 Jitender Sharma
Jitender Sharma Roopali Rajput
Roopali Rajput Manika Bhatia
Manika Bhatia Pooja Arora
Pooja Arora Vikas Sood
Vikas Sood- 1Department of Biochemistry, All India Institute of Medical Sciences, Bathinda, India
- 2Department of Biochemistry, School of Chemical and Life Sciences, Jamia Hamdard, New Delhi, India
- 3Department of Zoology, Hansraj College, University of Delhi, Delhi, India
The COVID-19 pandemic has caused huge socio-economic losses and continues to threat humans worldwide. With more than 4.5 million deaths and more than 221 million confirmed COVID-19 cases, the impact on physical, mental, social and economic resources is immeasurable. During any novel disease outbreak, one of the primary requirements for effective mitigation is the knowledge of clinical manifestations of the disease. However, in absence of any unique identifying characteristics, diagnosis/prognosis becomes difficult. It intensifies misperception and leads to delay in containment of disease spread. Numerous clinical research studies, systematic reviews and meta-analyses have generated considerable data on the same. However, identification of some of the distinct clinical signs and symptoms, disease progression biomarkers and the risk factors leading to adverse COVID-19 outcomes warrant in-depth understanding. In view of this, we assessed 20 systematic reviews and meta-analyses with an intent to understand some of the potential independent predictors/biomarkers/risk factors of COVID-19 severity and mortality.
Introduction
Coronaviruses belong to Coronaviridae family of viruses. The degree of disease caused by coronaviruses can vary from mild like common cold to severe like severe acute respiratory syndrome (SARS) and the middle east respiratory syndrome (MERS). These viruses have been successful in crossing inter-species barriers. SARS-coronavirus jumped from civet cats to humans while MERS-coronavirus got transmitted to humans from camels (Woo et al., 2012). The recent emergence of the novel SARS Coronavirus 2 (SARS-CoV-2) is another incidence of zoonotic transmission of coronaviruses. As per the genomic sequence analysis, the source of novel SARS-CoV-2 is speculated to be a previously identified bat coronavirus strain RaTG13 (96.2- 97.41% identity match) (Shi, 2021; Malaiyan et al., 2021) or pangolin-CoV (91.02- 92.22% genomic identity match) (Zhang T. et al., 2020; Malaiyan et al., 2021). However, the origin of the SARS-CoV-2 is still unclear due to the lack of definitive evidence. Further investigations are being undertaken in this regard (WHO News release, 2021).
Since the first case reported late in 2019, SARS-CoV-2 has taken more than 4.5 million human lives (as of September 08, 2021) and continues to spread worldwide with more than 221 million confirmed cases (WHO, 2021). The case fatality rate of the disease caused by the SARS-CoV-2 (3.26- 4.16% in Latin America; 5.8% in the United States) (Undurraga et al., 2021; Loomba et al., 2021) is way less as compared to the previous coronavirus outbreaks (Zhu et al., 2020). Nevertheless, the fatality caused by Coronavirus Disease 2019 (COVID-19) has surpassed that of the SARS and MERS combined (Song et al., 2019). The COVID-19 pandemic has also resulted in huge economic losses (speculated to be trillions of dollars) around the world (Emem, 2020).
COVID-19 initially emerged as novel pneumonia of unknown etiology with majorly non-specific symptoms and quite quickly engulfed the entire globe. During the initial months of the pandemic, lack of specific diagnostic modalities, the variable intensity of the disease surveillance, changing case definitions, asymptomatic period of infection and overwhelmed health care facilities largely contributed to the rapid spread of the virus, resulting in the global outbreak. Also, the novel COVID-19 in a way bridged the gap between the developing and developed world, bringing all on the same footing. With more than 85 million confirmed cases, the Americas are the worst affected, followed by Europe (> 66 million), South-East Asia (> 41 million), the East Mediterranean region (> 15 million), Western Pacific (> 7 million) and Africa (> 5 million) (WHO, 2021). A major breakthrough in the current pandemic period witnessed rapid development and administration of different vaccines against COVID-19. However, despite the massive vaccine roll-out programs, the emergence of virus variants sustains the challenge of controlling the pandemic and continues to spread in its wild-type and mutant forms across the globe.
Since the onset of the disease, several groups have published various systematic reviews and meta-analyses that aim to shed light on the disease prognosis. However, the evidence was limited and the data were mostly heterogenous. Further, due to ever-changing viral dynamics, multiple new symptoms have been witnessed. With the generation of more data, it is expected that the analysis will continue with a focus on identifying unique clinical manifestations, laboratory findings, radiological investigations, and therapy that could correlate with varying degree of COVID-19 or adverse outcomes, and fatality. However, the studies published earlier have highlighted the significance of some important biomarkers and clinical features in diagnosis, prognosis and management of mild to severe COVID-19.
Methodology
In the present work, we aim to identify key players of the disease and summarize important findings from already published studies on diverse clinical aspects of COVID-19. The search terms ‘COVID-19’, ‘SARS-CoV-2’, ‘clinical predictors’, ‘signs and symptoms’ were used individually or in appropriate combinations and only the ‘systematic reviews and/or meta-analysis’ articles that were published until February, 2021 were included for the present work. We carefully studied 20 systematic review/meta-analysis/meta-regression articles (Table 1A) that spanned the global population.
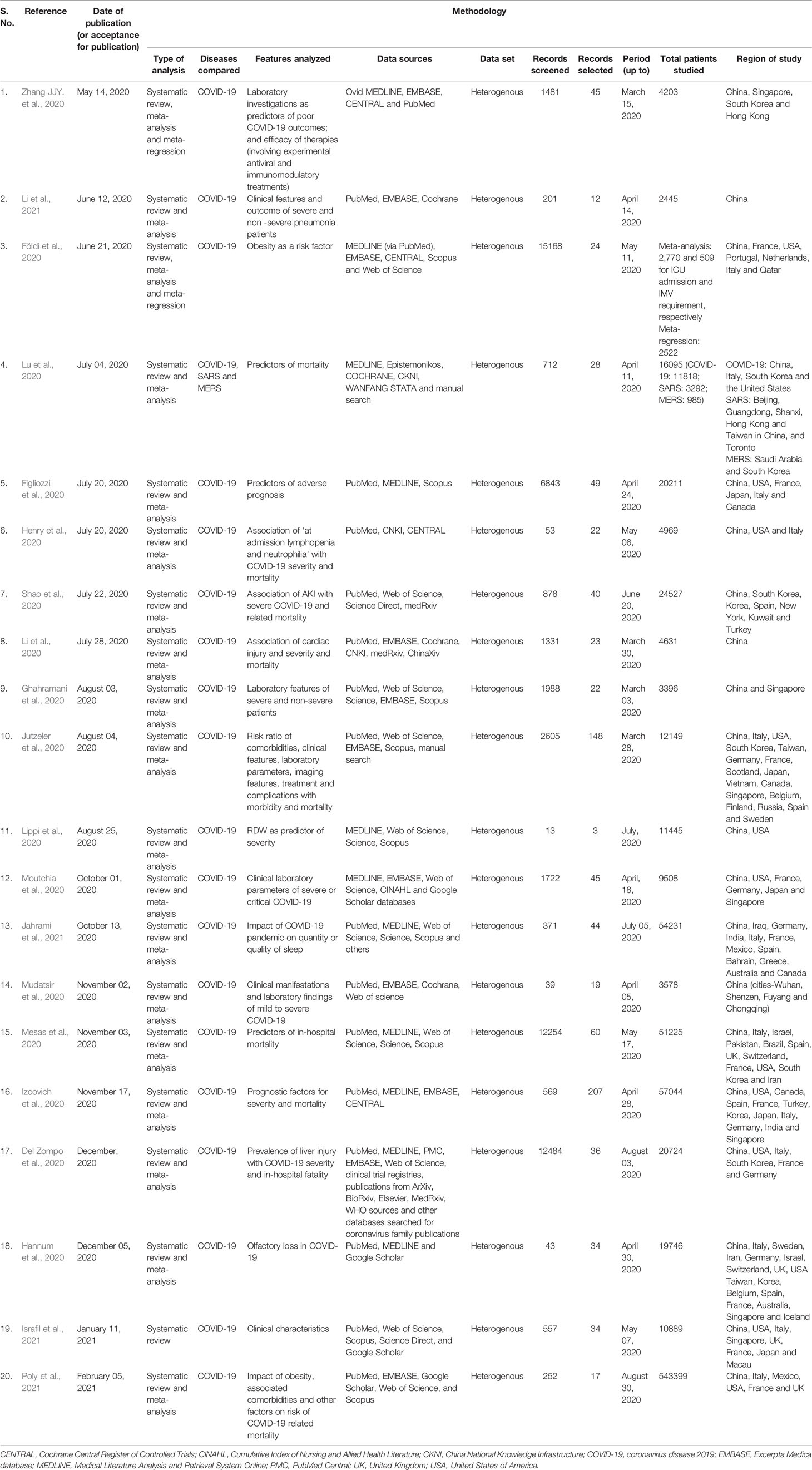
Table 1A Overview of the methodology of the analyzed systematic reviews and meta-analysis in relation to severity, adverse prognosis and mortality of COVID-19.
Prognostic Factors Associated with Severe COVID-19
Clinical Manifestations
Since the start of the pandemic, COVID-19 displayed a wide spectrum of clinical signs and symptoms, which included: fever, cough, sore throat, nasal congestion, sputum, headache, diarrhea, fatigue, dyspnea, chest tightness, myalgia, nausea, rhinorrhea, dizziness or confusion, hemoptysis, anorexia, vomiting, chest and abdominal pain (Huang et al., 2020; Jutzeler et al., 2020; Mudatsir et al., 2020). The eagerness to know any unique/distinct features was evident even in the layman. Fever, cough, fatigue, dyspnea (Figliozzi et al., 2020; Israfil et al., 2021) and a loss of sense of taste and smell (Hannum et al., 2020) remained some of the most experienced and identifying symptoms. In a systematic review involving more than 12000 patients, fever was the most common clinical manifestation in adults (78.5%), pregnant women (71.4%), pediatric and neonatal (53.1%) patients. Other important clinical signs and symptoms were cough (53.8%) and fatigue (25%) in adults, cough (41.4%) and myalgia (33.3%) in pregnant women and cough (47.9%) and sputum (27.5%) in children and neonates (Jutzeler et al., 2020). Only about 5% of patients were asymptomatic. Another meta-analysis, involving early data from 3578 patients, identified relation of dyspnea [odds ratio (OR)= 3.28, 95% confidence interval (CI) 2.09- 5.15], anorexia (OR= 1.83, 95% CI 1.00- 3.34), fatigue (OR= 2.00, 95% CI 1.25- 3.20) and dizziness (OR= 2.67, 95% CI 1.18- 6.01) with COVID-19 severity (Mudatsir et al., 2020). The vastly experienced COVID-19 symptoms, viz., fever, cough and breathing problem have been associated with problems in having sound sleep (Ferrando et al., 2016; Singh et al., 2020). An interesting systematic review and meta-analysis attempted to understand the impact of COVID-19 pandemic on quality or quantity of sleep under different study groups: COVID-19 patients, healthcare workers and the general population (Jahrami et al., 2021). As expected, about 75% of the COVID-19 patients had disturbed sleep, which was the highest prevalence among the different study groups (Jahrami et al., 2021). Physical pain or side-effects of the treatments were also speculated to impact the sound sleep in COVID-19 patients (Shi et al., 2020). These findings suggest that monitoring of sleep problems must not be ignored during COVID-19.
Comorbidities as Risk Factors for Adverse Outcomes of COVID-19
In one of the early meta-analyses aimed at assessing the impact of comorbidities on the course and clinical outcome of COVID-19, it was found that about 31% of adult patients (2329/7608) had comorbidities, with hypertension being the most prevalent condition (20.93%, 1352/6460), followed by heart failure (10.5%, 37/354), diabetes mellitus (10.4%, 678/6535) and coronary heart disease (8.5%, 194/2388) (Jutzeler et al., 2020). These pre-existing comorbidities were found to be linked with the severity of COVID-19 (relative risk, RR= 2.11, p= 0.046) (Jutzeler et al., 2020). Also, hypertension (RR= 2.15, p< 0.001), diabetes (RR= 2.56, p= 0.005), any heart condition (RR= 4.09, p< 0.001) and chronic obstructive pulmonary disease (COPD) (RR= 5.10, p< 0.001) were associated with adverse disease outcome. In addition, disease severity was more in male (RR= 1.11, p= 0.039) and old age patients (standardized mean difference, SMD= 0.68, p< 0.001) (Jutzeler et al., 2020). The meta-analysis revealed that older age (SMD= 1.25, 95% CI 0.78– 1.72, p< 0.001), male gender (RR= 1.32, 95% CI 1.13–1.54, p= 0.005) and pre-existing comorbidities (RR= 1.69, 95% CI 1.48– 1.94, p< 0.001) were associated with less survival. Furthermore, mechanical ventilation was also more frequently required for treatment of non-survivors as compared to survivors (RR= 6.05, 95% CI 1.41– 26.05, p= 0.026); with more common administration of extracorporeal membrane oxygenation (RR= 4.39, 95% CI 1.64– 11.78, p= 0.014) in the non-survivors (Jutzeler et al., 2020). The risk of developing complications during the course of COVID-19 was higher in the non-survivors as compared to the survivors. The complications included, in particular, acute kidney injury (AKI) (RR= 20.77, 95% CI 2.43– 177.44, p= 0.017) and acute respiratory distress syndrome (ARDS) (RR= 4.24, 95% CI 1.30–13.83, p= 0.026) (Jutzeler et al., 2020).
Liver injury has been reported as another comorbidity being associated with the severity and in-hospital fatality of COVID-19 patients. In a meta-analysis of 20724 COVID-19 confirmed cases from 36 articles, pre-existing liver disease was present in up to 37.6% of cases (Del Zompo et al., 2020) at the time of hospital admission. The etiology of abnormal liver function was mentioned in only a few of the studies analyzed in the said meta-analysis. The authors recommended frequent testing of liver function test (LFT) markers as an additional tool for early stratification and monitoring of COVID-19 patients (Del Zompo et al., 2020). Further prospective cohort investigations are need-of-the-hour to validate the significance of LFT biochemistries in the management of COVID-19. Likewise, about 4.5% of COVID-19 patients displayed pre-known viral hepatitis in a study conducted by a different research group (Gu et al., 2020).
Another noteworthy comorbidity is AKI. In view of this, a systematic review and meta-analysis was conducted involving 24527 COVID-19 patients, where the overall rate of severe COVID-19 and COVID-19 related fatality was 26.4% and 20.3%, respectively (Shao et al., 2020). The robust meta-analysis revealed significant association of AKI with severity (OR= 8.11, 95% CI 5.01- 13.13, p< 0.00001) and fatality (OR= 14.63, 95% CI 9.94- 21.51, p< 0.00001) in COVID-19 patients. Prevalence of severe COVID-19 and fatality due to COVID-19 was considerably high (55.6% and 63.1% respectively, p< 0.01) in patients with AKI as compared to those without AKI (17.7% and 12.9% respectively) (Shao et al., 2020). Cardiac impairment was a significant factor associated with severe COVID-19 outcomes (OR= 3.15, 95% CI 2.26- 4.41) and fatality (OR= 1.95, 95% CI 1.08- 3.54) (Figliozzi et al., 2020; Li et al., 2020). Smoking (OR= 2.24, 95% CI 1.40- 3.58), history of diabetes mellitus (OR= 2.34, 95% CI 1.64- 3.33), COPD (OR= 2.63, 95% CI 1.55- 4.44) or hypertension (OR= 2.25, 95% CI 1.80- 2.82) contributed to progression to adverse COVID-19 (Figliozzi et al., 2020). Diabetes mellitus (OR= 1.74, 95% CI 1.22- 2.48), cardiovascular disease (OR= 1.95, 95% CI 1.08- 3.54), COPD (OR= 2.98, 95% CI 1.38-6.44), or cerebrovascular disease (OR= 2.93, 95% CI 1.84- 4.26) indicated high mortality risk (Figliozzi et al., 2020).
Apart from the above-mentioned somewhat obvious comorbidities, obesity emerged as another major condition that would worsen the outcomes in COVID-19 patients (Földi et al., 2020; Poly et al., 2021). A meta-analysis involving 2770 patients revealed that obesity was a significant risk factor associated with admission to critical care units (OR= 1.21, 95% CI 1.002- 1.46) (Földi et al., 2020). Also, the requirement of invasive mechanical ventilation (IMV) was more (up to 78%) for obese patients as analyzed in 509 subjects. A body-mass-index (BMI) of ≥ 25 was a significant risk factor for IMV requirement (OR= 2.63, 95% CI 1.64- 4.22) (Földi et al., 2020). Like obesity, psychiatric comorbidities (like anxiety and depression) must also be considered during COVID-19 management. Potential bi-directional associations between psychiatric comorbidities and sleep have been reported (Jahrami et al., 2021), amounting to sleep problems during COVID-19. This may impact the recovery from the disease.
Biochemical Biomarkers as Independent Predictors of Severity, Adverse Prognosis or Mortality of COVID-19
Recent evidence highlighted the relevance of various biochemical tests as independent or combined correlates for the determination of severity, poor prognosis or mortality related to COVID-19. Clinical laboratory tests encompassing biochemical, hematological, inflammatory and coagulation parameters were considered useful to recognize severe or critical COVID-19. Additionally, these parameters also provided valuable clinical information for effective monitoring of the clinical course of COVID-19. As per findings of a large meta-analysis of 45 studies across 6 countries, neutrophilia (meta-median difference, MMD= 1.23 x 109 cells/µl) and lymphopenia (MMD= -0.39 x 109 cells/µl) were associated with critical COVID-19 (Moutchia et al., 2020). Similar findings were also reported in another meta-analysis comprising 4969 patients (Henry et al., 2020). In this meta-analysis, reduced lymphocyte count and increased neutrophil count at the time of admission were significantly associated with progression to severe disease (OR= 4.20, 95% CI 3.46- 5.09 and OR= 7.99, 95% CI 1.77- 36.14, respectively), and mortality (OR= 3.71, 95% CI, 1.63- 8.44 and OR= 7.87, 95% CI 1.75- 35.35, respectively) (Henry et al., 2020). Inflammatory markers, namely, C-reactive protein (CRP), Interleukin 6 (IL-6), and erythrocyte sedimentation rate (ESR) (MMD= 36.97 mg/l, 17.37 pg/ml, 21.93 mm/hr, respectively) were raised in severe COVID-19 cases (Moutchia et al., 2020). Biochemical indices like alanine aminotransferase (ALT), aspartate aminotransferase (AST), blood urea nitrogen (BUN), creatinine (MMD= 6.89 u/l, 11.96 u/l, 1.04 mmol/l, 4.87 µmol/l) were significantly elevated in severe or critical cases in comparison to non-severe COVID-19 patients (Moutchia et al., 2020). A meta-regression analysis observed that higher leukocyte counts (p< 0.0001), elevated levels of ALT (p= 0.024), AST (p= 0.0040), lactate dehydrogenase (LDH) (p< 0.0001) and raised procalcitonin (PCT) (p< 0.0001) were note-worthy predictors of admission to intensive care unit (Zhang JJY. et al., 2020). Further, the researchers found that elevated LDH (p< 0.0001) and high leukocyte counts (p= 0.0005) were significantly associated with COVID-19 led mortality. Other laboratory parameters that were found to be significantly associated with critical disease were myocardial biomarkers, Troponin I (MMD= 0.01 ng/ml), and creatine kinase-MB (CK-MB) (MMD= 1.46 u/l), tissue damage marker, LDH (MMD= 124.26 u/l), platelet count (MMD= -21.48 x 109 cells/l) and D-dimer (MMD= 0.65 mg/ml) (Moutchia et al., 2020). These laboratory parameters indicated that innate immune response gets activated during COVID-19 as indicated by markedly raised neutrophil to lymphocyte ratio (NLR) and CRP. In contrast, adaptive immune response is unable to limit virus replication during severe COVID-19, as evidenced by reduced levels of lymphocytes and its subsets. Thus, routine testing for NLR, CRP, ESR, Troponin-I, BUN, creatinine, AST, ALT, CK-MB, LDH and D-dimer in severe COVID-19 is beneficial in monitoring clinical progression and can predict outcome of the disease. Anisocytosis, a condition that is characterized by heterogeneity in volumes of circulating red blood cells (RBCs), has also been linked to severe COVID-19. This low-cost parameter is expressed as RBC distribution width (RDW) and may be calculated as either RDW- standard deviation (SD) or coefficient of variation (CV). In this view, an analysis of RDW in 11445 COVID-19 patients was conducted and a 0.69% increase (95% CI 0.40- 0.98, p< 0.001) in absolute RDW-CV value of severe COVID-19 patients was found in comparison to mildly ill COVID-19 patients (Lippi et al., 2020). Hence, estimation of RDW may assist in risk stratification of adverse COVID-19 progression (Lippi et al., 2020).
Laboratory results were useful in differentiating severe from non-severe COVID-19 patients at the time of admission to the intensive care unit, as per the systematic review and meta−analysis conducted by Ghahramani et al. (Ghahramani et al., 2020). Results of routine tests like LFT, kidney function tests (KFT), glucose, albumin, electrolytes and complete blood count (CBC) were significantly altered in severe or critical COVID-19 patients belonging to the Asian population. In the same systematic review and meta-analysis, elevated PCT levels and higher neutrophil count were associated with bacterial co-infection in severe COVID-19 patients. Further, sensitivity analysis revealed significant differences in pooled effect size (p-ES) for NLR, lymphocyte to CRP ratio (LCR), PCT, AST, ALT, sodium, glucose, BUN, creatinine, ESR, myoglobin and D-dimer (Ghahramani et al., 2020). Laboratory parameters like decreased platelet count (p-ES= -1.7), low hemoglobin concentration (p-ES= -0.6), low albumin (p-ES= -3.1), raised IL-6 (p-ES = 2.4), elevated creatinine (p-ES = 2.4) and higher troponin-I (p-ES = 0.7) were markedly associated with in-hospital mortality (Mesas et al., 2020). As per another meta-analysis, low albumin levels (SMD= -1.13, 95% CI -1.41– -0.85, p< 0.001) and lymphocyte counts (SMD= -0.92, 95% CI -1.3– -0.55, p< 0.001) as well as high IL-6 levels (SMD= 1.21, 95% CI 0.93– 1.5, p< 0.001), leucocyte counts (SMD= 2.21, 95% CI 0.61– 3.64, p= 0.06), and prolonged prothrombin time (SMD= 7.99, 95% CI 4.64– 11.34, p< 0.01) were found to be linked with COVID-19 related mortality (Jutzeler et al., 2020). Hence, abnormal indices of the above-mentioned parameters could be prognostic markers of adverse COVID-19 outcomes.
In another large-scale analysis, including more than 57000 COVID-19 patients, 49 parameters were identified as high/moderate predictors of poor prognosis (Izcovich et al., 2020). The variable parameters included demographic factors: increasing age, male gender and smoking; comorbidities: diabetes, cerebrovascular disease, COPD, cardiovascular disease, cardiac arrhythmia, arterial hypertension, chronic kidney disease, cancer, dementia and dyslipidemia; physical examination factors: respiratory failure, fever, myalgia or arthralgia, fatigue, abdominal pain, tachycardia, hypoxemia, dyspnea, anorexia, tachypnoea, low blood pressure, hemoptysis; laboratory assessments: elevated PCT, myocardial injury markers, increased WBC counts, elevated blood lactate, reduced lymphocyte count, reduced platelet count, increased neutrophil count, raised plasma creatinine, elevated D-dimer, raised LDH, elevated CRP, raised AST levels, decreased albumin, elevated IL-6 levels, raised B-type natriuretic peptide (BNP), elevated BUN, raised ESR, elevated CK and raised bilirubin; radiological factors: pleural effusion and consolidative infiltrate; and high sequential organ failure assessment (SOFA) score (Tables 1B, 2) (Izcovich et al., 2020).

Table 1B Summary of the major outcomes of the analyzed systematic reviews and meta-analyses.
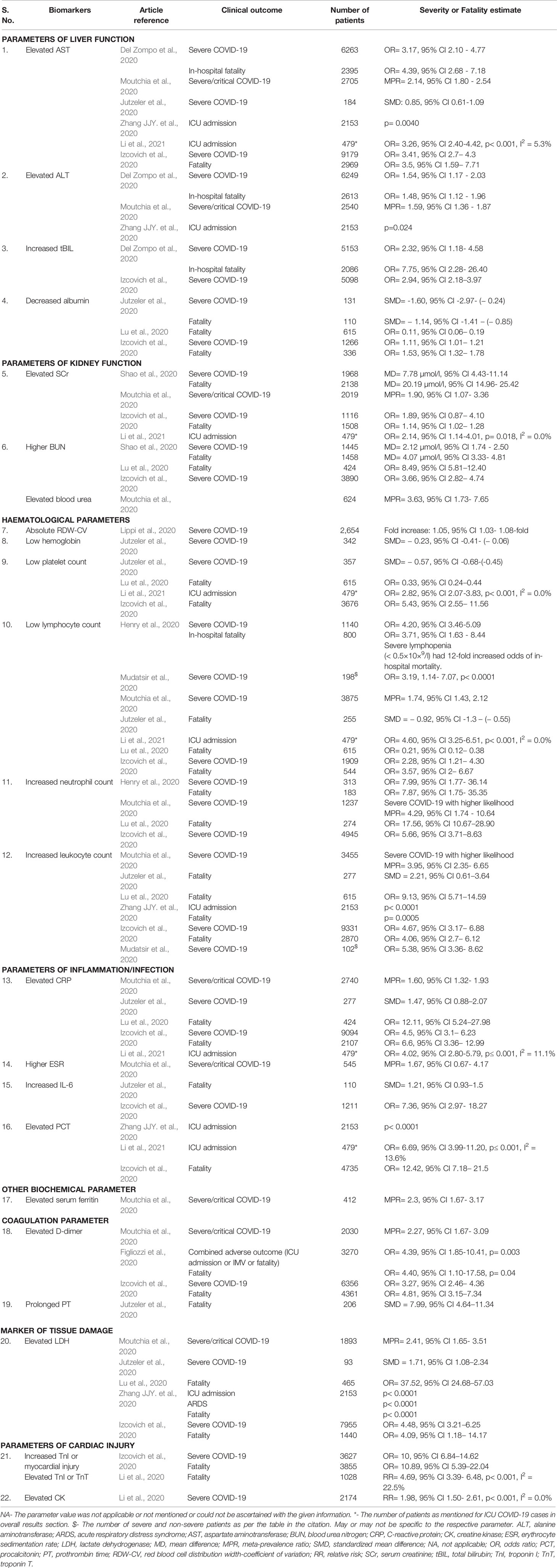
Table 2 Putative independent predictors of COVID-19 adverse prognosis, severity or mortality.
A systematic review and meta-analysis of 36 studies involving more than 20000 patients demonstrated important findings (Del Zompo et al., 2020). With an intent to correlate liver injury with clinical outcomes in COVID-19 patients, the researchers found that nearly 47% of COVID-19 cases had abnormal LFT. They also found that the laboratory tested AST, ALT and total bilirubin were independent predictors of COVID-19 severity and in-hospital mortality (Table 2) (Del Zompo et al., 2020). However, there was insufficient information on the etiology of pre-existing liver injury in COVID-19 patients at the time of hospitalization. Hence, further prospective cohort studies would be essential to validate these findings.
Other noteworthy biochemical findings are elevated levels of BUN and serum creatinine (SCr) (Shao et al., 2020). A robust meta-analysis recorded significant (p< 0.00001) rise in levels of BUN and SCr in severe COVID-19 cases and non-survivors (Table 1B) (Shao et al., 2020). Increased SCr and BUN values were identified as independent biomarkers for COVID-19 related severity and in-hospital mortality early during the pandemic (Chen et al., 2020; Cheng et al., 2020). However, the rate of severe and fatal cases in the study by Shao et al. was quite high, which could be due to the fact that the studies analyzed represented majorly poor COVID-19 outcomes (Shao et al., 2020). Hence, over-estimation of severity and fatality rate may be a limitation to this otherwise crucial set of findings.
Radiological Investigations
Identification of viral pathogens is possible by careful examination of imaging patterns since the latter are associated with viral pathogenesis. Since, viruses belonging to a single viral family share a similar pathogenesis, computed tomography (CT) was considered a trusted technique to distinguish patterns and features of COVID-19 in immunocompetent patients (Chung et al., 2020; Jin et al., 2020; Tao et al., 2020). The systematic review and meta-analysis conducted by Jutzeler et al. identified abnormal CT scans in nearly 90% (89.6% specifically) of the COVID-19 confirmed adult patients, 88.6% of the pregnant patients and 65% of the pediatric and neonatal patients (Jutzeler et al., 2020). The major finding in CT imaging was the occurrence of unilateral or bilateral pneumonia in 83.6% (6620/7917) adult patients, 88.6% (31/35) pregnant and 65% (194/298) pediatric and neonatal COVID-19 cases (Jutzeler et al., 2020). Other prominent abnormal CT features included air bronchogram (50.5%, 264/523) and ground-glass opacity (GGO) with consolidation (47.4%, 153/323) and without (43.8%, 2446/5591) in adult patients, GGO (85.3%, 29/34) and consolidation (50%, 8/16) in pregnant patients, and GGO (38.9%, 108/278) and local patchy shadowing (23.3%, 52/223) in pediatric and neonatal patients (Jutzeler et al., 2020).
Conclusions
Identification of high-risk clinical and laboratory features contribute to early prediction, diagnosis and efficient treatment of patients (Li et al., 2021). A fatality rate of 7.7% with about 8% of the COVID-19 patients being asymptomatic was observed during the early pandemic period (Jutzeler et al., 2020). Since, it is difficult to record the exact number of asymptomatic cases, owing to obvious reasons (like no hospital/clinic visit, hence no medical record; or lack of awareness that a potentially fatal disease can be asymptomatic in some patients) such value is deemed to be 6- to 10- fold higher (Jutzeler et al., 2020). Hence, more aggressive antigen detection, as well as serological surveillance of contacts of confirmed COVID-19 patients, is necessary to enable screening and identification of asymptomatic COVID-19 patients. Further, prospective well-planned cohort studies would be necessary to enable further characterization of the overall, gender-specific and/or geographical location-based risk factors.
It is imperative to categorize COVID-19 patients based on their comorbidities, like impaired kidney or liver functions or cardiac injury, etc. As discussed in the present work, AKI is a critical complication of COVID-19 and calls for immediate care and monitoring (Shao et al., 2020) to minimize the risk of severity and poor prognosis. Similarly, abnormal LFTs are important early predictors of COVID-19 severity and in-hospital mortality (Del Zompo et al., 2020). Also, pre-existing chronic liver disease, especially cirrhosis, is an indicator of a high risk of mortality. Hence, aggressive interventions for such cases must be exercised. This would enable better patient management and may improve the disease outcome. Measurement of anthropometric parameters, especially BMI, is also recommended for COVID-19 patient management, importantly for patients who are or above 65 years of age (Földi et al., 2020; Poly et al., 2021). Basic hematological screening that can be done with minimal resources can be a life-saver. The findings that lymphopenia and neutrophilia at the time of hospital admission indicate poor COVID-19 outcome call for routine hematological monitoring. It would enable an early careful intervention in such patients enabling better patient care. Such regular monitoring may also aid in the stratification and the management of risk associated with COVID-19 (Henry et al., 2020). Further, it is also important to stratify epidemiological data based on demographic characteristics and risk factors for adverse COVID-19 outcomes, to enable exact and aggressive patient care (Mesas et al., 2020). Based on the analysis in this work, we can conclude that careful monitoring of clinical data, risk factors and disease biomarkers (Israfil et al., 2021) may enable early determination of COVID-19-led severity. Such an early estimate would be helpful in efficient patient management and possibly minimize the related mortality.
Author Contributions
JS conceptualized the study, retrieved the articles, analyzed the data and guided inclusion of specific information, drafted and proof-read the manuscript. RR reviewed the data, analyzed the information, tabulated findings, drafted and proof-read the manuscript. MB helped in information retrieval and inclusion of findings. PA provided intellectual inputs and proof-read the manuscript. VS conceived the study, provided intellectual inputs, guided the inclusion of information, proof-read and approved the final version of the manuscript. All authors contributed to the article and approved the submitted version.
Funding
JS received institutional support from AIIMS, Bathinda, Punjab, India. RR is presently an independent research fellow (Research Associate) of the Council of Scientific and Industrial Research (CSIR), Government of India. VS received financial support (Faculty Recharge Programme) from the University Grants Commission (UGC), Govt. of India.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Coronavirus Could Cost the Global Economy Trillions on a Sars Baseline. Available at: https://www.ccn.com/coronavirus-could-cost-the-global-economy-trillions-on-a-sars-baseline/.
Cheng, Y., Luo, R., Wang, K., Zhang, M., Wang, Z., Dong, L., et al. (2020). Kidney Disease Is Associated With in-Hospital Death of Patients With COVID-19. Kidney Int. 97 (5), 829–838. doi: 10.1016/j.kint.2020.03.005
Chen, N., Zhou, M., Dong, X., Qu, J., Gong, F., Han, Y., et al. (2020). Epidemiological and Clinical Characteristics of 99 Cases of 2019 Novel Coronavirus Pneumonia in Wuhan, China: A Descriptive Study. Lancet 395 (10223), 507–513. doi: 10.1016/s0140-6736(20)30211-30217
Chung, M., Bernheim, A., Mei, X., Zhang, N., Huang, M., Zeng, X., et al. (2020). CT Imaging Features of 2019 Novel Coronavirus, (2019-Ncov). Radiology 295 (1), 202–207. doi: 10.1148/radiol.2020200230
Del Zompo, F., De Siena, M., Ianiro, G., Gasbarrini, A., Pompili, M., Ponziani, F. R. (2020). Prevalence of Liver Injury and Correlation With Clinical Outcomes in Patients With COVID-19: Systematic Review With Meta-Analysis. Eur. Rev. Med. Pharmacol. Sci. 24 (24), 13072–13088. doi: 10.26355/eurrev_202012_24215
Emem, M. (2020) Multi-Billion Dollar Coronavirus Vaccine Deal Could Save the Economy. CCN Headlines Opinion. Available at: https://www.ccn.com/coronavirus-could-cost-the-global-economy-trillions-on-a-sars-baseline/.
Ferrando, M., Bagnasco, D., Roustan, V., Canonica, G. W., Braido, F., Baiardini, I. (2016). Sleep Complaints and Sleep Breathing Disorders in Upper and Lower Obstructive Lung Diseases. J. Thorac. Dis. 8 (8), E716–E725. doi: 10.21037/jtd.2016.07.82
Figliozzi, S., Masci, P. G., Ahmadi, N., Tondi, L., Koutli, E., Aimo, A., et al. (2020). Predictors of Adverse Prognosis in COVID-19: A Systematic Review and Meta-Analysis. Eur. J. Clin. Invest. 50 (10), e13362. doi: 10.1111/eci.13362
Földi, M., Farkas, N., Kiss, S., Zádori, N., Váncsa, S., Szakó, L., et al. (2020). Obesity Is a Risk Factor for Developing Critical Condition in COVID-19 Patients: A Systematic Review and Meta-Analysis. Obes. Rev. 21 (10), e13095. doi: 10.1111/obr.13095
Ghahramani, S., Tabrizi, R., Lankarani, K. B., Kashani, S. M. A., Rezaei, S., Zeidi, N., et al. (2020). Laboratory Features of Severe vs. non-Severe COVID-19 Patients in Asian Populations: A Systematic Review and Meta-Analysis. Eur. J. Med. Res. 25 (1), 30. doi: 10.1186/s40001-020-00432-3
Gu, X., Li, X., An, X., Yang, S., Wu, S., Yang, X., et al. (2020). Elevated Serum Aspartate Aminotransferase Level Identifies Patients With Coronavirus Disease 2019 and Predicts the Length of Hospital Stay. J. Clin. Lab. Anal. 34, e23391. doi: 10.1002/jcla.23391
Hannum, M. E., Ramirez, V. A., Lipson, S. J., Herriman, R. D., Toskala, A. K., Lin, C., et al. (2020). Objective Sensory Testing Methods Reveal a Higher Prevalence of Olfactory Loss in COVID-19 Positive Patients Compared to Subjective Methods: A Systematic Review and Meta-Analysis. Chem. Senses. 45 (9), 865–874. doi: 10.1093/chemse/bjaa064
Henry, B., Cheruiyot, I., Vikse, J., Mutua, V., Kipkorir, V., Benoit, J., et al. (2020). Lymphopenia and Neutrophilia at Admission Predicts Severity and Mortality in Patients With COVID-19: A Meta-Analysis. Acta BioMed. 91 (3), e2020008. doi: 10.23750/abm.v91i3.10217
Huang, C., Wang, Y., Li, X., Ren, L., Zhao, J., Hu, Y., et al. (2020). Clinical Features of Patients Infected With 2019 Novel Coronavirus in Wuhan, China. Lancet 395, 497–506. doi: 10.1016/S0140-6736(20)30183-5
Israfil, S. M. H., Sarker, M. M. R., Rashid, P. T., Talukder, A. A., Kawsar, K. A., Khan, F., et al. (2021). Clinical Characteristics and Diagnostic Challenges of COVID-19: An Update From the Global Perspective. Front. Public Health 8, 567395. doi: 10.3389/fpubh.2020.567395
Izcovich, A., Ragusa, M. A., Tortosa, F., Lavena Marzio, M. A., Agnoletti, C., Bengolea, A., et al. (2020). Prognostic Factors for Severity and Mortality in Patients Infected With COVID-19: A Systematic Review. PloS One 15 (11), e0241955. doi: 10.1371/journal.pone.0241955
Jahrami, H., BaHammam, A. S., Bragazzi, N. L., Saif, Z., Faris, M., Vitiello, M. V. (2021). Sleep Problems During the COVID-19 Pandemic by Population: A Systematic Review and Meta-Analysis. J. Clin. Sleep Med. 17 (2), 299–313. doi: 10.5664/jcsm.8930
Jin, Y.-H., Cai, L., Cheng, Z.-S., Cheng, H., Deng, T., Fan, Y.-P., et al. (2020). A Rapid Advice Guideline for the Diagnosis and Treatment of 2019 Novel Coronaviru-Ncov) Infected Pneumonia (Standard Version). Mil. Med. Res. 7 (1), 4. doi: 10.1186/s40779-020-0233-6
Jutzeler, C. R., Bourguignon, L., Weis, C. V., Tong, B., Wong, C., Rieck, B., et al. (2020). Comorbidities, Clinical Signs and Symptoms, Laboratory Findings, Imaging Features, Treatment Strategies, and Outcomes in Adult and Pediatric Patients With COVID-19: A Systematic Review and Meta-Analysis. Travel Med. Infect. Dis. 37, 101825. doi: 10.1016/j.tmaid.2020.101825
Li, J., He, X., Yuan, Y., Zhang, W., Li, X., Zhang, Y., et al. (2021). Meta-Analysis Investigating the Relationship Between Clinical Features, Outcomes, and Severity of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-Cov-2) Pneumonia. Am. J. Infect. Control 49 (1), 82–89. doi: 10.1016/j.ajic.2020.06.008
Li, X., Pan, X., Li, Y., An, N., Xing, Y., Yang, F., et al. (2020). Cardiac Injury Associated With Severe Disease or ICU Admission and Death in Hospitalized Patients With COVID-19: A Meta-Analysis and Systematic Review. Crit. Care 24, 468. doi: 10.1186/s13054-020-03183-z
Lippi, G., Henry, B. M., Sanchis-Gomar, F. (2020). Red Blood Cell Distribution Is a Significant Predictor of Severe Illness in Coronavirus Disease 2019. Acta Haematol. 25, 1–5. doi: 10.1159/000510914
Loomba, R. S., Aggarwal, G., Aggarwal, S., Flores, S., Villarreal, E. G., Farias, J. S., et al. (2021). Disparities in Case Frequency and Mortality of Coronavirus Disease 2019 (COVID-19) Among Various States in the United States. Ann. Med. 53 (1), 151–159. doi: 10.1080/07853890.2020.1840620
Lu, L., Zhong, W., Bian, Z., Li, Z., Zhang, K., Liang, B., et al. (2020). A Comparison of Mortality-Related Risk Factors of COVID-19, SARS, and MERS: A Systematic Review and Meta-Analysis. J. Infect. 81 (4), e18–e25. doi: 10.1016/j.jinf.2020.07.002
Malaiyan, J., Arumugam, S., Mohan, K., Radhakrishnan, G. (2021). An Update on the Origin of SARS-Cov-2: Despite Closest Identity, Bat (Ratg13) and Pangolin Derived Coronaviruses Varied in the Critical Binding Site and O-Linked Glycan Residues. J. Med. Virol. 93 (1), 499–505. doi: 10.1002/jmv.26261
Mesas, A. E., Cavero-Redondo, I., Álvarez-Bueno, C., Sarriá Cabrera, M. A., Maffei de Andrade, S., Sequí-Dominguez, I., et al. (2020). Predictors of in-Hospital COVID-19 Mortality: A Comprehensive Systematic Review and Meta-Analysis Exploring Differences by Age, Sex and Health Conditions. PloS One 15 (11), e0241742. doi: 10.1371/journal.pone.0241742
Moutchia, J., Pokharel, P., Kerri, A., McGaw, K., Uchai, S., Nji, M., et al. (2020). Clinical Laboratory Parameters Associated With Severe or Critical Novel Coronavirus Disease 2019 (COVID-19): A Systematic Review and Meta-Analysis. PloS One 15 (10), e0239802. doi: 10.1371/journal.pone.0239802
Mudatsir, M., Fajar, J. K., Wulandari, L., Soegiarto, G., Ilmawan, M., Purnamasari, Y., et al. (2020). Predictors of COVID-19 Severity: A Systematic Review and Meta-Analysis. F1000Res 9, 1107. doi: 10.12688/f1000research.26186.2
Poly, T. N., Islam, M. M., Yang, H. C., Lin, M. C., Jian, W. S., Hsu, M. H., et al. (2021). Obesity and Mortality Among Patients Diagnosed With COVID-19: A Systematic Review and Meta-Analysis. Front. Med. 8, 620044. doi: 10.3389/fmed.2021.620044
Shao, M., Li, X., Liu, F., Tian, T., Luo, J., Yang, Y. (2020). Acute Kidney Injury Is Associated With Severe Infection and Fatality in Patients With COVID-19: A Systematic Review and Meta-Analysis of 40 Studies and 24,527 Patients. Pharmacol. Res. 161, 105107. doi: 10.1016/j.phrs.2020.105107
Shi, Z. L. (2021). Origins of SARS-Cov-2: Focusing on Science. Infect. Dis. Immun. 1 (1), 3–4. doi: 10.1097/ID9.0000000000000008
Shi, L., Lu, Z.-A., Que, J.-Y., Huang, X.-L., Lu, L., Ran, M.-S., et al. (2020). Prevalence of and Risk Factors Associated With Mental Health Symptoms Among the General Population in China During the Coronavirus Disease 2019 Pandemic. JAMA Netw. Open 3 (7), e2014053. doi: 10.1001/jamanetworkopen.2020.14053
Singh, D. P., Jamil, R. T., Mahajan, K. (2020). “Nocturnal Cough,” in Statpearls. Eds. Cascella, M., Rajnik, M., Cuomo, A., Dulebohn, S. C., Di Napoli, R. S. (Treasure Island, FL: StatPearls Publishing).
Song, Z., Xu, Y., Bao, L., Zhang, L., Yu, P., Qu, Y., et al. (2019). From SARS to MERS, Thrusting Coronaviruses Into the Spotlight. Viruses 11 (1), 59. doi: 10.3390/v11010059
Tao, A., Zhenlu, Y., Hongyan, H., Chenao, Z., Chong, C., Wenzhi, L., et al. (2020). Correlation of Chest CT and RT-PCR Testing in Coronavirus Disease 2019 (COVID-19) in China: A Report of 1014 Cases. Radiology 296 (2), E32–E40. doi: 10.1148/radiol.2020200642
Undurraga, E. A., Chowell, G., Mizumoto, K. (2021). COVID-19 Case Fatality Risk by Age and Gender in a High Testing Setting in Latin America: Chile, March–August 2020. Infect. Dis. Poverty 10, 11. doi: 10.1186/s40249-020-00785-1
WHO (2021) WHO Coronavirus Disease (COVID-19) Dashboard. Updated on: 27 February 2021. Available at: https://covid19.who.int/ (Accessed on: July 15, 2021).
WHO News release (2021) WHO Calls for Further Studies, Data on Origin of SARS-Cov-2 Virus, Reiterates That All Hypotheses Remain Open. Available at: https://www.who.int/news/item/30-03-2021-who-calls-for-further-studies-data-on-origin-of-sars-cov-2-virus-reiterates-that-all-hypotheses-remain-open.
Woo, P. C., Lau, S. K., Lam, C. S., Lau, C. C. Y., Tsang, A. K. L., Lau, J. H. N., et al. (2012). Discovery of Seven Novel Mammalian and Avian Coronaviruses in the Genus Deltacoronavirus Supports Bat Coronaviruses as the Gene Source of Alphacoronavirus and Betacoronavirus and Avian Coronaviruses as the Gene Source of Gammacoronavirus and Deltacoronavirus. J. Virol. 86, 3995–4008. doi: 10.1128/JVI.06540-11
Zhang, J. J. Y., Lee, K. S., Ang, L. W., Leo, Y. S., Young, B. E. (2020). Risk Factors for Severe Disease and Efficacy of Treatment in Patients Infected With COVID-19: A Systematic Review, Meta-Analysis, and Meta-Regression Analysis. Clin. Infect. Dis. 71 (16), 2199–2206. doi: 10.1093/cid/ciaa576
Zhang, T., Wu, Q., Zhang, Z. (2020). Probable Pangolin Origin of SARS-Cov-2 Associated With the COVID-19 Outbreak. Curr. Biol. 30 (8), 1578. doi: 10.1016/j.cub.2020.03.063
Keywords: SARS-CoV-2, prognosis, biomarkers, risk factors, obesity, diabetes, radiological, sleep
Citation: Sharma J, Rajput R, Bhatia M, Arora P and Sood V (2021) Clinical Predictors of COVID-19 Severity and Mortality: A Perspective. Front. Cell. Infect. Microbiol. 11:674277. doi: 10.3389/fcimb.2021.674277
Received: 01 March 2021; Accepted: 28 September 2021;
Published: 25 October 2021.
Edited by:
Heather Shannon Smallwood, University of Tennessee Health Sciences Center, United StatesReviewed by:
Masmudur Mohammed Rahman, Arizona State University, United StatesMatthias Walter, University Hospital Basel, Switzerland
Copyright © 2021 Sharma, Rajput, Bhatia, Arora and Sood. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jitender Sharma, aml0ZW5kZXJzaGFybWEuY2xpbmNoZW1AZ21haWwuY29t; Vikas Sood, di5zb29kQGphbWlhaGFtZGFyZC5hYy5pbg==; dmlrYXMxMTAxQGdtYWlsLmNvbQ==