 Per Trads Ørskov1*
Per Trads Ørskov1* Eik Runge1
Eik Runge1 Trine Theresa Holmberg Sainte-Marie1,2
Trine Theresa Holmberg Sainte-Marie1,2 Mathias Torp Ernst1,3
Mathias Torp Ernst1,3 Lars Clemmensen1,2
Lars Clemmensen1,2 Caroline Høier Dalsgaard1
Caroline Høier Dalsgaard1 Mia Beck Lichtenstein1,3
Mia Beck Lichtenstein1,3 Stéphane Bouchard2,4,5
Stéphane Bouchard2,4,5- 1Research Unit for Digital Psychiatry, Center for Digital Psychiatry, Mental Health Services in the Region of Southern Denmark, Odense, Denmark
- 2Department of Clinical Research, University of Southern Denmark, Odense, Denmark
- 3Department of Psychology, University of Southern Denmark, Odense, Denmark
- 4Department of Psychoeducation and Psychology, Université du Québec en Outaouais, Gatineau, Canada
- 5Centre de recherche, Centre Intégré de Santé et de Services Sociaux de l’Outaouais, Gatineau, Canada
Background: Social anxiety disorder (SAD) has a high prevalence and an early onset. It often persists well into adulthood, turning into a chronic disorder. Cognitive behavioral therapy (CBT) is effective in treating SAD, but real-life exposure conducted as part of CBT is often costly and time-consuming, and imaginary exposure might lack realism and intensity. Virtual reality (VR)-based exposure using 360° video offers a promising way to deliver exposure therapy.
Objective: To develop a complete psychotherapeutic treatment program including CBT with VR-based exposure using 360° videos (CBT-ExpVR) for adult patients with SAD and to test the treatment effect using the Social Interaction Anxiety Scale (SIAS) as the primary outcome.
Methods: This three-arm randomized controlled trial involved 51 participants who were recruited through self-referral. The interventions took place at Center for Digital Psychiatry in Denmark. Participants were randomized via computer program to CBT-ExpVR, CBT with in vivo exposure (CBT-Exp), or an active control group offered VR relaxation (RlxVR). Afterwards, participants assigned to RlxVR were re-randomized to one of the two CBT interventions. Allocation was not blinded.
Results: Intention-to-treat analysis showed that participants receiving CBT-ExpVR reported significantly fewer symptoms of social anxiety at post-treatment compared to pre-treatment, β = −14.89, 95% CI (−18.64, −11.14), p < 0.0001. At post-treatment, no difference in treatment effect was found between CBT-ExpVR and CBT-Exp, β = 3.643, 95% CI (−1.727, 9.013), p = 0.1839. However, CBT-ExpVR was more effective than RlxVR, β = −11.537, 95% CI (−16.163, −6.911), p < 0.0001. Dropout rates post-treatment were 16% (CBT-ExpVR), 38% (CBT-Exp), and 20% (RlxVR). No harms were registered during the study.
Conclusion: CBT-ExpVR represents an effective treatment for SAD comparable to standard CBT treatment. CBT-ExpVR was reported as less costly and requiring less effort by the therapist compared to CBT-Exp. Thus, VR-based exposure might pave the way for a broader implementation of exposure in psychotherapeutic interventions for social anxiety by providing easy and low-cost access to exposure scenarios.
Clinical Trials Registration: https://clinicaltrials.gov/study/NCT03973541, identifier NCT03973541.
1 Introduction
1.1 Social anxiety disorder and current treatment practice
Social anxiety disorder (SAD) describes an exaggerated and persistent fear of attracting attention from others. It is characterized by a fear of embarrassment and humiliation and often leads to avoidance of evaluative social interaction (World Health Organization, 1992). SAD is a common yet underreported mental disorder with a lifetime prevalence of 5.5% in high-income countries and a somewhat lower prevalence in upper-middle (2.9%) and low/low-middle income countries (1.6%) (D. J. Stein et al., 2017). It has an early onset, typically in mid-adolescence between 12 and 16 years of age (Fehm, Pelissolo, Furmark and Wittchen, 2005), and often persists to become a chronic disorder in adulthood (Stein and Stein, 2008). Approximately 70%–80% of individuals with SAD have a comorbid disorder such as substance abuse, depression, or attention deficit hyperactivity disorder (ADHD) (Heimberg and Magee, 2014). Furthermore, SAD is significantly associated with suicidal ideation (Olfson et al., 2000). It is, therefore, important to provide effective interventions for SAD.
The gold standard treatment for SAD is cognitive behavioral therapy (CBT) (M. G. Craske and Stein, 2016; Hofmann and Smits, 2008; M. B; Stein and Stein, 2008; Wolitzky-Taylor and LeBeau, 2023) and medical interventions (Emmelkamp, Meyerbröker and Morina, 2020; Pelissolo et al., 2019; Schneier and Goldmark, 2015). Only 30%–50% of individuals with SAD seek treatment (M. B. Stein and Stein, 2008), however, and they often wait years or even decades before seeking treatment (Wang et al., 2005) because they fear negative evaluation by health professionals or believe their condition is untreatable (Bruch, Hamer and Heimberg, 1995).
CBT for SAD includes various psychotherapeutic strategies such as building a therapeutic alliance, individual case conceptualization, addressing dysfunctional thoughts, and, most importantly, exposure. Exposure has traditionally been conducted either in vivo (i.e., directly facing the feared situation) or through imaginary strategies (i.e., imagining the feared situation). In vivo exposure is effective yet somewhat costly (Miloff et al., 2016), time-consuming (Emmelkamp, 2005), and may threaten patient confidentiality (Anderson, Jacobs and Rothbaum, 2004). Furthermore, patients are often unwilling to expose themselves to real-life situations because they consider it too aversive (Horigome et al., 2020; Olfson et al., 2000). Conversely, imaginary exposure may lack realism and intensity for some people (Hodges et al., 1995). Conducting exposure in virtual reality may help overcome these difficulties.
1.2 Virtual reality-based exposure therapy
Virtual reality (VR) is a technology with immersive qualities that enables the user to experience a sense of presence or the illusion of being there in the virtual environment instead of the psychotherapist’s office. VR scenarios can be very lifelike and realistic, and situational factors (e.g., the reactions of others) can be controlled by the therapist (Bouchard et al., 2017). Because patients are less apprehensive of virtual stimuli, they are willing to face difficult situations more readily than in real life. This might enable the patient to both engage in more adaptive behaviors and act in ways that exceed their own, often rigid, social norms (Clemmensen et al., 2020).
Meta-analyses generally find small and non-significant pooled effect sizes when comparing CBT with exposure in VR to CBT with exposure in vivo, suggesting comparable effects between the two forms of intervention. The base of evidence is still somewhat weak, however, with clinical trials varying in size and methodological quality (Caponnetto, Triscari, Maglia and Quattropani, 2021; Carl et al., 2019; Chesham, Malouff and Schutte, 2018; Horigome et al., 2020; Kampmann, Emmelkamp and Morina, 2016; Shahid, Kelson and Saliba, 2024; Wechsler, Kümpers and Mühlberger, 2019; Wong, Lai and Qin, 2023).
Most trials involving VR-based exposure for the treatment of SAD have used VR stimuli consisting of computer-generated environments that allow social interaction (Anderson et al., 2013; Bouchard et al., 2017; Kampmann, Emmelkamp, Hartanto, et al., 2016; Klinger et al., 2005) or combined with videos of audiences designed for fear of public speaking (Anderson et al., 2013). Despite rapid improvement in the quality of computer-generated virtual environments and the avatars that inhabit them, the VR-stimuli used in research have tended to lag behind those in the cinema or videogame industries. Consequently, the representational quality and realism of computer-generated environments used in VR to simulate social interactions have been lower than video recordings of real humans.
A new development in VR is the use of 360° videos that are recorded with an omnidirectional camera in real life to recreate an entire scene. When the video is shown in a VR-headset, the user can look around in the scene from the camera’s vantage point. Studies comparing 360° video with computer-generated images have shown that people tend to rate 360° videos as more realistic (Melo, Vasconcelos-Raposo and Bessa, 2018). Having human actors talk and interact in the scene can make the person immersed in VR feel as if they are being talked to and are interacting with other people. By editing and sampling video footage and allowing the therapist to switch between multiple scenes, the VR-setup can give the impression of bidirectional social interactions, potentially making scenes very believable and real (Della Libera, Simon, Larøi, Quertemont and Wagener, 2023; Ernst et al., 2024; Holmberg et al., 2020).
Few trials have been conducted using VR-based 360° videos in CBT for the treatment of SAD. Zainal, Chan, Saxena, Taylor, and Newman (2021) developed a self-guided VR exposure therapy for SAD that utilized 360° videos, standard audio scripts for instruction and psychoeducation, and handouts for homework between sessions. They found that an 8-session, self-guided intervention using 360° videos for exposure was more effective for symptom reduction than waitlist control, but they did not include an active control condition. Study protocols have been published for randomized controlled trials of active gold-standard treatment control versus VR-based 360° videos for exposure as part of CBT (Arnfred et al., 2021; Ørskov et al., 2022), but results have not yet been published.
The present study differs from the earlier study by Zainal and colleagues (2021) by testing the effect of a therapist-led CBT with VR-based exposure and by being a full-scale trial comparing an experimental condition to an active control (i.e., relaxation) (Clemmensen et al., 2020; Hofmann and Smits, 2008) and a gold-standard treatment control (i.e., individual CBT with exposure conducted in vivo) (Bouchard et al., 2017; Wolitzky-Taylor and LeBeau, 2023).
1.3 Study aim and hypotheses
This study aimed to test CBT with VR-based exposure for patients with SAD by comparing three groups: one group receiving CBT in combination with VR-based exposure (CBT-ExpVR), one group receiving CBT in combination with in vivo exposure (CBT-Exp), and one group receiving VR relaxation (RlxVR). The predefined hypotheses of the study were (Clemmensen et al., 2020):
- CBT-ExpVR will statistically significantly reduce symptoms of SAD (primary hypothesis).
- CBT-ExpVR will be more effective than both CBT-Exp and RlxVR at the end of treatment (secondary hypothesis).
- An effect on symptom reduction will be sustained at 6-month follow-up (secondary hypothesis).
2 Materials and methods
The study is reported in accordance with CONSORT guidelines for reporting multi-arm parallel-group randomized trials (Juszczak, Altman, Hopewell and Schulz, 2019). Furthermore, we followed the Template for Intervention Description and Replication (TIDieR) (Hoffmann et al., 2014).
2.1 Study design
The study was a three-arm randomized controlled trial comparing CBT-ExpVR (experimental), CBT-Exp (gold-standard treatment control), and a group receiving RlxVR (active control). Here, RlxVR is considered a treatment in its own right, but it is often also considered a placebo control (Hofmann and Smits, 2008). The study was conducted at the Center for Digital Psychiatry, Mental Health Services in the Region of Southern Denmark.
2.2 Participants and recruitment
The sample consisted of 51 adults diagnosed with SAD. Initially, 55 participants were enrolled in the study, but only 51 showed up for the first assessment and treatment session. There were 37 females (CBT-ExpVR: 14, CBT-Exp: 11, RlxVR: 12) and 14 males (CBT-ExpVR: 3, CBT-Exp: 5, RlxVR: 6). Sex was determined by the social security number, and participants were not asked about their gender identity. The mean age was 33.9 years (SD = 11.5).
Participants were self-referred via recruitment through various media, i.e., the study website, flyers and posters at universities, national TV news, videos and pictures posted on social media, job centers, and institutes and websites promoting mental health. Participants first completed an online version of the Social Interaction Anxiety Scale (SIAS) through the survey system SurveyXact (www.surveyxact.dk). If their total score reached 22 or above (total score range is 0–80), participants were asked if they would like to be invited to a diagnostic interview for further participation. If they responded positively, an invitation was sent through the Danish secure e-mail system e-Boks. Interviews were primarily face-to-face, but a few were conducted through video calls due to the COVID-19 pandemic. The diagnosis of SAD was corroborated by a trained psychologist using the short version of the semi-structured diagnostic interview Present State Examination (PSE), supplemented with the anxiety section of the full version.
The participants had to meet the following inclusion criteria: (a) aged 18 years or older, (b) able to understand and speak Danish, and (c) meeting the diagnostic criteria for Social Anxiety Disorder according to the ICD-10 (F40.1). We used the Danish version of ICD-10 as ICD-11 was not yet officially translated, but we later reviewed all cases and confirmed that participants would have met the ICD-11 criteria for SAD. The exclusion criteria were: (a) self-reported diagnosis of psychosis-related disorder, autism spectrum disorder (ASD), severe depression, or substance dependence disorder; (b) current participation in another psychotherapeutic treatment; (c) experiencing severe unwanted negative symptoms induced by immersions in VR (i.e., cybersickness); and (d) reporting significant changes in prescribed psychopharmacological medication within the last 6 months or during the study.
2.3 Procedure
The study was approved by the Research Ethics Committee in the Region of Southern Denmark (approval number S-20180085) and was conducted from December 2019 to March 2022. Before the first treatment session, participants were given verbal information about the project and signed an informed written consent. Once participants were allocated, they were manually registered with an ID number in REDCap (Research Electronic Data Capture). All the data were collected through REDCap. Questionnaires were administered to the participants on iPads by the therapist in charge of the intervention. The assessments were conducted before each treatment session except for the last treatment session, where the assessment was administered at the end of the treatment session. Six-month follow-up was conducted online, and participants were sent a link to an online questionnaire via secure e-mail. Participants who completed the 6-month follow-up were awarded a gift certificate worth 500 DKK (∼70 USD).
2.3.1 Interventions
CBT-ExpVR and CBT-Exp comprised ten 1-h treatment sessions over 10 weeks (one session every week). The treatment was face-to-face, individual, and guided by a trained psychologist. Four different psychologists were involved with the therapy, all of whom had experience with either face-to-face CBT or internet-based CBT. Once every 2 weeks, the psychologists were supervised by an external supervisor who had extensive experience with CBT but no specific experience with conducting exposure in VR.
RlxVR consisted of five treatment sessions over 10 weeks (one session every 2 weeks). The relaxation was guided both by trained psychologists and one psychologist student. At post-treatment, participants who completed the RlxVR (active control) were re-randomized into one of the CBT groups (CBT-ExpVR or CBT-Exp) in a 1:1 ratio.
CBT followed a manual developed for the current study (Clemmensen et al., 2021) and was based on the inhibitory learning approach (Craske et al., 2014) and the Bouchard et al. (2017) adaptation of Clark and Well’s model (Clark and Wells, 1995). The themes covered in therapy were the maintaining processes of social anxiety, negative automatic thoughts, the shifting of attention from self-focus to external focus, safety behaviors, expectancy violation, and functional analysis. The first three sessions centered on establishing the therapeutic alliance, defining treatment goals, and psychoeducation. Sessions four to nine involved exposure either in VR or in vivo. The 10th and last session involved relapse prevention. The interventions involved homework that comprised reading and worksheets but not exposure.
During exposure in VR, participants were equipped with the VR standalone headset Oculus Go (Graphics card: Adreno 530 GPU) (Facebook Technologies, US). This headset has a 90˚field of view horizontally, the resolution is 1280 × 1440 per eye, and the tracking capabilities are 3-DOF (built-in). The audio was delivered through the built-in speakers of the headset. Three 360° video scenarios recorded in 4K (3840 × 3840) were available for exposure and re-created the following social settings: 1) eating lunch in a workplace canteen, 2) going on a bus ride, and 3) participating in a job interview (see screenshots from the scenarios in supplementary files). Each scenario consisted of a series of scenes, starting with a neutral scene and followed by scenes that prompted social interaction. The videos were produced by Khora (https://khora.com/) and were available through an app on the VR-headset. Participants were instructed by the therapist to select a scenario. The therapist then followed the exposure on an iPad using the casting function in the Oculus Go app and controlled the progression of the exposure using the controller to choose different scenes and timing the transition from one scene to the next based on the participant’s behavior. In the job interview, for example, a scene transition would prompt the next question from the interviewers, and the therapist would adjust the timing of the transition to the participant’s answers to the interview questions. A few scene transitions required participants to make choices by using a pointer at the center of their gaze, choosing the options “yes” or “no” (e.g., to sit down at a table with colleagues in the canteen or to ask directions from the bus driver). Some transitions were from one scene to one of several other scenes, e.g., in the canteen scenario, the application randomly chose one of three scenarios where the colleagues would be either friendly, neutral, or hostile. With only three scenarios, the participants were exposed to the same scenarios more than once. The therapist added variation by giving different assignments. For example, the job interview might be about different jobs, and on the bus ride, the participant might be told to confront fellow passengers who were acting rudely or refusing to give up their seat to an older adult who had requested a place to sit down.
The in vivo exposure was conducted inside or outside the therapist’s office. It involved asking directions, initiating conversations, buying items at a drugstore and returning them afterwards, initiating awkward conversations with colleagues, and making oral presentations. Most exposures were conducted at the Center for Digital Psychiatry and surrounding areas, including the university hospital and campus.
Participants in the VR-relaxation placebo control group were immersed in a 360° relaxation scenario that depicted an underwater point of view in the Red Sea with dolphins swimming in groups. Dolphin Swim Club filmed and developed the scenario (https://thedolphinswimclub.com/medical-vr/). Participants were instructed to stay immersed in the environment for at least 15 min.
2.3.2 Treatment fidelity
A detailed treatment manual was produced to ensure treatment standardization (Clemmensen et al., 2021). The manual included several worksheets for use at specific times during the treatment program. Therapists were supervised once every 2 weeks, which also helped to ensure fidelity. In addition, the principal investigator (LC/PTØ) had weekly meetings with the therapists to follow up on treatment progress and maximize adherence. The research protocol stated a priori that 10% of sessions would be audio-recorded to ensure adherence to the manual and that recorded sessions would be evenly distributed across the treatment stages. The protocol did not specify how the audio-recordings would be evaluated, and no formal checklists or adherence metrics were defined in advance. Approximately 2%–4% of the sessions were audio-recorded at the therapist’s discretion and were evaluated during supervision. The supervisor provided individual feedback on the therapeutic practice and overall adherence to the manual. No standardized fidelity tools were used.
2.4 Measures
The following sections present the questionnaires used as outcomes and covariates in the trial. We had one primary outcome measure, three secondary outcome measures, and five other outcome measures.
2.4.1 Primary outcome
The Social Interaction Anxiety Scale (SIAS) measures the severity of social anxiety symptoms by assessing cognitive, affective, and behavioral responses to social interaction. It consists of 20 items that are scored on a five-point Likert scale (0 = not at all, 1 = slightly, 2 = moderately, 3 = very, 4 = extremely). Thus, the total score ranges from 0 to 80, where a higher score reflects more severe symptoms. The SIAS has shown good internal consistency (Cronbach’s α ranged from 0.88–0.93) (Brown et al., 1997). The SIAS was collected at baseline, at every treatment session, post-treatment, and at 6-month follow-up. The primary endpoint was post-treatment. Only two groups (CBT-ExpVR and CBT-Exp) were compared at the 6-month follow-up.
2.4.2 Secondary outcomes
The EQ-5D-5L measures standardized health status through five dimensions (mobility, self-care, usual activities, pain/discomfort, and anxiety/depression), each of which has five levels (1 = no problems, 2 = slight problems, 3 = moderate problems, 4 = severe problems, 5 = unable to/extreme problems). Based on the participant’s answers to the dimension levels, an index score can be applied (Jensen et al., 2021). Respondents are also asked to rate their overall health on a visual analog scale (VAS) from 0 (the worst health you can imagine) to 100 (the best health you can imagine). The EQ-5D-5L has shown excellent test-retest reliability (Feng, Kohlmann, Janssen and Buchholz, 2021) and good internal consistency (Cronbach’s α = 0.79) (Seng et al., 2020). In the two CBT groups, the EQ-5D-5L was measured at baseline, session 3, session 7, post-treatment, and at 6-month follow-up. In the RlxVR group, it was measured at baseline, session 3, session 7, and post-treatment.
The Beck Depression Inventory II (BDI-II) measures symptoms of depression and comprises 21 items, each scored on a Likert scale ranging from 0 to 3. The BDI-II global score ranges from 0 to 63, with a total score between 14 and 19 indicating “mild,” from 20 to 28 indicating “moderate,” and from 29 to 63 indicating “severe” depression. The BDI-II has shown good internal consistency (Cronbach’s α = 0.92) (Steer, Clark, Beck and Ranieri, 1999). In the two CBT groups, the BDI-II was measured at baseline, session 3, session 7, post-treatment, and at 6-month follow-up. In the RlxVR group, BDI-II was measured at baseline, session 3, session 7, and post-treatment.
The Specific Work for Exposure Applied in Therapy (SWEAT) measures the cost and effort required to conduct exposure. It comprises 11 items, each scored on Likert scales ranging from 0 (not at all) to 6 (totally), and provides a total score ranging between 0 and 66. The questionnaire has shown good internal consistency (Cronbach’s α = 0.83) (Robillard, Bouchard, Dumoulin and Guitard, 2011). The SWEAT questionnaire was completed by the therapists after each exposure session in the two CBT groups, thus six times in total. The instrument was not used for the RlxVR group as no exposure was conducted.
2.4.3 Other outcomes
The Alcohol Use Disorders Identification Test (AUDIT) is a 10-item self-administered questionnaire screening for risk of alcohol harm. Each item is scored on a 5-point Likert scale, ranging from 0–4. Thus, the total score ranges from 0 (low risk of alcohol harm) to 40 (extreme dependency on alcohol). The AUDIT has shown good internal consistency (Cronbach’s α = 0.93) (Saunders et al., 1993). The AUDIT was measured at baseline in all groups.
The Drug Use Disorders Identification Test (DUDIT) is an 11-item self-administered questionnaire screening for risk of drug-related problems. Each item is scored on a five-point Likert scale, ranging from 0–4. Thus, the total score ranges from 0 (low risk of drug-related problems) to 44 (extreme drug-related problems). The DUDIT has shown good internal consistency (Cronbach’s α > 0.90) (Hildebrand, 2015). The DUDIT was measured at baseline in all groups.
The Social Responsiveness Scale (SRS-2) measures the symptoms and severity of autism spectrum disorder and comprises 65 items relating to five domains (social awareness, social cognition, social communication, social motivation, and restricted interests and repetitive behavior). Each item is scored on a four-point Likert scale, ranging from 1 (not true) to 4 (almost always true), giving a total score ranging from 65 to 260. SRS-2 can be used in adults and children, and a validation study of the adult version showed good internal consistency (Cronbach’s α = 0.89) (Bölte, 2012). The SRS-2 was measured at baseline in all groups.
The Adult ADHD Self-Report Scale (ASRS) is an 18-item self-administered scale used for measuring symptoms of Attention Deficit Hyperactivity Disorder (ADHD) and comprises two sub-scales (part A and part B). Part A consists of six items scored on a five-point Likert scale, ranging from 0 to 4 (0 = never, 1 = rarely, 2 = sometimes, 3 = often, 4 = very often), giving a total score for part A ranging from 0 to 24. Part B consists of 12 items scored on a five-point Likert scale, giving a total score for part B ranging from 0 to 48. Part B is used to provide additional cues for the patient’s symptoms (Kessler et al., 2005). The total score of the ASRS ranges from 0 to 72. The ASRS has shown good internal consistency (Cronbach’s α = 0.88) (Adler et al., 2006). The ASRS was measured at baseline in all groups.
The Working Alliance Inventory-Short Revised (WAI-SR) is a 12-item questionnaire used to measure therapeutic alliance. It pertains to three domains (goal, task, bond), each consisting of four items answered on a five-point Likert scale (1 = seldom, 2 = sometimes, 3 = fairly often, 4 = often, 5 = very often). The total score ranges between 12 and 60, where a higher score indicates a better therapeutic alliance. The WAI-SR has shown good internal consistency (Cronbach’s α = 0.91) for the total score (Hatcher, 2006). Both a therapist-rated version and a patient-rated version of the WAI-SR were completed after the final session in each group (session 10 for the CBT groups and session five for the RlxVR group).
2.5 Sample size, randomization, and blinding
The study included a total of 51 patients. Recruitment was significantly impacted by challenges posed by the COVID-19 pandemic, which hindered the ability to achieve the originally intended sample size of 90 participants as specified in the clinical trial registration. Despite extending the study period, it was impossible to reach the targeted number of participants. A post hoc power analysis revealed that the study achieved a statistical power of 66%.
Participants were allocated into the three arms in a ratio of 1:1:1 using OPEN randomize, an online service delivered by the Open Patient data Explorative Network (OPEN), Region of Southern Denmark. The protocol stated that participants were to be randomly assigned while controlling for gender, age, and baseline severity of SAD, but no stratification was used in the actual trial. As we planned for a relatively large sample size, we assumed that a non-stratified randomization would result in comparable baseline measures across groups. Randomization was blocked to achieve a balance between the treatment arms; block sizes were 2, 4, and six and were concealed while the study was running. Post-treatment, participants in the RlxVR group were randomized 1:1 to the CBT groups. This was done partly to reduce the number of required participants and, for ethical reasons, to offer CBT to all participants.
Participants were invited to the first session by e-Boks and were informed about their allocation at the same time. They were not blind to their treatment allocation for any of their assessments. Keeping the allocation blind for patients and clinicians until the first exposure session was not feasible.
2.6 Statistical methods
The statistical analysis was conducted in accordance with a statistical analysis plan (SAP) that was registered at osf.io before data analysis was started. The statistical methods are summarized here, and for further details, we refer to the SAP (https://osf.io/zakdb). Intention-to-treat (ITT) analyses were made based on all included participants. The analyses were performed using mixed effects linear regression models with intercepts as random effects. This is the simplest mixed effects linear regression model and assumes that intercepts vary between participants. The models can take into account that participants in the RlxVR group were later randomized to one of the CBT groups. The fixed effects were time (as a categorical variable), treatment, and the interaction between time and treatment. Separate analyses were made for SIAS, EQ-5D-5L, and BDI-II. In addition to a model involving the interaction between time and treatment, we also tested a simpler model without the interaction term. We used a likelihood ratio test to determine whether the complex model involving the interaction performed better than the simple model.
Two sensitivity analyses were performed for the primary outcome measure. In the first sensitivity analysis, we compared CBT-ExpVR, CBT-Exp, and the RlxVR as in the ITT analysis, but only the original allocation was considered, and the analysis disregarded the data collected after the second randomization. This analysis was a more restricted approach than the original analysis. In the second sensitivity analysis, we only compared CBT-ExpVR to CBT-Exp, and we disregarded that some participants came from the group receiving the placebo treatment. The second sensitivity analysis was more lenient than the original analysis.
We repeated the original analysis for the primary outcome, adjusting for the following covariates: ASRS, AUDIT, DUDIT, and SRS-2. In addition to the ITT analysis, we also conducted a per-protocol analysis of the participants who adhered to the intervention. Adherence to the intervention was defined as completing at least six out of 10 sessions (exposure occurred at sessions 4–9) and completing the interventions within 15 weeks.
The WAI-SR at post-treatment was compared between CBT groups by linear regression with robust standard errors to account for repeated participants from RlxVR. A linear mixed effects regression model performed comparisons for SWEAT for an overall treatment difference, taking both therapist and patient into account as random intercepts, with the hypothesis that CBT-ExpVR would be more practical involving lower cost and less effort than CBT-Exp.
Model validation in the mixed effects linear regression model was performed by inspecting normal quantile-quantile plots of residuals to assess normality and plotting residuals against fitted values to check for homoscedasticity.
All statistical analyses were carried out in R 4.4.2 except for the tests related to the descriptive statistics in Table 1, which were carried out in Stata.
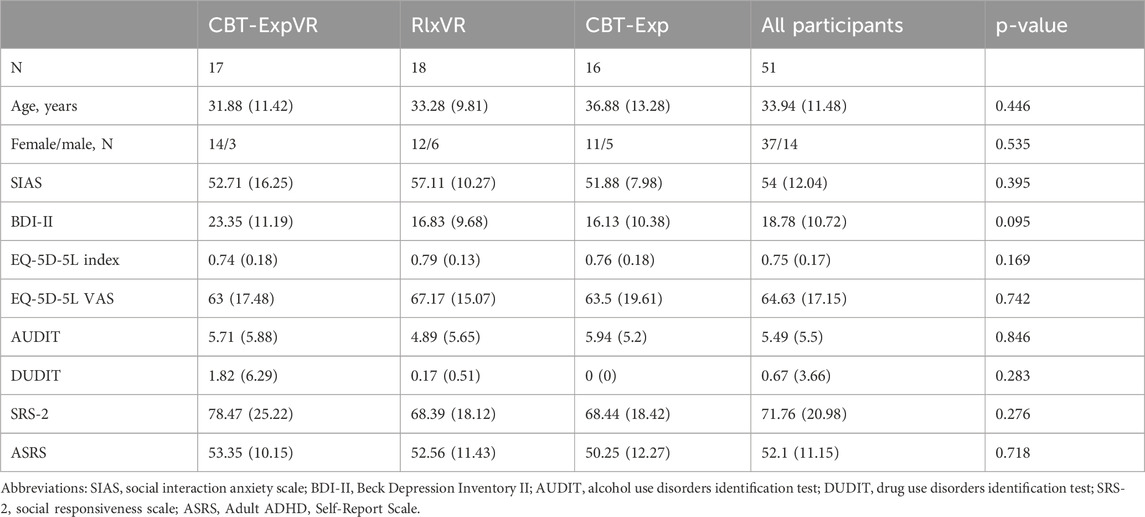
Table 1. Baseline characteristics for the study participants according to their allocation at baseline to CBT with VR based exposure (CBT-ExpVR), VR relaxation (RlxVR), or CBT with in vivo exposure (CBT-Exp). Data are means and standard deviations unless otherwise stated.
3 Results
3.1 CONSORT flowchart and baseline data
Table 1 describes the baseline characteristics and allocation for the 51 participants. The chi-squared test and one-way independent ANOVA with bootstrap showed no significant group differences at baseline. Figure 1 presents the CONSORT flowchart of the study. The attrition rate at post-treatment was 16% for CBT-ExpVR, 38% for CBT-Exp, and 20% for RlxVR.
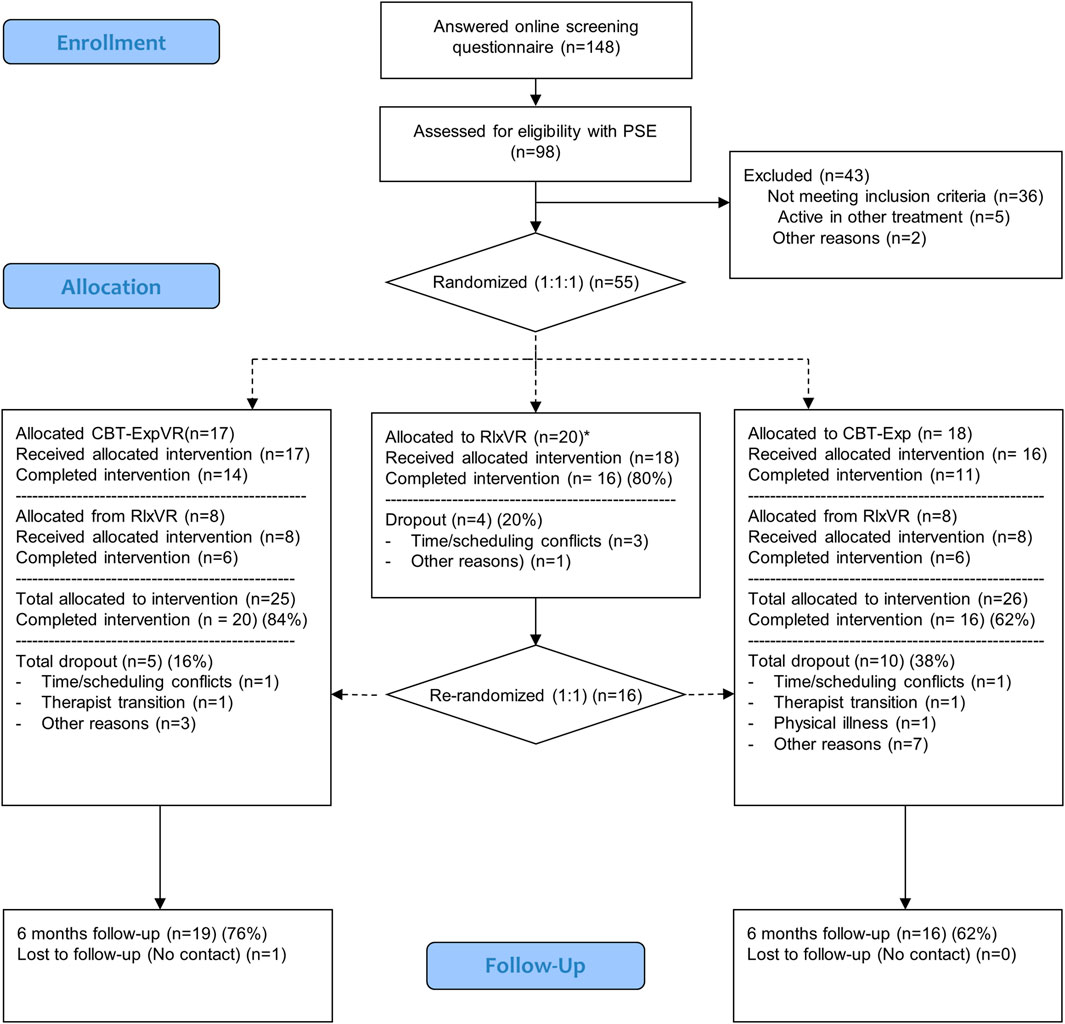
Figure 1. CONSORT flow diagram. Abbreviations: CBT-ExpVR = CBT with VR-based exposure, RlxVR = VR relaxation, CBT-Exp = CBT with in vivo exposure * Two participants were allocated directly to the placebo group and were not randomized as the rest of the participants; this decision was made due to time constraints of the recruitment. When they finished the placebo intervention, participants were randomized correctly to one of the CBT interventions.
3.2 Model selection and validation
We calculated the interclass correlation coefficient (ICC) for the null model for all outcomes and analyses. As specified in the SAP, our models had repeated measurements (level 1) nested within individuals (level 2). ICC ranged between 0.505 and 0.783, indicating that a large proportion of the variance could be attributed to the group (in this case, the participants). Thus, there was good reason to conduct multilevel analyses. For the secondary outcome measure SWEAT, we calculated the ICC for the null model, having repeated measurements (level 1) nested within therapist (level 2). The ICC was considerably lower (0.077), indicating that little variance was attributed to the group (in this case, the therapist) and indicating no compelling reason for the model to take the therapist into account; however, we chose to retain the therapist in the model. Comparisons between the complex model involving interaction between time and treatment and the simpler model without the interaction term showed that the more complex model was significantly better for SIAS [F (14, 436.88) = 2.839, p < 0.001] but performed similarly to the simple model for EQ-5D-5L index [F (7, 221.6) = 0.955, p = 0.4651], EQ-5D-5L VAS [F (7, 219.12) = 0.9295, p = 0.4844], and BDI-II [F (7, 218.14) = 1.6516, p = 0.1224]. Consequently, we report the results of the more complex model for all outcomes as this was the best fit for the primary outcome. Assumptions were checked for the statistical methods. Specifically, we checked the normality and homoscedasticity of the residuals and found that the distributional assumptions for running the analyses were met.
3.3 Primary outcome
Table 2 presents the change in SIAS scores for the CBT-ExpVR group, first for pre-to post-treatment and then for pre-treatment to 6-month follow-up, i.e., addressing the first and third hypotheses of the study. The first hypothesis postulated that CBT with VR-based exposure would statistically significantly reduce symptoms of SAD from pre- to post-treatment (primary hypothesis). The results confirm this hypothesis. The third hypothesis postulated that any improvement on SIAS scores for CBT with VR-based exposure would be sustained at the 6-month follow-up. The results again confirm this hypothesis, showing a significant reduction in SIAS score from pre-treatment to 6-month follow-up.
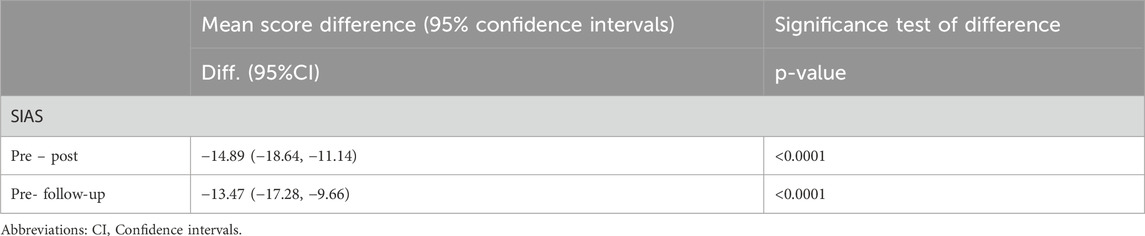
Table 2. Mean change in Social Interaction Anxiety Scale (SIAS) scores from pre-treatment to post-treatment, and from pre-treatment to 6-month follow-up for the treatment arm receiving CBT with VR-based exposure (CBT-ExpVR).
Table 3 as well as Figure 2 presents the scores at pre-treatment, post-treatment, and 6-month follow-up for CBT-ExpVR, CBT-Exp, and RlxVR. These results address the study’s second hypothesis, postulating that CBT-ExpVR at post-treatment would be more effective than CBT-Exp and RlxVR. While there was no significant difference between CBT-ExpVR and CBT-Exp at post-treatment, the participants receiving CBT-ExpVR had significantly fewer anxiety symptoms (a lower SIAS score) than those receiving RlxVR.
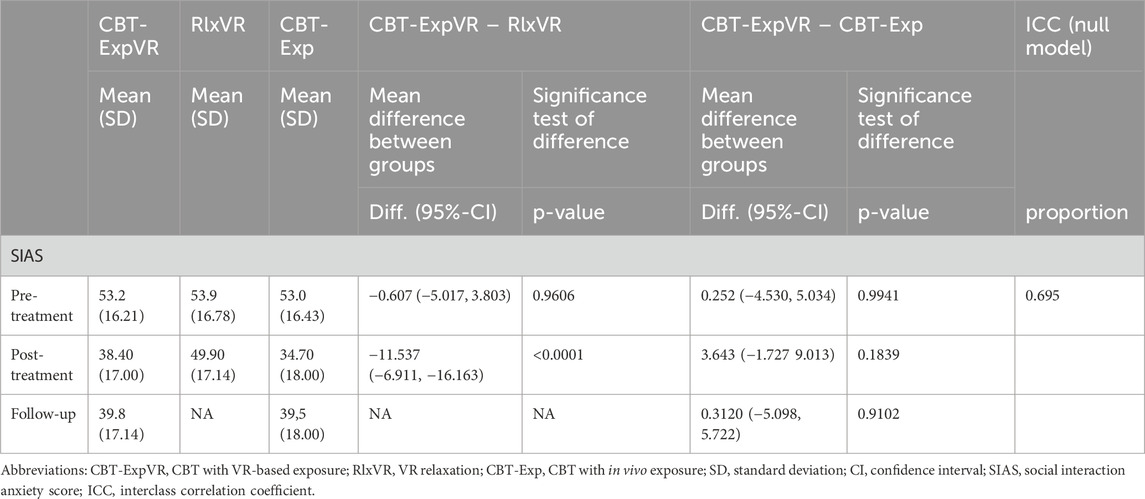
Table 3. Between-group comparisons of mean SIAS scores at pre-treatment, post-treatment, and follow-up.

Figure 2. Change in SIAS mean score over the study period for participants allocated to CBT with VR-based exposure (CBT-ExpVR), CBT with in vivo exposure (CBT-Exp), or VR relaxation (RlxVR). Error bars representing 95% CI.
3.4 Secondary outcomes
Table 4 presents the results for the mixed effect linear regression models analyzing changes in EQ-5D-5L index, EQ-5D-5L VAS, and BDI-II scores for the group receiving CBT-ExpVR. The EQ-5D-5L index scores showed a significant improvement from pre-to post-treatment, indicating improved health status. The small improvement in the EQ-5D-5L VAS score did not quite reach statistical significance. BDI-II scores showed a significant reduction in depressive symptoms with CBT-ExpVR.
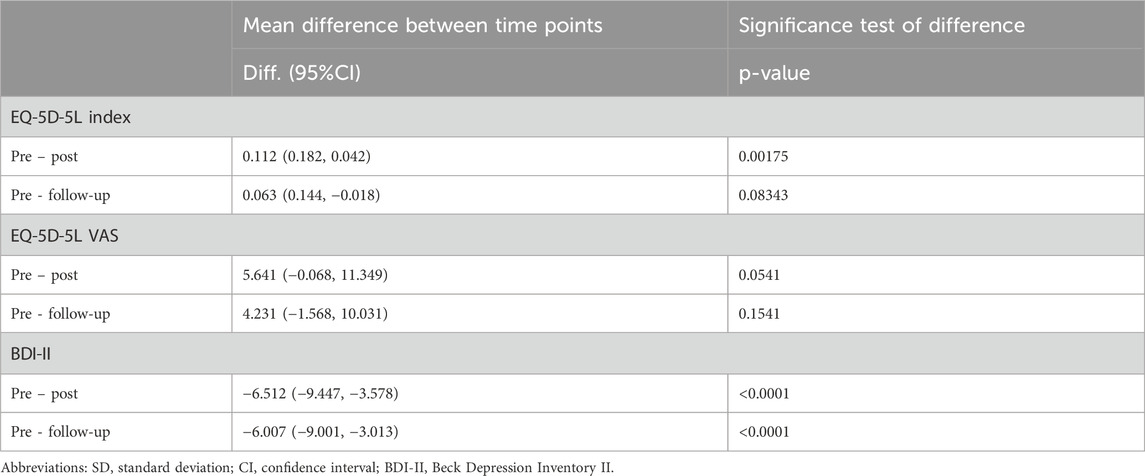
Table 4. Mean change in in EQ-5D-5L (index and VAS) and BDI-II when comparing pre-treatment to post-treatment, and from pre-treatment to 6-month follow-up for the treatment arm receiving CBT-ExpVR.
Despite improvements in the EQ-5D-5L index and the EQ-5D-5L VAS score from pre-treatment to 6-month follow-up, these changes were not statistically significant. The reduction in BDI-II scores was still significant at 6-month follow-up, however, indicating a sustained reduction in depressive symptoms after completion of CBT-ExpVR.
Table 5 shows the mixed effect linear regression model results analyzing differences in EQ-5D-5L index, EQ-5D-5L VAS, and BDI-II scores between the three groups at pre-treatment, post-treatment, and follow-up. At pre-treatment, there were no significant differences between participants receiving CBT-ExpVR and those receiving CBT-Exp or RlxVR for EQ-5D-5L index, EQ-5D-5L VAS, or BDI-II scores. This suggests that participants in all three treatment arms had similar levels of self-reported health and depressive symptoms at baseline (see also Table 1).
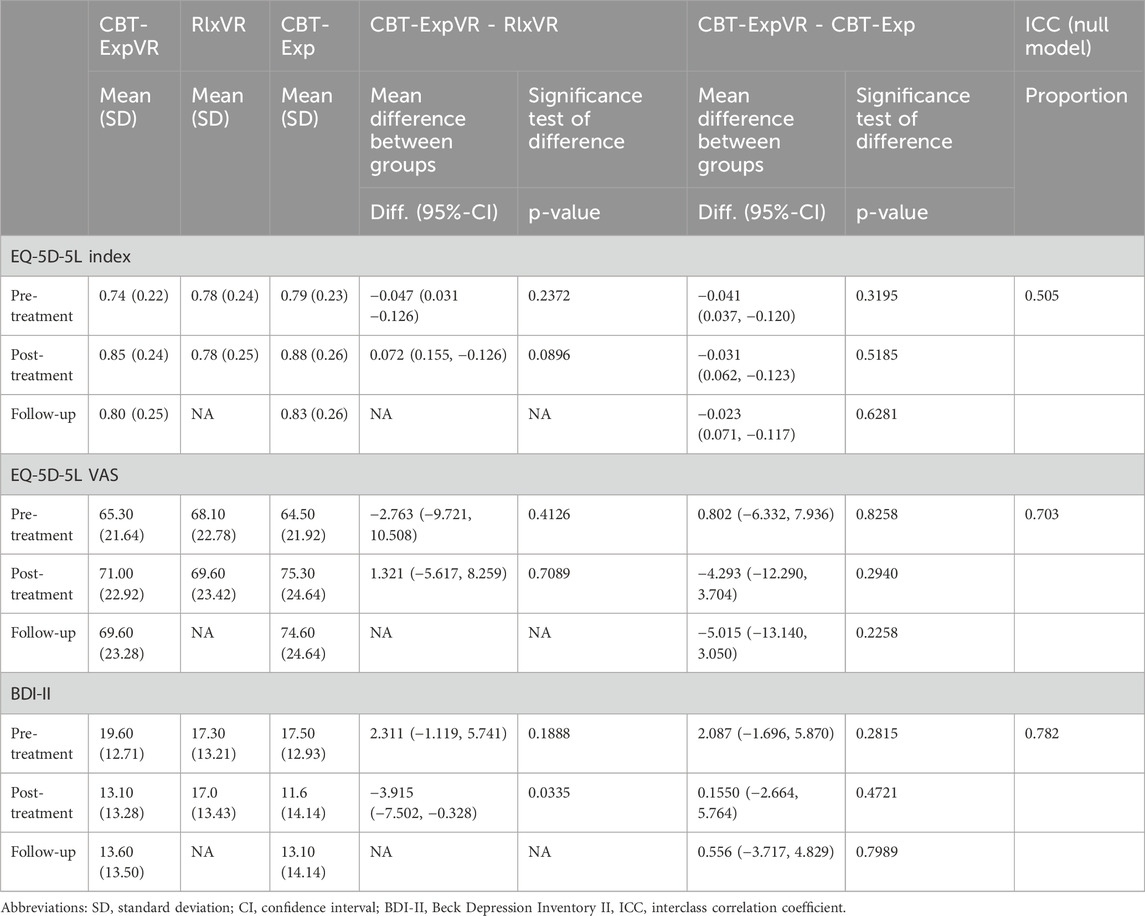
Table 5. Between-group comparisons of EQ-5D-5L (index and VAS) and BDI-II between treatment interventions at three different time points: pre, post and at follow-up.
In the post-treatment comparison, no significant differences were observed between participants receiving CBT-ExpVR and those receiving CBT-Exp for EQ-5D-5L index, EQ-5D-5L VAS or BDI-II. This suggests that after treatment, the outcomes health status, and depressive symptoms were very similar between the treatment arm receiving CBT-ExpVR and the treatment arm that received CBT-Exp. The slight differences in β indicate comparable effectiveness for both interventions in improving overall health and reducing symptoms of depression.
At post-treatment, a significant difference was found between participants receiving CBT-ExpVR and those receiving RlxVR on BDI-II scores, indicating that those receiving CBT-ExpVR reported less severe depressive symptoms. While no significant differences were observed between the two treatment arms on the EQ-5D-5L index or EQ-5D-5L VAS, the trend suggests that both treatment arms consistently reported better outcomes in self-reported health and symptoms of depression.
At 6-month follow-up, the results indicated no significant differences between the intervention receiving CBT-ExpVR and the treatment arm receiving CBT-Exp on any of the secondary outcome measures.
3.5 Adjustment for covariates
When we adjusted the main analysis for ASRS, AUDIT, DUDIT, and SRS-2, we saw no effect of alcohol disorder use scores (AUDIT) or drug use disorder scores (DUDIT) on the outcome of the interventions on SIAS. However, symptoms and severity of autism spectrum disorder (SRS-2) led to slightly higher scores on SIAS [β = 0.129, 95% CI (0.229, 0.030), p = 0.014735]. Similarly, self-reported symptoms of ADHD (ASRS) led to slightly higher scores on SIAS [β = 0.304, 95% CI (0.545, 0.063), p = 0.01164].
3.6 Planned sensitivity analyses
The first sensitivity analysis compared the effects of CBT-ExpVR and CBT-Exp when participants initially assigned to RlxVR were excluded. The mixed effects linear regression model showed significant reductions in social anxiety (SIAS) scores over time for CBT-ExpVR [pre-post: β = −17.514, 95% CI (−12.777, −22.250), p < 0.0001; pre-follow-up: β = −16.513, 95% CI (−11.777, −21.250), p < 0.0001], but no significant differences were observed between CBT-ExpVR and CBT-Exp at any time point (difference at pre-treatment: β = 0.831, 95% CI (−8.362, 10.023), p = 0.8598, difference at post-treatment: β = 4.540, 95% CI (−5.162, 4.242), p = 03,611, difference at follow-up: β = 0.085, 95% CI (−9.617, 9.787), p = 0.9863). These results suggest that while CBT-ExpVR showed substantial reductions in anxiety levels, there were no significant differences between the two CBT treatments at any time point.
In the second sensitivity analysis, we compared CBT-ExpVR to CBT-Exp while disregarding the fact that some patients came from the RlxVR intervention group. This analysis yielded consistent results, showing significant reductions in SIAS scores over time for CBT-ExpVR (pre-post: β = −14.872, 95% CI (−18.865, −10.880), p < 0.0001, pre-follow-up: β = −13.311, 95% CI (−17.365, −9.257), p < 0.0001) and no significant differences between the two groups receiving CBT (difference at pre-treatment: β = 0.728, 95% CI (−7.131, 8.588), p = 0.8564, difference at post-treatment: β = 4.814, 95% CI (−3.496, 13.125), p = 0.2594, difference at follow-up: β = 4.2600, 95% CI (−6.724, 0.7034), p = 0.7034.
Thus, the sensitivity analyses confirmed that the inclusion or exclusion of participants from RlxVR did not affect the findings. In both analyses, CBT-ExpVR and CBT-ExpVR resulted in similar reductions in SIAS scores, with no significant differences between the two interventions.
3.7 Planned subgroup analyses
A per-protocol analysis was conducted to assess the impact of the intervention on participants who adhered to the treatment protocol. The analysis included participants who completed a minimum of six sessions within 15 weeks, i.e., 29 participants. Due to time constraints, two participants had been allocated directly to RlxVR without being randomized, and they were omitted from the per-protocol analysis. The mixed effects linear regression model showed a significant reduction in SIAS scores over time for the treatment arm receiving CBT-ExpVR (pre-post: β = −14.387, 95% CI (−19.601, −9.173), p < 0.0001, pre-follow-up: β = −12.887, 95% CI (−18.244, −7.530), p < 0.0001). Again, there was no significant difference between CBT-ExpVR and CBT-Exp (pre-treatment: β = −0.831, 95% CI (−7.173, 5.441), p = 0.7951, post-treatment: β = 4.783, 95% CI (−1.567, 11.133), p = 0.1408, follow-up: β = 2.436 95% CI (−4.052, 0.4052), p = 0.4621.
3.8 Additional analyses
3.8.1 WAI-SR
After the last treatment session, participants assessed the working alliance between patient and therapist. We compared the working alliance between treatment groups using linear regression with robust standard errors to account for clustering. Results showed no significant difference between the group receiving CBT-ExpVR, M = 72.8, (SD = 15.36), and the group receiving CBT-Exp, M = 76.1, (SD = 13.43), p = 0.348, but the RlxVR intervention, M = 60.6, (SD = 23.43) showed a significantly lower WAI-SR score compared to both CBT-ExpVR, p = 0.0015 and CBT-Exp, p < 0.0001. Thus, the therapeutic alliance measured by the WAI-SR was similar for the two CBT interventions but weaker in the VR relaxation group.
3.8.2 SWEAT
A linear mixed effects regression model was applied to evaluate changes in SWEAT scores, with both therapist and participant included as random intercepts. The results showed that significantly higher cost and effort was required to conduct exposure in vivo compared to VR exposure, indicated by the negative scores in Table 6. This difference in cost and effort was evident at all exposure sessions four to 9 (Table 6).

Table 6. Difference in total SWEAT score between VR-based exposure and in vivo exposure for the six cognitive behavioral therapy sessions that involved exposure.
3.9 Attrition and missing data
Mixed effects linear regression models can successfully estimate parameters when data are missing at random (MAR) as long as the models are correctly specified and any covariates influencing missingness are included in the model. We compared the baseline data for participants completing or dropping out of CBT-ExpVR and CBT-Exp and found no significant differences on age, gender, SIAS score, or EQ-5D-5L index score. However, for the group receiving CBT-Exp, we saw a statistically significant difference in BDI-II and EQ-5D-5L VAS scores, where participants who dropped out of CBT-Exp reported more symptoms of depression and rated their health status lower at baseline than participants who completed the intervention. As this could mean that symptoms of depression and health status might be linked to dropout in CBT-Exp, we included BDI-II and EQ-5D-5L VAS as covariates in the model and ran the ITT analysis on the primary outcome to check if the parameters were affected by dropout. As in the primary analysis, we saw a significant reduction in SIAS score between pre- and post-treatment in the group receiving CBT-ExpVR, β = −10.17, 95% CI (−14.07, −6.27), p < 0.0001, and between pre-treatment and follow-up, β = −9.35, 95% CI (−13.30, −5.41), p < 0.0001. At post-treatment, there was no significant difference between CBT-ExpVR and CBT-Exp on SIAS score, but there was a significant difference between CBT-ExpVR and RlxVR, β = −10.73, 95% CI (−3.504, −14.166), p < 0.0002. Overall, the inclusion of the covariates in the model blunted the treatment effect, suggesting that dropout affected the results. However, the overall conclusion was unchanged.
3.10 Harms
No harms related to the interventions were registered during the study.
4 Discussion
The results of this RCT confirmed our primary hypothesis by showing a statistically significant reduction in symptoms of social anxiety (on SIAS) from pre-treatment to post-treatment in the group receiving CBT-ExpVR. The second hypothesis stated that CBT-ExpVR at post-treatment would be more effective in reducing symptoms of social anxiety than both CBT-Exp and RlxVR. While CBT-ExpVR did significantly reduce anxiety compared to RlxVR, we found no significant difference at post-treatment between CBT-ExpVR and CBT-Exp. This suggests that CBT-ExpVR has similar treatment effects to the gold standard treatment. The improvement in symptoms of social anxiety that was seen at the end of treatment was sustained at the 6-month follow-up, confirming the third hypothesis of the study.
Regarding the secondary outcomes, we found a significant reduction in symptoms of depression (on the BDI-II) from pre-treatment to post-treatment in the treatment arm receiving CBT-ExpVR. This was supported by significantly fewer symptoms of depression at post-treatment for CBT-ExpVR compared with RlxVR. There was no significant difference in BDI-II at post-treatment between CBT-ExpVR and CBT-Exp. Again, this reflects similar treatment effects of CBT-ExpVR and the gold-standard treatment control condition.
The results on the SWEAT measure showed the higher cost and increased effort required to conduct exposure in vivo compared to exposure in VR, as reported by the therapist. This difference was evident across all exposure sessions. CBT with VR-exposure might also be more acceptable to patients as it had an attrition rate of 16% compared to 38% for CBT with in vivo exposure.
The current study is one of few trials investigating CBT with VR-based exposure using 360° videos. The results indicate that the treatment effect sought in traditional in vivo exposure is also possible using 360° videos. This is consistent with Zainal et al. (2021), who used 360˚ videos for self-guided virtual reality exposure therapy, and with previous studies using 360° videos for the treatment of public speaking anxiety (Fehlmann et al., 2023; Lindner et al., 2019; Reeves, Elliott, Curran, Dyer and Hanna, 2021). Reeves et al. (2021) also saw a decrease in fear of negative evaluation (FNE) after treatment using 360° video for exposure, while similar studies using computer-generated images found inconsistent results (Anderson et al., 2013; Wallach, Safir and Bar-Zvi, 2009). Reeves et al. (2021) postulated that real-life recordings displaying realistic facial expressions might be central to treatment effects on FNE.
FNE is central to the symptomatology of SAD, so based on Reeves et al. (2021), one may think that 360° video could lead to a greater reduction in symptoms of social anxiety; however, based on our results, it does not seem like the treatment effects of CBT with VR-based exposure using 360° videos surpass the results seen in CBT with VR-based exposure using computer-generated images. Instead, it seems that CBT with VR-based exposure using 360° videos shows similar treatment effects as CBT with VR-based exposure using computer-generated images and CBT with in vivo exposure. Our results are also in line with recent meta-analyses that found a large pooled effect size when comparing CBT with VR-based exposure to waitlist control, and a small pooled effect size when comparing to VR-based exposure using computer-generated images, suggesting comparable effects between these two forms of intervention (Caponnetto et al., 2021; Carl et al., 2019; Chesham et al., 2018; Horigome et al., 2020; Kampmann, Emmelkamp and Morina, 2016; Opriş et al., 2012; Parsons and Rizzo, 2008; Powers and Emmelkamp, 2008; Shahid et al., 2024; Wechsler et al., 2019; Wong et al., 2023).
A German study showed that among cognitive behavioral therapists working in hospitals, only 46.8% used exposure in the treatment of anxiety disorders (Pittig and Hoyer, 2017; Pittig, Kotter and Hoyer, 2019). When reporting obstacles to in-session exposure, they reported time constraints, lack of access to appropriate exposure situations, the difficulty of planning exposure, and that it increased the risk that patients would not show up for their session. Use of VR exposure might remove many of these practical obstacles that may refrain cognitive behavioral therapist from conducting exposure. The results of the current study and from previous research (Bouchard et al., 2017) show that the cost and effort related to exposure are significantly lower for VR-based exposure than exposure in vivo.
4.1 Strengths and limitations
The present study had several limitations. First, the study had a relatively small sample size, and the preregistered study intended to include 90 participants instead of only 51. The study started in December 2019, with recruitment and treatment planned to last 12 months, but this was affected by the COVID-19 pandemic that caused several lockdowns during 2020. Although the recruitment and treatment period was extended, and additional funding was secured, recruitment was still challenging even after the final lockdown ended in early 2021. The recruitment and treatment period was stopped in April 2022 due to time and funding restrictions despite a shortfall of 39 participants based on the a priori power analysis. A sample size of 51 participants is still above average in this field of research. According to Wong et al. (2023), the largest RCT in the field has 112 participants, whereas the smallest RCT only has 10 participants. Across all studies included in their meta-analysis, the mean number of participants was 48. That said, the low sample size naturally affects the study’s statistical power, and increases the risk of a type II error. At post-treatment, we found no difference between CBT-ExpVR and CBT-Exp, but if CBT-ExpVR were superior to CBT-Exp, we would only have a 66% chance of detecting it. In other words, the probability of not detecting a difference is 44%, which is substantially higher than the 20% we usually accept (Cohen, 1992), and this should be taken into account when interpreting the results.
A methodological limitation was that participants were informed about their allocation before they gave their informed consent and completed the baseline assessment. This was also a deviation from the protocol, which intended that participants and therapists were informed about the allocation at session four, i.e., the first session that included exposure. It is difficult to fully blind clinical trials of psychological interventions, and the participants and therapists will typically know the allocation once the intervention starts (Cuijpers et al., 2015). Knowing the allocation before consenting to participate in the study might have affected the attrition rate in our study as participants had not committed to the study in advance of the allocation. While all participants allocated to CBT-ExpVR started their treatment, two participants allocated to RlxVR and two allocated to CBT-Exp did not receive the allocated treatment. The lack of blinding might also have affected the baseline data due to expectancy effects or by introducing performance or ascertainment bias (Renjith, 2017). The risk of bias is increased by the study relying on self-reported symptoms (Hulley, Cummings, Browner, Grady and Newman, 2013).
Another methodological limitation concerns the randomization as two participants were allocated to RlxVR outside the randomization process. After finishing placebo treatment, these two individuals were correctly randomized to CBT-ExpVR or CBT-Exp. This deviation from the randomization process could introduce some bias because the allocation is no longer totally random.
In the study protocol, it was stated that 10% of sessions would be audio-recorded to ensure adherence to the manual. Although several treatment sessions were recorded and evaluated with the supervisor, adherence was not assessed in a systematic fashion, and no standardized fidelity tools were used. Based on the weekly meetings between the principal investigator and the therapists, we believe that the therapists did adhere to the treatment manual and that the treatment was delivered as planned.
The current study could have benefitted from including a behavioral avoidance test to assess the participant’s behavior in a social scenario before and after treatment. In this way, the self-reported measurements used could have been corroborated by a more objective measure of the treatment effect on real-world behavior. Self-report measures are susceptible to bias stemming from social desirability but often show superior construct validity compared to behavioral measures (Haeffel and Howard, 2010). Kampmann, Emmelkamp, and Morina (2018) found that self-report measures (FNE and Liebowitz Social Anxiety Scale) were better at predicting social anxiety in everyday life than performance on behavioral avoidance tests, testifying to the ecological validity of using self-report measures in assessing social anxiety. A limitation of the study of Kampmann et al. (2018) was that social anxiety in everyday life was measured using self-report measures. Future studies should ideally assess anxiety symptoms in several ways, including behavioral and self-report measures. Finally, assessment of cybersickness before and after exposure in VR and measurement of presence would have made it possible to evaluate 360° video against computer-generated images of other virtual environments.
The strengths of the current RCT include comparing the experimental condition to both the gold standard treatment and an active control. Further, the 6-month follow-up period allowed us to evaluate the longer term effects of treatment. Furthermore, the study was preregistered at ClinicalTrials.org, and the SAP was made publically available before the data analysis was initated. Finally, this study adds to the sparse pool of RCTs investigating the effect of 360˚video for exposure in SAD.
4.2 Implications
CBT with VR-based exposure using 360° videos is an effective alternative to CBT with in vivo exposure for patients with SAD. Exposure with 360° video offers real-life recordings that display realistic body language and facial expressions, conveying what others think and feel. Having the therapist control the transitions between video clips and switching between multiple scenes enables bidirectional social interactions relevant to exposure in people with SAD. Exposure in VR using 360° video seems comparable to exposure in VR using computer-generated images, and the increased realism inherent to 360° video does not seem to add any obvious advantage for treatment effects. As CBT with VR-based exposure using 360° video appeared more acceptable to patients and was considered by therapists to require less effort and have fewer costs than CBT with in vivo exposure, it may remove some of the obstacles faced by cognitive behavioral therapists when conducting in-session exposure. VR-based exposure has the potential to play a major role in the wider dissemination of exposure therapy for treatment of SAD and other anxiety disorders.
Data availability statement
The datasets presented in this article are not readily available because data sharing is restricted according to the General Data Protection Regulation (GDPR) in the European Union (EU). Requests to access the datasets should be directed to cGVyLnRyYWRzLm9yc2tvdkByc3lkLmRr.
Ethics statement
The studies involving humans were approved by The Regional Committees on Health Research Ethics for Southern Denmark. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was not obtained from the individual(s) for the publication of potentially identifiable images included in this article because images are used with permission from the owner, Khora (www.khora.com).
Author contributions
PØ: Data curation, Formal Analysis, Investigation, Methodology, Project administration, Writing – original draft, Writing – review and editing. ER: Data curation, Investigation, Project administration, Writing – original draft, Writing – review and editing. TS-M: Investigation, Writing – original draft, Writing – review and editing. ME: Investigation, Writing – review and editing. LC: Conceptualization, Data curation, Funding acquisition, Investigation, Methodology, Project administration, Software, Writing – review and editing. CD: Formal Analysis, Writing – original draft, Writing – review and editing. ML: Conceptualization, Writing – review and editing. SB: Conceptualization, Writing – review and editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. The study was funded by the Research Fund of the Mental Health Services of Southern Denmark (A2985) and the Jascha Fund (7668). The funding sources did not have any role in the study’s design, execution, analysis, and interpretation of the data, nor in the writing of manuscripts and the decision to submit results.
Acknowledgments
We thank OPEN Statistics at Open Patient data Explorative Network (OPEN), Odense University Hospital, Region of Southern Denmark, for supervising the statistical analyses. We thank Pia Veldt Larsen, Mental Health Services, Region of Southern Denmark, for assistance with the statistical analyses, and Christine S.T. Madsen for preparing the data for analysis and running the descriptive analyses on baseline data. Thanks to Maxime Sainte-Marie for helping to create the visualization/data presentation. Finally, thanks to Claire Gudex, Department of Clinical Research, University of Southern Denmark, for editing a previous version of this paper.
Conflict of interest
SB is a consultant and owns equity in Cliniques et Développement In Virtuo, which develops virtual environments. Cliniques et Développement In Virtuo did not create any virtual environments investigated in this study.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/frvir.2025.1588181/full#supplementary-material
References
Adler, L. A., Spencer, T., Faraone, S. V., Kessler, R. C., Howes, M. J., Biederman, J., et al. (2006). Validity of pilot adult ADHD self- report scale (ASRS) to rate adult ADHD symptoms. Ann. Clin. Psychiatry 18 (3), 145–148. doi:10.1080/10401230600801077
Anderson, P., Jacobs, C., and Rothbaum, B. O. (2004). Computer-supported cognitive behavioral treatment of anxiety disorders. J. Clin. Psychol. 60 (3), 253–267. doi:10.1002/jclp.10262
Anderson, P. L., Price, M., Edwards, S. M., Obasaju, M. A., Schmertz, S. K., Zimand, E., et al. (2013). Virtual reality exposure therapy for social anxiety disorder: a randomized controlled trial. J. Consult. Clin. Psychol. 81 (5), 751–760. doi:10.1037/a0033559
Arnfred, B., Bang, P., Hjorthøj, C., Winding, C., Møller, K., Hvenegaard, M., et al. (2021). Res. Square. doi:10.21203/rs.2.504/v1
Bölte, S. (2012). Brief report: the social responsiveness scale for adults (SRS-A): initial results in a German cohort. J. Autism Dev. Disord. 42 (9), 1998–1999. doi:10.1007/s10803-011-1424-5
Bouchard, S., Dumoulin, S., Robillard, G., Guitard, T., Klinger, É., Forget, H., et al. (2017). Virtual reality compared with in vivo exposure in the treatment of social anxiety disorder: a three-arm randomised controlled trial. Br. J. Psychiatry 210 (4), 276–283. doi:10.1192/bjp.bp.116.184234
Brown, E. J., Turovsky, J., Heimberg, R. G., Juster, H. R., Brown, T. A., and Barlow, D. H. (1997). Validation of the social interaction anxiety scale and the social phobia scale across the anxiety disorders. Psychol. Assess. 9 (1), 21–27. doi:10.1037/1040-3590.9.1.21
Bruch, M. A., Hamer, R. J., and Heimberg, R. G. (1995). Shyness and PublicSelf-consciousness: additive orInteractive relation withSocial interaction? J. personality 63 (1), 47–63. doi:10.1111/j.1467-6494.1995.tb00801.x
Caponnetto, P., Triscari, S., Maglia, M., and Quattropani, M. C. (2021). The simulation game—virtual reality therapy for the treatment of social anxiety disorder: a systematic review. Int. J. Environ. Res. public health 18 (24), 13209. doi:10.3390/ijerph182413209
Carl, E., Stein, A. T., Levihn-Coon, A., Pogue, J. R., Rothbaum, B., Emmelkamp, P., et al. (2019). Virtual reality exposure therapy for anxiety and related disorders: a meta-analysis of randomized controlled trials. J. anxiety Disord. 61, 27–36. doi:10.1016/j.janxdis.2018.08.003
Chesham, R. K., Malouff, J. M., and Schutte, N. S. (2018). Meta-analysis of the efficacy of virtual reality exposure therapy for social anxiety. Behav. Change 35 (3), 152–166. doi:10.1017/bec.2018.15
Clark, D. M., and Wells, A. (1995). “A cognitive model of social phobia,” in Social phobia: diagnosis, assessment, and treatment (New York, NY, US: The Guilford Press), 69–93.
Clemmensen, L., Bouchard, S., Rasmussen, J., Holmberg, T. T., Nielsen, J. H., Jepsen, J. R. M., et al. (2020). STUDY PROTOCOL: EXPOSURE IN VIRTUAL REALITY FOR SOCIAL ANXIETY DISORDER - a randomized controlled superiority trial comparing cognitive behavioral therapy with virtual reality based exposure to cognitive behavioral therapy with in vivo exposure. BMC Psychiatry 20 (1), 32. doi:10.1186/s12888-020-2453-4
Clemmensen, L., Torp Ernst, M., Nielsen, C. S., Runge, E., and Helweg-Jørgensen, S. (2021). Kognitiv adfærdsterapi for socialfobi: En behandlingsmanual med eksponering i enten in vivo eller Virtual Reality. Syddansk Univ. Telepsykiatrisk cent. doi:10.21996/jc31-kb73
Cohen, J. (1992). Statistical power analysis. Curr. Dir. Psychol. Sci. 1 (3), 98–101. doi:10.1111/1467-8721.ep10768783
Craske, M. G., and Stein, M. B. (2016). Anxiety. Lancet 388 (10063), 3048–3059. doi:10.1016/s0140-6736(16)30381-6
Craske, M. G., Treanor, M., Conway, C. C., Zbozinek, T., and Vervliet, B. (2014). Maximizing exposure therapy: an inhibitory learning approach. Behav. Res. Ther. 58, 10–23. doi:10.1016/j.brat.2014.04.006
Cuijpers, P., Karyotaki, E., Andersson, G., Li, J., Mergl, R., and Hegerl, U. (2015). The effects of blinding on the outcomes of psychotherapy and pharmacotherapy for adult depression: a meta-analysis. Eur. Psychiatry 30 (6), 685–693. doi:10.1016/j.eurpsy.2015.06.005
Craske, M. G., Treanor, M., Conway, C. C., Zbozinek, T., and Vervliet, B. (2024). Maximizing exposure therapy: An inhibitory learning approach, Behaviour Research and Therapy. 58, 10–12. doi:10.1016/j.brat.2014.04.006
Della Libera, C., Simon, J., Larøi, F., Quertemont, E., and Wagener, A. (2023). Using 360-degree immersive videos to assess multiple transdiagnostic symptoms: a study focusing on fear of negative evaluation, paranoid thoughts, negative automatic thoughts, and craving. Virtual Real. 27 (4), 3565–3580. doi:10.1007/s10055-023-00779-y
Emmelkamp, P. M. (2005). Technological innovations in clinical assessment and psychotherapy. Psychotherapy Psychosomatics 74 (6), 336–343. doi:10.1159/000087780
Emmelkamp, P. M., Meyerbröker, K., and Morina, N. (2020). Virtual Reality Therapy in Social Anxiety Disorder. Curr Psychiatry Rep. 13;22 (7), 32. doi:10.1007/s11920-020-01156-1
Ernst, M, Bouchard, S., Andersen, T, Orskov, PT, Tarp, K., and Lictenstein, MB (2024). Virtual reality–based exposure with 360° environments for social anxiety disorder: usability and feasibility study JMIR Form. Res. 8:e55679. doi:10.2196/55679
Fehlmann, B., Mueller, F. D., Wang, N., Ibach, M. K., Schlitt, T., Bentz, D., et al. (2023). Virtual reality gaze exposure treatment reduces state anxiety during public speaking in individuals with public speaking anxiety: a randomized controlled trial. J. Affect. Disord. Rep. 14, 100627. doi:10.1016/j.jadr.2023.100627
Fehm, L., Pelissolo, A., Furmark, T., and Wittchen, H.-U. (2005). Size and burden of social phobia in Europe. Eur. Neuropsychopharmacol. 15 (4), 453–462. doi:10.1016/j.euroneuro.2005.04.002
Feng, Y. S., Kohlmann, T., Janssen, M. F., and Buchholz, I. (2021). Psychometric properties of the EQ-5D-5L: a systematic review of the literature. Qual. Life Res. 30 (3), 647–673. doi:10.1007/s11136-020-02688-y
Haeffel, G. J., and Howard, G. S. (2010). Self-report: psychology’s four-letter word. Am. J. Psychol. 123 (2), 181–188. doi:10.5406/amerjpsyc.123.2.0181
Hatcher, R. L., and Gillaspy, J. A. (2006). Development and validation of a revised short version of the working alliance inventory. Psychotherapy Res. 16 (1), 12–25. doi:10.1080/10503300500352500
Heimberg, R. G., and Magee, L. (2014). “Social anxiety disorder,” in Clinical handbook of psychological disorders: a step-by-step treatment manual. 5th ed. (New York, NY, US: The Guilford Press), 114–154.
Hildebrand, M. (2015). The psychometric properties of the drug use disorders identification test (DUDIT): a review of recent research. J. Subst. Abuse Treat. 53, 52–59. doi:10.1016/j.jsat.2015.01.008
Hodges, L. F., Kooper, R., Meyer, T. C., Rothbaum, B. O., Opdyke, D., Graaff, J. J. d., et al. (1995). Virtual environments for treating the fear of heights. IEEE Comput. 28 (7), 27–34. doi:10.1109/2.391038
Hofmann, S. G., and Smits, J. A. (2008). Cognitive-behavioral therapy for adult anxiety disorders: a meta-analysis of randomized placebo-controlled trials. J. Clin. psychiatry 69 (4), 621–632. doi:10.4088/jcp.v69n0415
Hofmann, T. C., Glasziou, P. P., Boutron, I., Milne, R., Perera, R., Moher, D., et al. (2014). Better reporting of interventions: template for intervention description and replication (TIDieR) checklist and guide. BMJ. Mar 7 (348), 1687. doi:10.1136/bmj.g1687
Holmberg, T. T., Eriksen, T. L., Petersen, R., Frederiksen, N. N., Damgaard-Sørensen, U., and Lichtenstein, M. B. (2020). Social anxiety can Be triggered by 360-degree videos in virtual reality: a pilot study exploring fear of shopping. Cyberpsychology, Behav. Soc. Netw. 23 (7), 495–499. doi:10.1089/cyber.2019.0295
Horigome, T., Kurokawa, S., Sawada, K., Kudo, S., Shiga, K., Mimura, M., et al. (2020). Virtual reality exposure therapy for social anxiety disorder: a systematic review and meta-analysis. Psychol. Med. 50, 2487–2497. doi:10.1017/s0033291720003785
Hulley, S. B., Cummings, S. R., Browner, W. S., Grady, D. G., and Newman, T. B. (2013). Designing Clinical Research, 4e. Lippincott Williams and Wilkins.
Jensen, C. E., Sørensen, S. S., Gudex, C., Jensen, M. B., Pedersen, K. M., and Ehlers, L. H. (2021). The Danish EQ-5D-5L value set: a hybrid model using cTTO and dce data. Appl. health Econ. health policy 19 (4), 579–591. doi:10.1007/s40258-021-00639-3
Juszczak, E., Altman, D. G., Hopewell, S., and Schulz, K. (2019). Reporting of multi-arm parallel-group randomized trials: extension of the CONSORT 2010 statement. Jama 321 (16), 1610–1620. doi:10.1001/jama.2019.3087
Kampmann, I. L., Emmelkamp, P. M., Hartanto, D., Brinkman, W.-P., Zijlstra, B. J., and Morina, N. (2016). Exposure to virtual social interactions in the treatment of social anxiety disorder: a randomized controlled trial. Behav. Res. Ther. 77, 147–156. doi:10.1016/j.brat.2015.12.016
Kampmann, I. L., Emmelkamp, P. M., and Morina, N. (2016). Meta-analysis of technology-assisted interventions for social anxiety disorder. J. anxiety Disord. 42, 71–84. doi:10.1016/j.janxdis.2016.06.007
Kampmann, I. L., Emmelkamp, P. M., and Morina, N. (2018). Self-report questionnaires, behavioral assessment tasks, and an implicit behavior measure: do they predict social anxiety in everyday life? PeerJ 6, e5441. doi:10.7717/peerj.5441
Kessler, R. C., Adler, L., Ames, M., Demler, O., Faraone, S., Hiripi, E., et al. (2005). The World Health Organization Adult ADHD Self-Report Scale (ASRS): a short screening scale for use in the general population. Psychol. Med. 35 (2), 245–256. doi:10.1017/s0033291704002892
Klinger, E., Bouchard, S., Légeron, P., Roy, S., Lauer, F., Chemin, I., et al. (2005). Virtual reality therapy versus cognitive behavior therapy for social phobia: a preliminary controlled study. Cyberpsychology and Behav. 8 (1), 76–88. doi:10.1089/cpb.2005.8.76
Lindner, P., Miloff, A., Fagernäs, S., Andersen, J., Sigeman, M., Andersson, G., et al. (2019). Therapist-led and self-led one-session virtual reality exposure therapy for public speaking anxiety with consumer hardware and software: a randomized controlled trial. J. anxiety Disord. 61, 45–54. doi:10.1016/j.janxdis.2018.07.003
Melo, M., Vasconcelos-Raposo, J., and Bessa, M. (2018). Presence and cybersickness in immersive content: effects of content type, exposure time and gender. Comput. and Graph. 71, 159–165. doi:10.1016/j.cag.2017.11.007
Miloff, A., Lindner, P., Hamilton, W., Reuterskiöld, L., Andersson, G., and Carlbring, P. (2016). Single-session gamified virtual reality exposure therapy for spider phobia vs. traditional exposure therapy: study protocol for a randomized controlled non-inferiority trial. Trials 17 (1), 60. doi:10.1186/s13063-016-1171-1
Olfson, M., Guardino, M., Struening, E., Schneier, F. R., Hellman, F., and Klein, D. F. (2000). Barriers to the treatment of social anxiety. Am. J. Psychiatry 157 (4), 521–527. doi:10.1176/appi.ajp.157.4.521
Opriş, D., Pintea, S., García-Palacios, A., Botella, C., Szamosközi, Ş., and David, D. (2012). Virtual reality exposure therapy in anxiety disorders: a quantitative meta-analysis. Depress. anxiety 29 (2), 85–93. doi:10.1002/da.20910
Ørskov, P. T., Lichtenstein, M. B., Ernst, M. T., Fasterholdt, I., Matthiesen, A. F., Scirea, M., et al. (2022). Cognitive behavioral therapy with adaptive virtual reality exposure vs. cognitive behavioral therapy with in vivo exposure in the treatment of social anxiety disorder: a study protocol for a randomized controlled trial. Front. psychiatry 13. doi:10.3389/fpsyt.2022.991755
Parsons, T. D., and Rizzo, A. A. (2008). Affective outcomes of virtual reality exposure therapy for anxiety and specific phobias: a meta-analysis. J. Behav. Ther. Exp. psychiatry 39 (3), 250–261. doi:10.1016/j.jbtep.2007.07.007
Pelissolo, A., Abou Kassm, S., and Delhay, L. (2019). Therapeutic strategies for social anxiety disorder: where are we now? Expert Rev. Neurother. 19 (12), 1179–1189. doi:10.1080/14737175.2019.1666713
Pittig, A., and Hoyer, J. (2017). Exposition aus Sicht niedergelassener Verhaltenstherapeutinnen und Verhaltenstherapeuten: Anwendung und systemische Barrieren [Utilization and barriers of exposure in private practice: The perspective of behavioral psychotherapists]. Zeitschrift für Klinische Psychologie und Psychotherapie: Forschung und Praxis, 46 (4), 223–235. doi:10.1026/1616-3443/a000441
Pittig, A., Kotter, R., and Hoyer, J. (2019). The struggle of behavioral therapists with exposure: self-reported practicability, negative beliefs, and therapist distress about exposure-based interventions. Behav. Ther. 50 (2), 353–366. doi:10.1016/j.beth.2018.07.003
Powers, M. B., and Emmelkamp, P. M. (2008). Virtual reality exposure therapy for anxiety disorders: a meta-analysis. J. anxiety Disord. 22 (3), 561–569. doi:10.1016/j.janxdis.2007.04.006
Reeves, R., Elliott, A., Curran, D., Dyer, K., and Hanna, D. (2021). 360 Video virtual reality exposure therapy for public speaking anxiety: a randomized controlled trial. J. anxiety Disord. 83, 102451. doi:10.1016/j.janxdis.2021.102451
Renjith, V. (2017). Blinding in randomized controlled trials: what researchers need to know? Manipal J. Nurs. Health Sci. (MJNHS) 3 (1), 45–50. Available online at: https://impressions.manipal.edu/mjnhs/vol3/iss1/14.
Robillard, G., Bouchard, S., Dumoulin, S., and Guitard, T. (2011). The development of the SWEAT questionnaire: a scale measuring costs and efforts inherent to conducting exposure sessions. Stud. Health Technol. Inf. 167, 105–110. doi:10.3233/978-1-60750-766-6-105
Saunders, J. B., Aasland, O. G., Babor, T. F., De la Fuente, J. R., and Grant, M. (1993). Development of the alcohol use disorders identification test (AUDIT): WHO collaborative project on early detection of persons with harmful alcohol consumption-II. Addiction 88 (6), 791–804. doi:10.1111/j.1360-0443.1993.tb02093.x
Schneier, F., and Goldmark, J. (2015). Social anxiety disorder. In D. J. Stein, and B. Vythilingum Editors, Anxiety disorders and gender. Springer International Publishing/Springer Nature. 49–67. doi:10.1007/978-3-319-13060-6_3
Seng, J. J. B., Kwan, Y. H., Fong, W., Phang, J. K., Lui, N. L., Thumboo, J., et al. (2020). Validity and reliability of EQ-5D-5L among patients with axial spondyloarthritis in Singapore. Eur. J. Rheumatol. 7 (2), 71–78. doi:10.5152/eurjrheum.2020.19043
Shahid, S., Kelson, J., and Saliba, A. (2024). Effectiveness and user experience of virtual reality for social anxiety disorder: systematic review. JMIR Ment. Health 11 (1), e48916. doi:10.2196/48916
Steer, R. A., Clark, D. A., Beck, A. T., and Ranieri, W. F. (1999). Common and specific dimensions of self-reported anxiety and depression: the BDI-II versus the BDI-IA. Behav. Res. Ther. 37 (2), 183–190. doi:10.1016/s0005-7967(98)00087-4
Stein, D. J., Lim, C. C. W., Roest, A. M., de Jonge, P., Aguilar-Gaxiola, S., Al-Hamzawi, A., et al. (2017). The cross-national epidemiology of social anxiety disorder: data from the world mental health survey initiative. BMC Med. 15 (1), 143. doi:10.1186/s12916-017-0889-2
Stein, M. B., and Stein, D. J. (2008). Social anxiety disorder. lancet 371 (9618), 1115–1125. doi:10.1016/S0140-6736(08)60488-2
Wallach, H. S., Safir, M. P., and Bar-Zvi, M. (2009). Virtual reality cognitive behavior therapy for public speaking anxiety: a randomized clinical trial. Behav. Modif. 33 (3), 314–338. doi:10.1177/0145445509331926
Wang, P. S., Berglund, P., Olfson, M., Pincus, H. A., Wells, K. B., and Kessler, R. C. (2005). Failure and delay in initial treatment contact after first onset of mental disorders in the National Comorbidity Survey Replication. Archives General Psychiatry 62 (6), 603–613. doi:10.1001/archpsyc.62.6.603
Wechsler, T. F., Kümpers, F., and Mühlberger, A. (2019). Inferiority or Even Superiority of Virtual Reality Exposure Therapy in Phobias?-A Systematic Review and Quantitative Meta-Analysis on Randomized Controlled Trials Specifically Comparing the Efficacy of Virtual Reality Exposure to Gold Standard in vivo Exposure in Agoraphobia, Specific Phobia, and Social Phobia. Front Psychol. Sep 10 (10), 1758. doi:10.3389/fpsyg.2019.01758
Wolitzky-Taylor, K., and LeBeau, R. (2023). Recent advances in the understanding and psychological treatment of social anxiety disorder. Fac. Rev. 12, 8. doi:10.12703/r/12-8
Wong, K. P., Lai, C. Y. Y., and Qin, J. (2023). Systematic review and meta-analysis of randomised controlled trials for evaluating the effectiveness of virtual reality therapy for social anxiety disorder. J. Affect. Disord. 333, 353–364. doi:10.1016/j.jad.2023.04.043
World Health Organization (1992). The ICD-10 classification of mental and behavioural disorders. Clinical descriptions and diagnostic guidelines. Geneva: World Health Organization.
Keywords: virtual reality, cognitive behavioral therapy, exposure, social anxiety disorder, randomized controlled trial, 360° video
Citation: Ørskov PT, Runge E, Sainte-Marie TTH, Ernst MT, Clemmensen L, Dalsgaard CH, Lichtenstein MB and Bouchard S (2025) Virtual reality-based exposure with 360° video as part of cognitive behavioral therapy for social anxiety disorder: a three-arm randomized controlled trial. Front. Virtual Real. 6:1588181. doi: 10.3389/frvir.2025.1588181
Received: 05 March 2025; Accepted: 21 May 2025;
Published: 17 June 2025.
Edited by:
Clint Bowers, University of Central Florida, United StatesReviewed by:
Richard Skarbez, La Trobe University, AustraliaNayeefa Chowdhury, Khalifa University, United Arab Emirates
Slawomir Murawiec, Harmonia Luxmed Medical Center, Poland
Copyright © 2025 Ørskov, Runge, Sainte-Marie, Ernst, Clemmensen, Dalsgaard, Lichtenstein and Bouchard. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Per Trads Ørskov, cGVyLnRyYWRzLm9yc2tvdkByc3lkLmRr