 Margaretha Stenmarker
Margaretha Stenmarker Maria Björk
Maria Björk Marie Golsäter
Marie Golsäter Karin Enskär
Karin Enskär- 1Institute of Clinical Sciences, Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden
- 2Department of Pediatrics, Region Jönköping County, Jönköping, Sweden
- 3Department of Biomedical and Clinical Sciences, Faculty of Medicine and Health Sciences, Linköping University, Linköping, Sweden
- 4School of Health and Welfare, Jönköping University, Jönköping, Sweden
- 5CHILD—Research Group, School of Health and Welfare, Jönköping University, Jönköping, Sweden
- 6Child Health Services, Region Jönköping County, Jönköping, Sweden
- 7Department of Women’s and Children’s Health, Uppsala University, Uppsala, Sweden
Background: Being diagnosed with cancer in childhood often has a direct impact on the child's opportunities to participate in activities and the child's sense of belonging in different life situations. Experiences of illness in youth affect the lives of these individuals in numerous ways and they need pronounced support to regain their normal life after treatment.
Purpose: To illustrate how childhood cancer survivors describe the role of the caring support provided by healthcare professionals at diagnosis and during the cancer trajectory.
Methods: A mixed methods approach was applied. Swanson's Theory of Caring was used to deductively analyze the answers in a study-specific questionnaire with Likert scales (1–5). Descriptive and comparative statistics and exploratory factor analyses were performed.
Results: Sixty-two former patients, diagnosed with solid tumors/lymphoma in 1983 to 2003 in Sweden, participated. The mean time passed since treatment was 15.7 years. Swanson's caring processes Being with and Doing for were the most prominent loading categorical factor indicators. Higher scores for healthcare professionals being emotionally present (Being with), doing for others what they would do for themselves (Doing for) and being willing to understand the sick child's situation (Knowing) were highlighted by survivors older than 30 years, compared to those younger than 30 years (p = 0.041, p = 0.045, and p = 0.013, respectively). An increased vulnerability regarding their ability to cope with difficulties (Maintain belief) was found among participants who were treated during adolescence, related to schoolchildren (p = 0.048), and among those who had been treated with extra-cranial irradiation in comparison with no extra-cranial irradiation (p = 0.004). The role of having a partner in comparison with being single was underlined among those who felt they had acquired the tools they needed to take care of themselves (Enabling) (p = 0.013). The total explained variance was 63%.
Conclusions: A person-centered care approach during treatment for childhood cancer, reflected by a caring model, highlights the role of healthcare professionals being emotionally present, involving children, performing actions, and with an approach that has potential long-term implications. Childhood cancer patients and survivors need not only clinically competent professionals, but professionals who provide caring interactions with compassion.
Introduction
Long-term survivors of childhood cancer experience physical problems, psychological issues, as well as activity and participation challenges following treatment completion (1, 2). There has been growing attention to these individuals and their experiences of illness in childhood, during growth and development, but also how these circumstances have affected the survivors’ lives in numerous ways (3).
Over 80% of children diagnosed with cancer are now cured (4, 5) and they will become long-term survivors with many potential years of life ahead of them (6). In Sweden, the number of childhood cancer survivors is approximately 11 000, and among these survivors the majority, about 70%, have developed late complications (7). Despite this, it is important to not just focus on their illness and late complications but also on their health. Health is a resource for everyday life and a positive concept emphasizing social and personal resources as well as physical capabilities (WHO, 1986) (8). Health is related to the child's ability to perform the activities he/she wants, but also to the possibility to participate in an everyday life (9). When children participate in different forms of activities, it positively influences their health, development and well-being (10, 11). Still, the physical and social environment as well as limited resources can act as barriers limiting participation (12). If healthcare personnel are to be able to give all of these affected individuals good person-centered care, they need to start with the specific person they have in front of them and to identify their various needs, resources and experiences (13). However, Sundler et al. (2020) highlights that a person-centered approach to care encompasses a caring approach based on humanistic values (14). In addition, researchers have pointed out the need of “employing a Life Course lens” as methodological assessment following the complex and multifactorial consequences of childhood cancer (15).
The concept of caring is essential in all healthcare, but there is no uniform definition of it (16). Still, healthcare professionals' (HCPs') actions and expectations can be studied and improved by systematically linking them to a theoretical perspective (16, 17). Swanson's Theory of Caring (1993) which is built on the foundational work of Jean Watson, exemplified an approach that promoted a practical application of caring theory. Swanson stated that “Caring is a nurturing way of relating to a valued other person, towards whom one feels a personal sense of commitment and responsibility” (18). The theory depicts caring as grounded in maintenance of a basic belief in persons, anchored by knowing the other's reality, conveyed through: knowing, being with, doing for, enabling/empowering, and maintaining belief (19). All these components are essential elements of any professional-patient relationship with the outcome in interventions that “promote, restore, and maintain optimal wellness for individuals” (20). Thus, Swanson's middle-range theory explains the link between the caring processes and the intended outcome, which is the patient's well-being (19).
Caring as perceived by people with cancer involves HCPs' having professional attitudes and skills with the intention of providing good care (21). In order to facilitate the childhood cancer survivors' everyday life during and after ending cancer-directed treatment, it is important to focus on how they experience received support. Therefore, the aim of the present study was to illustrate how childhood cancer survivors describe the role of the caring support provided by HCPs at diagnosis and during the cancer trajectory. The research group hypothesized that the quality of care delivered by HCPs during the childhood cancer trajectory has long-term psycho-social consequences. The following research questions were formulated: What aspects of caring are reported among childhood cancer survivors? Do caring experiences from childhood cancer treatment have percussions in adult life? Can Swanson's caring theory be verified among childhood cancer survivors?
Methods and materials
Design
An exploratory sequential mixed-method design with integrated quantitative and qualitative data was used (22), as well as descriptive and comparative analysis. A study-specific questionnaire was developed based on a qualitative approach with interviews (22) with former childhood cancer patients and a literature review (23). The present retrospective cross-sectional study collected data through this study-specific questionnaire. In the operationalization process, the results from the questionnaire were deductively analyzed with content analysis (24) using Swanson's Theory of Caring (1991; 1993) (18, 19) and the domains were statistically described and compared.
Participants and context
Inclusion criteria
(1) Former patients diagnosed with solid tumors and lymphoma from 1983 to 2003, being eight to 17 years old at diagnosis, being more than 17 years old when giving their informed consent to participate, and at least three years had passed since the end of the cancer-directed treatment;
(2) Treatment modalities which included cytotoxic treatment and/or surgery and/or extra-cranial irradiation.
Exclusion criteria
Patients who may have received cranial irradiation.
All patients were diagnosed at the Child Cancer Centre at Queen Silvia Children's Hospital, Gothenburg, Sweden. The center has a catchment area comprising the whole of western Sweden, with a child population of about 400,000 and an annual incidence of 80–100 cases, in comparison with the annual incidence in Sweden of 300–350 cases (7). Since the beginning of 1980, the center has established a well-thought-out philosophy aiming at open communication about the disease and the adverse side effects of the treatment, and underlining the importance of comprehensive support to the patients and their families throughout the entire treatment period.
In all, 96 former patients were treated according to the above mentioned inclusion criteria and were eligible. Thus, they constituted the target group. These participants had been diagnosed with lymphoma, i.e., Hodgkin's disease (HL) and Non-Hodgkin's disease (NHL) and the rest of the group were defined as “other diagnosis”. The latter group included former patients with miscellaneous sarcomas and rare malignant disorders, for example ovarian tumors, thyroid and nasal-pharyngeal cancers. The exclusion criteria included patients who may have received cranial irradiation, i.e., primarily patients with central nervous system tumors and patients treated for leukemia. This stance was based on previous research regarding the risk of neurocognitive complications and possible difficulties in participating in a retrospective study (25).
Data collection
The target group, i.e., a total population of 96 individuals, was invited by mail or telephone to take part in the study. When the informed consent process was ended, a study-specific questionnaire was distributed by mail and returned in pre-paid envelopes. In all, 15 eligible individuals could not be reached. Ten former patients refused participation and nine did not return the questionnaire despite being reminded three times. Overall, the individuals who did not participate represent all of the subgroups which are presented in Table 1. Thus, the final study population was considered to mirror the target group.
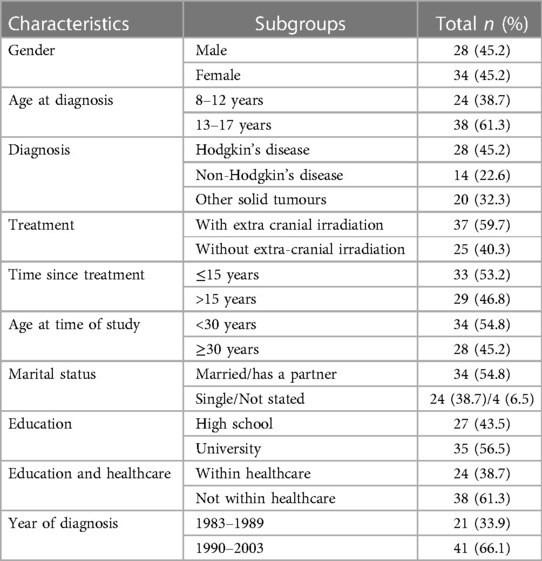
Table 1. Characteristics of the study population (n = 62).
The questionnaire used for this study was designed specifically for the target population (26). In total, the questionnaire included 225 items with two main themes: Quality of life in childhood cancer survivors (n = 133 items) and Caring aspects during the cancer trajectory (n = 92). The answer options were presented on five-point Likert scales ranging from 1 (“I disagree”) to 5 (“I fully agree”). The content validity was determined by a process which included interviews with childhood cancer survivors and a literature review. The relevance of the items posed and the interpretability of the questionnaire were discussed with the interview contributors and experts within the field of pediatric oncology, and in relation to the concepts of quality of life (QoL) and caring aspects. An item selection and reduction process was performed using a factor analysis with the aim of strengthening the construct validity of the questionnaire. To some of the items open-ended questions were posed. The main theme Caring aspects during the cancer trajectory included questions such as: What memories do you have of the conversation when you were told about your disease diagnosis? Was there anything in the conversation you were not satisfied with? Which procedures were frightening or painful? A detailed description of the development of the questionnaire has been presented in a publication regarding the main theme Quality of life in childhood cancer survivors (23).
Data analysis
Deductive analysis
Data were analyzed using qualitative content analysis with a deductive approach according to Elo and Kyngas (2008) (24). Deductive content analysis is used when the structure of analysis is operationalized on the basis of previous knowledge (24). All items in the study-specific questionnaire dealing with caring (n = 92 items) were read through several times to get an overview of the content. This action was performed independently by all the authors. The first step in the deductive approach was to develop a categorization matrix based on the domains in Swanson's Theory of Caring. The data were coded according to Swanson's five caring domains (knowing, being with, doing for, enabling, and maintaining belief) and appropriate associated subdomains for each caring domain. The intended outcome is the client's well-fare. The coding process in the present study was intended to develop and use related concepts for each domain, to illustrate how the survivors described the caring support provided by HCPs during the period of illness. The posed related concepts are presented in Figure 1 with the number (n) of items within each domain. In Elo and Kyngas (2008) content analysis model, a domain is described as Generic category and a sub domain as Sub category (24).

Figure 1. The role of caring support. Summary of the study categorization matric based on Swanson’s Theory of Caring.
Statistics
The descriptive statistics consist of frequencies, median values, mean values and standard deviations. Before the analyzes were performed, all negative items were reversed. Chi-square statistics were obtained in order to compare proportions of categorical variables between demographic data/characteristics. Fisher's exact test was used when more than 15% of the cells had an expected value of <5. To compare values between two independent variables, the Mann-Whitney test was used, while the Kruskal-Wallis test was used to compare three independent variables. Statistical significance was obtained at the level of p < 0.05.
The coded data identified by the previously described deductive content analysis (24) was analyzed using principal component analysis. Kaiser-Meyer-Olkin (KMO) and Bartlett's test of sphericity were performed. The obtained value for KMO was 0.624 and for Bartlett's test 0.000, which indicates a matrix capable of factorization. The extraction method was based on five fixed factors. Items (descriptors) with correlations above 0.5 were organized into factor groups describing their correlation to the five domains in Swanson's Theory of Caring (19). Reliability within each domain (factor) was verified by calculating the internal consistency, using the Cronbach's alpha value, for each domain separately (26). A criterion of 0.60–0.90 is proposed to be a good internal consistency, in exploratory studies (27). The statistical analyzes were performed using IBM SPSS Statistics version 22.0 (IBM Corp, Armonk, New York, USA).
Ethical considerations
The participants were given oral and written information about the study before they gave their informed consent to participate. The Regional Research Ethics Board, Gothenburg Sweden, approved the study (Dnr 289-07).
Results
Study participants
The final study group consisted of 62 persons (34 women and 28 men). The mean age at diagnosis was 12.9 years (range 8–17, SD 2.3, median value 13 years). The mean current age of the participants was 28.7 years (range 18–45, SD 6.3, median value 28.5 years) and the mean time passed since treatment was 15.7 years (range 4–28, SD 2.4, median value 15 years). The response rate was 65%. Sub-group analyzes were performed including gender, being a school-age child (8–12 years) or adolescent (13–17 years) at the time of diagnosis, diagnosis (HL, NHL, other solid tumors), and treatment with or without extra-cranial irradiation. Furthermore, sub-group analyzes regarding time since treatment (cut off: median value 15 years), being a child or a young adult, i.e., younger than 30 years (28), or older than 30 years when participating in the study, living with/without a partner, education at university level or not and having an education within healthcare or not. The year of diagnosis was defined in two categories, 1983–1989 or 1990–2003, i.e., before or after the early 1990s. In the beginning of the 1990s there was a shift in treatment modality vis-à-vis patients with HL, in particular with the main goal of creating protocols with reduced radiotherapy (29) (Table 1).
Categorization matrix based on Swanson's middle-range theory of caring
A summary of the study categorization matric based on Swanson's Theory of Caring, with the distribution of the total number of descriptors from each domain (study-specific questionnaire) and the sub domains identified in this study is presented in Figure 1. The contributing descriptors with values above 0.5, for each of the five latent factors/domains together with the strength of the correlation are presented in Table 2. In total, 26 descriptors out of 92 fulfilled the correlation criteria. The total explained variance was 62.4%. Few participants answered the open-ended questions and therefore, these questions were not analyzed separately with qualitative methods. The free worded answers have partly influenced the analysis process and the interpretation of data in the discussion.
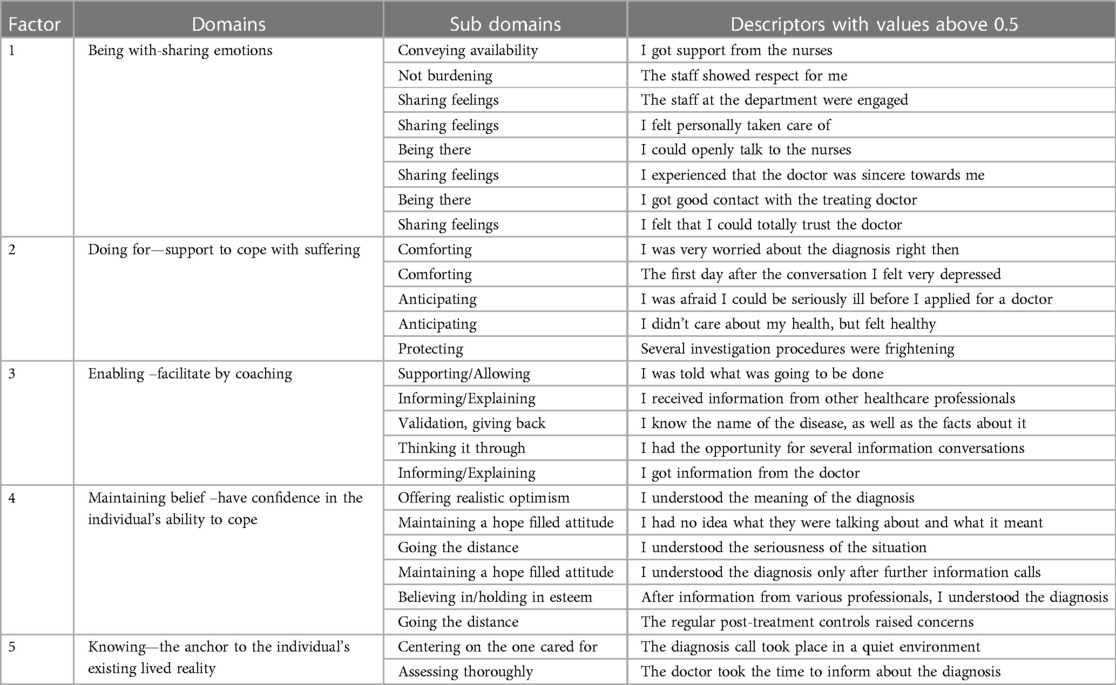
Table 2. Description of the domains, sub domains and descriptors with values above 0.5, based on Swanson's Theory of Caring.
The concept of caring and sub-group analysis (characteristics of the study population)
Factor 1 being with—sharing emotions
Being with—sharing emotions was the most prominent loading categorical factor indicator. This domain reflects the caring process of being with. According to Swanson (Swanson, 1993; Wojnar, 2006) (19, 30) being with includes being genuinely present for others in order to convey that their experiences have significance. The items included in this domain, from the study-specific questionnaire, were linked to the subdomains; being there, conveying availability, not burdening, and sharing feelings (Table 2). The Cronbach's alpha value was equal to 0.89.
Childhood cancer survivors belonging to the older age group (>30 years) rated the role of being with—sharing emotions as more salient, in comparison with young adults (<30 years), (p = 0.041) (Tables 3A–C).
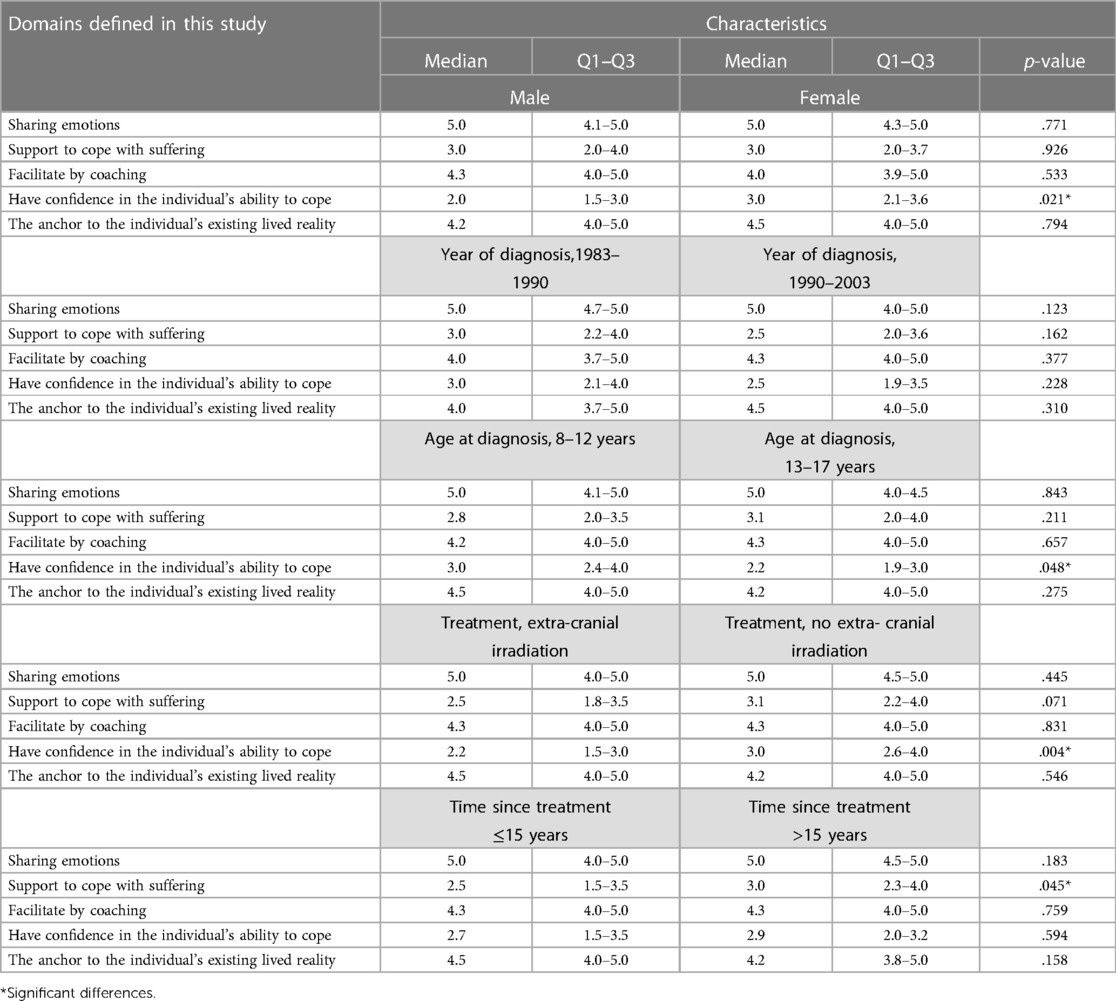
Table 3A. Domains and sub-groups characteristics in comparison (Mann-Whitney).
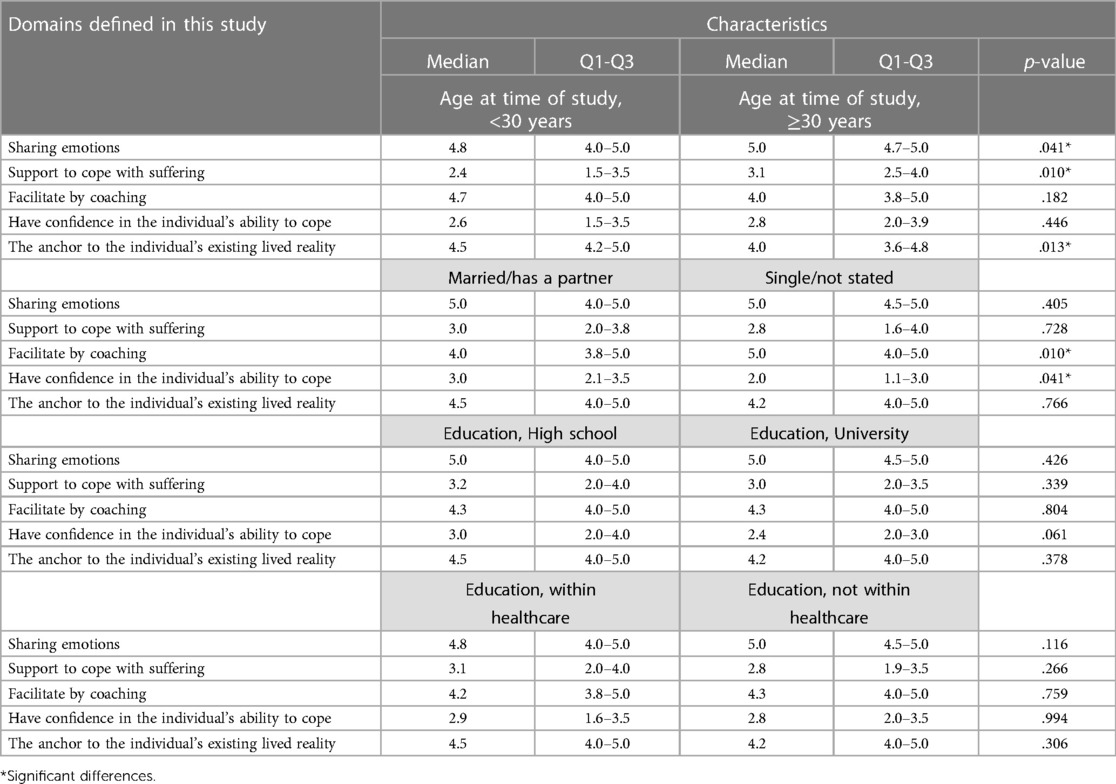
Table 3B. Domains and sub-groups characteristics in comparison (Mann-Whitney).
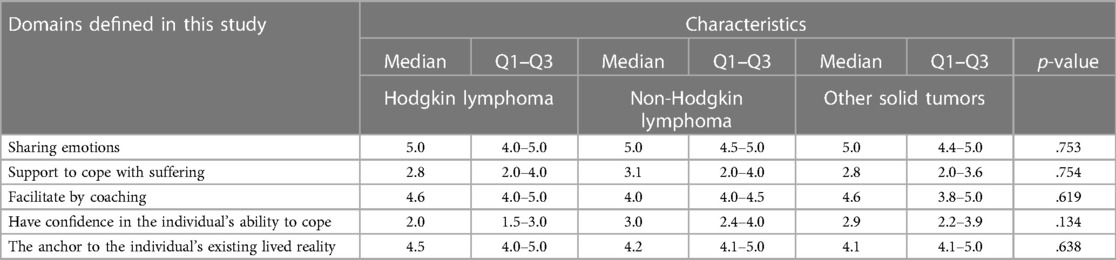
Table 3C. Domains and sub-group characteristics in comparison (Kruskal-Wallis).
Factor 2 doing for—support to cope with suffering
Doing for—support to cope with suffering was the second most prominent loading factor. This factor reflects Swanson's process of doing for (19, 30) which consists of doing for other persons what they would do for themselves, if possible. Items in this study cover the subdomains of comforting, protecting and anticipating (Table 2). The Cronbach's alpha value was equal to 0.79.
Survivors with long-term follow-up, defined as more than 15 years post-treatment, and those in the older age group (more than 30 years) when participating in the study, reported higher rating regarding HCPs doing for others what they would do for themselves, compared to those with a shorter time of follow-up and who were young adults (p = 0.045 and p = 0.010, respectively) (Tables 3A–C).
Factor 3 enabling—facilitate by coaching
Enabling—facilitate by coaching corresponds to Swanson's concept of enabling (19, 30) and entails assisting individuals to acquire the tools they need to be able to care for themselves, including periods with life-transitioning events. The study-specific items in this domain are related to the subdomains of explaining/informing, supporting/allowing, validating/giving feedback, and thinking it through (Table 2). The Cronbach's alpha value was equal to 0.77.
This caring process was rated higher among individuals living with a partner compared to those who were single (p = 0.013) (Tables 3A–C).
Factor 4 maintaining belief—have confidence in the individual's ability to cope
Having confidence in an individual's ability to cope is in line with Swanson's concept of maintaining belief (19, 30), which incorporates a fundamental belief in people and their ability to make it through events and transitions and to face a future with purpose. The subdomains of maintain a hopeful attitude, offering realistic optimism, believing in/holding in esteem, and going the distance (Table 2) are present in this study. The Cronbach's alpha value was equal to 0.70.
Participants who lived with a partner conveyed higher rating about having been assisted with tools to take care of themselves and the ability to cope with difficulties, in comparison with persons who were single (p = 0.041). An increased vulnerability regarding the ability to cope was more salient among men compared to women (p = 0.021), among those who were treated during adolescence (13–17 years) related to schoolchildren (8–12 years) (p = 0.048) and among participants who had been treated with extra-cranial irradiation, in comparison with no extra-cranial irradiation (p = 0.004) (Tables 3A–C).
Factor 5 knowing—the anchor to the individual's existing lived reality
The anchor between the HCPs' and the individual's existing lived reality is associated with the caring process of knowing (19, 30). Knowing can be defined as the starting point for the striving “to understand an event as it has meaning in the life of another person” (30). The items included reflect the subdomains of centering on the one cared for and assessing thoroughly (Table 2). The Cronbach's alpha value was equal to 0.89.
The HCPs' willingness to understand the sick child's situation was highlighted particularly in the older age group compared to those being less than 30 years of age when they participated in the study (p = 0.013) (Tables 3A–C).
No significant differences were found within the following sub-groups; year of diagnosis (Table 3A), education (high school/university) (Table 3B), education within or not within healthcare (Table 3B) and the cancer diagnosis in childhood (Table 3C).
Discussion
The results of this study highlight that through the lens of Swanson's Theory of Caring, childhood cancer survivors experience the HCPs as being emotionally present, carrying out actions, and involving children in their treatment and follow-up care.
The caring process of being with, in the present study defined as “Being with—sharing emotions”, had the most prominent loading and showed how the survivors appreciated care, engagement, openness and trust in HCPs. Being with can be considered as a way of deepening the role of knowing, i.e., by trying to see events from the perspective of the person affected. In the present study the older age group of survivors rated the role of HCPs being emotionally present, as well the HCPs' willingness to understand the sick child's situation, as more salient in comparison with young adults. The long-term survivors' lives involve a process of struggle to overcome numerous difficulties. According to previous studies, cancer survivors need pronounced support and information to get life back to normal after treatment (31–33). For participants belonging to the older age group, several years had passed since they were diagnosed with childhood cancer. These participants had high ratings regarding the role of HCPs being emotionally present to comfort worried and depressed children/adolescents at the time of diagnosis, as well as giving support to cope with frightening procedures. These actions probably reflect the experiences of the role of creating good relationships and HCPs being available during illness and after treatment. This is in line with the study of Cantrell and Matula (2009) (34), which points to the fact that it is not exclusively the extraordinary efforts that leave a mark; rather, simple acts of caring are meaningful. Such actions can mediate comfort during treatment, facilitate participation in everyday life, and also have implications in a long-term perspective. In addition, when patients feel they are seen and heard by the HCPs they are likely to more actively participate in their own care and if needed seek care (14).
In the present study, vulnerability was related to gender, age at diagnosis, marital status and oncological treatment in childhood, regarding the individual's ability to cope with the impediments. These data confirm previously identified risk groups for susceptibility, namely persons living alone, being male, falling ill as a teenager, and having been treated with radiotherapy (35, 36). Previous research has shown that survivors of childhood cancer live with worries and uncertainty (37), but also rate high on positive life changes and sense of purpose (3). Furthermore, they may have grown positively due to their negative past experience (3). The role of healthcare providers is crucial as the patient's susceptibility can increase or decrease related to the manner in which HCPs interact with the patient (38). Therefore, it is vital to address the fact that patients’ and professionals' perceptions of the overall caring can differ significantly, as well as perceptions of individual behaviors (16). Thus, it is fundamental that children and adolescents are seen, heard and listened to in order to have a healthy life. The meeting with the HCPs will be important and will reflect how the children/adolescents experience their ongoing cancer trajectory and their opportunities to dare to look ahead. Consequently, it can be considered important that the HCPs train in caring, based on an approach with a comprehensive theory to be able to define and measure verbal and non-verbal caring and non-caring behaviors. The Caring Behavior Coding Scheme (the CBCS), based on Swanson's Theory of Caring, has been proposed to fulfil such a purpose and could be a way to assess care efforts (39).
Involving the child
Involving the child is a process which starts at the time of diagnosis, runs through the entire treatment period, the transition to a healthy life, and goes beyond post-treatment, with long-term implications. Research has shown that the desire to participate and to be involved applies to all children, even the very smallest treated for malignant diseases (40).
The study results highlight the HCPs' efforts to try to go the whole distance by understanding, sharing emotions, performing actions to help the child to cope with suffering, and sustaining faith in the child's capacity. Focusing on the child's participation and the consequences in a long-term perspective is crucial. Previous studies within pediatric oncology caring science have well-being and QoL as central themes, but mainly from the view of the parents and rarely show the child's or the survivor's perspective (41, 42).
Childhood cancer survivors require age-appropriate and flexible care. They experience social withdrawal and awkwardness due to adaptation difficulties caused by social life interruption, family issues, social prejudice, and discrimination. In our previous publication with the theme of QoL in childhood cancer survivors, the results revealed the importance of social support for well-being during the child's active treatment phase (23). The physical and social struggles may result in experiences of mental stress and psychological withdrawal followed by rebound (37). It is important to watch for these signs and to provide early support to survivors so that their daily life and development are not hindered by the treatment or its side effects, and to offer long-term support focusing on individual patient characteristics (43). In the long-term perspective, the need for psychological support is highlighted (23). Regarding psychological side effects, there is a call for support in the transition back to normal life after the cancer experience (44). In addition, Barnett et al. (2016) found that young cancer survivors' experiences are nuanced, with interacting variables contributing to post-treatment outcomes (44). In line with the model of participation described by Imms et al. 2017, the two concepts of attendance in activities as well as involvement in activities are essential (45). Therefore, providing good care and being caring are central factors when highlighting the role of participation. In the context presented in this study these actions can be defined as sharing the child's emotions and experiences, being with the child, doing things for the child that he/she cannot do for himself/herself, and trying to make life easier for the child by informing and explaining. It is also important to sustain faith in the child and the child's ability to cope with the circumstances and the future, as well as wanting to find out the child's lived reality. All these actions represent a way of reflecting the willingness of the HCPs to facilitate life for each child. When the HCPs enable the child to be present in his/her own treatment, through severe conditions, and support the child in everyday life, then the HCPs will help the child to be involved in his/her own life and promote the child's personal health.
Implications for healthcare professionals
Swanson's Theory of Caring includes processes which at a deeper level suggest actionable interventions that make the theory-practice construction understandable and suitable for clinicians (46). HCPs in pediatric oncology care need to be aware of the effects of the disease on the whole family, i.e., the role of systems for care improvement, provision of QoL, education and support, and empowerment of children and families (41). Above all it is important to underline that the role of participation goes beyond treatment and childhood. Therefore, understanding and awareness of late effects and how survivorship is applied in the context of childhood cancer survivors is critically important to the practice of HCPs. This insight will offer them new possibilities for providing guidance, support, and assistance in enhancing outcomes for childhood cancer survivors and their families (47). In practice, this means that professionals need to help survivors in the transition to a new normality, create hope by nurturing a trustful relationship, support coping by giving knowledge and information, decrease distress, anxiety and pain, show genuine interest in the persons' lives outside the hospital, and have a plan for follow-up (48). The practical transfer of knowledge can advantageously take place via information brochures and educational material with a person-centered adaptation. To improve HCPs' caring behavior, with the aim of increasing the patient's well-being, the above mentioned coding scheme (the CBCS) could be useful (39). However, all efforts presuppose that children are actively involved and listened to, i.e., they are partners in shared decision-making from the point of diagnosis (49).
Strengths and limitations
The study has been performed with a cohort of former patients treated at the same childhood cancer center, which has had a clear care philosophy over decades. Still, the study population is heterogeneous and in retrospective studies researchers always need to take into account the role of time and how the study participants' memory can influence the study results. Based on the demographic data (Table 1) we can conclude that the invited participants who did not answer represent all of the defined subgroups. However, we do not know how these individuals would have answered the questionnaire. We need to be aware of the risk of the possible systematic error and conclusions need to be drawn with caution. To avoid the risk of recall bias another approach is to perform longitudinal studies, quantitative as well as qualitative. Preferably, the study starts at diagnosis and with focus on the role of participation in everyday life during the child's cancer treatment trajectory and at follow-up.
Conclusion
With a large number of children surviving childhood cancer worldwide, numerous investigations have assessed psychological and social adjustments among childhood cancer survivors. The results from this study underline the role of caring from a long-term perspective. The results yield improved understanding of the population of childhood cancer survivors, help draw attention to their challenges, and contribute to their more effective integration into society, helping those individuals' live healthy and positive lives (3, 37). The journey to this healthy life starts by promptly involving the sick child. The role of participation persists through and beyond treatment with a lifelong perspective to foster autonomy for long-term survivorship.
Data availability statement
The data sets presented in this study include personally identifying information that present risks to confidentiality. According to the ethics approval the data cannot be shared and therefore, we do not include an email address where requests for the data set can be sent.
Ethics statement
The participants were given oral and written information about the study before they gave their informed consent to participate. The Regional Research Ethics Board, Gothenburg Sweden, approved the study (Dnr 289-07).
Author contributions
MS contributed in conceptualization, design and methodology of the study. MS, MB, MG and KE were involved in the literature search, data analyzes and reviewed and revised the manuscript. All authors contributed to the article and approved the submitted version.
Funding
The Swedish Cancer Childhood Fund supported funding for data collection and analysis. Futurum paid the publication fee.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Björklund AC, Granlund M, Santacroce SJ, Enskär K, Carlstein S, Björk M. Using icf to describe problems with functioning in everyday life for children who completed treatment for brain tumor: an analysis based on Professionals’ documentation. Front Rehabil Sci. (2021) 2:708265. doi: 10.3389/fresc.2021.708265
2. Norsker FN, Pedersen C, Armstrong GT, Robison LL, McBride ML, Hawkins M, et al. Late effects in childhood cancer survivors: early studies, survivor cohorts, and significant contributions to the field of late effects. Pediatr Clin North Am. (2020) 67(6):1033–49. doi: 10.1016/j.pcl.2020.07.00233131533
3. Kim Y. Exploration of life experiences of positive growth in long-term childhood cancer survivors. Eur J Oncol Nurs. (2017) 30:60–6. doi: 10.1016/j.ejon.2017.08.00129031315
4. Gatta G, Botta L, Rossi S, Aareleid T, Bielska-Lasota M, Clavel J, et al. Childhood cancer survival in Europe 1999–2007: results of eurocare-5–a population-based study. Lancet Oncol. (2014) 15(1):35–47. doi: 10.1016/s1470-2045(13)70548-524314616
5. Bertuccio P, Alicandro G, Malvezzi M, Carioli G, Boffetta P, Levi F, et al. Childhood cancer mortality trends in Europe, 1990-2017, with focus on geographic differences. Cancer Epidemiol. (2020) 67:101768. doi: 10.1016/j.canep.2020.10176832593162
6. Nathan PC, Hayes-Lattin B, Sisler JJ, Hudson MM. Critical issues in transition and survivorship for adolescents and young adults with cancers. Cancer. (2011) 117(10 Suppl):2335–41. doi: 10.1002/cncr.2604221523755
7. National Care Program for Long-Term Follow-up after Childhood Cancer (2022). Available at: https://cancercentrum.se/globalassets/cancerdiagnoser/barn/vardprogram/vp-langtidsuppfoljning-barncancer.pdf (Accessed November 11, 2022).
8. Organisation WH. Ottawa Charter for Health Promotion (1986). Available at: https://www.euro.who.int/__data/assets/pdf_file/0004/129532/Ottawa_Charter.pdf (Accessed November 1, 2022).
9. Almqvist L, Hellnäs P, Stefansson M, Granlund M. “I can play!” young Children's Perceptions of health. Pediatr Rehabil. (2006) 9(3):275–84. doi: 10.1080/1363849050052130317050405
10. Larson RW. Toward a psychology of positive youth development. Am Psychol. (2000) 55(1):170–83. doi: 10.1037//0003-066x.55.1.17011392861
11. Larson RW, Verma S. How children and adolescents spend time across the world: work, play, and developmental opportunities. Psychol Bull. (1999) 125(6):701–36. doi: 10.1037/0033-2909.125.6.70110589300
12. Coster W, Law M, Bedell G, Liljenquist K, Kao YC, Khetani M, et al. School participation, supports and barriers of students with and without disabilities. Child Care Health Dev. (2013) 39(4):535–43. doi: 10.1111/cch.1204623763254
13. Peters VJT, Meijboom BR, Bunt JEH, Bok LA, van Steenbergen MW, de Winter JP, et al. Providing person-centered care for patients with Complex healthcare needs: a qualitative study. PLoS One. (2020) 15(11):e0242418. doi: 10.1371/journal.pone.024241833196659
14. Sundler AJ, Darcy L, Råberus A, Holmström IK. Unmet health-care needs and human rights-a qualitative analysis of Patients’ complaints in light of the right to health and health care. Health Expect. (2020) 23(3):614–21. doi: 10.1111/hex.1303832069375
15. Plage S, Kuskoff E, Hoang N-P, Povey J. Educational participation of primary school children with cancer from a life course perspective: a critical review of the literature. Int J Educ Res. (2022) 114:101990. doi: 10.1016/j.ijer.2022.101990
16. Poirier P, Sossong A. Oncology patients’ and nurses’ perceptions of caring. Can Oncol Nurs J. (2010) 20(2):62–5. doi: 10.5737/1181912x-202626520572428
17. Wilkin K, Slevin E. The meaning of caring to nurses: an investigation into the nature of caring work in an intensive care unit. J Clin Nurs. (2004) 13(1):50–9. doi: 10.1111/j.1365-2702.2004.00814.x14687293
18. Swanson KM. Empirical development of a middle range theory of caring. Nurs Res. (1991) 40(3):165. doi: 10.1097/00006199-199105000-00008
19. Swanson KM. Nursing as informed caring for the well-being of others. Image J Nurs Sch. (1993) 25(4):352–7. doi: 10.1111/j.1547-5069.1993.tb00271.x8288305
20. Wojnar DM. Kristen swanson: Theory of caring. Nursing theorists and their work. 6th ed. St. Louis, MO: Mosby (2006). 769 p.
21. Iranmanesh S, Axelsson K, Sävenstedt S, Häggström T. A caring relationship with people who have cancer. J Adv Nurs. (2009) 65(6):1300–8. doi: 10.1111/j.1365-2648.2009.04992.x19374671
22. Creswell JW, Plano Clark VL. Designing and conducting mixed methods research. 3 ed. Thousand Oaks, CA: SAGE (2018).
23. Stenmarker M, Enskär K, Björk M, Pinkava M, Rolander B, Golsäter M. Childhood cancer survivors: self-reported quality of life during and after the cancer trajectory. Asia Pac J Oncol Nurs. (2020) 7(4):336–45. doi: 10.4103/apjon.apjon_22_2033062828
24. Elo S, Kyngas H. The qualitative content analysis process. J Adv Nurs. (2008) 62(1):107–15. doi: 10.1111/j.1365-2648.2007.04569.x18352969
25. Kline CN, Mueller S. Neurocognitive outcomes in children with brain tumors. Semin Neurol. (2020) 40(3):315–21. doi: 10.1055/s-0040-170886732392601
26. Terwee CB, Bot SD, de Boer MR, van der Windt DA, Knol DL, Dekker J, et al. Quality criteria were proposed for measurement properties of health status questionnaires. J Clin Epidemiol. (2007) 60(1):34–42. doi: 10.1016/j.jclinepi.2006.03.01217161752
27. Hair, Anderson, Tatham, Black. Multivariate data analysis. 5th ed. Upper Saddle River, New Jersey: A Simon & Schuster Company (1998). 118 p.
28. Ferrari A, Thomas D, Franklin AR, Hayes-Lattin BM, Mascarin M, van der Graaf W, et al. Starting an adolescent and young adult program: some success stories and some obstacles to overcome. J Clin Oncol. (2010) 28(32):4850–7. doi: 10.1200/jco.2009.23.809720479411
29. Hodgson DC, Hudson MM, Constine LS. Pediatric hodgkin lymphoma: maximizing efficacy and minimizing toxicity. Semin Radiat Oncol. (2007) 17(3):230–42. doi: 10.1016/j.semradonc.2007.02.00917591570
30. Wojnar DM. Kristen swanson: theory of caring. Nursing theorists and their work. 6th ed. St. Louis, MO: Mosby (2006).
31. Engvall G, Cernvall M, Larsson G, vonsEssen L, Mattsson E. Cancer during adolescence: negative and positive consequences reported three and four years after diagnosis. PLoS One. (2011) 6(12):e29001. doi: 10.1371/journal.pone.002900122194973
32. Zebrack B, Isaacson S. Psychosocial care of adolescent and young adult patients with cancer and survivors. J Clin Oncol. (2012) 30(11):1221–6. doi: 10.1200/jco.2011.39.546722412147
33. Warner EL, Kent EE, Trevino KM, Parsons HM, Zebrack BJ, Kirchhoff AC. Social well-being among adolescents and young adults with cancer: a systematic review. Cancer. (2016) 122(7):1029–37. doi: 10.1002/cncr.2986626848713
34. Cantrell MA, Matula C. The meaning of comfort for pediatric patients with cancer. Oncol Nurs Forum. (2009) 36(6):E303–9. doi: 10.1188/09.Onf.E303-e30919887343
35. Armstrong GT, Stovall M, Robison LL. Long-term effects of radiation exposure among adult survivors of childhood cancer: results from the childhood cancer survivor study. Radiat Res. (2010) 174(6):840–50. doi: 10.1667/rr1903.121128808
36. Brinkman TM, Krasin MJ, Liu W, Armstrong GT, Ojha RP, Sadighi ZS, et al. Long-term neurocognitive functioning and social attainment in adult survivors of pediatric cns tumors: results from the st jude lifetime cohort study. J Clin Oncol. (2016) 34(12):1358–67. doi: 10.1200/jco.2015.62.258926834063
37. Kim Y, Lee KS, Koh KN. Difficulties faced by long-term childhood cancer survivors: a qualitative study. Eur J Oncol Nurs. (2018) 36:129–34. doi: 10.1016/j.ejon.2018.08.00330322503
38. Råberus A, Holmström IK, Galvin K, Sundler AJ. The nature of patient complaints: a resource for healthcare improvements. Int J Qual Health Care. (2019) 31(7):556–62. doi: 10.1093/intqhc/mzy215
39. Mårtensson S, Hodges EA, Knutsson S, Hjelm C, Broström A, Swanson KM, et al. Caring behavior coding scheme based on Swanson’s theory of caring—development and testing among undergraduate nursing students. Scand J Caring Sci. (2021) 35(4):1123–33. doi: 10.1111/scs.12927
40. Darcy L, Enskär K, Björk M. Young children’s experiences of living an everyday life with cancer—a three year interview study. Eur J Oncol Nurs. (2019) 39:1–9. doi: 10.1016/j.ejon.2018.12.00730850132
41. Enskär K, Huus K, Björk M, Granlund M, Darcy L, Knutsson S. An analytic review of clinical implications from nursing and psychosocial research within Swedish pediatric oncology. J Pediatr Nurs. (2015) 30(4):550–9. doi: 10.1016/j.pedn.2014.11.001
42. Enskär K, Björk M, Knutsson S, Granlund M, Darcy L, Huus K. A Swedish perspective on nursing and psychosocial research in paediatric oncology: a literature review. Eur J Oncol Nurs. (2015) 19(3):310–7. doi: 10.1016/j.ejon.2014.10.013
43. Takei Y, Ogata A, Ozawa M, Moritake H, Hirai K, Manabe A, et al. Psychosocial difficulties in adolescent and young adult survivors of childhood cancer. Pediatr Int. (2015) 57(2):239–46. doi: 10.1111/ped.1249525203461
44. Barnett M, McDonnell G, DeRosa A, Schuler T, Philip E, Peterson L, et al. Psychosocial outcomes and interventions among cancer survivors diagnosed during adolescence and young adulthood (Aya): a systematic review. J Cancer Surviv. (2016) 10(5):814–31. doi: 10.1007/s11764-016-0527-626920873
45. Imms C, Granlund M, Wilson PH, Steenbergen B, Rosenbaum PL, Gordon AM. Participation, both a means and an End: a conceptual analysis of processes and outcomes in childhood disability. Dev Med Child Neurol. (2017) 59(1):16–25. doi: 10.1111/dmcn.1323727640996
46. Tonges M, Ray J. Translating caring theory into practice: the Carolina care model. J Nurs Adm. (2011) 41(9):374–81. doi: 10.1097/NNA.0b013e31822a732c21881444
47. Song A, Fish JD. Caring for survivors of childhood cancer: it takes a village. Curr Opin Pediatr. (2018) 30(6):864–73. doi: 10.1097/mop.000000000000068130124580
48. Enskär K, Darcy L, Björk M, Knutsson S, Huus K. Experiences of young children with cancer and their parents with Nurses’ caring practices during the cancer trajectory. J Pediatr Oncol Nurs. (2020) 37(1):21–34. doi: 10.1177/1043454219874007
Keywords: childhood cancer survivor, child, adolescents, swanson caring theory, participation, every day life, long term health conditions
Citation: Stenmarker M, Björk M, Golsäter M and Enskär K (2023) Everyday life during the childhood cancer trajectory—childhood cancer survivors' descriptions of the role of caring support. Front. Rehabil. Sci. 4:1098933. doi: 10.3389/fresc.2023.1098933
Received: 15 November 2022; Accepted: 5 June 2023;
Published: 16 June 2023.
Edited by:
Jochen Rössler, Insel Gruppe AG, SwitzerlandReviewed by:
Mateusz Krystian Grajek, Medical University of Silesia in Katowice, PolandStefanie Plage, The University of Queensland, Australia
© 2023 Stenmarker, Björk, Golsäter and Enskär. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Margaretha Stenmarker bWFyZ2FyZXRoYS5zdGVubWFya2VyQHJqbC5zZQ==