 Doha Alhashmi
Doha Alhashmi Aislinn Lalor2,3
Aislinn Lalor2,3- 1Department of Rehabilitation, College of Health and Rehabilitation Sciences, Princess Nourah Bint Abdulrahman University, Riyadh, Saudi Arabia
- 2Department of Occupational Therapy, School of Primary and Allied Health Care, Faculty of Medicine, Nursing and Health Sciences, Monash University, Frankston, Victoria, Australia
- 3Rehabilitation, Ageing and Independent Living Research Centre, School of Primary and Allied Health Care, Monash University, Frankston, Victoria, Australia
- 4Living with Disability Research Centre, School of Allied Health, La Trobe University, Melbourne, Victoria, Australia
Driving is essential for independence, community involvement and quality of life. Driving is the primary transportation method in Saudi Arabia. Despite the high rates of brain injuries and disability in Saudi Arabia, currently there are no guidelines regarding driver assessment and rehabilitation to facilitate people with brain injuries to resume driving. Therefore, this systematic review aimed to understand the assessment methods used internationally to evaluate driving competence for people with acquired brain injuries (ABI). A systematic search of six electronic databases was conducted by two authors and twenty-six studies were identified for review. Four main approaches to driver assessment: clinical assessments such as neuropsychological tests, off-road screening tools, simulator testing, and comprehensive driving assessment were identified. However, our findings revealed a lack of consistency in their use to assess driving competence after ABI. On-road driving performance tests were predominantly used to determine driving competence either independently or in combination with another method in over two-thirds of the reviewed studies. While clinical assessments of cognitive impairments showed some capacity to predict driving performance of people with ABI, they should be used with caution since they cannot replace on-road driving performance tests. Driver assessment should be part of rehabilitation following high prevalence conditions such as ABI. This systematic review offers guidance for Saudi clinicians, as well as policymakers, about providing rehabilitation services for people with ABI, and recommendations for further research and collaborations to improve this much-needed area of practice.
Introduction
Driving is an activity that supports people's independence and community involvement (1). Having a driver's license is important as it enables people to participate in valued daily activities (2, 3). Driving status and mobility affects physical and psychological health, as well as social participation and life satisfaction. Driving cessation conversely is related to decrease social participation, depression and isolation (4, 5).
In the Kingdom of Saudi Arabia (KSA), motor vehicles are considered the primary means of transportation within and between cities (6). Given driving is essential to many aspects of daily life for most people in Saudi Arabia, resuming driving is a priority for many patients following major injury for occupational, socio-economic and socio-cultural reasons (17). Traumatic brain injury (TBI) and stroke are leading causes of disabilities in Saudi Arabia (7). Driving is a complex activity that requires a variety of critical abilities such as cognitive, motor, perceptual, and executive functions, many of which could be impaired following acquired brain injuries (ABI) (10). Therefore, the ability to return to driving safely is of particular concern in this population.
People with brain injuries are reported to have a higher crash rate in comparison with the base rate of crashes in the United States general population (11), and between 58%–80% of stroke patients are not able to return to drive (12, 13). Similarly, a multicentre study in the United Kingdom reported only 36.5% of people resume driving following head injury (14). Moreover, multiple research studies report clients returning to driving without medical clearance (3, 15, 16). The situation is less well understood in Saudi Arabia, but a recent study reported only 7 out of 94 patients resumed driving post stroke and none had undergone any form of driving assessment or received driving-related information (17).
There is international agreement on the importance of assessing the driving competence of people considered medically at-risk drivers. Driving competency as defined by the Transportation Research Board (2016) is “the demonstration of fitness to drive that meets criteria recognized by a body responsible for driver licensing” (18, p.6). In Australia, the United Kingdom, Canada and the United States, published medical guidelines regarding driving assessments are available to regulate the medical practice and inform health professionals including physicians, occupational therapists, and optometrists (19–21). In comparison, there is no structured guideline to facilitate the process of returning to driving safely for people with disability in Saudi Arabia (17). Yet, the high rates of stroke and traumatic injuries in Saudi Arabia mean that a growing number of potentially medically at-risk drivers need assessment to enable safe driving.
Several systematic reviews and meta-analyses have been completed to facilitate evidence-based decision-making regarding driving assessment methods following stroke or traumatic brain injuries (TBI) (2, 22-25). In terms of assessing driving competence, Classen et al. (2009) (2) reviewed assessment methods used following severe, moderate and mild TBI. This review extracted data from 13 studies and classified the assessment methods used to assess driving competence following TBI. The review authors classified them as neuropsychological, simulator, off-road, self-report, and comprehensive driving evaluation (2). However, regardless of the assessment methods used, the authors concluded that there was no consistency on reporting the level of TBI severity within the included studies. Thus, recommendations on what methods to use in assessing driving competence were not generalizable to clients with different TBI severity levels (2). Systematic reviews by Baker, Unsworth, and Lannin (2015) (22) and Egeto, Badovinac, Hutchison, Ornstein, and Schweizer (2019) (23) attempted to address the gap presented by Classen et al. (2009) (2) via investigating driving competence with mild TBI separately from moderate and severe TBI. Both of these reviews identified a lack of consistent and standardised guidelines on competence to drive following TBI (22, 23). Other reviews by Devos et al. (2011) (24) and Hird, Vetivelu, Saposnik, and Schweizer (2014) (25) focused on driving assessment methods used following stroke. Devos et al. (2011) (24) reviewed clinical assessments, while Hird et al. (2014) (25) looked broadly into clinical, simulators and on road assessment methods. These two reviews reached similar conclusions about the heterogeneity of methods used to assess fitness to drive after stroke.
Given the lack of available guidelines in Saudi Arabia, the present systematic review focuses on identifying the available international evidence about methods of assessing driving competence following ABI, including both stroke and TBI. This evidence may then be used to inform decision-making about driving competence in rehabilitation policy and practice within Saudi Arabia.
Methods
This systematic review is reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist (26), however, the protocol was not registered for this review. The research question is: What assessment methods inform the evaluation of driving competence following ABI, including TBI and stroke?
Information resources
Six electronic databases including: CINAHL (Cumulative Index to Nursing and Allied Health Literature) Plus, Transportation Research Information Database (TRID), Ovid Emcare, Ovid MEDLINE, Ovid Embase, and PsycINFO, were searched on 20th March 2019. A follow up search was conducted on 2nd August 2021 to identify any additional eligible publications.
Eligibility criteria
Articles were eligible for inclusion in this systematic review if each of the following criteria were satisfied: i) the population included in the study had sustained any type of ABI, including participants with other conditions as long as participants with ABI were included; and ii) the assessment methods typically used in driving assessment practice had been included. For the purpose of this review, these assessment methods are categorized as: a) Clinical assessments including neuropsychological tests, and off-road screening tools, b) Simulator testing, and c) Comprehensive driving assessment. Also, iii) articles were included if they reported peer-reviewed original research studies. Articles were excluded if one or more of these criteria were identified: i) data for the ABI group were not reported separately or not able to be separated from other participant groups; ii) study designs were either opinion-based articles, narrative case studies, or assessments based on self-report or feedback of significant others; or, iii) they were not available in English. Additionally, only studies published after 1994 were included since research in the driving field has mainly been shaped after the mid-1990s (2).
Search strategy and study selection
The search strategy comprised combinations of free-text terms and thesaurus (e.g., MeSH) terms relating to assessments of fitness to drive for people with ABI and was developed by the primary author (DA) with the help of a specialist tertiary librarian.
The initial search strategy was developed for and used in Ovid MEDLINE, and was then adapted and replicated for use in the other five databases (see Supplementary file). Keywords included automobile driv*; OR automobile driver examination; OR driv* assess*; OR fit* drive*; OR driv* abilit*; OR read* driv*; OR driv* test; OR driv* rehab*; combined with the keywords brain injur*; OR stroke; OR traumatic brain injur*. (Refer to the Supplementary file for search strategy). The initial search identified 301 citations which were downloaded to a bibliographic management software (EndNote version 8), and 133 duplicate studies were removed as shown in the flow chart (see Figure 1). Two authors (DA and AL) completed title and abstract screening using systematic review software, Covidence to assess eligibility for inclusion in the systematic review. Consensus for inclusion of a study was reached through agreement between the two authors and where agreement could not be reached, a third author (EF) was consulted. On the 7 studies where DA and AL differed in their initial appraisal of eligibility, consensus was reached for 5 studies through discussion and the third author was consulted to reach consensus on 2 studies. This resulted in 75 articles for full text screening. Two authors (DA and AL) completed full text screening and reviewed the reference list of articles from key authors in the field resulting in 26 studies that met the inclusion criteria for the review. Articles were excluded predominantly due to ineligible study design.
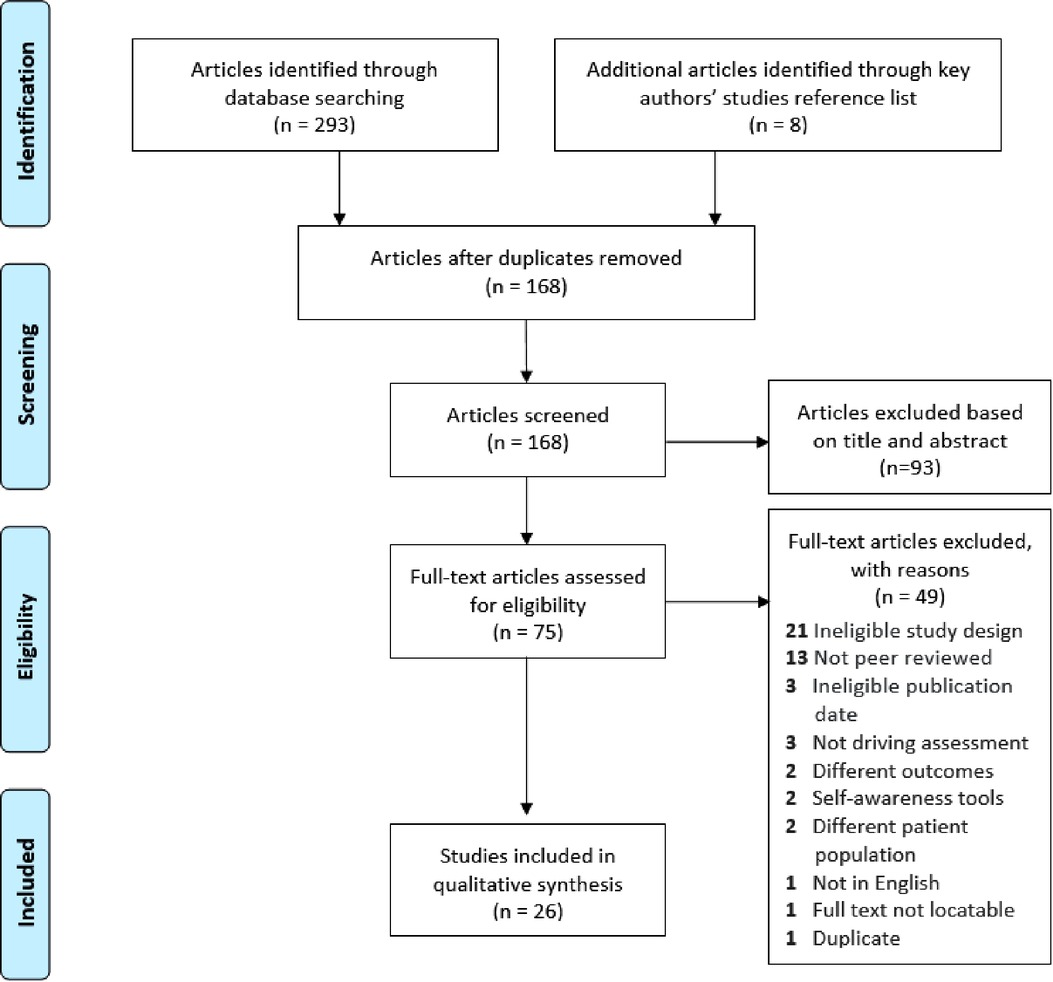
Figure 1. Flowchart of the systematic literature search.
Quality assessment
Quality assessment of eligible studies was independently completed by two authors (DA and AL) using a modified version of the Downs and Black Instrument (27).
The Downs and Black Instrument (1998) is a checklist for the assessment of the methodological quality of randomised and non-randomised studies comprising 27 items with Yes, No, or Not Applicable as response options. A score of 1 is granted for each Yes. In the unmodified Downs and Black Instrument, scores range from 0 to 34, where 34 indicates a study is high quality and 0 indicates low quality. Items are grouped to measure: i) reporting, ii) internal validity, iii) external validity, and iv) power. The checklist has acceptable face, content validity, and internal consistency (KR-20: 0.89), test–retest reliability (r 0.88), and inter-rater reliability (r 0.75) (27). Moreover, the Downs and Black Instrument can be modified to suit the requirements different research questions (27). Thus, modifications were made in a similar way to that described by Baker et al. (2015) (22), with six items (4, 8, 14, 19, 23, and 24) eliminated because they relate to intervention studies which were not applicable to the present systematic review as this review includes a population (people with ABI including TBI and stroke) and outcome (driving competence). Item 27 was also modified to Yes or No to assess the study power, as has been done previously in other studies (28). For the purpose of this study, the maximum score was 22 instead of 34.
Two authors (DA and AL) also reviewed all included studies for their level of evidence to ensure trustworthiness and creditability. The Oxford Centre for Evidence Based Medicine-Level of Evidence, in which the highest level of evidence is 1, and the lowest level of evidence is 5, was used for this purpose in this review (29).
Data extraction
Two authors (DA and AL) independently completed data extraction for all 26 studies meeting eligibility for inclusion. Data extracted for each study included: i) the citation (authors, publication year, title, journal, article type); ii) demographics (sample size, age of participants, gender ratio, study location, participant condition, time after injury, driving experience); iii) study methods (aim(s), design, assessment measure used to assess or screen fitness to drive, components measured by the assessment, simulator used or not, who conducted the assessment, clinical/on-road assessment conducted); and iv) results (ability to determine or inform competence to drive decision, overall results, potential sources of bias).
Data analysis
When planning this systematic review, it was anticipated that this systematic review could include a wide variety of study designs and competence to drive assessment methods and outcome measures that might not be sufficiently homogenous for quantitative synthesis. Thus, the data were descriptively categorised by assessment type: a) Clinical assessments including neuropsychological tests, and off-road screening tools, b) Simulator testing, and c) Comprehensive driving evaluation (CDE) which is defined as “clinical assessment using tools that correlate with driving performance or crash, followed by on-the-road assessment” (2) p.582.
Results
Descriptive profile of the primary studies
In total, 26 studies were identified for review, with publication date ranging between 1997 and 2019. Included studies were conducted in eight different countries, however over 70% of the included studies were conducted in Unite States, Australia and Sweden. Sample sizes varied from 26 to 269 participants with predominantly male participants (58%) and a mean age of 54.5 years where the youngest participant's age was 16 years old and the oldest was 93 years old (see Table 1). As Table 1 shows, the most studied population (n = 9) was the stroke population, while five studies investigated only people with TBI. In five other studies, both stroke and TBI were investigated under the umbrella of ABI; while the remaining seven studies comprised mixed population with various neurological conditions. The time since injury onset was reported in 20 studies and varied between 24 h to 7 years.
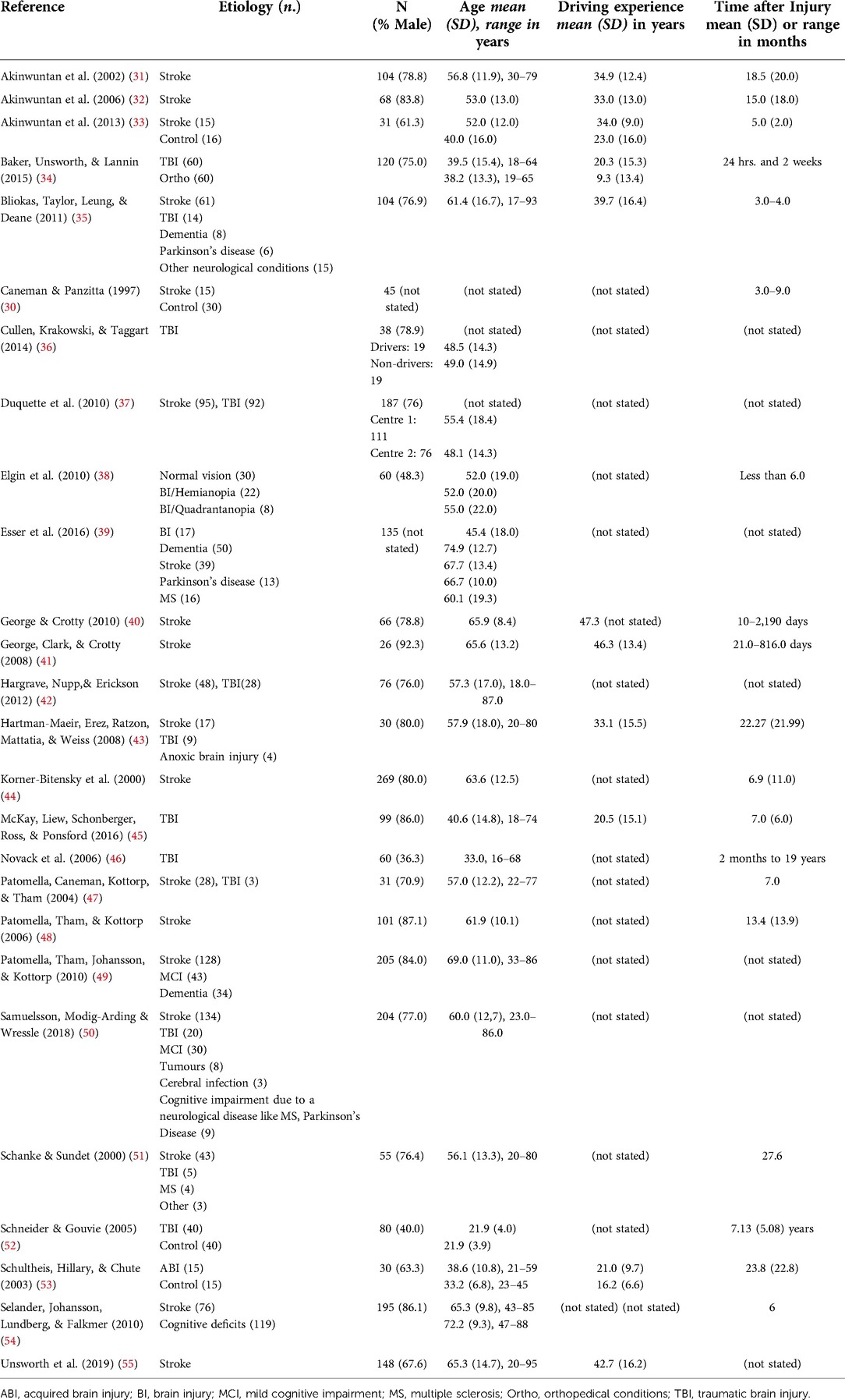
Table 1. Participant’s characteristics.
Study designs included 24 cohort studies, one case control and one unspecified quantitative study (see Table 2). Nearly all included studies had level 4 evidence using the Oxford Centre for Evidence Based Medicine- Level of Evidence (29) except for one where sufficient information to determine the level of evidence was unavailable (30). Small sample size was one of the most common methodological limitations amongst the included studies. Use of a retrospective approach contributed to sample heterogeneity around demographic, driving history and injury related variables in some studies. For example, driving experience was not reported in 9 of the included studies, whereas the other 17 studies measured it in different ways. Table 2 provides a summary of characteristics of each study included in this systematic review.

Table 2. Summary of studies included in the systematic review.
Assessment methods used to evaluate driving competence for people with ABI
The majority of the included studies investigated clinical assessment methods to evaluate driving competence following ABI (80.77%, n = 21) either by examining individual assessment tools or a battery of tools used in combination. Three studies used CDE (31, 32, 50) and three studies investigated use of the Performance Analysis of Driving Ability (P-Drive) (47–49). P-Drive is a measuring tool based on an analysis of the action needed to perform the activity of driving that can be used with simulated driving tests (47, 48) or on road driving test (49). Only one study reviewed the use of a simulator as a method to assess driving competence (30).
The common clinical assessment tools identified to predict on-road driving performance and inform the decision of competence to drive of individuals with ABI in this systematic review are presented in Table 3, together with variables from the International Classification of Functioning (56) measured by each tool. The clinical assessment tools in Table 3 are mostly administered using paper and pencil or via table top activities (such as card games), except for The Useful Field of View UFOV (57) which is a computer-based assessment. Aspects of cognitive function were assessed by all of the tools included in each study (see Table 3). Although all tools also displayed some capacity to predict on road driving performance in participants with ABI, most of the included studies highlighted that clinical assessment tools are to be used with caution, and cannot replace a test of real-life (on road) driving performance.
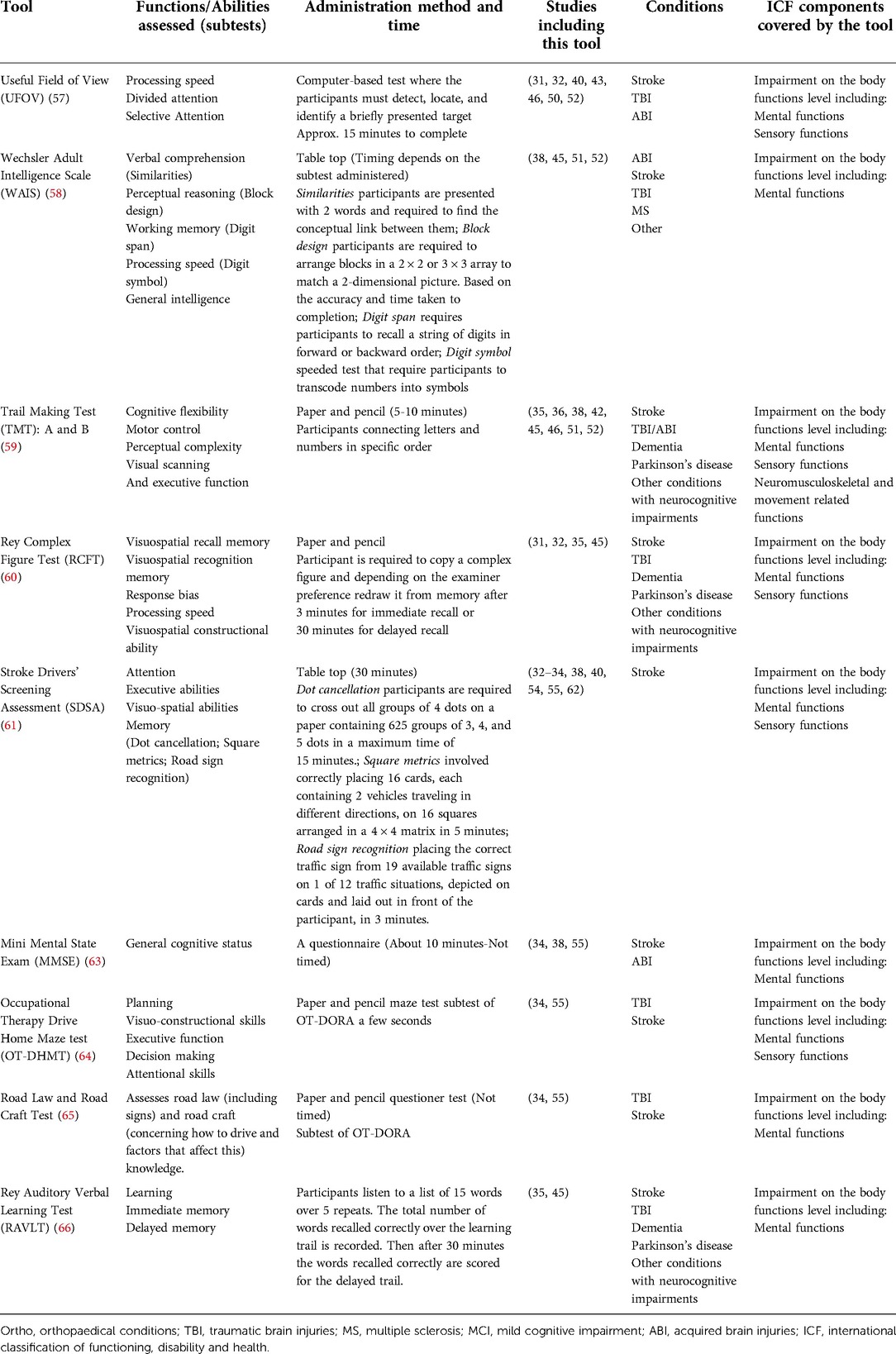
Table 3. Clinical assessment tools used in assessing competence to drive following ABI.
Three studies reported using CDE that consists of clinical and on-road testing to inform team decision on driving competence after ABI (31, 32, 50). The clinical part of the studies (31, 32) included visual tests and neuropsychological tests such as (UFOV, Figure of Ray). Moreover, the Stroke Driver Screening Assessment SDSA components that had proven to be predictive of on road testing were also measured in (32). Similarly, the UFOV and the SDSA were used in a study (50) as part of the clinical assessment, however, this study included a simulated driving test as part of the CDE in addition to on road driving test. Findings from one study were inconclusive (31), while another (32) identified that a combination of the Figure of Ray, visual neglect and the on road testing is the best model to assess driving competence after stroke. One study (50) recommended the use of the UFOV with a driving simulator.
P-Drive was found to be a valid scoring method that could be used to assess driving competence for an on road test (49). While only one study undertaken in 1997, with very limited data, investigated the use of a driving simulator as an assessment method of driving competence after stroke (30).
Outcome measures used to determine driving competency after ABI
There was no consistency in the outcome measures used to determine driving competency after ABI between the studies included in this systematic review. On-road driving performance was the predominant method to determine driving competence after ABI in 15 of the included studies. On the other hand, four studies measured driving performance on a simulator and two used a self-report method reporting driving status or accident involvement (34, 52). Two studies relied on team decision as an outcome measure (32, 50) and another study relied on re-instatement of driving licence (36). Furthermore, one study combined on-road driving performance with team decision (31) and another combined on-road testing with comprehensive hospital-based evaluation of visual, motor and perceptual functions to determine driving competency (53). The outcome variables for on-road driving performance were also reported in various ways: (i) a dichotomous scale of (pass, fail) (n = 9); or, (ii) a 3-point ordinal scale of either (pass, fail, requires lessons) or (pass, pass with conditions, fail) (n = 4). Three studies used variations of 4- or 5-point ordinal scales based on different factors. Noting the sample heterogeneity around demographic, driving history and injury related variables in addition to the outcome measures used (as outlined), a meta-analysis could not be performed.
Driving assessment administration practices
Clinical and on-road assessments were administered by an occupational therapist, either a generalist or specialist in driving rehabilitation in 21 out of the 26 studies (80.8%) included. In 13 studies, driver instructors/evaluators were involved in the on-road assessment with the occupational therapist. Both professionals would accompany the client in a dual-brake car, where the role of the driver instructor/evaluator generally would be to ensure safety and provide the trip instructions, while the occupational therapist would evaluate the performance of driving on the road. Other medical professionals such as physicians, neurologist, neuropsychologists and psychologist administered the clinical assessments in five other studies, while trained graduate students administered the assessments in one study (33). Additionally, clients were usually referred by a physician when further assessment to determine competence to drive was needed. For example, some states and territories in Australia mandate having a medical clearance for the occupational therapist to initiate the assessment process.
Discussion
Our systematic review of the available evidence indicates that there continues to be no consensus regarding the assessment methods for determining driving competence following ABI. A possible explanation may be the lack of high-quality research as most of the included studies were at level 4 of the Oxford Centre for Evidence-Based Medicine Levels of evidence (29). Another explanation could be linked to confounding factors that are frequently presented in the reviewed studies, such as the length of time between the injury, or the diagnosis, and patients' participation in driver assessment, or the severity of their disability which was not always reported in the studies. These confounding factors might directly or indirectly affect the driver assessment outcome. For instance, a person with a severe disability following a brain injury will likely have different outcomes when assessed for driving competence compared to someone whose abilities are less severely affected. Similarly, driver assessment outcomes could be expected to differ between earlier and later stages of recovery following brain injury. Finally, methodological limitations such as small sample size, lack of blinding, uncontrolled conditions and sample heterogeneity found in this review seem to be consistent with the findings of previous systematic reviews of driving related assessment methods focused on either TBI or stroke (2, 24, 68).
Clinical assessments
The present systematic review identified a number of clinical assessment tools that could be used to inform decisions regarding driving competency following ABI, comparable with findings reported by Hird et al. (2014) (25). Their review emphasised that driving tests that measure multiple cognitive components of driving-related performance, including TMT-A, TMT-B, RCFT, SDSA and UFOV, have the ability to predict driving fitness after stroke (25). Furthermore, Baker et al. (2015) (34) reported TMT-A, TMT-B, MMSE, OT-DHMT, Clock Drawing Test, Road Law and Road Craft Test as the most appropriate tools to be used in an acute setting with mild TBI population.
Measuring cognitive functions appears to be a common practice when assessing fitness to drive for people with brain injuries. Processing speed, executive function, attention, visuospatial skills, memory and mental flexibility are frequently measured components of cognition that should be considered when assessing driving competency (73). Nevertheless, Novack et al. (2006) (46), argue that cognitive tests are weak predictors to the on-road assessment outcome. Therefore, clinical assessments of cognitive functions may provide assistance when considering a referral to on-road driving evaluation, however, they should not replace on-road assessment (22, 34, 73). Applying the ICF, a possible explanation is that available clinical assessments are focused on impairments in the body functions/structures, whereas driving is a complex task better assessed at activity participation level and as undertaken within relevant environmental conditions (71). The use of on-road driving performance testing is therefore supported and widely recognized as an appropriate method to determine driving competence, suggesting it merits consideration as part of the establishment of driver assessment practices in Saudi Arabia.
On-Road assessment
An on-road driving test was the most common method used to determine driving competence in the reviewed studies and in other reviews, such as Devos et al. (2011) (24) who described the on-road test as a practical method of assessing driving performance. Most of the assessment methods investigated within the primary studies in this review were eventually compared to the outcome of an on road test to establish their predictive ability to determine driver competence. Even though the on road assessment method is recognised in many countries as a standard of relicensing after ABI, some valid methodological issues with using on-road testing were identified in this research. First, the professional assessors of the on-road test were not always blinded to the patient's data, which could result in over/under estimation of the test results. Second, although some studies used standardised test routes for all participants, it is impossible to control all test conditions including: weather, traffic density, and unexpected hazards (25, 35, 68). Third, the outcome of the on road testing remains subjective due to the lack of standardized scoring methods (31). As part of the development of on-road assessment practice within Saudi Arabia, establishing some standardized test routes that replicate the variety of road types, such as inner city heavy traffic conditions, long distance highways and dirt roads in the rural areas, will be necessary.
Driving simulator assessment
Driving simulators may potentially provide a safe alternative option to on-road driving testing (30, 69) as they can be adjusted and manipulated to different driving scenarios that cannot easily be reproduced in a real-life on-road test. Moreover, driving simulators may provide a controlled environment for testing and/or research where participants with differing medical conditions would undergo the same testing procedure to assess their driving abilities. However, Iisufficient evidence was found to support the use of driving simulators in rehabilitation practice as a driving assessment method following ABI. Indeed, this review identified only one low quality study of the validity of simulators following stroke (30). Similar findings about the lack of research supporting the use of driving simulators following TBI were reported by Classen et al. (2009) (2). Moreover, there is wide variability in terms of hardware, software, available driving scenarios and scoring methods between simulators (18, 25), and they are also not widely available and somewhat expensive to purchase. Motion sickness is also mentioned in the literature (71), although it was not measured or raised in any of the studies eligible for this review. Use of simulators in practice therefore needs to be considered with caution.
The performance analysis of driving ability (P-Drive)
While this review confirms previous findings regarding the lack of standardized scoring methods and consequent subjectivity of scoring used to report the outcomes of both on road testing and simulated testing (31, 71), it identified a tool developed over a series of research studies to provide a valid method for analyzing and scoring the performance of driving tasks (47–49). The P-Drive was initially developed for assessing driving performance following stroke on a high-fidelity simulator. It mainly focuses on observing the driver's actions and rating them based on an occupational perspective rather than relying on rating the underlying impairments (49). It is the only assessment tool reported in this review that is an activity and performance-based tool, not an impairment-based tool according to the ICF classifications when compared to the clinical assessment tools reported in Table 3. Using a valid and reliable scoring method, such as P-Drive would be useful to report the outcome of driving performance in simulated or an on road test.
Comprehensive driving evaluation
It has been stated in the literature that CDE is the gold standard for assessing driving competence, although its validity is unknown (2, 51, 72). This approach combines clinical and on road assessment, then the result of all the tests are weighted to determine driving competence. In the studies included in this review, we found some similarities as they all used UFOV in the clinical section and a dual brake car for the on road test. However, many differences appeared as to what was the best model that could predict the team decision of driving competence (31, 32, 50). This is in line with previous research that found the clinical assessment, as well as on road testing, may vary between practitioners (2, 51). This method is expensive and time-consuming to apply in clinical practice and still more research is needed to validate the clinical assessment as well as on road assessment for people with ABI. However, it is a safe and fair mean to assess driving competence, since neither using clinical assessment nor on road assessment independent of each other is always sufficient (72).
Limitations
Limitations of this review include not considering studies with languages other than English. Additionally, since the primary studies in this review were too different, this prevented the possibility of a meta-analysis (73). Because of the heterogeneity of the sample, study designs, settings, metrics, the assessment of driving competence, and the outcome measures used in each of the individual studies, these have been described in detail within the result section.
Implications and future research in relation to Saudi Arabia
The assessment of driving competency after ABI has not been investigated in the Saudi medical literature. It is essential to understand how clinicians address their patients' need to resume driving after ABI in Saudi Arabia. Since the results of this review identified occupational therapists and physicians as those who are most frequently involved in the process of driving fitness assessment and decision making, a qualitative approach to gain the perspective of both professions about this issue would be useful. Moreover, in agreement with Almosallam et al. (2021), a collaborative approach to engage stakeholders in a national initiative to establish a practice model of driver assessment and rehabilitation based on the highest available level of evidence is recommended. As aspects of this practice model, the use of clinical assessments and on-road testing for assessing driving competence are indicated.
Conclusion
This systematic review identified a number of assessment methods that could be used to inform the decision of fitness to drive following ABI, including clinical assessments, driving simulator assessment, and on-road test assessment. Clinical assessment of cognitive functions may be of assistance when considering the need for on-road driving performance assessment but is not a substitute for an on-road performance test when driving competence needs to be evaluated.
In Saudi rehabilitation services, clinicians should use functional measures, such as range of motion, brake reaction time, vision testing, and cognitive assessment, to identify potential areas of impairments that could affect driving competence of people with ABI. Further, the development of clinical guidelines for clinicians, especially occupational therapists, is crucial to inform recommendations regarding driving competence following ABI, so as to restore the community mobility and independence of those who are competent drivers and maximise the safety for road users in Saudi Arabia.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
Author contributions
DA has made substantial contributions to the conception or design of the work; the acquisition, analysis and interpretation of the data; drafting of the work, and the final approval of the version to be published. AL also contributed to the conception or design of the work; the analysis and interpretation of the data; revising the work critically for important intellectual content, and the final approval of the version to be published. EF contributed to the conception or design of the work; the interpretation of the data; revising the work critically for important intellectual content, and the final approval of the version to be published. All authors agree to be accountable for the content of the work. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fresc.2022.1020420/full#supplementary-material.
References
1. American Occupational Therapy Association. Occupational Therapy Practice Framework: Domain and Process—Fourth Edition. 2020.
2. Classen S, Levy C, McCarthy D, Mann WC, Lanford D, Waid-Ebbs JK. Traumatic brain injury and driving assessment: an evidence-based literature review. Am J Occup Ther. (2009) 63(5):580–91. doi: 10.5014/ajot.63.5.580
3. Turner B, Fleming J, Cornwell P, Worrall L, Ownsworth T, Haines T, et al. A qualitative study of the transition from hospital to home for individuals with acquired brain injury and their family caregivers. Brain Inj. (2007) 21(11):1119–30. doi: 10.1080/02699050701651678
4. Oxley J, Whelan M. It cannot be all about safety: the benefits of prolonged mobility. Traffic Inj Prev. (2008) 9(4):367–78. doi: 10.1080/15389580801895285
5. Pellerito JM Jr. The effects of driving retirement on elderly men and women living in metropolitan detroit. Top Geriatr Rehabil. (2009) 25(2):135–53. doi: 10.1097/TGR.0b013e3181a1038d
6. Mansuri FA, Al-Zalabani AH, Zalat MM, Qabshawi RI. Road safety and road traffic accidents in Saudi Arabia: a systematic review of existing evidence. Saudi Med J. (2015) 36(4):418. doi: 10.15537/smj.2015.4.10003
8. Al-Habib A, A-shail A, Alaqeel A, Zamakhshary M, Al-Bedah K, AlQunai M, et al. Causes and patterns of adult traumatic head injuries in Saudi Arabia: implications for injury prevention. Ann Saudi Med. (2013) 33(4):351–5. doi: 10.5144/0256-4947.2013.351
9. Ansari S, Akhdar F, Mandoorah M, Moutaery K. Causes and effects of road traffic accidents in Saudi Arabia. Public Health. (2000) 114(1):37–9. doi: 10.1016/S0033-3506(00)00306-1
10. Liddle J, Fleming J, McKenna K, Turpin M, Whitelaw P, Allen S. Driving and driving cessation after traumatic brain injury: processes and key times of need. Disabil Rehabil. (2011) 33(25-26):2574–86. doi: 10.3109/09638288.2011.582922
11. Coleman RD, Rapport LJ, Ergh TC, Hanks RA, Ricker JH, Millis SR. Predictors of driving outcome after traumatic brain injury. Arch Phys Med Rehabil. (2002) 83(10):1415–22. doi: 10.1053/apmr.2002.35111
12. Fisk GD, Owsley C, Pulley LV. Driving after stroke: driving exposure, advice, and evaluations. Arch Phys Med Rehabil. (1997) 78(12):1338–45. doi: 10.1016/S0003-9993(97)90307-5
13. Legh-Smith J, Wade D, Hewer RL. Driving after a stroke. J R Soc Med. (1986) 79(4):200–3. doi: 10.1177/014107688607900404
14. Hawley CA. Return to driving after head injury. J Neurol Neurosurg Psychiatry. (2001) 70(6):761–6. doi: 10.1136/jnnp.70.6.761
15. Leon-Carrion J, Dominguez-Morales M, Barroso y Martin J. Driving with cognitive deficits: neurorehabilitation and legal measures are needed for driving again after severe traumatic brain injury. Brain Inj. (2005) 19(3):213–9. doi: 10.1080/02699050400017205
16. Liddle J, Turpin M, McKenna K, Kubus T, Lambley S, McCaffrey K. The experiences and needs of people who cease driving after stroke. Brain Impair. (2009) 10(3):271–81. doi: 10.1375/brim.10.3.271
17. Almosallam A, Qureshi AZ, Ullah S, Alibrahim A. Return to driving post stroke patients’ perspectives and challenges in Saudi Arabia. Top Stroke Rehabil. (2022) 29(3):192–200. doi: 10.1080/10749357.2021.1905201
19. Association for Driver Rehabilitation Specialists. Best Practice Guidelines for the Delivery of Driver Rehabilitation Services 2016 [cited 2020 09/09].
20. Austroads tNTC. Assessing fitness to drive for commercial and private vehicle drivers: Medical standards for licensing and clinical management guidelines. Sydney; 2016.
21. Driver and Vehicle Licensing Agency. Assessing fitness to drive: a guide for medical professionals. Driving and Motoring Group; 2018.
22. Baker A, Unsworth CA, Lannin NA. Determining fitness to drive: a systematic review of the methods and assessments used after mild traumatic brain injury. Br J Occup Ther. (2015) 78(2):73–84. doi: 10.1177/0308022614562405
23. Egeto P, Badovinac SD, Hutchison MG, Ornstein TJ, Schweizer TA. A systematic review and meta-analysis on the association between driving ability and neuropsychological test performances after moderate to severe traumatic brain injury. J Int Neuropsychol Soc. (2019) 25(8):868–77. doi: 10.1017/S1355617719000456
24. Devos H, Akinwuntan AE, Nieuwboer A, Truijen S, Tant M, De Weerdt W. Screening for fitness to drive after stroke: a systematic review and meta-analysis. Neurol. (2011) 76(8):747–56. doi: 10.1212/WNL.0b013e31820d6300
25. Hird MA, Vetivelu A, Saposnik G, Schweizer TA. Cognitive, on-road, and simulator-based driving assessment after stroke. J Stroke Cerebrovasc Dis. (2014) 23(10):2654–70. doi: 10.1016/j.jstrokecerebrovasdis.2014.06.010
26. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Br Med J. (2009) 339:b2535. doi: 10.1136/bmj.b2535
27. Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. (1998) 52(6):377–84. doi: 10.1136/jech.52.6.377
28. Trac MH, McArthur E, Jandoc R, Dixon SN, Nash DM, Hackam DG, et al. Macrolide antibiotics and the risk of ventricular arrhythmia in older adults. CMAJ. (2016) 188(7):E120–E9. doi: 10.1503/cmaj.150901
29. Almosallam A. Oxford Centre for Evidence-Based Medicine. “ The Oxford 2011 Levels of Evidence.” Oxford Centre for Evidence-Based Medicine. http://wwwcebm net/index aspx?o=5653. 2011
30. Caneman G, Panzitta MJ. Driving simulation for neurological evaluation: an assessment tool in occupational therapy. Simulators and Traffic Psychol. (1997):69–75.
31. Akinwuntan AE, Feys H, DeWeerdt W, Pauwels J, Baten G, Strypstein E. Determinants of driving after stroke. Arch Phys Med Rehabil. (2002) 83(3):334–41. doi: 10.1053/apmr.2002.29662
32. Akinwuntan AE, Feys H, De Weerdt W, Baten G, Arno P, Kiekens C. Prediction of driving after stroke: a prospective study. Neurorehabil Neural Repair. (2006) 20(3):417–23. doi: 10.1177/1545968306287157
33. Akinwuntan AE, Gantt D, Gibson G, Kimmons K, Ross V, Rosen PN, et al. United States Version of the stroke driver screening assessment: a pilot study. Top Stroke Rehabil. (2013) 20(1):87–92. doi: 10.1310/tsr2001-87
34. Baker A, Unsworth CA, Lannin NA. Fitness-to-drive after mild traumatic brain injury: mapping the time trajectory of recovery in the acute stages post injury. Accid Anal Prev. (2015) 79:50–5. doi: 10.1016/j.aap.2015.03.014
35. Bliokas VV, Taylor JE, Leung J, Deane FP. Neuropsychological assessment of fitness to drive following acquired cognitive impairment. Brain Inj. (2011) 25(5):471–87. doi: 10.3109/02699052.2011.559609
36. Cullen N, Krakowski A, Taggart C. Early neuropsychological tests as correlates of return to driving after traumatic brain injury. Brain Inj. (2014) 28(1):38–43. doi: 10.3109/02699052.2013.849005
37. Duquette J, McKinley P, Mazer B, Gélinas I, Vanier M, Benoit D, et al. Impact of partial administration of the cognitive behavioral Driver's Inventory on concurrent validity for people with brain injury. Am J Occup Ther. (2010) 64(2):279–87. Language: English. Entry Date: 20130215. Revision Date: 20150711. Publication Type: Journal Article. doi: 10.5014/ajot.64.2.279
38. Elgin J, McGwin G, Wood JM, Vaphiades MS, Braswell RA, DeCarlo DK, et al. Evaluation of on-road driving in people with hemianopia and quadrantanopia. Am J Occup Ther. (2010) 64(2):268–78. doi: 10.5014/ajot.64.2.268
39. Esser P, Dent S, Jones C, Sheridan BJ, Bradley A, Wade DT, et al. Utility of the MOCA as a cognitive predictor for fitness to drive. J Neurol Neurosurg Psychiatry. (2016) 87(5):567–8. doi: 10.1136/jnnp-2015-310921
40. George S, Crotty M. Establishing criterion validity of the useful field of view assessment and stroke Drivers’ screening assessment: comparison to the result of on-road assessment. Am J Occup Ther. (2010) 64(1):114–22. doi: 10.5014/ajot.64.1.114
41. George S, Clark M, Crotty M. Validation of the visual recognition slide test with stroke: a component of the New South Wales occupational therapy off-road driver rehabilitation program. Aust Occup Ther J. (2008) 55(3):172–9. doi: 10.1111/j.1440-1630.2007.00699.x
42. Hargrave DD, Nupp JM, Erickson RJ. Two brief measures of executive function in the prediction of driving ability after acquired brain injury. Neuropsychol Rehabil. (2012) 22(4):489–500. doi: 10.1080/09602011.2012.662333
43. Hartman-Maeir A, Erez AB, Ratzon N, Mattatia T, Weiss P. The validity of the color trail test in the pre-driver assessment of individuals with acquired brain injury. Brain Inj. (2008) 22(13-14):994–8. doi: 10.1080/02699050802491305
44. Korner-Bitensky NA, Mazer BL, Sofer S, Gelina I, Meyer MB, Morrison C, et al. Visual testing for readiness to drive after stroke: a multicenter study. Am J Phys Med Rehabil. (2000) 79(3):253–9. doi: 10.1097/00002060-200005000-00007
45. McKay A, Liew C, Schonberger M, Ross P, Ponsford J. Predictors of the on-road driving assessment after traumatic brain injury: comparing cognitive tests, injury factors, and demographics. J Head Trauma Rehabil. (2016) 31(6):E44–52. doi: 10.1097/HTR.0000000000000209
46. Novack TA, Banos JH, Alderson AL, Schneider JJ, Weed W, Blankenship J, et al. UFOV Performance and driving ability following traumatic brain injury. Brain Inj. (2006) 20(5):455–61. doi: 10.1080/02699050600664541
47. Patomella A, Caneman G, Kottorp A, Tham K. Identifying scale and person response validity of a new assessment of driving ability. Scand J Occup Ther. (2004) 11(2):70–7. Language:English. Entry Date: 20050107. Revision Date: 20150820. Publication Type: Journal Article. doi: 10.1080/11038120410020520
48. Patomella AH, Tham K, Kottorp A. P-Drive: assessment of driving performance after stroke. J Rehabil Med. (2006) 38(5):273–9. doi: 10.1080/16501970600632594
49. Patomella A, Tham K, Johansson K, Kottorp A. P-Drive on-road: internal scale validity and reliability of an assessment of on-road driving performance in people with neurological disorders. Scand J Occup Ther. (2010) 17(1):86–93. doi: 10.3109/11038120903071776 Language: English. Entry Date: 20100430. Revision Date: 20171010. Publication Type: Journal Article.19565409
50. Samuelsson K, Modig-Arding I, Wressle E. Driving after an injury or disease affecting the brain: an analysis of clinical data. Br J Occup Ther. (2018) 81(7):376–83. doi: 10.1177/0308022618755999
51. Schanke AK, Sundet K. Comprehensive driving assessment: neuropsychological testing and on-road evaluation of brain injured patients. Scand J Psychol. (2000) 41(2):113–21. doi: 10.1111/1467-9450.00179
52. Schneider JJ, Gouvier WD. Utility of the UFOV test with mild traumatic brain injury. Appl Neuropsychol. (2005) 12(3):138–42. doi: 10.1207/S15324826AN1203_3
53. Schultheis MT, Hillary F, Chute DL. The neurocognitive driving test: applying technology to the assessment of driving ability following brain injury. Rehabil Psychol. (2003) 48(4):275–80. doi: 10.1037/0090-5550.48.4.275
54. Selander H, Johansson K, Lundberg C, Falkmer T. The nordic stroke driver screening assessment as predictor for the outcome of an on-road test. Scand J Occup Ther. (2010) 17(1):10–7. doi: 10.3109/11038120802714898
55. Unsworth CA, Baker A, Lannin N, Harries P, Strahan J, Browne M. Predicting fitness-to-drive following stroke using the occupational therapy - driver off road assessment battery. Disabil Rehabil. (2019) 41(15):1797–802. doi: 10.1080/09638288.2018.1445784
56. World Health Organization. Towards a common language for functioning, disability, and health: ICF. The international classification of functioning, disability and health. 2002.
58. Lichtenberger EO, Kaufman AS, Kaufman NL. Essentials of WAIS®-IV assessment. Hoboken, New Jersey: John Wiley & Sons; 2012.
59. Bowie C, Harvey P. Administration and interpretation of trail making test. Nat Protoc. (2006) 1:2277–81. doi: 10.1038/nprot.2006.390
60. Meyers JE, Meyers KR. Rey Complex figure test and recognition trial professional manual: psychological assessment resources; (1995).
61. Lincoln N, Radford K, Nouri F. Stroke drivers screening assessment: Revised manual. Nottingham, England: University of Nottingham (2004).
62. Al-Naami MY, Arafah MA, Al-Ibrahim FS. Trauma care systems in Saudi Arabia: an agenda for action. Ann Saudi Med. (2010) 30(1):50–8. doi: 10.5144/0256-4947.59374
63. Folstein MF, Folstein SE, Fanjiang G. Mini-mental state examination: clinical guide: psychological assessment resources; (2002).
64. Krishnasamy C, Unsworth CA. Normative data, preliminary inter-rater reliability and predictive validity of the drive home maze test. Clin Rehabil. (2011) 25(1):88–95. doi: 10.1177/0269215510382846
65. Unsworth CA, Pallant JF, Russell KJ, Germano C, Odell M. Validation of a test of road law and road craft knowledge with older or functionally impaired drivers. Am J Occup Ther. (2010) 64(2):306–15. doi: 10.5014/ajot.64.2.306
66. Schmidt M. Rey auditory verbal learning test: A handbook: Western Psychological Services Los Angeles, CA; 1996.
67. Ortoleva C, Brugger C, Van der Linden M, Walder B. Prediction of driving capacity after traumatic brain injury: a systematic review. J Head Trauma Rehabil. (2012) 27(4):302–13. doi: 10.1097/HTR.0b013e3182236299
68. Lew HL, Poole JH, Lee EH, Jaffe DL, Huang H-C, Brodd E. Predictive validity of driving-simulator assessments following traumatic brain injury: a preliminary study. Brain Inj. (2005) 19(3):177–88. doi: 10.1080/02699050400017171
69. Shechtman O, Classen S, Stephens B, Bendixen R, Belchior P, Sandhu M, et al. The impact of intersection design on simulated driving performance of young and senior adults. Traffic Inj Prev. (2007) 8(1):78–86. doi: 10.1080/15389580600994321
70. Fields SM, Unsworth CA. Revision of the competency standards for occupational therapy driver assessors: an overview of the evidence for the inclusion of cognitive and perceptual assessments within fitness-to-drive evaluations. Aust Occup Ther J. (2017) 64(4):328–39. doi: 10.1111/1440-1630.12379
Keywords: driving assessment, driving fitness, readiness to drive, brain injury, driving screening, occupational therapy
Citation: Alhashmi D, Lalor A and Fossey E (2023) Methods to evaluate driving competence for people with acquired brain injury (ABI): A systematic review. Front. Rehabilit. Sci. 3:1020420. doi: 10.3389/fresc.2022.1020420
Received: 16 August 2022; Accepted: 29 November 2022;
Published: 4 January 2023.
Edited by:
Jennifer Coker, Craig Hospital, United StatesReviewed by:
Zhuoying QIU, China Rehabilitation Research Center/WHO Collaborating Center for Family International Classifications, ChinaKornanong Yuenyongchaiwat, Thammasat University, Thailand
Ângela Fernandes, Polytechnic Institute of porto, Portugal
© 2023 Alhashmi, Lalor and Fossey. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Doha Hassan Alhashmi ZG9oYS5hbGhhc2htaUBtb25hc2guZWR1
Specialty Section: This article was submitted to Disability, Rehabilitation, and Inclusion, a section of the journal Frontiers in Rehabilitation Sciences