 Alan L. Peterson1,2,3*
Alan L. Peterson1,2,3* Brian A. Moore4Wyatt R. Evans5,6
Brian A. Moore4Wyatt R. Evans5,6 Stacey Young-McCaughan1,2Abby E. Blankenship1†Casey L. Straud1,3Christopher S. McLean7Tashina L. Miller7Eric C. Meyer8 and
Stacey Young-McCaughan1,2Abby E. Blankenship1†Casey L. Straud1,3Christopher S. McLean7Tashina L. Miller7Eric C. Meyer8 and  for the STRONG STAR Consortium
for the STRONG STAR Consortium- 1Department of Psychiatry and Behavioral Sciences, University of Texas Health Science Center at San Antonio, San Antonio, TX, United States
- 2Research and Development Service, South Texas Veterans Health Care System, San Antonio, TX, United States
- 3Department of Psychology, University of Texas at San Antonio, San Antonio, TX, United States
- 4Department of Psychological Science, Kennesaw State University, Kennesaw, GA, United States
- 5VA North Texas Health Care System, Dallas, TX, United States
- 6Department of Psychiatry, University of Texas Southwestern Medical Center, Dallas, TX, United States
- 73rd Security Force Assistance Brigade, Fort Cavazos, TX, United States
- 8Department of Counseling and Behavioral Health, University of Pittsburgh, Pittsburgh, PA, United States
Background: Enhancing resiliency and optimizing readiness in military personnel is a high priority for the U.S. Department of Defense. Most military resiliency-enhancement programs are evidence-informed interventions. However, few randomized studies have demonstrated efficacy of any intervention or training program to enhance resiliency and prevent the development of psychological health symptoms in military personnel when exposed to operational stressors. This manuscript provides an overview of the theoretical foundation, research design, and research methods of a preventive intervention trial designed to evaluate the efficacy of a training program to enhance resiliency and prevent psychological health symptoms in military personnel. The resiliency training intervention is based on Acceptance and Commitment Therapy (ACT), an evidence-based intervention with broad empirical support for improving functioning in those living with psychological and medical conditions.
Method/design: This study will evaluate the efficacy of a two-day training program based on ACT for fostering psychological flexibility, the central target in ACT, for enhancing resiliency, and for preventing the development of psychological health symptoms. The research participants will be a non-clinical population of active duty military personnel (N = 600). The ACT-based training program (n = 300) will be compared to a military resiliency training as usual, known as Master Resilience Training (n = 300). Assessment measures will be administered at the baseline assessment, after training, prior to a military deployment, and after returning from a deployment. Qualitative interviews will be conducted to provide feedback on the training program.
Clinical Trial Registration: NCT05094115.
1 Introduction
Maintaining health, optimizing performance, and enhancing resiliency to occupational stressors in military personnel who are frequently exposed to austere environments and trauma is a significant challenge. The Department of Defense has invested significant resources to develop and evaluate programs to enhance resiliency, optimize operational readiness, and prevent deployment-related psychological health casualties in military personnel (1). A limited amount of previous literature has shown positive effects of self-reflection on the subsequent development of mental health symptoms in Australian military cadets (2, 3) and on posttraumatic stress symptoms following a debriefing intervention among recently deployed U.S. soldiers (4). These studies highlight the importance of using a valid control group, as well as the importance of implementing interventions to prevent or mitigate the development of psychological health symptoms in military personnel when exposed to occupational or operational stressors. Most military resiliency-enhancement programs, such as the U.S. Army’s Comprehensive Soldier Fitness Program, are evidence-informed interventions that are implemented as population health programs (5, 6). Indeed, the effectiveness of the Comprehensive Soldier Fitness Program, which is the Army’s current resiliency-enhancement program of record, has not been supported based on the results of controlled trials (7).
There are several reasons for the lack of rigorous (i.e., prospective, randomized controlled) resiliency-enhancement trials in U.S. military populations. First, scientifically evaluating the potential efficacy of a resiliency-enhancement training program requires a prospective study in which military personnel are randomized to different arms of a controlled intervention trial, which can be difficult in the contemporary operating environment. Second, various groups of military personnel might be ideal populations to study, but with each presenting with unique challenges. For example, one population might be new military recruits who are enrolled, randomized, trained, and evaluated as they complete basic military training, a demanding and highly stressful environment (8). Another population might be military special forces trainees who are about to start a training program, such as the U.S. Navy’s Basic Underwater Demolition/Sea, Air, and Land Teams (SEALs) course, which has been found to have a washout or dropout rate of about 80% (9, 10). Such intense training programs would provide a proxy for a high-stress environment that might be encountered during a deployment. However, most military trainees are considered protected populations, and their training programs are part of established training curricula that require high levels of military coordination and approval to modify for the purpose of conducting research. A final group who might be ideal to study are individuals who are scheduled to deploy to a high-risk/high-threat environment. However, designing and obtaining research regulatory review approval for a prospective study such as this would be extremely difficult, especially with the discontinuation of U.S. military combat deployments in support of Operation Iraqi Freedom in 2010 and Operation Enduring Freedom in 2014 (11). A rigorous schedule of deployment preparation activities makes adding something such as supplemental resilience training a challenge.
The current manuscript is a description of the methods for a research project funded through the U.S. Department of Defense’s Military Operational Medicine Research Program’s Resilience and Readiness Optimization/Enhancement (R2OE) Translational Research Award (W81XWH1910628; PI: Alan Peterson). The aim of the project is to conduct a randomized controlled trial evaluating the efficacy of psychological flexibility training based on Acceptance and Commitment Training to enhance resiliency in military personnel.
1.1 Acceptance and commitment therapy and acceptance and commitment training
Acceptance and Commitment Therapy (ACT; pronounced as one word) is a contemporary, evidence-based, cognitive-behavioral approach that was originally developed to improve psychological health and functioning in those experiencing psychological health challenges (12, 13). It is also a promising psychological approach for resilience enhancement in adults (14, 15). We recently described the potential of this model for fostering resilience enhancement in military personnel (16). The present grant was funded to adapt and evaluate a military-relevant psychological flexibility training intervention based on ACT to enhance resilience and optimize readiness.
There are over 1,000 published randomized controlled trials (RCTs) of ACT for improving a broad range of biopsychosocial outcomes. These RCTs span applications of ACT for depression, anxiety disorders, substance use disorders, psychosis, tobacco use, eating disorders, general well-being, and a range of medical challenges (17–24). ACT has been found to optimize functional outcomes in diverse domains including improving workplace performance under stressful conditions, completing physical exercise regimens, improving parenting skills, and adhering to dietary restrictions (15). Moreover, ACT has been found to be efficacious when delivered by individuals from different professional disciplines and in a broad range of formats including individual and group psychotherapy, brief training workshops, and online delivery. This underscores the robustness of the model and the potential for scalability (25–28). When used in a training context, ACT may be referred to as Acceptance and Commitment Training.
In ACT, the broad goal is to help individuals identify and act consistently with their personal values and goals and to align their actions with those values even if they are experiencing psychological or physical discomfort (9, 10). According to the ACT model, suffering and impairment are primarily the consequence of psychological inflexibility (i.e., inability to persist in or change behavior according to situational or contextual factors and personally chosen values due to problematic, inflexible reactions to negatively evaluated internal experiences). Psychological inflexibility may be particularly detrimental when an individual is confronted with stress or adversity (12, 13). ACT also incorporates mindfulness as a method for increasing awareness of and for promoting a nonjudgmental stance toward unwanted internal experiences, as these are key elements of fostering psychological flexibility (12). Interventions targeting increased psychological flexibility—ACT being the foremost in this field—are recommended not only for facilitating recovery after stressors but also for enhancing resilience (14, 16, 29, 30). The psychological flexibility model aligns well with the flexibility sequence model, arguably the most thoroughly researched and well supported model of the resilience process across numerous populations (31).
2 Materials and methods
2.1 Institutional review board
This project has been reviewed and approved by the Institutional Review Board (IRB) at the University of Texas Health Science Center at San Antonio (UTHSCSA; 20210486HU) as the IRB of record. The University of Pittsburgh deferred its review to UTHSCSA as part of a single IRB authorization agreement.
2.2 Design
The present RCT (N = 600) was designed to evaluate the efficacy of a novel, military-relevant, ACT-based resilience training that we refer to as Psychological Flexibility Training and that we developed for this project. The primary goal of this intervention is to enhance resiliency and optimize readiness in military personnel. For the proposed study, it is hypothesized that the ACT principles will also improve the psychological health outcomes by reducing symptoms of anxiety, depression, and posttraumatic stress disorder (PTSD) in military operational settings, as suggested by the Cochrane Database of Systematic Reviews on Psychological Interventions for Resilience Enhancement in Adults (14). We have two primary research hypotheses. First, we hypothesize that military personnel who receive psychological flexibility training will demonstrate a statistically significant increase in psychological resiliency compared to military personnel receiving training as usual over the course of the study. Second, we hypothesize that military personnel who receive Psychological Flexibility Training will demonstrate a statistically significant increase in psychological resiliency after completing a military operational deployment compared to a group of military personnel receiving military resilience training as usual. Military training as usual for the Army is Master Resilience Training, which is the resilience enhancement component of the broader Comprehensive Soldier Fitness Initiative (32). Of note, all participants receive Master Resilience Training as part of their training as usual. Thus, the current study is testing the incremental value of adding Psychological Flexibility Training.
2.2.1 Randomization
Recruited personnel will be randomized as a group to Resilience Enhancement through Acceptance and Commitment Training (REACT) or regular programming. Group randomization will be completed prior to recruitment or consent. Groups will be randomized by a randomization list generated by the research team’s Biostatistics Core. The randomization list will use random blocks of 4, 6, and 8 to ensure roughly equal numbers of groups in each condition as the study progresses and to reduce the anticipation of group assignment and thereby the potential for bias.
2.3 Participants
2.3.1 Source of population
Active duty U.S. Army soldiers assigned to Fort Cavazos (formerly Fort Hood), Texas, will be eligible to participate in the R2OE study. One unit that has already agreed to participate representing a military unit regularly scheduled to deploy to high-risk/high-threat environments is the 3rd Security Force Assistance Brigade (SFAB). SFABs are specialized Army units formed to train, advise, assist, enable, and accompany operations with allied and partner nations. They were created with the intent to reduce the burden of such operations on conventionally organized Brigade Combat Teams (BCTs), allowing BCTs to focus on fighting near-peer threats. Designed on the model of a standard infantry BCT, SFABs are composed of approximately 800 experienced senior personnel, primarily commissioned, warrant, and non-commissioned officers. They are selected from regular Army units and given additional training at the Military Advisor Training Academy at Fort Moore, Georgia. We will begin recruitment efforts with the 3rd SFAB. Should recruitment from SFABs prove insufficient, we will recruit from additional units stationed at Fort Cavazos, such as Brigade Combat Teams and other units that most closely resemble the SFABs in terms of military service characteristics.
2.4 Recruitment & randomization
Soldiers are recruited through briefings at various unit meetings as well as at the unit’s Newcomers’ Briefing held monthly. Any soldier, 18 years or older, is eligible for inclusion. There are no exclusion criteria. Participants are equally randomized between the two groups stratifying for rank to ensure equal numbers of junior non-commissioned officers (NCOs; grades E-4 to E-6), senior NCOs (grades E-7 to E-9), and officers (warrant and commissioned) are in each group. In accordance with Department of Defense (DoD) Instruction 3216.02, participants can be compensated if study participation does not adversely impact their ability to perform their assigned duties. Five assessments are scheduled. Each time an assessment is completed, $25 can be compensated, for a total of $125.
2.5 Consent
An authorized and trained member of the research team engages potential participants in an interactive explanation of the study guided by the informed consent document. Individual informed consent is obtained following recruitment briefings or at another time when a member of the research team can meet with interested individuals. Soldiers who are not interested in participating in the study continue with unit training as usual.
2.6 Measures
Ideally, resiliency enhancement training for military personnel demonstrates not only improvements in self-reported resiliency and other related constructs but also demonstrates positive adaptation in the face of significant stress or adversity as a result of the training (33). Related to this, the present study examines a range of resilience-related constructs (i.e., dispositional recovery, stress response, and grit) and correlates (dysfunctional cognitions, depression, and anxiety). Given our theoretical approach, we anticipate that resilience-related outcomes would be associated with increased psychological flexibility (16). The schedule of assessments is outlined in Table 1. A brief description of each measure is provided below. A more detailed description of each measure including information on validity and reliability of each measure is included in Supplement 1. Administered assessments address the constructs of psychological resilience, trait resilience, psychological flexibility, self-efficacy, mindset, life satisfaction, psychological health, unit cohesion, family functioning, and evaluation and feedback about the training (see Table 1).
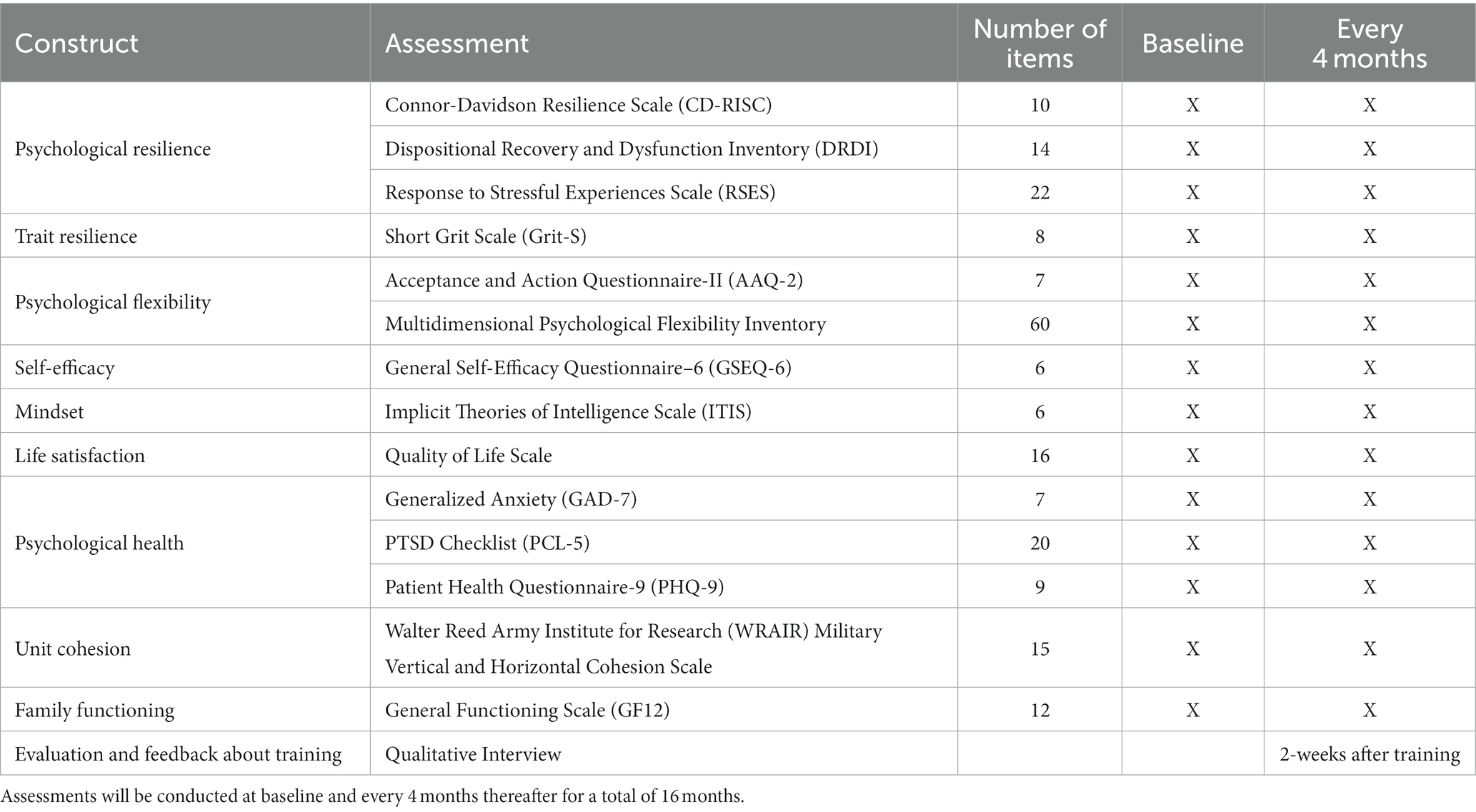
Table 1. Schedule of assessments involved in the Resilience and Readiness Optimization/Enhancement (R2OE) study.
2.6.1 Measures of psychological resilience
2.6.1.1 Connor-Davidson resilience scale
The CD-RISC (34, 35) is a 25-item questionnaire examining attitudes toward coping with adversity. The shorter, 10-item questionnaire is being administered for this study. The CD-RISC is the primary outcome measure for this study.
2.6.1.2 Dispositional recovery and dysfunction inventory
The DRDI (36) is a 14-item measure comprised of two subscales (recovery and dysfunctional cognitions). Participants rate themselves concerning their perception of themselves on a Likert scale of 1 (not at all characteristic of me) to 7 (entirely characteristic of me).
2.6.1.3 Response to stressful experiences scale
The RSES (37) is a 22-item questionnaire that asks participants to assess how well each statement describes them, both during and after stressful events in their lives.
2.6.2 Measure of trait resilience
2.6.2.1 Short grit scale (Grit-S)
The Grit-S (38) is an eight-item grit scale that examines trait-level perseverance and passion for long-term goals. Participants are asked to rate themselves on items such as “My interests change from year to year” or “I am a hard worker” on a Likert scale ranging from “not at all like me” to “very much like me.”
2.6.3 Measures of psychological flexibility
2.6.3.1 Acceptance and action questionnaire-II
The AAQ-II (39) is a seven-item measure of experiential avoidance and psychological inflexibility. Participants are asked to rate themselves on items such as “Emotions cause problems in my life” on a Likert scale of 1 (never true) to 7 (always true).
2.6.3.2 Multidimensional psychological flexibility inventory
The MPFI (40) is a 60-item measure of the six core processes underlying the ACT psychological flexibility model. Each core process is rated in terms of both flexibility and inflexibility. For each of the six core processes, there are six items reflecting flexibility (acceptance, present moment awareness, self-as-context, cognitive defusion, values, and committed action) and six items reflecting inflexibility (experiential avoidance, lack of contact with the present moment, self-as-content, cognitive fusion, lack of contact with values, and inaction).
2.6.4 Measure of self-efficacy
2.6.4.1 General self-efficacy questionnaire–6
The GSEQ-6 (41) is a six-item, self-report measure that assesses general self-efficacy as related to an individual’s ability to adapt to stressful events.
2.6.5 Measure of mindset
2.6.5.1 Implicit theories of intelligence scale
The Dweck ITIS (42, 43) is a six-item, self-report scale examining individual fixed/growth mindsets concerning intelligence. Participants are asked about their agreement on a 6-point Likert scale from 1 (strongly agree) to 6 (strongly disagree) to items such as, “You have a certain amount of intelligence, and you really cannot do much to change it.”
2.6.6 Measure of life satisfaction
2.6.6.1 Quality of life scale
The QOLS (44) is a 16-item, self-report measure of life satisfaction during the past year in 16 life domains, including health, participation in community and relationships, and creative expression. Items are rated on a scale from 1 (delighted) to 7 (terrible).
2.6.7 Measures of psychological health
2.6.7.1 Generalized anxiety disorder-7 scale
The GAD-7 (45) is a seven-item measure that asks participants to rate the frequency with which they have been bothered by anxiety symptoms within the past 2 weeks on a scale ranging from 0 (not at all) to 3 (nearly every day).
2.6.7.2 PTSD checklist for DSM-5
The PCL-5 (46) is a 20-item, self-report measure of PTSD symptoms, with higher scores reflecting greater PTSD severity. Scoring is based on how much the patient has been bothered by the symptoms in the past month on a scale from 0 (not at all) to 4 (extremely).
2.6.7.3 Patient health questionnaire-9
The PHQ-9 is a widely used and well-validated measure of depressive symptoms (47, 48). It consists of nine items that correspond to the DSM diagnostic criteria for major depressive disorder. Respondents rate the frequency with which they have been bothered by depressive symptoms within the past 2 weeks. Respondents also indicate the degree to which their depressive symptoms have made it difficult for them to do their work, take care of things at home, or get along with other people.
2.6.8 Measure of unit cohesion
2.6.8.1 Walter reed army institute of research (WRAIR) horizontal and vertical cohesion
The WRAIR cohesion scales (49, 50) are the established method of evaluating attitudes about support from peers (horizontal) and leaders (vertical). Horizontal cohesion is assessed using three items, and vertical cohesion is assessed using 13 items. Participant agreement to these 16 statements is rated on a 5-point scale (1 = “strongly disagree” to 5 = “strongly agree”). Individuals answer the questionnaire for their current unit.
2.6.9 Measure of family functioning
2.6.9.1 General functioning 12-item subscale (GF12) of the McMaster family assessment device (FAD)
The GF12 is a 12-item, self-report measure that is a subscale of the FAD (51, 52) designed to assess family functioning. The GF12 subscale includes six items assessing healthy family functioning and six items assessing unhealthy family functioning. Participants are asked about their agreement on a 4-point Likert scale from “strongly agree” to “strongly disagree” to items such as “Planning family activities is difficult because we misunderstand each other” and “In times of crisis we can turn to each other for support.”
2.6.10 Evaluation and feedback about training
2.6.10.1 Qualitative interview
Focus groups will be semi-structured interviews conducted approximately 2 weeks after the training. These groups are designed to assess participants’ perceptions of the training and to solicit recommendations for future training modifications. Qualitative data collected during the focus groups will be recorded and analyzed using a method like that described in the 2015 New Hampshire Medicaid Management Focus Groups (53). Notes and recordings will be transcribed and analyzed for common themes.
2.7 Data analytic plan
The primary outcome to address study aims is the change score difference between group (psychological flexibility vs. treatment as usual) on the Connor-Davidson Resilience Scale (CD-RISC) over time. Analyses will be intent-to-treat using data from all randomized participants regardless of the extent of participation. The statistical analysis model is a mixed-effects regression with repeated measures using all assessment time points. Advantages of likelihood-based regression models over conventional ANOVA include the ability to use data from all participants even if they only have baseline data, relaxation of the assumption of equal variances, specification of data distributions other than normal, and the ability to analyze longitudinal data in the presence of missing data. Models will include the fixed effects of group, time, and the respective two-way interaction. Deployment history will also be entered into models as a covariate. Random intercepts and slopes will be tested, and covariance structure selection will be based on likelihood criteria model comparisons (e.g., Akaike’s Information Criteria). Little’s (1988) missing completely at random test and regression-based sensitivity analyses will be used to investigate the nature of missingness and the appropriateness of likelihood-based modeling (54). We will also derive and report on minimally important difference metrics on the CD-RISC (55, 56). Supplementary analyses of the other measures will use the same statistical analysis design. We will report on minimally important change and reliable change indices for the Posttraumatic Stress Disorder Checklist-5 (PCL-5), for which these metrics have been established (55, 57). We will assess deployment history at all time-points and will use this as a covariate in all pre-post analyses. All tests will be two-tailed with unadjusted p = 0.05. Analyses will be done using the LME4 package using R statistical software.
2.7.1 Power analysis
Statistical power estimates were obtained from the PASS15 software (NCSS, 2017) modules for comparison of two means or two proportions in a cluster randomized design. Estimates were obtained for a range of standardized mean differences (Cohen’s d) from 0.35 to 0.50, which range from modest (d = 0.35) to medium in size (d = 0.50). Effect sizes below 0.35 are unlikely to be clinically significant and d = 0.50 is often considered to be a threshold for a meaningful difference. We also estimated the reduction in Failure % that was detectable at 0.80 assuming a base rate of 80%. We specified a total of 12 clusters of 50 participants for a total N = 600. The proposed sample size (N = 600) provides statistical power of at least 80% to detect a standardized mean difference (or change over time) in the “small to moderate” range (Cohen’s d of 0.30). This applies not only to analyses involving the entire randomized sample but also for analyses based on subsamples based on factors such as deployment, demographics, or other military service characteristics.
2.7.2 Addressing hypotheses
The first research question relates to the pre-post training effect of workshop participation. Analyses will be based on changes during the 4 months before and following the training and will analyze data from all randomized participants. The second research question relates to the effect of training on change during deployments. Analyses will use data only from deployed participants. As deployments occur at varied points in time and are variable in duration, the selection of the baseline and post-deployment assessments for these analyses will be based on the deployment dates of each participant.
2.7.3 Qualitative data analysis
Preliminary themes will be discussed among the study team. Common themes will be developed into a coding scheme. The study team will independently code the interviews using the identified coding scheme. Any differences in coding will be resolved by examining the transcripts. Participants will be invited to participate in a focus group with other participants who engaged in the same type of training (i.e., psychological flexibility training or training as usual). Focus groups will continue until data saturation has occurred and the study team is no longer identifying new themes. Data will be summarized into themes and analyzed using standard qualitative techniques.
2.8 Intervention
In coordination with unit leadership, two consecutive days of psychological flexibility training will be integrated into the military training calendar to deliver the intervention to study participants randomized to the intervention arm. The training as usual condition is the U.S. Army’s Master Resiliency Training, which is part of the Comprehensive Soldier Fitness Program (30). Master Resiliency Training is a team training program grounded in principles of positive psychology and strengths-based leadership. Identified soldiers in each unit volunteer to complete master resiliency training and then serve as consultants to units conducting their training as usual resiliency training initiatives.
2.8.1 Psychological flexibility training
Psychological Flexibility Training will be delivered as a 2-day workshop lasting approximately 8 h per day (see Table 2). Table 1 provides an overview of the topics to be covered. An additional description of these concepts as applied to resilience enhancement in the military has been published elsewhere (32). Consistent with the ACT model, experiential exercises will be integrated throughout the training. The primary goals of Day 1 are to provide an overview of the training and to describe the “posture” that prepares one to respond to challenging situations in a psychologically flexible manner. We refer to this as psychological situational awareness. These skills include (1) adopting a position of mindful awareness, (2) increasing clarity regarding one’s core values across different life domains, and (3) adopting an attitude that balances traditional military characteristics such as toughness with acceptance and willingness. This last skill helps to maximize an individual’s ability to cope across the broadest possible range of challenges and life domains and, importantly, to avoid problems associated with engaging an overly narrow or rigid set of coping skills. We also highlight differences between the psychological flexibility stance and some common or “traditional” notions of resilience within military culture. The primary goals of Day 2 are to deepen the rationale for cultivating greater psychological flexibility and to practice core skills based on the psychological flexibility model. Experiential exercises are used to highlight the long-term unworkability of control-based coping attempts (i.e., those based on avoidance and suppression). Psychological flexibility is defined in terms of combining the three elements of (1) contextual sensitivity, (2) awareness of both short and long-term consequences of a given response, and (3) developing and flexibly utilizing an arsenal of skills to meet varied situations and forms of emotional distress. Finally, a series of core psychological flexibility skills are practiced, including noticing and detaching from thoughts, engaging in willingness to experience discomfort, noticing the connection between personal values and the degree of willingness to experience discomfort, and acceptance of emotional distress.
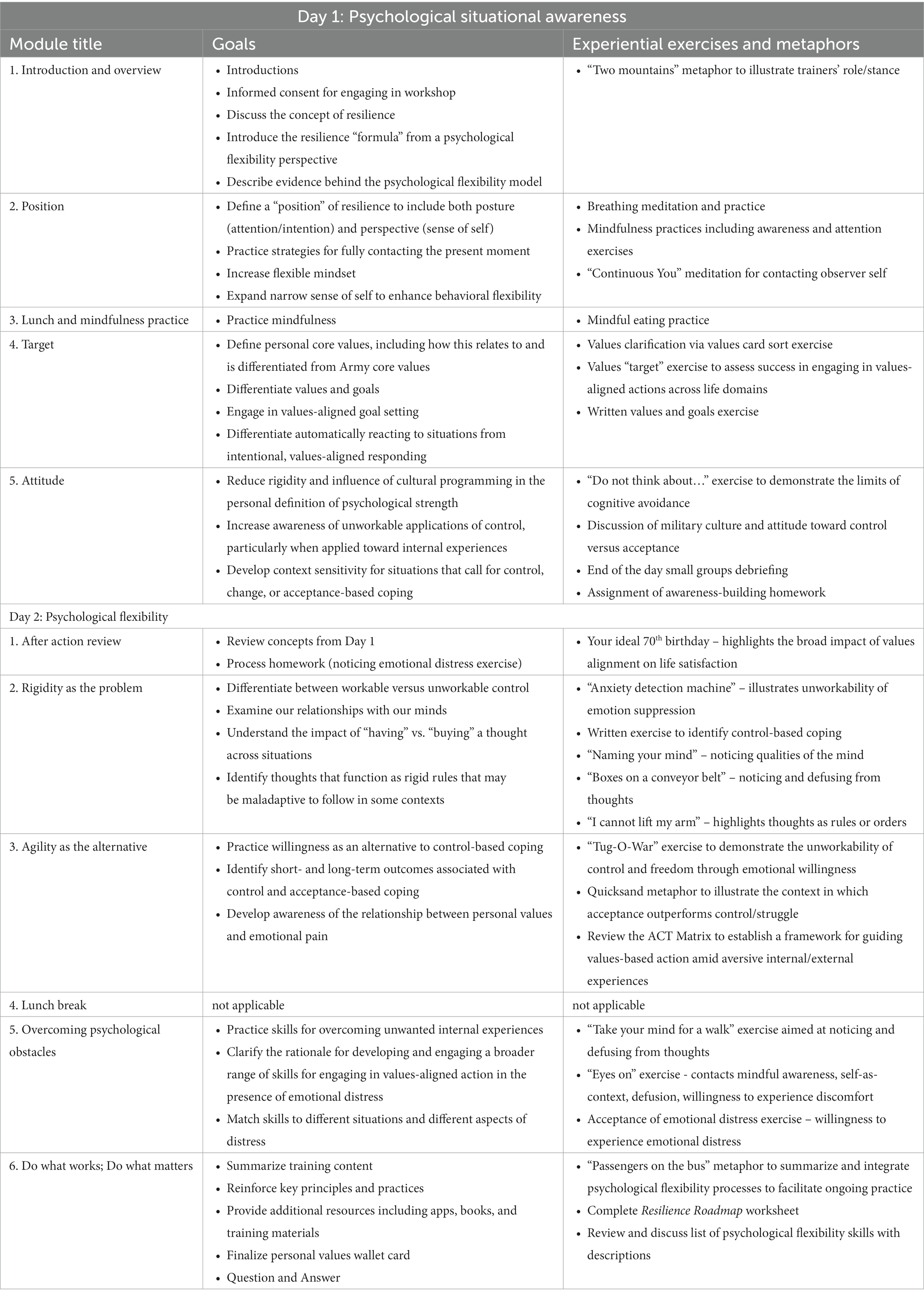
Table 2. Overview of psychological flexibility training workshop.
To promote retention and practice, participants are provided with handouts summarizing the workshop content, a wallet card that lists their core values identified during the workshop and key points from the workshop, and resources for further reading. In addition, following the workshop, four optional, 1-h booster sessions are offered via video conferencing. The booster sessions are intended to serve as training refreshers and practice/consultation sessions without introducing new content or skills. These sessions follow a standard structure: an opening experiential exercise to highlight one or more processes covered during the workshop, a brief recap of the content presented during the workshop (first booster session only), questions from attendees about applying the concepts in their lives, and responses to questions and additional comments from the facilitators to encourage the application of the concepts.
3 Conclusion
Across the DoD, there is an increasing need to train service members to meet worldwide military operational needs. Through collaboration between military leaders and civilian experts in psychological resiliency and applied military research, we believe that the project described will have potential applicability to all U.S. military branches. By combining our collective expertise, we will use the existing scientific evidence to test a culturally competent program designed to enhance resiliency and optimize readiness among active duty service members. For example, Helmreich et al. (14) examined 43 resilience enhancement RCTs and identified numerous “best practices” to implement when developing a resilience enhancement intervention, many of which are implemented herein. Specifically, they posit that a resilience enhancement intervention must describe the underlying resilience concept the intervention is based on (i.e., psychological flexibility within the ACT framework (16)), utilize an a priori sample calculation to ensure adequate power, have specified inclusion and exclusion criteria, adequate follow-up periods (herein we utilize four), and conduct a comprehensive baseline assessment. Additionally, the present study uses a detailed randomization process to reduce bias, and a comprehensive assessment battery to maximize the identification of malleable, multi-level resilience factors.
Through the recruitment of many service members (N = 600), we will be able to determine the efficacy of the R2OE training program and the extent to which it enhances resiliency and optimizes readiness in comparison to training as usual. The psychological flexibility training, if demonstrated to be effective, will have the potential for dissemination and implementation in other U.S. military units and training communities. In consideration of the potential for widespread implementation, our qualitative interviews will address factors such as motivation to participate in the training, the trainee experience during the workshop, logistical factors that could promote or impede implementation, and both personal and professional impacts of the psychological flexibility training. We view this study design as reflecting a starting point in examining this intervention approach. As such, we chose to use self-report measures of resilience and other outcomes as opposed to biological or behavioral markers, which may be viewed as a limitation of the current study.
Beyond the potential for enhanced military readiness, ACT is broadly applicable and has been demonstrated to be an efficacious intervention across a spectrum of concerns. Psychological flexibility, the central concept within this model, has been described as a fundamental aspect of health (58) any may be synonymous with resilience processes (16, 31). This literature also highlights that ACT is an acceptable intervention that is associated with high trainee satisfaction. We anticipate the present training program could have immediate applicability and benefits for people entering other high-risk occupations. For example, emergency services and medical personnel working in high-stress settings would likely benefit from enhanced psychological flexibility. Psychological flexibility training holds the potential to be a readily modifiable platform to preempt stressor exposure and provide individuals with the psychological tools needed to function effectively in the face of high levels of adversity and emotional distress.
Ethics statement
The studies involving humans were approved by University of Texas Health Science Center, San Antonio and Brooke Army Medical Center. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
AP: Conceptualization, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Writing – review & editing. BM: Investigation, Methodology, Resources, Writing – original draft. WE: Conceptualization, Funding acquisition, Investigation, Writing – review & editing. SY-M: Conceptualization, Funding acquisition, Investigation, Methodology, Project administration, Supervision, Writing – review & editing. AB: Data curation, Formal analysis, Investigation, Supervision, Writing – review & editing. CS: Writing – review & editing. CM: Investigation, Resources, Writing – review & editing. TM: Investigation, Writing – review & editing, Resources. EM: Writing – review & editing, Conceptualization, Funding acquisition, Investigation, Methodology, Project administration, Supervision.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This research is supported by the U.S. Department of Defense’s Military Operational Medicine Research Program’s Resilience and Readiness Optimization/Enhancement (R2OE) Translational Research Award (W81XWH1910628; PI: AP).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Author disclaimer
The views expressed herein are solely those of the authors and do not reflect an endorsement by or the official policy or position of the U.S. Army, the Department of Defense, the Department of Veterans Affairs, or the U.S. Government.
References
1. Peterson, AL, Cigrang, JA, and Isler, WC. Future directions: trauma, resilience, and recovery research In: SM Freeman, B Moore, and A Freeman, editors. Living and surviving in Harm's way: A psychological treatment handbook for pre-and post-deployment of military personnel. New York: Routledge (2009). 467–93.
2. Crane, MF, Boga, D, Karin, E, Gucciardi, DF, Rapport, F, Callen, J, et al. Strengthening resilience in military officer cadets: a group-randomized controlled trial of coping and emotion regulatory self-reflection training. J Consult Clin Psychol. (2019) 87:125–40. doi: 10.1037/ccp0000356
3. Falon, SL, Karin, E, Boga, D, Gucciardi, DF, Griffin, B, and Crane, MF. A clustered-randomized controlled trial of a self-reflection resilience-strengthening intervention and novel mediators. J Occup Health Psychol. (2021) 26:1–19. doi: 10.1037/ocp0000268
4. Adler, AB, Bliese, PD, McGurk, D, Hoge, CW, and Castro, CA. Battlemind debriefing and battlemind training as early interventions with soldiers returning from Iraq: randomization by platoon. J Consult Clin Psychol. (2009) 77:928–40. doi: 10.1037/a0016877
5. Meredith, LS, Sherbourne, CD, Gaillot, SJ, Hansell, L, Ritschard, HV, Parker, AM, et al. Promoting psychological resilience in the U.S. military. RAND Health Q. (2011) 1:2.
6. Steenkamp, MM, Nash, WP, and Litz, BT. Post-traumatic stress disorder: review of the comprehensive soldier fitness program. Am J Prev Med. (2013) 44:507–12. doi: 10.1016/j.amepre.2013.01.013
7. Denning, LA, Meisnere, M, and Warner, KE. Institute of Medicine of the National Academies, preventing psychological disorders in service members and their families: An assessment of programs. Washington, DC: National Academies Press (2014).
8. Jackson, S, Agius, R, Bridger, R, and Richards, P. Occupational stress and the outcome of basic military training. Occup Med. (2011) 61:253–8. doi: 10.1093/occmed/kqr036
9. Farina, EK, Thompson, LA, Knapik, JJ, Pasiakos, SM, McClung, JP, and Lieberman, HR. Physical performance, demographic, psychological, and physiological predictors of success in the U.S. Army special forces assessment and selection course. Physiol Behav. (2019) 210:112647. doi: 10.1016/j.physbeh.2019.112647
10. McDonald, DG, Norton, JP, and Hodgdon, JA. Training success in U.S. navy special forces. Aviat Space Environ Med. (1990) 61:548–54.
11. Moore, B.A., and Peterson, A.L., OEF/OIF/OI give up: making sense of U.S. military operations. ISTSS stress points. (2018). Available at: http://sherwood-istss.informz.net/admin31/content/template.asp?sid=60250&brandid=4463&uid=1044618441&mi=7495336&mfqid=39892239&ptid=&ps=60250.
12. Hayes, SC . Acceptance and commitment therapy, relational frame theory, and the third wave of behavioral and cognitive therapies. Behav Ther. (2004) 35:639–65. doi: 10.1016/S0005-7894(04)80013-3
13. Hayes, SC, Luoma, JB, Bond, FW, Masuda, A, and Lillis, J. Acceptance and commitment therapy: model, processes and outcomes. Behav Res Ther. (2006) 44:1–25. doi: 10.1016/j.brat.2005.06.006
14. Helmreich, A, Kunzler, A, Chmitorz, J, König, H, Binder, M, and Wessa, K. Lieb, psychological interventions for resilience enhancement in adults. Cochrane Database Syst Rev. (2017) 2, CD012527. doi: 10.1002/14651858.CD012527
15. Moran, DJ . Acceptance and commitment training in the workplace. Curr Opin Psychol. (2015) 2:26–31. doi: 10.1016/j.copsyc.2014.12.031
16. Evans, WR, Meyer, EC, Moore, BA, and Peterson, AL. psychological flexibility training to enhance resilience in military personnel. Mil Behav Health. (2023) 23:1–13. doi: 10.1080/21635781.2023.2246900
17. A-Tjak, JG, Davis, ML, Morina, N, Powers, MB, Smits, JA, and Emmelkamp, PM. A meta-analysis of the efficacy of acceptance and commitment therapy for clinically relevant mental and physical health problems. Psychother Psychosom. (2015) 84:30–6. doi: 10.1159/000365764
18. Di Sante, J, Akeson, B, Gossack, A, and Knäuper, B. Efficacy of ACT-based treatments for dysregulated eating behaviours: a systematic review and meta-analysis. Appetite. (2022) 171:105929. doi: 10.1016/j.appet.2022.105929
19. Du, S, Dong, J, Jin, S, Zhang, H, and Zhang, Y. Acceptance and commitment therapy for chronic pain on functioning: a systematic review of randomized controlled trials. Neurosci Biobehav Rev. (2021) 131:59–76. doi: 10.1016/j.neubiorev.2021.09.022
20. Herbert, MS, Dochat, C, Wooldridge, JS, Materna, K, Blanco, BH, Tynan, M, et al. Technology-supported acceptance and commitment therapy for chronic health conditions: a systematic review and meta-analysis. Behav Res Ther. (2022) 148:103995. doi: 10.1016/j.brat.2021.103995
21. Sakamoto, R, Ohtake, Y, Kataoka, Y, Matsuda, Y, Hata, T, Otonari, J, et al. Efficacy of acceptance and commitment therapy for people with type 2 diabetes: systematic review and meta-analysis. J Diabetes Investig. (2022) 13:262–70. doi: 10.1111/jdi.13658
22. Soondrum, T, Wang, X, Gao, F, Liu, Q, Fan, J, and Zhu, X. The applicability of acceptance and commitment therapy for obsessive-compulsive disorder: a systematic review and meta-analysis. Brain Sci. (2022) 12:656. doi: 10.3390/brainsci12050656
23. Thompson, B, Moghaddam, N, Evangelou, N, Baufeldt, A, and das Nair, R. Effectiveness of acceptance and commitment therapy for improving quality of life and mood in individuals with multiple sclerosis: a systematic review and meta-analysis. Mult Scler Relat Disord. (2022) 63:103862. doi: 10.1016/j.msard.2022.103862
24. van Agteren, J, Iasiello, M, Lo, L, Bartholomaeus, J, Kopsaftis, Z, Carey, M, et al. A systematic review and meta-analysis of psychological interventions to improve mental wellbeing. Nat Hum Behav. (2021) 5:631–52. doi: 10.1038/s41562-021-01093-w
25. Ferreira, MG, Mariano, LI, de Rezende, JV, Caramelli, P, and Kishita, N. Effects of group acceptance and commitment therapy (ACT) on anxiety and depressive symptoms in adults: a meta-analysis. J Affect Disord. (2022) 309:297–308. doi: 10.1016/j.jad.2022.04.134
26. Sun, Y, Ji, M, Zhang, X, Chen, J, Wang, Y, and Wang, Z. Comparative effectiveness and acceptability of different ACT delivery formats to treat depression: a systematic review and network meta-analysis of randomized controlled trials. J Affect Disord. (2022) 313:196–203. doi: 10.1016/j.jad.2022.06.017
27. Thompson, EM, Destree, L, Albertella, L, and Fontenelle, LF. Internet-based acceptance and commitment therapy: a transdiagnostic systematic review and meta-analysis for mental health outcomes. Behav Ther. (2021) 52:492–507. doi: 10.1016/j.beth.2020.07.002
28. Trindade, IA, Guiomar, R, Carvalho, SA, Duarte, J, Lapa, T, Menezes, P, et al. Efficacy of online-based acceptance and commitment therapy for chronic pain: a systematic review and meta-analysis. J Pain. (2021) 22:1328–42. doi: 10.1016/j.jpain.2021.04.003
29. Meyer, EC, Kotte, A, Kimbrel, NA, DeBeer, BB, Elliott, TR, Gulliver, SB, et al. Predictors of lower-than-expected posttraumatic symptom severity in war veterans: the influence of personality, self-reported trait resilience, and psychological flexibility. Behav Res Ther. (2019) 113:1–8. doi: 10.1016/j.brat.2018.12.005
30. Meyer, EC, Szabo, YZ, Frankfurt, SB, Kimbrel, NA, DeBeer, BB, and Morissette, SB. Predictors of recovery from post-deployment posttraumatic stress disorder symptoms in war veterans: the contributions of psychological flexibility, mindfulness, and self-compassion. Behav Res Ther. (2019) 114:7–14. doi: 10.1016/j.brat.2019.01.002
31. Bonanno, G . The end of trauma: How the new science of resilience is changing how we think about PTSD. New York: Basic Books (2021).
32. Cornum, R, Matthews, MD, and Seligman, MEP. Comprehensive soldier fitness: building resilience in a challenging institutional context. Am Psychol. (2011) 66:4–9. doi: 10.1037/a0021420
33. Britt, TW, Sinclair, RR, and McFadden, AC. Introduction: the meaning and importance of military resilience In: RR Sinclair and TW Britt, editors. Building psychological resilience in military personnel: Theory and practice. Washington: American Psychological Association (2013). 3–17.
34. Campbell-Sills, L, and Stein, MB. Psychometric analysis and refinement of the Connor-davidson resilience scale (CD-RISC): validation of a 10-item measure of resilience. J Trauma Stress. (2007) 20:1019–28. doi: 10.1002/jts.20271
35. Connor, KM, and Davidson, JRT. Development of a new resilience scale: the Connor-Davidson resilience scale (CD-RISC), depress. Anxiety. (2003) 18:76–82. doi: 10.1002/da.10113
36. Moore, BA, Hale, WJ, Judkins, JL, and Peterson, AL. Development and psychometric validation of the dispositional recovery and dysfunction inventory: a tool to assess for positive and negative cognitions following trauma exposure. Behav Cogn Psychother. (2022) 50:203–18. doi: 10.1017/S1352465821000230
37. Johnson, DC, Polusny, MA, Erbes, CR, King, D, King, L, Litz, BT, et al. Development and initial validation of the response to stressful experiences scale. Mil Med. (2011) 176:161–9. doi: 10.7205/milmed-d-10-00258
38. Duckworth, AL, and Quinn, PD. Development and validation of the short grit scale (grit–S). J Pers Assess. (2009) 91:166–74. doi: 10.1080/00223890802634290
39. Bond, FW, Hayes, SC, Baer, RA, Carpenter, KM, Guenole, N, Orcutt, HK, et al. Preliminary psychometric properties of the acceptance and action questionnaire-II: a revised measure of psychological inflexibility and experiential avoidance. Behav Ther. (2011) 42:676–88. doi: 10.1016/j.beth.2011.03.007
40. Rolffs, JL, Rogge, RD, and Wilson, KG. Disentangling components of flexibility via the Hexaflex model: development and validation of the multidimensional psychological flexibility inventory (MPFI). Assessment. (2018) 25:458–82. doi: 10.1177/1073191116645905
41. Romppel, M, Herrmann-Lingen, C, Wachter, R, Edelmann, F, Düngen, H-D, Pieske, B, et al. A short form of the general self-efficacy scale (GSE-6): development, psychometric properties and validity in an intercultural non-clinical sample and a sample of patients at risk for heart failure. Psychosoc Med. (2013) 10:Doc01. doi: 10.3205/psm000091
42. Blackwell, LS, Trzesniewski, KH, and Dweck, CS. Implicit theories of intelligence predict achievement across an adolescent transition: a longitudinal study and an intervention. Child Dev. (2007) 78:246–63. doi: 10.1111/j.1467-8624.2007.00995.x
43. Dweck, C, and Dweck, CS. Self-theories: their role in motivation, personality, and development. Philadelphia, PA: Psychology Press (2000).
44. Burckhardt, CS, and Anderson, KL. The quality of life scale (QOLS): reliability, validity, and utilization. Health Qual Life Outcomes. (2003) 1:60. doi: 10.1186/1477-7525-1-60
45. Spitzer, RL, Kroenke, K, Williams, JBW, and Löwe, B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. (2006) 166:1092–7. doi: 10.1001/archinte.166.10.1092
46. Weathers, F.W., Litz, B.T., Keane, T.M., Palmieri, P.A., Marx, B.P, and Schnurr, P.P., The PTSD checklist for DSM-5 (PCL-5), (2013). Available at: https://www.ptsd.va.gov/
47. Cameron, IM, Crawford, JR, Lawton, K, and Reid, IC. Psychometric comparison of PHQ-9 and HADS for measuring depression severity in primary care. Br J Gen Pract. (2008) 58:32–6. doi: 10.3399/bjgp08X263794
48. Kroenke, K, Spitzer, RL, and Williams, JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. (2001) 16:606–13. doi: 10.1046/j.1525-1497.2001.016009606.x
49. Podsakoff, PM, and MacKenzie, SB. An examination of the psychometric properties and nomological validity of some revised and reduced substitutes for leadership scales. J Appl Psychol. (1994) 79:702–13. doi: 10.1037/0021-9010.79.5.702
50. Vaitkus, MA . Unit manning system: Human dimensions filed evaluation of the COHORT company replacement model. Washington, DC: Walter Reed Army Inst of Research (1994).
51. Kabacoff, RI, Miller, IW, Bishop, DS, Epstein, NB, and Keitner, GI. A psychometric study of the McMaster family assessment device in psychiatric, medical, and nonclinical samples. J Fam Psychol. (1990) 3:431–9. doi: 10.1037/h0080547
52. Miller, IW, Epstein, NB, Bishop, DS, and Keitner, GI. The McMaster family assessment device: reliability and validity. J Marital Fam Ther. (1985) 11:345–56. doi: 10.1111/j.1752-0606.1985.tb00028.x
53. Palmer, A., McMorrow, S., and Kenney, G. M., (2015). Risk-based managed care in New Hampshire’s Medicaid program: a qualitative assessment of implementation and beneficiary experiences in year one. Available at: https://urban.org/sites/default/files/publication/39596/2000100-Risk-Based-Managed-Care-in-New-Hampshires-Medicaid-Program.pdf
54. Little, RJA . A test of missing completely at random for multivariate data with missing values. J Am Stat Assoc. (1988) 83:1198–202. doi: 10.1080/01621459.1988.10478722
55. Blanchard, BE, Johnson, M, Campbell, SB, Reed, DE 2nd, Chen, S, Heagerty, PJ, et al. Minimal important difference metrics and test-retest reliability of the PTSD checklist for DSM-5 with a primary care sample. J Trauma Stress. (2023) 36:1102–14. doi: 10.1002/jts.22975
56. Revicki, DA, Erickson, PA, Sloan, JA, Dueck, A, Guess, H, and Santanello, NC. Mayo, FDA patient-reported outcomes consensus meeting group. Interpreting and reporting results based on patient-reported outcomes. Value Health. (2007) 10:S116–24. doi: 10.1111/j.15244733.2007.00274.x
57. Marx, BP, Lee, DJ, Norman, SB, Bovin, MJ, Sloan, DM, Weathers, FW, et al. Reliable and clinically significant change in the clinician-administered PTSD scale for DSM-5 and PTSD checklist for DSM-5 among male veterans. Psychol Assess. (2022) 34:197–203. doi: 10.1037/pas0001098
58. Kashdan, TB, and Rottenberg, J. Psychological flexibility as a fundamental aspect of health. Clin Psychol Rev. (2010) 30:865–78. doi: 10.1016/j.cpr.2010.03.001
Glossary

Keywords: resilience, psychological flexibility, acceptance and commitment therapy, military personnel, military optimization, readiness
Citation: Peterson AL, Moore BA, Evans WR, Young-McCaughan S, Blankenship AE, Straud CL, McLean CS, Miller TL and Meyer EC (2024) Enhancing resiliency and optimizing readiness in military personnel through psychological flexibility training: design and methodology of a randomized controlled trial. Front. Psychiatry. 14:1299532. doi: 10.3389/fpsyt.2023.1299532
Edited by:
Giulio Maria Pasinetti, Icahn School of Medicine at Mount Sinai, United StatesReviewed by:
Alicia E. Meuret, Southern Methodist University, United StatesVrinda Saxena, Mount Sinai Hospital, United States
Copyright © 2024 Peterson, Moore, Evans, Young-McCaughan, Blankenship, Straud, McLean, Miller and Meyer. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alan L. Peterson, cGV0ZXJzb25hM0B1dGhzY3NhLmVkdQ==
†Present address: Abby E. Blankenship, School of Social Work, University of Texas at Austin, Austin, TX, United States