 Piumee Bandara1
Piumee Bandara1 Andrew Page1
Andrew Page1 Lennart Reifels2*
Lennart Reifels2* Karolina Krysinska2
Karolina Krysinska2 Karl Andriessen2Marisa Schlichthorst2Anna Flego2Long Khanh-Dao Le3Cathrine Mihalopoulos3,4
Karl Andriessen2Marisa Schlichthorst2Anna Flego2Long Khanh-Dao Le3Cathrine Mihalopoulos3,4 Jane Pirkis2
Jane Pirkis2- 1Translational Health Research Institute, Western Sydney University, Campbelltown, NSW, Australia
- 2Centre for Mental Health, Melbourne School of Population and Global Health, The University of Melbourne, Parkville, VIC, Australia
- 3Health Economics Group, School of Public Health and Preventive Medicine, Faculty of Medicine, Nursing and Health Sciences, Monash University, Melbourne, VIC, Australia
- 4Deakin Health Economics, Institute for Health Transformation, School of Health and Social Development, Deakin University, Geelong, VIC, Australia
Objective: Each year approximately 3,000 Australians die by suicide. We estimated the population attributable risk for identified target populations to provide evidence on how much of the overall burden of suicide in the Australian population is experienced by each of them.
Methods: We identified 17 demographic and clinical target populations at risk of suicide and calculated the population attributable fraction (PAF) using a single or pooled suicide risk and the proportional representation of each target population within Australia.
Results: Large PAF estimates were found for men (52%, 95% confidence interval (CI) 51%–53%), people bereaved by suicide (35%, 95% CI 14%–64%), people with a mental health or behavioural condition (33%, 95%CI 17%–48%), people with a chronic physical condition (27%, 95%CI 18%–35%), adults aged 25–64 years (13%, 95%CI 12%–14%), LGB populations (9%, 95%CI 6%–13%), offenders (9%, 95%CI 8%–10%), and people employed in blue collar occupations (8%, 95%CI 4%–12%).
Limitations: The PAF is limited by assumptions, namely, that risk factors are independent, and that the relationship between risk factors and outcomes are unidirectional and constant through time.
Conclusions and implications for public health: Considerable reductions in the overall suicide rate in Australia may occur if risk factors are addressed in identified populations with large PAF estimates. These estimates should be considered as an adjunct to other important inputs into suicide prevention policy priorities.
Introduction
Suicide is the leading cause of death among Australians aged 15–44 years. In 2021, over 3,000 people died by suicide in Australia (1). Despite consistent efforts to reduce suicide in Australia, the suicide rate has remained relatively stable over the last two decades (2).
Suicide prevention remains a national health priority and in recent years there has been substantial attention to and investment in suicide prevention. The Prime Minister’s National Suicide Prevention Adviser has spearheaded a new focus on a whole-of-government approach for suicide prevention to comprehensively address the social, economic, health, cultural, and environmental factors contributing to suicide risk in the population (3). This approach recognises that specific populations are disproportionately impacted by suicidal behaviour and therefore warrant particular policy and research attention.
One way of examining the extent to which certain populations are at heightened risk is to calculate the population attributable fraction (PAF). The PAF estimates the proportion of cases of a particular health issue (e.g., suicide) that would be prevented if the effects of certain risk factors were comprehensively addressed (4). The PAF takes into consideration both the relative risk and the underlying prevalence of the risk factor in the population. This is important since risk factors with high relative risk but low prevalence, may have similar attributable risk to risk factors with lower relative risk but high prevalence (5). However, there are key assumptions of the PAF, namely, that the risk factors are independent, and that the relationship between risk factors and outcomes are unidirectional and constant through time (6, 7). In practical terms, these theoretical assumptions are not always met however, despite this, PAF estimates are a parsimonious and relatively objective way of quantifying risk that can complement other considerations to guide policy in particular areas.
Given the PAF assumes elimination of the risk factor will result in reductions in the outcome, studies have predominantly focused on modifiable clinical and social risk factors. A review of PAF used in suicidology showed psychiatric disorders are commonly identified as a large contributor to the risk of suicide and self-harm in high-income countries (4). A recent 2019 systematic review on the association between psychiatric disorders and suicide showed a PAF up to 21% for psychiatric disorders (8). Previous self-harm has also been identified as a significant contributor to self-harm in older adults in China (35%) (9) and in repeat self-harm (41%) (10), although the PAF of previous self-harm has not been examined, to our knowledge, for suicide mortality. In addition, unemployment and low socioeconomic position have been investigated as a potential contributor to suicide risk, with estimates ranging between 3% to 13% (4). The contribution appears to be larger among males, with a systematic review indicating an attributable suicide risk of 33% for manual labour/‘blue collar’ occupational status (5). Although risk factor elimination is not viable when considering sociodemographic categories such as occupational status, it is helpful to identify which population groups have a high attributable risk so that suicide prevention strategies may be targeted to address the risk factors specific to these groups. To our knowledge, no studies have systematically utilised the PAF to examine the attributable risk of a range of demographic sub-populations (e.g., men, young people, rural populations) to overall suicide risk in Australia. Accordingly, we estimate the attributable risk (the PAF) of suicide mortality for 17 identified target populations in Australia to serve as an adjunct to other inputs into suicide prevention policy decision-making.
Methods
Target populations
There are various taxonomies for considering groups that warrant attention in suicide prevention. For practical reasons, we used a taxonomy from one of our previous projects that had been developed for a different purpose (i.e., to identify Australian research priorities for suicide prevention) (11, 12). This was adapted slightly to include some additional target populations that had both well-documented high suicide risk (13–16) and relatively high proportion in the Australian population (17). In total, we identified 17 target populations: (1) men; (2) young people (aged 24 years or less); (3) adults (aged 25–64 years); (4) older adults (aged 65 years or more); (5) people born overseas; (6) Aboriginal and Torres Strait Islander people; (7) people residing in rural or remote Australia [i.e., living outside of a major city according to Australian Statistical Geography Standard (18)]; (8) people with a mental health or behavioural condition; (9) people with a chronic physical health condition; (10) people who have previously attempted suicide; (11) current or ex-serving military personnel; (12) offender populations; (13) lesbian, gay, or bisexual (LGB) populations (we were unable to include transgender people due to insufficient population-based data); (14) people bereaved by suicide; (15) people from lower socioeconomic backgrounds; (16) people employed in manual trade or “blue-collar” occupations; and (17) unemployed people.
Suicide risk estimates for target populations
To calculate the PAF for a given target population, a relative risk estimate is needed. To identify the best available evidence, we conducted a rapid review of the literature for studies on [or allowing for the extraction of) suicide mortality risk (e.g., rate ratio, risk ratio, odds ratio) for each target population (see Table 1 for sources of suicide mortality risk estimates]. Initially, we searched the bibliographic database Medline for meta-analyses published between January 1 1990 to March 31 2023, using medical subject headings (MeSH) and text terms related to suicide and identified target populations. The search was augmented by secondary searches of identified articles and Google Scholar. If no meta-analyses were available relating to a given target population, estimates were sought from Australian population-based studies, and if no Australian-based studies were available, estimates were sought from international population-based studies. We excluded studies if they did not consider any of the target populations of interest; did not measure suicide mortality as the outcome; or did not report any empirical measure of association. The literature search did not identify reliable meta-analyses or population-based studies specifically relating to men, young people, adults, older adults, and Aboriginal and Torres Strait Islander people. For these populations, we calculated suicide mortality risk estimates using the Australian Bureau of Statistics (ABS) Causes of Death data (35) and corresponding 2016 Census population denominator data to estimate the incidence rate ratios.
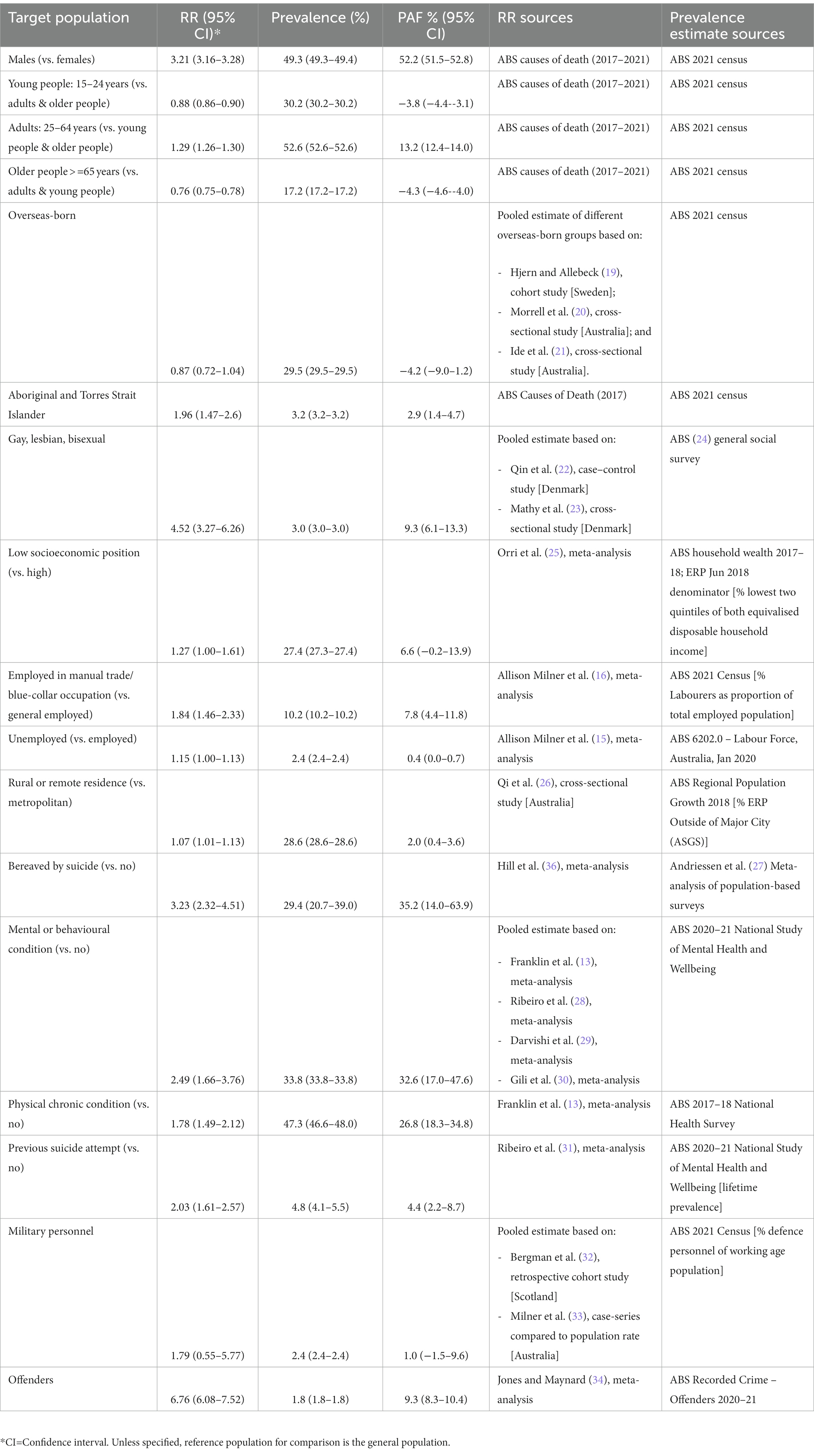
Table 1. Target populations for suicide prevention in Australia: relative risk (RR), prevalence in the population, and population attributable fraction.
Population proportion estimates for target populations
We ascertained estimates of the proportional representation of most of the target populations within the Australian population from the 2016 ABS Census data. We used specific sources (predominantly national surveys and registries) to determine the proportional representation of the following target groups: people with a chronic physical health condition and people currently managing via treatment or medication a mental health or behavioural condition (37), offender populations (38), LGB populations (24), current and ex-serving military personnel (39), people with a previous suicide attempt (37), and people bereaved by suicide (27) (Table 1). It is important to note that comparisons between PAF estimates can only be made for target groups from the same source population (i.e., with the same population denominator in the PAF calculation).
Statistical analysis
Where no meta-analysis was identified for a given target population, we pooled the relative risk of suicide from population-based studies using a series of random effects meta-analyses. No meta-analysis was conducted for target populations where only a single effect size was identified. We then calculated PAF estimates for each target population using the single or pooled relative risk estimate and the estimated population proportion for each target population. We conducted meta-analyses in Stata (version 15.1), using the “metan” function to pool risk estimates. Monte-Carlo simulation models using Ersatz Software 1.35 (40) were used to estimate the 95% confidence intervals for PAF estimates, to account for the uncertainty around relative risk and population proportion estimates. These simulations allowed for multiple re-calculation of PAF estimates taken from randomly drawn values from the distributions defined for relative risk and proportion estimates. We used a beta probability distribution for population proportion estimates using the ErBeta function, and a normal distribution (for the natural logarithm of the relative risk) was used for relative risk estimates using the ErRelativeRisk function, to estimate 95% confidence intervals for PAF estimates after 10,000 iterations to ensure convergence of model outcomes.
Results
Large PAF estimates for suicide in Australia were associated with men (52.2%, 95% CI 51.5%–52.8%), people bereaved by suicide (35.2%, 95%CI 14.0%–63.9%), people with a mental health or behavioural condition (32.6%, 95%CI 17.0%–47.6%), people with a chronic physical condition (26.8%, 95%CI 18.3%–34.8%), adults aged 25–64 years (13.2%, 95%CI 12.4%–14.0%), LGB populations (9.3%, 95%CI 6.1%–13.3%), offenders (9.3%, 95%CI 8.3%–10.4%), and people employed in blue collar occupations (7.8%, 95%CI 4.4%–11.8%) (Table 1). PAF estimates of 4.4% were estimated for people with a previous suicide attempt (95%CI 2.2%–8.7%) and 2.9% for Aboriginal and Torres Strait Islander populations (95%CI, 1.4%–4.7%) (Table 1).
Discussion
The PAF is an objective and parsimonious metric to help guide policy decision-making, alongside other important inputs and considerations, such as stakeholder consultations, dynamic simulation modelling, equity criteria, and cost-effectiveness (41). The PAF estimates from the current study indicated sizable reductions in the overall Australian suicide rate if suicide risk is comprehensively addressed among men, people bereaved by suicide, people with a mental health or behavioural condition, people with a chronic physical condition, and the adult population. PAF estimates also indicated considerable reductions in suicide could be achieved if effective approaches were delivered for LGB populations, offenders, and people employed in blue collar occupations. The high PAF estimates of these populations indicate the need for the development and evaluation of targeted interventions.
Given the PAF is often applied to modifiable risk factors, evidence for most of the identified (largely static) populations is scarce. However, results for people with a mental or behavioural condition were consistent with a recent systematic review of psychiatric disorder and suicide mortality which estimated a PAF of 21% (8). PAF estimates for suicide associated with blue-collar occupation have been previously shown to be higher in males (33%) than females (7%) (5). Due to insufficient statistical power, it was not possible to conduct sex-stratified analyses, however, the lower overall PAF estimate for suicide associated with blue-collar occupations in the current study (8%) may be explained by the low proportional representation of blue-collar occupations in the Australian working population. In addition, the low overall PAF estimate for suicide associated with unemployment was consistent with previous studies which range between 2% for females to 4% for males (5). Further research is needed among other sub-populations to confirm the findings. It is also important to note that these groups are not necessarily mutually exclusive and are likely to also comprise those with mental or behavioural conditions and diverse socio-demographic groups (for example in terms of migrant status and other markers of socio-economic status).
Evidence is still emerging for interventions for the whole population, and very few studies have been conducted to determine whether certain interventions are differentially effective for particular groups (42, 43). In many other areas of health (e.g., heart disease), PAF estimates assume that a particular risk factor (e.g., smoking) is eliminated from the population. In the current study, where the risk factor is a specific target population, this assumption is clearly not appropriate; but we do want to address and mitigate the factors that place these populations at greater risk. If we can do this, considerable reductions in suicide may be made. As an example, the high PAF of 52% highlights the need to explore factors that place men at greater risk. A 2019 scoping review of suicide prevention strategies for men highlighted the importance of reframing help-seeking as masculine, offering support in informal settings by trusted individuals, and providing emotional regulation techniques (44).
Although PAFs are one input into policy decision-making, they represent a metric that should serve as an adjunct to other important considerations, including health inequities. Aboriginal and Torres Strait Islander people, despite representing a small proportion of the total Australian population (3%) and thus a having relatively small PAF, are twice as likely to die by suicide compared to the general population (45). There is a clear need to prioritise and tailor culturally appropriate suicide prevention research and resources for this population (46). Similarly, although young people have a relatively low PAF, they are disproportionately represented in hospital admissions for self-harm (47), indicating the importance of early intervention.
Limitations
There are important methodological limitations that should be considered when interpreting the results. First, although the search strategy for relative risk estimates identified key meta-analyses and population-based studies, we did not conduct systematic reviews of individual studies relevant to each target population. It is possible that some key studies may have been missed which could have potentially biased the relative risk estimate used in calculating a given PAF. In addition, no formal quality assessment of the studies was conducted, therefore, sources of bias and confounding may affect the risk estimates used. Furthermore, the underlying population proportion estimate used to calculate the PAF is likely under-enumerated for some target populations (e.g., LGB groups and people with a previous suicide attempt), due to stigma and poor surveillance (48, 49). Additionally, although comparisons can be theoretically made between PAF estimates for target groups from the same source population (i.e., same population denominator in the PAF calculation), caution should be exercised. PAF estimates assume that relative risk and prevalence estimates are not affected by sources of bias or confounding, that exposure variables are independent, and relationships between exposures and outcomes are unidirectional, linear, and constant through time (6, 7, 50). These assumptions are difficult to uphold given the multifactorial nature of suicide risk, the likelihood that risk distributions will change over time, and the intersection and overlap of multiple exposures and identities across the target populations. Despite these limitations, PAF estimates can serve as an adjunct to other priority-setting exercises and an initial starting point prior to more sophisticated considerations.
Conclusions and implications for public health
PAF estimates are one means of informing suicide prevention efforts and can augment other important inputs that are used in policy decision-making. Findings from the current study suggest that addressing determinants of suicide among men, people bereaved by suicide, people with a mental health or behavioural condition, people with a chronic physical condition, the adult population, LGB population, offenders, and people employed in a manual trade may contribute substantially to reductions in the overall suicide rate in Australia.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
PB: Conceptualization, Data curation, Formal analysis, Methodology, Writing – original draft, Writing – review & editing. AP: Conceptualization, Data curation, Formal analysis, Methodology, Writing – review & editing. LR: Conceptualization, Funding acquisition, Methodology, Supervision, Writing – review & editing. KK: Writing – review & editing. KA: Writing – review & editing. MS: Writing – review & editing. AF: Writing – review & editing. LL: Writing – review & editing. CM: Writing – review & editing. JP: Conceptualization, Funding acquisition, Methodology, Supervision, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was conducted in the context of the LIFEWAYS Project, which is funded by the Australian Government Department of Health. The funder had no role in the study design, data collection, analysis and interpretation of the data, writing and decision to submit the article for publication. JP is supported by NHMRC Investigator and Partnership Project Grants (1173126, 1191874). KA is supported by a National Health and Medical Research Council (NHMRC) Early Career Fellowship (1157796) and an Early Career Researcher Grant of The University of Melbourne (ECR1202020). LL was supported by the Alfred Deakin Postdoctoral Research Fellowship 2021–2022.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Australian Bureau of Statistics. (2021). Intentional self-harm deaths (suicide) in Australia. In Causes of Death, Australia. Available at: https://www.abs.gov.au/statistics/health/causes-death/causes-death-australia/2020#intentional-self-harm-deaths-suicide-in-australia
2. Jorm, AF. Lack of impact of past efforts to prevent suicide in Australia: please explain. Aust N Z J Psychiatry. (2019) 53:379–80. doi: 10.1177/0004867419838053
3. Australian Government Department of Health. (2020). National suicide prevention adviser final advice. Available at: https://www.health.gov.au/resources/publications/national-suicide-prevention-adviser-final-advice
4. Krysinska, K, and Martin, G. The struggle to prevent and evaluate: application of population attributable risk and preventive fraction to suicide prevention research. Suicide Life Threat Behav. (2009) 39:548–57. doi: 10.1521/suli.2009.39.5.548
5. Li, Z, Page, A, Martin, G, and Taylor, R. Attributable risk of psychiatric and socio-economic factors for suicide from individual-level, population-based studies: a systematic review. Soc Sci Med. (2011) 72:608–16. doi: 10.1016/j.socscimed.2010.11.008
6. Eide, GE. Attributable fractions for partitioning risk and evaluating disease prevention: a practical guide. Clin Respir J. (2008) 2:92–103. doi: 10.1111/j.1752-699X.2008.00091.x
7. Page, A, Atkinson, J-A, Heffernan, M, McDonnell, G, Prodan, A, Osgood, N, et al. Static metrics of impact for a dynamic problem: the need for smarter tools to guide suicide prevention planning and investment. Aust N Z J Psychiatry. (2018) 52:660–7. doi: 10.1177/0004867417752866
8. Too, LS, Spittal, MJ, Bugeja, L, Reifels, L, Butterworth, P, and Pirkis, J. The association between mental disorders and suicide: a systematic review and meta-analysis of record linkage studies. J Affect Disord. (2019) 259:302–13. doi: 10.1016/j.jad.2019.08.054
9. Tsoh, J, Chiu, HF, Duberstein, PR, Chan, SS, Chi, I, Yip, PS, et al. Attempted suicide in elderly Chinese persons: a multi-group, controlled study. Am J Geriatr Psychiatry. (2005) 13:562–71. doi: 10.1097/00019442-200507000-00004
10. Kapur, N, Cooper, J, King-Hele, S, Webb, R, Lawlor, M, Rodway, C, et al. The repetition of suicidal behavior: a multicenter cohort study. J Clin Psychiatry. (2006) 67:1599–609. doi: 10.4088/JCP.v67n1016
11. Reifels, L, Ftanou, M, Krysinska, K, Machlin, A, Robinson, J, and Pirkis, J. Research priorities in suicide prevention: review of Australian research from 2010–2017 highlights continued need for intervention research. Int J Environ Res Public Health. (2018) 15:807. doi: 10.3390/ijerph15040807
12. Schlichthorst, M, Reifels, L, Krysinska, K, Ftanou, M, Machlin, A, Robinson, J, et al. Trends in suicide-related research in Australia. Int J Ment Health Syst. (2020) 14:2. doi: 10.1186/s13033-019-0335-2
13. Franklin, JC, Ribeiro, JD, Fox, KR, Bentley, KH, Kleiman, EM, Huang, X, et al. Risk factors for suicidal thoughts and behaviors: a meta-analysis of 50 years of research. Psychol Bull. (2017) 143:187–232. doi: 10.1037/bul0000084
14. Klingelschmidt, J, Milner, A, Khireddine-Medouni, I, Witt, K, Alexopoulos, EC, Toivanen, S, et al. Suicide among agricultural, forestry, and fishery workers: a systematic literature review and meta-analysis. Scand J Work Environ Health. (2018) 44:3–15. doi: 10.5271/sjweh.3682
15. Milner, A, Page, A, and Lamontagne, AD. Cause and effect in studies on unemployment, mental health and suicide: a meta-analytic and conceptual review. Psychol Med. (2014) 44:909–17. doi: 10.1017/S0033291713001621
16. Milner, A, Spittal, MJ, Pirkis, J, and LaMontagne, AD. Suicide by occupation: systematic review and meta-analysis. Br J Psychiatry. (2013) 203:409–16. doi: 10.1192/bjp.bp.113.128405
17. ABS. (2016). Statistics by topic: occupation. Available at: https://www.abs.gov.au/ausstats/abs@.nsf/ViewContent?readform&view=ProductsbyTopic&Action=Expand&Num=5.9.12
18. ABS. (2016). Australian statistical geography standard (ASGS). Available at: https://www.abs.gov.au/websitedbs/d3310114.nsf/home/australian+statistical+geography+standard+(asgs)
19. Hjern, A, and Allebeck, P. Suicide in first-and second-generation immigrants in Sweden a comparative study. Soc Psychiatry Psychiatr Epidemiol. (2002) 37:423–9. doi: 10.1007/s00127-002-0564-5
20. Morrell, S, Taylor, R, Slaytor, E, and Ford, P. Urban and rural suicide differentials in migrants and the Australian-born, New South Wales, Australia 1985–1994. Soc Sci Med. (1999) 49:81–91. doi: 10.1016/S0277-9536(99)00083-0
21. Ide, N, Kolves, K, Cassaniti, M, and De Leo, D. Suicide of first-generation immigrants in Australia, 1974–2006. Soc Psychiatry Psychiatr Epidemiol. (2012) 47:1917–27. doi: 10.1007/s00127-012-0499-4
22. Qin, P, Agerbo, E, and Mortensen, PB. Suicide risk in relation to socioeconomic, demographic, psychiatric, and familial factors: a national register–based study of all suicides in Denmark, 1981–1997. Am J Psychiatr. (2003) 160:765–72. doi: 10.1176/appi.ajp.160.4.765
23. Mathy, RM, Cochran, SD, Olsen, J, and Mays, VM. The association between relationship markers of sexual orientation and suicide: Denmark, 1990–2001. Soc Psychiatry Psychiatr Epidemiol. (2011) 46:111–7. doi: 10.1007/s00127-009-0177-3
25. Orri, M, Gunnell, D, Richard-Devantoy, S, Bolanis, D, Boruff, J, Turecki, G, et al. In-utero and perinatal influences on suicide risk: a systematic review and meta-analysis. Lancet Psychiatry. (2019) 6:477–92. doi: 10.1016/S2215-0366(19)30077-X
26. Qi, X, Hu, W, Mengersen, K, and Tong, S. Socio-environmental drivers and suicide in Australia: Bayesian spatial analysis. BMC Public Health. (2014) 14:681. doi: 10.1186/1471-2458-14-681
27. Andriessen, K, Rahman, B, Draper, B, Dudley, M, and Mitchell, PB. Prevalence of exposure to suicide: a meta-analysis of population-based studies. J Psychiatr Res. (2017) 88:113–20. doi: 10.1016/j.jpsychires.2017.01.017
28. Ribeiro, JD, Huang, X, Fox, KR, and Franklin, JC. Depression and hopelessness as risk factors for suicide ideation, attempts and death: Meta-analysis of longitudinal studies. Br J Psychiatry. (2018) 212:279–86. doi: 10.1192/bjp.2018.27
29. Darvishi, N, Farhadi, M, Haghtalab, T, and Poorolajal, J. Alcohol-related risk of suicidal ideation, suicide attempt, and completed suicide: a meta-analysis. PLoS One. (2015) 10:e0126870. doi: 10.1371/journal.pone.0126870
30. Gili, M, Castellví, P, Vives, M, de la Torre-Luque, A, Almenara, J, Blasco, MJ, et al. Mental disorders as risk factors for suicidal behavior in young people: a meta-analysis and systematic review of longitudinal studies. J Affect Disord. (2019) 245:152–62. doi: 10.1016/j.jad.2018.10.115
31. Ribeiro, J, Franklin, J, Fox, KR, Bentley, K, Kleiman, EM, Chang, B, et al. Self-injurious thoughts and behaviors as risk factors for future suicide ideation, attempts, and death: a meta-analysis of longitudinal studies. Psychol Med. (2016) 46:225–36. doi: 10.1017/S0033291715001804
32. Bergman, B, Mackay, D, Smith, D, and Pell, J. Suicide in Scottish military veterans: a 30-year retrospective cohort study. Occup Med. (2017) 67:350–5. doi: 10.1093/occmed/kqx047
33. Milner, A, Witt, K, Maheen, H, and LaMontagne, AD. Suicide among emergency and protective service workers: a retrospective mortality study in Australia, 2001 to 2012. Work. (2017) 57:281–7. doi: 10.3233/WOR-172554
34. Jones, D, and Maynard, A. Suicide in recently released prisoners: a systematic review. Ment Health Pract. (2013) 17:20–7. doi: 10.7748/mhp2013.11.17.3.20.e846
35. Australian Bureau of Statistics. (2020). Causes of death. Available at: https://www.abs.gov.au/statistics/health/causes-death/causes-death-australia/2019#intentional-self-harm-suicides-key-characteristics
36. Hill, NTM, Robinson, J, Pirkis, J, Andriessen, K, Krysinska, K, Payne, A, et al. (2020). Association of suicidal behavior with exposure to suicide and suicide attempt: a systematic review and multilevel meta-analysis. PLoS Med. (2016) 17:e1003074. doi: 10.1371/journal.pmed.100307
37. ABS. (2020). National Study of mental health and wellbeing. Available at: https://www.abs.gov.au/statistics/health/mental-health/national-study-mental-health-and-wellbeing/latest-release
38. ABS. (2021-22). Recorded crime – offenders. Available at: https://www.abs.gov.au/statistics/people/crime-and-justice/recorded-crime-offenders/latest-release
39. Australian Bureau of Statistics. (2021). Population: census. Available at: https://www.abs.gov.au/statistics/people/population/population-census/latest-release
41. Chalkidou, K, Glassman, A, Marten, R, Vega, J, Teerawattananon, Y, Tritasavit, N, et al. Priority-setting for achieving universal health coverage. Bull World Health Organ. (2016) 94:462–7. doi: 10.2471/BLT.15.155721
42. Mann, JJ, Michel, CA, and Auerbach, RP. Improving suicide prevention through evidence-based strategies: a systematic review. Am J Psychiatr. (2021) 178:611–24. doi: 10.1176/appi.ajp.2020.20060864
43. Zalsman, G, Hawton, K, Wasserman, D, van Heeringen, K, Arensman, E, Sarchiapone, M, et al. Suicide prevention strategies revisited: 10-year systematic review. Lancet Psychiatry. (2016) 3:646–59. doi: 10.1016/S2215-0366(16)30030-X
44. Struszczyk, S, Galdas, PM, and Tiffin, PA. Men and suicide prevention: a scoping review. J Ment Health. (2019) 28:80–8. doi: 10.1080/09638237.2017.1370638
45. ABS. (2018). Cause of death. Available at: https://www.abs.gov.au/statistics/health/causes-death/causes-death-australia/2018#leading-causes-of-death-in-aboriginal-and-torres-strait-islander-people
46. Dudgeon, P, Calma, T, and Holland, C. The context and causes of the suicide of indigenous people in Australia. J Indig Wellbeing. (2017) 2:5–15.
47. CEE. (2019). Health stats NSW: intentional self-harm hospitalisations. Available at: www.healthstats.nsw.gov.au. Accessed 15 April 2020.
48. Hawton, K, Saunders, KE, and O'Connor, RC. Self-harm and suicide in adolescents. Lancet. (2012) 379:2373–82. doi: 10.1016/S0140-6736(12)60322-5
49. Patterson, JG, Jabson, JM, and Bowen, DJ. Measuring sexual and gender minority populations in health surveillance. LGBT Health. (2017) 4:82–105. doi: 10.1089/lgbt.2016.0026
Keywords: population attributable fraction, population attributable risk, suicide, suicide prevention, Australia
Citation: Bandara P, Page A, Reifels L, Krysinska K, Andriessen K, Schlichthorst M, Flego A, Le LK-D, Mihalopoulos C and Pirkis J (2024) Attributable risk of suicide for populations in Australia. Front. Psychiatry. 14:1285542. doi: 10.3389/fpsyt.2023.1285542
Edited by:
Shannon Lange, University of Toronto, CanadaReviewed by:
György Purebl, Semmelweis University, HungaryAlessandra Costanza, University of Geneva, Switzerland
David Benrimoh, McGill University, Canada
Copyright © 2024 Bandara, Page, Reifels, Krysinska, Andriessen, Schlichthorst, Flego, Le, Mihalopoulos and Pirkis. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lennart Reifels, bC5yZWlmZWxzQHVuaW1lbGIuZWR1LmF1