 Guillaume R. Ragetly
Guillaume R. Ragetly Ângela Martins2,3,4
Ângela Martins2,3,4 Ciprian A. Ober
Ciprian A. Ober Céline S. Nicolas
Céline S. Nicolas- 1Centre Hospitalier Vétérinaire Frégis, Gentilly, France
- 2Faculty of Veterinary Medicine, Lusofona University, Lisbon, Portugal
- 3Superior School of Health, Protection and Animal Welfare, Polytechnic Institute of Lusophony, Lisbon, Portugal
- 4Arrábida Veterinary Hospital, Arrábida Animal Rehabilitation Center, Azeitão, Portugal
- 5Department of Surgery and Intensive Care, Faculty of Veterinary Medicine, University of Agricultural Sciences and Veterinary Medicine, Cluj-Napoca, Romania
- 6Clinica Veterinaria Vezzoni, Cremona, Italy
- 7Virbac SA, MU Petfood Petcare, Carros, France
The management of osteoarthritis (OA) in dogs is typically multimodal, including weight management, activity adjustment, joint supplements, and medical treatments when needed. This study evaluated the efficacy of a joint supplement containing eggshell membrane, krill meal with omega-3 fatty acids, Haematococcus pluvialis as a source of astaxanthin, hyaluronic acid and a Boswellia Serrata extract, in dogs with OA, in a multicenter, randomized, placebo-controlled trial. Fifty-two dogs with confirmed OA were given the test supplement or a placebo, for 90 days. Owners regularly completed two validated questionnaires for osteoarthritis (CBPI and LOAD) and rated their dog’s discomfort every 15 to 30 days. Monthly evaluations by investigators included assessments of the dog’s posture, gait, joint pain upon palpation and range of motion (from 1-normal to 4-severe or severely impacted) to determine a clinical score. Statistical analyses included both within-group and between-group comparisons. Of the 52 dogs enrolled, 46 completed the study, with 22 receiving the supplement and 24 receiving the placebo. All main parameters significantly improved over time in the supplement group (CBPI pain severity, CBPI pain interference, LOAD, discomfort, clinical score). In the placebo group, only the CBPI pain interference and LOAD improved. However, there was a statistically significant difference between groups for the CBPI pain interference (p = 0.009). Therefore, this study demonstrates that the test supplement can improve the mobility and quality of life of osteoarthritic dogs.
1 Introduction
Osteoarthritis (OA) is a chronic inflammatory disease impacting the entire joint (1). It is one of the most diagnosed diseases in dogs (2, 3). The prevalence of OA can range from 2.5% in a dog population under primary veterinary care to more than 80% of older and obese dogs (2–4). Although OA can be present in young dogs, age, body weight, breed and neuter status have been identified as risk factors (5–8). The most commonly affected joints are elbows, hips, tarsus, shoulders and stifles (8, 9).
Clinically, the structural and functional changes in the joint will lead to pain, inflammation and an altered mobility. This will translate into a change in gait and weight distribution, the presence of lameness, pain upon palpation, and decreased joint range of movement (10, 11). Owners will describe their dogs as being stiff (with variability throughout the day), having difficulty to perform certain activities (like walking or running, jumping, or even playing) or being reluctant to exercise (12, 13). A change of behavior or demeanor is also usually observed and described by owners (12, 13). Radiographic changes like osteophytes, subchondral bone sclerosis and joint effusion can be observed and used as a diagnostic tool (14). Overall, the diagnosis of OA can be based on objective and subjective measures like clinical metrology instruments, gait assessment and radiography. Clinical metrology instruments (CMIs) are validated questionnaires filled in by owners to evaluate and address clinically relevant questions about a specific construct (13). There are several validated CMIs for OA, including the Canine Brief Pain Inventory (CBPI) and Liverpool Osteoarthritis in Dogs index (LOAD), which are commonly used (13, 15–17).
The therapeutic goals center on alleviating joint pain and enhancing motor function to improve the quality of life of the affected animals. Based on the American Animal Hospital Association (AAHA) guidelines for pain management, a multimodal approach is necessary to improve dogs affected by OA (18). This approach includes a nutritional management to control the dog’s body weight with a therapeutic diet rich in omega-3 fatty acids (FA) to also limit the inflammation, an adaptation of the dog’s exercise and environment to limit high impact activities while still facilitating movements, and a physical rehabilitation program (at home and in specialized centers) to maintain the dog’s mobility (1, 11, 18–21). When needed, effective analgesics may be used. According to the AAHA guidelines, medications that seem the most effective are non-steroidal anti-inflammatory drugs (NSAIDs) and, potentially, anti-nerve growth factor monoclonal antibodies (anti-NGF) (18). Adjunctive analgesic therapies (like amantadine, gabapentin, acetaminophen, steroids or tramadol) may also be considered if necessary (1, 18).
The need for frequent administration of NSAIDs or other pain medicines, along with their side effects and burden of care on the owner, necessitates the use of alternative therapies (22, 23). Among alternatives, nutraceuticals are a good option as they are usually safe. In fact, regardless of the OA severity, efficient joint supplements could still help maintain healthy parts of joints and slow down their degradation (1, 24). However, joint supplements are not all the same and it was found in a recent meta-analysis that those with omega-3 fatty acids showed evident clinical analgesic efficacy, those with collagen (including eggshell membrane-based supplements) showed only a weak efficacy while those only based on chondroitin sulfate and/or glucosamine had no proven efficacy (20). In the AAHA guidelines for pain management, the omega-3-based supplements are considered the most efficacious, based on evidence-based veterinary medicine while those not based on omega-3 FA are considered only as adjuncts, with fewer or no demonstrated efficacy (18).
The test supplement is a joint supplement with a mix of five key ingredients of natural origin, independently known to improve joint health and mobility in dogs or to have antioxidant effects. It contains eggshell membrane (ESM), a complex ingredient full of different molecules naturally found in joints, including collagen, glucosamine, glycosaminoglycans, elastin, hyaluronic acid, and other proteins and amino acids (mainly proline, glutamic acid, and glycine) that can help support protein synthesis (25, 26). The eggshell membrane used in the test supplement has proven efficacy in humans and dogs with mobility disorders (27–29). Other studies, in humans and dogs, with different types of ESM have also shown the beneficial effects of this ingredient in joints (30–34).
The supplement also contains hyaluronic acid (HA) of different molecular weights (MW, below 50 kDa and above 1 MDa). Indeed, the action of HA can depend on its MW, with higher MW being mostly involved in the lubrication and viscoelasticity of the synovial fluid and resilience of the cartilage, while lower MW HA could help initiate the restorative processes (35, 36). Although the effect of HA has mainly been investigated when injected (but not only), the oral bioavailability of HA and distribution in joints has been demonstrated in dogs, even with high molecular weight HA (37).
Haematococcus pluvialis, one of five key ingredients, is one of the richest and safest natural sources of astaxanthin, a powerful antioxidant which can be absorbed by dogs when given orally (38–40). Since oxidative stress plays an important role in OA evolution, controlling it with antioxidants may help delay joint degradation (41).
Krill has also been added as a source of omega-3 fatty acids (FA) that come in the form of readily absorbed phospholipids (42, 43). It is a better source of omega-3 FA than fish oil, based on the omega-3 index observed in dogs fed fish oil or krill meal (43, 44). Krill is effective in improving joint health in animal models and humans and in supporting active dogs (45–49). The phospholipids in krill can also facilitate the absorption of astaxanthin and HA (50–52), providing a synergistic effect with these ingredients. Supplements combining krill, astaxanthin and HA have shown promising results in human and animal models of OA, modulating the inflammatory cascade, reducing cartilage degradation and improving pain and joint function (53–55).
Finally, the test supplement also contains a Boswellia serrata extract. It is rich in boswellic acids known to modulate inflammatory processes, and has been shown to have beneficial effects on joints and mobility, including in dogs (56–58). The bioavailability of the boswellic acids has only been assessed in other species than dogs (56). They are known to be lipophilic and their bioavailability might therefore be increased by the addition of lipids (56), like the krill phospholipids.
When the test supplement was given to owners of dogs with mobility issues for two months, the general mobility and other mobility parameters assessed by the owners significantly improved, with some improvements observed as early as day 7 (59). Similar formulations of this ESM-based supplement have also demonstrated good effectiveness in dogs with mobility disorders, including in dogs with OA in a pilot clinical study (60, 61). However, a blinded placebo-controlled clinical trial involving veterinarians and a sufficient number of dogs still had to be performed to evaluate the efficacy of this formula.
The objective of the study presented here is to evaluate the efficacy of a supplement containing the five main ingredients described above in improving the mobility of dogs with OA, in a blind placebo-controlled clinical trial.
2 Materials and methods
This clinical study was a multicenter double-blind randomized placebo-controlled trial performed on client-owned dogs with confirmed OA. It was approved by the Virbac Ethical Review Committee prior to the start of the study (Approbation number; EU-ERC 2022008–02). The protocol complied with European Directive 2010-63-EU and application of the 3Rs principles and Virbac Code of Animal Care. The study took place in nine specialized veterinary clinics in seven European countries (Hungary, Romania, Latvia, Portugal, Spain, Italy, and France) between January 2023 and February 2024. All owners gave their consent to participate in the study.
2.1 Animals
Client-owned dogs with signs of mobility issues were recruited based on the following inclusion criteria: at least 3 years of age; body weight between 15 and 35 kg; mobility disorders present for at least 3 months, according to the owner; presenting at least two signs of mobility issues (difficulty to walk / lag behind during walks; difficulty to stand up after lying down; difficulty to jump; difficulty to walk up or down stairs; clear lameness or stiffness after exercise); and radiographic evidence of OA, with definite osteophytes, in at least the hip, elbow, carpal or tarsal joint. Exclusion criteria included any concomitant systemic or neurological disease such as cardiovascular disease, immune-mediated disease (e.g., lupus), obesity (body condition score >7/9 or 4/5), infection, neoplastic disease, or allergies. Pregnant or lactating bitches were also excluded. Dogs who received NSAIDs, glucocorticoids or analgesics recently were excluded unless a wash-out period was respected: 2 weeks for NSAIDs, ‘short-acting’ glucocorticoids (e.g., oral prednisone, and topical glucocorticoid preparations), gabapentin or tramadol; 2 months for oral or parenteral ‘long-acting’ glucocorticoids (e.g., injectable methylprednisolone acetate) and anti-NGF monoclonal antibodies; 3 months for intra-articular injection of any material into any joint. Dogs with any joint instability due to ruptured ligament, dogs with stifle disease, and dogs who had surgery on any joint within 180 days before enrollment were excluded. Indeed, short-term progression (6 months as defined by Cook et al. (62)) could be constant after surgery and could introduce a bias. Dogs with stifle OA were excluded to avoid bias, as their lameness could stem from post-operative complications, mechanical instability, or meniscal damage rather than OA alone (14, 63). For ethical reasons, acute pain management with analgesic drugs (e.g., gabapentin, tramadol) were authorized in case of severe pain or marked decrease of quality of life (QoL), if stopped at least 1 week before the next visit. All treatments given for pain were noted down and considered rescue treatments. Nutraceuticals were allowed if administered for at least 12 weeks prior to enrollment and maintained during the whole study period.
2.2 Products and randomization
The product tested was a joint supplement (MovoflexⓇ Soft Chews, Virbac, France), containing eggshell membrane (3.3%), krill meal (1.85%), algae meal (Haematococcus pluvialis – 0.26% – as a source of astaxanthin), hyaluronic acid (of high & low molecular weights – 0.49%), and a Boswellia serrata extract (0.57%). Other ingredients included pre-gelatinized rice, glycerine, derivatives of vegetable origin, pre-gelatinized maize starch, sunflower refined oil, sorbitol, sugars, pea protein, yeasts, pre-gelatinized rice starch, maltodextrin, minerals, rapeseed oil, and powder cellulose. The placebo (same formula but without the 5 key ingredients listed above: eggshell membrane, krill meal, algae meal, hyaluronic acid and Boswellia serrata extract) was a soft chew that matched in size the joint supplement. The supplement and its placebo were in white jars labeled A or B so that both investigators and owners were blinded to the treatment group. Each jar contained 30 chews and three jars were given for the duration of the study. One soft chew per day (test or placebo) adapted to dogs 15–35 kg was given for 90 days. Dogs were randomly allocated to product A or B using a table of random numbers with a block randomization design of size 2.
2.3 Design and outcomes measured
After inclusion of an animal in the study on day 0, the owner completed the Canine Brief Pain Inventory (CBPI) and Liverpool Osteoarthritis in Dogs index (LOAD), two validated clinical tools to assess osteoarthritis in dogs (15–17). At the end of the CBPI inventory, the owner must grade the dog’s quality of life from 1-poor to 5-excellent. The owner also had to grade the dog’s discomfort from 1-none to 4-unbearable. Explanations about the questionnaires and guidance for the replies to provide were given to the owners. The same questionnaires were completed after 15, 30, 60, and 90 days by the same owner (except for one dog, on one occasion). The investigator performed a clinical evaluation to grade the dog and affected joints. Measures included evaluation of the effect on the dog’s posture and motion (from 1-normal to 4-severely abnormal) and on the joint’s pain upon palpation (from 1-none to 4-severe) and passive range of movement (ROM – from 1-normal to 4-severely abnormal), as described previously (64). The sum of the four scores given was used as the clinical score (from 4 to 16). This clinical evaluation was also performed after 30, 60 and 90 days in the study.
2.4 Statistical analysis
Based on the LOAD data from a previous pilot study performed on a similar formulation, with a mean of 15 in the test group and of 24 in the placebo group on Day 84, and a standard deviation of 9, at least 22 cases per group were required in order to see a statistically significant difference with an α of 0.05 and power level of 0.9 (61). The mean dogs’ age and body weight were compared between groups at D0 using a Student’s t-test in case of normal distribution and otherwise using the Mann–Whitney (Wilcoxon) test. A Friedman test was used for intragroup comparisons of the scores over time. In case of significance, post hoc pairwise comparisons were performed using Dunn’s multiple comparisons test for comparison of data versus day 0. If a statistical significance was obtained in both groups, a generalized linear mixed-effects model was used for intergroup analyses of the scores over time (with the time as fixed effect and the dog as random effect), focusing on the time x treatment interaction for significance. The use of rescue analgesia and the compliance were compared between groups using Kendall’s Tau b.
The significance level was set at p < 0.05. Analyses were performed using the Statgraphics Centurion (version XVI.II) and GraphPad Prism (version 10) softwares.
3 Results
3.1 Study population
A total of fifty-two dogs were recruited. Twenty-six dogs received the test supplement and twenty-six received the placebo. In the supplement group, one dog abandoned the study after three weeks for a lack of improvement, two had OA on the knee at inclusion (an exclusion criteria) and one was euthanized for a cardiac tumor. These four dogs were therefore removed from the analysis. In the placebo group, one dog was lost to follow-up and one had OA on the knee and were therefore removed from the analysis. In the end, twenty-two dogs in the supplement group and twenty-four dogs in the placebo group were analyzed. The compliance was overall very good in all dogs. A few dogs (eight in each group) missed some administrations in both groups but only occasionally (less than a third of the time) and were therefore kept for analysis. The percentage of non-compliance was not significantly different between groups (p > 0.5 at each period). No side effects were reported during the study.
Among the analyzed dogs, fifteen dogs received NSAIDs at some point since being diagnosed with OA. Two were still taking NSAIDs two weeks prior the enrollment and had to apply a wash-out period before starting the study. Two dogs received anti-NGF monoclonal antibodies in the past, including one in the last two months before enrollment. This dog had to apply a wash-out period before starting the study. Some dogs also received joint supplements (n = 19) and/or fish oil (n = 9) that could be continued if given for at least twelve weeks prior to inclusion and continued throughout the study. Other past therapies included IA injections (n = 3), rehabilitation/physiotherapy (n = 3), laser and magnetic therapy (n = 1, each).
On day 0, there was no difference between the groups for the breed, sex, age, body weight, OA grade (assessed by radiography) or joint(s) affected (Table 1). There were also no significant differences between groups on day 0 for the LOAD, discomfort, clinical score and subscores despite apparent higher scores in the supplement group (Table 2). However, the CBPI scores for pain interference, total, and quality of life were significantly higher (worse) in the supplement group (Table 2).
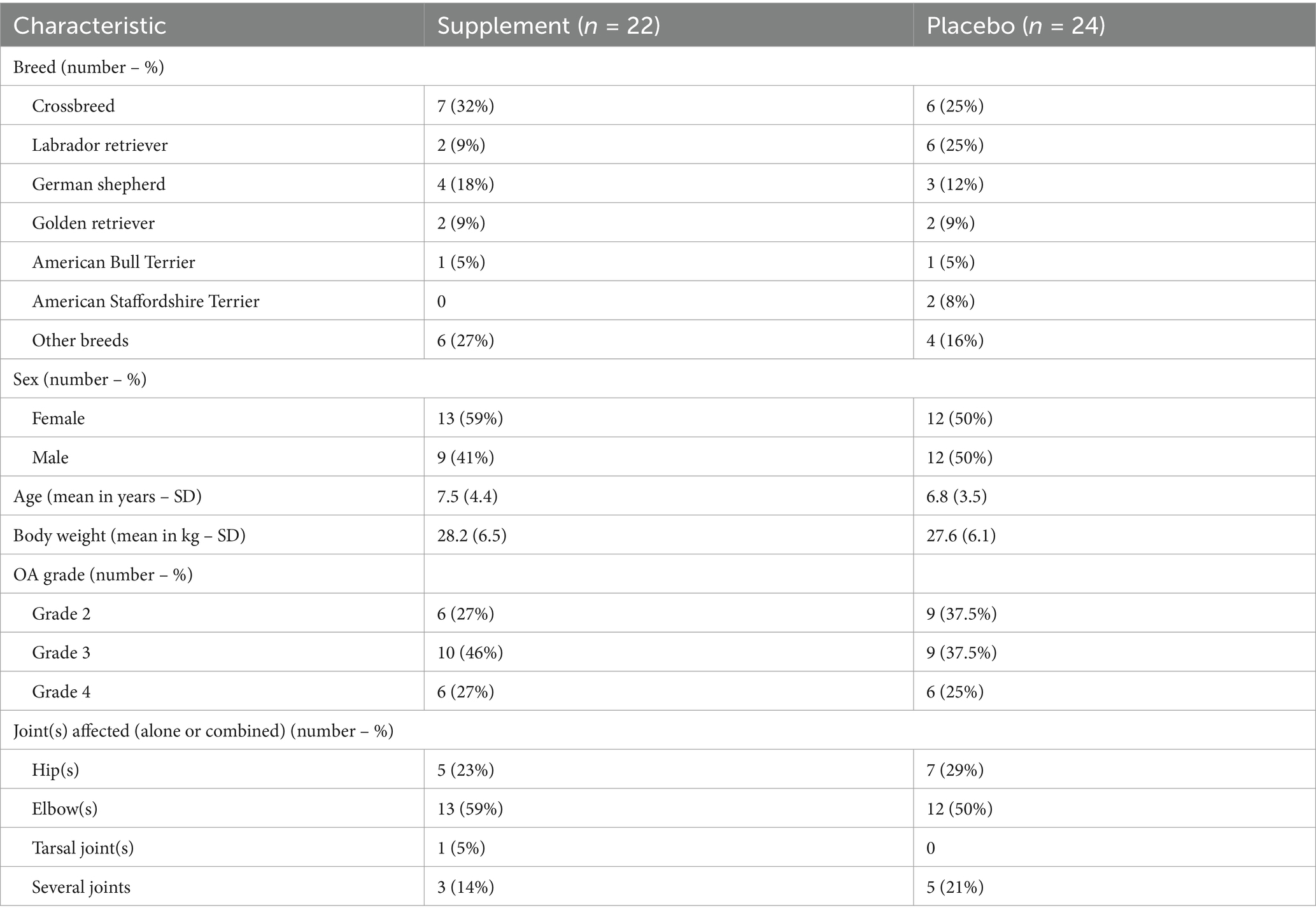
Table 1. Demographic information of enrolled dogs that completed the 3-month study and were included in data analysis.
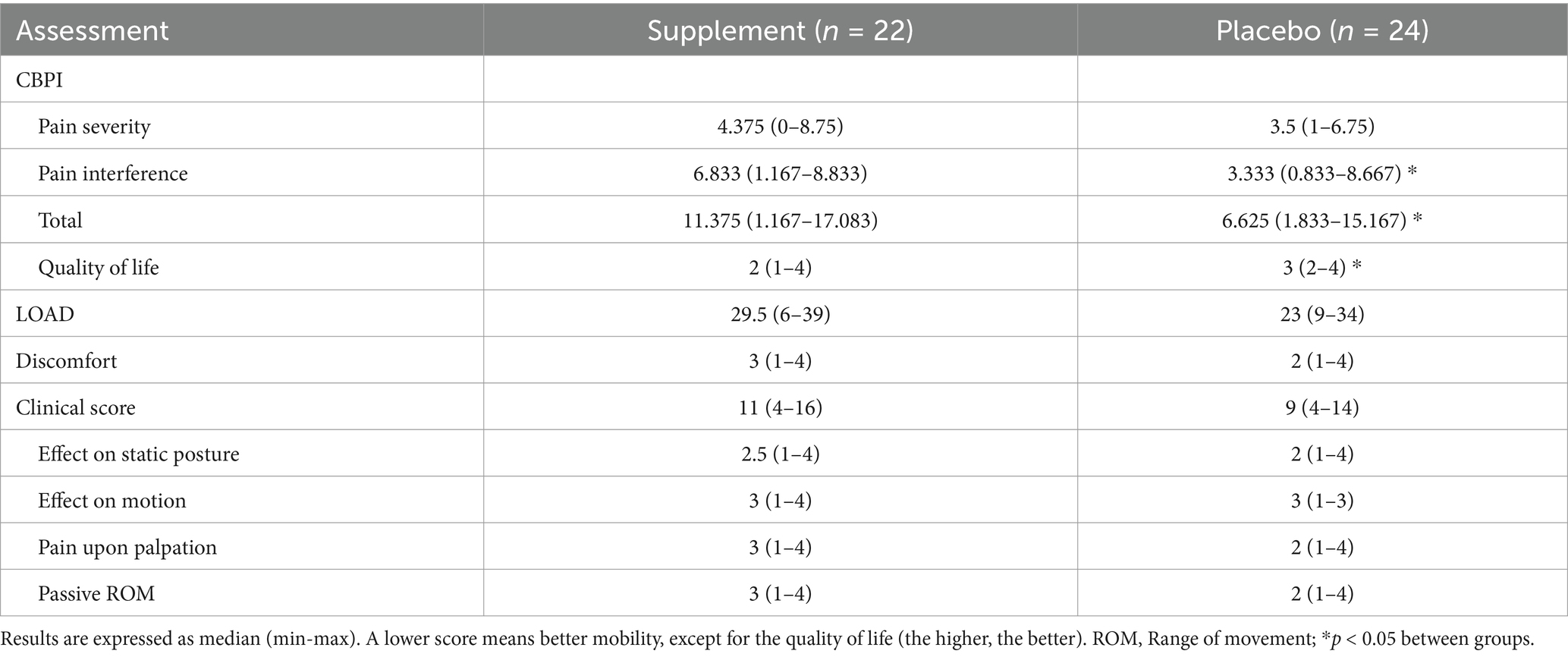
Table 2. Baseline scores of the parameters assessed by owners and veterinarians.
3.2 Evolution of parameters assessed by owners
The CBPI pain severity score (PSS) significantly improved over time in the supplement group (−57% in median score by day 90, p = 0.0003, Table 3) but not in the placebo group (−46%, p = 0.1008, Table 3). Pairwise comparisons versus day 0 showed a significant improvement on day 90 in the supplement group (p = 0.0034, Figure 1A; Table 3).
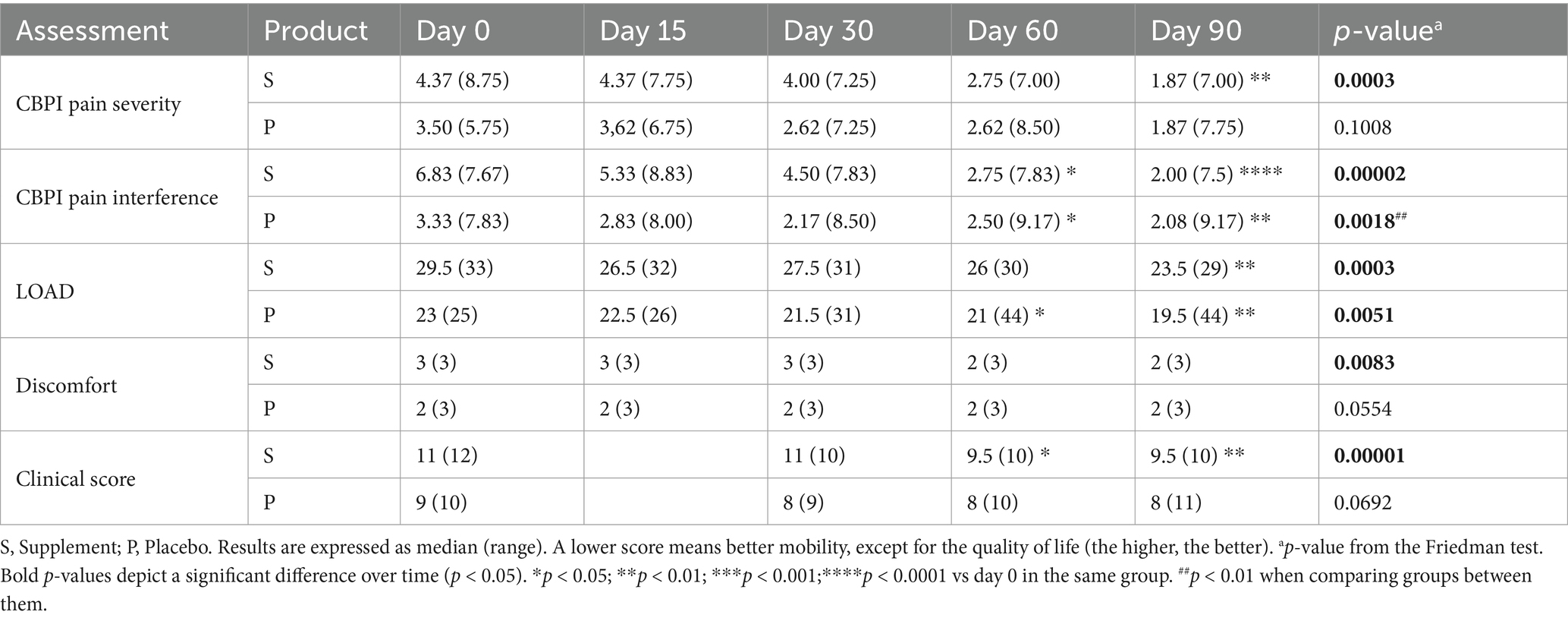
Table 3. Evolution of the main parameters over time.
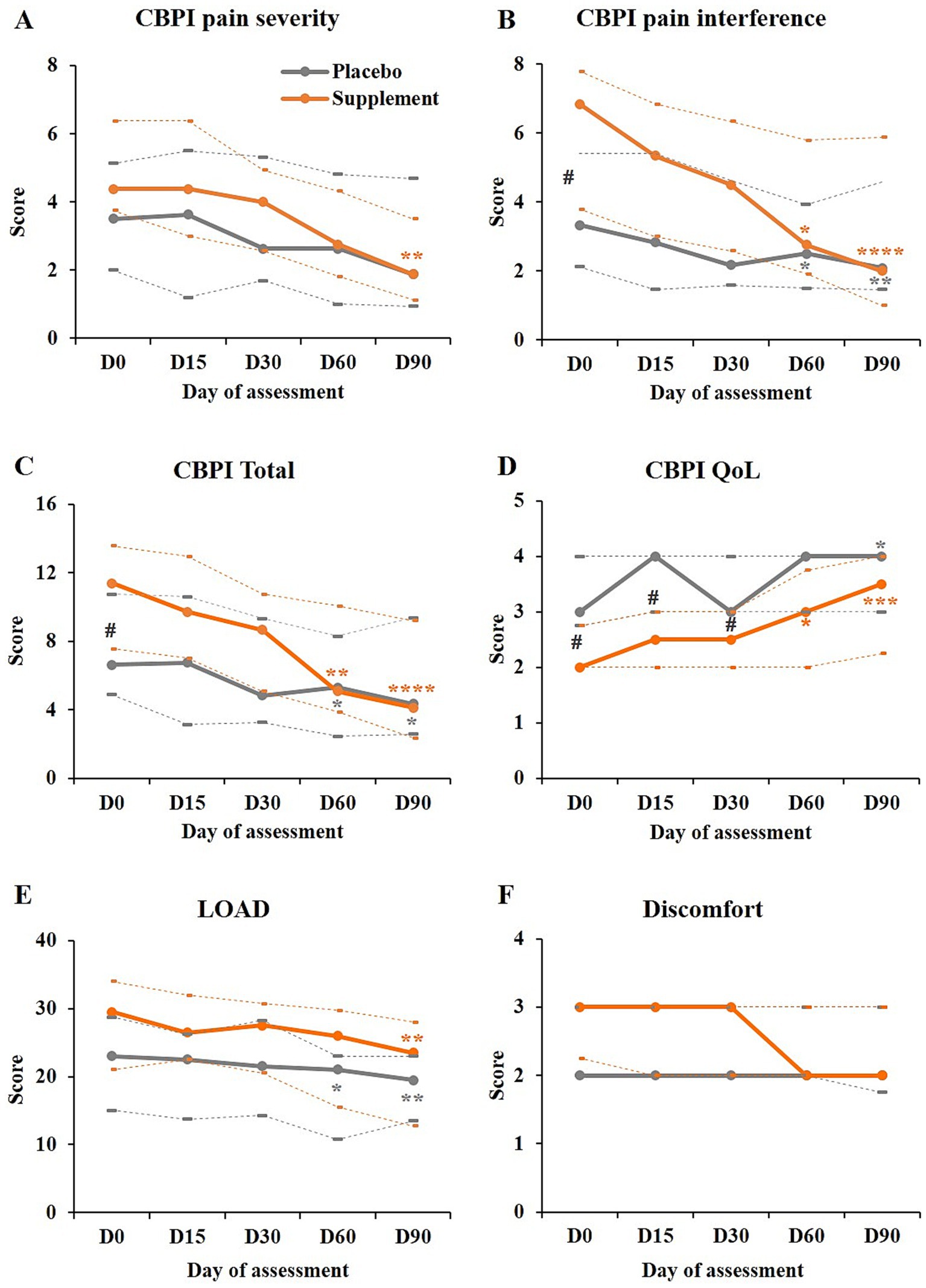
Figure 1. Evolution of the parameters assessed by owners. (A–D) Scores obtained for the CBPI pain severity, pain interference, total, and for the quality of life (QoL), as indicated, in the supplement group (orange) and placebo group (grey). (E,F) LOAD and discomfort scores obtained in both groups [legend as in (A)]. In all graphs, the plain lines represent the medians, and dotted lines below and above represent the first and third quartiles, respectively. In all graphs except the CBPI quality of life, a decrease in score represents an improvement. Pairwise comparisons versus day 0: *p < 0.05; **p < 0.01; ***p < 0.001; ****p < 0.0001. #p < 0.05 between groups.
The CBPI pain interference score (PIS) significantly improved over time in both groups: −71% in median score by day 90 in the supplement group (p < 0.0001) and −38% in the placebo group (p = 0.0018, Table 3). However, the improvement over time was significantly greater with the supplement than with the placebo (p = 0.009). Pairwise comparisons versus day 0 showed a significant improvement on days 60 and 90 in the supplement group (p = 0.0304 and p < 0.0001, respectively) and in the placebo group (p = 0.0139 and p = 0.001, respectively, Figure 1B; Table 3).
The total CBPI score (sum of both previous scores) significantly improved over time in both groups: −64% in median score by day 90 in the supplement group (p < 0.0001, Supplementary Table 1) and −35% in the placebo group (p = 0.0186, Supplementary Table 1). The improvement over time was also significantly greater with the supplement than with the placebo (p = 0.0187, Supplementary Table 1). The improvement versus day 0 was significant as of day 60 in the supplement group (p = 0.0048 and p < 0.0001 on days 60 and 90, respectively) and in the placebo group (p = 0.0423 and p = 0.0104, respectively, Figure 1C; Supplementary Table 1).
The quality of life in the supplement group was significantly worse (lower score) than in the placebo group on days 0 to 30 (p < 0.05, Figure 1D); by day 60, there was no more difference between groups. While both groups showed a significant improvement over time (p < 0.0001 and p = 0.0071 in the supplement and placebo groups, respectively, Supplementary Table 1), with no significant difference between groups, the improvement in median score by day 90 was only of 33% in the placebo group but of 75% in the supplement group. Pairwise comparisons versus day 0 showed a significant improvement on days 60 and 90 in the supplement group (p = 0.0145 and p = 0.0005, respectively) and on day 90 in the placebo group (p = 0.0371, Figure 1D; Supplementary Table 1).
The LOAD score significantly improved over time in both groups (p = 0.0003 and p = 0.0051 in the supplement and placebo groups, respectively, Table 3). The median scores decreased by 20% in the supplement group and by 15% in the placebo group by day 90, with no significant difference between groups. Pairwise comparisons versus day 0 showed a significant improvement on day 90 in the supplement group (p = 0.0017) and on days 60 and 90 in the placebo group (p = 0.0186 and p = 0.0029, Figure 1E; Table 3).
Consistently with the other parameters, the discomfort in the supplement group seemed to be more severe than in the placebo group on day 0, although not to a significant level (median of 3 vs. 2, respectively, Table 1; Figure 1F). Over time, the dog’s discomfort significantly improved in the supplement group (−1 point in median score or 33% change by day 90; p = 0.0083) but not in the placebo group (no change in median score; p = 0.0554, Figure 1F; Table 3). However, pairwise comparisons with day 0 did not show any significant difference in the supplement group (Figure 1F; Table 3).
3.3 Evolution of parameters assessed by investigators
The clinical score significantly improved in the supplement group (by 14% by day 90, p < 0.0001) but not in the placebo group (11% improvement, p = 0.0692). The improvement in the supplement group was significant as of day 60 (p = 0.0426 and p = 0.0014 on days 60 and 90 respectively, Figure 2A; Table 3).
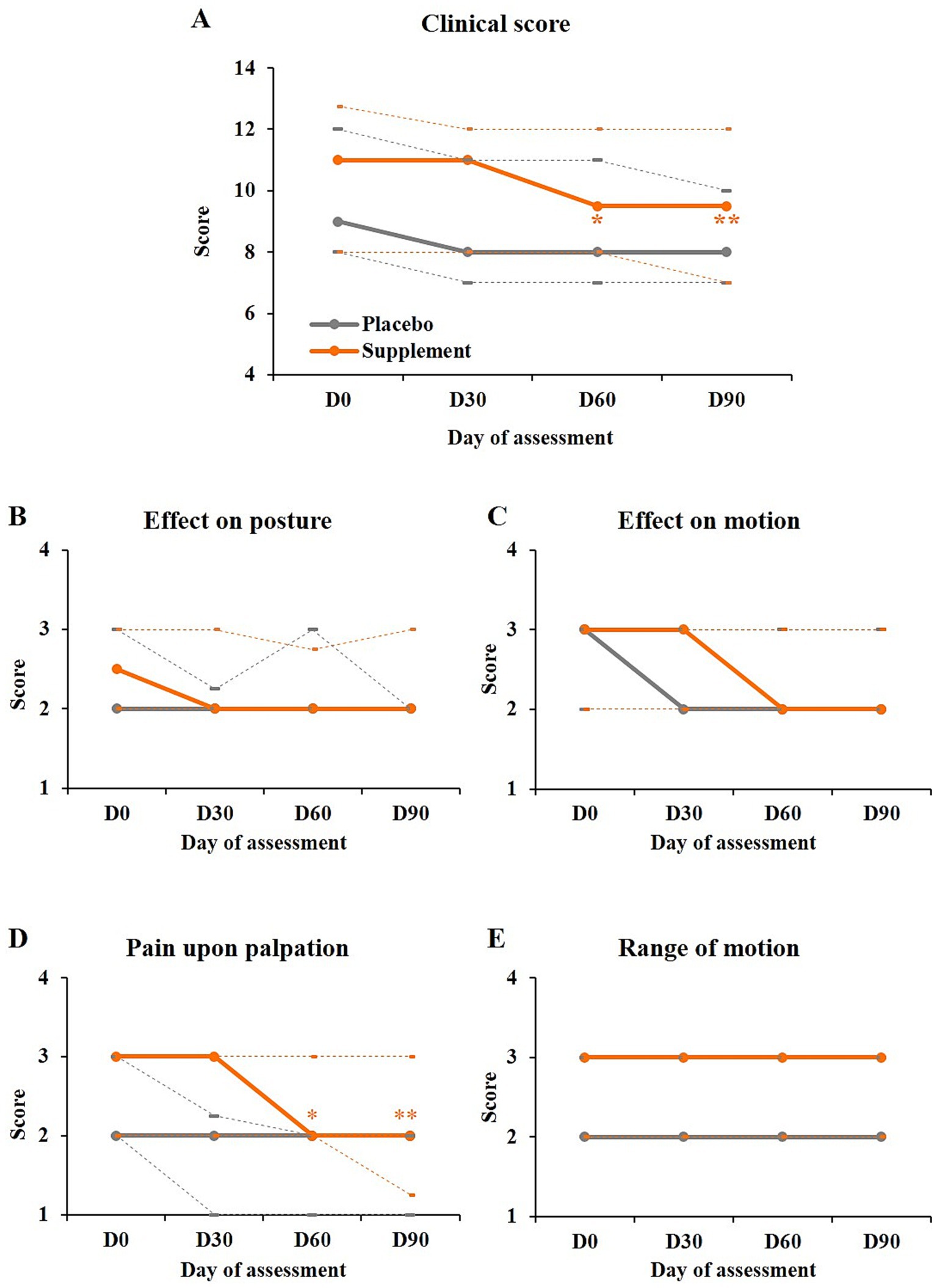
Figure 2. Evolution of the parameters assessed by the investigators. (A) Clinical scores (sum of the four subscores) obtained in both groups. (B–E) Subscores of the clinical score as indicated. Legend as in Figure 1. Pairwise comparisons versus day 0: *p < 0.05; **p < 0.01.
The data from each subscore (Figures 2B–E; Supplementary Table 1) showed that the effect in the supplement group mainly came from the pain upon palpation which was significantly improved over time (p < 0.0001) and as of day 60 in this group (p = 0.0152 and p = 0.0032 on days 60 and 90 respectively, Figure 2D; Supplementary Table 1).
3.4 Rescue analgesia
For ethical reasons, dogs were allowed to receive rescue analgesia if stopped at least one week before the next visit. Five dogs in the supplement group needed rescue analgesia once during the study for one to ten days. Another one needed it twice during the study for seven days each time. Three dogs in the placebo group received rescue analgesia once during the study, for one to seven days. The frequency of rescue analgesia was not significantly different between groups.
4 Discussion
This study evaluated the efficacy of a joint supplement for dogs containing a mixture of five main ingredients: ESM, hyaluronic acid (HA of different molecular weight), krill meal [rich in omega-3 fatty acids (42)], a natural source of astaxanthin [Haematococcus pluvialis (38)], and a Boswellia serrata extract. The results of this placebo-controlled study showed that all five main parameters assessed (LOAD, CBPI pain severity, CBPI pain interference, discomfort and clinical score) were significantly improved with the supplement while only the LOAD and CBPI pain interference were improved in the placebo group. Furthermore, the improvement of the latter parameter was significantly higher in the supplement group than in the placebo group. The test supplement is therefore efficacious in improving mobility and discomfort in osteoarthritic dogs.
A previous placebo-controlled pilot study with a similar formula as the one tested here (but without krill and low molecular weight HA) had shown promising results based on the LOAD score and inflammatory biomarkers like IL2 (61). This previous study had a lower number of animals per group and some parameters like the CBPI scores were not improved. In the present study, all main parameters assessed, including the CBPI and LOAD were improved. It is still unclear why the CBPI scores were not significantly improved in the preliminary study (61). The addition of krill, rich in omega-3 fatty acids (42–44), to the tested formula could be a potential explanation but it could also be due to a type II error in the previous study (61) or to other unexplained factors. The LOAD and CBPI, two main outcome measures in this study, are validated client-reported outcomes measures (CROMs – or clinical metrology instruments – CMIs) for the assessment of OA in dogs that have been used in many studies and are known to correlate well (15, 17, 61, 65–70). The CBPI assesses the magnitude of the pain over the last seven days (pain severity) and its impact on the dog’s mobility and daily activities like standing, walking, running or climbing up stairs (pain interference). The LOAD assesses the dog’s general mobility and mobility during exercise (no precision on the type of exercise), focusing on the level of activity and willingness to exercise, and on lameness rather than on the joint function (13). It also includes questions about the effect of weather on the dog’s activity (17). The rating scales are also different since the CBPI is based on an 11-point numerical rating scale while the LOAD is based on a 5-point Likert scale. Such differences could explain the discrepancies in this study and others (62, 70, 71). The results and interpretation of different CROMs may also vary depending on the dog population studied (breed, body weight, etc.), joint(s) affected, and components of the disease captured by the questionnaires, as outlined in previous studies (13, 65, 71). It is also possible that the owners have paid more attention to the way their dogs were moving over time, knowing which questions would be asked. This may explain partly the improvement observed in the placebo group for the CBPI pain interference and LOAD and could limit the conclusions of the study.
In the present study, we selected dogs with OA of the hip(s), elbow(s), tarsal or carpal joint(s) and excluded dogs with knee OA. Some dogs also had several joints affected. Despite the inclusion criteria to purposely limit the uncontrolled variability, the population selected varied in terms of joints affected (elbows, hips, tarsal joints or several of these). The proportion of joints affected did not differ significantly between groups. However, the OA grade and all assessed parameters tended to be worse in the supplement group than in the placebo group on day 0, with a significant difference between groups for the CBPI scores. This is opposed to what was found in the pilot study where dogs in the placebo group tended to be more severely affected (61). This difference, together with the differences in number of animals, formula and study population, could partly explain the differences in results observed between both studies.
The results obtained in discomfort and clinical scores, with significant differences in the supplement group but not in the placebo group, also support the beneficial action of the joint supplement. The effect would be particularly important on pain (as captured by the pain upon palpation and CBPI) rather than on the joint’s range of movement. This latter parameter may indeed depend on mechanical ones, like the presence of osteophytes and reduction of synovial space, that the supplement may not address as well. Other modalities, like activity modulation and rehabilitation, that may take longer to act, could also influence this parameter. A veterinary assessment was not performed in the pilot study but the change in some blood inflammatory markers like IL2 also suggested a positive evolution of the inflammatory process (61).
Based on the ingredients in the test supplement, an improvement in mobility is not surprising. Mobility improvements were also observed in studies assessing the effect of ESM in dogs with hip dysplasia or suboptimal joint function or in studies assessing the effect of Boswellia serrata in canine inflammatory joint and spinal disease (29, 34, 58). The omega-3 fatty acids (FA) found in krill may also play a part in this improvement, especially in the improvement of pain. Omega-3 FA have indeed been proven to have clinical analgesic efficacy in a meta-analysis (20). Studies have shown that amounts as low as 70 mg/kg body weight/day of eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) from fish could decrease pain score and improve the quality of life of OA dogs (72, 73). However, the absorption and hence the efficacy of omega-3 FA also depends on the form and quality of these omega-3. It was found that the omega-3 from krill, bound to phospholipids, were better absorbed than those from other sources like fish or flaxseed, leading to a higher omega-3 index in dogs (42–44). These properties make krill a promising ingredient for joint disorders, including osteoarthritis, and other diseases (42, 45–48, 74, 75). The richness in phospholipids in krill can also help the absorption of other ingredients like astaxanthin – a potent antioxidant present in Haematococcus pluvialis and krill (38, 76) – and hyaluronic acid (50, 52). The addition of krill and HA of low molecular weight – for its known effect on cartilage maintenance (35, 36) – to the supplement already containing ESM, astaxanthin, a Boswellia serrata extract and hyaluronic acid of high molecular weight, has indeed given better results in dogs with mobility issues (60). The test supplement contains 1.86% of krill (around 74 mg) and therefore a lower dose of omega-3 FA than the one proven to be efficient in other studies. It is probably the combination of all the ingredients present in the test supplement and the synergy between them that make the test supplement efficient. The onset of action may depend on the severity of the disease, though. In dogs with light mobility disorders, owners felt an improvement in some mobility aspects in as early as seven days (59, 60). In this study, although some scores started to decrease by day 15, significant improvements were only observed by day 60 or 90, suggesting a longer onset of action in dogs with more severe OA. Importantly, all the ingredients present in the test supplement, from natural origin, are known to be safe and the good tolerance observed in this study and previous ones confirms it (59–61). The acceptability of the test supplement was also very good, allowing good compliance.
The significant difference observed between groups on day 0 for some parameters, despite the randomization, is the main limitation of the study. However, showing that all main parameters significantly improved with the supplement but not always with the placebo (or to a lesser extent) while the dogs were more severely affected in the former group, is a strong argument toward a beneficial action of the supplement. The lack of objective gait analysis is another limitation of this study that should be taken into account for future studies to limit the well-known placebo effect (13, 77). A previous study found that to detect a treatment effect in dogs with OA based on the CBPI, thresholds should be applied at inclusion (PIS and PSS ≥ 2) and success for each patient predefined as a decrease ≥ 1 in PSS and a decrease ≥ 2 in PIS (78). Success for each patient could be defined as a score decrease ≥ 4 for the LOAD (79). The current study design did not include these criteria due to their association with evaluating more severely impacted dogs and the need for an increased sample size, which would make recruitment especially challenging for a supplement trial. Furthermore, these criteria may be more applicable to test a drug and less so to test a supplement, which should not be given as a sole treatment for these advanced OA cases.
For the purpose of the study, we had to limit the treatments received by dogs but an efficient OA treatment cannot be based only on joint supplements and should include a variety of approaches including drugs (anti-inflammatory and analgesics) and physical therapy (18). However, efficient chondroprotective joint supplement like the one tested are still beneficial in OA dogs, regardless of the OA stage (1, 24).
5 Conclusion
This multicenter, double-blind, randomized, placebo-controlled study showed that the test supplement, containing ESM, krill meal, astaxanthin (via the algae meal Haematococcus pluvialis), hyaluronic acid and a Boswellia serrata extract, can improve the mobility and quality of life of dogs with OA. Indeed, all five main parameters tested (CBPI pain severity, CBPI pain interference, LOAD, discomfort, and clinical score) were significantly improved during the 90-day study in the group of dogs receiving the supplement while only two of them (CBPI pain interference and LOAD) improved in the placebo group and to a lesser extent. This study is in agreement with previous studies showing the effectiveness of the ingredients present in the test supplement in improving joint health. The test supplement could then be considered a valuable component of a multimodal approach to managing OA in dogs. Additionally, it may be beneficial for maintaining joint health, particularly in dogs predisposed to OA.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The animal studies were approved by Virbac Ethical Review Committee. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent was obtained from the owners for the participation of their animals in this study.
Author contributions
GR: Conceptualization, Investigation, Methodology, Writing – original draft, Writing – review & editing. ÂM: Conceptualization, Investigation, Methodology, Writing – original draft, Writing – review & editing. CO: Investigation, Writing – original draft, Writing – review & editing. SB: Investigation, Writing – original draft, Writing – review & editing. CN: Conceptualization, Formal analysis, Methodology, Project administration, Resources, Supervision, Validation, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. The study was financed by Virbac SA.
Acknowledgments
The authors would like to thank Zsolt Sebestyén, Levente Szilvássy, Guntars Avdoško, Gustavs Krauklis, Sergio Ruiz, Enrico Panichi, and their colleagues for their participation as investigators in this study. The authors are grateful for permission to use the Liverpool Osteoarthritis in Dogs (LOAD) index, a clinical metrology instrument developed by the University of Liverpool and exclusively distributed by Elanco Animal Health, for the evaluation of the supplement in this study.
Conflict of interest
CN is a Virbac SA employee. GR, ÂM, CO, and SB received financial support from Virbac SA to conduct the study.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fvets.2025.1561793/full#supplementary-material
References
1. Mosley, C, Edwards, T, Romano, L, Truchetti, G, Dunbar, L, Schiller, T, et al. Proposed Canadian Consensus Guidelines on Osteoarthritis Treatment based on OA-COAST Stages 1–4. Front Vet Sci. (2022) 9:830098. doi: 10.3389/fvets.2022.830098
2. O’Neill, DG, James, H, Brodbelt, DC, Church, DB, and Pegram, C. Prevalence of commonly diagnosed disorders in UK dogs under primary veterinary care: results and applications. BMC Vet Res. (2021) 17:69. doi: 10.1186/s12917-021-02775-3
3. Forsyth, KK, BM, MC, Schmid, SM, Promislow, DEL, Snyder-Mackler, N, and Creevy, KE. Lifetime prevalence of owner-reported medical conditions in the 25 most common dog breeds in the dog aging project pack. Front Vet Sci. (2023) 10:1140417. doi: 10.3389/fvets.2023.1140417
4. Marshall, WG, Bockstahler, BA, Hulse, DA, and Carmichael, S. A review of osteoarthritis and obesity: current understanding of the relationship and benefit of obesity treatment and prevention in the dog. Vet Comp Orthop Traumatol. (2009) 22:339–45. doi: 10.3415/VCOT-08-08-0069
5. Anderson, KL, O’Neill, DG, Brodbelt, DC, Church, DB, Meeson, RL, Sargan, D, et al. Prevalence, duration and risk factors for appendicular osteoarthritis in a UK dog population under primary veterinary care. Sci Rep. (2018) 8:5641. doi: 10.1038/s41598-018-23940-z
6. Anderson, KL, Zulch, H, O’Neill, DG, Meeson, RL, and Collins, LM. Risk factors for canine osteoarthritis and its predisposing arthropathies: a systematic review. Front Vet Sci. (2020) 7:220. doi: 10.3389/fvets.2020.00220
7. Graves, JL, McKenzie, BA, Koch, Z, Naka, A, Spofford, N, and Morrison, J. Body weight, gonadectomy, and other risk factors for diagnosis of osteoarthritis in companion dogs. Front Vet Sci. (2023) 10:1275964. doi: 10.3389/fvets.2023.1275964
8. Enomoto, M, de Castro, N, Hash, J, Thomson, A, Nakanishi-Hester, A, Perry, E, et al. Prevalence of radiographic appendicular osteoarthritis and associated clinical signs in young dogs. Sci Rep. (2024) 14:2827. doi: 10.1038/s41598-024-52324-9
9. Roitner, M, Klever, J, Reese, S, and Meyer-Lindenberg, A. Prevalence of osteoarthritis in the shoulder, elbow, hip and stifle joints of dogs older than 8 years. Vet J. (2024) 305:106132. doi: 10.1016/j.tvjl.2024.106132
10. Alves, JC, Santos, A, Jorge, P, Lavrador, C, and Carreira, LM. Clinical and diagnostic imaging findings in police working dogs referred for hip osteoarthritis. BMC Vet Res. (2020) 16:425. doi: 10.1186/s12917-020-02647-2
11. Cachon, T, Frykman, O, Innes, JF, Lascelles, BDX, Okumura, M, Sousa, P, et al. COAST Development Group’s international consensus guidelines for the treatment of canine osteoarthritis. Front Vet Sci. (2023) 10:1137888. doi: 10.3389/fvets.2023.1137888
12. Belshaw, Z, Dean, R, and Asher, L. Could it be osteoarthritis? How dog owners and veterinary surgeons describe identifying canine osteoarthritis in a general practice setting. Prev Vet Med. (2020) 185:105198. doi: 10.1016/j.prevetmed.2020.105198
13. Clark, N, and Comerford, E. An update on mobility assessment of dogs with musculoskeletal disease. J Small Anim Pract. (2023) 64:599–610. doi: 10.1111/jsap.13650
14. Ramírez-Flores, GI, Del Angel-Caraza, J, Quijano-Hernández, IA, Hulse, DA, Beale, BS, and Victoria-Mora, JM. Correlation between osteoarthritic changes in the stifle joint in dogs and the results of orthopedic, radiographic, ultrasonographic and arthroscopic examinations. Vet Res Commun. (2017) 41:129–37. doi: 10.1007/s11259-017-9680-2
15. Brown, DC, Boston, RC, Coyne, JC, and Farrar, JT. Ability of the canine brief pain inventory to detect response to treatment in dogs with osteoarthritis. J Am Vet Med Assoc. (2008) 233:1278–83. doi: 10.2460/javma.233.8.1278
16. Brown, DC, Boston, RC, Coyne, JC, and Farrar, JT. Development and psychometric testing of an instrument designed to measure chronic pain in dogs with osteoarthritis. Am J Vet Res. (2007) 68:631–7. doi: 10.2460/ajvr.68.6.631
17. Walton, MB, Cowderoy, E, Lascelles, D, and Innes, JF. Evaluation of construct and criterion validity for the “Liverpool Osteoarthritis in Dogs” (LOAD) clinical metrology instrument and comparison to two other instruments. PLoS One. (2013) 8:e58125. doi: 10.1371/journal.pone.0058125
18. Gruen, ME, Lascelles, BDX, Colleran, E, Gottlieb, A, Johnson, J, Lotsikas, P, et al. 2022 AAHA pain management guidelines for dogs and cats. J Am Anim Hosp Assoc. (2022) 58:55–76. doi: 10.5326/JAAHA-MS-7292
19. Cordingley, DM, and Cornish, SM. Omega-3 fatty acids for the management of osteoarthritis: a narrative review. Nutrients. (2022) 14:3362. doi: 10.3390/nu14163362
20. Barbeau-Grégoire, M, Otis, C, Cournoyer, A, Moreau, M, Lussier, B, and Troncy, E. A 2022 systematic review and meta-analysis of enriched therapeutic diets and nutraceuticals in canine and feline osteoarthritis. Int J Mol Sci. (2022) 23:10384. doi: 10.3390/ijms231810384
21. Calder, PC. Omega-3 fatty acids and inflammatory processes: from molecules to man. Biochem Soc Trans. (2017) 45:1105–15. doi: 10.1042/BST20160474
22. Rossi, F, Cancedda, S, Leone, VF, Rohrer Bley, C, and Laganga, P. Megavoltage radiotherapy for the treatment of degenerative joint disease in dogs: results of a preliminary experience in an Italian radiotherapy centre. Front Vet Sci. (2018) 5:74. doi: 10.3389/fvets.2018.00074
23. Pye, C, Clark, N, Bruniges, N, Peffers, M, and Comerford, E. Current evidence for non-pharmaceutical, non-surgical treatments of canine osteoarthritis. J Small Anim Pract. (2024) 65:3–23. doi: 10.1111/jsap.13670
24. Hoffman, JM, Tolbert, MK, and Promislow, DEL. Dog Aging Project Consortium. Demographic factors associated with joint supplement use in dogs from the Dog Aging Project. Front Vet Sci. (2022) 9:906521. doi: 10.3389/fvets.2022.906521
25. Baláž, M, Boldyreva, EV, Rybin, D, Pavlović, S, Rodríguez-Padrón, D, Mudrinić, T, et al. State-of-the-Art of eggshell waste in materials science: recent advances in catalysis, pharmaceutical applications, and mechanochemistry. Front Bioeng Biotechnol. (2020) 8:612567. doi: 10.3389/fbioe.2020.612567
26. Rath, NC, Liyanage, R, Makkar, SK, and Lay, JO Jr. Protein profiles of hatchery egg shell membrane. Proteome Sci. (2016) 15:4. doi: 10.1186/s12953-017-0112-6
27. Blasco, JM-Í, Aguirre, A, Gil-Quintana, E, and Fenaux, M. The effect of daily administration of 300 mg of Ovomet® for treatment of arthritis in elderly patients. Int J Clin Rheumtol. (2016). 11, 077–081. Available at: https://www.openaccessjournals.com/articles/the-effect-of-daily-administration-of-300-mg-of-ovomet174-for-treatment-of-arthritis-in-elderly-patients.pdf
28. Gil-Quintana, E, Fenaux, M, La Nuez, M, Molero, A, and Aguirre, A. Short-term effects of ovomet®, eggshell membrane. Joint pain: A double-blind and placebo study. J Osteopor Phys Act. (2018). 6:1. doi: 10.4172/2329-9509.1000211
29. Aguirre, A, Gil-Quintana, E, and Fenaux, M (2018). The efficacy of Ovopet in the treatment of hip dysplasia in dogs. Journal of Veterinary Medicine and Animal Health. (2018) 10:198–207. doi: 10.5897/JVMAH2018.0687
30. Cánovas, F, Abellán-Ruíz, MS, García-Muñoz, AM, Luque-Rubia, AJ, Victoria-Montesinos, D, Pérez-Piñero, S, et al. Randomised clinical trial to analyse the efficacy of eggshell membrane to improve joint functionality in knee osteoarthritis. Nutrients. (2022) 14:2340. doi: 10.3390/nu14112340
31. Cánovas, F, Planes-Muñoz, D, Jaione Zurbano, M, Messia, P, and Isabel, VM. Randomized clinical trial to analyze the efficacy of an eggshell membrane dietary supplementation in the concomitant treatment of osteoarthritis in dogs. World J Food Sci Technol. (2023). 14:2340. doi: 10.11648/j.wjfst.20230703.11
32. Fladerer, J-P, and Grollitsch, S. Eggshell membrane as promising supplement to maintain bone health: A systematic review. Bone Rep. (2024) 21:101776. doi: 10.1016/j.bonr.2024.101776
33. García-Muñoz, AM, Abellán-Ruiz, MS, García-Guillén, AI, and Victoria-Montesinos, D. Efficacy of eggshell membrane in knee osteoarthritis: a systematic review and meta-analysis. Nutrients. (2024) 16:2640. doi: 10.3390/nu16162640
34. Ruff, KJ, Kopp, KJ, Von Behrens, P, Lux, M, Mahn, M, and Back, M. Effectiveness of NEM® brand eggshell membrane in the treatment of suboptimal joint function in dogs: a multicenter, randomized, double-blind, placebo-controlled study. Vet Med. (2016) 7:113–21. doi: 10.2147/VMRR.S101842
35. Gupta, RC, Lall, R, Srivastava, A, and Sinha, A. Hyaluronic Acid: Molecular Mechanisms and Therapeutic Trajectory. Front Vet Sci. (2019) 6:192. doi: 10.3389/fvets.2019.00192
36. Iturriaga, V, Vásquez, B, Bornhardt, T, and Del Sol, M. Effects of low and high molecular weight hyaluronic acid on the osteoarthritic temporomandibular joint in rabbit. Clin Oral Investig. (2021) 25:4507–18. doi: 10.1007/s00784-020-03763-x
37. Balogh, L, Polyak, A, Mathe, D, Kiraly, R, Thuroczy, J, Terez, M, et al. Absorption, uptake and tissue affinity of high-molecular-weight hyaluronan after oral administration in rats and dogs. J Agric Food Chem. (2008) 56:10582–93. doi: 10.1021/jf8017029
38. Oslan, SNH, Tan, JS, Oslan, SN, Matanjun, P, Mokhtar, RAM, Shapawi, R, et al. Haematococcus pluvialis as a potential source of astaxanthin with diverse applications in industrial sectors: current research and future directions. Molecules. (2021) 26:6470. doi: 10.3390/molecules26216470
39. Snell, TW, and Carberry, J. Astaxanthin Bioactivity Is Determined by Stereoisomer Composition and Extraction Method. Nutrients. (2022) 14:1522. doi: 10.3390/nu14071522
40. Park, JS, Kim, HW, Mathison, BD, Hayek, MG, Massimino, S, Reinhart, GA, et al. Astaxanthin uptake in domestic dogs and cats. Nutr Metab. (2010) 7:52. doi: 10.1186/1743-7075-7-52
41. Zahan, O-M, Serban, O, Gherman, C, and Fodor, D. The evaluation of oxidative stress in osteoarthritis. Med Pharm Rep. (2020) 93:12–22. doi: 10.15386/mpr-1422
42. Burri, L, and Johnsen, L. Krill products: an overview of animal studies. Nutrients. (2015) 7:3300–21. doi: 10.3390/nu7053300
43. Burri, L, Heggen, K, and Storsve, AB. Higher omega-3 index after dietary inclusion of omega-3 phospholipids versus omega-3 triglycerides in Alaskan Huskies. Vet World. (2020) 13:1167–73. doi: 10.14202/vetworld.2020.1167-1173
44. Lindqvist, H, Dominguez, T, Dragøy, R, Ding, Y, and Burri, L. Comparison of Fish, Krill and Flaxseed as Omega-3 Sources to Increase the Omega-3 Index in Dogs. Vet Sci China. (2023) 10:162. doi: 10.3390/vetsci10020162
45. Lee, M, Kim, D, Park, S-J, Yun, JM, Oh, DH, and Lee, J. Antarctic krill oil ameliorates monosodium iodoacetate-induced irregularities in articular cartilage and inflammatory response in the rat models of osteoarthritis. Nutrients. (2020) 12:3550. doi: 10.3390/nu12113550
46. Wang, K, Li, Y, Dai, Y, Han, L, Zhu, Y, Xue, C, et al. Peptides from Antarctic Krill (Euphausia superba) improve osteoarthritis via inhibiting HIF-2α-mediated death receptor apoptosis and metabolism regulation in osteoarthritic mice. J Agric Food Chem. (2019) 67:3125–33. doi: 10.1021/acs.jafc.8b05841
47. Suzuki, Y, Fukushima, M, Sakuraba, K, Sawaki, K, and Sekigawa, K. Krill oil improves mild knee joint pain: a randomized control trial. PLoS One. (2016) 11:e0162769. doi: 10.1371/journal.pone.0162769
48. Stonehouse, W, Benassi-Evans, B, Bednarz, J, Vincent, AD, Hall, S, and Hill, CL. Krill oil improved osteoarthritic knee pain in adults with mild to moderate knee osteoarthritis: a 6-month multicenter, randomized, double-blind, placebo-controlled trial. Am J Clin Nutr. (2022) 116:672–85. doi: 10.1093/ajcn/nqac125
49. Burri, L, Wyse, C, Gray, SR, Harris, WS, and Lazzerini, K. Effects of dietary supplementation with krill meal on serum pro-inflammatory markers after the Iditarod sled dog race. Res Vet Sci. (2018) 121:18–22. doi: 10.1016/j.rvsc.2018.10.002
50. Mercke Odeberg, J, Lignell, A, Pettersson, A, and Höglund, P. Oral bioavailability of the antioxidant astaxanthin in humans is enhanced by incorporation of lipid based formulations. Eur J Pharm Sci. (2003) 19:299–304. doi: 10.1016/S0928-0987(03)00135-0
51. Chitchumroonchokchai, C, and Failla, ML. Bioaccessibility and intestinal cell uptake of astaxanthin from salmon and commercial supplements. Food Res Int. (2017) 99:936–43. doi: 10.1016/j.foodres.2016.10.010
52. Huang, S-L, Ling, P-X, and Zhang, T-M. Oral absorption of hyaluronic acid and phospholipids complexes in rats. World J Gastroenterol. (2007) 13:945–9. doi: 10.3748/wjg.v13.i6.945
53. Park, DR, Ko, R, Kwon, SH, Min, B, Yun, SH, Kim, MH, et al. FlexPro MD, a mixture of krill oil, astaxanthin, and hyaluronic acid, suppresses lipopolysaccharide-induced inflammatory cytokine production through inhibition of NF-κB. J Med Food. (2016) 19:1196–203. doi: 10.1089/jmf.2016.3787
54. Park, MH, Jung, JC, Hill, S, Cartwright, E, Dohnalek, MH, Yu, M, et al. FlexPro MD®, a combination of krill oil, astaxanthin and hyaluronic acid, reduces pain behavior and inhibits inflammatory response in monosodium iodoacetate-induced osteoarthritis in rats. Nutrients. (2020) 12:956. doi: 10.3390/nu12040956
55. FlexPro MD®. (2016) Valensa. Available online at: https://valensa.com/vproducts/flex-pro-md/ (Accessed September 4, 2024)
56. Abdel-Tawab, M, Werz, O, and Schubert-Zsilavecz, M. Boswellia serrata: an overall assessment of in vitro, preclinical, pharmacokinetic and clinical data. Clin Pharmacokinet. (2011) 50:349–69. doi: 10.2165/11586800-000000000-00000
57. Almeida-da-Silva, CLC, Sivakumar, N, Asadi, H, Chang-Chien, A, Qoronfleh, MW, Ojcius, DM, et al. Effects of Frankincense Compounds on Infection, Inflammation, and Oral Health. Molecules. (2022) 27:4174. doi: 10.3390/molecules27134174
58. Reichling, J, Schmökel, H, Fitzi, J, Bucher, S, and Saller, R. Dietary support with Boswellia resin in canine inflammatory joint and spinal disease. Schweiz Arch Tierheilkd. (2004) 146:71–9. doi: 10.1024/0036-7281.146.2.71
59. Nicolas, CS, Jouty, N, Rème, CA, and Ereau, C. Movoflex® Soft chews can improve dogs’ mobility, according to owners. EC Vet Sci. (2022) 7:13–21. Available at: https://ecronicon.net/assets/ecve/pdf/ECVE-07-00528.pdf
60. Nicolas, CS, Schreiber, P, Rème, CA, Lopez, J, and Ereau, C. Adding krill oil and low molecular weight hyaluronic acid to Movoflex® soft chews helps improve dog’s mobility. Global J Med Res. (2022) 22:21–32. doi: 10.34257/GJMRGVOL22IS1PG21
61. Muller, C, Enomoto, M, Buono, A, Steiner, JM, and Lascelles, BDX. Placebo-controlled pilot study of the effects of an eggshell membrane-based supplement on mobility and serum biomarkers in dogs with osteoarthritis. Vet J. (2019) 253:105379. doi: 10.1016/j.tvjl.2019.105379
62. Cook, JL, Evans, R, Conzemius, MG, Lascelles, BDX, McIlwraith, CW, Pozzi, A, et al. Proposed definitions and criteria for reporting time frame, outcome, and complications for clinical orthopedic studies in veterinary medicine. Vet Surg. (2010) 39:905–8. doi: 10.1111/j.1532-950X.2010.00763.x
63. Shimada, M, Mizokami, N, Ichinohe, T, Kanno, N, Suzuki, S, Yogo, T, et al. Long-term outcome and progression of osteoarthritis in uncomplicated cases of cranial cruciate ligament rupture treated by tibial plateau leveling osteotomy in dogs. J Vet Med Sci. (2020) 82:908–16. doi: 10.1292/jvms.19-0613
64. Cachon, T, Frykman, O, Innes, JF, Lascelles, BDX, Okumura, M, Sousa, P, et al. Face validity of a proposed tool for staging canine osteoarthritis: Canine OsteoArthritis Staging Tool (COAST). Vet J. (2018) 235:1–8. doi: 10.1016/j.tvjl.2018.02.017
65. Alves, JC, Santos, A, Jorge, P, Lavrador, C, and Carreira, LM. Evaluation of Four Clinical Metrology Instruments for the Assessment of Osteoarthritis in Dogs. Animals. (2022) 12:2808. doi: 10.3390/ani12202808
66. Muller, C, Gaines, B, Gruen, M, Case, B, Arrufat, K, Innes, J, et al. Evaluation of clinical metrology instrument in dogs with osteoarthritis. J Vet Intern Med. (2016) 30:836–46. doi: 10.1111/jvim.13923
67. Varney, JL, Fowler, JW, and Coon, CN. Impact of supplemented undenatured type II collagen on pain and mobility in healthy Labrador Retrievers during an exercise regimen. Transl Anim Sci. (2022) 6:txac123. doi: 10.1093/tas/txac123
68. Matos Cruz, AM, and Mason, DR. Owner assessed outcomes following elbow arthroscopy with or without platelet rich plasma for fragmented medial coronoid process. Front Vet Sci. (2022) 9:938706. doi: 10.3389/fvets.2022.938706
69. Robertson-Plouch, C, Stille, JR, Liu, P, Smith, C, Brown, D, Warner, M, et al. A randomized clinical efficacy study targeting mPGES1 or EP4 in dogs with spontaneous osteoarthritis. Sci Transl Med. (2019) 11:eaaw9993. doi: 10.1126/scitranslmed.aaw9993
70. Lascelles, BDX, Knazovicky, D, Case, B, Freire, M, Innes, JF, Drew, AC, et al. A canine-specific anti-nerve growth factor antibody alleviates pain and improves mobility and function in dogs with degenerative joint disease-associated pain. BMC Vet Res. (2015) 11:101. doi: 10.1186/s12917-015-0413-x
71. Alves, JC, Santos, A, Jorge, P, Lavrador, C, and Carreira, LM. A report on the use of a single intra-articular administration of autologous platelet therapy in a naturally occurring canine osteoarthritis model – a preliminary study. BMC Musculoskelet Disord. (2020) 21:127. doi: 10.1186/s12891-020-3140-9
72. Carlisle, C, Metzger, BT, Tintle, NL, Polley, K, Jackson, KH, Le Brun-Blashka, S, et al. The effects of omega-3 supplementation on the omega-3 Index and quality of life and pain scores in dogs. Animals. (2024) 14:3108. doi: 10.3390/ani14213108
73. Mehler, SJ, May, LR, King, C, Harris, WS, and Shah, Z. A prospective, randomized, double blind, placebo-controlled evaluation of the effects of eicosapentaenoic acid and docosahexaenoic acid on the clinical signs and erythrocyte membrane polyunsaturated fatty acid concentrations in dogs with osteoarthritis. Prostaglandins Leukot Essent Fatty Acids. (2016) 109:1–7. doi: 10.1016/j.plefa.2016.03.015
74. Deutsch, L. Evaluation of the effect of Neptune Krill Oil on chronic inflammation and arthritic symptoms. J Am Coll Nutr. (2007) 26:39–48. doi: 10.1080/07315724.2007.10719584
75. Ierna, M, Kerr, A, Scales, H, Berge, K, and Griinari, M. Supplementation of diet with krill oil protects against experimental rheumatoid arthritis. BMC Musculoskelet Disord. (2010) 11:136. doi: 10.1186/1471-2474-11-136
76. Duo, L, Yang, J, Wang, X, Zhang, G, Zhao, J, Zou, H, et al. Krill oil: nutraceutical potential in skin health and disease. Front Nutr. (2024) 11:1388155. doi: 10.3389/fnut.2024.1388155
77. Conzemius, MG, and Evans, RB. Caregiver placebo effect for dogs with lameness from osteoarthritis. J Am Vet Med Assoc. (2012) 241:1314–9. doi: 10.2460/javma.241.10.1314
78. Brown, DC, Bell, M, and Rhodes, L. Power of treatment success definitions when the Canine Brief Pain Inventory is used to evaluate carprofen treatment for the control of pain and inflammation in dogs with osteoarthritis. Am J Vet Res. (2013) 74:1467–73. doi: 10.2460/ajvr.74.12.1467
Keywords: mobility issues, joint disorder, nutraceutical, canine osteoarthritis, Movoflex, pain, movement, mobility improvement
Citation: Ragetly GR, Martins Â, Ober CA, Boiocchi S and Nicolas CS (2025) Efficacy of a joint supplement containing eggshell membrane among other ingredients to improve the mobility of dogs with osteoarthritis: a multicenter double-blind randomized placebo-controlled study. Front. Vet. Sci. 12:1561793. doi: 10.3389/fvets.2025.1561793
Edited by:
Yun Qian, Shanghai Jiao Tong University, ChinaReviewed by:
Ingrida Monkeviciene, Lithuanian University of Health Sciences, LithuaniaFernando Cánovas, University of Algarve, Portugal
Copyright © 2025 Ragetly, Martins, Ober, Boiocchi and Nicolas. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Céline S. Nicolas, Y2VsaW5lLm5pY29sYXNAdmlyYmFjLmNvbQ==