 Anna Sellarès-Crous1†‡
Anna Sellarès-Crous1†‡ Arturo Martínez-Trejo2,3‡Natàlia Arnalda-Muñoz2Giulia Gatti4Miriam Villanueva-López1
Arturo Martínez-Trejo2,3‡Natàlia Arnalda-Muñoz2Giulia Gatti4Miriam Villanueva-López1 Andrea Vergara-Gómez1,2,3,5
Andrea Vergara-Gómez1,2,3,5 Francesc Marco-Reverté1,2,3Mateu Espasa-Soley1,2,3
Francesc Marco-Reverté1,2,3Mateu Espasa-Soley1,2,3 Jordi Vila-Estapé1,2,3,5*
Jordi Vila-Estapé1,2,3,5*- 1Department of Clinical Microbiology, Hospital Clínic, Barcelona, Spain
- 2Barcelona Institute for Global Health (ISGlobal), Barcelona, Spain
- 3School of Medicine and Health Sciences, University of Barcelona, Barcelona, Spain
- 4Department of Surgical and Medical Sciences (DIMEC), Alma Mater Studiorum-University of Bologna, Bologna, Italy
- 5Centro de Investigación Biomédica en Red (CIBER) de Enfermedades Infecciosas (CIBERINFEC), Instituto Salud Carlos III, Madrid, Spain
Introduction: Hospital-acquired pneumonia (HAP) is a serious infection affecting patients in the hospital setting. This study aimed to evaluate a novel multiplex detection method using loop-mediated isothermal amplification (LAMP) technology to identify six primary bacterial pathogens responsible for HAP directly from respiratory samples.
Methods: A total of 119 clinical samples were analyzed by LAMP technology, including mainly bronchoalveolar lavages, endotracheal aspirates, and bronchoaspirates.
Results and discussion: The results of the LAMP and traditional culture methods showed an accuracy of 93.0%. In some discordant cases between culture and LAMP, multiplex PCR (FilmArray Pneumonia Panel) showed a strong correlation with the LAMP results, confirming the potential use of this technique as a diagnostic detection tool. The clinical sensitivity of the LAMP assay was 93.3% with a specificity of 92.0%. Correlation analysis revealed a weak negative relationship between bacterial load and time to positivity (r = −0.177, p = 0.05). This study underscores the potential of LAMP as a rapid and accurate tool for the diagnosis of HAP, facilitating the turnaround time for microbiology laboratory results, which is critical for improving the outcomes of patients with HAP.
1 Introduction
Hospital-acquired pneumonia (HAP) involves infection of the pulmonary parenchyma, which develops in hospitalized patients within 48 h or more after admission. It is usually caused by microorganisms present in hospital settings. Ventilator-acquired pneumonia (VAP) is a significant subset of HAP, which occurs more than 48 h after endotracheal intubation in patients in an intensive care unit (ICU) (Kalil et al., 2016; Torres et al., 2017).
Healthcare-associated infections (HAIs) are a major public health burden. HAP is the second most common nosocomial infection and the most frequent ICU-acquired infection (including VAP), and it is currently the main cause of death from nosocomial infection in critically ill patients (Blot et al., 2022; Candel et al., 2023). According to the etiological agent, Pseudomonas aeruginosa and Staphylococcus aureus are the main pathogens causing HAP, followed by Klebsiella pneumoniae complex and Escherichia coli (Candel et al., 2023; Gallego-Berciano et al., 2023). The frequency of these pathogens varies between regions and countries. In ICU patients, other non-fermenting Gram-negative bacilli, such as Stenotrophomonas maltophilia and Acinetobacter baumannii, are especially relevant (Torres et al., 2017; Candel et al., 2023; SEMICYUC, 2023).
In patients with nosocomial infections, the selection of initial empiric antibiotic therapy is crucial, particularly when resistant pathogens are involved, as it can significantly affect patient outcomes. The impact of HAIs, especially VAP, on morbidity, mortality, and healthcare costs is well-documented. Delays in administering appropriate therapy have been linked to worse outcomes, extended hospital stays, increased healthcare expenses, and higher mortality rates (Rello, 2007; Kuti et al., 2008; Bonine et al., 2019; Zasowski et al., 2020).
Traditional microbiological tests, such as Gram staining and culture, are time-consuming but remain the standard techniques for the diagnosis of respiratory infections. However, new molecular tests allow reducing the time to achieve results to only hours, enabling rapid diagnosis and facilitating patient management. There are multiple panels for the syndromic diagnosis of respiratory infections, including community-acquired, viral, or upper respiratory tract infections, but fewer panels are available for more invasive infections or those caused by bacteria resulting in HAI (Ramanan et al., 2018; Candel et al., 2023). Most panels are based on real-time polymerase chain reactions (qPCR), but other technologies, such as loop-mediated isothermal amplification (LAMP), are available for the detection of the nucleic acid material of the bacteria.
LAMP was developed in 2000 by Notomi (2000) and is a simple nucleic acid amplification method, which primarily features the amplification of nucleic acids in the sample at a constant temperature. This is achieved using a multiple set of primers that amplify the target present in the sample more efficiently and specifically due to their loop-shaped configuration. Thus, LAMP is used as an alternative to PCR for its more rapid and cost-effective detection of targets in samples and has already been used with good results for diagnosing respiratory infections, among others (Anastasiou et al., 2021; Feleke et al., 2021; Gaber et al., 2022; Jang et al., 2024; Nikolova, 2024). Additionally, LAMP can detect more than one target in a single reaction, thereby facilitating the design of syndromic panels, streamlining workload, and reducing response time in the microbiology laboratory. However, when the number of bacterial targets increases (i.e., multiplexing), there is a higher risk of primer–primer interactions, competition for reagents, and non-specific amplification, which may lead to reduced specificity and lower amplification efficiency for individual targets, ultimately impacting sensitivity. This is particularly relevant in LAMP, which uses multiple primers per target (typically four to six), increasing the complexity of multiplex designs. Conversely, assays with fewer targets typically achieve higher sensitivity and specificity (Notomi, 2000; Zhang et al., 2014; Zhou et al., 2014).
Although several studies have addressed the use of LAMP to individually detect each of the main bacterial pathogens involved in HAP from respiratory specimens (S. aureus, E. coli, P. aeruginosa, S. maltophilia, A. baumannii, and K. pneumoniae) (Lin et al., 2017; Poirier et al., 2022; Ferrusca Bernal et al., 2024), very few have evaluated these pathogens collectively. Thus, the aim of this study was to evaluate a set of pathogens causing HAP using LAMP technology. The detection panel analyzed here contributes to the limited existing literature by providing a broader and more integrated analysis of the use of panels based on LAMP, which have scarcely been investigated previously.
2 Materials and methods
We devised a Swift protocol for the discrimination of six distinct bacteria causing HAP using LAMP technology directly in respiratory samples. The bacteria targeted were E. coli, S. aureus, P. aeruginosa, K. pneumoniae, S. maltophilia, and A. baumannii. Subsequently, we compared the performance of LAMP with traditional culture methods. Our study included different types of specimens: bronchoalveolar lavage (BAL), endotracheal aspirate (EA), bronchoaspirate (BAS), and sputum.
2.1 Sample collection
Positive and negative samples were collected from the Clinical Microbiology Laboratory at the Hospital Clínic in Barcelona, Spain. A large part of the samples was collected between 2022 and 2024. The types and microbiological findings of the samples are presented in Supplementary Table S1.
2.2 Routine microbiological methods
Sterile containers were utilized to collect respiratory specimens, which were then transported to the laboratory for processing within 2 h.
To assess specimen quality, Gram staining of the specimens was performed and evaluated following the Murray–Washington criteria (Murray and Washington, 1975), selecting only good quality samples (grades 4–6) for culture and LAMP analysis. All respiratory samples were Gram-stained to determine the presence of Gram-negative bacilli, Gram-positive cocci or mixed microbiota followed by quantitative culture (blood and chocolate agar). Significant bacterial growth related to respiratory pathogens was quantified and identified utilizing mass spectrometry technology (MALDI-TOF, Bruker Daltonics, Germany). The LAMP assay was further carried out.
2.3 Loop-mediated isothermal amplification
Taking into account the nature of each specimen, viscous and dense samples, including EAs and BAS, were prediluted 1:5 with Sputum Liquefying Solution (SLSolution™, COPAN, Italy) (300 µL of sample plus 1,200 µL of COPAN), a DTT-containing (dithiothreitol) liquefying solution. After gentle vortex and 5 min of incubation (or until fully liquified), 25 µL of the mixture was transferred to a recipient containing 500 µL of RALF buffer for bacterial lysis (AmplexDiagnostics, GmbH, Germany). The sample was then heated for 2 min at 99 °C for DNA extraction, followed by a brief 30-s centrifugation at 13,000 rpm. The supernatant was used for LAMP. Concerning BALs, 25 µL of the specimen was directly transferred to the RALF buffer, and then the previously described protocol was followed (Figure 1).

Figure 1. Respiratory samples for the LAMP measurement workflow. Depending on the physical characteristics of the respiratory sample, a dilution was performed if the specimen was dense, as in the case of endotracheal aspirates and bronchoaspirates. In the case of bronchoalveolar lavage, this step was omitted. The sample was then transferred to a recipient with RALF buffer and incubated for DNA extraction. After spinning, the sample was transferred to the LAMP reaction tubes, and the reaction was performed at 65°C for 25 min. Finally, the results were interpreted.
eazyplex® PneumoBug test strips (AmplexDiagnostics GmbH, Germany) were used, and freeze-dried ready-to-use amplification components detected each bacterial target in individual wells. The wells were rehydrated with 25 µL of the final supernatant mentioned above. The LAMP reaction was performed in the Genie® II Mk2 instrument (AmplexDiagnostics GmbH, Germany) at 65 °C for 25 min.
The following genes were used as targets for species-specific detection: E. coli gene phoA, S. aureus gene femA, P. aeruginosa gene oprL, K. pneumoniae gene phoE, S. maltophilia gene hrpA, and A. baumannii gene encoding the OXA-51 β-lactamase.
2.4 Determination of the limits of detection
The limit of detection (LoD) was calculated for each bacterium included in the test. Bacterial suspensions were performed for each bacterial strain at different concentrations ranging from 106 to 102 colony-forming units (CFUs)/mL. The strains used were S. aureus ATCC 25923, E. coli ATCC 25922, P. aeruginosa ATCC 27853, A. baumannii ATCC 19606, K. pneumoniae ATCC 13883, and a clinical strain of S. maltophilia.
A 0.9% NaCl solution was used as a diluent. To determine the final concentration, the number of CFU was calculated based on the approximate concentration determined by the culture, plating 50 µL of each suspension on TSA agar and incubating at 37 °C for 18 h. After culturing the suspension, the LAMP protocol described above was followed (the use of the mucolytic was omitted), adding 25 µL of bacterial suspension to 500 µL of RALF buffer and following the next steps described for the reaction. Each suspension was analyzed in triplicate. The dilution performed with the RALF buffer was considered for the final CFU/mL determination.
2.5 BioFire® FilmArray® Pneumonia Panel protocol
To analyze discrepancies between culture and LAMP results, the BioFire® FilmArray® Pneumonia Panel Plus v2.0 system (BioFire® Pneumonia Panel Plus 2.0, BioFire Diagnostics, bioMérieux, Marcy l’Étoile, France) was used for microbial identification. Sample processing followed the manufacturer’s instructions. The sample was inoculated into the injection vial using the manufacturer-provided swab, which contains the buffer required for proper homogenization of the sample prior to panel injection. Before sample loading, the reaction panel was pretreated with the hydration solution. Subsequently, the panel was placed into the FilmArray® instrument, in which the reaction was carried out. Each sample was processed individually to maintain analytical integrity.
2.6 Statistical analysis
The sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) as described elsewhere (Altman and Bland, 1994; Park et al., 2024) and the accuracy of the LAMP panel were calculated using the MedCalc software for Windows Ver. 23.0.2 (MedCalc Software, Ostend, Belgium). Major errors were characterized as instances when the microorganism identified by LAMP differed entirely from those identified in culture, or when LAMP failed to detect a pathogen that had grown in culture. Minor errors were described as cases for which the main pathogen was correctly identified, but LAMP also detected additional microorganisms.
A correlation study was performed to determine the association between LAMP detection time and pathogen concentration in the clinical samples, as determined by quantitative culture in clinical samples. Negative samples were excluded, and only cases with the same culture and LAMP results were included. In samples in which multiple microorganisms were detected and culture results aligned with LAMP identification, the values of each microorganism were individually analyzed. Log10 CFU/mL value detection time in total minutes was used for consistency and to ease the result analysis. Data normality was evaluated using the Shapiro–Wilk test, which is adequate for small and moderate sample sizes such as those in the present study, followed by a one-tailed Spearman correlation analysis given that the data obtained did not follow a normal distribution. The p-value for statistical significance was <0.05. Additionally, to observe the statistical dispersion of the detection time, the median and the interquartile range (IQR) for each of the different pathogens detected by LAMP were determined. The statistical analyses were conducted using the R Studio software package (ver. 4.4.3), using the same software for the generation of graphs.
3 Results
3.1 LAMP compared to the standard protocol
A total of 119 respiratory samples were collected: 61 EAs, 43 BAS, 13 BALs, and 2 sputum samples. In 105 out of 119 cases (88.23%), LAMP results were fully concordant with those of conventional culture: in 82 samples, the result was positive in both tests, while in 23 samples, the result was also negative in both assays. Notably, in 7 positive samples, a two- or five-fold dilution with COPAN was required to validate the internal control.
Nine major errors were detected: in six samples, the LAMP result was negative, while the culture was significantly positive; in two samples, the rapid test only detected one of the two microorganisms identified in the culture, and in one sample, the culture result was negative, while molecular detection was positive. On the other hand, in four samples, an additional microorganism was detected by LAMP apart from the microorganism isolated in the culture. In one sample, culture detected Morganella morganii, but the LAMP kit detected S. aureus. These five samples were classified as minor errors (Table 1).

Table 1. Results obtained by eazyplex® PneumoBug HAP test strips according to the results obtained by conventional culture.
3.2 Sensitivity determined by the LoD
The estimated LoD for the bacteria included in the detection test was 2.3 × 103 CFU/mL for S. aureus, 8.6 × 103 CFU/mL for E. coli, 6.7 × 103 CFU/mL for P. aeruginosa, 3.6 × 103 CFU/mL for S. maltophilia, 1 × 105 CFU/mL for A. baumannii, and 9.3 × 103 CFU/mL for K. pneumoniae.
3.3 Additional molecular method to compare LAMP results
Additionally, to elucidate discrepancies between conventional culture and LAMP assay results, six samples were selected for further study. The BioFire® FilmArray® Pneumonia Panel Plus v2.0 system was employed as a second molecular assay. In all six samples with discrepancies, but one, FilmArray® confirmed the results found by LAMP. In the sample that was not confirmed (sample 104), LAMP was positive for P. aeruginosa and S. maltophilia, and FilmArray® only confirmed P. aeruginosa (Table 2).
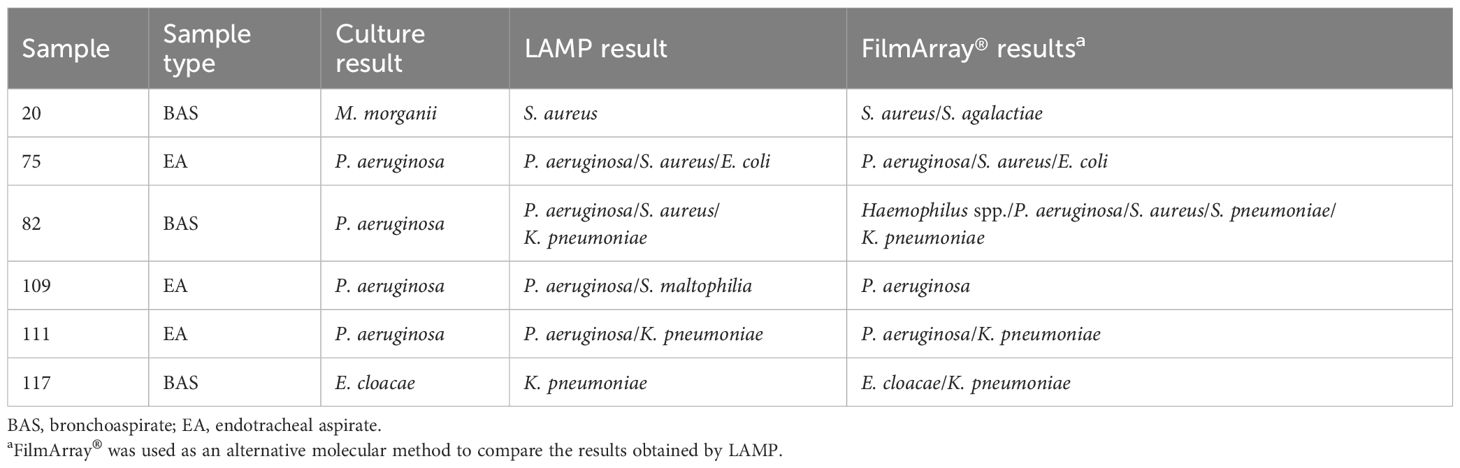
Table 2. Comparison of the results obtained by conventional culture, LAMP, and FilmArray assays in six selected samples.
3.4 Performance of the LAMP detection panel
For the calculation of panel performance, minor errors were considered as true positives, and mixed cultures were excluded. The sensitivity of the test was 93.33%, whereas the specificity was 92.00%. The PPV was 97.67% and the NPV was 79.31%. The accuracy of panel performance was 93.04% with a kappa value of 0.806 (Table 3).
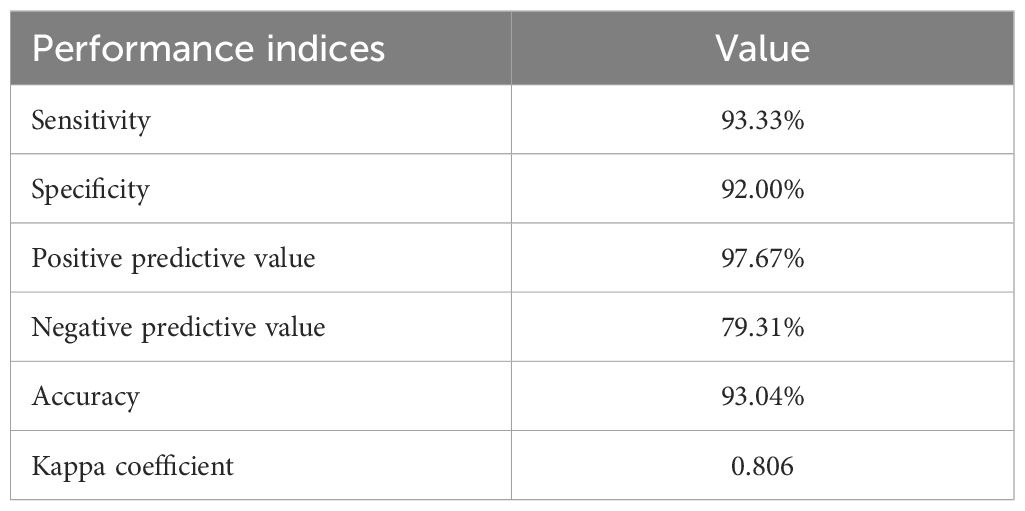
Table 3. Summary of the performance metrics and evaluation results for the diagnostic test assessed.
Among the 119 samples analyzed, the same microorganism was identified in 87 cases by both the LAMP test and the quantitative culture, with a mean detection time of 11.95 min (Q1 = 9.86, Q3 = 14.55). Figure 2 shows the mean and first and third quartiles for each microorganism included in the test. The time of positivity for S. maltophilia presented the highest variability, whereas K. pneumoniae showed the most homogeneous time detection.
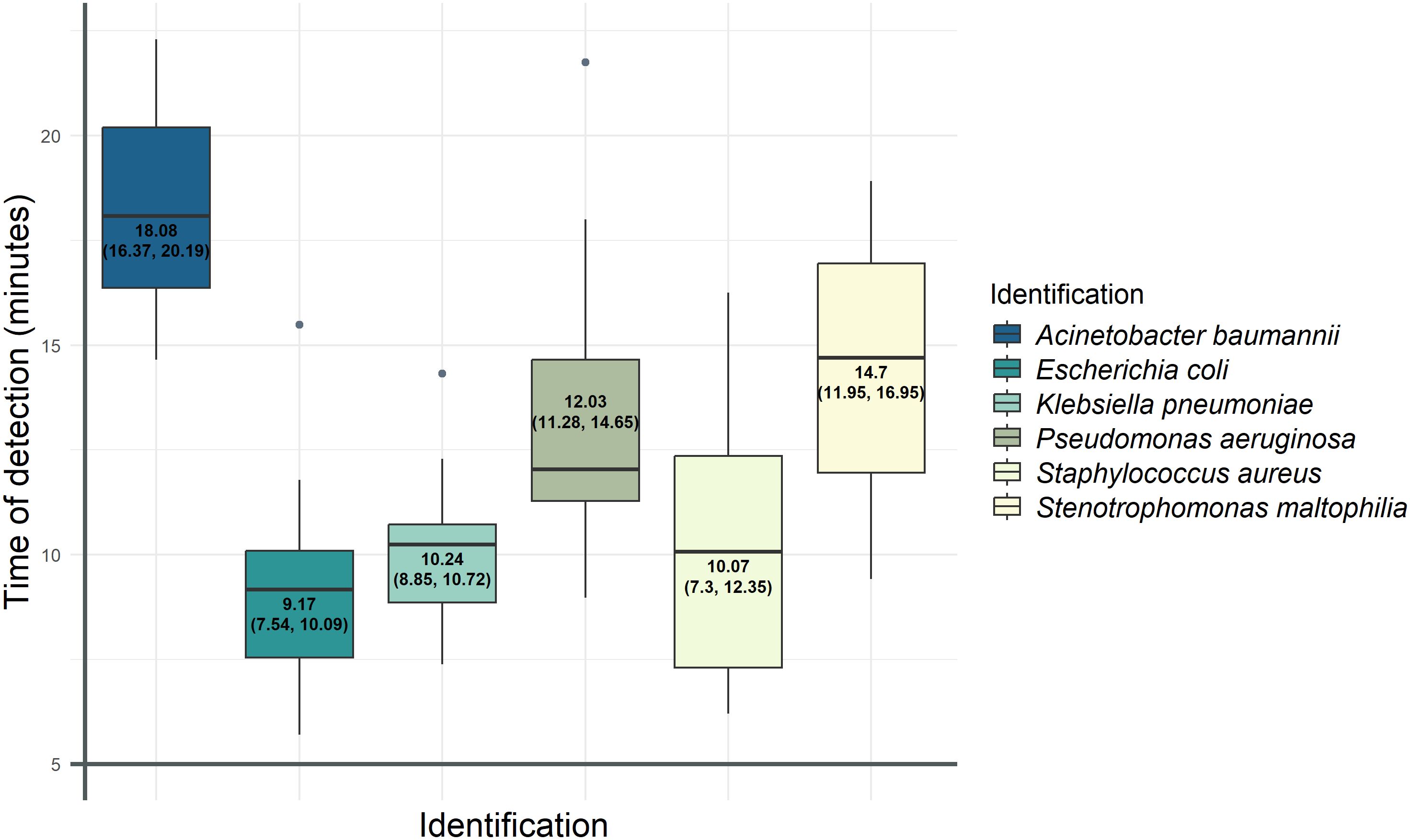
Figure 2. Representation of the media and the first and third quartiles of the positivity time for each bacterium detected by the LAMP technique. For each bacterium detected by LAMP, the mean time of positivity and the IQR were calculated and shown in colored boxes. The values corresponding to the mean, Q1, and Q3 (in brackets) are written inside the boxes. The horizontal line of each of these boxes corresponds to the median detection time; outliers are shown as gray dots.
The results of the correlation analysis showed a weak negative relationship between bacterial concentrations determined by bacteriological culture and detection time by LAMP (r = −0.177, p = 0.0508) (Figure 3).
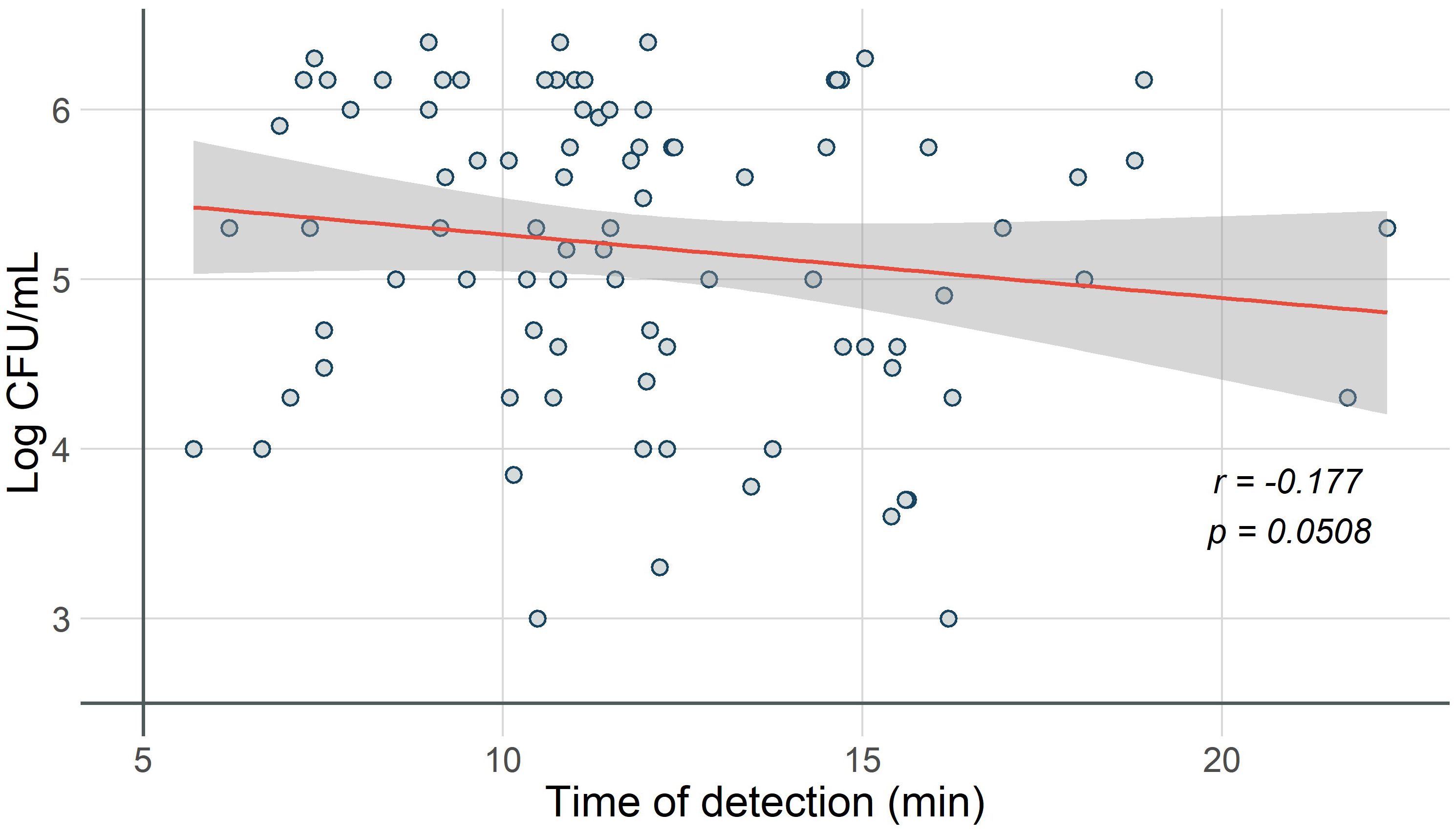
Figure 3. Correlation of time to positivity by LAMP and bacterial load in conventional culture. The correlation between bacterial load (Log CFU/mL) and time to positivity (minutes) is represented in the scatter plot. The trend line shows a weak negative relationship between the variables (r = −0.177, p = 0.0508), and the area with a 95% confidence interval is indicated (gray area).
3.5 Correlating Gram staining with LAMP
Gram staining of respiratory samples was performed as a routine procedure in the microbiology laboratory prior to performing the LAMP assay (Table 4). In 86 (72.3%) samples, the Gram staining results were consistent with those obtained from the LAMP assay: in 41 cases, Gram-negative bacilli were observed and detected; in 4 cases, Gram-positive cocci of the staphylococcal type were observed and detected; in 15 cases, mixed microbiota with a predominance of Gram-negative bacilli was observed and one or two Gram-negative bacilli species were detected; in 6 cases, mixed microbiota with a predominance of Gram-positive cocci was found; and in 20 cases, both the Gram stain and LAMP assay results were negative. On the other hand, in 33 samples, the Gram staining results did not correspond with the LAMP assay findings: in 18 Gram stains that appeared negative, the LAMP assay was positive; in 9 samples with observed mixed microbiota, only one microorganism was detected by the LAMP assay; and in 6 samples in which Gram-negative bacilli were observed, the LAMP assay result was negative. However, when we subsequently compared the data from the LAMP assay results with those from conventional culture, in these discordant GRAM/LAMP cases, we found that in 23 out of 33 cases, the microorganism detected by LAMP corresponded to the same isolate identified in the culture.
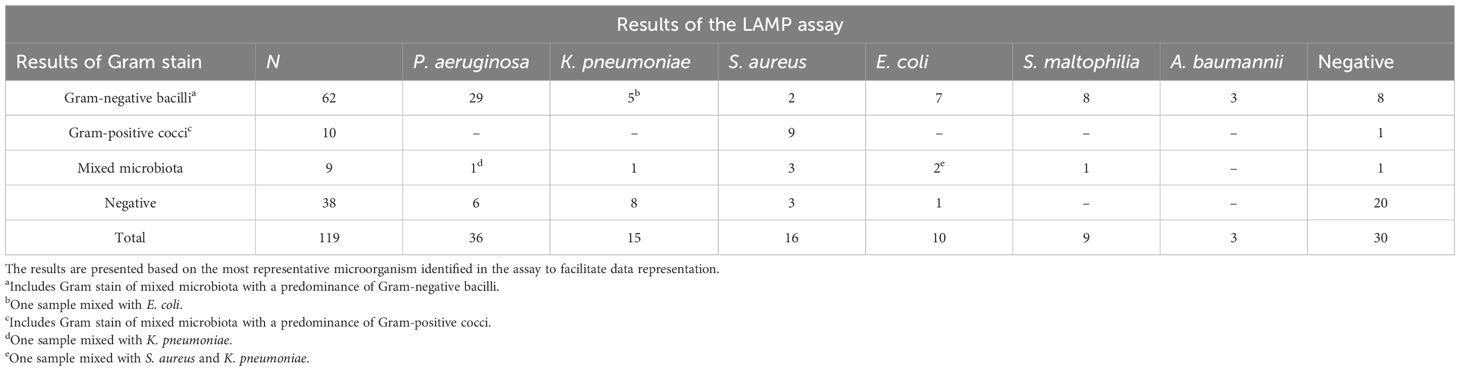
Table 4. Comparison of the results obtained with Gram staining and those from the LAMP assay.
4 Discussion
Despite significant efforts to prevent nosocomial infections, HAP remains the second most common nosocomial infection and the leading cause of death from nosocomial infections in critically ill patients (Kalil et al., 2016; Torres et al., 2017). When pneumonia is suspected, it is crucial to initiate appropriate antibiotic therapy as early as possible, as numerous studies have shown that delays in administering the correct therapy result in worse outcomes, increasing healthcare costs and mortality (Rello, 2007; Kuti et al., 2008; Bonine et al., 2019). Therefore, rapid diagnosis by the microbiology laboratory is essential, and several rapid molecular tests are increasingly shortening turnaround times without sacrificing accuracy.
The LAMP panel used in this study included the main bacteria that can cause HAP. We found an overall accuracy of 93.04% between LAMP and culture, and the different performance metrics and evaluation results analyzed showed a strong overall performance with high sensitivity (93.33%) and specificity (92.0%). The PPV (97.67%) suggests that most positive results were related to true infections. The NPV (79.31%) shows that negative results may not always exclude infection. This could be related to the challenges in detecting pathogens at low concentrations or due to the intrinsic characteristics of the sample, which can affect LAMP performance. A larger sample size could help improve the reliability of this metric. The accuracy and the kappa coefficient (0.8) suggest a strong correlation between this test and the gold standard method (culture). These findings are consistent with the data reported in a previous study that used LAMP for the detection of HAP pathogens, which reported an accuracy of 95.2% and a kappa index of 0.89 (Vergara et al., 2020a). This emphasizes the potential of LAMP for use as a point-of-care test.
The target genes used in the kit for species-specific detection were single genes reported to be useful for correct identification in the literature. In E. coli, the phoA gene is a molecular marker that is well preserved in this species (Elabbasy et al., 2021), while in A. baumannii, the gene encoding OXA-51 is an intrinsic and exclusive gene of this species (Turton et al., 2006). For P. aeruginosa, the oprL gene has been detected in all the strains analyzed in different studies (Chand et al., 2021; Liu et al., 2023). In S. aureus, the femA gene codifies an essential protein exclusively presented in this species (Meng et al., 2020), and for S. maltophilia, the stmPr gene detected has shown to have a high prevalence in clinical strains (Kang et al., 2012). In the case of K. pneumoniae detection, the phoE gene has been widely described for its detection in clinical and environmental samples (Sun et al., 2010; Dong et al., 2015). Thus, the use of these target genes has proven to be a reliable tool for the detection of the pathogens analyzed.
Klebsiella pneumoniae and S. maltophilia were the pathogens in which the most major errors were detected (two each), which could be related to variations in the target genes. In the case of K. pneumoniae, it has been reported that genetic variation of the phoE gene rarely occurs because of antibiotic exposure (Diancourt et al., 2005; Bialek-Davenet et al., 2017). For S. maltophilia, it has been reported that some genes related to virulence, such as hrpA, may present variations in their sequence (Youenou et al., 2015) that could affect the detection performance of the primers used. In addition, the presence of LAMP reaction inhibitors in these clinical samples might explain these non-concordant results.
The major errors detected may be related to the amount of pathogen in the samples in which these errors occurred. The sensitivity according to the calculated LoD of the test shows that the sensitivity is adequate and is within the acceptable range reported in the literature, considering that the test analyzed is a rapid detection test (Burd and Kehl, 2011; Xu et al., 2021). Some of the primers used in this kit were previously analyzed, and their LoD was calculated. In the case of P. aeruginosa and K. pneumoniae, the LoD was 102 CFU/mL, while for E. coli and S. aureus, the LoD was 103 CFU/mL and 104 CFU/mL, respectively (Vergara et al., 2020a). Comparison of these data with our results indicates similarity. However, in the present study, the LoD calculated for P. aeruginosa and K. pneumoniae was one-fold higher (103 CFU/mL); in E. coli, the LoD range was the same (103 CFU/mL), and the LoD calculated in S. aureus was one-fold lower. This could be related to technical and biological factors, such as the device used for the reaction and result analysis. Here, we used a device designed exclusively for use with this kit, and the previously mentioned study used a thermocycler. Furthermore, matrix effects may have influenced detection sensitivity; while the previous study used spiked samples, we used a bacterial suspension made with saline solution. In addition, variations in the LAMP protocol, such as the volumes and concentrations used, may have influenced the different LoDs determined.
It is possible that the pathogen concentrations in the samples in which major errors were detected were low, and this could affect the quantity of DNA extracted, considering that a simple DNA extraction was performed. Moreover, the physical characteristics of the sample could affect the LAMP results. As shown in Table 2, all the samples with discrepancies between LAMP and culture results were EA or BAS, which are generally viscous and dense. These characteristics may hinder the effectiveness of the pretreatment done, making it insufficient to fully liquefy the sample, thereby affecting the LAMP results.
It is important to mention that the target panel must be adapted according to the local epidemiology of each hospital ICU and region (Stewart et al., 2021) to cover all the most prevalent pathogens. One limitation of syndromic panels is that they only detect the microorganisms included in the panel, and thus, additional tests or assays may be needed to complement the study. Therefore, it is important to select or design panels that cover the most prevalent microorganisms in our environment. In this sense, it was difficult to collect positive samples for A. baumannii for this study, as it is not a very common pathogen in the ICUs of our hospital. Another limitation of this study was the number of samples. For some pathogens, the number of cases isolated was low, and for some sample types such as sputum, the number of samples processed was also low. Having more information about this type of sample is relevant because it may help improve the processing of these non-invasive samples.
An additional interesting study would be to perform a second LAMP assay, after the microorganism causing the infection is known, to determine whether the microorganism carries any known antibiotic resistance mechanisms (extended-spectrum beta-lactamases, carbapenemases, resistance to methicillin, etc.), as done in previous studies (Vergara et al., 2014, 2020b). In the current epidemiological scenario, a significant portion of nosocomial and HAP cases are caused by multidrug-resistant microorganisms (Candel et al., 2023).
The samples used for the validation study in the present study were retrospective; however, the use of prospective samples would help assess the clinical impact of the diagnostic method used. While it may not be cost-effective to use the LAMP test in all samples received in the laboratory, determining which patient populations would most benefit from early diagnosis could be helpful. Gram staining followed by LAMP testing in positive stains could be useful. As observed in this study, in 86 out of 119 cases, the Gram stain result effectively predicted the outcome obtained by the LAMP technique or conventional culture results. These findings support the use of Gram staining as a useful initial screening method for predicting subsequent microbiological outcomes in respiratory samples, which, in addition, would also be more economical. The discrepancies between Gram staining and LAMP findings may stem from the inherent subjectivity and technical sensitivity of Gram staining, especially for respiratory specimens, where studies report up to 42% discordance with culture results (Samuel et al., 2016). In addition, automated systems may reduce variability but still show discrepancies (Froböse et al., 2020). In contrast, LAMP amplifies bacterial DNA directly, allowing the detection of both viable and non-viable organisms with high analytical sensitivity and specificity (Sadeghi et al., 2021). Thus, LAMP-positive/Gram-negative or LAMP-negative/Gram-positive results can reflect true differences in bacterial state or limitations of each method, underscoring the value of combining both approaches for comprehensive diagnosis.
Although the LAMP method does not provide a quantitative measurement of the pathogen, the time LAMP required for achieving a positive result provides a relative estimate of microorganism quantity as observed in this study. However, factors other than bacterial load may affect the detection time, and therefore, it cannot be used as a semiquantitative measure of the pathogen load of a sample. According to our results, most targets were detected within the first 15 min. In other cases, LAMP detected a secondary microorganism not identified by culture: the primary microorganism in the culture samples was isolated in large quantities, possibly masking the lower counts of the secondary microorganism. Other factors, such as the inability of certain microorganisms to grow in culture media or prior antibiotic treatment administered to the patient before sample collection, could affect the LAMP results, similar to what is reported with other molecular techniques (Driscoll et al., 2017; Harris et al., 2017). Notably, these discrepancies could be related to the sensitivity of the LAMP technique, which could be higher compared to culture. This is further supported by the results of FilmArray®, which is able to detect a wider range of pathogens than LAMP. This could support the hypothesis that the lack of bacterial growth may be related to factors inhibiting growth, such as previous antibiotic treatment.
Several respiratory syndromic panels based on molecular techniques are available today (Dien Bard and McElvania, 2020; Lade et al., 2022). One advantage of the LAMP technology is its low cost and reduced turnaround time. In previous studies, the cost of the LAMP assay to detect six pathogens was calculated to be 12 euros with a total turnaround time of circa 4 h (Vergara et al., 2020b). Other multiplex panels available are based on PCR, and the sensitivity and specificity of molecular techniques vary widely (Ramanan et al., 2018; Candel et al., 2023). FilmArray® (bioMérieux®, Marcy-l’Étoile, France) can simultaneously detect 15 bacteria in a nested-multiplex rt-qPCR, with a turnaround time of 1 h and an estimated cost of 155 euros per sample (Ferrer et al., 2023). In previous studies, the overall sensitivity of FilmArray® for respiratory samples ranged from 75% to 100%, while the specificity varied between 88.9% and 99.5% (Murphy et al., 2020; Enne et al., 2022; Kamel et al., 2022). Unyvero™ HPN (Hospitalized Pneumonia) (Curetis, Holzgerlingen, Germany) enables rapid identification of 29 microorganisms and 19 resistance genes within a turnaround time of 6–8 h, with an overall sensitivity ranging from 55.6% to 100% and a specificity from 14.3% to 99% depending on different factors and the version of the panel (Luyt et al., 2020; Peiffer-Smadja et al., 2020; Darie et al., 2022; Enne et al., 2022). Nevertheless, many of the other panels available primarily focus on identifying viral infections, community-acquired pneumonias, or atypical pneumonias, rather than HAPs (Ramanan et al., 2018; Candel et al., 2023). Moreover, testing frequently relies on nasopharyngeal swabs rather than the more invasive sample types such as those used in this study. This is relevant because invasive samples can generally provide more precise information about the infection since they may contain a higher concentration of the causative pathogen and reduce the presence of the upper airway microbiota, improving diagnostic reliability.
5 Conclusions
This study demonstrates that performing the LAMP technique directly on respiratory samples offers a rapid, straightforward, and cost-effective method for identifying the primary bacterial pathogens responsible for HAP. By significantly reducing the time to diagnosis compared to conventional microbiological methods, this approach enables earlier and more targeted antimicrobial therapy. Timely initiation of appropriate treatment is associated with improved patient outcomes, shorter hospital stays, and reduced healthcare costs. Furthermore, integrating such rapid diagnostic tools into clinical workflows can support antimicrobial stewardship efforts by minimizing the empirical use of broad-spectrum antibiotics. These findings underscore the practical value of LAMP as a point-of-care diagnostic tool, with direct implications for frontline healthcare professionals managing hospital-acquired pneumonia.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by the Ethics Committee of the Hospital Clínic of Barcelona, Spain, HCB/2023/0652. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin because we used leftovers of the samples that were submitted to the clinical microbiology laboratory. The samples were not specifically collected for this study.
Author contributions
JV-E: Conceptualization, Methodology, Validation, Writing – review & editing, Supervision, Funding acquisition. AS-C: Conceptualization, Methodology, Validation, Formal analysis, Investigation, Data curation, Writing – original draft, Visualization. AM-T: Conceptualization, Methodology, Validation, Formal analysis, Investigation, Data curation, Writing – original draft, Visualization. NA-M: Investigation, Writing – review & editing. GG: Investigation, Writing – review & editing. MV-L: Resources, Writing – review & editing. AV-G: Conceptualization, Methodology, Validation, Resources, Writing – review & editing, Supervision. FM-R: Resources, Writing – review & editing. ME-S: Writing – review & editing.
Funding
The author(s) declare financial support was received for the research and/or publication of this article. ISGlobal (CEX2018-000806-S) is a recipient of a Severo Ochoa Award of Excellence from MINECO (Government of Spain). ISGlobal acknowledges support from the Generalitat de Catalunya through the CERCA Program. This work was also supported by the Instituto de Salud Carlos III (Carlos III Institute of Health) (PI23/01537); award 2021SGR01569 from the Agència de Gestió d’Ajuts Universitaris i de Recerca of the Generalitat de Catalunya (Agency for Management of University and Research Grants of the Catalan Government).
Acknowledgments
AM-T received grant-aided support from the “Secretaría de Ciencia, Humanidades, Tecnología e Innovación (SECIHTI)” [former “Consejo Nacional de Humanidades, Ciencias y Tecnologías” (CONAHCyT)] from Mexico. The PhD scholarship of GG was funded by the European Union—NextGenerationEU through the Italian Ministry of University and Research under PNRR—Mission 4 Component 2, Investment 3.3 “Partnerships extended to universities, research centers, companies and funding of basic research projects” D.M. 352/2021—CUP J33C22001330009.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcimb.2025.1609666/full#supplementary-material
References
Altman, D. G. and Bland, J. M. (1994). Diagnostic tests. 1: Sensitivity and specificity. BMJ 308, 1552. doi: 10.1136/bmj.308.6943.1552
Anastasiou, O. E., Holtkamp, C., Schäfer, M., Schön, F., Eis-Hübinger, A. M., and Krumbholz, A. (2021). Fast detection of SARS-coV-2 RNA directly from respiratory samples using a loop-mediated isothermal amplification (LAMP) test. Viruses 13, 801. doi: 10.3390/v13050801
Bialek-Davenet, S., Mayer, N., Vergalli, J., Duprilot, M., Brisse, S., Pagès, J.-M., et al. (2017). In-vivo loss of carbapenem resistance by extensively drug-resistant Klebsiella pneumoniae during treatment via porin expression modification. Sci. Rep. 7, 6722. doi: 10.1038/s41598-017-06503-6
Blot, S., Ruppé, E., Harbarth, S., Asehnoune, K., Poulakou, G., Luyt, C.-E., et al. (2022). Healthcare-associated infections in adult intensive care unit patients: Changes in epidemiology, diagnosis, prevention and contributions of new technologies. Intensive Crit. Care Nurs. 70, 103227. doi: 10.1016/j.iccn.2022.103227
Bonine, N. G., Berger, A., Altincatal, A., Wang, R., Bhagnani, T., Gillard, P., et al. (2019). Impact of delayed appropriate antibiotic therapy on patient outcomes by antibiotic resistance status from serious gram-negative bacterial infections. Am. J. Med. Sci. 357, 103–110. doi: 10.1016/j.amjms.2018.11.009
Burd, E. M. and Kehl, K. S. (2011). A critical appraisal of the role of the clinical microbiology laboratory in the diagnosis of urinary tract infections. J. Clin. Microbiol. 49, S34–S38. doi: 10.1128/JCM.00788-11
Candel, F. J., Salavert, M., Estella, A., Ferrer, M., Ferrer, R., Gamazo, J. J., et al. (2023). Ten issues to update in nosocomial or hospital-acquired pneumonia: an expert review. J. Clin. Med. 12, 6526. doi: 10.3390/jcm12206526
Chand, Y., Khadka, S., Sapkota, S., Sharma, S., Khanal, S., Thapa, A., et al. (2021). Clinical Specimens are the Pool of Multidrug- resistant Pseudomonas aeruginosa Harbouring oprL and toxA Virulence Genes: Findings from a Tertiary Hospital of Nepal. Emerg. Med. Int. 2021, 4120697. doi: 10.1155/2021/4120697
Darie, A. M., Khanna, N., Jahn, K., Osthoff, M., Bassetti, S., Osthoff, M., et al. (2022). Fast multiplex bacterial PCR of bronchoalveolar lavage for antibiotic stewardship in hospitalised patients with pneumonia at risk of Gram-negative bacterial infection (Flagship II): a multicentre, randomised controlled trial. Lancet Respir. Med. 10, 877–887. doi: 10.1016/S2213-2600(22)00086-8
Diancourt, L., Passet, V., Verhoef, J., Grimont, P. A. D., and Brisse, S. (2005). Multilocus sequence typing of klebsiella pneumoniae nosocomial isolates. J. Clin. Microbiol. 43, 4178–4182. doi: 10.1128/jcm.43.8.4178-4182.2005
Dien Bard, J. and McElvania, E. (2020). Panels and syndromic testing in clinical microbiology. Clin. Lab. Med. 40, 393–420. doi: 10.1016/j.cll.2020.08.001
Dong, D., Liu, W., Li, H., Wang, Y., Li, X., Zou, D., et al. (2015). Survey and rapid detection of Klebsiella pneumoniae in clinical samples targeting the rcsA gene in Beijing, China. Front. Microbiol. 6. doi: 10.3389/fmicb.2015.00519
Driscoll, A. J., Deloria Knoll, M., Hammitt, L. L., Baggett, H. C., Brooks, W. A., Feikin, D. R., et al. (2017). The effect of antibiotic exposure and specimen volume on the detection of bacterial pathogens in children with pneumonia. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc Am. 64, S368–S377. doi: 10.1093/cid/cix101
Elabbasy, M. T., Hussein, M. A., Algahtani, F. D., Abd El-Rahman, G. I., Morshdy, A. E., Elkafrawy, I. A., et al. (2021). MALDI-TOF MS Based Typing for Rapid Screening of Multiple Antibiotic Resistance E. coli and Virulent Non-O157 Shiga Toxin-Producing E. coli Isolated from the Slaughterhouse Settings and Beef Carcasses. Foods 10, 820. doi: 10.3390/foods10040820
Enne, V. I., Aydin, A., Baldan, R., Owen, D. R., Richardson, H., Ricciardi, F., et al. (2022). Multicentre evaluation of two multiplex PCR platforms for the rapid microbiological investigation of nosocomial pneumonia in UK ICUs: the INHALE WP1 study. Thorax 77, 1220–1228. doi: 10.1136/thoraxjnl-2021-216990
Feleke, D. G., Alemu, Y., and Yemanebirhane, N. (2021). Performance of rapid diagnostic tests, microscopy, loop-mediated isothermal amplification (LAMP) and PCR for malaria diagnosis in Ethiopia: a systematic review and meta-analysis. Malar. J. 20, 384. doi: 10.1186/s12936-021-03923-8
Ferrer, J., Clari, M.Á., Giménez, E., Carbonell, N., Torres, I., Blasco, M. L., et al. (2023). The Biofire® Filmarray® Pneumonia Plus panel for management of lower respiratory tract infection in mechanically-ventilated patients in the COVID-19 era: a diagnostic and cost-benefit evaluation. Diagn. Microbiol. Infect. Dis. 105, 115847. doi: 10.1016/j.diagmicrobio.2022.115847
Ferrusca Bernal, D., Mosqueda, J., Pérez-Sánchez, G., Chávez, J. A. C., Neri Martínez, M., Rodríguez, A., et al. (2024). Loop-mediated isothermal amplification coupled with reverse line blot hybridization for the detection of pseudomonas aeruginosa. Microorganisms 12, 2316. doi: 10.3390/microorganisms12112316
Froböse, N. J., Bjedov, S., Schuler, F., Kahl, B. C., Kampmeier, S., and Schaumburg, F. (2020). Gram staining: a comparison of two automated systems and manual staining. J. Clin. Microbiol. 58, e01914–e01920. doi: 10.1128/JCM.01914-20
Gaber, M., Ahmad, A. A., El-Kady, A. M., Tolba, M., Suzuki, Y., Mohammed, S. M., et al. (2022). Dengue fever as a reemerging disease in upper Egypt: Diagnosis, vector surveillance and genetic diversity using RT-LAMP assay. PloS One 17, e0265760. doi: 10.1371/journal.pone.0265760
Gallego-Berciano, P., Parra, L. M., Gallego-Munuera, M., Cantero, M., León-Gómez, I., Sastre-García, M., et al. (2023). Encuesta de prevalencia de las infecciones relacionadas con la asistencia sanitaria y uso de antimicrobianos en los hospitales de Españ. Bol. Epidemiológico Sem. 31, 113–132. doi: 10.4321/s2173-92772023000200005
Harris, A. M., Bramley, A. M., Jain, S., Arnold, S. R., Ampofo, K., Self, W. H., et al. (2017). Influence of antibiotics on the detection of bacteria by culture-based and culture-independent diagnostic tests in patients hospitalized with community-acquired pneumonia. Open Forum Infect. Dis. 4, ofx014. doi: 10.1093/ofid/ofx014
Jang, W. S., Park, S., Bae, J. H., Yoon, S. Y., Lim, C. S., and Cho, M.-C. (2024). Development of a multiplex Loop-Mediated Isothermal Amplification (LAMP) for the diagnosis of bacterial periprosthetic joint infection. PloS One 19, e0302783. doi: 10.1371/journal.pone.0302783
Kalil, A. C., Metersky, M. L., Klompas, M., Muscedere, J., Sweeney, D. A., Palmer, L. B., et al. (2016). Management of adults with hospital-acquired and ventilator-associated pneumonia: 2016 clinical practice guidelines by the infectious diseases society of america and the american thoracic society. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc Am. 63, e61–e111. doi: 10.1093/cid/ciw353
Kamel, N. A., Alshahrani, M. Y., Aboshanab, K. M., and El Borhamy, M. I. (2022). Evaluation of the BioFire FilmArray Pneumonia Panel Plus to the Conventional Diagnostic Methods in Determining the Microbiological Etiology of Hospital-Acquired Pneumonia. Biology. 11, 377. doi: 10.3390/biology11030377
Kang, Y., Deng, R., Wang, C., Deng, T., Peng, P., Cheng, X., et al. (2012). Etiologic diagnosis of lower respiratory tract bacterial infections using sputum samples and quantitative loop-mediated isothermal amplification. PloS One 7, e38743. doi: 10.1371/journal.pone.0038743
Kuti, E. L., Patel, A. A., and Coleman, C. I. (2008). Impact of inappropriate antibiotic therapy on mortality in patients with ventilator-associated pneumonia and blood stream infection: a meta-analysis. J. Crit. Care 23, 91–100. doi: 10.1016/j.jcrc.2007.08.007
Lade, H., Kim, J.-M., Chung, Y., Han, M., Mo, E.-K., and Kim, J.-S. (2022). Comparative evaluation of allplex respiratory panels 1, 2, 3, and bioFire filmArray respiratory panel for the detection of respiratory infections. Diagnostics 12, 9. doi: 10.3390/diagnostics12010009
Lin, Q., Xu, P., Li, J., Chen, Y., and Feng, J. (2017). Direct bacterial loop-mediated isothermal amplification detection on the pathogenic features of the nosocomial pathogen – Methicillin resistant Staphylococcus aureus strains with respiratory origins. Microb. Pathog. 109, 183–188. doi: 10.1016/j.micpath.2017.05.044
Liu, S., Huang, S., Li, F., Sun, Y., Fu, J., Xiao, F., et al. (2023). Rapid detection of Pseudomonas aeruginosa by recombinase polymerase amplification combined with CRISPR-Cas12a biosensing system. Front. Cell. Infect. Microbiol. 13. doi: 10.3389/fcimb.2023.1239269
Luyt, C.-E., Hékimian, G., Bonnet, I., Bréchot, N., Schmidt, M., Robert, J., et al. (2020). Usefulness of point-of-care multiplex PCR to rapidly identify pathogens responsible for ventilator-associated pneumonia and their resistance to antibiotics: an observational study. Crit. Care 24, 378. doi: 10.1186/s13054-020-03102-2
Meng, X., Zhang, G., Sun, B., Liu, S., Wang, Y., Gao, M., et al. (2020). Rapid Detection of mecA and femA Genes by Loop-Mediated Isothermal Amplification in a Microfluidic System for Discrimination of Different Staphylococcal Species and Prediction of Methicillin Resistance. Front. Microbiol. 11. doi: 10.3389/fmicb.2020.01487
Murphy, C. N., Fowler, R., Balada-Llasat, J. M., Carroll, A., Stone, H., Akerele, O., et al. (2020). Multicenter Evaluation of the BioFire FilmArray Pneumonia/Pneumonia Plus Panel for Detection and Quantification of Agents of Lower Respiratory Tract Infection. J. Clin. Microbiol. 58, e00128-20. doi: 10.1128/JCM.00128-20
Murray, P. R. and Washington, J. A. (1975). Microscopic and baceriologic analysis of expectorated sputum. Mayo Clin. Proc. 50, 339–344.
Nikolova, E. (2024). Application of lamp as a point-of-care diagnostic assay in remote and low-income regions: mini-review. Acta Med. Bulg. 51, 53–57. doi: 10.2478/amb-2024-0020
Notomi, T. (2000). Loop-mediated isothermal amplification of DNA. Nucleic Acids Res. 28, 63e–663. doi: 10.1093/nar/28.12.e63
Park, C., Park, S. Y., Kim, H. J., and Shin, H. J. (2024). Statistical methods for comparing predictive values in medical diagnosis. Korean J. Radiol. 25, 656–661. doi: 10.3348/kjr.2024.0049
Peiffer-Smadja, N., Bouadma, L., Mathy, V., Allouche, K., Patrier, J., Reboul, M., et al. (2020). Performance and impact of a multiplex PCR in ICU patients with ventilator-associated pneumonia or ventilated hospital-acquired pneumonia. Crit. Care Lond. Engl. 24, 366. doi: 10.1186/s13054-020-03067-2
Poirier, A. C., Kuang, D., Siedler, B. S., Borah, K., Mehat, J. W., Liu, J., et al. (2022). Development of loop-mediated isothermal amplification rapid diagnostic assays for the detection of klebsiella pneumoniae and carbapenemase genes in clinical samples. Front. Mol. Biosci. 8. doi: 10.3389/fmolb.2021.794961
Ramanan, P., Bryson, A. L., Binnicker, M. J., Pritt, B. S., and Patel, R. (2018). Syndromic panel-based testing in clinical microbiology. Clin. Microbiol. Rev. 31, e00024–e00017. doi: 10.1128/CMR.00024-17
Rello, J. (2007). Importance of appropriate initial antibiotic therapy and de-escalation in the treatment of nosocomial pneumonia. Eur. Respir. Rev. 16, 33–39. doi: 10.1183/09059180.00010302
Sadeghi, Y., Kananizadeh, P., Moghadam, S. O., Alizadeh, A., Pourmand, M. R., Mohammadi, N., et al. (2021). The sensitivity and specificity of loop-mediated isothermal amplification and PCR methods in detection of foodborne microorganisms: A systematic review and meta-analysis. Iran. J. Public Health 50, 2172–2182. doi: 10.18502/ijph.v50i11.7571
Samuel, L. P., Balada-Llasat, J. M., Harrington, A., and Cavagnolo, R. (2016). Multicenter assessment of Gram stain error rates. J. Clin. Microbiol. 54, 1442–1447. doi: 10.1128/JCM.03066-15
SEMICYUC (2023). ENVIN. Semicyuc. Available online at: https://semicyuc.org/envin/ (Accessed March 31, 2025).
Stewart, S., Robertson, C., Pan, J., Kennedy, S., Dancer, S., Haahr, L., et al. (2021). Epidemiology of healthcare-associated infection reported from a hospital-wide incidence study: considerations for infection prevention and control planning. J. Hosp. Infect. 114, 10–22. doi: 10.1016/j.jhin.2021.03.031
Sun, F., Wu, D., Qiu, Z., Jin, M., Wang, X., and Li, J. (2010). Development of real-time PCR systems based on SYBR Green for the specific detection and quantification of Klebsiella pneumoniae in infant formula. Food Control 21, 487–491. doi: 10.1016/j.foodcont.2009.07.014
Torres, A., Niederman, M. S., Chastre, J., Ewig, S., Fernandez-Vandellos, P., Hanberger, H., et al. (2017). International ERS/ESICM/ESCMID/ALAT guidelines for the management of hospital-acquired pneumonia and ventilator-associated pneumonia: Guidelines for the management of hospital-acquired pneumonia (HAP)/ventilator-associated pneumonia (VAP) of the European Respiratory Society (ERS), European Society of Intensive Care Medicine (ESICM), European Society of Clinical Microbiology and Infectious Diseases (ESCMID) and Asociación Latinoamericana del Tórax (ALAT). Eur. Respir. J. 50, 1700582. doi: 10.1183/13993003.00582-2017
Turton, J. F., Woodford, N., Glover, J., Yarde, S., Kaufmann, M. E., and Pitt, T. L. (2006). Identification of Acinetobacter baumannii by Detection of the blaOXA-51-like Carbapenemase Gene Intrinsic to This Species. J. Clin. Microbiol. 44, 2974–2976. doi: 10.1128/JCM.01021-06
Vergara, A., Boutal, H., Ceccato, A., López, M., Cruells, A., Bueno-Freire, L., et al. (2020a). Assessment of a loop-mediated isothermal amplification (LAMP) assay for the rapid detection of pathogenic bacteria from respiratory samples in patients with hospital-acquired pneumonia. Microorganisms 8, 103. doi: 10.3390/microorganisms8010103
Vergara, A., Moreno-Morales, J., Roca, I., Pitart, C., Kostyanev, T., Rodriguez-Baño, J., et al. (2020b). A comparative study between real-time PCR and loop-mediated isothermal amplification to detect carbapenemase and/or ESBL genes in Enterobacteriaceae directly from bronchoalveolar lavage fluid samples. J. Antimicrob. Chemother. 75, 1453–1457. doi: 10.1093/jac/dkaa031
Vergara, A., Zboromyrska, Y., Mosqueda, N., Morosini, M. I., García-Fernández, S., Roca, I., et al. (2014). Evaluation of a loop-mediated isothermal amplification-based methodology to detect carbapenemase carriage in Acinetobacter clinical isolates. Antimicrob. Agents Chemother. 58, 7538–7540. doi: 10.1128/AAC.03870-14
Xu, R., Deebel, N., Casals, R., Dutta, R., and Mirzazadeh, M. (2021). A new gold rush: A review of current and developing diagnostic tools for urinary tract infections. Diagnostics 11, 479. doi: 10.3390/diagnostics11030479
Youenou, B., Favre-Bonté, S., Bodilis, J., Brothier, E., Dubost, A., Muller, D., et al. (2015). Comparative genomics of environmental and clinical stenotrophomonas maltophilia strains with different antibiotic resistance profiles. Genome Biol. Evol. 7, 2484–2505. doi: 10.1093/gbe/evv161
Zasowski, E. J., Bassetti, M., Blasi, F., Goossens, H., Rello, J., Sotgiu, G., et al. (2020). A systematic review of the effect of delayed appropriate antibiotic treatment on the outcomes of patients with severe bacterial infections. Chest 158, 929–938. doi: 10.1016/j.chest.2020.03.087
Zhang, X., Lowe, S. B., and Gooding, J. J. (2014). Brief review of monitoring methods for loop-mediated isothermal amplification (LAMP). Biosensors Bioelectronics 61, 491–499. doi: 10.1016/j.bios.2014.05.039
Keywords: hospital-acquired pneumonia, LAMP, rapid diagnostic test, pathogen detection, respiratory samples
Citation: Sellarès-Crous A, Martínez-Trejo A, Arnalda-Muñoz N, Gatti G, Villanueva-López M, Vergara-Gómez A, Marco-Reverté F, Espasa-Soley M and Vila-Estapé J (2025) Assessment of a rapid diagnostic test based on loop-mediated isothermal amplification (LAMP) to identify the most frequent pathogens causing hospital-acquired pneumonia. Front. Cell. Infect. Microbiol. 15:1609666. doi: 10.3389/fcimb.2025.1609666
Received: 10 April 2025; Accepted: 12 August 2025;
Published: 08 September 2025.
Edited by:
Sherry Dunbar, Luminex, United StatesReviewed by:
Mohammad Tahir Siddiqui, Indian Institute of Technology Delhi, IndiaNazente Atçeken, Koç University, Türkiye
Copyright © 2025 Sellarès-Crous, Martínez-Trejo, Arnalda-Muñoz, Gatti, Villanueva-López, Vergara-Gómez, Marco-Reverté, Espasa-Soley and Vila-Estapé. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jordi Vila-Estapé, anZpbGFAY2xpbmljLmNhdA==
†Present address: Anna Sellarès-Crous, CLILAB Diagnòstics, Consorci del Laboratori Intercomarcal de l’Alt Penedès, l’Anoia i el Garraf, Vilafranca del Penedès, Barcelona, Spain
‡These authors have contributed equally to this work and share first authorship