 and block scores range from −20 to 20. Positive net and block scores indicate advantageous decision-making.
Statistical Analysis
Comparison of the three groups (SI, NSI, and CG) with regard to sociodemographic and clinical variables were performed by means of one-way analysis of variance, Kruskal–Wallis test, and the Chi-square test, depending on the variable type (normally distributed, non-normally distributed and categorical, respectively). Checks for deviations from normality were performed by means of the Kolmogorov–Smirnov test. Post-hoc pairwise comparisons (by t-test, Mann–Whitney U-test, or Chi-square test, respectively) were conducted only if the overall group comparison yielded a significant result (p < 0.05). In the case of three groups, this sequential testing procedure allowed testing of group differences without adjustment for multiple comparisons.
The same procedure was also used to compare the three groups with PSQI and the DM task IGT. As the IGT consists of five consecutive blocks, we performed an additional repeated-measures analysis of variance with time as a within-subjects factor and group as a between-subjects factor to adjust for potential learning effects.
Spearman correlation analysis was used to analyze the correlations among sleep (PSQI and its seven component scores), DM function, and suicidal ideation in late pregnancy women.
Results
A total of 100 participants (SI group, n = 30; NSI group, n = 35; CG group, n = 35) were included. Sociodemographic and clinical data are presented in Table 1. The three groups did not differ with respect to age, years of education, marital status, family monthly income, subjective occupational stress, the number of children, or the number of abortions.
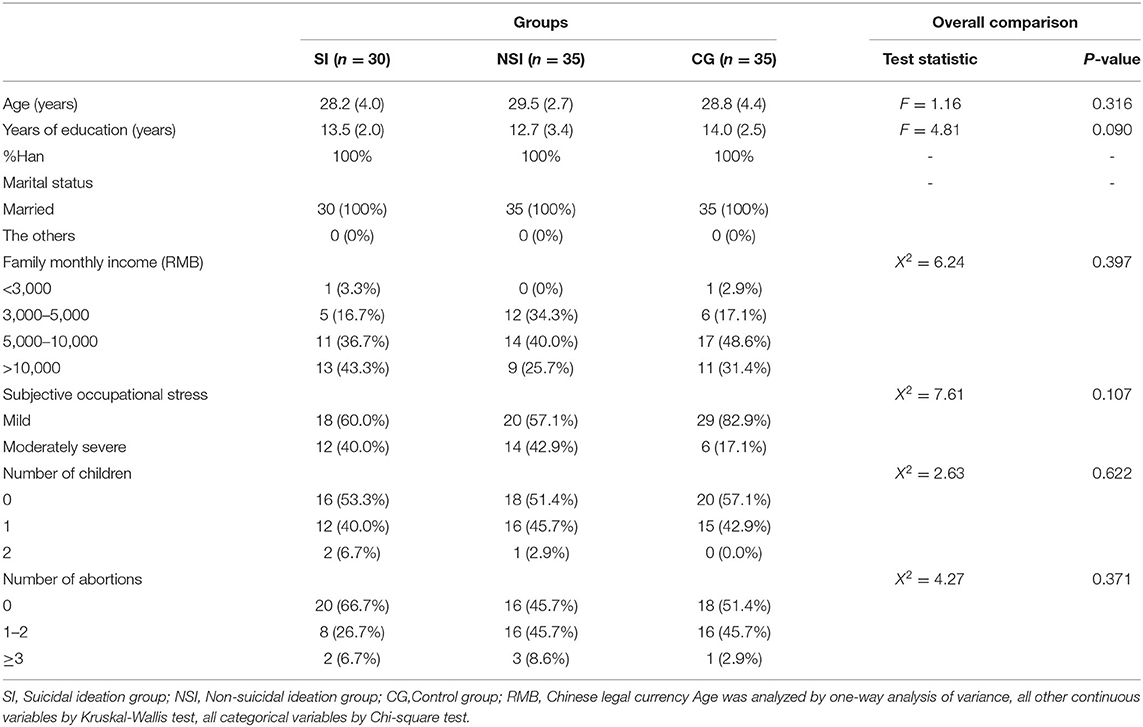
Table 1. Sociodemographic and clinical variables.
Table 2 shows the results of the EPDS scores, EPDS scores without suicidal ideation, and PSQI between groups. Compared with the NSI group, the EPDS scores of the SI group were significantly increased, which was due to the higher score of the suicide ideation factor on the EPDS. There were significant differences between the three groups except for the PSQI scale and the EPDS scale without suicidal factor scores. There were also significant differences in subjective sleep quality, sleep disturbance, and daytime function in the PSQI scale. For the subjective sleep quality, the SI group showed a significantly higher score than the other two groups. This means that women with suicidal ideation had worse subjective sleep quality than women without suicidal ideation and healthy controls. No significant differences were found between the NSI and CG groups. The scores of sleep disturbances and daytime function in the SI group were significantly higher than those in the CG group.
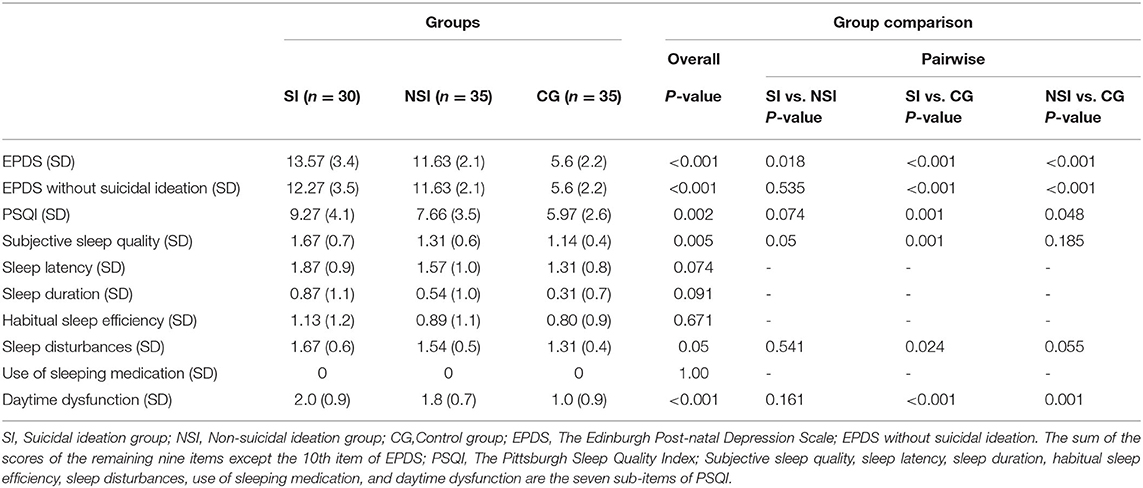
Table 2. Differences in scores of PSQI and EPDS among the three groups (SI, NSI, CG).
There were significant differences of in the IGT scores and block3-block5 scores among the groups (Table 3). Among these differences, the block 5 group were significant after comparison. Repeated measures ANOVA revealed significant positive effects in the different groups of IGT (F = 10.653, p < 0.001) and significant learning effects from the first to fifth blocks of the IGT (F = 17.905, p < 0.001). In addition, test time interacted with the group (F = 3.706, P = 0.001).
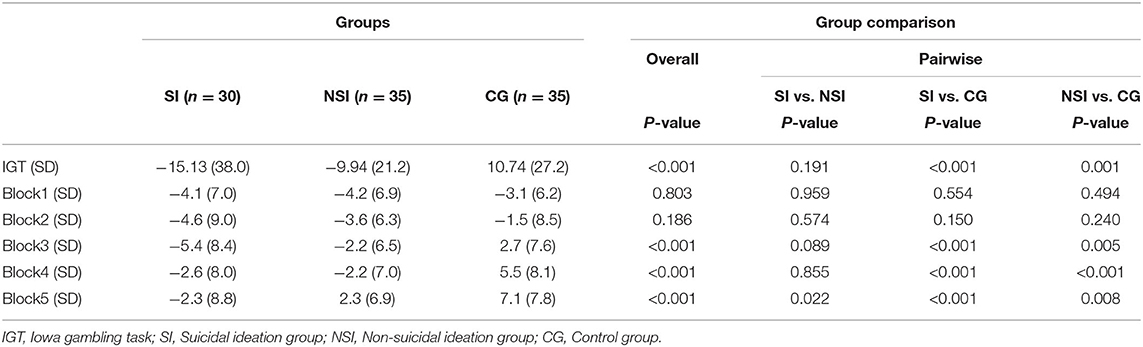
Table 3. Differences in decision-making functions among three groups (SI, NSI, CG).
Spearman correlation analysis (Table 4) showed that suicide ideation positively correlated with pre-natal depression (r = 0.415, P < 0.001), PSQI (r = 0.289, P = 0.004), subjective sleep quality (r = 0.305, P = 0.002), sleep duration (r = 0.212, P = 0.034), and daytime dysfunction (r = 0.299, P = 0.002), and negatively correlated with IGT total score (r = −0.265, p = 0.008).
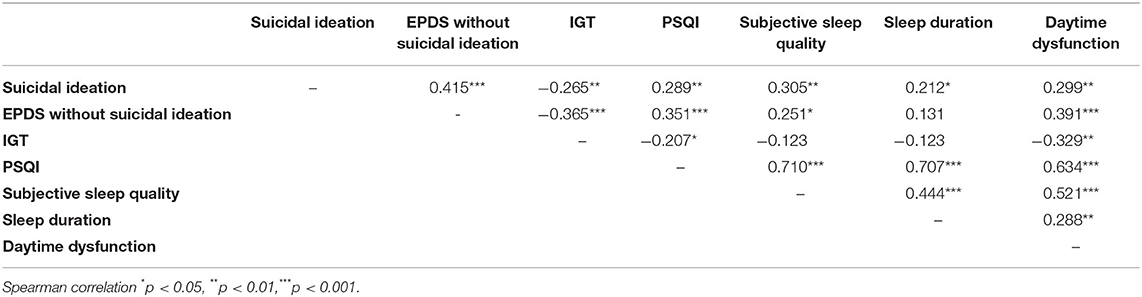
Table 4. Spearman correlation matrix of suicidal ideation, PSQI and IGT.
Discussion
To the best of our knowledge, this is the first study to assess DM and sleep in pre-natal depression patients with suicidal ideation. The risk-decision made by the suicidal ideation group in the fifth block of the IGT was significantly higher than that of the NSI group and the healthy control group, which indicates that people with DM defects have stronger suicidal ideation. Suicide ideation positively correlated with pre-natal depression, subjective sleep quality, sleep duration, and daytime dysfunction, and negatively correlated with DM function. The three groups in our study did not differ significantly in social demographics.
Our findings are generally consistent with the existing literature documenting the association of poor subjective sleep quality with the likelihood of suicidal ideation among men and non-pregnant women (62, 63). However, there are few studies on sleep and pre-natal depression and suicidal ideation during pregnancy. Among them, one study showed that poor subjective sleep quality was associated with an increased likelihood of suicidal ideation (36). The article mentioned that after adjusting for depression, the probability of suicidal ideation increases by 18% for every unit increase in the global PSQI score. The proportion of subjective sleep quality and suicidal ideation in patients with depression increased by 3.5-fold compared with patients without risk factors. Another study published in 2016 showed similar results (37).
Our study confirmed the correlation between suicidal ideation and subjective sleep quality, and the difference was also significantly related to sleep duration and daytime dysfunction. The causal relationship between sleep disorders and suicide in major depression is unclear, however, there is evidence that the activities of the three neurobiological systems play a key role in the pathophysiology of suicidal behavior, i.e., hyperactivity of the hypothalamus-pituitary-adrenal axis, dysfunction of the serotoninergic system and overactivity of the noradrenergic system. Not only the first and last systems appear to be involved in the response to stress events, the hyperactivity of the HPA axis and the dysfunction of the serotonergic system are also associated with changes in the sleep-wake cycle, such as insomnia (64–67). In depression, HPA hyperactivity can have many negative effects on sleep. It can lead to sleep fragmentation, decreased slow-wave sleep, and shortened sleep time (66). It can therefore be assumed that neurobiological dysfunction mediates the occurrence of suicidal behavior through the disturbed regulation of basic neuropsychological functions. The main clinical significance of suicidal ideation/sleep disturbance is that sleep assessment may help assess the risk of suicide in patients with antenatal depression.
Previous studies of DM and suicidal ideation have produced controversial results. Some studies have shown that IGT scores are significantly lower in people who currently have suicidal ideation compared with healthy controls (68). However, in contrast, some studies found no association between suicidal ideation and DM (69, 70). DM deficiencies were related to suicide attempts in adolescents and adults, and the group differences in DM did not persist after controlling for current emotional problems and the use of psychotropic substances. In this study, there was no significant difference in the IGT net score between the SI group and the NSI group, but there was a significant difference compared with the healthy control, indicating that there was a decision deficit in the pre-natal depression groups with or without suicidal ideation. By comparing the net scores and their trends in different blocks, we analyzed the DM characteristics and strategy adjustment of the subjects in the income-loss situation (71). There was no significant difference in the net scores of blocks 1–2 between the three groups in this study. In blocks 3–4, both groups with depression had significantly lower scores than the healthy controls, while there was no significant difference between the SI and NSI groups. The two groups of pregnant women with pre-natal depression showed no difference in performance at the beginning and the middle stage. As the task progressed, the net scores of the two groups in the fifth block were different. The SI group scores were significantly lower than those in the NSI group, and the scores of both groups were lower than those of the healthy control group. These data shows that patients with pre-natal depression lack decision-making ability, have poor strategy adjustment, and do not show the “learning effect” of normal healthy people or improve the net score, while the DM function defects of pre-natal depression patients with suicidal ideation are more serious.
A previous study suggested that IGT performance was not mediated by the conscious knowledge of risk. Patients selected cards that brought higher immediate rewards despite more severe penalties, and patients with OFC/VMPFC lesions often showed this pattern of behavior (25, 72). Another study found that REM sleep in emotion-guided decision making plays a selective role, the subjects performed highly on the IGT, whose OFC/VMPFC regions were selectively activated in REM sleep (73). Sleep disturbances, including insomnia and sleep deprivation, can produce a labile mood (74), which may correspond with neural responses that suggest abnormal reward processing and autonomic hyperarousal (75), limbic overactivity (76), and loss of medial pre-frontal cortex connectivity (77). Having sleep disturbance could worsen the altered reward processes in mothers with depression and SI (78). We hypothesized that sleep inefficiency and daytime dysfunction would aggravate impairment of DM function in patients and the correlation results support our hypothesis.
Our study shows that suicidal ideation and depressive symptoms of pregnant women need to be carefully monitored, especially in those with poor sleep quality. Pregnant women often report poor sleep quality and those with poor subjective sleep quality should be evaluated for suicide ideation. Actively dealing with sleep problems may reduce suicide behavior of pregnant women. For example, investigators have noted that behavioral (e.g., sleep hygiene, stimulus control, and imagery rehearsal therapy) and pharmacological interventions may be particularly promising modalities for reducing the risk of suicidal ideation (79). This study suggests that the decision-making function impairment may be associated with pre-natal depression and suicidal ideation in pregnant women, However, further studies on the neuropathological mechanism are needed, such as functional magnetic resonance imaging (fMRI).
This study reports the DM profile of recent pre-natal depression subjects with suicidal ideation and confirms the existence of decision deficits in this population. The study also found correlations between antenatal depression, suicidal ideation and sleep disturbance. There is an urgent need to raise awareness of this issue and further longitudinal studies should be encouraged to examine other cognitive functions that may be related to suicide status.
There are several limitations in our study. Firstly, the sample size was relatively small (n = 100) and it will be necessary to study a larger sample size to reduce the type II error rate. Secondly, due to the nature of cross-sectional studies, we are not sure of the dynamic relationship between suicidal ideation and sleep in perinatal depression patients during pregnancy, nor can we infer the causal relationship between suicidal ideation and impaired DM function. Longitudinal studies are needed to address these questions and verify our findings. Thirdly, In this study, only the subjective scale (PSQI) was used to evaluate sleep, without using objective evaluation indicators, such as polysomnography test. Finally, due to the absence of brain imaging, in this study we do not know whether any neuroanatomical/functional changes in the patients' brains occurred.
Data Availability Statement
The data analyzed in this study is subject to the following licenses/restrictions: Due to relevant data protection laws. Requests to access these datasets should be directed to YmFvY2lxaW5nQDE2My5jb20=.
Ethics Statement
The studies involving human participants were reviewed and approved by Ethics Committee of Wenzhou Medical University. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
CB and KZ conceived and designed the study and developed it in discussion with LX, WT, SS, and WZ. SS, WT, and LX were involved in the acquisition and analysis of the data. DX and XY provided research funding. CB wrote the first draft of the article. All authors participated in the interpretation of the data, contributed to critically revising the paper, read, and approved the final manuscript.
Funding
This work were supported by the Natural Science Foundation of Zhejiang Province (LQ18H090009 and LY19H090015). The preparation of the material scales were part of the funding of the fund.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We wish to thank all the participants and medical staff of the First Affiliated Hospital of Wenzhou Medical University who supported our research. We thank all of the volunteers for their study participation and the support of the First Affiliated Hospital of WenZhou Medical University.
Abbreviations
DM, decision-making; IGT, Iowa Gambling Task; PSQI, Pittsburgh Sleep Quality Index; EPDS, Edinburgh Post-natal Depression Scale; OFC, orbitofrontal cortex; VMPFC, ventromedial PFC.
References
1. Lindahl V, Pearson JL, Colpe L. Prevalence of suicidality during pregnancy and the postpartum. Arch Women Ment Health. (2005) 8:77–87. doi: 10.1007/s00737-005-0080-1
2. Bridge JA, McBee-Strayer SM, Cannon EA, Sheftall AH, Reynolds B, Campo JV, et al. Impaired decision making in adolescent suicide attempters. J Am Acad Child Adolesc Psychiatry. (2012) 51:394–403. doi: 10.1016/j.jaac.2012.01.002
3. Deisenhammer EA, Schmid SK, Kemmler G, Moser B, Delazer M. Decision making under risk and under ambiguity in depressed suicide attempters, depressed non-attempters and healthy controls. J Affect Disord. (2018) 226:261–6. doi: 10.1016/j.jad.2017.10.012
4. Joiner TE, Rudd D, Rouleau MR, Wagner KD. Parameters of suicidal crises vary as a function of previous suicide attempts in youth inpatients. J Am Acad Child Adolesc Psychiatry. (2000) 39:876–80. doi: 10.1097/00004583-200007000-00016
5. Swogger MT, Van Orden KA, Conner KR. The relationship of outwardly-directed aggression to suicidal ideation and suicide attempts across two high-risk samples. Psychol Violence. (2014) 4:184–95. doi: 10.1037/a0033212
6. Gelaye B, Kajeepeta S, Williams MA. Suicidal ideation in pregnancy: an epidemiologic review. Arch Women Ment Health. (2016) 19:741–51. doi: 10.1007/s00737-016-0646-0
7. Mbroh H, Zullo L, Westers N, Stone L, King J, Kennard B, et al. Double trouble: nonsuicidal self-injury and its relationship to suicidal ideation and number of past suicide attempts in clinical adolescents. J Affect Disord. (2018) 238:579–85. doi: 10.1016/j.jad.2018.05.056
8. Newport DJ, Levey LC, Pennell PB, Ragan K, Stowe ZN. Suicidal ideation in pregnancy: assessment and clinical implications. Arch Women Ment Health. (2007) 10:181–7. doi: 10.1007/s00737-007-0192-x
9. Ishida K, Stupp P, Serbanescu F, Tullo E. Perinatal risk for common mental disorders and suicidal ideation among women in Paraguay. Int J Gynecol Obstet. (2010) 110:235–40. doi: 10.1016/j.ijgo.2010.03.027
10. Coelho FM, Pinheiro RT, Silva RA, de Avila Quevedo L, de Mattos Souza LD, de Matos MB, et al. Parental bonding and suicidality in pregnant teenagers: a population-based study in southern Brazil. Soc Psychiatry Psychiatr Epidemiol. (2014) 49:1241–8. doi: 10.1007/s00127-014-0832-1
11. Alhusen JL, Frohman N, Purcell G. Intimate partner violence and suicidal ideation in pregnant women. Arch Women Ment Health. (2015) 18:573–8. doi: 10.1007/s00737-015-0515-2
12. Huang H, Faisal-Cury A, Chan YF, Tabb K, Katon W, Menezes PR. Suicidal ideation during pregnancy: prevalence and associated factors among low-income women in São Paulo, Brazil. Arch Women Ment Health. (2012) 15:135–8. doi: 10.1007/s00737-012-0263-5
13. Kim JJ, La Porte LM, Silver RK. Suicide risk among perinatal women who report thoughts of self-harm on depression screens reply. Obstet Gynecol. (2015) 126:217. doi: 10.1097/AOG.0000000000000941
14. Fisher J, Tran TD, Biggs B, Dang TH, Nguyen TT, Tran T. Intimate partner violence and perinatal common mental disorders among women in rural Vietnam. Int Health. (2013) 5:29–37. doi: 10.1093/inthealth/ihs012
15. Farias DR, Pinto Tde J, Teofilo MM, Vilela AA, Vaz Jdos S, Nardi AE, et al. Prevalence of psychiatric disorders in the first trimester of pregnancy and factors associated with current suicide risk. Psychiatry Res. (2013) 210:962–8. doi: 10.1016/j.psychres.2013.08.053
16. Eggleston AM, Calhoun PS, Svikis DS, Tuten M, Chisolm MS, Jones HE. Suicidality, aggression, and other treatment considerations among pregnant, substance-dependent women with posttraumatic stress disorder. Compr Psychiat. (2009) 50:415–23. doi: 10.1016/j.comppsych.2008.11.004
17. Ebeid E, Nassif N, Sinha P. Prenatal depression leading to postpartum psychosis. J Obstet Gynaecol. (2010) 30:435–8. doi: 10.3109/01443611003802321
18. Bechara A, Damasio AR, Damasio H, Anderson SW. Insensitivity to future consequences following damage to human prefrontal cortex. Cognition. (1994) 50:7–15. doi: 10.1016/0010-0277(94)90018-3
19. Pushkarskaya H, Tolin D, Ruderman L, Kirshenbaum A, Kelly JM, Pittenger C, et al. Decision-making under uncertainty in obsessive-compulsive disorder. J Psychiatr Res. (2015) 69:166–73. doi: 10.1016/j.jpsychires.2015.08.011
20. Fond G, Bayard S, Capdevielle D, Del-Monte J, Mimoun N, Macgregor A, et al. A further evaluation of decision-making under risk and under ambiguity in schizophrenia. Eur Arch Psy Clin N. (2013) 263:249–57. doi: 10.1007/s00406-012-0330-y
21. Must A, Szabo Z, Bodi N, Szasz A, Janka Z, Keri S. Sensitivity to reward and punishment and the prefrontal cortex in major depression. J Affect Disord. (2006) 90:209–15. doi: 10.1016/j.jad.2005.12.005
22. Thames AD, Streiff V, Patel SM, Panos SE, Castellon SA, Hinkin CH. The role of HIV infection, cognition, and depression in risky decision-making. J Neuropsychiatry Clin Neurosci. (2012) 24:340–8. doi: 10.1176/appi.neuropsych.11110340
23. Richard-Devantoy S, Berlim MT, Jollant F. A meta-analysis of neuropsychological markers of vulnerability to suicidal behavior in mood disorders. Psychol Med. (2014) 44:1663–73. doi: 10.1017/S0033291713002304
24. Clark L, Dombrovski AY, Siegle GJ, Butters MA, Shollenberger CL, Sahakian BJ, et al. Impairment in risk-sensitive decision-making in older suicide attempters with depression. Psychol Aging. (2011) 26:321–30. doi: 10.1037/a0021646
25. Daurat A, Ricarrere M, Tiberge M. Decision making is affected in obstructive sleep apnoea syndrome. J Neuropsychol. (2013) 7:139–44. doi: 10.1111/j.1748-6653.2012.02039.x
26. Jalbrzikowski M, Larsen B, Hallquist MN, Foran W, Calabro F, Luna B. Development of white matter microstructure and intrinsic functional connectivity between the amygdala and ventromedial prefrontal cortex: associations with anxiety and depression. Biol Psychiatry. (2017) 82:511–21. doi: 10.1016/j.biopsych.2017.01.008
27. Klauser P, Fornito A, Lorenzetti V, Davey CG, Dwyer DB, Allen NB, et al. Cortico-limbic network abnormalities in individuals with current and past major depressive disorder. J Affect Disord. (2015) 173:45–52. doi: 10.1016/j.jad.2014.10.041
28. Krawczak EM, Minuzzi L, Simpson W, Hidalgo MP, Frey BN. Sleep, daily activity rhythms and postpartum mood: a longitudinal study across the perinatal period. Chronobiol Int. (2016) 33:791–801. doi: 10.3109/07420528.2016.1167077
29. Ko SH, Chang SC, Chen CH. A comparative study of sleep quality between pregnant and nonpregnant Taiwanese women. J Nurs Scholarship. (2010) 42:23–30. doi: 10.1111/j.1547-5069.2009.01326.x
30. Skouteris H, Germano C, Wertheim EH, Paxton SJ, Milgrom J. Sleep quality and depression during pregnancy: a prospective study. J Sleep Res. (2008) 17:217–20. doi: 10.1111/j.1365-2869.2008.00655.x
31. Kamysheva E, Skouteris H, Wertheim EH, Paxton SJ, Milgrom J. A prospective investigation of the relationships among sleep quality, physical symptoms, and depressive symptoms during pregnancy. J Affect Disord. (2010) 123:317–20. doi: 10.1016/j.jad.2009.09.015
32. Mellor R, Chua SC, Boyce P. Antenatal depression: an artefact of sleep disturbance?. Arch Women Ment Health. (2014) 17:291–302. doi: 10.1007/s00737-014-0427-6
33. Yang Y, Mao J, Ye Z, Zeng X, Zhao H, Liu Y, et al. Determinants of sleep quality among pregnant women in China: a cross-sectional survey. J Matern Fetal Neonatal Med. (2018) 31:2980–5. doi: 10.1080/14767058.2017.1359831
34. Jomeen J, Martin CR. Replicability and stability of the multidimensional model of the Edinburgh Postnatal Depression Scale in late pregnancy. J Psychiatr Ment Health Nurs. (2007) 14:319–24. doi: 10.1111/j.1365-2850.2007.01084.x
35. Krawczak EM, Minuzzi L, Hidalgo MP, Frey BN. Do changes in subjective sleep and biological rhythms predict worsening in postpartum depressive symptoms? A prospective study across the perinatal period. Arch Women Ment Hlth. (2016) 19:591–8. doi: 10.1007/s00737-016-0612-x
36. Gelaye B, Barrios YV, Zhong QY, Rondon MB, Borba CPC, Sanchez SE, et al. Association of poor subjective sleep quality with suicidal ideation among pregnant Peruvian women. Gen Hosp Psychiat. (2015) 37:441–7. doi: 10.1016/j.genhosppsych.2015.04.014
37. Gelaye B, Addae G, Neway B, Larrabure-Torrealva GT, Qiu CF, Stoner L, et al. Poor sleep quality, antepartum depression and suicidal ideation among pregnant women. J Affect Disord. (2017) 209:195–200. doi: 10.1016/j.jad.2016.11.020
38. Sit D, Luther J, Buysse D, Dills JL, Eng H, Okun M, et al. Suicidal ideation in depressed postpartum women: associations with childhood trauma, sleep disturbance and anxiety. J Psychiatr Res. (2015) 66–67:95–104. doi: 10.1016/j.jpsychires.2015.04.021
39. Palagini L, Cipollone G, Masci I, Novi M, Caruso D, Kalmbach DA, et al. Stress-related sleep reactivity is associated with insomnia, psychopathology and suicidality in pregnant women: preliminary results. Sleep Med. (2019) 56:145–50. doi: 10.1016/j.sleep.2019.01.009
40. Pace-Schott EF, Nave G, Morgan A, Spencer RMC. Sleep-dependent modulation of affectively guided decision-making. J Sleep Res. (2012) 21:30–9. doi: 10.1111/j.1365-2869.2011.00921.x
41. Mazor E, Sheiner E, Wainstock T, Attias M, Walfisch A. The association between depressive state and maternal cognitive function in postpartum women. Am J Perinatol. (2019) 36:285–90. doi: 10.1055/s-0038-1667376
42. Meena PS, Soni R, Jain M, Jilowa CS, Omprakash. Cognitive dysfunction and associated behaviour problems in postpartum women: a study from North India. East Asian Arch Psychiatry. (2016) 26:104–8
43. Hampson E, Phillips SD, Duff-Canning SJ, Evans KL, Merrill M, Pinsonneault JK, et al. Working memory in pregnant women: relation to estrogen and antepartum depression. Horm Behav. (2015) 74:218–27. doi: 10.1016/j.yhbeh.2015.07.006
44. Logan DM, Hill KR, Jones R, Holt-Lunstad J, Larson MJ. How do memory and attention change with pregnancy and childbirth? A controlled longitudinal examination of neuropsychological functioning in pregnant and postpartum women. J Clin Exp Neuropsychol. (2014) 36:528–39. doi: 10.1080/13803395.2014.912614
45. Farrar D, Tuffnell D, Neill J, Scally A, Marshall K. Assessment of cognitive function across pregnancy using CANTAB: a longitudinal study. Brain Cogn. (2014) 84:76–84. doi: 10.1016/j.bandc.2013.11.003
46. Buckwalter JG, Buckwalter DK, Bluestein BW, Stanczyk FZ. Pregnancy and post partum: changes in cognition and mood. Prog Brain Res. (2001) 133:303–19. doi: 10.1016/S0079-6123(01)33023-6
47. Fonseca A, Canavarro MC. Cognitive correlates of women's postpartum depression risk and symptoms: the contribution of dysfunctional beliefs and negative thoughts. J Ment Health. (2020) 29:614–22. doi: 10.1080/09638237.2019.1581331
48. Leuner B, Fredericks PJ, Nealer C, Albin-Brooks C. Chronic gestational stress leads to depressive-like behavior and compromises medial prefrontal cortex structure and function during the postpartum period. PLoS ONE. (2014) 9:e89912. doi: 10.1371/journal.pone.0089912
49. Cox JL, Holden JM, Sagovsky R. Detection of postnatal depression. Development of the 10-item Edinburgh Postnatal Depression Scale. Br J Psychiatry. (1987) 150:782–6. doi: 10.1192/bjp.150.6.782
50. Joshi U, Lyngdoh T, Shidhaye R. Validation of hindi version of Edinburgh postnatal depression scale as a screening tool for antenatal depression. Asian J Psychiatr. (2020) 48:101919. doi: 10.1016/j.ajp.2019.101919
51. Kozinszky Z, Dudas RB. Validation studies of the Edinburgh Postnatal Depression Scale for the antenatal period. J Affect Disord. (2015) 176:95–105. doi: 10.1016/j.jad.2015.01.044
52. Stewart RC, Umar E, Tomenson B, Creed F. Validation of screening tools for antenatal depression in Malawi–a comparison of the Edinburgh Postnatal Depression Scale and Self Reporting Questionnaire. J Affect Disord. (2013) 150:1041–7. doi: 10.1016/j.jad.2013.05.036
53. Zhao Y, Kane I, Wang J, Shen B, Luo J, Shi S. Combined use of the postpartum depression screening scale (PDSS) and Edinburgh postnatal depression scale (EPDS) to identify antenatal depression among Chinese pregnant women with obstetric complications. Psychiatry Res. (2015) 226:113–9. doi: 10.1016/j.psychres.2014.12.016
54. Wang Y, Guo X, Lau Y, Chan KS, Yin L, Chen J. Psychometric evaluation of the Mainland Chinese version of the Edinburgh Postnatal Depression Scale. Int J Nurs Stud. (2009) 46:813–23. doi: 10.1016/j.ijnurstu.2009.01.010
55. Gaynes BN, Gavin N, Meltzer-Brody S, Lohr KN, Swinson T, Gartlehner G, et al. Perinatal depression: prevalence, screening accuracy, and screening outcomes. Evid Rep Technol Assess. (2005) 119:1–8. doi: 10.1037/e439372005-001
56. Zhong QY, Gelaye B, Rondon MB, Sanchez SE, Simon GE, Henderson DC, et al. Using the Patient Health Questionnaire (PHQ-9) and the Edinburgh Postnatal Depression Scale (EPDS) to assess suicidal ideation among pregnant women in Lima, Peru. Arch Women Ment Health. (2015) 18:783–92. doi: 10.1007/s00737-014-0481-0
57. Toreki A, Ando B, Dudas RB, Dweik D, Janka Z, Kozinszky Z, et al. Validation of the Edinburgh Postnatal Depression Scale as a screening tool for postpartum depression in a clinical sample in Hungary. Midwifery. (2014) 30:911–8. doi: 10.1016/j.midw.2014.02.008
58. da Silva RA, da Costa Ores L, Jansen K, da Silva Moraes IG, de Mattos Souza LD, Magalhaes P, et al. Suicidality and associated factors in pregnant women in Brazil. Commun Ment Health J. (2012) 48:392–5. doi: 10.1007/s10597-012-9495-0
59. Buysse DJ, Reynolds CF III, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. (1989) 28:193–213. doi: 10.1016/0165-1781(89)90047-4
60. Tsai PS, Wang SY, Wang MY, Su CT, Yang TT, Huang CJ, et al. Psychometric evaluation of the Chinese version of the Pittsburgh Sleep Quality Index (CPSQI) in primary insomnia and control subjects. Qual Life Res. (2005) 14:1943–52. doi: 10.1007/s11136-005-4346-x
61. Bechara A, Tranel D, Damasio H. Characterization of the decision-making deficit of patients with ventromedial prefrontal cortex lesions. Brain. (2000) 123:2189–202. doi: 10.1093/brain/123.11.2189
62. Agargun MY, Kara H, Solmaz M. Subjective sleep quality and suicidality in patients with major depression. J Psychiatr Res. (1997) 31:377–81. doi: 10.1016/S0022-3956(96)00037-4
63. Turvey CL, Conwell Y, Jones MP, Phillips C, Simonsick E, Pearson JL, et al. Risk factors for late-life suicide: a prospective, community-based study. Am J Geriatr Psychiatry. (2002) 10:398–406. doi: 10.1097/00019442-200207000-00006
64. Riemann D, Berger M, Voderholzer U. Sleep and depression - results from psychobiological studies: an overview. Biol Psychol. (2001) 57:67–103. doi: 10.1016/S0301-0511(01)00090-4
65. Buckley TM, Schatzberg AF. On the interactions of the hypothalamic-pituitary-adrenal (HPA) axis and sleep: normal HPA axis activity and circadian rhythm, exemplary sleep disorders. J Clin Endocrinol Metab. (2005) 90:3106–14. doi: 10.1210/jc.2004-1056
66. Steiger A. Neurochemical regulation of sleep. J Psychiatr Res. (2007) 41:537–52. doi: 10.1016/j.jpsychires.2006.04.007
67. Hatzinger M, Hemmeter UM, Brand S, Ising M, Holsboer-Trachsler E. Electroencephalographic sleep profiles in treatment course and long-term outcome of major depression: association with DEX/CRH-test response. J Psychiatr Res. (2004) 38:453–65. doi: 10.1016/j.jpsychires.2004.01.010
68. Westheide J, Quednow BB, Kuhn KU, Hoppe C, Cooper-Mahkorn D, Hawellek B, et al. Executive performance of depressed suicide attempters: the role of suicidal ideation. Eur Arch Psychiatry Clin Neurosci. (2008) 258:414–21. doi: 10.1007/s00406-008-0811-1
69. Keilp JG, Wyatt G, Gorlyn M, Oquendo MA, Burke AK, John Mann J. Intact alternation performance in high lethality suicide attempters. Psychiatry Res. (2014) 219:129–36. doi: 10.1016/j.psychres.2014.04.050
70. Sheftall AH, Davidson DJ, McBee-Strayer SM, Ackerman J, Mendoza K, Reynolds B, et al. Decision-making in adolescents with suicidal ideation: a case-control study. Psychiatry Res. (2015) 228:928–31. doi: 10.1016/j.psychres.2015.05.077
71. Bereczkei T. The manipulative skill: cognitive devices and their neural correlates underlying Machiavellian's decision making. Brain Cogn. (2015) 99:24–31. doi: 10.1016/j.bandc.2015.06.007
72. Beebe DW, Gozal D. Obstructive sleep apnea and the prefrontal cortex: towards a comprehensive model linking nocturnal upper airway obstruction to daytime cognitive and behavioral deficits. J Sleep Res. (2002) 11:1–16. doi: 10.1046/j.1365-2869.2002.00289.x
73. Neider M, Pace-Schott EF, Forselius E, Pittman B, Morgan PT. Lucid dreaming and ventromedial versus dorsolateral prefrontal task performance. Conscious Cogn. (2011) 20:234–44. doi: 10.1016/j.concog.2010.08.001
74. Zohar D, Tzischinsky O, Epstein R, Lavie P. The effects of sleep loss on medical residents' emotional reactions to work events: a cognitive-energy model. Sleep. (2005) 28:47–54. doi: 10.1093/sleep/28.1.47
75. Franzen PL, Buysse DJ. Sleep disturbances and depression: risk relationships for subsequent depression and therapeutic implications. Dialogues Clin Neurosci. (2008) 10:473–81. doi: 10.31887/DCNS.2008.10.4/plfranzen
76. Gujar N, Yoo SS, Hu P, Walker MP. Sleep deprivation amplifies reactivity of brain reward networks, biasing the appraisal of positive emotional experiences. J Neurosci. (2011) 31:4466–74. doi: 10.1523/JNEUROSCI.3220-10.2011
77. Yoo SS, Gujar N, Hu P, Jolesz FA, Walker MP. The human emotional brain without sleep - a prefrontal amygdala disconnect. Curr Biol. (2007) 17:R877–R8. doi: 10.1016/j.cub.2007.08.007
78. Walker MP, van der Helm E. Overnight therapy? The role of sleep in emotional brain processing. Psychol Bull. (2009) 135:731–48. doi: 10.1037/a0016570
Keywords: sleep disturbance, antenatal depression, suicidal ideation, decision-making function, pregnancy
Citation: Bao C, Xu L, Tang W, Sun S, Zhang W, He J, Zhao K, Xu D and Ye X (2021) Poor Sleep and Decision-Making Disturbance Are Associated With Suicidal Ideation in Pre-natal Depression. Front. Psychiatry 12:680890. doi: 10.3389/fpsyt.2021.680890
Received: 15 March 2021; Accepted: 03 May 2021;
Published: 28 May 2021.
Edited by:
Seog Ju Kim, Sungkyunkwan University, South KoreaReviewed by:
Rosalia Cesarea Silvestri, University of Messina, ItalyAxel Steiger, Ludwig Maximilian University of Munich, Germany
Copyright © 2021 Bao, Xu, Tang, Sun, Zhang, He, Zhao, Xu and Ye. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xiaodan Ye, NjAyNDAxNDI3QHFxLmNvbQ==; Dongwu Xu, d3pzZHdAMTI2LmNvbQ==; Ke Zhao, Y2hlcnJpc0AxNjMuY29t